Over the past year, vaccine incentives have become a popular strategy among businesses and state and local governments. From free donuts to free Mets tickets, Americans have had opportunities to get bonus rewards along with protection from the coronavirus. And one particularly common incentive is cash, offered through small payments accompanying vaccinations and lotteries that only vaccinated people can enter.
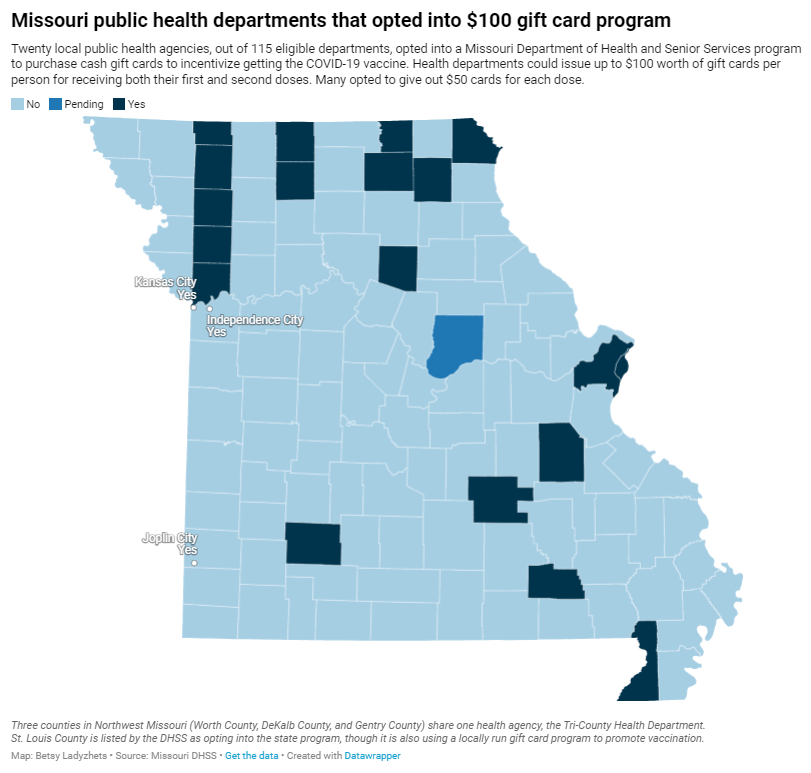
While politicians at all levels have praised cash incentives, research has shown that this strategy has little impact on actually convincing Americans to get vaccinated. A recent investigation I worked on (at the Documenting COVID-19 project and the Missouri Independent) provides new evidence for this trend: the state of Missouri allocated $11 million for gift cards that residents could get upon receiving their first or second vaccine dose, but the vast majority of local health departments opted not to participate in the program—and a very small number of gift cards have been distributed thus far.
The Missouri program’s limited success fits into a national pattern. “It’s hard to tease out a causal effect of a program that’s not introduced with the purpose of a research experiment,” Dr. Allan Walkey, an epidemiologist at Boston University who’s studied vaccine incentives, told me. Still, Walkey said, the majority of research on these programs has found that cash incentives are not driving huge numbers of people to get their shots.
Walkey specifically studied a vaccine lottery in Ohio, the first state to set up such a program. While initial reports by state leaders suggested that a lot of people got vaccinated after the lottery was announced, Walkey found that, in fact, the new vaccinations were more likely caused by an expansion of vaccine eligibility. Two days before the lottery was announced, the Pfizer vaccine was authorized for children between the ages of 12 and 15.
For this story, I also spoke to Ashley Kirzinger, a polling expert at the Kaiser Family Foundation (KFF) who helps run KFF’s Vaccine Monitor surveys. In these surveys, KFF sorts unvaccinated Americans into categories based on their vaccine attitudes: “wait and see,” “only if required,” and “definitely not.” Kirzinger told me that cash incentives, vaccine requirements for events, and other social pressures are more likely to “motivate the ‘wait and see’ or ‘only if required’” groups.
But for those Americans who “definitely” don’t want to get vaccinated, these incentives aren’t likely to move the needle. In fact, the people in this group may be angered by incentives, because they could see such programs as unfair pressure from the health system.
This was true in some Missouri local public health departments. For example, in Carter County—where the local agency did opt in to the state gift card program—a planned vaccination drive with the gift cards was canceled due to local opposition.
“So many parents and community members were upset, we were not allowed to hold the vaccination event at the school,” said Michelle Walker, the county health center administrator.
Overall, out of 115 local public health agencies in Missouri that were eligible to participate in the incentive program, just 20 opted to get gift cards. Most departments purchased $50 gift cards, so that residents could get $50 at their first vaccine dose and $50 at their second dose.
Through surveying the local agencies that participated, my colleague Tessa Weinberg and I obtained data from 10. Out of 6,378 gift cards that the agencies were able to purchase with state funding, we found that just 1,712 had been distributed so far, as of late November.
!function(){“use strict”;window.addEventListener(“message”,(function(e){if(void 0!==e.data[“datawrapper-height”]){var t=document.querySelectorAll(“iframe”);for(var a in e.data[“datawrapper-height”])for(var r=0;r<t.length;r++){if(t[r].contentWindow===e.source)t[r].style.height=e.data["datawrapper-height"][a]+"px"}}}))}();
Read the full story for more on why many departments didn’t participate in this gift card program, and how it’s going for the departments that did opt in.
This past Monday, President Biden gave a speech about the Omicron variant. He told America that Omicron is “cause for concern, not a cause for panic,” and thanked the South African scientists who alerted the world to this variant. (Though a travel ban is not a great way to thank those scientists!)
Towards the end of the speech, he said: “We’re throwing everything we can at this virus, tracking it from every angle.” Which I, personally, found laughable. As I’ve pointed out in a previous post about booster shots, the U.S.’s anti-COVID strategy basically revolves around vaccines, and has for most of 2021.
wild to hear Biden say "we are throwing everything we can at this virus" … like, sir, no we aren't. we are throwing ONE THING (vaccines) at this virus.
My Tweet about Biden’s vaccine-only strategy got more attention than I’m used to receiving on the platform, so I thought it was a worthwhile topic to expand upon in the COVID-19 Data Dispatch. Why aren’t vaccines enough to address Omicron—or our current surge, for that matter—and what else could the Biden administration be doing to slow the coronavirus’ spread?
Why aren’t vaccines enough?
Prior to Delta’s spread, there was some talk of reaching herd immunity: perhaps if 70% or 80% of Americans got fully vaccinated, it would be sufficient to tamp down on the coronavirus. But Delta’s increased capacity to spread quickly, combined with the vaccines’ decreased capacity to protect against infection and transmission, have shown that vaccines are not enough to eradicate the virus.
Here, then, is the current pandemic dilemma: Vaccines remain the best way for individuals to protect themselves, but societies cannot treat vaccines as their only defense. And for now, unvaccinated pockets are still large enough to sustain Delta surges, which can overwhelm hospitals, shut down schools, and create more chances for even worse variants to emerge. To prevent those outcomes, “we need to take advantage of every single tool we have at our disposal,” [Shweta Bansal of Georgetown University] said. These should include better ventilation to reduce the spread of the virus, rapid tests to catch early infections, and forms of social support such as paid sick leave, eviction moratoriums, and free isolation sites that allow infected people to stay away from others.
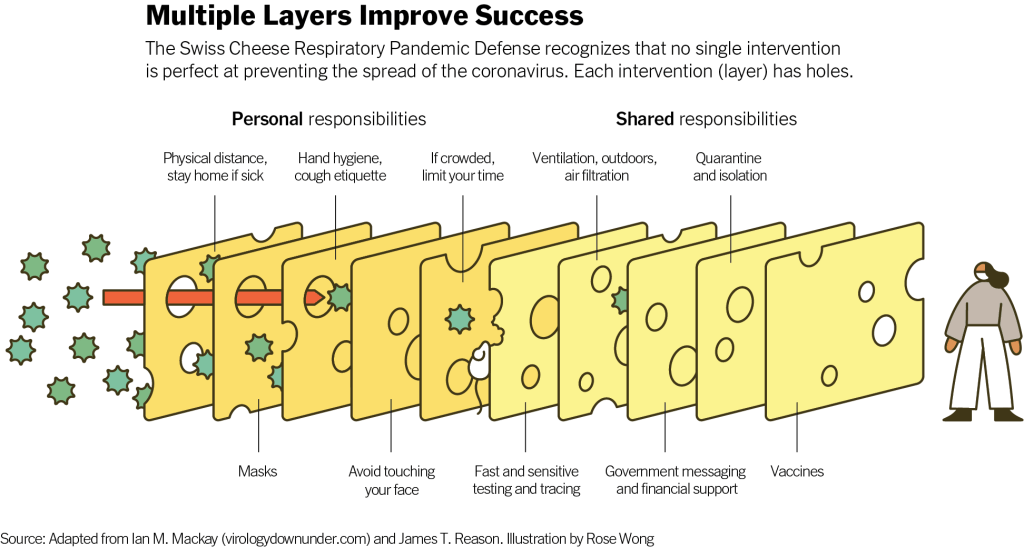
Remember that Swiss cheese model of pandemic interventions? Vaccines may be the best protection we have against the coronavirus, but they’re still just one layer of protection. All the other layers—masks, testing, ventilation, etc.—are still necessary, too. Especially when we’re dealing with a new variant that might not respond as well to our vaccines.
Re-upping this brilliant image from last year as a reminder on how mitigation measures work together to prevent the spread of coronavirus. pic.twitter.com/p7Z8u7fS2w
One strategy that we could employ against Omicron, as well as against the current Delta surge, is better masks. While cloth masks certainly make it less likely for the coronavirus to spread from one person to another, their efficacy varies greatly depending on the type of material, the number of layers, and the mask’s fit.
N95 masks do the best job at stopping the coronavirus from spreading, followed by KN95 masks. Surgical masks do a better job than cloth masks, but making sure these masks fit properly can be a challenge for some people (including yours truly, who has a very narrow face!). Layering a surgical mask and cloth mask may be a safer option to get both good fit and protection, though two layers of mask can be challenging to wear for long periods of time.
Some experts have recommended that the U.S. mail N95 or KN95 masks to all Americans, or at least require these masks in high-risk areas, such as on flights. Germany and other European countries established similar requirements last summer.
Given how transmissible Delta is—and the likelihood that Omicron is also highly transmissible—consider upgrading to an N95/KN95 mask or equivalent when indoors and around others, especially if you're elderly or immunocompromised.
In many countries—including the U.K., Germany, India, and others—rapid tests are freely available. Here in the U.S., on the other hand, the tests are quite expensive (often upwards of $10 for one test) and difficult to find, with pharmacies often limiting the number of packages that people can buy at once.
Biden has attempted to increase rapid testing access as part of his latest COVID-19 plan: in January, private insurance companies will be required to cover the cost of rapid tests. But this doesn’t solve the supply issue, and it doesn’t really make the tests more accessible, either. The measure would still require people to buy tests out of pocket, then fill out insurance reimbursement forms to maybe get their money back. Can you imagine anyone actually doing this?
In addition, as some experts have pointed out, the people most likely to need rapid tests—essential workers and others in high-risk environments—are also those less likely to have insurance. Biden is also distributing some rapid tests to community health centers, but that’s not enough to meet the need here.
This part of Biden’s omicron plan is also short-sighted.
Sure reimbursement by private health insurance of rapid test costs is a nice thing to have, but the people who MOST need rapid tests are the same people who DONT have private health care. What’s the plan for helping them? pic.twitter.com/tnlC8T0PDk
Ideally, the Biden administration would mail every American a pack of, like, 20 rapid tests, along with that pack of N95 or KN95 masks I mentioned above. Free of charge.
And at the same time, of course, we need more readily available PCR testing. Even in New York City, which has a better testing infrastructure than most other parts of the country, the lines at free testing sites are getting long again as cases go up. Any American who wants to get tested should be able to easily make an appointment within a day or two, and get their results within another day after that.
Increased testing is not only important for identifying Omicron cases (and cases of any other new variant); it’s also key for the Merck and Pfizer antiviral treatments due to be approved in the U.S. soon. Without efficient testing, patients won’t be able to start these treatments within days of their symptoms starting.
What we could do: improve genetic surveillance
The U.S. is doing a lot more coronavirus sequencing than we were in early 2021: we’ve gone from under 5,000 cases sequenced a week to over 80,000. The CDC worked with state and local health agencies, as well as research organizations and private companies, to increase sequencing capacity across the country.
Urban centers close to large academic centers tend to be well covered, while rural areas are less so. That means public health departments in large parts of the country are still flying blind, even as they are figuring out ways to prioritize Omicron-suspicious samples.
A lack of testing compounds this problem. If someone doesn’t confirm their COVID-19 case with a PCR test, their genetic information will never make it to a testing lab, much less a sequencing lab. While rapid tests are very useful for quickly finding out if you’re infected with the coronavirus, you need a PCR test for your information to actually be entered into the public health system.
In addition, even where the U.S. is sequencing a lot of samples, the process can take weeks. Vox’s Umair Irfan writes:
Still, it takes the US a median time of 28 days to sequence these genomes and upload the results to international databases. Contrast that with the United Kingdom, which sequences 112 genomes per 1,000 cases, taking a median of 10 days to deposit their results. A delay of only a few days in detection can give variants time to silently spread within communities and across borders.
Despite sequencing shortfalls in the U.S., we’re still doing much more surveillance than the majority of countries. Many nations in Africa, Asia, South America, and other parts of the world are sequencing fewer than 10 cases per 1,000, Irfan reports. As the U.S. should be doing more to get the world vaccinated, the U.S. should also do more to help other countries increase their sequencing capacity—monitoring for the variants that will inevitably follow Omicron.
What we could do: stricter domestic travel requirements
Starting on Monday, all international travelers coming into the U.S. by air will need to show a negative COVID-19 test, taken no more than one day before their flight. This includes all travelers regardless of nationality or vaccination status. At the same time, any non-U.S. citizens traveling into the country must provide proof of their vaccination against COVID-19.
But travelers flying domestically don’t face any such requirements. There are mask mandates on airplanes, true, but people can wear cloth masks, often pulled down below their noses, and airports tend to have limited enforcement of any mask rules.
Both experts and polls have supported requiring vaccination for domestic air travel, though the Biden administration seems very hesitant to put this requirement in place. Speaking for myself, I felt very unsafe the last time I flew domestically. A vaccine mandate for air travel would make me much more likely to fly again.
What we could do: more social support
In the U.S., a positive COVID-19 test usually means that you’re in isolation for 10 to 14 days, along with everyone else in your household. This can pull kids out of school, and pull income from families. As has been the case throughout the pandemic, support is needed for people who test positive, whether that’s a safe place to isolate for two weeks, grocery delivery, or rapid tests for the rest of the household.
This type of support could make people actually want to get tested when they have symptoms or an exposure risk, rather than avoiding the public health system entirely.
State vaccination data: This weekend, I updated my annotations on state and national vaccination data sources in the U.S. A few more states are now reporting information on booster shots, and several states have adjusted their vaccine coverage metrics to reflect vaccine eligibility for children in the 5 to 11 age group. Notably, since my last update, Alaska, D.C., Utah, and Vermont’s health agencies have all started reporting some demographic information regarding booster shot recipients in their states.
Moral injury among healthcare workers during COVID-19: There have been a lot of headlines recently about burnout among healthcare workers. This study, based on a survey of 1,300 healthcare workers and published this week in JAMA Network Open, provides some statistics to underlie the trend. See the supplemental materials for sample quotations from the survey respondents, demonstrating their feelings of fatigue, isolation, and betrayal.
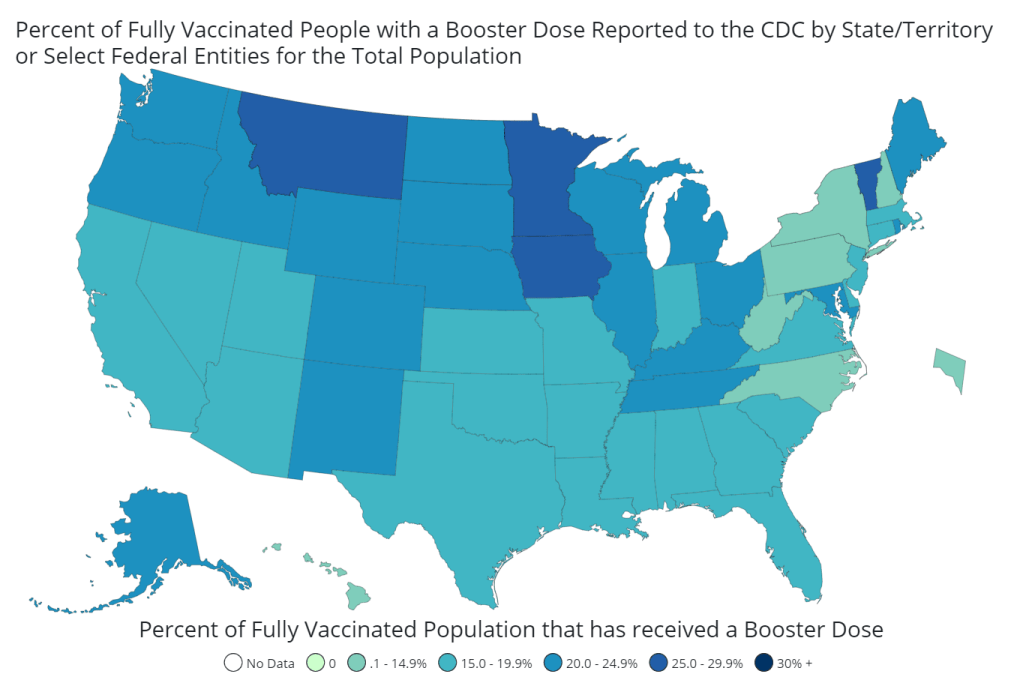
As of November 20, almost 35 million Americans have received a booster shot. That number is likely to shoot up in the coming weeks with expanded eligibility. Chart via the CDC.
On Friday morning, the FDA authorized booster shots of Pfizer’s and Moderna’s COVID-19 vaccines for all adults in the U.S., six months after their first two doses. The CDC’s vaccine advisory committee voted to support this expanded booster eligibility that afternoon, and CDC leadership signed off on it a few hours later.
Although the Biden administration has supported boosters for all adults since August, this specific federal eligibility expansion was preceded by several state and local leaders. Prior to Friday, the governors of Colorado, New Mexico, California, and other states said that any adult living in their jurisdictions could go get a booster, even if they didn’t fit the current national criteria. New York City leaders made a similar announcement this past Monday.
Perhaps spurred on by these state decisions, the FDA and CDC moved quite quickly to authorize booster shots for a larger group of Americans. The FDA was originally just considering the move for Pfizer’s vaccine, then added Moderna to the mix just this week (when Moderna sent in a formal application).
And the CDC’s vaccine advisory committee meeting had somewhat less time for deliberation than this committee typically tends to take. As Helen Branswell wrote in STAT News:
The meeting was called on such short notice — it was announced Tuesday — that only 13 of the committee’s members were able to attend. When the meeting went longer than scheduled, two members had to leave without voting.
new today at @FiveThirtyEight: me, @maggiekb1, and Chadwick Matlin talking about how the question "who should get booster shots?" became so complicated. this was an interesting conversation, and I'd like to highlight a couple of main points here. (1/8) pic.twitter.com/Jf5WfWodkk
The short answer here is 1) more compelling evidence that boosters provide additional protection against coronavirus infection and 2) cases are rising in the U.S., and boosters might help make the surge less severe. Also, so far, very few cases of severe side effects have been reported following booster shots.
Since the last FDA and CDC booster shot deliberations, more evidence has rolled in showing their efficacy. One notable study, from the Imperial College of London, was published this past Wednesday; the report suggests that people who’ve received two COVID-19 vaccine doses are more than twice as likely to test positive than those who’ve received three doses.
While the study hasn’t yet been peer-reviewed, it’s part of a long-running surveillance project in the U.K. that examines COVID-19 prevalence in the entire population—including all age groups and comparing those who received Pfizer and AstraZeneca vaccines. “What they found is very, very strong data showing that as soon as 7 days after a third COVID-19 vaccine dose, the risk of infection is cut in half when you look at the entire population,” wrote Dr. Jorge Caballero in a Twitter thread summarizing the study.
At the same time, cases are going up in the U.S.—appearing to indicate a new winter surge. It’s no coincidence that Colorado and New Mexico, two of the states that were among the first to expand booster eligibility to all adults, are also among the states with the highest COVID-19 case rates.
When Delta hit Israel this past summer, the country started administering booster shots: first to seniors at the end of July, then for younger and younger age groups until all adults were able to get the shots. Data from the country’s national health agency suggest that these booster shots played a key role in driving down case numbers among both vaccinated and unvaccinated Israelis.
Personally, I am still a bit skeptical that Israel’s drop in cases was thanks to booster shots alone, as the data don’t necessarily show causation. But for a lot of U.S. leaders, the Israeli data provide a compelling model: it seems like booster shots can potentially drive down a case surge. This fits nicely into the national strategy that the Biden administration has already been preaching for months, which I call “vaccinate out of the pandemic.”
Listening to the advisory-committee meetings, I noticed that there seems to be this tension between the scientific experts who want to make robust evidence-based decisions — and the sense that, here in the U.S., our overall pandemic strategy is basically “vaccinate our way out of the pandemic.” If we had better masking, distancing, contact tracing, ventilation, rapid tests and everything else, we would not need boosters to stop people’s mild cases. But we’re not doing a great job at any of those other things, so … we kinda need boosters.
Maggie Koerth also pointed out that booster shots are also politically easier for a lot of leaders than some of the other COVID-19 strategies I mentioned. We already have the shots stockpiled, so it’s just a matter of telling people to go get them—unlike, say, expanding contact tracing, which would take a huge investment in hiring and training people.
In addition, the eligibility expansion solves communication and logistics challenges: now, every adult in the U.S. can just go get a booster shot, once enough time has passed from their first two doses. Almost 90% of vaccinated Americans were eligible already, but a lot of people were confused about whether they fit the criteria; the situation became much simpler after Friday.
Should you get a booster shot?
If you’re over 65 or you have a health condition that makes you particularly vulnerable to severe COVID-19 symptoms, answering this question is easy: YES. Go get a booster shot, as soon as you’re able to do so.
If you live or work in a setting that puts you at risk of contracting the coronavirus—or if you live or work in a setting with other people who are more vulnerable than you—then you also have a pretty solid argument towards getting a booster shot.
Even if you’re very unlikely to have a severe case of COVID-19 thanks to your initial vaccination, a mild case could still disrupt your work, your household, and others in your community. A teacher with breakthrough COVID-19 might cause their classroom to shut down for a week, for example, while a parent with breakthrough COVID-19 may interrupt their kids’ lives if those kids are too young to be vaccinated themselves.
For those who don’t fall into these categories (like me!), the situation is a bit more complicated. But after following all of the news this week, I’ve decided that it does make sense for me to get my booster shot.
Here’s why: much as I wish that national leadership and my own local leaders in NYC were investing in other measures to control COVID-19 cases, I don’t foresee widespread mask mandates, rapid tests, contact tracing, or any other safety overhauls anytime soon. Instead, my public health leaders are asking me (and those around me) to get booster shots in order to potentially lower case rates. So, I’ll do my part to contribute to that “vaccinate out of the pandemic” strategy, though I don’t necessarily agree with it.
It’s also important to note here that vaccinating the people who are still unvaccinated is much more important for lowering overall case counts—and for keeping people out of the hospital—than boosters. That includes kids in the 5 to 11 age group. As Maggie Koerth said in our chat:
If you’re under 65 and you’re not immune compromised, it almost certainly matters more to get your kiddos vaxxed the first time than to get yourself a booster. That’s my parent-centric takeaway from all this reading.
And, of course, to end the pandemic on a global scale, we need to get first and second doses to everyone in the world. Right now, booster shots are hindering global vaccination: according to the WHO, there are about six times more boosters administered daily in wealthy nations right now than there are first and second doses administered in low-income nations.
The U.S. has already chosen to stockpile millions of doses for boosters, so refusing a booster shot on an individual level doesn’t have any impact on the global situation. But there are other options for people who want to take action about vaccine inequality: for example, you can contact your congressional representatives about the issue.
What happens after a lot of Americans get booster shots?
Someone asked me this question on Twitter earlier this week. Do booster shots lead to other loosening COVID-19 restrictions, or something else?
It’s difficult to answer that right now, because the U.S. is still close to the beginning of our booster shot rollout. Within a couple of months—and millions more doses—we’ll have some data on whether booster shots here lead to a drop in cases, like what we saw in Israel. At the same time, many European countries are similarly offering booster shots to wide swaths of their populations; we can also watch what happens in those nations.
The U.S. is still likely to face a case surge this holiday season, I think, simply due to cold weather combined with travel and gatherings. But perhaps booster shots will mean that hospitalizations don’t rise as much as cases do, or that a higher share of the cases are mild. We’ll have to see.
Looking beyond this winter, we could see three shots become standard for COVID-19 vaccines. (Several other vaccines, such as HPV, are three-shot series.) We could also see annual boosters for COVID-19, similar to flu shots. More study of the booster shots’ effectiveness and of long-term COVID-19 immunity in general will help scientists figure this out.
Finally, I couldn’t end this post without pointing out the continued data gaps here. The U.S. is still not tracking breakthrough cases in any kind of comprehensive manner, and a lot of information is missing on who’s getting booster shots—the CDC and most states are not reporting demographic data on booster recipients.
And this is it. This [three small studies] is all the data the CDC presented today. Which is insane— the United States does not have a real-time, comprehensive picture of our vaccines, nor the number of breakthrough cases, nor who’s more likely to have a breakthrough case or not. I cannot emphasize enough of how detrimental this is to our public health response. Bad data produces (potentially) bad policy. We are flying blind.
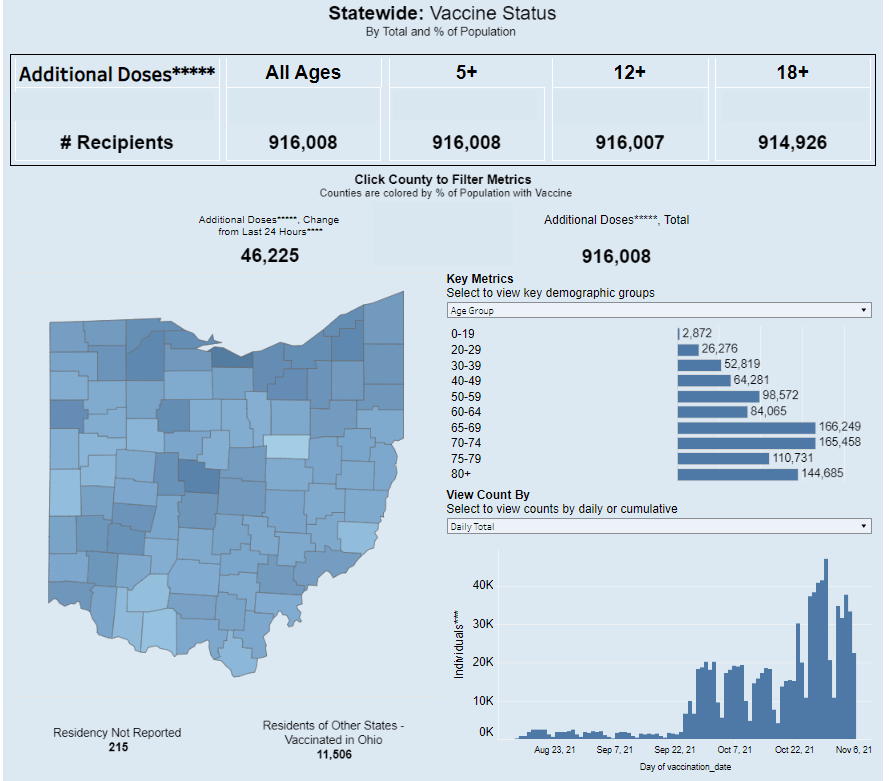
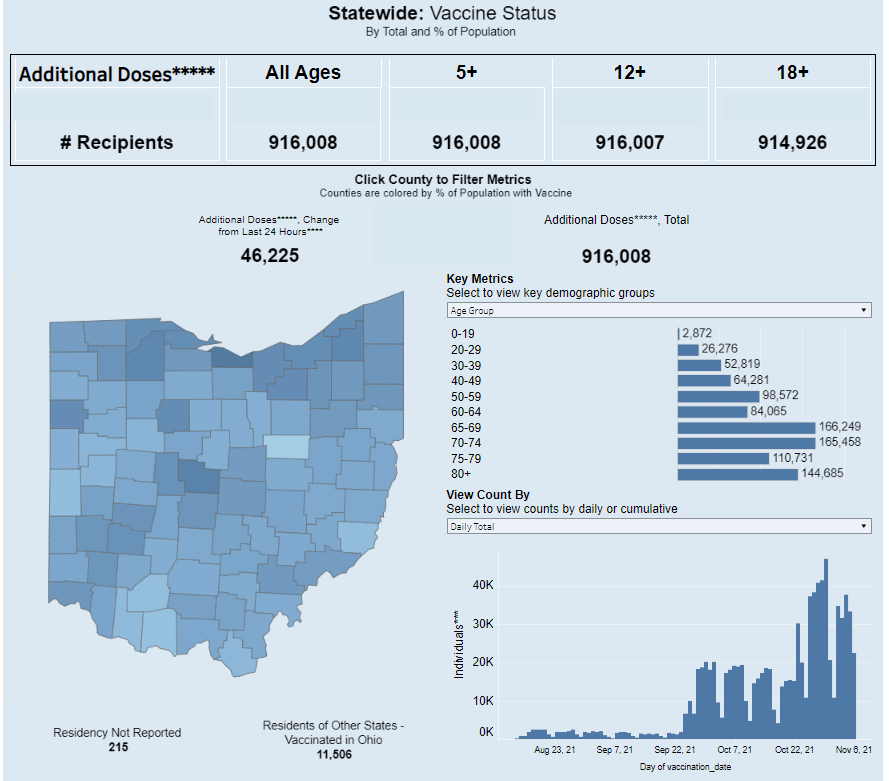
Ohio is one of just eight states reporting demographic data for booster shots administered in the state. Screenshot taken on November 7.
It’s now been over a month since the FDA and the CDC authorized third doses of Pfizer’s COVID-19 vaccine for a large swath of the U.S. population, and a couple of weeks since the agencies did the same thing for additional doses of Moderna and Johnson & Johnson’s vaccines. In that time, over 20 million Americans have received their boosters.
This weekend, I set out to see what data are now available on these booster shots. I updated my vaccination data in the U.S. resource page, which includes detailed annotations on every state’s vaccine reporting along with several national and international sources.
The majority of states (and national dashboards) are now including booster shots in their vaccine reporting, I found. But in most cases, the reporting stops at just one statistic: the total number of residents who have received an additional dose. A few states are reporting time series information—i.e. booster shots administered by day—and a few are reporting demographics—i.e. booster shot recipients by age, gender, race, and ethnicity—but these metrics are lacking across most dashboards.
Demographic information, particularly race and ethnicity, should be a priority for booster shot data, as it should be for numerous other COVID-19 metrics. At the beginning of the U.S.’s vaccine rollout, Black and Hispanic/Latino Americans lagged behind white Americans in getting their shots, but limited data hindered the public health system’s ability to respond to this trend. (Now, the trends have evened out somewhat, though Black vaccination rates still lag white rates in some states.)
Will we see the same pattern with booster shots? Considering the immense confusion that has surrounded America’s booster shot rollout in the last couple of months, it would not be surprising if disadvantaged communities are less likely to know about their potential need for a booster, or where and how to get those shots.
But so far, we don’t have enough data to tell us whether this pattern is playing out. The CDC has yet to report booster shot data by race or ethnicity, though the agency is now reporting some figures by age and by state. Note: the CDC still has yet to report detailed vaccination data by race and ethnicity, period; the agency just reports national figures, nothing by state or other smaller geographies.
At the state level, just eight states are reporting booster shots by race and ethnicity. 13 states are reporting some kind of time series (boosters administered by day or week), and three are reporting doses administered by vaccine manufacturer.
Here are all the states that I found reporting booster shot data, with links to their dashboards:
Wyoming: Total boosters and doses administered by manufacturer.
Local reporters: If your state is reporting demographic data, I recommend taking a look at those numbers. How does the population receiving booster shots compare to the overall population of your state, or to the population that’s received one or two doses? And if your state is not reporting demographic data (or any booster data at all), ask your public health department for these numbers!
This past Thursday, an advisory committee to the CDC recommended that booster doses of the Pfizer vaccine be authorized for seniors and individuals with high-risk health conditions. The committee’s recommendation, notably, did not include individuals who worked in high-risk settings, such as healthcare workers—whom the FDA had included in its own Emergency Use Authorization, following an FDA advisory committee meeting last week.
Then, very early on Friday morning, CDC Director Rochelle Walensky announced that she was overruling the advisory committee—but agreeing with the FDA. Americans who work in high-risk settings can get booster shots. (At least, they can get booster shots if they previously received two doses of Pfizer’s vaccine.)
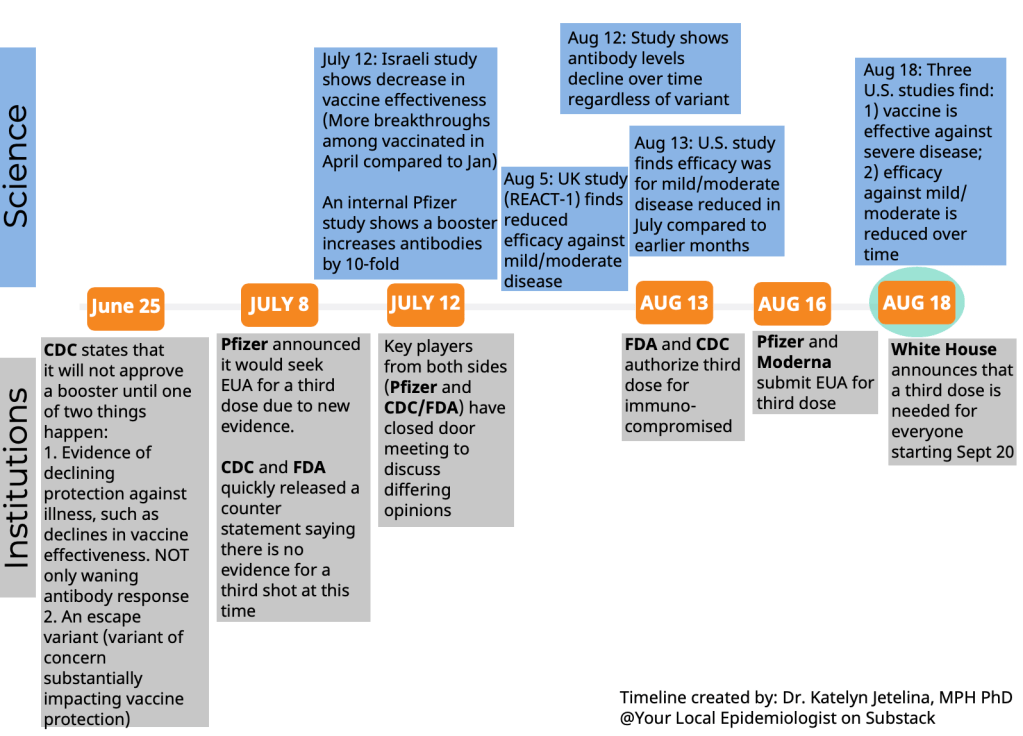
This week’s developments have been just the latest in a rather confusing booster shot timeline:
The US timeline for boosters. You'd have to work really hard to mess this up this badly and engender this much confusion. 😬 pic.twitter.com/KHNWEQJyLg
Why has this process been so confusing? Why don’t the experts agree on whether booster shots are necessary, or on who should get these extra shots? Part of the problem, of course, is that the Biden administration announced booster shots were coming in August, before the scientific agencies had a chance to review all the relevant evidence.
But from my (data journalist’s) perspective, the booster shot confusion largely stems from a lack of data on breakthrough cases.
Let’s go back in time—back four months, or about four years in pandemic time. In May, the CDC announced a major change in its tracking of breakthrough cases. The agency had previously investigated and published data on all breakthrough cases, including those that were mild. But starting in May, the CDC was only investigating and publishing data on those severe breakthrough cases, i.e. those which led to hospitalization or death.
At the time, I called this a lazy choice that would hinder the U.S.’s ability to track how well the vaccines are working. I continued to criticize this move, when researchers and journalists attempted to do the CDC’s job—but were unable to provide data as comprehensive as what the CDC might make available.
Think about what might have been possible if the CDC had continued tracking all breakthrough cases, or had even stepped up its investigation of these cases through increased testing and genomic sequencing. Imagine if we had data showing breakthrough cases by age group, by high-risk health condition, or by occupational setting—all broken out by their severity. What if we could compare the risk of someone with diabetes getting a breakthrough case, to the risk of someone who works in an elementary school?
If we had this kind of data, the FDA and CDC advisory committees would have information that they could use to determine the potential benefits of booster shots for specific subsets of the U.S. population. Instead, these committees had to make guesses. Their guesses didn’t come out of nowhere; they had scientific studies to review, data from Pfizer, and information from Israel and the U.K., two countries with better public health data systems than the U.S. But still, these guesses were much less informed than they might have been if the CDC had tracked breakthrough cases and outbreaks in a more comprehensive manner.
From that perspective, I can’t really fault the CDC and the FDA for casting their guesses with a fairly wide net—including the majority of Americans who received Pfizer shots in their authorization. There’s also a logistical component here; the U.S. has a lot of doses that are currently going unused (thanks to vaccine hesitancy), and may be wasted if they aren’t used as boosters.
But it is worth emphasizing how a lack of data on breakthrough cases has driven a booster shot decision based on fear of who might be at risk, rather than on hard evidence about who is actually at risk. Other than seniors; the risk for that group is fairly clear.
The booster shot decision casts a wide net. But at the same time, it creates a narrow band of booster eligibility: only people who got two doses of Pfizer earlier in 2021 are now eligible for a Pfizer booster. Recipients of the Moderna and Johnson & Johnson vaccines are still left in the dark, even though some of those people may need a booster more than many people who are now eligible for additional Pfizer shots. (Compare, say, a 25-year-old teacher who got Pfizer to a 80-year-old, living in a nursing home, with multiple health conditions who got Moderna.)
That Pfizer-only restriction also stems from a data issue. The federal government’s current model for approving vaccines is very specific: first a pharmaceutical company submits its data to the FDA, then the FDA reviews these data, then the FDA makes a decision, then the CDC reviews the data, then the CDC makes a decision.
By starting with the pharmaceutical company, the decision-making process is restricted to options presented by that company. As a result, we aren’t seeing much data on mixing-and-matching different vaccines, which likely wouldn’t be profitable for vaccine manufacturers. (Even though immunological evidence suggests that this could be a useful strategy, especially for Johnson & Johnson recipients.)
In short, the FDA and CDC’s booster shot decision is essentially both ahead of evidence on who may benefit most from a booster, but behind evidence for non-Pfizer vaccine recipients. It’s kind-of a mess.
I also can’t end this post without acknowledging that we need to vaccinate the whole world, not just the U.S. Global vaccination went largely undiscussed at the FDA and CDC meetings, even though it is a top concern for many public health experts outside these agencies.
48. An observation: There was zero discussion today about the global vaccine supply situation or how use of boosters in the United States might affect getting first doses to billions around the world. Not. One. Word. #ACIP
At an international summit this week, President Biden announced more U.S. donations to the global vaccine effort. His administration seems convinced that the U.S. can manage both boosters at home and donations abroad. But the White House only has so much political capital to spend. And right now, it’s pretty clearly getting spent on boosters, rather than, say, incentivizing the vaccine manufacturers to share their technology with the Global South.
Among the top vaccine donors: -13% of vaccines donated by US have been delivered – 49% of China's donations delivered – 34% of Japan's donations delivered – 4% of Germany's delivered – 8% of UK's delivered
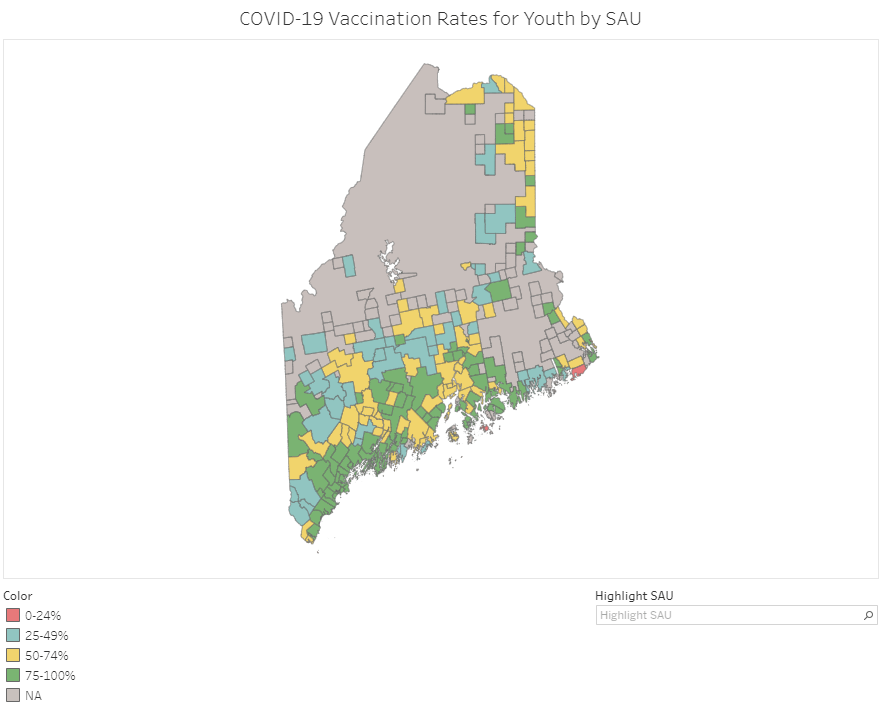
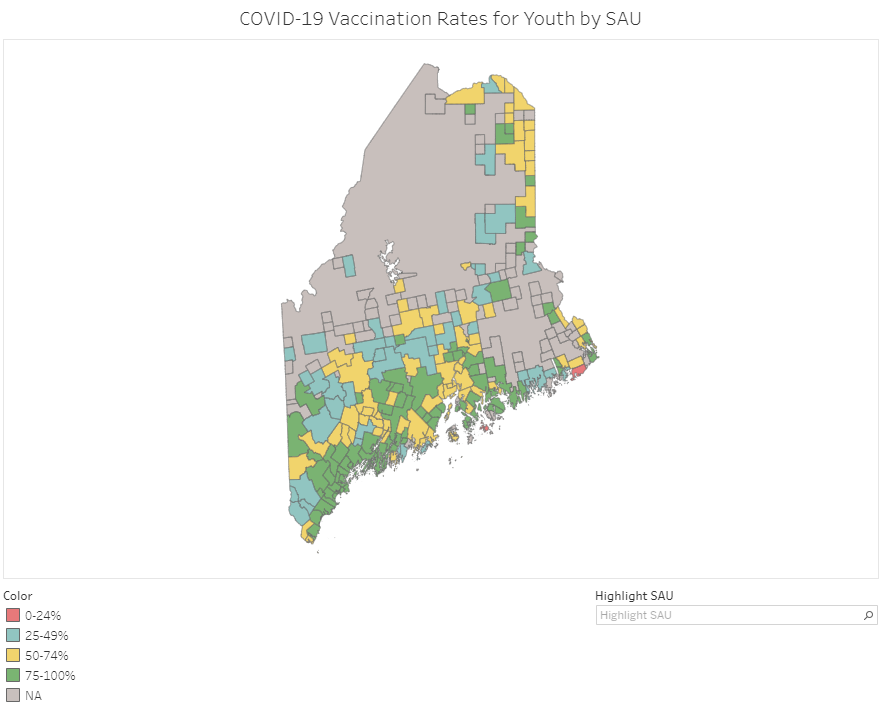
Vaccination rates in Maine’s school administrative units (SAUs). Screenshot taken on September 18.
At this point in America’s vaccine rollout, almost every state has a detailed dashboard. (Nebraska and Florida used to have detailed dashboards, before taking those sites down earlier this summer in a growing trend of states reducing their COVID-19 reporting.)
This dashboard is incredibly useful; individual school districts can compare their vaccination rates to those of their neighbors, while anyone doing state-level research can get a quick overview of where districts stand. As of September 18, just two districts have under 25% of their teens vaccinated (Cutler Public Schools and MSAD 76), while a few districts have vaccination rates over 95%.
Maine’s Division of Disease Surveillance intends to update these data “about every two weeks,” according to the agency’s website.
This past Friday, the Food and Drug Administration (FDA)’s vaccine advisory committee voted to recommend booster shots of the Pfizer-BioNTech vaccine for all Americans over age 65 and those who are particularly vulnerable to the virus, due to their health conditions and/or work environments. This was a notable recommendation because it went against the FDA’s ask: booster shots for everyone over the age of 16.
Let’s walk through the data behind this decision.
How is the current two-dose vaccine regimen faring against severe COVID-19 disease?
Before we get into any numbers, it’s important to remember the initial goal of the COVID-19 vaccines: protect people against severe disease, hospitalization, and death, basically reducing the coronavirus’ power to cause deadly harm.
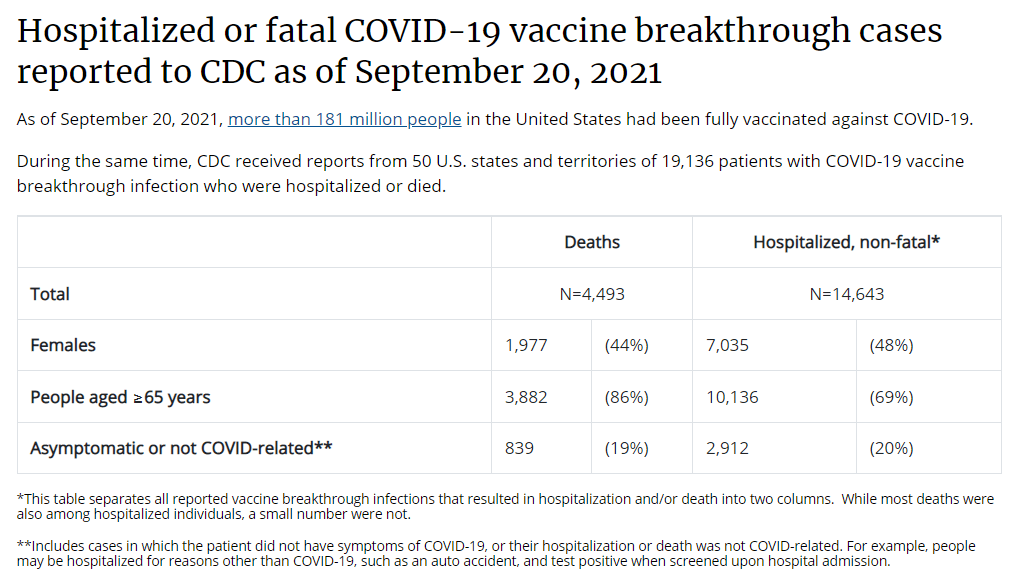
On this front, all of the vaccines are performing well. Numerous papers cited during the advisory meeting, as well as the U.S.’s breakthrough case data, suggest that vaccination protects against severe COVID-19 disease for the vast majority of recipients. Among over 178 million people who had been fully vaccinated in the U.S. by mid-September, just 3,000 have died following a positive COVID-19 test. Those 3,000 deaths account for just about 1% of all COVID-19 deaths in the U.S. since January 2021.
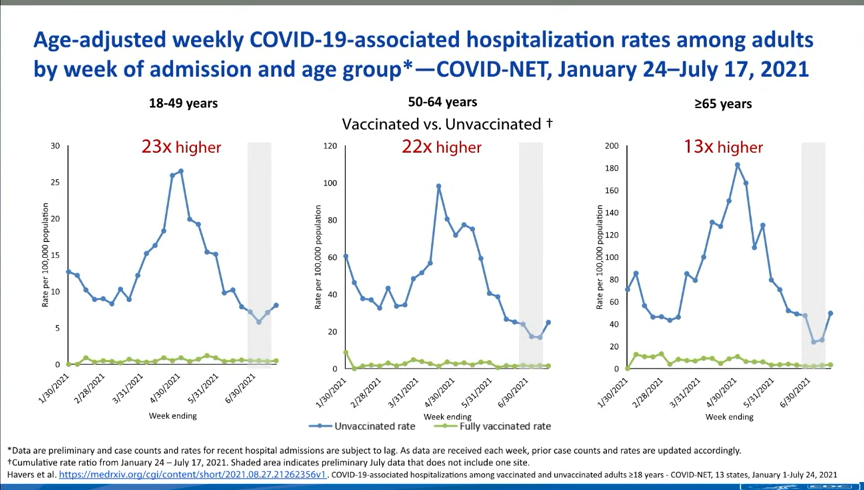
The numbers get a bit more complex, however, when you look at older adults and other vulnerable populations. Those who were more vulnerable to a severe COVID-19 case in the first place are also more vulnerable to having a severe breakthrough case, if they encounter the virus after vaccination. One chart, presented at the FDA meeting, provides a picture of this trend. From late January to mid-July, 2021, the hospitalization rate among younger adults (ages 18-49) was 23 times higher for the unvaccinated than for the vaccinated. For seniors (over age 65), however, the rate was 13 times higher for the unvaccinated.
Seniors are more likely to experience a severe breakthrough case than younger adults, CDC data suggest.
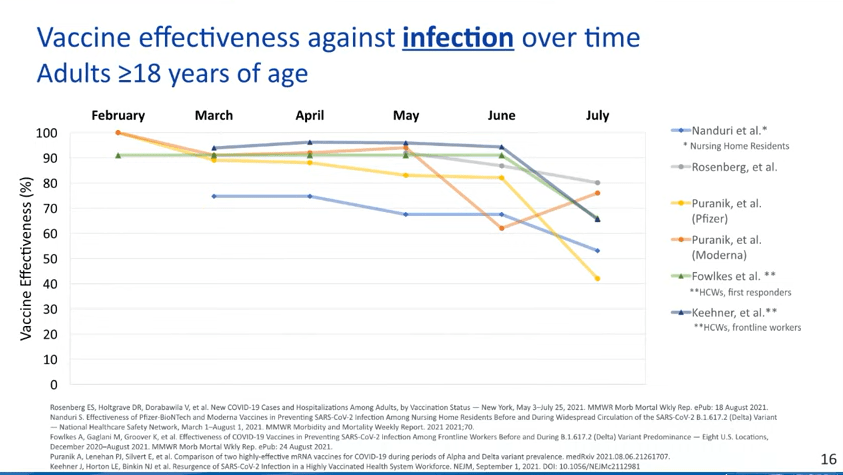
How is that current regimen faring against coronavirus infection?
This is where we see a bigger drop in efficacy. Multiple studies point to the Pfizer and Moderna vaccines becoming less capable of protecting recipients against infection, over time; in other words, if you got your two shots in April 2021, you’re more likely to get a positive test result now, in September, than you were in May. (Though your case will likely be mild or asymptomatic!)
While the vaccines are still highly effective against severe disease, their effectiveness against coronavirus infection appears to be waning.
We can also see this in breakthrough case numbers when we look at all infections, as opposed to only those cases that lead to severe disease or death. This type of analysis is difficult to do in the U.S., as the CDC is only systematically tracking those severe cases, but we can see patterns in the data from local jurisdictions that are reporting their breakthrough cases more comprehensively.
For example, let’s look at Washington, DC, which reports breakthrough cases in extensive detail:
Washington, D.C. is seeing many more breakthrough cases now than it was earlier in 2021.
During the week of March 8, DC reported 14 breakthrough cases. The district reported about 800 cases overall that week, meaning that breakthroughs accounted for 2% of all cases.
During the week of August 23, however, the district reported almost 500 breakthrough cases. In that week, the district reported about 1,400 cases overall—meaning that breakthrough cases have jumped from 2% of all weekly DC cases to 35% of all weekly DC cases.
DC also reports a breakdown of breakthrough cases according to the time it’s been since residents were fully vaccinated. This reveals that most breakthroughs occur at least two months after an individual completed their dose series, with the highest number of breakthroughs in people who’d been vaccinated three to four months ago. We can assume that similar patterns are occurring elsewhere in the country.
It’s also worth noting that we don’t have a great sense of how well the vaccines protect against Long COVID—though data thus far suggest that post-vaccination Long COVID cases are much rarer than non-breakthrough cases.
Why are the vaccines appearing to lose their effectiveness?
This was a big point of discussion for the FDA advisory committee. Are the Pfizer and Moderna vaccines appearing to lose their ability to protect us against coronavirus infection because Delta has a special ability to evade the vaccines or because the vaccines become less effective over time?
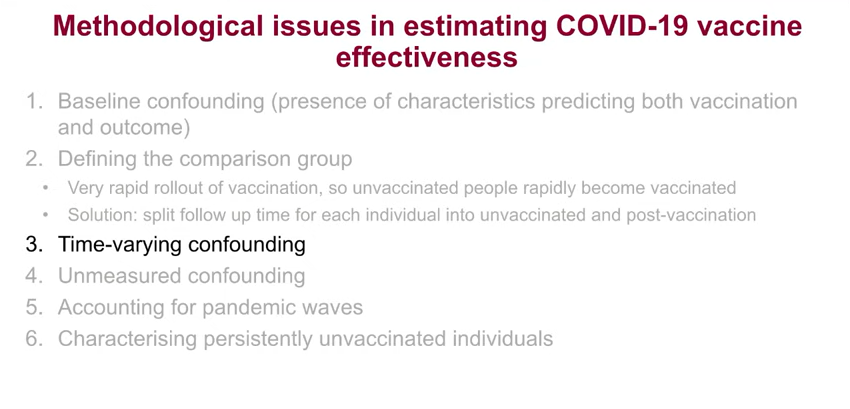
One early-morning presenter at the FDA meeting, medical statistician Jonathan Sterne from the University of Bristol, dove into this issue. His presentation focused on confounders, a statistical term for an outside force that influences the question a researcher is trying to study. In the case of vaccine effectiveness, Sterne said, there are a lot of confounders; these include vaccine recipients’ ages, how long ago they were vaccinated, and when they were vaccinated (i.e. in which phase of the pandemic?).
Sterne’s presentation focused on the confounders that make it difficult to estimate vaccine effectiveness.
Sterne and other British researchers have taken advantage of the U.K.’s extensive electronic health records to analyze how well the vaccines are working, attempting to take these confounders into consideration. Overall, he said, it’s very challenging to get trustworthy effectiveness numbers—though the U.K. has approved boosters for residents over age 50, so it’s clear that the country’s public health agency does see some need for the additional shots.
Sterne’s presentation, as did a presentation from Israeli public health officials, also underscored the need for the U.S. to collect more standardized data on breakthrough cases, among other things.
This current discussion from the CDC on collecting data about the vaccines just reveals how terrible the U.S. collection of health data are. All of it goes back to our fragmented IT infrastructure. Compare it to the data coming from the U.K.'s NHS.
Why did the FDA advisory committee vote against booster shots for everyone, ages 16 and over?
When this advisory committee votes on a question regarding vaccines or another biological product, the committee is specifically asked to consider whether the benefits of the product outweigh the risks. In this case, do the benefits of widespread boosters outweigh the risks of potential side effects from those additional doses?
When it comes to those risks of potential side effects, the committee had strikingly little data to evaluate. Pfizer did conduct a clinical trial of booster shots, but it only included 306 participants—an incredibly small number, when compared to the massive trials of the vaccine’s original two-dose regimen. The trial didn’t include any participants under age 18 or over age 55, which some advisory committee members found problematic, as they were being asked to consider approval for all Americans over age 16.
Israel—which has now administered booster shots to over 2.8 million residents—provided some data on side effects, but their utility is limited. The country started giving boosters to older adults before moving to younger adults, limiting Israeli health officials’ ability to identify potential risk for myocarditis or other severe side effects that might be more common in the younger population.
Israel has only identified 19 serious vaccine side effects from its booster shot rollout thus far, but the majority of the country’s young adults have yet to be vaccinated.
While data from Israel do suggest that booster shots can bring down infection numbers in an overall population, the FDA advisory committee did not find that a sufficient argument to recommend boosters for all Americans. Not at this time, anyway.
Why did the committee vote to support boosters for seniors and other vulnerable populations?
The risks of booster shots may not be clear for younger adults, but the risks of a breakthrough COVID-19 case are clear for older adults and others with health conditions that make them more vulnerable to severe COVID-19 case. The committee’s vote to recommend boosters for vulnerable groups aligns with a growing scientific consensus: that the U.S. should protect seniors, nursing home residents, and others who are at higher risk for serious COVID-19 cases.
What happens next?
It’s important to underscore here that this booster shot recommendation came from a committee that advises the FDA, not from the FDA itself. The agency typically follows its committee’s recommendations, but it doesn’t have to. We can expect the FDA’s decision—approval of booster shots for vulnerable groups, for everyone over age 16, or something else—within a couple of days.
Next week, on Wednesday and Thursday, a CDC advisory committee is set to meet to further discuss booster shots. If both the FDA and CDC approve boosters, health departments across the country are prepared to begin administering them to eligible Americans; this will likely include seniors and other vulnerable adults who previously got two shots of the Pfizer vaccine.
What about everyone who got the Moderna or Johnson & Johnson vaccines?
Again, this decision focused on the Pfizer vaccine, so Moderna and J&J recipients will need to wait for more data and more deliberation. Moderna has formally applied to the FDA for authorization of its booster shot, so we may see a similar series of meetings about that vaccine in the coming weeks.
J&J vaccine recipients will likely experience a longer wait as researchers collect data on the effectiveness of this one-shot vaccine. CNET has a good explainer of the situation.
Also: If you’d like to read a more detailed breakdown of everything that happened at Friday’s advisory committee meeting, I highly recommend the STAT News liveblog by Helen Branswell and Matthew Herper, which I drew upon heavily in writing this post.
This week, we have a couple of source updates and a couple of additional data news items.
Pediatric data from the CDC: In a rather timely update, the CDC has added a pediatric data tab to its COVID Data Tracker dashboard. The new page links to all the data on COVID-19 and kids that the agency has available: including multisystem inflammatory syndrome in children (MIS-C), demographic data for vaccinations and hospitalizations, and COVID-19 outcomes during pregnancy.
Additional vaccine doses (also CDC): The CDC recently added an important new field to the vaccination page of its dashboard: people who received an additional vaccine dose. This includes about 1.3 million people as of September 4. The count started on August 13, when the CDC’s vaccine advisory committee endorsed additional shots for immunocompromised Americans—though the CDC’s dashboard doesn’t distinguish between those additional dose recipients who are and are not immunocompromised, according to their “about the data” page.
More states pull back on COVID-19 reporting: Here at the CDD, we love to call out states that stop reporting key COVID-19 data points or make that reporting less frequent. A new article from KHN’s Andy Miller speaks to this trend, which has continued in recent weeks despite the Delta surge. The article specifically calls out government websites in Georgia, which stopped updating public data on COVID-19 in prisons and long-term care facilities “just as the dangerous Delta variant was taking hold,” Miller reports.
New study provides rigorous evidence that masks work: On Wednesday, authors of a randomized control trial study—the gold standard of scientific research—shared their findings in a preprint. The study investigated mask use by providing different levels of free mask supplies and promotion to different villages in Bangladesh. Villages that received the masks and learned about their use had fewer COVID-19 cases, with the villages that received surgical masks (as opposed to cloth masks) seeing the biggest impact. This study is a pretty big deal, with one commenter calling it “arguably the most important single piece of epidemiological research of the entire pandemic.” For more context, see this Washington Post article.
This week, the federal government announced that the U.S. intends to provide third vaccine doses to all Americans who received the Pfizer or Moderna vaccines. This booster shot distribution will start in September, with adults becoming eligible once they hit eight months after their second shot.
While the booster shot regimen still must be approved by the FDA and CDC, federal officials are making it sound like a pretty sure thing—President Biden himself announced the decision at a press conference on Wednesday. However, many epidemiologists, vaccine experts, global health experts, and other scientists have criticized the decision.
Here are three main criticisms I’ve seen in the past few days.
First: Scientific evidence is lacking. As the booster shot decision was announced on Wednesday, the CDC published threenewstudies that appear to show a decline in the Pfizer and Moderna vaccines’ ability to stave off symptomatic COVID-19 infection after several months. One of these reports, from a network of U.S. nursing homes, suggests that efficacy among nursing home residents fell to just 53% by June and July 2021, many months after this vulnerable population was vaccinated. The other two reports show similar declines, though the CDC found that vaccination remains effective against severe disease, hospitalization, and death.
The federal government—and others arguing in favor of booster shots—have also pointed to data from Israel, which appear to similarly demonstrate that the vaccines lose their effectiveness after several months. In Israel, where almost 80% of residents over age 12 are vaccinated, the majority of those hospitalized with COVID-19 are now fully vaccinated individuals.
But the act of interpreting these data is more complicated than it first appears. In a blog post at COVID-19 Data Science, biostatistics professor Jeffrey Morris explains that, when the majority of a population is vaccinated, vaccination numbers will go up in this population simply because they are the majority. But the risk remains far higher for the unvaccinated. Plus, Morris explains, stratifying hospitalization numbers by age reveals that older adults are more likely to have a severe COVID-19 case regardless of vaccination status, while younger adults are less likely to be vaccinated (and thus have a non-breakthrough case).
Simply put, the vaccines do still work well against severe COVID-19—you just need to be precise in calculating effectiveness. And yet, the U.S. government is saying that vaccine efficacy wanes so much, everyone’s going to need a third shot in the fall or early next year. This suggests that the federal government has more data that it is not sharing publicly, which leads us to the second criticism.
Second: Transparency is also lacking. Typically, when the government makes a decision about approving a new medical product, this decision follows a series of prescribed steps: data submission from the company behind the product, review by FDA scientists, FDA approval, followed by more review by other agencies (such as the CDC or the Centers for Medicare & Medicaid Services) as needed. Review meetings are typically open to the public, with data shared in advance of a decision. In the case of these booster shots, however, the president has announced a specific rollout plan before full scientific review has taken place.
To many experts, including Baylor, the sequencing of the decisions being made is also out of whack. While U.S. health officials said booster shots could start being offered the week of Sept. 20, the Food and Drug Administration has not even ruled yet on Pfizer’s application for approval of a third shot; it was filed only Monday. Moderna hasn’t yet asked the agency to authorize a third shot at all.
The FDA and CDC will certainly still be reviewing the need for booster shots, but the experts cited in Branswell’s piece are skeptical that any decision other than, “Yes, go ahead” will be considered. I, for one, will be very curious to see how the discussions proceed—and what data get cited—at the FDA and CDC committee meetings.
Third: We need to vaccinate the world. As I’ve explained in the CDD before, getting vaccines to the low-income nations that have yet to start their rollouts is not just a humanitarian priority. It also protects us, here in the U.S., because the longer the coronavirus circulates, the more opportunities it has to mutate into increasingly-dangerous variants.
By moving to provide booster shots to everyone—not just the immunocompromised, the elderly, or the otherwise extra-vulnerable—the U.S. is likely delaying shots to other countries, prolonging the pandemic overall.
As Dr. Michael Ryan, emergencies chief at the World Health Organization, told reporters last week: “We’re planning to hand out extra life jackets to people who already have life jackets, while we’re leaving other people to drown without a single life jacket.”
Following the end of the federal public health emergency in May, the CDC has lost its authority to collect vaccination data from all state and local health agencies that keep immunization records. As a result, the CDC is no longer providing comprehensive vaccination numbers on its COVID-19 dashboards. But we still have some information about this year’s vaccination campaign, thanks to continued CDC efforts as well as reporting by other health agencies and research organizations.
This week, the FDA authorized Novavax’s updated COVID-19 vaccine. Here’s why some people are excited to get Novavax’s vaccine this fall, as opposed to Pfizer’s or Moderna’s.
Last week, I asked you, COVID-19 Data Dispatch readers, to send me your stories of challenges you experienced when trying to get this fall’s COVID-19 vaccines. I received 35 responses from readers across the country, demonstrating issues with insurance coverage, pharmacy logistics, and more.