In the past week (February 9 through 15), the U.S. officially reported about 260,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 37,000 new cases each day
79 total new cases for every 100,000 Americans
8% fewer new cases than last week (February 2-8)
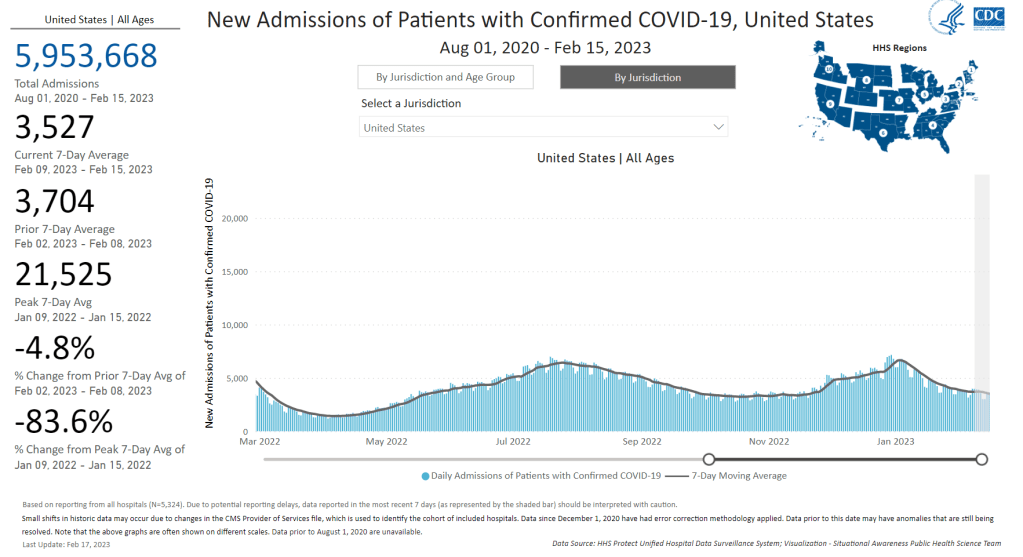
In the past week, the U.S. also reported about 25,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 3,500 new admissions each day
7.5 total admissions for every 100,000 Americans
5% fewer new admissions than last week
Additionally, the U.S. reported:
2,800 new COVID-19 deaths (400 per day)
80% of new cases are caused by Omicron XBB.1.5; 16% by BQ.1 and BQ.1.1; 1% by CH.1.1 (as of February 18)
An average of 70,000 vaccinations per day
Nationally, official COVID-19 cases and hospitalizations continue to trend slowly downward, suggesting that we’re in a high plateau of consistent virus spread. Reported cases have only declined by about 18% in the last month, while new hospital admissions have declined by 28%.
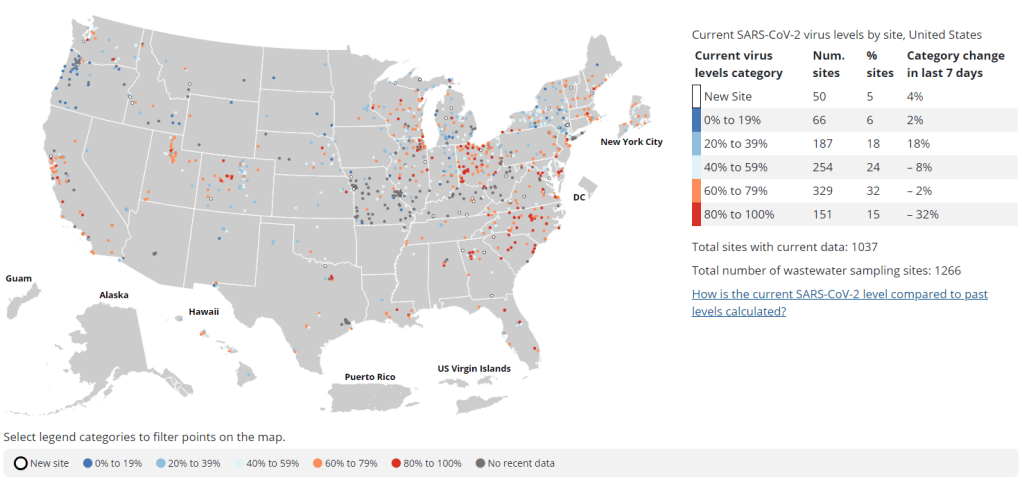
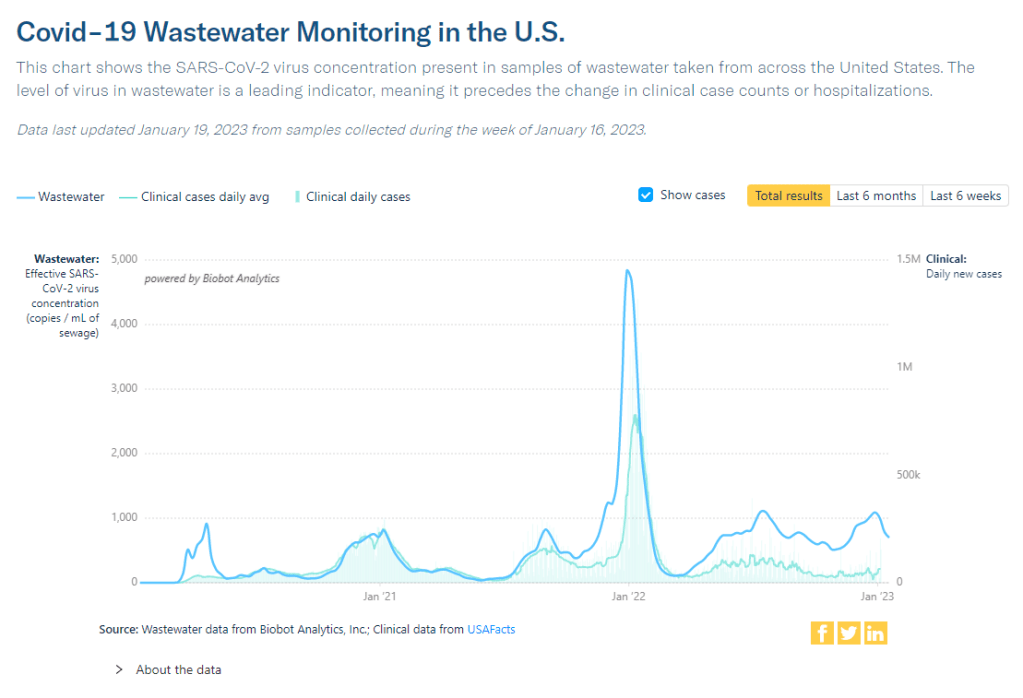
Wastewater surveillance data from Biobot also continue to indicate that COVID-19 spread has plateaued nationally, with slightly different trends at the regional level: a potential uptick in the Northeast, a trend back down in the Midwest, and slight declines in the West and South.
At the state level, some Midwest states continue to report increases in their COVID-19 cases and hospitalizations. These states include: Wyoming, Alaska, Montana, Utah, Nebraska, Michigan, and Missouri. (Though the wastewater decline could indicate that these trends in clinical case data may turn around soon.)
As I pointed out last week, the current COVID-19 plateau is unique from what the U.S. experienced around this time in 2022 and 2021. In both of those years, virus spread declined significantly after a winter surge, leading to relatively low levels in the spring. But this year, the decline has been shorter and has stopped earlier, leaving us with continued high COVID-19.
Biobot’s communications team pointed out on Twitter recently that the national average of coronavirus concentrations in wastewater is “about 60% higher than it was at this time in 2022” and “almost two times what it was at this time in 2021.”
Why isn’t transmission declining more? The XBB.1.5 could be playing a role here, as it spreads further across the country. This highly-contagious version of Omicron accounted for about 80% of new cases in the U.S. last week, according to the CDC’s estimates, and is now heavily dominant in almost every region of the country.
But I suspect a bigger culprit here is likely the complete lack of COVID-19 safety protocols right now. In spring 2021, first-round vaccines and continued non-pharmaceutical interventions played a big role in preventing disease, while in 2022, the U.S. had a lot of immunity from vaccinations and the recent, massive Omicron BA.1 surge, combined with some continuation of other measures. (Though that immunity quickly faded when BA.2 came on the scene.)
Now, we have less population immunity, less non-pharmaceutical interventions, and less overall awareness of the continued problems posed by COVID-19. This broad apathy towards the coronavirus hides the fact that over 400 people are still dying from this disease every day.
Biobot provides wastewater testing and analysis for more than 400 sites in the NWSS network, accounting for about one-third of the system’s total 1,200 sites. The CDC/Biobot arrangement basically makes it easy for these wastewater treatment plants to participate in COVID-19 and mpox testing, since sites can send in samples without spending the time and resources needed to build up their own testing programs.
I was glad to see this news, as the continued contract will mean no interruptions in CDC NWSS data for at least another six months. Long-time readers might remember that there were major wastewater data gaps last spring, when the CDC switched contractors from LuminUltra to Biobot.
Of course, six months is far from the long-term investment that the U.S. should be making in wastewater surveillance… but that’s a topic for another week.
This week, I had a new article published in The Atlantic about how COVID-19 wastewater surveillance can be useful beyond entire sewersheds, the setting where this testing usually takes place. Sewershed testing is great for broad trends about large populations (like, an entire city or county), the story explains. But if you’re a public health official seeking truly actionable data to inform policies, it’s helpful to get more specific.
My story focuses on one wastewater testing setting that’s been in the news a lot lately: airplane bathrooms, from which researchers can identify new variants arriving with international travelers. But airplanes are far from the only place where specific wastewater surveillance can be valuable. Here are some of those other places, highlighting some information that I learned in reporting this story (but couldn’t fit in the final article).
K-12 schools
Early in the pandemic, colleges and universities became a hub for wastewater surveillance innovation. At campuses like Columbia University in NYC, researchers tested the sewage at individual dorms in order to determine exactly which students were getting sick—and take quick action, usually by requiring students at the infected dorm to get PCR-tested and quarantining the people who tested positive.
But the same technique can apply to schools with younger students. In late 2020, the University of California San Diego expanded its testing program to elementary schools, in an initiative called the Safer at School Early Alert System. The program started with 10 schools in the 2020-21 school year, then expanded to 26 in the 2021-22 year. Wastewater testing at specific sewershed points next to the schools led researchers to identify asymptomatic COVID-19 cases with high accuracy, program leader Rebecca Fielding-Miller told me.
The San Diego program isn’t alone: other public school systems have tried out building-level wastewater testing, usually in collaboration with nearby research groups. While the research projects tend to successfully show that wastewater surveillance can pick up infections, it’s challenging for school systems to get the funding to do these programs long-term. (Unlike universities, which are in total control of their funding, public schools need to rely on local governments).
As a consequence of these funding challenges, the San Diego program wasn’t renewed for the 2022-23 school year. “We really would have wanted to keep doing it, but funding ran out,” Fielding-Miller said.
Hospitals, other healthcare facilities
Much of the U.S.’s health strategy throughout the pandemic has focused on keeping hospitals from becoming overwhelmed—or at least helping hospitals weather COVID-19 surges. Wastewater surveillance can help accomplish this, by giving hospital administrators warnings about potential increased transmission; wastewater trends usually predict hospitalization trends by a week or more. And when wastewater surveillance is happening at hospitals themselves, these warnings can be really specific.
At NYC Health + Hospitals, the city’s public hospital system, administrators can get these warnings from wastewater testing at the system’s eleven hospitals. The surveillance program includes weekly tests for COVID-19, flu, and mpox (formerly called monkeypox), in collaboration with local researchers. The resulting data “gives us better situational awareness,” said Leopolda Silvera, a global health administrator at Health + Hospitals. If the health system notices a coming surge at one hospital, they can adjust resources accordingly—such as sending more staff to the emergency department.
The Health + Hospitals wastewater program has been running for about a year, Silvera said. At this point, it’s the only program she knows of that does building-level surveillance at hospitals. In the future, the hospital system might start testing for other pathogens and health threats like antimicrobial resistance.
Congregate facilities
Congregate facilities like nursing homes and senior living facilities can include a lot of vulnerable people who are at higher risk for severe COVID-19, all living in close quarters. As a result, this is another category of settings where it could be helpful to have building-level wastewater surveillance: facility administrators could learn quickly about upcoming surges and respond, by doing widespread PCR testing or instituting a temporary mask mandate.
The state of Maryland used to have a program doing exactly this, with a focus on correctional facilities throughout the state—particularly facilities housing the most vulnerable residents. The wastewater surveillance program ran through May 2022, at which point it “quietly ended,” according to local outlet the Maryland Daily Record. An initial $1 million in funding for wastewater testing in Maryland ran out; while the CDC National Wastewater Surveillance System picked up testing at wastewater treatment plants, no new entity was able to continue testing at the congregate living facilities.
According to the Daily Record, the building-level wastewater testing was incredibly helpful for informing COVID-19 measures at correctional facilities and helped keep cases down. I hope the Maryland program isn’t the last example we see of this testing in the U.S.
Large, communal workplaces
Early in the pandemic, some of the U.S.’s worst COVID-19 outbreaks happened at factories, particularly large food processing plants. People in these settings are often working in close quarters, easily able to infect each other—and when an outbreak happens, there are ramifications for both individual employees and the company’s business.
These large facilities could be another target for wastewater surveillance: if company administrators see a warning about rising COVID-19 from their buildings’ sewage, they could institute basic public health measures to curb the spread. Such is the strategy for some mine companies in rural Canada, which work with biotech company LuminUltra to test their wastewater. People often live and work at these sites, making them relatively closed settings for transmission.
At these locations, COVID-19 was previously “kind-of out of control, clinical testing was very reactive,” said Jordan Schmidt, director of product applications at LuminUltra. With wastewater testing, the mining companies can keep outbreaks “to a handful of people.” Fewer people get sick and there’s less interruption to business, he said.
Neighborhood-level testing
As public health agencies face lower budgets and overall lower awareness about COVID-19, some officials want to maximize their limited resources. If you only have the funding and staff for two mobile PCR testing sites this week, you’d want to make sure they go to a neighborhood where the testing would be most helpful, right?
The Boston Public Health Commission had this goal in mind when they launched a new neighborhood-level wastewater testing program, in collaboration with Biobot Analytics. The program includes testing twice a week at 11 sites across Boston, selected to provide good coverage of the city and also enable testing without too much disruption to traffic. While testing just started in January, the program is already helpful for identifying specific COVID-19 patterns, said Kathryn Hall, deputy commissioner for the health agency.
Boston’s program is focused on COVID-19 right now, but could expand to other diseases as needed, Hall said: “Now that we have the infrastructure in place, it allows us to be really be prepared and also to ask novel and interesting questions.”
Airplanes
Airplane surveillance fits into a slightly different category than the other settings I described here. When researchers test airplane wastewater, they aren’t seeking to get advanced warnings of new surges or inform public health policies. Instead, the goal is to track variants—with a focus on any new coronavirus mutations that might come into the U.S. from abroad. (Read the Atlantic story for more details on how this works!)
Other transportation hubs could be useful for tracking variants too, experts told me. This could mean large train stations, bus stations, shipping ports—any location that involves a lot of people moving from one place to another. After all, variants can evolve in the U.S. as easily as they can in other parts of the world.
Overall, the specific wastewater testing settings described here could be valuable pieces of expanding the U.S.’s overall surveillance network, along with the more-traditional sewershed testing. But all these testing sites need sustained funding to actually provide valuable data in the long run, something that could be in jeopardy as the federal public health emergency ends.
Washington’s dashboard includes coronavirus concentration levels over time from a selection of wastewater treatment plants in the state, with data going back to early 2022. It also includes some helpful notes about how to interpret wastewater data and maps showing the service areas for each treatment plant.
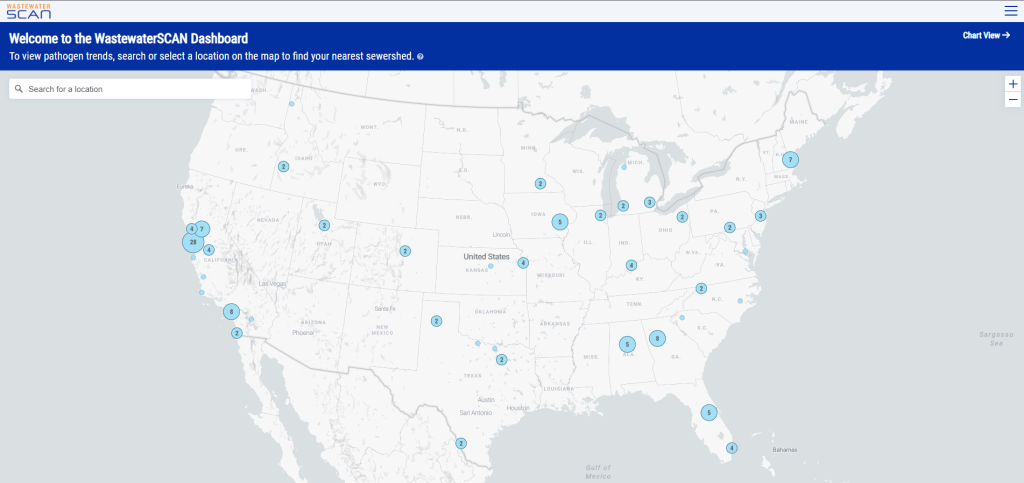
I also recently learned that WastewaterSCAN has released a new, upgraded dashboard to share its surveillance data. WastewaterSCAN is a project started by researchers at Stanford and Emory universities (with a focus on sites in California) that has since expanded across the country. The new dashboard makes it easier for users to find SCAN testing sites in their areas and answer specific questions with the data.
As official case numbers become less and less reliable, I’m glad to see public agencies and research efforts step up to make wastewater surveillance more accessible. Both the Washington dashboard and new WastewaterSCAN link are now included on my wastewater data resource page.
New York State expands wastewater surveillance program: This week, the New York State health department announced a major investment in the state’s wastewater surveillance program: the program has received a $6.6 million grant from the CDC and $15 million from the governor (over the next three years). With this investment, New York’s wastewater surveillance network will grow from 125 to 215 testing sites and will expand from COVID-19 to include flu, RSV, hepatitis, norovirus, and antimicrobial resistance. This is great news for New York—I hope to see other states make similar investments.
Bivalent boosters vs. XBB lineages: The bivalent, Omicron-specific booster shots provide some protection against XBB.1.5 and related Omicron subvariants, according to a new study published this week in the CDC’s Morbidity and Mortality Weekly Report. CDC researchers used data from COVID-19 testing at pharmacies to compare results among people who had received the new booster and those who hadn’t. Booster recipients were significantly less likely to have a symptomatic XBB/XBB.1.5 infection compared to people who hadn’t received the shot, the researchers found (with a vaccine effectiveness value of 48%). While the boosters work less well against XBB.1.5 than they did against BA.4/BA.5, they’re still a valuable protective measure.
CDC overhauling data communications: The CDC is creating new internal offices that will change how it processes, publishes, and communicates about data, according to POLITICO. The new offices include an Office of Health Equity and an Office of Public Health Data, Surveillance, and Technology—both of which have new acting directors as of this week. It’s currently unclear what the new offices will do, exactly, or how they will improve upon a fractured nationwide health data system (with decisions about how to store and share key data largely left up to state agencies and private companies). Still, it’s good to see movement on the CDC’s efforts.
WHO deliberates ending the global health emergency: On Friday, a World Health Organization committee met to discuss whether the official global health emergency over COVID-19 should be ended. The committee’s decision will be made public tomorrow, as a recommendation to WHO Director-General Tedros Adhanom Ghebreyesus; Tedros will ultimately decide whether or not to end the emergency. Global health experts who spoke to STAT reporter Helen Branswell suggested that the WHO likely isn’t ready to end this emergency yet, but it may happen later in 2023.
KFF compiles Long COVID data: A new report from the Kaiser Family Foundation compiles and provides context for Long COVID data reported by the Census and CDC’s Household Pulse Survey. The share of people who reported ever having Long COVID symptoms following a COVID-19 case has declined slightly over time, the KFF report finds; this number went from 35% in June 2022 to 28% in January 2023. However, the number is still high and Long COVID can be debilitating for many, as 79% of people with Long COVID report limitations to their day-to-day activities.
Health of Congressional Districts: Finally: a new dashboard, published this week by researchers at NYU Langone Health, provides detailed health metrics for all 435 Congressional districts in the U.S. (plus Washington, D.C.). The dashboard is a helpful source for researchers and policymakers looking to understand health patterns in specific districts. One of its key metrics is a “COVID Local Risk Index” that reflects the risk residents face for severe health, social, and economic outcomes of COVID-19.
New CDC dashboards track respiratory illness hospitalizations: This week, the CDC released two new dashboards that combine COVID-19 data with data on other respiratory illnesses. First, the RESP-NET dashboard summarizes information from population-based hospital surveillance systems in 13 states for COVID-19, the flu, and RSV; it includes overall trends and demographic data. Second, the National Emergency Department Visits dashboard provides data on emergency department visits for COVID-19, the flu, RSV, and all three diseases combined; this dashboard includes data from all 50 states, though not all hospitals are covered.
Early results from NIH at-home test self-reporting: Last week, ABC News shared early results from MakeMyTestCount.org, an online tool run by the National Institutes of Health allowing Americans to self-report their rapid, at-home test results. Between the site’s launch in late November and early January, “24,000 people have reported a test result to the site,” according to ABC. (While the article says “people have reported,” I think this number actually represents the number of test results reported, given that the website doesn’t track when one person submits multiple test results over time.) The majority of results reported are positive and women are more likely to self-report than men, per ABC. It’s unclear how useful these early data may be for any analysis, but I’m glad to see some numbers becoming public.
New preprint updates county-level excess death estimates: A new preprint from Boston University demographer Andrew Stokes and colleagues, posted this week on medRxiv, shares updated estimates on excess deaths and COVID-19 deaths by U.S. county. According to the analysis, about 270,000 excess deaths were not officially attributed to COVID-19 during the first two years of the pandemic, representing 24% of all excess deaths during that time. And the analysis reveals regional patterns: for example, in the South and in rural patterns, excess deaths were less likely to be officially attributed to COVID-19. For more context on these data, see MuckRock’s Uncounted project (which is a collaboration with Stokes and his team).
Factors contributing to low bivalent booster uptake: Another notable paper from this week: results from a survey of Americans who were previously vaccinated about their reasons for receiving (or not receiving) a bivalent, Omicron-specific booster this fall, conducted by researchers at Duke University, Georgia Institute of Technology, and others. Among about 700 people who didn’t get the booster, their most common reasons were a lack of awareness that the respondent was eligible for this vaccine, a lack of awareness that the bivalent vaccine was widely available, and a perception that the respondent already had sufficient protection against COVID-19. This survey shows how governments at every level have failed to advertise the bivalent boosters, likely to dire results.
More wastewater surveillance on airplanes: And one more notable paper: researchers at Bangor University tested wastewater from three international major airports in the U.K., including samples from airplanes and airport terminals. About 93% of the samples from airplanes were positive for SARS-CoV-2, while among the airport terminal samples, 100% at two airports were positive and 85% at the third airport were positive. Similar to the study from Malaysia I shared last week, this paper suggests that there’s a lot of COVID-19 going around on air travel—to put it mildly. The paper also adds more evidence that airplane/airport wastewater can be a useful source for future COVID-19 surveillance.
Nursing home infections ran rampant early in the pandemic: A new report from the Health and Human Services Office of Inspector General examines how much COVID-19 spread through nursing homes in 2020. The report’s authors used Medicare data from about 15,000 nursing homes nationwide, identifying those with “extremely high infection rates” in spring and fall 2020. In more than 1,300 of these facilities, 75% or more of the Medicare patients had COVID-19 during these surges; the same facilities had way-above-average mortality rates. “These findings make clear that nursing homes in this country were not prepared for the sweeping health emergency that COVID-19 created,” the authors write in the report’s summary.
Nearly a year after the CDC’s National Wastewater Surveillance System began reporting public data, the system still has very unequal representation across the U.S.
This week, the National Academies of Sciences, Engineering, and Medicine (NASEM) released a major report about the state of wastewater surveillance for infectious diseases in the U.S. The report, written by a committee of top experts (and peer-reviewed before its release), is an extensive description of the promise and the challenges of wastewater testing.
Its authors describe how a grassroots network of researchers, public officials, and wastewater treatment plant staff developed strategies for sewage testing, analysis, and communicating results. Now, as committee chair Guy Hughes Palmer writes in the report’s introduction, broader collaboration and resources are needed to “solidify this emergency response to the COVID-19 pandemic into a national system” that continues to monitor COVID-19 as well as other public health threats. To this end, the report includes specific recommendations for the CDC’s National Wastewater Surveillance System.
Here are some key findings from the report, taken from its summary section and a NASEM webinar presentation last Thursday:
Overall, the report finds that wastewater surveillance data “are useful for informing public health action and that wastewater surveillance is worthy of further development and continued investment.” The authors recommend that public agencies at all levels keep funding and promoting this monitoring tool.
Wastewater surveillance is not a new technology; it’s been used for decades to monitor the spread of polio. But COVID-19 led to widespread adoption of this technology and innovation into how it could be used, driven by some municipalities and universities that were early to embrace wastewater.
As a population-level tool, wastewater surveillance provides data on how diseases spread through a community without relying on access to clinical testing. This surveillance is becoming more important for COVID-19 as people opt for at-home tests over PCR tests, and should be used specifically to track new variants.
Community sewersheds that may be tested range in size from serving hundreds of people to serving millions; they also differ based on geography, demographics, and many other factors. As a result, early researchers in this space developed testing and analysis methods that were specific to their communities.
Now, however, the CDC faces a challenge: “to unify sampling design, analytical methods, and data interpretation to create a truly representative national system while maintaining continued innovation.” In other words, standardize the system while allowing local communities to keep doing what works best for them.
Sites in the CDC’s National Wastewater Surveillance System (NWSS) are currently not representative of the U.S. as a whole, as the system is based on wastewater utilities and public health agencies choosing to participate.
The CDC needs to expand this system to be more equitable across the country, with targeted outreach, offering resources to sites not currently participating, and other similar tactics. This expansion process should be open and transparent, the report’s authors write.
As NWSS expands, the CDC should select and prioritize “sentinel sites” that can help detect new coronavirus variants and other new emerging health threats early on. These sites might include international airports as well as zoos and livestock farms, where potential animal-to-human transmission may be monitored.
Better public communication is needed: the CDC (and other agencies) should improve its public outreach about wastewater data, including addressing any privacy concerns that people may have. The report specifically recommends that the CDC “convene an ethics advisory committee” to assist with privacy concerns and data-sharing concerns.
In assessing potential new targets for wastewater surveillance, the report recommends three criteria: “(1) public health significance of the threat, (2) analytical feasibility for wastewater surveillance, and (3) usefulness of community-level wastewater surveillance data to inform public health action.”
NWSS needs more funding from the federal government to expand its sites, continue its COVID-19 tracking efforts, fund projects at state and local levels, and pivot to new public health threats as needed. This funding needs to be “predictable and sustained,” the report’s authors write.
In the past week (January 12 through 18), the U.S. officially reported about 330,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 47,000 new cases each day
101 total new cases for every 100,000 Americans
24% fewer new cases than last week (January 5-11)
In the past week, the U.S. also reported about 35,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 5,000 new admissions each day
10.7 total admissions for every 100,000 Americans
16% fewer new admissions than last week
Additionally, the U.S. reported:
4,000 new COVID-19 deaths (560 per day)
49% of new cases are caused by Omicron XBB.1.5; 40% by BQ.1 and BQ.1.1 (as of January 21)
An average of 150,000 vaccinations per day (CDC link)
National COVID-19 metrics continue to suggest that the U.S. is coming out of its holiday surge, though some parts of the country may face increased transmission as the Omicron variant XBB.1.5 spreads.
Official COVID-19 case numbers and new hospital admissions both reported declines this week, according to the CDC (of 24% and 16% respectively, compared to the prior week). Biobot’s wastewater surveillance data also show a decline, with coronavirus concentration at a similar level to mid-November 2022, just before Thanksgiving.
This trend is fairly consistent across states and regions, according to case and hospitalization data from the latest HHS Community Profile Report. However, Biobot’s regional and county-level data suggest that COVID-19 spread is in a plateau or even starting to increase in some parts of the South and Midwest regions.
Hospitalizations for the flu and RSV are following a similar pattern to COVID-19, according to a new CDC dashboard that reports on all three illnesses together. Almost all states reported moderate or low levels of influenza-like activity in the week ending January 14, very different from the patterns we were seeing a few weeks ago. The only areas still reporting high influenza-like activity are California, North Dakota, New Mexico, Texas, Puerto Rico, New York City, and Washington D.C.
All of this is good news, suggesting that the worst of this winter’s respiratory virus surges may be behind us. But COVID-19 is still spreading across the country at fairly high levels, reflecting the high baseline that the U.S. has faced ever since new Omicron subvariants started to hit in spring 2022.
We also need to continue watching XBB.1.5, the latest and most contagious version of Omicron. This subvariant caused about half of new cases in the U.S. in the last week, according to CDC estimates. It’s most prevalent in the Northeast but is quickly gaining ground in the Southeast and other regions. (And the BQ lineages that currently dominate these regions can spread quickly, too.)
In the coming weeks, we’ll see how much XBB.1.5 (and any other variants) contribute to increased transmission in these regions. Meanwhile, COVID-19 deaths went up recently as the holiday surge took its toll: more than 500 people have died from COVID-19 every day in the last two weeks. Deaths are always the most delayed—and the most tragic—metric.
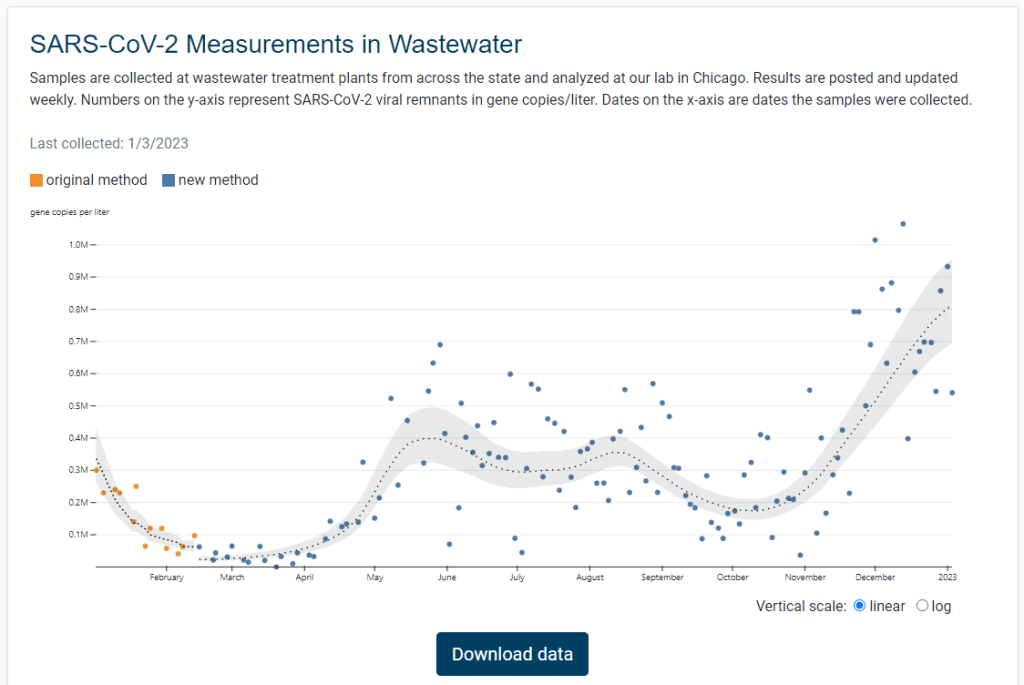
Illinois is the latest state to get its own dashboard for COVID-19 wastewater surveillance, with a new website that launched earlier this week. It includes data for 75 sites across the state.
The new dashboard—like the state’s wastewater surveillance program itself—is a collaboration between the Illinois Department of Public Health and the Discovery Partners Institute, a research center at the University of Illinois. Illinois’ agency received more than $6.5 million in federal grants to fund wastewater testing, according to local TV station WTTW.
I poked around a bit on the new dashboard, and I’m a fan: it includes a map of sampling locations, charts showing COVID-19 trends over time, easily-downloadable data, and ample information on how to interpret results. Nice work, Illinois!
New Long COVID review from PLRC and Scripps: Leading Long COVID researchers from the Patient-Led Research Collaborative and the Scripps Research Translational Institute collaborated on a review paper published this week in Nature, summarizing major findings from the literature so far. The paper includes summaries of major symptoms (ranging from cardiac damage to cognitive impairment), correlations between Long COVID and other chronic diseases (ME/CFS, POTS, etc.), treatment options for specific symptoms and/or biological mechanisms, and much more. I haven’t had a chance to read the paper in full yet, but I anticipate that it will be a valuable resource for future research.
Vaccines still reduce risk of transmission: Another recent paper in Nature reports on the impact of vaccination among inmates in the California state prison system. Researchers at the University of California San Francisco analyzed COVID-19 surveillance data from 35 prisons during the early months of Omicron (December 2021 to May 2022). They found patients infected with Omicron after vaccination and/or a prior infection had lower risks of transmitting the virus to others. The study suggests that vaccination (and prior infection) is still helpful in reducing COVID-19 spread in addition to reducing severe symptoms, even at this point in the pandemic. (H/t Your Local Epidemiologist.)
Coronavirus found in airplane wastewater on international flights: In a small study, researchers at the National Public Health Laboratory of Malaysia tested wastewater samples from 29 flights that arrived at Kuala Lumpur from outside the country. The researchers found that SARS-CoV-2 was present on 28 of the 29 flights—and testing for the remaining flight wasn’t yet complete, according to a local news outlet that covered the study. While this is a relatively small sample, the results suggest that COVID-19 is very prevalent in travel settings. The study also serves as a helpful example for future plane wastewater testing.
New report highlights nursing home issues: A recent report from the American Health Care Association shares results from a survey of 524 nursing homes across the U.S. The findings show challenges with staffing and economic challenges; for example, 84% of the nursing homes surveyed reported “moderate to high levels of staffing shortages,” and 67% of the homes surveyed reported concerns that they may need to close their facilities due to staffing problems. (H/t POLITICO Pulse.)
End of Ebola outbreak in Uganda: Finally, a bit of (non-COVID-19) good news: this week, health officials in Uganda declared the end of the country’s recent Ebola outbreak. The outbreak started in September 2022, and included a total of 164 cases and 55 deaths. The final patient of this outbreak was released from healthcare on November 30, according to the World Health Organization; Uganda successfully curbed the disease’s spread despite a lack of vaccines and treatments approved against the strain of Ebola that was spreading.