Utah was one of the first states to begin reporting antigen tests back in early August. The state is also one of only three to report an antigen testing time series, rather than simply the total number of tests conducted. However, the format in which Utah presents these data is… challenging.
Rather than reporting daily antigen test counts—or daily PCR test counts, for that matter—in a table or downloadable spreadsheet, Utah requires users to hover over an interactive chart in an extremely precise fashion. Interactive charts are useful for visualizing data, but far from ideal for accessibility.
Hot tip for anyone interacting with this chart: you can make your life easier by clicking “Compare data on hover,” toggling the chart to show all four of its daily data points at once. (Sad story: I did not learn this strategy until I’d already spent an hour carefully zooming in and around the chart to record all of Utah’s antigen test numbers.)
In related news: keep an eye out for a COVID Tracking Project blog post on antigen testing, likely to be published in the coming week.
Dear Pandemic: This source describes itself as “a website where bona fide nerdy girls post real info on COVID-19.” It operates as a well-organized FAQ page on the science of COVID-19, run by an all-female team of researchers and clinicians.
Mutual Aid Disaster Relief: This past spring saw an explosion of mutual aid groups across the country, as people helped their neighbors with food, medical supplies, and other needs in the absence of government-sponsored aid. These groups may no longer be in the spotlight, but as federal relief bills continue to stall, they still need support. Organizations like Mutual Aid Disaster Relief can help you find a mutual aid group in your area.
I drew on my experience managing Stacker’s COVID-19 coverage and volunteering for the COVID Tracking Project to explain common COVID-19 metrics, principles, and data sources. The story starts off pretty simple (differentiating between confirmed and probable COVID-19 cases), then delves into the complexities of reporting on testing, outcomes, and more. As a reader of this newsletter, you likely already know much of the information in the story, but it may be a good article to forward to friends and family members who don’t follow COVID-19 data quite so closely.
(I also made a custom graphic for the “seven-day average cases” slide, which was a fun test of my burgeoning Tableau skills.)
The CDC was busy last week. In addition to their vaccination playbook, the agency released indicators for COVID-19 in schools intended to help school administrators make decisions about the safety of in-person learning. The indicators provide a five-tier system, from “lowest risk of transmission” (under 5 cases per 100,000 people, under 3% test positivity) to “highest risk” (over 200 cases per 100,000 people, over 10% test positivity). It is unclear what utility these guidelines will have for the many school districts that have already started their fall semesters, but, uh, maybe New York City can use them?
Speaking of New York: the state’s dashboard on COVID-19 in schools that I described in last week’s issue is now live. Users can search for a specific school district, then view case and test numbers for that district’s students and staff. At least, they should be able to; many districts, including New York City, are not yet reporting data. (The NYC district page reports zeros for all values as of my sending this issue.)
Los Angeles Unified, the nation’s second-largest school district, is building its own dashboard, the Los Angeles Times reported last week. The district plans to open for in-person instruction in November or later, at which point all students and staff will be tested for COVID-19. Test results down to the classroom level will be available on a public dashboard.
Wisconsin journalists have stepped in to monitor COVID-19 outbreaks in schools, as the state has so far failed to report these data. A public dashboard available via the Milwaukee Journal Sentinel and the USA Today Network allows users to see case counts and resulting quarantine and cleaning actions at K-12 schools across the state. Wisconsin residents can submit additional cases through a Google form.
According to the COVID Monitor, states that report K-12 COVID-19 case counts now include: Arkansas, Hawaii, Kentucky, Louisiana, Mississippi, New Hampshire, Ohio, South Carolina, South Dakota, Tennessee, Texas, and Utah. Some of these state reports are far more precise than others; Texas and Utah, for example, both report only total case counts. The COVID Monitor reports over 10,000 COVID-19 confirmed cases in K-12 schools as of September 20, with another 17,000 reported cases pending.
A recent article in the Chronicle of Higher Education by Michael Vasquez explains common issues with reporting COVID-19 cases on college and university campuses: inconsistencies across school dashboards, administrations unwilling to report data, and other challenges.
I spent the bulk of last week’s issue unpacking a new testing dataset released by the Centers for Medicare & Medicaid Services which provides test positivity rates for U.S. counties. At that point, I had some unanswered questions, such as “When will the dataset next be updated?” and “Why didn’t CMS publicize these data?”
The dataset was updated this past week—on Thursday, September 17, to be precise. So far, it appears that CMS is operating on a two-week update schedule (the dataset was first published on Thursday, September 3). The data themselves, however, lag this update by a week: the spreadsheet’s documentation states that these data are as of September 9.
CMS has also changed their methodology since the dataset’s first publication. Rather than publishing 7-day average positivity rates for each county, the dataset now presents 14-day average positivity rates. I assume that the 14 days in question are August 27 through September 9, though this is not clearly stated in the documentation.
This choice was reportedly made “in order to use a greater amount of data to calculate percent test positivity and improve the stability of values.” But does it come at the cost of more up-to-date data? If CMS’s future updates continue to include one-week-old data, this practice would be antithetical to the actual purpose of the dataset: letting nursing home administrators know what the current testing situation is in their county so that they can plan testing at their facility accordingly.
Additional documentation and methodology updates include:
The dataset now includes raw testing totals for each county (aggregated over 14 days) and 14-day test rates per 100,000 population. Still, without total positive tests for the same time period, it is impossible to replicate the CMS’s positivity calculations.
As these data now reflect a 14-day period, counties with under 20 tests in the past 14 days are now classified as Green and do not have reported positivity rates.
Counties with low testing volume, but high positivity rates (over 10%), are now sometimes reassigned to Yellow or Green tiers based on “additional criteria.” CMS does not specify what these “additional criteria” may be.
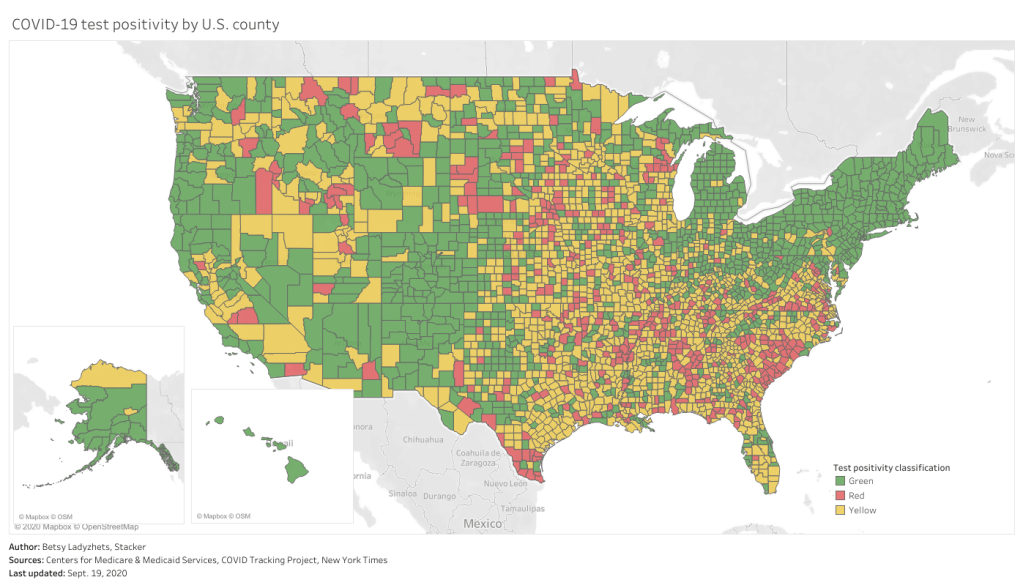
This chart is color-coded according to CMS’s test positivity classifications. As you can see, New England is entirely in the green, while parts of the South, Midwest, and West Coast are spottier.
Finally: CMS has a long way to go on data accessibility. A friend who works as a web developer responded to last week’s newsletter explaining how unspecific hyperlinks can make life harder for blind users and other people who use screenreaders. Screenreaders can be set to read all the links on a page as a list, rather than reading them in-text, to give users an idea of their navigation options. But when all the links are attached to the same text, users won’t know what their options are. The CMS page that links to this test positivity dataset is a major offender: I counted seven links that are simply attached to the word “here.”
This practice is challenging for sighted users as well—imagine skimming through a page, looking for links, and having to read the same paragraph four times because you see the words “click here” over and over. (This is my experience every time I check for updates to the test positivity dataset.)
“This is literally a test item in our editor training, that’s how important it is,” my friend said. “And yet people still get it wrong. ALL THE TIME.”
One would think an agency dedicated to Medicare and Medicaid services would be better at web accessibility. And yet.
If the title of this week’s newsletter sounds ominous, that’s because this situation feels ominous. While many scientific experts have pushed back against President Trump’s claims that a vaccine for the novel coronavirus will be available this October, state public health agencies have been instructed to prepare for vaccine distribution starting in November or December.
Of course, the possibility of a COVID-19 vaccine before the end of 2020 is promising. The sooner healthcare workers and other essential workers can be inoculated, the better protected our healthcare system will be against future outbreaks. (And eventually, maybe, regular people like me will be able to attend concerts and fly out of the country again.) But considering the Center for Disease Control and Prevention (CDC)’s many missteps in both distributing and tracking COVID-19 tests this spring, I have a wealth of concerns about this federal agency’s ability to implement a national vaccination program.
I’m far from the only person thinking about this. The release of the CDC’s interim playbook for vaccine distribution this past Wednesday, along with President Trump’s public contradiction of the vaccination timeline described by CDC Director Dr. Robert Redfield, has sparked conversations on whether America could have a vaccine ready this fall and, if we do, what it would take to safely distribute this technology to the people who need it most.
In this issue, I will offer my takeaways on what the CDC’s playbook means for COVID-19 vaccination data, and a few key elements that I would like to see prioritized when public health agencies begin reporting on vaccinations.
Data takeaways from the CDC playbook
I’m not going to try to summarize the whole playbook here, because a. other journalists have already done a great job of this, and b. it would take up the whole newsletter. Here, I’m focusing specifically on what the CDC has told us about what vaccination data will be collected and how they will be reported.
We do not yet know which vaccines will be available, nor do we know vaccine volumes, timing, efficacy, or storage and handling requirements. It seems clear, however, that we should prepare for not just one COVID-19 vaccine but several, used in conjunction based on which vaccines are most readily available for a particular jurisdiction.
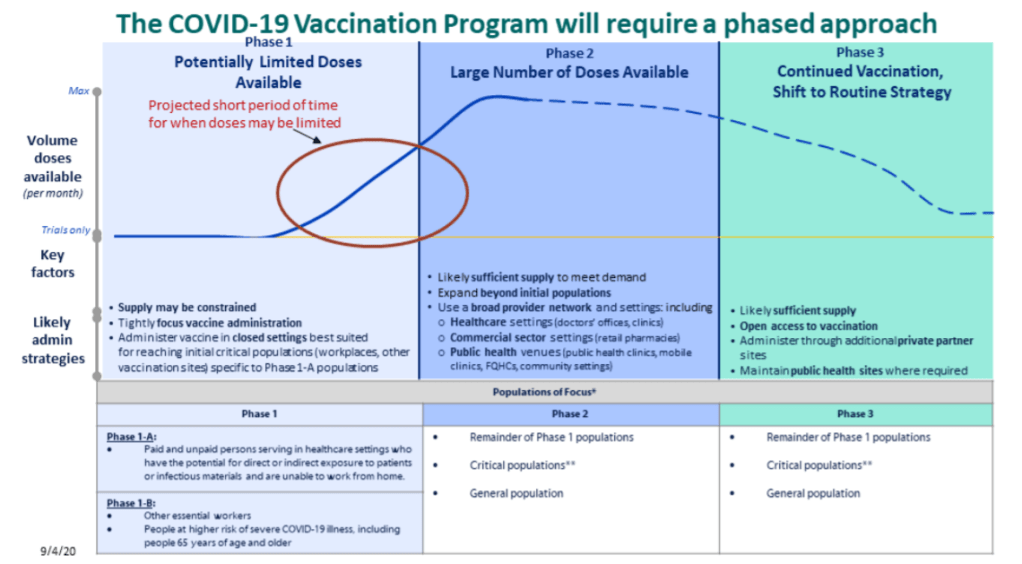
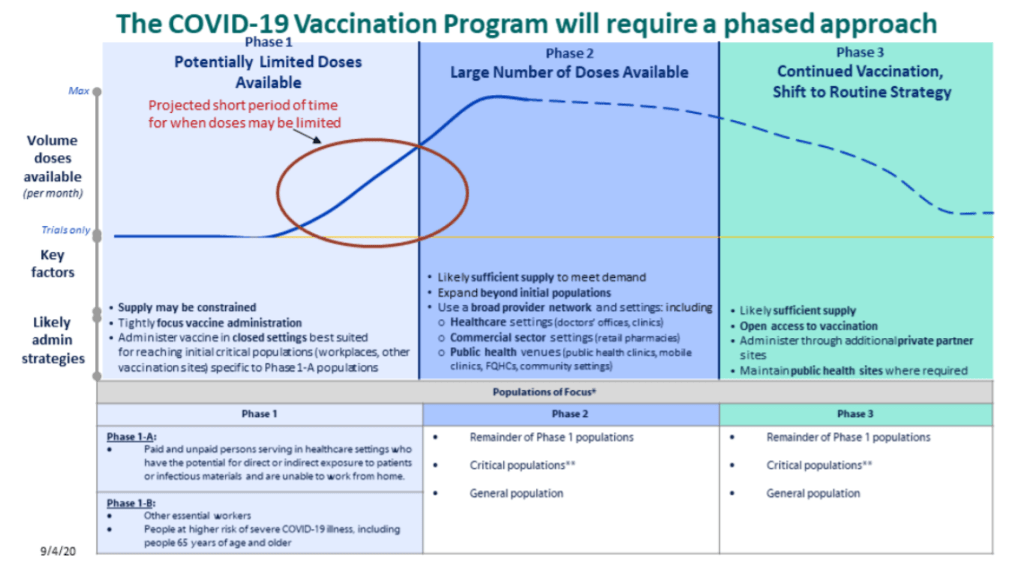
Vaccination will occur in three stages (as pictured in the above graphic). First, limited doses will go to critical populations, such as healthcare workers, other essential workers, and the medically vulnerable. Second, more doses will go to the remainder of those critical populations, and vaccine availability will open up to the general public. Finally, anyone who wants a vaccine will be able to get one.
“Critical populations,” as described by the CDC, basically include all groups who have been demonstrably more vulnerable to either contracting the virus or having a more severe case of COVID-19. The list ranges from healthcare workers, to racial and ethnic minorities, to long-term care facility residents, to people experiencing homelessness, to people who are under- or uninsured.
The vaccine will be free to all recipients.
Vaccine providers will include hospitals and pharmacies in the first phase, then should be expanded to clinics, workplaces, schools, community organizations, congregate living facilities, and more.
Most of the COVID-19 vaccines that may come on the market will require two doses, separated by 21 or 28 days. For each recipient, both doses will need to come from the same manufacturer.
Along with the vaccines themselves, the CDC will send supply kits to vaccine providers. The kits will include medical equipment, PPE, and—most notably for me—vaccination report cards. Medical staff are instructed to fill out these cards with a patient’s vaccine manufacturer, the date of their first dose, and the date by which they will need to complete their second dose. Staff and data systems should be prepared for patients to receive their two doses at two different locations.
All vaccine providers will be required to report data to the CDC on a daily basis. When someone gets a vaccine, their information will need to be reported within 24 hours. Reports will go to the CDC’s Immunization Information System (IIS).
The CDC has a long list of data fields that must be reported for every vaccination patient. You can read the full list here; I was glad to see that demographic fields such as race, ethnicity, and gender are included.
The CDC has set up a data transferring system, called the Immunization Gateway (or IZ Gateway), which vaccine providers can use to send their daily data reports. Can is the operative word here; as long as providers are sending in daily reports, they are permitted to use other systems. (Context: the IZ Gateway is an all-new system which some local public health agencies see as redundant to their existing vaccine trackers, POLITICO reported earlier this week.)
Vaccine providers are also required to report “adverse events following immunization” or poor patient outcomes that occur after a vaccine is administered. These outcomes can be directly connected to the vaccine or unrelated; tracking them helps vaccine manufacturers detect new adverse consequences and keep an eye on existing side effects. Vaccine providers are required to report these adverse events to the Vaccine Adverse Event Reporting System (VAERS), which, for some reason, is separate from the CDC’s primary IIS.
Once COVID-19 vaccination begins, the CDC will report national vaccination data on a dashboard similar to the agency’s existing flu vaccination dashboard. According to the playbook, this dashboard will include estimates of the critical populations that will be prioritized for vaccination, locations of CDC-approved vaccine providers and their available supplies, and counts of how many vaccines have been administered.
I have to clarify, though: all of the guidelines set up in the CDC’s playbook reflect what should happen when vaccines are implemented. It remains to be seen whether already underfunded and understaffed public health agencies, hospitals, and health clinics will be able to store, handle, and distribute multiple vaccine types at once, to say nothing of adapting to another new federal data system.
This second section is inspired by an opinion piece in STAT, in which physicians and public health experts Luciana Borio and Jesse L. Goodman outline three necessary conditions for effective vaccine distribution. They argue that confidence around FDA decisions, robust safety monitoring, and equitable distribution of vaccines are all key to getting this country inoculated.
The piece got me thinking: what would be my necessary conditions for effective vaccine data reporting? Here’s what I came up with; it amounts to a wishlist for available data at the federal, state, and local levels.
Unified data definitions, established well before the first reported vaccination. Counts of people who are now inoculated should be reported in the same way in every state, county, and city. Counts of people who have received only one dose, as well as those who have experienced adverse effects, should similarly be reported consistently.
No lumping of different vaccine types. Several vaccines will likely come on the market around the same time, and each one will have its own storage needs, procedures, and potential effects. While cumulative counts of how many people in a community have been vaccinated may be useful to track overall inoculation, it will be important for public health researchers and reporters to see exactly which vaccine types are being used where, and in what quantities.
Demographic data. When the COVID Racial Data Tracker began collecting data in April, only 10 states were reporting some form of COVID-19 race and ethnicity data. North Dakota, the last state to begin reporting such data, did not do so until August. Now that the scale of COVID-19’s disproportionate impact on racial and ethnic minorities is well documented, such a delay in demographic data reporting for vaccination would be unacceptable. The CDC and local public health agencies will reportedly prioritize minority communities in vaccination, and they must report demographic data so that reporters like myself can hold them accountable to that priority.
Vaccination counts for congregate facilities. The CDC specifically acknowledges that congregate facilities, from nursing homes to university dorms to homeless shelters, must be vaccination priorities. Just as we need demographic data to keep track of how minority communities are receiving vaccines, we need data on congregate facilities. And such data should be consistently reported from the first phase of vaccination, not added to dashboards sporadically and unevenly, as data on long-term care facilities have been reported so far.
Easily accessible resources on where to get vaccinated. The CDC’s vaccination dashboard will reportedly include locations of CDC-approved vaccine providers. But will it include each provider’s open hours? Whether the provider requires advance appointments or allows walk-ins? Whether the provider has bilingual staff? How many vaccines are available daily or weekly at the site? To be complete, a database of vaccine providers needs to answer all the questions that an average American would have about the vaccination experience. And such a database needs to be publicized widely, from Dr. Redfield all the way to local mayors and school principals.
Someday, I will write a parody stage play called “Waiting for Texas.” It will feature a squadron of diligent COVID Tracking Project volunteers, eagerly refreshing Texas’ COVID-19 dashboard, wondering if today, maybe, will be the day that the site updates by its promised time of 4 PM Central (5 PM Eastern).
This past weekend, I was not so lucky. Texas’ data came late enough on Saturday that the Project decided to publish its daily update without this state. How late did it come? 6:30 PM Central, or 7:30 PM Eastern. I understand the procrastination, Texas (see: the sending time of this newsletter today), but a little heads up might be nice next time.
COVID-19 Cutback Tracker: Researchers at the Tow Center for Digital Journalism at Columbia University have tracked layoffs, furloughs, closures, and other cutbacks to journalistic outlets since March 2020. Findings from the project were released this past Wednesday in a new tracker.
We Rate Covid Dashboards: Two weeks ago, I analyzed college and university COVID-19 dashboards for my newsletter. This project from public health experts at Yale and Harvard, meanwhile, goes much further: the researchers have developed a rating scheme based on available metrics, legibility, update schedules, and more, and rated over 100 dashboards so far.
GenderSci Lab’s US Gender/Sex Covid-19 Data Tracker: The GenderSci Lab, an interdisciplinary research project, is tracking COVID-19 by gender by compiling information from state reports. The tracker includes case counts, death counts, and mortality rates.
COVIDcast: This dashboard, by the Delphi Group at Carnegie Mellon University, features interactive maps for a variety of COVID-19 indicators, including movement trends, doctors’ visits , and even test positivity based on antigen tests.
2019 baby name popularity: Okay, this one isn’t COVID-19 related. But as Stacker’s resident baby names expert, I feel obligated to inform my readers that, last week, the Social Security Administration finally released its counts of how many babies were given which names in 2019. (The annual update is usually released in March, but was delayed this year due to COVID-19 concerns.) Olivia has beat out Emma for the number one-ranked baby girl name, after Emma’s five years at the top. Personally, I always get a kick out of scrolling through the long tails to see what unique and creative names parents are using.
New York Governor Andrew Cuomo discussed this dashboard in his online briefing last Tuesday, September 8. (If you’d like to watch, start at about 18:00.) He explained that every school district is now required to report test and case numbers daily to New York’s Department of Health. Local public health departments and state labs performing testing are also required to report these numbers, so that the state department can cross-check against three different sources. Cases and tests will be published by school on the new dashboard, called the COVID Report Card.
In his briefing, Governor Cuomo showed a mockup of what the Report Card will look like. The available data includes positive cases by date, tests administered by the school (including test type, lab used, and test wait time), the school’s opening status (i.e. is it operating remotely, in person, or with a hybrid model), and the percentage of on-site students and staff who test positive.
This dataset promises to be much more complete than any other state’s reporting on COVID-19 in schools. But I haven’t been able to closely examine these data yet, because the dashboard has yet to come online.
According to reporting from Gothamist, state officials planned for the dashboard to begin showing data on September 9. As I send this newsletter on September 13, however, the dashboard provides only a message stating that the COVID Report Card will be live “when the reporting starts to come back.”
“The facts give people comfort,” Governor Cuomo said in his briefing. So, Governor, where are the facts? Where are the data? When will New York students, parents, and teachers be able to follow COVID-19 in their schools? My calls to Governor Cuomo’s office and the New York State Department of Health have as yet gone unanswered, and subsequent press releases have not issued updates on the status of these data.
I hope to return with an update on this dashboard next week. In the meantime, for a thorough look at why school COVID-19 data are so important and the barriers that such data collection has faced so far, I highly recommend this POLITICO feature by Biana Quilantan and Dan Goldberg.
On September 3, 2020, the Center for Medicare & Medicaid Services (CMS) posted a county-level testing dataset. The dataset specifically provides test positivity rates for every U.S. county, for the week of August 27 to September 2.
This is huge. It’s, like, I had to lie down after I saw it, huge. No federal health agency has posted county-level testing data since the pandemic started. Before September 3, if a journalist wanted to analyze testing data at any level more local than states, they would need to aggregate values from state and county public health departments and standardize them as best they could. The New York Times did just that for a dashboard on school reopening, as I discussed in a previous issue, but even the NYT’s data team was not able to find county-level values in some states. Now, with this new release, researchers and reporters can easily compare rates across the county and identify hotspot areas which need more testing support.
So Betsy, you might ask, why are you reporting on this new dataset now? It’s been over a week since the county-level data were published. Well, as is common with federal COVID-19 data releases, this dataset was so poorly publicized that almost nobody noticed it.
The dataset’s release was, instead, brought to my attention thanks to a tweet by investigative reporter Liz Essley Whyte of the Center for Public Integrity:
🚨 Coronavirus data nerds: @CMSGov has started posting county-level test positivity data
Here are the top 20 counties for test positivity according to their data
In today’s issue, I’ll share my analysis of these data and answer, to the best of my ability, a couple of the questions that have come up about the dataset for me and my colleagues in the past few days.
Analyzing the data
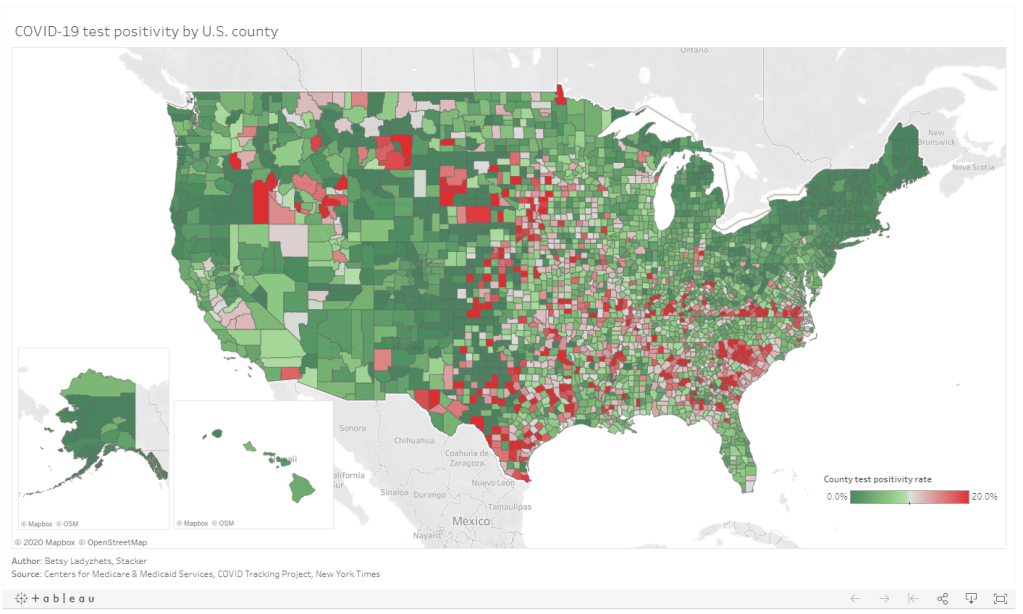
Last week, I put together two Stacker stories based on these data. The first includes two county-level Tableau visualizations; these dashboards allow you to scroll into the region or state of your choice and see county test positivity rates, how those county rates compare to overall state positivity rates (calculated based on COVID Tracking Project data for the same time period, August 27 to September 2), and recent case and death counts in each county, sourced from the New York Times’ COVID-19 data repository. You can also explore the dashboards directly here.
The second story takes a more traditional Stacker format: it organizes county test positivity rates by state, providing information on the five counties with the highest positivity rates in each. The story also includes overall state testing, case, and outcomes data from the COVId Tracking Project.
As a reminder, a test positivity rate refers to the percent of COVID-19 tests for a given population which have returned a positive result over a specific period of time. Here’s how I explained the metric for Stacker:
These positivity rates are typically reported for a short period of time, either one day or one week, and are used to reflect a region’s testing capacity over time. If a region has a higher positivity rate, that likely means either many people there have COVID-19, the region does not have enough testing available to accurately measure its outbreak, or both. If a region has a lower positivity rate, on the other hand, that likely means a large share of the population has access to testing, and the region is diagnosing a more accurate share of its infected residents.
Test positivity rates are often used as a key indicator of how well a particular region is controlling its COVID-19 outbreak. The World Health Organization (WHO) recommends a test positivity rate of 5% or lower. This figure, and a more lenient benchmark of 10%, have been adopted by school districts looking to reopen and states looking to restrict out-of-state visitors as a key threshold that must be met.
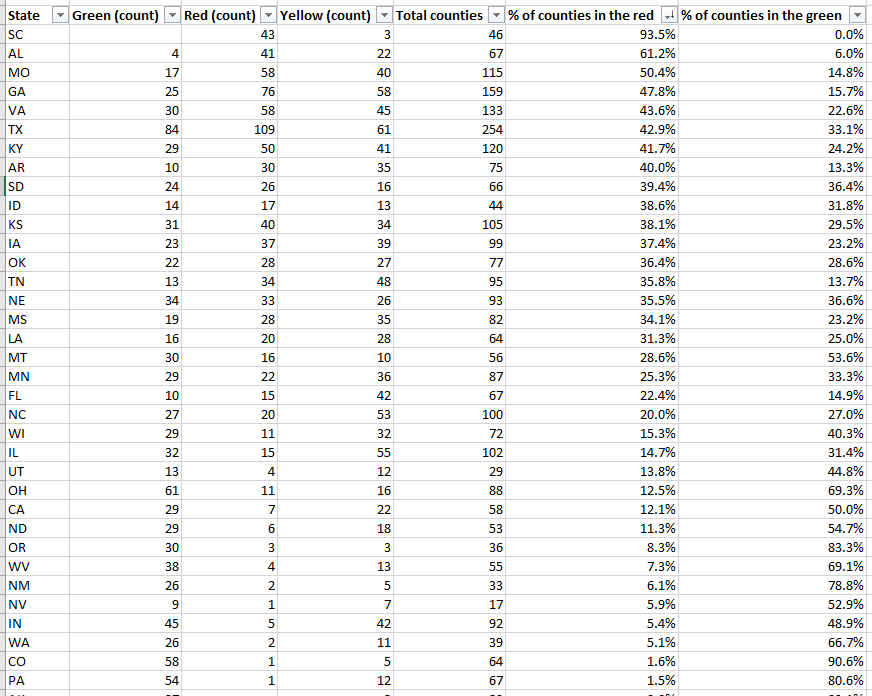
Which counties are faring the worst, according to this benchmark? Let’s take a look:
This screenshot includes the 33 U.S. counties with the highest positivity rates. I picked the top 33 to highlight here because their rates are over 30%—six times the WHO’s recommended rate. The overall average positivity rate across the U.S. is 7.7%, but some of these extremely high-rate counties are likely driving up that average. Note that two counties, one in South Dakota and one in Virginia, have positivity rates of almost 90%.
Overall, 1,259 counties are in what CMS refers to as the “Green” zone: their positivity rates are under 5%, or they have conducted fewer than 10 tests in the seven-day period represented by this dataset. 874 counties are in the “Yellow” zone, with positivity rates between 5% and 10%. 991 counties are in the “Red” zone, with positivity rates over 10%. South Carolina, Alabama, and Missouri have the highest shares of counties in the red, with 93.5%, 61.2%, and 50.4%, respectively:
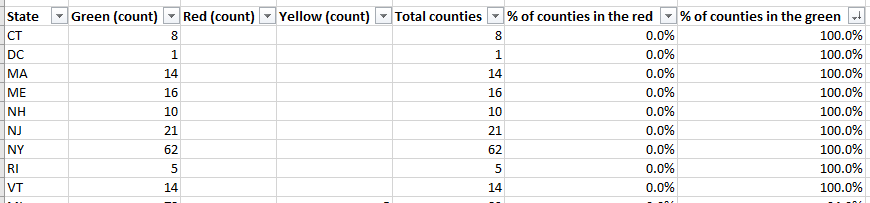
Meanwhile, eight states and the District of Columbia, largely in the northeast, have all of their counties in the green:
My Tableau visualizations of these data also include an interactive table, which you can use to examine the values for a particular state. The dashboards are set up so that any viewers can easily download the underlying data, and I am, as always, happy to share my cleaned dataset and/or answer questions from any reporters who would like to use these data in their own stories. The visualizations and methodology are also open for syndication through Stacker’s RSS feed—I can share more details on this if anyone is interested.
Answering questions about the data
Why is the CMS publishing this dataset? Why not the CDC or HHS overall?
These test positivity rates were published as a reference for nursing home administrators, who are required to test their staff regularly based on the prevalence of COVID-19 in a facility’s area. A new guidance for nursing homes dated August 26 explains the minimum testing requirement: nursing homes in green counties must test all staff at least once a month, those in yellow counties must test at least once a week, and those in red counties must test at least twice a week.
It is important to note that facilities are only required to test staff, not residents. In fact, the guidance states that “routine testing of asymptomatic residents is not recommended,” though administrators may consider testing those residents who leave their facilities often.
Where did the data come from?
The CMS website does not clearly state a source for these data. Digging into the downloadable spreadsheet itself, however, reveals that the testing source is a “unified testing data set,” which is clarified in the sheet’s Documentation field as data reported by both state health departments and HHS:
COVID-19 Electronic Lab Reporting (CELR) state health department-reported data are used to describe county-level viral COVID-19 laboratory test (RT-PCR) result totals when information is available on patients’ county of residence or healthcare providers’ practice location. HHS Protect laboratory data (provided directly to Federal Government from public health labs, hospital labs, and commercial labs) are used otherwise.
What are the units?
As I discussed at length in last week’s newsletter, no testing data can be appropriately contextualized without knowing the underlying test type and units. This dataset reports positivity rates for PCR tests, in units of specimens (or, as the documentation calls them, “tests performed.”) HHS’s public PCR testing dataset similarly reports in units of specimens.
How are tests assigned to a county?
As is typical for federal datasets, not every field is exactly what it claims to be. The dataset’s documentation elaborates that test results may be assigned to the county where a. a patient lives, b. the patient’s healthcare provider facility is located, c. the provider that ordered the test is located, or d. the lab that performed the test is located. Most likely, the patient’s address is used preferentially, with these other options used in absence of such information. But the disparate possiblities lead me to recommend proceeding with caution in using this dataset for geographical comparisons—I would expect the positivity rates reported here to differ from the county-level positivity rates reported by a state or county health department, which might have a different documentation procedure.
How often will this dataset be updated?
Neither the CMS page nor the dataset’s documentation itself indicate an update schedule. A report from the American Health Care Association suggests that the file will be updated on the first and third Mondays of each month—so, maybe it will be updated on the 21st, or maybe it will be updated tomorrow. Or maybe it won’t be updated until October. I will simply have to keep checking the spreadsheet and see what happens.
Why won’t the dataset be updated every week, when nursing homes in yellow- and red-level counties are expected to test their staff at least once a week? Why is more public information about an update schedule not readily available? These are important questions which I cannot yet answer.
Why wasn’t this dataset publicized?
I really wish I could concretely answer this one. I tried submitting press requests and calling the CMS’ press line this past week; their mailbox, when I called on Friday, was full.
But here’s my best guess: this dataset is intended as a tool for nursing home facilities. In that intention, it serves a very practical purpose, letting administrators know how often they should test their staff. If CMS or HHS put out a major press release, and if an article was published in POLITICO or the Wall Street Journal, the public scrutiny and politically-driven conspiracy theorists which hounded HHS during the hospitalization data switch would return in full force. Nursing home administrators and staff have more pressing issues to worry about than becoming part of a national political story—namely, testing all of their staff and residents for the novel coronavirus.
Still, even for the sake of nursing homes, more information about this dataset is necessary to hold accountable both facilities and the federal agency that oversees them. How were nursing home administrators, the intended users of this dataset, notified of its existence? Will the CMS put out further notices to facilities when the data are updated? Is the CMS or HHS standing by to answer questions from nursing home staff about how to interpret testing data and set up a plan for regular screening tests?
For full accountability, it is important for journalists like myself to be able to access not only data, but also the methods and processes around its collection and use.