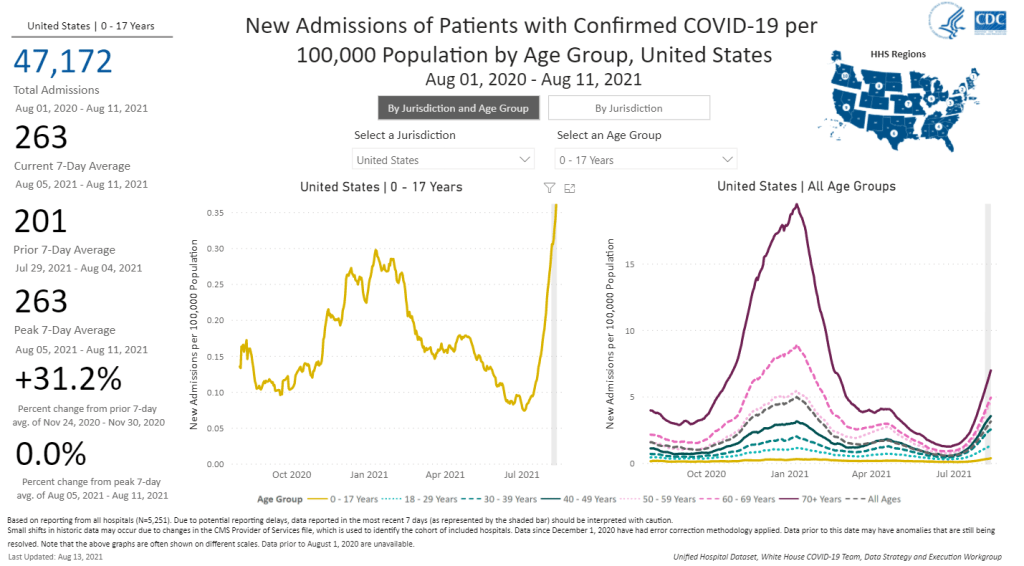
The number of children hospitalized with COVID-19 has shot up in recent weeks. Chart from the CDC COVID Data Tracker.
A couple of additional items from this week’s COVID-19 headlines:
1,900 children now hospitalized with COVID-19 in the U.S.: More kids are now seriously ill with COVID-19 than at any other time in the pandemic. The national total hit 1,902 on Saturday, according to HHS data. Asked about this trend at a press briefing on Thursday, Dr. Anthony Fauci explained that, thanks to Delta’s highly contagious properties, we’re now seeing more children get sick with COVID-19 just as we are seeing more adults get it. The vast majority of kids who contract the virus have mild cases, but this is still a worrying trend as schools reopen with, in many cases, limited safety measures. For more on this issue, I recommend Katherine J. Wu’s recent article in The Atlantic.
2.7% of Americans now eligible for a third vaccine dose: Both the FDA and the CDC have now given the go-ahead for cancer patients, organ transplant recipients, and other immunocompromised Americans to get additional vaccine doses. There are about 7 million Americans eligible, comprising 2.7% of the population. Studies have shown that two Pfizer or Moderna doses do not provide these patients with sufficient COVID-19 antibodies to protect against the virus, while three doses bring the patients up to the same immune system readiness that a non-immunocompromised person would get out of two dioses. Still, this move goes against the World Health Organization’s push for wealthy nations to stop giving out boosters until the rest of the world has received more shots.
203 cases so far linked to Lollapalooza, out of 385,000 attendees: Chicago residents and public health experts worried that Lollapalooza, a massive music festival held in the city in late July, would become a superspreader event. Two weeks out from the festival, however, local public health officials are seeing no evidence of superspreading, with a low number of cases identified in attendees. Lollapalooza may thus be an indicator that large events can still be held safely during the Delta surge—if events are held outdoors and the vast majority of attendees are vaccinated. (Officials estimated that 90% of the Lollapalooza crowd had gotten their shots.)
This week, the World Health Organization (WHO) called for wealthy nations to stop giving out booster shots in a push towards global vaccine equity.
These nations should stall any booster shots until at least September, said WHO Director-General Tedros Adhanom Ghebreyesus at a press conference on Wednesday. Instead, excess vaccines should be donated to COVAX, the international vaccine distributor that aims to mitigate COVID-19 in low-income countries. When 10% of the population in every country has been vaccinated, then wealthy countries could resume administering boosters, Tedros said.
I understand the concern of all governments to protect their people from the Delta variant. But we cannot and we should not accept countries that have already used most of the global supply of vaccine using even more of it while the world’s most vulnerable people remain unprotected.
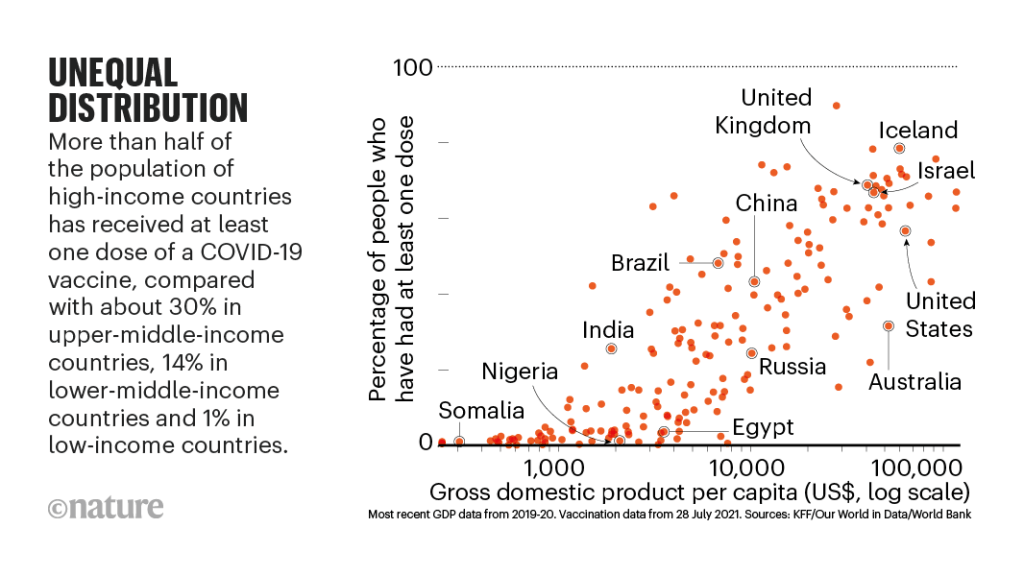
It may seem counterintuitive for a country to not provide its citizens with extra protection when it has the means to do so. But the global numbers are staggering. About 50% of the U.S. population has now been fully vaccinated, and we have doses to spare (some of which are going to waste). Meanwhile, in most African countries, 1% or less of the population is vaccinated. This is even though vaccine demand is actually far higher in low-income nations than in the U.S.
An internal analysis from the World Health Organization (WHO) estimates that if the 11 rich countries that are either rolling out boosters or considering it this year were to give the shots to everyone over 50 years old, they would use up roughly 440 million doses of the global supply. If all high-income and upper-middle-income nations were to do the same, the estimate doubles.
About 3.5 billion people in low- and lower-middle-income countries have yet to be vaccinated, Maxmen estimates. Give one dose to 10% of that number, and you use 350 million doses—less than the 440 million that rich nations would use up with boosters.
The longer that these low-income countries go without widespread vaccination, the more likely it is that new variants will emerge from their outbreaks. This is because, with every new COVID-19 case, the virus has a new opportunity to mutate. We’re already seeing Delta adapt to become even more transmissible and monitoring other potentially-concerning variants, like Lambda.
It’s unclear how much power the WHO has to enforce a booster shot moratorium, especially now that some countries (like Israel) have already gotten started on administering these extra shots. And it’s also worth noting that public health officials in the U.S. are shifting away from using “booster” to describe third shots for immunocompromised people or second shots who for those who received the one-and-done Johnson & Johnson vaccine; they say that these shots rather bring patients up to the same immunity levels as those who received two mRNA doses.
Following the end of the federal public health emergency in May, the CDC has lost its authority to collect vaccination data from all state and local health agencies that keep immunization records. As a result, the CDC is no longer providing comprehensive vaccination numbers on its COVID-19 dashboards. But we still have some information about this year’s vaccination campaign, thanks to continued CDC efforts as well as reporting by other health agencies and research organizations.
This week, the FDA authorized Novavax’s updated COVID-19 vaccine. Here’s why some people are excited to get Novavax’s vaccine this fall, as opposed to Pfizer’s or Moderna’s.
Last week, I asked you, COVID-19 Data Dispatch readers, to send me your stories of challenges you experienced when trying to get this fall’s COVID-19 vaccines. I received 35 responses from readers across the country, demonstrating issues with insurance coverage, pharmacy logistics, and more.
The U.S. missed President Biden’s big vaccination goal: 70% of adults vaccinated with at least one dose by July 4. As of July 3, we are at 67% of adults with one dose, and 58% fully vaccinated.
I did a data-driven look at the vaccination goal this week in a story for the Daily Mail. The story focuses on which parts of the country have met the goal—and which areas fell short. Those under-vaccinated areas are highly vulnerable to the Delta variant (B.1.617.2), which is now spreading rapidly in many of those pockets. Reminder: the Delta variant is much more transmissible than even the Alpha variant (B.1.1.7), and its presence is doubling in the U.S. every two weeks.
There are over 1,000 counties in the U.S. with one-dose vaccination rates under 30%, CDC Director Dr. Walensky said at a press briefing last week. The U.S. has about 3,100 counties in total.
Is your county one of them? Check it out on this interactive map, reflecting data as of July 1:
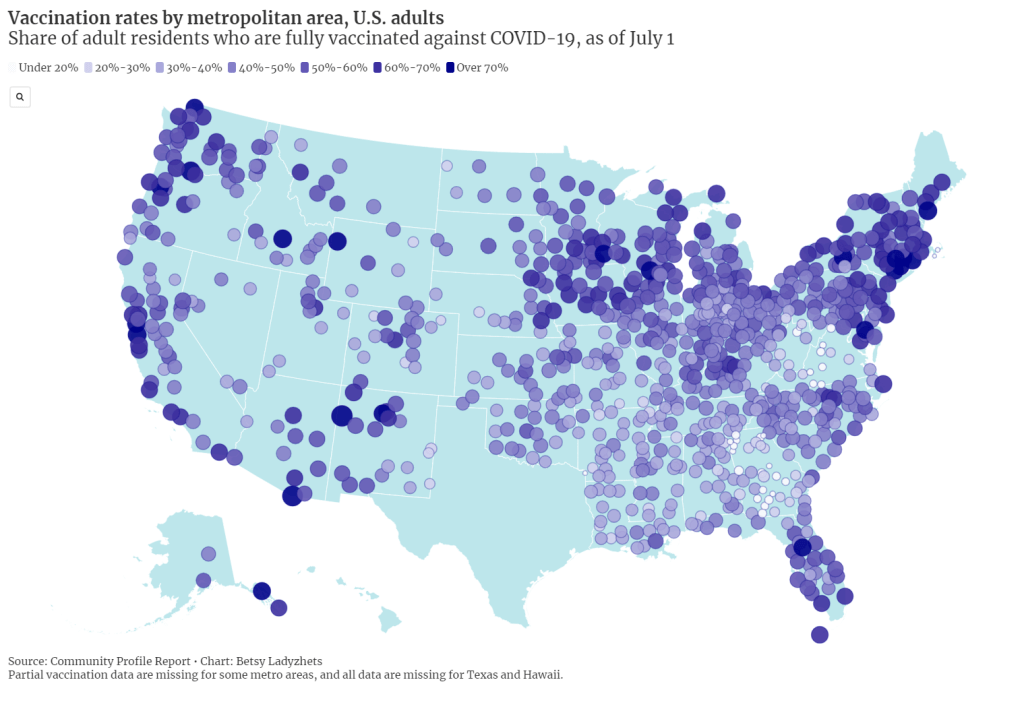
I also made a map showing vaccination rates by metropolitan area. You can clearly see clusters of high vaccination in the Northeast and on the West coast, while parts of the South and Midwest are under-vaccinated. Note that Texas is missing in both this dataset and the county-level data due to issues in the state’s reporting to the CDC.
For my Daily Mail story, I also asked two of the COVID-19 science communicators I most admire to explain the significance of that missed 70% goal. I talked to Dr. Uché Blackstock, physician and founder of the organization Advancing Health Equity, and Dr. Katelyn Jetelina, epidemiologist at the University of Texas and writer of the Your Local Epidemiologist newsletter.
Here are both of their takes on the missed goal:
So, we didn’t meet the 70% goal. It means that we fell short. It also means that we just don’t have enough people vaccinated, not even close, to reach herd immunity.
To me, as an epidemiologist, someone in the field and also someone within a community, it means that we have reached—or are about to reach—saturation [of the vaccine market]. We need to start becoming very innovative about how to address vaccine hesitancy, as well as how to address vaccine equity.
That’s really going to be the next phase of public health approaches. And then, how do we go about doing this… You know, we’re well beyond billboards now. We really need to mobilize a grassroots movement. We need to listen about concerns, we need to educate about these concerns.
And then, we need to make vaccines more accessible. Especially among pediatrics, where—pediatrician offices can’t store the vaccine. So we have to go to schools and really engage with families in a “nontraditional sense.”
Dr. Katelyn Jetelina
This 70%, especially for one dose, is sort of an arbitrary number, because we know that being fully vaccinated is what’s needed to fully protect you against variants. I think it was obviously wise and aspirational to have a goal. But at this point, because we’re basically seeing the number of people vaccinated decreasing weekly, and substantially since last April… I think we need to change our perspective.
We had the early adopters who came in droves to get vaccinated. We’re not going to see the same numbers anytime soon. And so, I think that this idea of having a goal, while it’s aspirational, I think that we have to put that aside and think more realistically about the challenges we’re dealing with.
And the challenges we’re dealing with are actually quite complicated… There are still access issues, although I do think the Biden administration is doing—at least trying to do a substantial job in knocking down those barriers. They’re providing transportation, childcare, increasing the access points for getting vaccinations, encouraging small businesses to offer their workers paid sick leave to get vaccinated and to recover from the vaccine.
But I think this other issue that we’re seeing among people who are not vaccinated, it varies depending on the population, the geographical area. We know rural populations are less likely [to get vaccinated]. And we know that, among the “wait and see” group, about half of those are people of color.
I hate to blame it on this so-called “vaccine hesitancy” because I don’t think it’s that simple. I do think, though, that there is a significant distrust of government, there is distrust of the healthcare system, and there is a lot of misinformation out there about the vaccines. All of these are essentially creating the perfect storm that is preventing us from getting to this aspirational [70%] number.
But here, we’re at this point where it’s a race against the variants, and I think that we just have to get as many people vaccinated as possible. I know that sounds incredibly vague, but that really is the goal.
Dr. Uché Blackstock
I made a third chart for today’s issue, visualizing vaccination rates by state from March through June. It really shows how vaccine enthusiasm has leveled off, just about everywhere in the country—but the plateaus started earlier in many of those states that have lower rates now.
I typically try to avoid anything approaching medical advice in the COVID-19 Data Dispatch, as I am a journalist with just an undergraduate biology degree and a couple of years of science reporting experience. But this week, it feels appropriate to wholeheartedly, unambiguously encourage vaccination.
I know the audience for a publication like this one skews towards people who probably have their shots already. Rather, I want to encourage you to find those people in your community who aren’t yet vaccinated, and help them take that step.
Recent research suggests that lotteries and other large-scale incentives do not significantly encourage vaccination; instead, we need small-scale incentives. One-on-one conversations with people, opportunities for concerns to be voiced and addressed, appointments that can be tailored to the individual’s needs. Anything that you can do to play a role in these initiatives, please get out there and do it.
Of course, if you (or your friends/family/community members/etc.!) have questions about vaccines, or anything else COVID-19 related, you know where to find me. Inquiries welcome at betsy@coviddatadispatch.com.
Following the end of the federal public health emergency in May, the CDC has lost its authority to collect vaccination data from all state and local health agencies that keep immunization records. As a result, the CDC is no longer providing comprehensive vaccination numbers on its COVID-19 dashboards. But we still have some information about this year’s vaccination campaign, thanks to continued CDC efforts as well as reporting by other health agencies and research organizations.
This week, the FDA authorized Novavax’s updated COVID-19 vaccine. Here’s why some people are excited to get Novavax’s vaccine this fall, as opposed to Pfizer’s or Moderna’s.
Last week, I asked you, COVID-19 Data Dispatch readers, to send me your stories of challenges you experienced when trying to get this fall’s COVID-19 vaccines. I received 35 responses from readers across the country, demonstrating issues with insurance coverage, pharmacy logistics, and more.
COVID-19 Vaccine Rollout across US Congressional Districts: This dashboard, from the Harvard Center for Population and Development Studies, breaks down the U.S. vaccine rollout by a geography I haven’t yet seen: Congressional districts. The interactive maps highlight the partisan nature of this vaccine rollout—as POLITICO reporters pointed out in an article citing the tracker, “All but one of the 39 congressional districts where at least 60 percent of residents have received a coronavirus shot are represented by Democrats.”
Vaccination time series from the CDC: The CDC’s vaccine dashboard doesn’t allow users to download time series data (i.e. vaccinations by day), but now, you can find this information on the agency’s data portal. The dataset includes county-level vaccine administrations and coverage rates going back to December 13, 2020.
Methodology changes for Bloomberg’s COVID-19 Vaccine Tracker: Bloomberg’s vaccine tracker is one of the most widely cited in the U.S., and for good reason—it’s incredibly comprehensive, compiling data from every country with an active vaccine rollout (and, in the early weeks of the rollout, from every U.S. state). After months of collecting data by hand, the Bloomberg team is now starting to automate their data collection, Health Editor Drew Armstrong announced this week. Many countries and the WHO are now providing stable enough data sources that such a change is possible.
Fiscal accountability for COVID-19 responses: The International Budget Partnership, a global nonprofit working to improve government budgets, has produced a report and interactive website analyzing accountability measures that international governments have—and have not—implemented as part of emergency COVID-19 responses. Notably, out of 120 countries surveyed, none have “substantive” accountability and only four have “adequate” accountability. (H/t Data Is Plural.)
COVID-19 risk levels for kid-related activities: This one isn’t a data source, per se, but I thought readers might find it helpful. A team of epidemiologists, immunologists, and public health scientists—including Katelyn Jetelina of Your Local Epidemiologist—compiled this detailed guide for families with unvaccinated children. The guide aims to help parents and families navigate their risk levels this summer.
In the reader survey I sent out a few weeks ago, I asked, “What is one question you have about COVID-19 in the U.S. right now?” One reader responded with an inquiry into vaccine equity: “What will it look like when the U.S. is ‘open’ and vaccinated and many other parts of the world are not?”
That question feels especially relevant this week. On Thursday, the Biden administration made a big (and long-awaited) announcement: the federal government is sending 25 million vaccine doses from America’s stockpile to other countries. The administration has previously promised to send at least 80 million doses abroad by the end of June, but this week’s announcement included more details—such as countries that will receive these initial doses and other logistics.
Out of the 25 million, about 19 million doses are going to COVAX. COVAX, a global effort run by the World Health Organization and other international government bodies and philanthropic organizations, brings vaccines to low-income nations at no cost. The COVAX doses will go to India, other parts of Asia, Central and South America, and Africa, Bloomberg’s Josh Wingrove reports.
The remaining 6 million doses will be sent directly to countries, including Ukraine, Kosovo, Haiti, Georgia, Egypt, Jordan and Iraq. Some doses are going directly to India as well—while the worst of this nation’s surge may be over, it’s still facing high case counts, full hospitals, and a terrifying “black fungus” linked with the Delta variant (B.1.617).
At first glance, this might seem like a noble move on the Biden administration’s part. The U.S. is seeing low case numbers and widespread reopenings, so we can share some supplies to “help the pandemic around the globe,” as COVID-19 response coordinator Jeff Zients said at a briefing on Thursday.
But 25 million doses—or even the 80 million doses that the administration has promised by the end of this month—is a drop in the bucket compared to actual international needs. For example: COVAX needs 1.8 billiondoses to vaccinate about half the adult population in low-income countries. COVAX has specifically prioritized 92 low-income nations, representing a total population of 3.8 billion.
That 1.8 billion dose number is a highlight of a major report released last week by the Rockefeller Foundation, a global charitable foundation, discussing what it would take to vaccinate the world. I covered the report for Science News. According to this report, Gavi (the Vaccine Alliance), an international public-private body that runs COVAX, needs to raise $9.3 billion in order to pay for those 1.8 billion doses. Gavi has been working to raise this money from countries and independent donors at a global health summit this past week.
While $9.3 billion might seem like a massive price tag, the cost of failing to provide these vaccines would actually be far greater. The global economy may lose up to $9.2 trillion if richer nations fail to support equitable vaccine distribution, according to an estimate from the International Chamber of Commerce.
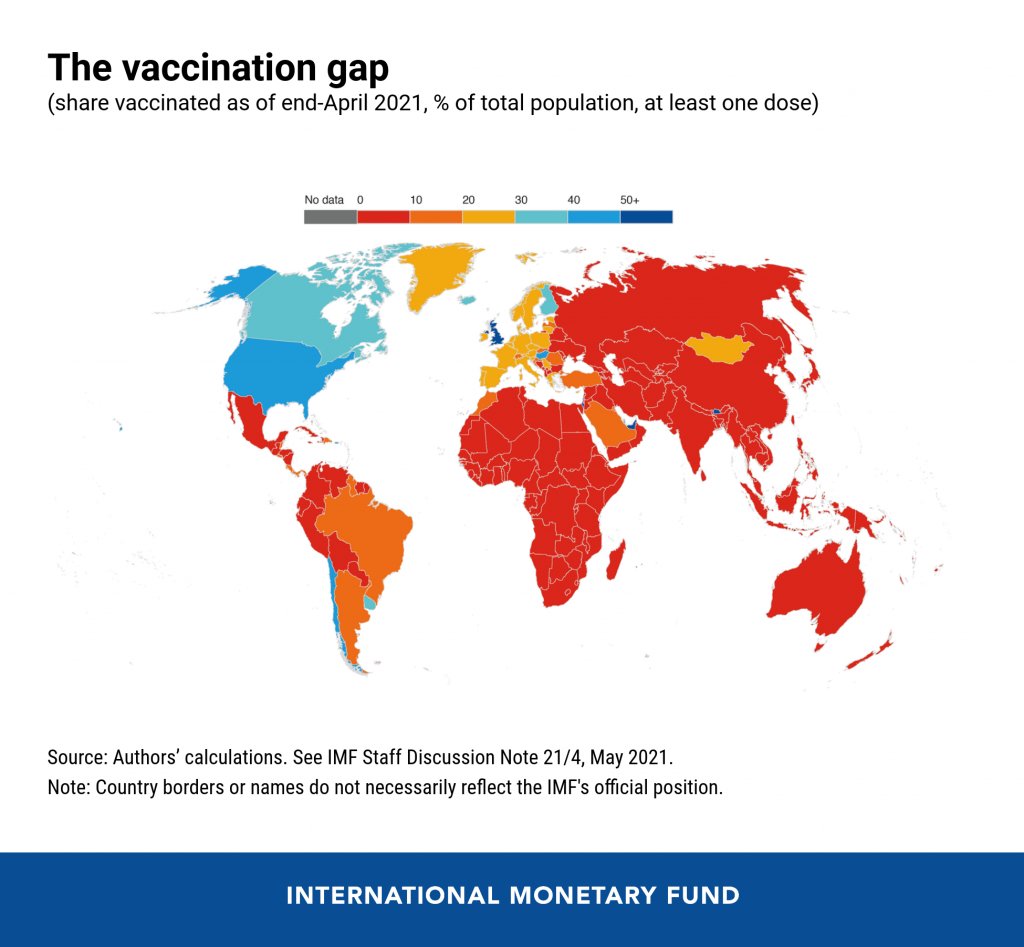
So far, the U.S. has administered about 300 million vaccine doses (as of yesterday), covering over half the total population. In a number of low-income countries, less than one percent of the population has received a dose. Tedros Adhanom Ghebreyesus, Director General of the WHO, said at a recent assembly that, if all doses administered globally had been sent out equitably, the doses would have covered “all health workers and older people.” Instead, high-income nations are largely protected while low-income nations are vulnerable to future surges and highly-transmissible variants.
Through this lens, the 25 million dose shipment announced this week is far from impressive. It’s a useful start, certainly, but it’s not going to end the pandemic anywhere. Even the 80 million doses promised by the end of June is a tiny number—about 4% of the doses COVAX is hoping to obtain. It’s also only 11% of the doses that vaccine makers have pledged to deliver to the U.S. by the end of July, according to Bloomberg.
That larger June shipment has also been held up because the Biden administration is planning to send AstraZeneca vaccines—which are under review from the FDA because they were produced at the Emergent factory that infamously wasted millions of Johnson & Johnson doses. The AstraZeneca vaccine is not authorized for use in the U.S., so of course it will make up the majority of the doses we send abroad this summer.
Speaking of unused doses: the Biden administration may also start sending unused doses from states to other countries, POLITICO reported this week. The administration wants to get thousands of Pfizer, Moderna, and J&J doses—on the verge of expiring—to countries that would actually use them. While this possible policy hasn’t yet been realized, it hammers home a clear message: the U.S. will donate “unwanted” vaccine doses only when we are absolutely certain that we don’t need them here.
Now, let’s return to our reader’s question. What happens when the U.S. is safely vaccinated, but other parts of the world aren’t?
From a health standpoint, the U.S. will probably be okay. The vaccines are very effective, even against variants—likely protecting the country from another major surge. We will need careful surveillance to guard against future variants that may evolve beyond the vaccines (see: last week’s issue), and it’s possible that overly zealous reopening this summer will lead to outbreaks next fall and winter. But seniors and other vulnerable people would be more protected than they have been in past surges, and booster shots (for the variants) will likely be on their way soon. In short, America’s wealth will protect us.
Around the world, however, outbreaks will continue. Every time a new person gets infected with the coronavirus, the virus has a new opportunity to mutate. And with every mutation, the virus learns to spread faster, to evade common treatments, even to evade vaccines. Thanks to globalization, as long as the virus is a threat anywhere, it continues to be a threat everywhere.
Plus, as low-income nations suffer from continued outbreaks, the global economy will continue to suffer. Out of that $9.2 trillion cost estimated by the International Chamber of Commerce, the majority will likely fall on wealthier nations (like the U.S.) that rely on other countries for products and labor.
“The pandemic itself has gone beyond a health crisis — it has now gone into an economic crisis,” Christy Feig, the Rockefeller Foundation’s director of communications and advocacy, told me when I spoke to her for Science News. “The only way to unchoke the economy is by getting the vaccines to as many countries as possible, so that we can stop the spread of the disease before more variants come.”
For months, I’ve been calling on the CDC to release state-by-state demographic data on who is getting vaccinated. While the vast majority of states report this information themselves, the state data are completely unstandardized—making it difficult to perform comprehensive analyses or compare one state to another.
“The vaccine data that individual states are publishing replicate the patchwork nature of the other state-level COVID-19 data our teams have been compiling,” COVID Tracking Project leaders Alice Goldfarb and Erin Kissane wrote in The Atlantic in January.
While many more states are reporting vaccination demographics now than in January—Montana and Wyoming are the only two states that now fail to report vaccinations by race—the data continue to be patchwork and hard to analyze.
Bloomberg has devoted a small team to analyzing and presenting these data in the publication’s U.S. Vaccine Demographics Tracker. But Bloomberg isn’t making their underlying data public, so other journalists and researchers are unable to build on this work. And really, it shouldn’t be on journalists to standardize from a fragmented state-by-state landscape—it should be the work of the CDC.
That’s why I was thrilled when, this week, we finally got that data from the CDC. Well… sort-of.
The data indicate that, despite promises from the White House to prioritize vulnerable communities in the vaccination campaign, a lot of inequities persist: “KHN’s analysis shows that only 22% of Black Americans have gotten a shot, and Black rates still trail those of whites in almost every state.”
!function(){“use strict”;window.addEventListener(“message”,(function(a){if(void 0!==a.data[“datawrapper-height”])for(var e in a.data[“datawrapper-height”]){var t=document.getElementById(“datawrapper-chart-“+e)||document.querySelector(“iframe[src*=’”+e+”‘]”);t&&(t.style.height=a.data[“datawrapper-height”][e]+”px”)}}))}();
In some states, white residents have been vaccinated at almost twice the rate of Black residents. In Iowa, for example, 15% of the Black population has received at least one dose—compared with 37% of the white population. Other states with high disparities include Florida, New Hampshire, Maine, Wisconsin, New Jersey, New York, Hawaii, and Connecticut.
Hispanic/Latino vaccination rates also lag behind the rates for white residents in some states, but the disparities are not as drastic as those for the Black population. Nationwide, 22% of Black Americans have received at least one dose, compared to 33% of white Americans.
Both Native Americans and Asian Americans have higher vaccination rates than the white population. Many tribes, in particular, have made dedicated efforts to promote vaccination.
And another hopeful caveat: vaccination rates for minorities have improved in recent weeks as the rate for white Americans goes down. In the last two weeks, about half of first doses administered in the U.S. have gone to people of color. This includes about 24% of doses going to Hispanic/Latino Americans, 10% going to Black Americans, and 8% going to Asian Americans.
The day after KHN’s analysis was published, Victoria Knight (another KHN reporter) asked CDC Director Dr. Rochelle Walensky whether the agency would add state-level race and ethnicity vaccination data to its dashboard.
“We have been updating our website,” Dr. Walensky said in response. “I can’t say that it’s daily; I believe that it’s weekly.”
And yet as of Sunday morning, May 23, state-by-state demographic data are nowhere to be found on the CDC’s site.
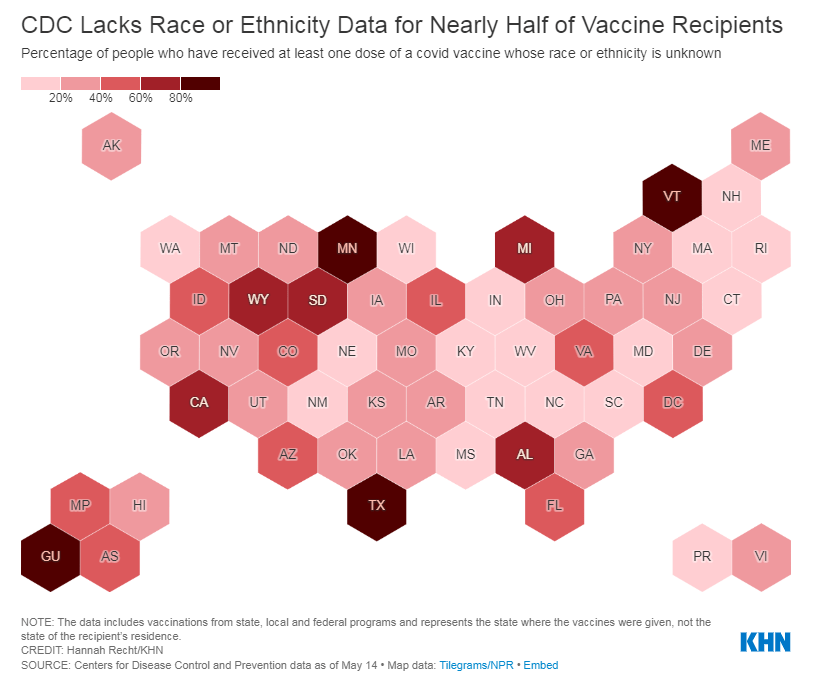
Knight also asked what the CDC is doing to address the high number of vaccinations for which demographic details are unknown. Race/ethnicity data are missing for about 44% of vaccinated Americans, meaning that true disparities may be even starker.
!function(){“use strict”;window.addEventListener(“message”,(function(a){if(void 0!==a.data[“datawrapper-height”])for(var e in a.data[“datawrapper-height”]){var t=document.getElementById(“datawrapper-chart-“+e)||document.querySelector(“iframe[src*=’”+e+”‘]”);t&&(t.style.height=a.data[“datawrapper-height”][e]+”px”)}}))}();
In some states, that unknown percentage is much higher than 44%. Eight states “either refuse to provide race and ethnicity details to the CDC or are missing that information for more than 60% of people vaccinated,” according to KHN. These states are excluded from KHN’s analysis as a result: they are Alabama, California, Michigan, Minnesota, South Dakota, Texas, Vermont and Wyoming.
Dr. Walensky told reporters the CDC is working with state and local public health departments to improve demographic reporting, but didn’t provide specifics.
In order to continue improving vaccination rates for minority communities, the CDC needs to actually make all of the agency’s data public. If state-by-state demographic data were easily available, researchers and reporters like me could more easily identify both the success stories and the disappointments—and help the states that are lagging catch up.
As Hannah Recht put it on Twitter: “we should not have to keep FOIAing for CDC state-level data that they could just put online if they wanted to.”
Following the end of the federal public health emergency in May, the CDC has lost its authority to collect vaccination data from all state and local health agencies that keep immunization records. As a result, the CDC is no longer providing comprehensive vaccination numbers on its COVID-19 dashboards. But we still have some information about this year’s vaccination campaign, thanks to continued CDC efforts as well as reporting by other health agencies and research organizations.
This week, the FDA authorized Novavax’s updated COVID-19 vaccine. Here’s why some people are excited to get Novavax’s vaccine this fall, as opposed to Pfizer’s or Moderna’s.
Last week, I asked you, COVID-19 Data Dispatch readers, to send me your stories of challenges you experienced when trying to get this fall’s COVID-19 vaccines. I received 35 responses from readers across the country, demonstrating issues with insurance coverage, pharmacy logistics, and more.
Most states report some variation on the same COVID-19 vaccination metrics: doses allocated, doses administered, state residents who’ve been partially and fully vaccinated, and so on. But some states go beyond those basics.
This week, I’m showing some appreciation for:
Washington D.C.: Reports numbers of District residents who have stuck to their second dose appointments. The dashboard’s “Adherence” tab includes those who are fully vaccinated, waiting on their second dose appointment, or more than a week overdue for that second dose appointment—both District-wide and by ward.
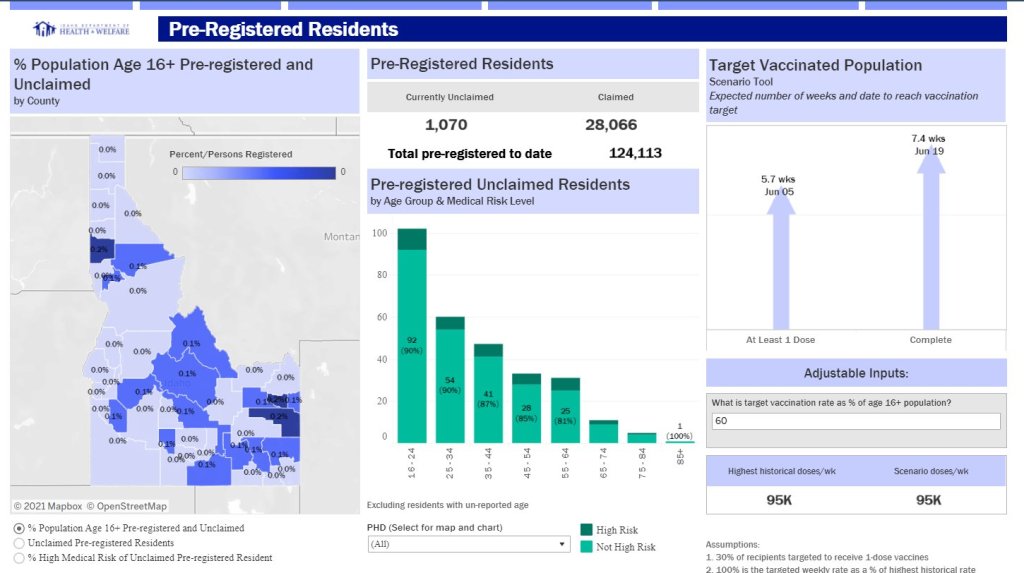
Idaho: Reports detailed data on state residents who have pre-registered for appointments. On the “Pre-registered residents” tab, you can see how many people have claimed their pre-registered appointments, as well as breakdowns of the pre-registered residents by county, age, and medical risk level.
Illinois: Reports both a count of unusable vaccine doses and information on vaccine breakthrough cases. The “unusable” vaccine doses count includes doses that have been discarded, dropped, or had some other issue in the storage and handling process. For vaccine breakthroughs, Illinois reports total patients hospitalized and died due to COVID-19 after vaccination.
New Hampshire: Reports counts of vaccine doses distributed and administered by individual vaccination sites, such as hospitals and public health networks. (New Hampshire includes vaccination data once a week in its COVID-19 news reports, usually on Thursdays. The state figures differ significantly from CDC-reported numbers, for as-yet-undetermined reasons.)
AstraZeneca still isn’t out of the woods yet. In fact, the woods seem to be just getting deeper, and now I’m fairly certain it’s not me jinxing things.
Last time we covered AstraZeneca’s blood clot woes, the European Medicines Agency (EMA) had said in a March 18 press conference that “[t]he committee… concluded that the vaccine is not associated with an increase in the overall risk of thromboembolic events or blood clots.” (Thrombosis just means blood clotting.)
But this week, authorities had enough data to posit a possible connection between blood clots known as cerebral venous sinus thrombosis (CVST) and the Oxford-AstraZeneca vaccine. The EMA has now advised, as of April 7, that “that unusual blood clots with low blood platelets should be listed as very rare side effects of Vaxzevria (formerly COVID-19 Vaccine AstraZeneca).” They are still recommending its use given the gravity of the COVID-19 pandemic, but it’s another blow to the vaccine that held much of the world’s hopes in inoculating the entire population. A mechanism by which the vaccine is causing these thromboses has not been discovered.
As of April 4, there had been 222 cases of abnormal thromboses in Britain and the European Economic Area after receiving the Oxford-AstraZeneca vaccine, according to the New York Times. This is out of about 34 million people being vaccinated, and they estimated that the frequency was about 1 in 100,000. In total, the EMA committee looked at “62 cases of cerebral venous sinus thrombosis and 24 cases of splanchnic vein thrombosis reported in the EU drug safety database (EudraVigilance) as of 22 March 2021, 18 of which were fatal.”
This made us wonder how this compares to the early reports of anaphylaxis (serious allergic reactions) in recipients of the Pfizer-BioNTech and Moderna mRNA vaccines. According to an early report from the CDC, there were 21 cases out of 1,893,360 Pfizer-BioNTech first doses, for a frequency of 11.1 cases per million, or about 1 in 90,000. A later JAMA paper reported updated rates of about 4.7 cases per million doses for Pfizer-BioNTech and 2.5 cases per million for Moderna. To make the scales easier to compare, this works out to about 1 in 213,000 and 1 in 400,000, respectively.
Comparing 1 in 213,000 and 1 in 400,000 cases of anaphylaxis to 1 in 100,000 cases of serious blood clots, it makes sense why some authorities are starting to hit the brakes on the AstraZeneca vaccine. No deaths were reported with the anaphylaxis reactions, but out of the sample of thromboses that the EMA examined, 18 people died. Not only are the numbers worse, but anaphylaxis reactions can also be easier to prepare for. In that early CDC report, 71% of anaphylaxis reactions occurred within 15 minutes of vaccination. For this reason, vaccine clinics monitor you for about 15 minutes (mine sure did). That’s harder to do with blood clots, which take much longer than 15 minutes to manifest and can’t be treated with an EpiPen on the spot.
Again, this is definitely a blow for what’s still a very effective vaccine. But taking these precautions is how faith in vaccines is earned and kept. We hold vaccines to a high standard for a reason.
Following the end of the federal public health emergency in May, the CDC has lost its authority to collect vaccination data from all state and local health agencies that keep immunization records. As a result, the CDC is no longer providing comprehensive vaccination numbers on its COVID-19 dashboards. But we still have some information about this year’s vaccination campaign, thanks to continued CDC efforts as well as reporting by other health agencies and research organizations.
This week, the FDA authorized Novavax’s updated COVID-19 vaccine. Here’s why some people are excited to get Novavax’s vaccine this fall, as opposed to Pfizer’s or Moderna’s.
Vaccination data update: Two more states are now reporting vaccinations by race/ethnicity. New Hampshire has reported the figures in one of the state’s recent daily updates, which include vaccination data on a weekly basis. And South Dakota has added race/ethnicity to the vaccines tab of its dashboard. As always, you can find detailed annotations on state and national vaccine data sources (updated yesterday) on the COVID Data Dispatch website.
KFF COVID-19 Vaccine Monitor: The Kaiser Family Foundation released the latest update for their Vaccine Monitor, an ongoing survey project to track public attitudes and experiences with COVID-19 vaccines. In this update, published this past Tuesday, KFF reports that 62% of those surveyed say they’ve already gotten a shot or plan to do so as soon as possible, while 17% want to “wait and see” how the rollout goes. That “wait and see” share is down from previous reports.
CDC Provisional Mortality Data for 2020: This past Wednesday, the CDC released death counts for 2020. As we’ve discussed before, mortality data tend to be reported with a lag compared to other types of public health numbers due to the complex processes involved with tallying up death certificates. About 3.3 million deaths occurred overall in 2020, according to these new data; this was a 16% increase from 2019. COVID was the third leading cause of death that year, accounting for 345,000 lives lost.
Federal COVID-19 Chart Gallery: Peter Walker, former data visualization co-lead for the COVID Tracking Project, has put together a new Tableau gallery using data from the CDC COVID Tracker and HHS Protect. The gallery includes many chart formats that CTP fans may recognize, such as national views, four-pane views, and regional comparisons. More charts are coming!
Pfizer COVID-19 Clinical Trials: An interactive, searchable map from Pfizer lets you look up vaccine trials around the world. For each trial, you can see the location, the trial’s phase, who’s eligible to join, and a link out to more information on ClinicalTrials.gov. Trials are happening in the U.S., the U.K., Spain, and Japan.
mRNA sequence for the Moderna vaccine: A group of scientists at Stanford used small amounts of Moderna vaccine left after all doses were extracted from vials to sequence the mRNA in that vaccine, then posted the sequence publicly on GitHub. The full sequence takes up two pages. You can read more about the scientists’ work and their decision to post the sequence in Motherboard.
Pulse of the Purchaser 2021 Report: This new report from the National Alliance of Healthcare Purchaser Coalitions examines how employer attitudes to healthcare have shifted during the COVID-19 pandemic. The report presents results from a survey of 151 major employers, representing diverse industries and sizes; it includes attitudes towards COVID-19 vaccines, telehealth, equity, and other healthcare topics.
The problem child of COVID-19 vaccines was back in the news this week. After South Africa suspended the Oxford-AstraZeneca vaccine’s use when it failed to slow the spread of the predominant B.1.351 variant, vaccination using this vaccine has been suspended and then resumed in many European countries following reports of blood clots in some people who received it.
According to a release from AstraZeneca, there have been 15 cases of deep vein thrombosis and 22 cases of pulmonary embolism in people who have gotten the vaccine, as of March 8. These are serious complications—seven of those people died. Countries that suspended the vaccine’s use include Spain, Italy, France, and Germany, among others. (Europe tends to act as more of a bloc than North America when it comes to vaccines. Consider: Canada has authorized use of the AstraZeneca vaccine while the US has literal fridges full of the stuff just sitting there waiting for approval.)
Since the initial suspension, investigations have been launched and apparently concluded that there is no causative relationship between the vaccine and these symptoms. According to Emer Cooke, the executive director of the European Medicines Agency (EMA), in a press conference on March 18: “The committee… concluded that the vaccine is not associated with an increase in the overall risk of thromboembolic events or blood clots.”
And, according to the WHO on March 17: “At this time, WHO considers that the benefits of the AstraZeneca vaccine outweigh its risks and recommends that vaccinations continue.” Europe has since started to resume vaccinating with the Oxford-AstraZeneca vaccine, starting with France, Germany, and Italy. (Except not in Finland, where they just suspended it again after two people got similar blood clots.)
So all’s well that ends well right? Well, not necessarily. Besides that Finland wrinkle, some scientists and officials are concerned that this entire rigmarole could undermine public trust in the AstraZeneca vaccine. It’s worth noting that a tiny population experienced these effects out of the millions of people who have already gotten the vaccine. And blood clots are fairly common in the population; you’re going to expect some people to develop them just by sheer chance. But it’s also worth noting that these complications are serious, and rare among the age group that they were reported in. Not slowing down could have the same fear-inducing effect. As Shobita Parthasarathy says in her Slate column, “[T]his crisis isn’t about science at all. It’s about public trust, and scared citizens cannot be easily convinced by expertise that feels remote. Our solutions need to reflect that.”
We’ll see if anything else happens. But in the meantime, the US has since promised to share its stockpile of the Oxford-AstraZeneca vaccine with Canada and Mexico, so it looks like it’s at least medium-steam ahead for now.
Following the end of the federal public health emergency in May, the CDC has lost its authority to collect vaccination data from all state and local health agencies that keep immunization records. As a result, the CDC is no longer providing comprehensive vaccination numbers on its COVID-19 dashboards. But we still have some information about this year’s vaccination campaign, thanks to continued CDC efforts as well as reporting by other health agencies and research organizations.
This week, the FDA authorized Novavax’s updated COVID-19 vaccine. Here’s why some people are excited to get Novavax’s vaccine this fall, as opposed to Pfizer’s or Moderna’s.