Update, May 22, 2022: After this post was published, Becca Malizia, Biobot’s science communication manager, reached out to provide some clarification on the current state of wastewater data in the U.S., as well as on Biobot’s relationship with the CDC. See this follow-up post for more details.
As I mentioned last week: something strange is going on with the CDC’s National Wastewater Surveillance System (NWSS) data.
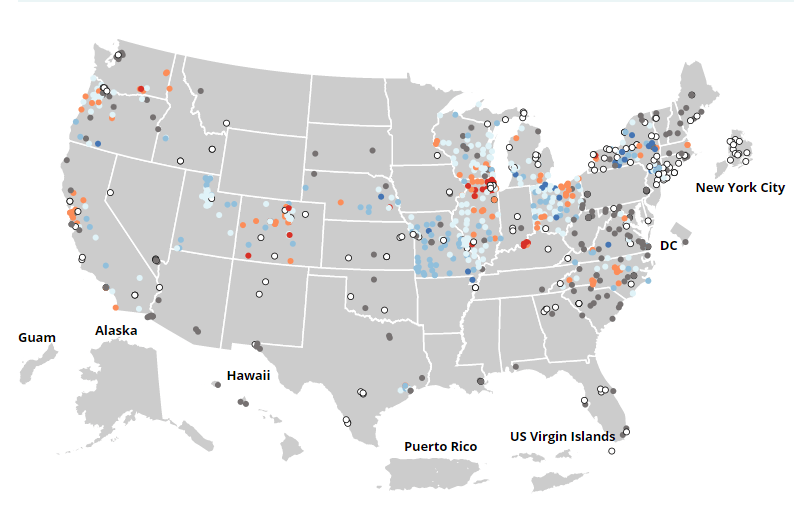
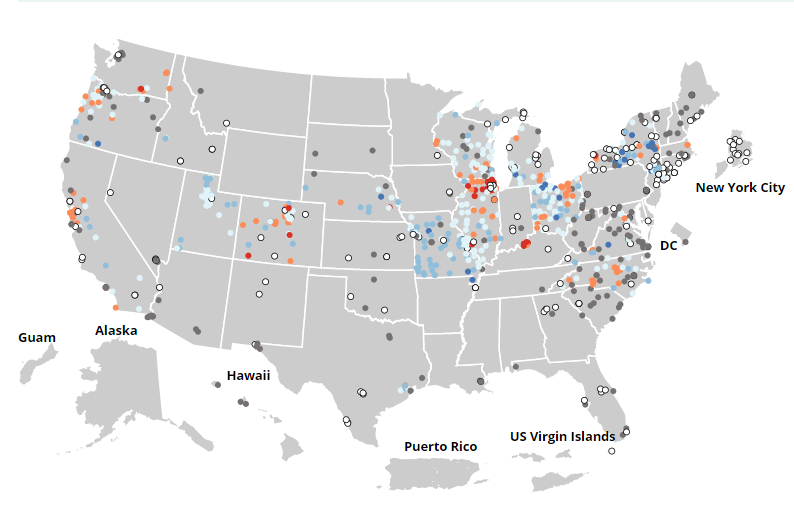
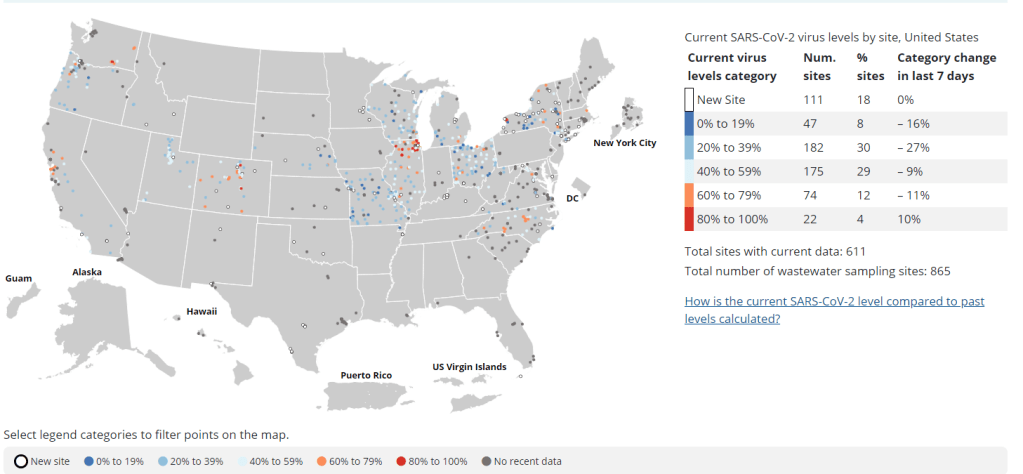
Hundreds of sites on the CDC NWSS dashboard have been labeled as showing “no recent data” for a couple of weeks. As a New Yorker, I pay special attention to the New York City sites; twelve sites in the city were actually removed from the dashboard, then re-added as “new sites,” even though researchers in the city have been testing wastewater for the coronavirus since 2020.
I have yet to do dedicated reporting on this topic, but I wanted to share a bit of information on why I think this is happening. (Please take this with a grain of salt!)
Last winter, as part of CDC NWSS’ efforts to enable more states and counties across the country to test their wastewater for the coronavirus, the agency contracted with LuminUltra, a biological testing company that has become one of the leading wastewater testers during the pandemic. LuminUltra, in conjunction with NWSS and the Water Environment Federation, was responsible for testing and analyzing wastewater for state and local health departments that wanted to set up this monitoring, but didn’t have internal capacity to do so themselves.
LuminUltra’s contract expired last month. In its place, CDC NWSS has set up a new contract with Biobot, another leading wastewater contractor, the company announced this week. Biobot will be responsible for collecting and analyzing wastewater data at 500 sites across the country; it’s unclear from the press release how many of these sites were also part of the old LuminUltra contract, but I’m guessing there’s a lot of overlap.
Here’s the problem, though: LuminUltra stopped testing wastewater at hundreds of NWSS sites last month, but Biobot hasn’t yet resumed testing, data analysis, reporting to the CDC, etc. at all of these locations. As a result, the CDC NWSS dashboard currently includes a number of sites labeled as “new” or “no recent data,” making it difficult to actually use this federal source for evaluating wastewater trends.
Considering that we’re facing a surge and U.S. case data are less reliable than ever, this is not exactly a great time to have a gap in our wastewater data! (Also, I think that something else may be going on with the New York City sites, but that’s a topic for another post.)
As I said above, I haven’t done much reporting on this myself yet, but I wanted to share a relevant section from a recent Tampa Bay Times investigation about wastewater surveillance in Florida:
One of the largest players in the private testing market is Biobot Analytics, an MIT start-up that wants to market the technology.
Last year the company raised $20 million. It already has contracts with more than 700 municipalities in all 50 states, according to the Boston Globe, including Hillsborough County. But Biobot does not report that data to the CDC. Instead the company shares the data on its website, using its methodology.
Biobot, which collects data from six Florida counties, said it’s up to local governments to share COVID-19 data with the CDC.
The company started collecting Hillsborough’s data in June 2021. A county spokesperson said they haven’t received any reports from Biobot.
The amount of coronavirus detected in Hillsborough’s wastewater has doubled in the past month, according to Biobot’s website. It’s an estimate based on the county’s Northwest Regional Water Reclamation Facility and the city of Tampa’s Howard F. Curren facility.
It’s unclear if Biobot’s data-sharing policy will affect the nation’s wastewater surveillance program. The company took over the federal program on April 15, when it was awarded a $10.2 million contract to oversee the next year of testing.
That contract covers 500 utility providers across the country, according to the CDC. But Biobot and the CDC say the company won’t share COVID-19 data from the 700 utilities not covered by the contract.
I’m elevating this because, first of all, everyone should read the Tampa Bay Times piece—it is excellent local reporting on this issue. And second of all: does this mean that, even as Biobot takes over sampling and analysis for sites in the CDC NWSS network, the Biobot and CDC data systems will not be fully integrated?
This seems like a major challenge for a data network that is already quite fragmented, and I would love to see more transparency from the CDC on the whole situation. If anyone else is reporting on this or has additional information, please reach out!
Anyone who’s pulled up the CDC’s National Wastewater Surveillance System (NWSS) dashboard in the last week or two has likely noticed this trend: hundreds of sewershed sites are currently marked as “no recent data.” I keep a particularly close eye on the sites in New York City, which have been reporting “no recent data” for at least two weeks.
According to the CDC, a site marked as “no recent data” has reported findings from fewer than two wastewater samples in the last 15 days. In practice, it could either indicate that a site actually isn’t sampling its wastewater frequently enough for the CDC’s standards, or it could indicate a lack of capacity to process those samples. Probably, both things are happening at a lot of these sites.
From corresponding with press officers at NWSS, I know that the team is working with state and local health agencies, as well as with individual sewershed sites, to ensure accurate data and standardize reporting. This is a massive task, considering that wastewater surveillance started as a grassroots effort in labs with many different sampling and analytical methods, and I appreciate the NWSS team’s efforts.
But I think they could increase transparency about the sites where recent data isn’t available—either on the dashboard itself or in other public communications. I shouldn’t have to hunt through Twitter replies to find the most basic info about wastewater data updates! Especially when this source is becoming increasingly important in the wake of less reliable case data.
Yes. @amylizk said they have been having some staffing issues. They are looking into it.
CDC adds second boosters to its vaccine dashboard: In the latest update to the CDC’s COVID Data Tracker, you can now find a national tally of Americans who have received second booster shots on the “COVID-19 Vaccinations in the United States” page. About 10 million people have received these additional shots as May 6, about one-tenth the number of first booster recipients. The CDC has yet to add state-by-state or demographic data for second boosters.
KFF updates COVID-19 Vaccine Monitor: This week, the Kaiser Family Foundation published the latest update of its Vaccine Monitor, a long-running project tracking Americans’ attitudes towards COVID-19 vaccines and related issues. One notable finding from the April update: just 18% of parents with children under age five are “eager to get their child vaccinated right away,” compared to 27% who say they will “definitely not” get their child vaccinated. This report also includes survey findings on mask-wearing, COVID-19 in the workplace and in schools, and future booster shots.
Biobot on GitHub: I recently learned that Biobot Analytics, the leading COVID-19 wastewater surveillance company, publishes its underlying data on GitHub. This repository includes coronavirus concentrations in wastewater treatment plants monitored by Biobot across the country, along with regional wastewater data, national data, and COVID-19 case numbers for comparison.
TON’s Guide to Tracking Source Diversity: Not directly COVID-related, but a resource that I thought readers may find useful: The Open Notebook (TON) has published a detailed guide for journalists seeking to track the diversity of sources interviewed for their stories. While TON is geared towards science writers, this guide is broadly applicable to any reporter who spends a lot of time seeking out and talking to experts.
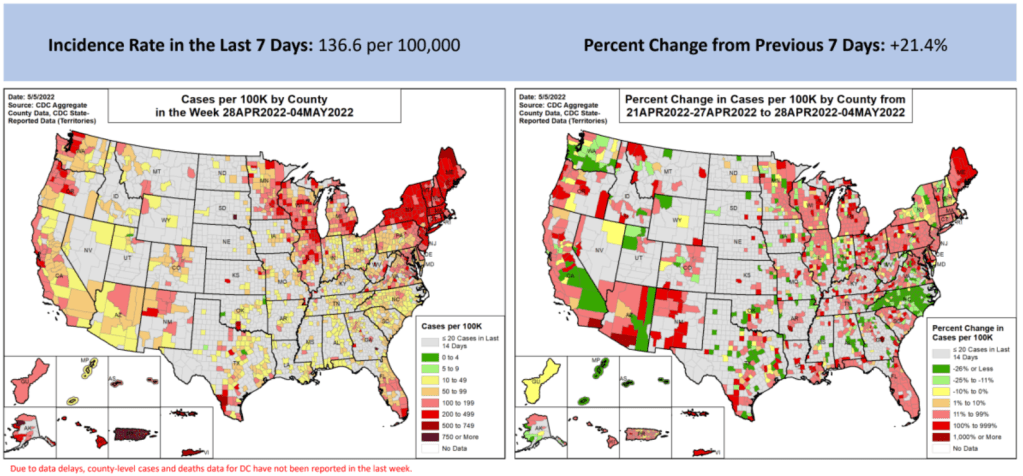
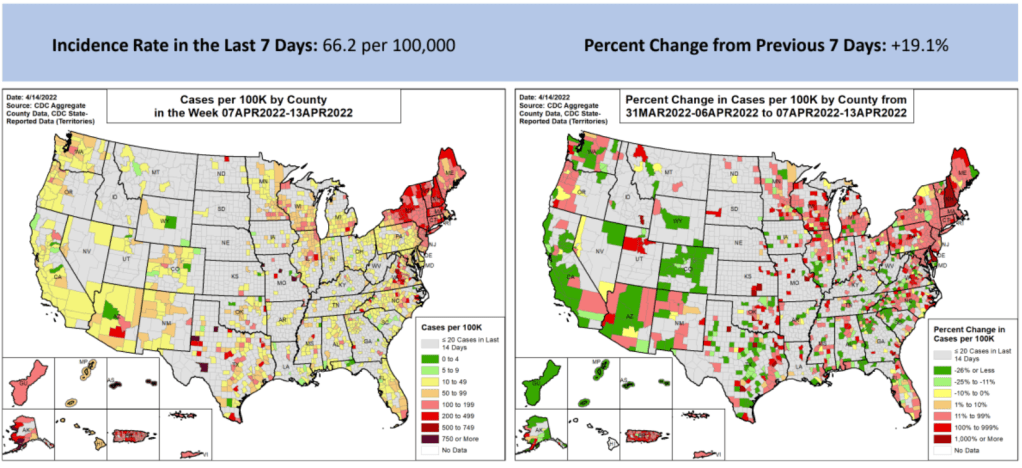
These maps from the May 5 Community Profile Report look pretty different from the CDC’s all-green “Community Levels” map, huh?
In the past week (April 30 through May 6), the U.S. reported about 450,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 65,000 new cases each day
138 total new cases for every 100,000 Americans
21% more new cases than last week (April 23-29)
In the past week, the U.S. also reported about 16,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 2,200 new admissions each day
4.7 total admissions for every 100,000 Americans
17% more new admissions than last week
Additionally, the U.S. reported:
2,300 new COVID-19 deaths (0.7 for every 100,000 people)
98% of new cases are Omicron BA.2-caused; 37% BA.2.12.1-caused (as of April 30)
An average of 70,000 vaccinations per day (per Bloomberg)
New COVID-19 cases are still rising in the U.S., as the country continues to face the Omicron subvariant BA.2 and its offshoots. While at levels much lower than what we saw in December and January, daily new cases have more than doubled in the last month.
And, as I frequently note these days, case numbers are capturing a small fraction of actual COVID-19 infections, as PCR testing becomes less available and at-home rapid tests become more popular. Hospital admissions, a more reliable metric, have also shot up in recent weeks, with about 50% more COVID-19 patients admitted to U.S. hospitals last week than in the first week of April.
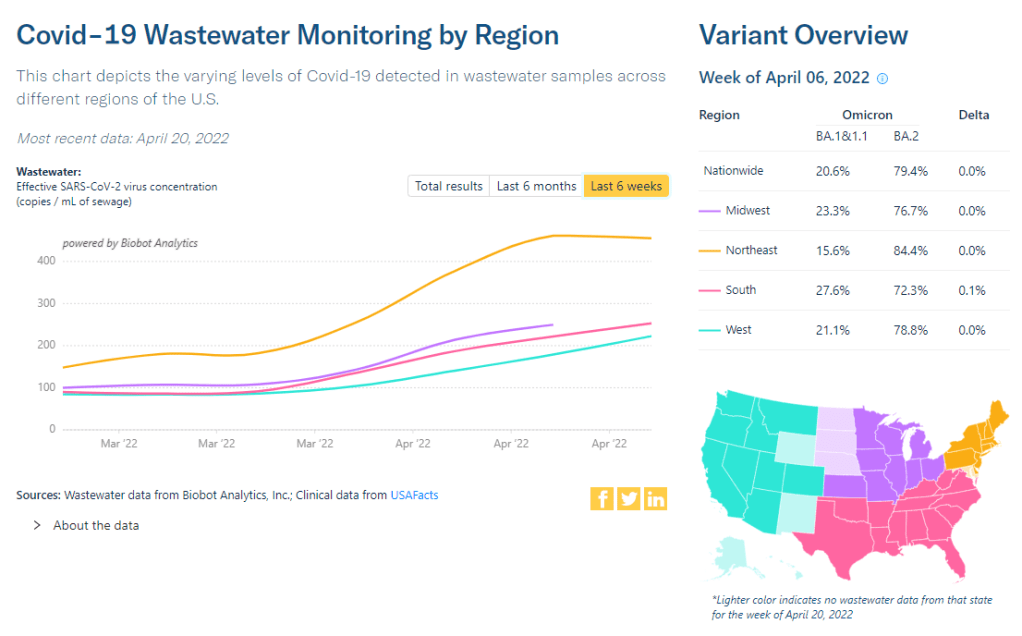
Wastewater data suggest that COVID-19 transmission nationwide may be increasing slightly or in a plateau, far from the kind of exponential increase we saw during the first Omicron surge. Biobot’s dashboard shows that coronavirus levels in wastewater in the Northeast, South, and Midwest continue to increase slightly, while in the West, virus levels have shifted back down in the most recent week of data.
The CDC’s wastewater dashboard similarly suggests that fewer parts of the country are seeing major coronavirus upticks than the national system reported a couple of weeks ago. But this dashboard is a bit incomplete at the moment, with hundreds of sites reporting no recent data, so I take that finding with a grain of salt.
Northeast states continue to report the highest case rates, according to the May 5 Community Profile Report. Maine, Rhode Island, Vermont, Massachusetts, Hawaii, New York, New Jersey, Illinois, New Hampshire, and Connecticut all reported more than 200 new cases for every 100,000 residents in the last week, passing the CDC threshold for a medium “Community Level” (or, under the agency’s old guidance, more than double the threshold for high transmission).
The map on the L is what CDC wants you to see. The map on the R is what you need to see. The map on the L says all but 13% of US is low risk. The map on the R says only 13% is low risk. Hosps have increased 20% over the last 2 weeks. Get boosted & wear a mask in crowded spaces. pic.twitter.com/cUDn8WMink
The BA.2 subvariant is now causing almost 100% of new COVID-19 cases in the country, according to CDC estimates, with the even-more-contagious BA.2.12.1 sub-subvariant causing about one in three of those cases. In the coming weeks, we’ll see how well protection from vaccines and recent Omicron BA.1 infections holds up against these more-transmissible versions of the virus.
For my recent wastewater data story, I’ve been looking at a lot of wastewater surveillance dashboards from different health agencies and research groups.
One of my favorites is from Sewer Coronavirus Alert Network (SCAN), a project based out of Stanford University. The project started with sewershed sites in California but is now expanding to other parts of the country, I learned from Marlene Wolfe, an environmental scientist at Emory University who works on the project (and whom I interviewed for the story).
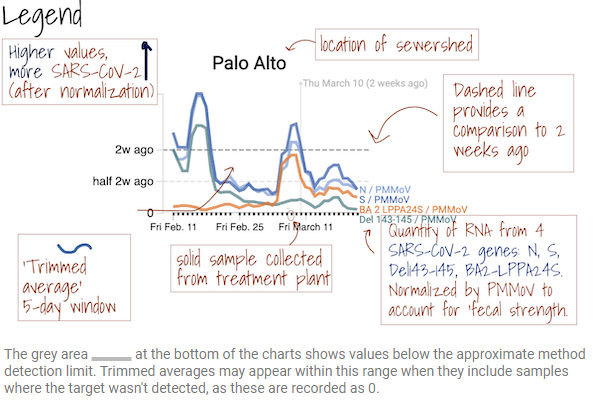
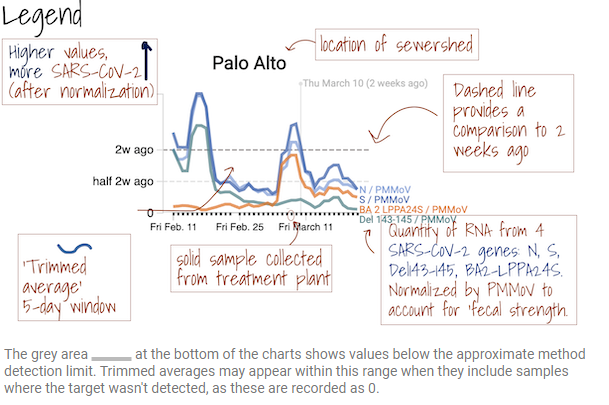
The SCAN dashboard includes a detailed legend instructing users on how to view wastewater data.
I like this dashboard because it does a good job of explaining exactly what users are looking at. On the top of the page, you see a legend walking you through the charts that appear below, along with a map showing the regions covered by these sewersheds.
The charts themselves have built-in context for users seeking to interpret recent trends: you can see how current coronavirus levels compare to levels from two weeks ago. And you have the option to toggle between different timescales: four weeks, six weeks, 12 weeks, six months, a year, and all surveillance since fall 2020. Other parts of the dashboard allow users to look at data that have been smoothed and normalized, showing how interpretations of coronavirus levels in wastewater may change depending on the analysis method.
COVID-19 levels in waste—or, from our poop—have become an increasingly popular data source in the last couple of months (in this newsletter and for many other reporters and commentators), as PCR testing sites close and at-home tests become the norm. Wastewater can provide us with early warnings of rising transmission, and it includes COVID-19 infections from people who can’t or don’t want to get a PCR test.
But wastewater surveillance is very uneven across the country, as I’ve noted before. A lot of local health agencies, research groups, and utility companies are now trying to expand their COVID-19 monitoring in wastewater, but they face a lot of barriers. My reporting suggests that we are many months (and a lot of federal investment) out from having a national wastewater surveillance system that can actually replace case data as a reliable source for COVID-19 trends and a driver for public health action.
Wastewater surveillance is highly sensitive to changes in a community’s coronavirus transmission levels, particularly when those levels are low, as has been the case across the U.S. in recent weeks.
Every wastewater collection site is different, with unique environmental and demographic factors – such as weather patterns or popularity with tourists – that must be accounted for.
While the CDC has led some coordinated efforts through the National Wastewater Surveillance System (NWSS), wastewater sampling techniques overall aren’t standardized across the country, leading to major differences in data quality.
Sparsely populated, rural communities are particularly challenging to monitor, as their small sizes lead to even more heightened sensitivity in wastewater.
Wastewater data is hard to communicate, especially when public health officials themselves aren’t sure how to use it. The CDC’s NWSS dashboard is a prime example.
As bonus material in today’s COVID-19 Data Dispatch, I wanted to share one of the interviews I did for the story, which provides a good case study of the benefits and challenges of COVID-19 surveillance in wastewater.
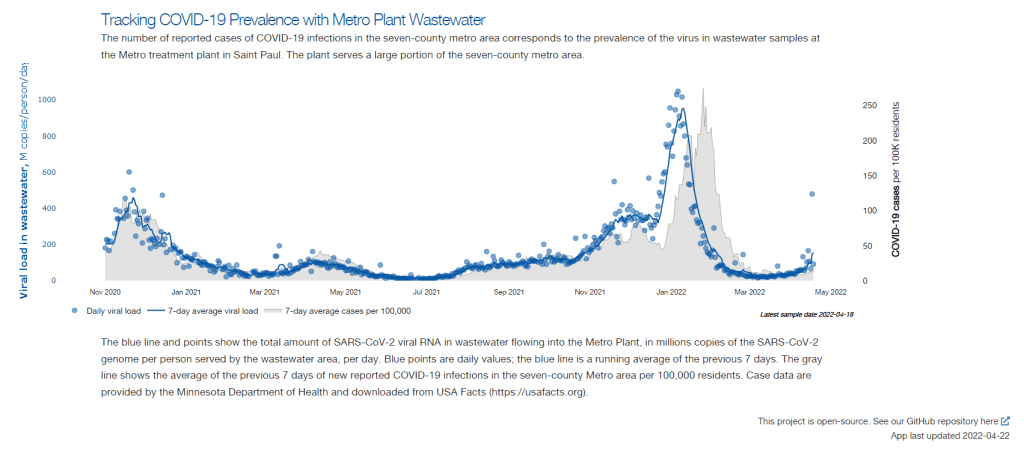
In this interview, I talked to Steve Balogh, a research scientist at the Metropolitan Council, a local agency in the Twin Cities, Minnesota metro area that manages the public water utility (along with public transportation and other services). Balogh and his colleagues started monitoring Twin Cities’ wastewater for COVID-19 in 2020, working with a research lab at the University of Minnesota.
Balogh gave me a detailed description of his team’s process for analyzing wastewater samples. Our conversation also touches on the learning curve that it takes to set up this surveillance, the differences between monitoring in urban and rural areas, and the dynamics at play when a wastewater plant suddenly becomes an important source for public health information. Later in the interview, Bonnie Kollodge, public relations manager at the Metropolitan Council, chimed in later to discuss the wastewater data’s media reception.
This interview has been lightly edited and condensed for clarity. Also, it’s worth noting that the interview was conducted in early April; since then, COVID-19 levels have started rising again in the Twin Cities metro area’s wastewater.
Betsy Ladyzhets: The first thing I wanted to ask about was, the backstory of sampling at the Metro Plant. I saw the dashboard goes back to November 2020, and I was wondering if that’s when you got started, and how that happened?
Steve Balogh: We actually started looking into it in April of 2020. And we contracted with Biobot at that time… But in May, their price went up, so we started looking for alternatives. Then, we started a partnership with people at the University of Minnesota Genomics Center, who know about measuring RNA in things.
At that point, we tried to figure out how to extract the RNA from our samples. They [University of Minnesota researchers] didn’t know anything about wastewater, but they knew everything about RNA. We know all about wastewater, but we don’t know anything about RNA. So it was a good match.
That summer, [the university researchers] started trying to do the extractions and it didn’t really work out so well… So we said, “Okay, we’re going to try this.” By September of 2020, we had built our own lab, and we were trying out our own extractions, based on what we were seeing in the literature, and all the preprints that were piling up. In October, basically we settled on [a sampling process] that worked. And by November 1, we were actually getting data.
BL: Yeah, that definitely aligns with what I’ve heard from some of the other scientists I’ve talked to who have worked on this, where it’s like, everybody was figuring [wastewater sampling methods] out on their own back in 2020.
SB: Yeah, it was on the fly. Papers were coming out daily, just about, with new ideas on how to do things. And we had, like, four different extraction methods that we wanted to look at, also looking at sludge, in addition to influent wastewater… Honestly, it was pretty much pure luck that we settled on [a method] that really, really worked.
We tried to get daily samples, and to put up numbers and see what [the data] looked like. And it actually did work—it actually tracked the reported caseload quite well. We figured, well, it must be working. We also did QA [quality assurance] in the lab, spiking the samples with known amounts of RNA, and trying to get that back. And all of that came back really well, too. So, we have a lot of confidence in our method.
BL: So that [QA] is like, you put in certain RNA, and then you check to make sure that it shows up in the sample?
SB: Exactly, yeah.
BL: What is your process for analyzing the samples and distinguishing those trends, like seeing how they match the case numbers?
SB: We do the extractions at our lab, with the samples from the Metro Plant. We take three milliliters of wastewater and we add 1.5 milliliters of something called Zymo DNA/RNA Shield, from a company in California called Zymo. That’s a buffer that stabilizes the RNA—it basically explodes whatever virus particles are in there, breaks them up, and then it stabilizes the RNA in the sample. So you can actually store those samples at room temperature for days, or maybe even weeks, because the RNA is stabilized.
Then, we put that treated sample through a two-step extraction process. The first step is, we put the whole thing into a Zymo III-P column, combined with 12 milliliters of pure ethanol, and run that through the column. This is a silica column, so the RNA in the sample binds to the silica. Then we wash it and elute that RNA in 200 microliters of water. And then we take that 200 microliters, and run it though the second stage, which is just a smaller silica column. The RNA that’s in that 200 microliters binds onto the smaller column, and then we wash it and elute that into 20 microliters.
Our total concentration is going from three milliliters of wastewater down to 20 microliters of pure water. That’s a concentration factor of 150. We figured that would work for pretty much most situations, and it’s turned out to be true.
Then, we store those samples at minus 80 degrees Celsius. Until we take them over weekly to the University of Minnesota, where they do droplet digital PCR, RT-PCR, to amplify and detect the RNA that’s in our samples. We started out just getting the total viral load back in November 2020. But then, in the early part of 2021 when Alpha showed up, we started doing variant analysis as well. We’re now also looking for specific mutations that distinguish the different variants of concern, like Alpha and Delta and Omicron.
BL: So, you take the samples every day, but then you bring them over [to the university] once a week, is that correct?
SB: That’s correct.
BL: When you’re getting that data, coming from the U of MN lab, what are you doing to interpret it? Or, in communicating the data on your dashboard, what are the considerations there?
SB: We work up the numbers and calculate a total load of the virus, or the particular variants, that’s coming into the plant. And then we basically put that up on the dashboard. There’s not a whole lot of interpretation or manipulation of the data—we’re simply importing the load, basically, of what we see coming into the plant. The load is the concentration that we’ve measured in the sample, times the total volume of wastewater coming into the plant.
We think that’s a sufficient normalization procedure for a large wastewater treatment plant. I know some groups are using other normalization techniques, but we think load is sufficient to tell us what’s happening out in our sewer shed.
BL: Yeah, that makes sense. I know this gets more complicated when you have smaller sites, but your sewer shed is serving a big population—
SB: Almost two million people. Yeah, it’s a big sewershed. If you had 50% of your population leaving during the day to go to work in the next community, that would be something that you might have to consider using other normalization techniques. But that just isn’t the case [in the Twin Cities]. We see a pretty steady signal here.
BL: Makes sense. Have you considered expanding to other sites? Or are is the plan to just stick with sampling at the main sewer ship location?
SB: We already have, actually. We operate nine different wastewater treatment plants in the seven-county metro area. And we’ve already expanded to three of those other sites, so we now have four total plants that we’re taking samples at and having them analyzed at the Genomic Center. It only started within the last month, so we don’t have quite the database to really start showing it on our dashboard yet. But when we do [have more data], our plan is to put that up [on the dashboard] as well.
BL: Do you have a sense of how much time it might take before you feel the data is useful enough to put on the dashboard?
SB: Part of the problem has been, all of these samples that we’re getting from these other plants, we’re just taking the entire sample over to the Genomics Center, and they’re doing the extractions. They’re using my extraction procedure, but they’re doing it in their lab. So, there was some learning curve for them to figure that out. And also to hire staff and come up to speed in terms of facility, and procedure, and people… Now, it’s been a few weeks, and I think they’re just about there [in getting a handle on the RNA extraction methods]. So, I think our data will start to shape up pretty quickly.
Another thing that may be keeping us, at this point, from showing the data is, nothing’s happening. We’re at this bottom [with low coronavirus levels in the wastewater] where everything just looks noisy, because nothing’s changing. But as soon as we start to go up, and if we get higher—the current position is just going to look like a flat line. But right now, people could look at it and say, “Well, that’s just junk.”
So, in that sense, we just don’t want to confuse matters and say, “Here’s a bunch of junk for you to look at. We want to put it into some context. And the context really is, when things start taking off, then you see, “Oh, it used to be very low. And now it’s very high.”
BL: That makes a lot of sense. Also, I hear you on the challenges of learning these methods. I was a biology major in school, and I worked in a lab, briefly, that did RNA extraction. And I remember how tricky it is, so I can envision the learning curve.
SB: Well, these are experts at the Genomics Center, they know what they’re doing. But I think even they have been surprised at how how robust the viral RNA is in wastewater. A lot of people at the beginning of this pandemic said, “You’ll never see it in wastewater. It’s RNA, RNA is very sensitive, it’ll break down.” But that just isn’t the case—the RNA is quite robust in wastewater, and the signal lasts for a long time. It has to last for many hours, for it to travel from the far end of our sewershed to get to us [at the treatment plant]. And then, even in the refrigerator, when you refrigerate just the raw sample, it’ll stay in a reasonable concentration without dropping too much for days.
BL: What has the reception to this work been from the public, the state health department, or from local media or other people who are using and watching the data?
SB: It’s been incredible. You can ask Bonnie more about it.
Bonnie Kollodge: It’s ginormous. I mean, it just has spread everywhere. I don’t even know the social spread, but I think somebody was tracking our impressions in print and online media… I think there were, like, 11 million impressions between January and the end of March. And we get lots of requests for Steve’s time, lots of requests for a daily accounting [of the data].
When we began this work, it really was out of public service—seeing that there’s a pandemic going on, and what can we do to help? That’s when they started developing this idea, then working with the Depratment of Health, which is really our state lead on this [COVID-19 response]. They came to rely heavily on our information, to compare it against what their test results were showing. Then, as people started to do home testing, that was a whole other factor. It was really wastewater that was taking the lead on showing what was happening with the virus and the variants…
Every week, we put an update online, and reporters go right to it, to determine how they’re gonna position [their COVID-19 updates]. Steve also provides, in addition to the data, a little narrative about what’s happening that helps reporters—some who are very conversant in data, but others who are not—it helps them it understand what we’re seeing.
BL: I can see how that would be helpful, especially if you’re releasing a week’s worth of data points at once. You sort-of have a mini trend to talk about.
BK: Yeah, and we send it to the governor’s office, and to the Health Department. They appreciate the transparency… They know what’s happening [with the virus], and can adapt.
BL: Right. And Bonnie, you mentioned something I wanted to ask more about, which is how the increased use of at-home tests and lower availability of PCR tests has increased the demand for wastewater data in the last few months, in particular. Now that you maybe have less reliable case data to compare against, has the thinking and interpreting the wastewater data shifted at all?
SB: I think we’ve actually had that statement from reporters. They’ve said, “We can’t trust the testing data anymore. And it’s going to be wastewater from here on out.”
BK: Just this week, there was a reporter who asked to get early results tomorrow. And he said, “This [wastewater data] is what I’m watching.” … The public has glommed on to this resource as a demonstration of what’s happening. And, like Steve said, it’s not a small sample. There are almost two million people served by this by this particular plant.
BL: From what I understand, part of what can be really helpful [with wastewater data] is when you have that longevity of data, as you all do. You have a year and a half of trends. And so when you see a new spike, it’s easier to compare to past numbers than for other parts of the country that are just starting their wastewater surveillance right now.
SB: Yeah. I think the other thing that has been really useful for our [state] department of health is, they’ve really appreciated the variant data that we have. That was really the first thing that got their attention… And we were giving them [variant] data ahead of time. The clinical tests were taking days or weeks to come back, and we could give them variant data the same week. So, that was the first thing that got our department of health here interested. But when they saw that we can track trends, they recognized that this has value at lower levels when testing goes away, basically.
BL: How would you want to see support from the federal government in expanding this wastewater work? Like you mentioned, getting it in more treatment plants, and any other resources that you feel would be helpful.
SB: Well, I think that’s underway, as we understand it, with the National Wastewater Surveillance System, NWSS. I think they’re funded through 2025, and I think the goal there is to basically sign up as many treatment plants as they can in the country.
Hopefully, that’s the beginning of something that is going to go beyond the pandemic, and give us a measure of community health in the future. Because wastewater is a community urine test, basically. It’s everybody contributing, and it can be useful for other pathogens and viruses in the future. So, yeah, [expanding that network] would be great. Let’s do it.
BL: Do you envision adding other viruses to the testing that you’re doing? Flu or RSV are ones that I’ve heard some folks are considering.
SB: Yeah, that would be something to do going forward for us. Though, it’s not clear how long we continue this work, just because these other projects are expanding, like the national project. And even our department of health here [in Minnesota] is talking about bringing this type of analysis into their own laboratory. Certainly going forward, long-term, that would be a goal for any work done here in Minnesota—to add those things to the menu of what we’re analyzing.
BL: Right. So you might be taking the samples to the Minnesota health department instead of the university, or something like that?
SB: Someday. Yeah, we just don’t know at this point.
BK: This is an evolving scinece. And this is not what we typically do—I mean, we do wastewater collection and treatment. So this [COVID-19 reporting] is a little outside of our regular parameters. But, like Steve and his superiors have been saying, this is an evolving science, so let’s see where this takes us, in terms of infectious disease.
It’s funny, when I go out and talk to people and say, “I work for the Met Council, and I help in communications with the wastewater analysis,” everybody knows what I’m talking about. It’s just so much out there. But I think that these things [testing for other diseases] are all being explored, and this has really opened up new possibilities.
SB: From the beginning, it’s just been a scramble. You don’t know what’s going to be coming. What I’m doing, a lot, is trying to get ourselves in a position so that, when the next variant of concern pops up, we have an assay that can measure it. There’s still a lot of unknowns about what’s going on, and everything’s new every day, just about.
Coronavirus levels in wastewater may be plateauing in the Northeast, while the remaining regions of the country catch up. Chart via Biobot, retrieved on April 24.
In the past week (April 16 through 22), the U.S. reported about 300,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 43,000 new cases each day
91 total new cases for every 100,000 Americans
35% more new cases than last week (April 9-15)
In the past week, the U.S. also reported about 11,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 1,600 new admissions each day
3.4 total admissions for every 100,000 Americans
8% more new admissions than last week
Additionally, the U.S. reported:
2,600 new COVID-19 deaths (0.8 for every 100,000 people)
93% of new cases are Omicron BA.2-caused; 19% BA.2.12.1-caused (as of April 16)
An average of 100,000 vaccinations per day (per Bloomberg)
After weeks of me warning about it, a BA.2 surge is upon us. Nationwide, new COVID-19 cases have gone up for the third week in a row; we’ve seen a 68% increase since the last week of March.
And that’s just the reported cases: Americans may be doing about four times more at-home tests than they’re doing lab-based PCR tests, according to Mara Aspinall, a COVID-19 testing expert (who cowrites a testing-focused newsletter). The vast majority of these at-home tests are never reported to public health officials and don’t make it into our trends analysis.
But there are other metrics that similarly indicate a national rise in coronavirus transmission. Viral levels in wastewater are going up, according to both Biobot’s tracker and the CDC’s national monitoring system; the CDC’s COVID-19 data team noted in this Friday’s Weekly Review that “more than half of all sites reporting wastewater data are experiencing a modest increase in SARS-CoV-2 levels.” Some of these increases are going from very low to still low, but they’re still worth watching.
The U.S. is also reporting an increase in new COVID-19 patients admitted to hospitals: about 11,000 people this week, up from 10,000 last week. New hospitalizations lag behind cases slightly, but they are a more reliable metric, as anyone with symptoms severe enough to require hospitalization generally will seek care (so, underreporting is less of a concern.)
At the regional level, the Northeast is still seeing the highest case rates: leading jurisdictions include Vermont, Washington D.C., New York, Rhode Island, and Massachusetts, according to the April 21 Community Profile Report. The Northeast—particularly New York and New Jersey—is also a hotspot for the Omicron sub-subvariant, BA.2.12.1.
To borrow an analogy from my sister (an engineering student): the emergence of these new Omicron sublineages feels like when you’re trying to do a problem set that claims to have five problems, but then each problem has several sub-problems, and those sub-problems themselves have more sub-problems. In the coming weeks, we’ll see just how much more transmissible Omicron can get.
There’s some good news, though: cases in some parts of the Northeast might be plateauing. It’s hard to tell for sure because of the aforementioned unreliable data, but wastewater data for the region (as well as for individual cities like Boston) seem to be leveling off; we’ll see next week if this trend continues.
A Poor People’s Pandemic Report: This new report, compiled by the Poor People’s Campaign (a national activist group that advocates for low-income Americans) as well as U.N. economists and other researchers, shows the pandemic’s disproportionate impacts by income levels. Overall, people in poorer counties died of COVID-19 at nearly twice the rate of those in richer counties, the report found. On this dashboard, users can see the correlations of COVID-19 death rates with income, population density, and other factors. This article from the Guardian includes more context on the findings.
SARS-CoV-2 in Animals: I recently learned about this dashboard while working on an upcoming Documenting COVID-19 story: the U.S. Department of Agriculture (USDA) reports on COVID-19 cases in animals, identified through both PCR and antibody tests. In addition to the case numbers, the dashboard includes announcements of notable cases and recent research in this area. It’s important to note that these numbers are likely undercounts, because the U.S. doesn’t actively monitor animals for COVID-19, unlike some other countries.
The Role of Wastewater Data in Pandemic Management: This new report from the Rockefeller Foundation examines how state and local public health agencies are using wastewater surveillance. The foundation surveyed 12 state and 194 local agencies, many of which have been monitoring wastewater for a year or more; this report includes findings on the populations served by wastewater surveillance, data used to make pandemic management decisions, barriers that agencies face for expanding their surveillance, and more.
GAO report on Wastewater Surveillance: Speaking of wastewater, the U.S. Government Accountability Office (GAO) also released a report on the monitoring tool this week. The GAO report provides an overview of how wastewater surveillance works and its potential for providing early warnings of outbreaks, along with challenges faced by agencies seeking to start testing their wastewater. From the report’s highlights: “the lack of national coordination and standardized methods pose challenges to wider adoption.”
Protection from vaccination and previous infection: A new study, published in the CDC MMWR this week, assesses the benefits of COVID-19 vaccination for people who had a prior infection. During the Omicron surge, the study shows, people who had been previously infected and vaccinated were less likely to be hospitalized due to a COVID-19 reinfection, compared to those who weren’t vaccinated. Vaccine effectiveness against hospitalization was 35% for those who had two doses, and 69% for those who had received a booster.
Pfizer seeks booster shot for 5-11 year olds: This week, Pfizer announced that it’s asking the FDA to authorize a booster shot for children in the 5 to 11 age group. The company cited new data showing that kids who got a booster shot six months after their primary series experienced a significant increase in antibodies that protect against COVID-19. These data have yet to be published in a scientific report or vetted by experts, though. Also, still no news on Pfizer’s vaccine for younger children (which could also require three doses).
In the past week (April 9 through 15), the U.S. reported about 220,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 31,000 new cases each day
67 total new cases for every 100,000 Americans
19% more new cases than last week (April 2-8)
In the past week, the U.S. also reported about 10,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 1,400 new admissions each day
3.1 total admissions for every 100,000 Americans
1% more new admissions than last week
Additionally, the U.S. reported:
2,900 new COVID-19 deaths (0.9 for every 100,000 people)
100% of new cases are Omicron-caused; 86% BA.2-caused (as of April 9)
An average of 100,000 vaccinations per day (per Bloomberg)
New COVID-19 cases in the U.S. have gone up for the second week in a row, and the increase was sharper this week. While the daily average of new cases (about 31,000) remains low compared to the Omicron surge, this trend is still concerning—especially when factoring in all the at-home rapid tests that are going unreported right now.
Wastewater trends suggest that cases will continue rising in the coming weeks. Biobot’s dashboard suggests a national increase (most pronounced in the Northeast region), while about 60% of sites in the CDC’s network have reported increasing coronavirus levels in the last two weeks.
Newly hospitalized COVID-19 patients, an indicator that’s typically behind cases but more reliable, is also showing a small increase as of this week. This will be an important metric to watch in the next few weeks: will BA.2 strain hospitals the same way that Omicron BA.1 did in December and January?
BA.2, it’s important to note, is now causing the vast majority of new COVID-19 cases in the U.S. The CDC’s latest estimates suggested that this sublineage made up 86% of cases in the week ending April 9. And some parts of the country may be seeing further mutation of BA.2—more on that later in the issue.
The Northeast continues to be a leader in this surge, as shown by both the wastewater trends and case data. According to the April 14 Community Profile Report, states with the highest case rates in the last week include: Vermont, Washington D.C., Rhode Island, New York, Massachusetts, Alaska, New Jersey, Maine, Connecticut, and New Hampshire.
All of these states are seeing high transmission, according to the CDC’s old guidance. But the new guidance places most counties in these states in low or medium “community levels;” largely because hospitalizations—which, again, are a lagging indicator—haven’t started rising yet.
This week, Philadelphia became the first major U.S. city to once again require masks in public indoor spaces, in response to rising cases and hospitalizations. I hope to see other cities and localities follow Philadelphia’s lead, but I know current attitudes make this unlikely.
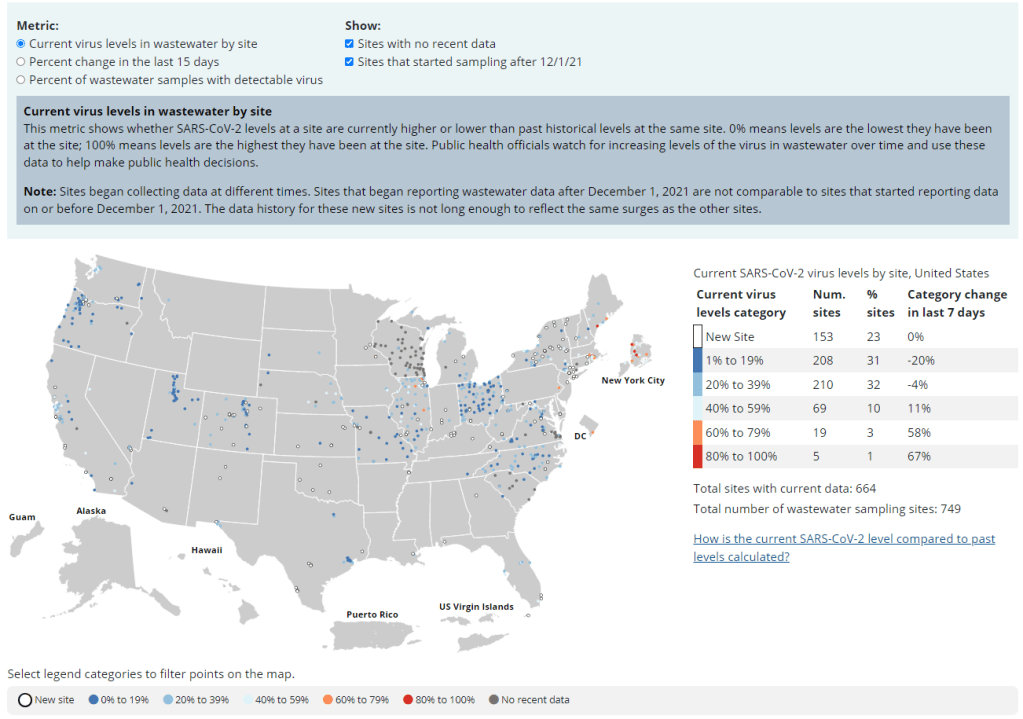
The CDC’s updated wastewater dashboard includes more metrics and more context for people seeking to understand wastewater trends in their area.
After the CDC released its National Wastewater Surveillance System (NWSS) dashboard in February, the agency faced some criticism from scientists, data reporters, and others who found this dashboard didn’t actually do a very good job of presenting wastewater data. The initial dashboard only included one metric, percent change in wastewater levels over the last 15 days; without more context, it was difficult to understand where a high percent change was actually cause for concern.
But the CDC has responded to its criticism! This past Friday, the agency updated its wastewater dashboard to include a lot more context. Among the changes:
You can now toggle between three metrics: the old percent change value, along with current virus levels in a site’s wastewater and the share of wastewater samples at a given site that tested positive for the coronavirus in the last 15 days.
Clicking on a specific site provides users with a mini-chart of wastewater levels at that collection spot over the last few weeks.
The dashboard lets you toggle on and off sites with no recent data and sites that started sampling during the Omicron wave.
Above and below the dashboard, the CDC has added more definitions and explanations to help users understand what they’re looking at.
On Friday evening, I posted on Twitter, asking wastewater and data viz experts to weigh in on the updated dashboard:
wastewater people and/or data viz people, what are your thoughts on the updated CDC NWSS dashboard? is it clearer to read and interpret now? cc @COVIDPoops19pic.twitter.com/xOoCWEVFdE
Responses were mostly positive, with researchers saying that they were glad to see the CDC respond to criticism and add more information to the dashboard. Still, there’s more the agency can do, such as adding the population sizes covered by each site and, maybe, moving away from percentage changes as such a central metric.
To quote Claire Duvallet, data scientist at Biobot: “I think collapsing all three metrics to have the same units, and to choose percentage as that unit, is very confusing. Percentage changes are already so 🤯 to think about, & percentage changes of categories of percentages is just too much for my brain.”
I *really* appreciate the rapid response to public feedback from CDC NWSS & am happy to see this update, and actually think that the metric of "how high are recent samples relative to all other measurements from this site?" is a useful way to interpret WW data. https://t.co/tOznP5e6Nr