Scientists are moving closer to biomarkers, or clear biological indicators, of Long COVID. A new study—posted this week in Nature ahead of full publication—identifies clear differences between blood samples of people who have the condition and those who don’t.
The study was a collaborative effort between researchers at Mount Sinai (David Putrino and his team) and Yale University (Akiko Iwasaki and her team). Both of these research groups have been leaders in studying Long COVID: Mount Sinai was one of the first health institutions to start caring for people with Long COVID back in spring 2020, while the Yale group has analyzed patients’ immune systems in ways that go far beyond typical medical testing.
The differences identified by this study fall into “three big areas,” Putrino wrote in a Twitter thread describing the findings. These are hormonal differences (particularly low cortisol levels in the Long COVID group during morning hours), immune differences (particularly differences in T cell and B cells for people with Long COVID), and evidence of a coronavirus infection re-activating other viruses that might have already been present in people with Long COVID.
While other research has pointed at these Long COVID markers before, the new study goes further in connecting a Long COVID diagnosis to specific medical tests. If backed up by further research, those tests could be used as biomarkers, informing clinical trials of Long COVID treatments. Notably, as Iwasaki pointed out in a statement, the tests done in this study would not be included in a patient’s “routine lab work,” signifying the higher level of inquiry needed to understand this condition.
Long COVID is incredibly complex and may have different causes from one person to another. So, any biomarkers (from this study or another one) likely would not be universal points of success for all patients. This study also isn’t “proof that Long COVID is real,” as you might have seen some headlines suggest; we’ve had plenty of proof for years now, from prior research and patient experiences. Still, the study is a major step forward in identifying key tests that may be used for diagnosis and treatment.
CDC respiratory virus updates: The CDC has a new webpage dedicated to “updates on the respiratory illness season.” So far, it just includes summaries of the agency’s two reports on new variant BA.2.86. Going forward, the page will be updated weekly with further information on COVID-19, flu, RSV, and other viruses spreading this fall and winter.
Potential biomarker for Long COVID brain fog: A new paper, published this week in Nature by a coalition of researchers in the U.K., connects blood clot issues during acute COVID-19 to cognitive symptoms later on. The researchers found that some patients had low levels of two specific proteins connected to blood clots, based on blood samples taken early in their infections; the same patients were likely to experience brain fog and similar symptoms. If these results are replicated in other studies, the proteins could be used as biomarkers (i.e. medical indicators) of Long COVID symptoms, potentially a big step for research and treatments.
Long COVID research presented at Keystone Symposia event: Speaking of Long COVID research: scientists gathered to discuss this condition at a conference last week in New Mexico. The conference was hosted by Keystone Symposia, an organization that convenes meetings on important life sciences topics. Highlights from the event included a presentation showing changes to muscle tissue during post-exertional malaise, along with presentations from the Patient-Led Research Collaborative, the National Institutes of Health, Resia Pretorius from Stellenbosch University in South Africa, Akiko Iwasaki from Yale University, and more. I look forward to seeing papers expanding on the talks that occurred at this meeting.
COVID-19’s impact on Native Americans: Another notable paper from this week examined COVID-19’s disproportionate impacts on Native Americans in New Mexico. Researchers at the University of New Mexico Hospital analyzed patient outcomes in early pandemic waves, from spring 2020 through winter 2021. Compared to white and Hispanic patients, Native Americans were more likely to experience severe COVID-19 outcomes such as more time spent in the hospital and going on a ventilator. “Self-reported AI/AN race/ethnicity emerged as the highest risk factor for severe COVID-19,” the researchers reported, suggesting that this vulnerable group of people deserves additional safety resources.
COVID-19 burden for cancer patients: One more study to highlight: researchers at Massachusetts General Hospital examined COVID-19 mortality among cancer patients during the first two years of the pandemic, using data from the CDC. People with cancer were more likely to die of COVID-19 during the winter Omicron wave in 2021-2022, compared to the surge during the prior winter (with 18% higher deaths). Meanwhile, deaths among the general population went down from the first to the second winters. Like the study above, this paper suggests that greater protections are needed for vulnerable people during times of high COVID-19 spread. (For example: we could keep masks in healthcare settings!)
This Tweet, from the NIH’s Community Engagement Alliance, sparked criticism on social media—some of which was hidden by the NIH account.
By Miles W. Griffis
The National Institute of Health (NIH) is under fire for censoring comments from patients on social media — the latest in a trend of heavy criticism from people living with Long COVID for failing to listen to patients and implement their input into its $1.15 billion study, RECOVER. Patient concerns have been echoed by both scientists and healthcare professionals who have criticized the study’s lack of results, glacial pace, potentially harmful clinical trials, and wasted funds.
Last month, the NIH Community Engagement Alliance (NIH CEAL) tweeted, “Some people don’t feel sick when they have #COVID19 but develop symptoms of #LongCOVID later on. If this sounds familiar, speak with your health care provider to find a treatment plan that works for you.” The controversial tweet received over one hundred responses, many from people with Long COVID and other infection-associated illnesses.
Patients claimed the post contained misinformation about Long COVID treatments, as this debilitating multi-systemic condition affecting millions does not have any approved treatments or cures. Other commenters shared their negative experiences with their primary health care providers, who they say didn’t offer them any treatment plans or worse, gaslit them and wrote their symptoms off completely. Over 35 of these comments were hidden by the NIH CEAL account.
When asked about this comment hiding, the NIH told me that their social media policy was “overapplied” and that comments on the post were “inappropriately hidden.”
Olenka Sayko, a person with Long COVID whose comment was hidden, said the censorship added to a feeling of hopelessness: “Are we ever going to find solutions for Long COVID if patient voices aren’t being listened to?” She said the censorship is especially concerning since it came from an NIH account dedicated to community engagement. “Who are they engaging with? They’re hiding comments.” Lauren, another person with Long COVID who also was censored, said that the NIH CEAL’s tweet rhetoric sweeps Long COVID and the people experiencing it “under the rug.”
NIH CEAL clarified their tweet earlier this month. “While there’s no cure for Long COVID,” the new post read, “there may be treatment options that can address one’s symptoms & may help people living with Long COVID have better days.”
Although there are no treatments or cures for Long COVID, there are some treatments for conditions associated with or triggered by COVID-19 or Long COVID, including dysautonomia, cardiac disease, diabetes, and others. Many healthcare professionals recommend that patients who have prolonged symptoms following COVID-19 should be screened for life-threatening medical events that can be caused by COVID-19 or Long COVID, including pulmonary embolisms, deep vein thrombosis, or strokes. Long COVID can be fatal. A CDC analysis found that more than 3,500 people have died of the condition, though many experts believe this is a vast undercount.
And while there are many Long COVID clinics around the country that may give the illusion of successful treatment plans, patients often don’t have successful experiences. In an article I wrote for Popular Science, I found that some clinics recommend potentially harmful treatments like graded exercise therapy. Others rejected and gaslit patients. Some only offered generic informational handouts.
During an August 31 NIH RECOVER press conference, the director of the National Institute of Neurological Disorders and Stroke (NINDS), Walter Koroshetz, responded to my question about what Long COVID treatment plans the NIH CEAL account was referring to. He said that the NIH does not make treatment recommendations, adding that the NIH CEAL tweet might have been a misunderstanding. When I asked why the agency was censoring tweets from Long COVID patients, Lawrence Tabek, the acting director of the NIH, said he couldn’t speak to my question and said he has “no idea how social media works”.
I later followed up with the NIH over email about the censored comments. The agency wrote that “The National Heart, Lung, and Blood Institute (NHLBI) and the National Institute on Minority Health and Health Disparities (NIMHD) co-manage the NIH Community Engagement Alliance (CEAL) social media accounts and follow the NHLBI Privacy Statement and Comment Policy.” The policy states commenters should post “on topic,” “be respectful,” and “truthful.” It also prohibits spam and product endorsements.
The NIH wrote over email that, in the case of the censored comments on the July 25th tweet, their policy was “overapplied” and that comments on the post were “inappropriately hidden.” They added that upon further review, comments on the post are now “public,” or unhidden. Some comments, however, were still hidden at the time of publication.
But Eric Goldman, the co-director of the High Tech Law Institute at Santa Clara University School of Law, said this very policy may not be even constitutional. “Assuming that the NIH is a state actor, then anytime they take an action on social media to control the conversation, their decisions are governed by the First Amendment, which protects our right to free speech,” he said.
Instances like the NIH censoring comments on social media are complicated, but upcoming Supreme Court cases may provide some clarity, Goldman said.
Two cases, Lindke v. Freed (from the 6th Circuit Court of Appeals) and Garnier v. O’Connor-Ratcliff (from the 9th Circuit Court of Appeals) may be heard by the Supreme Court this fall. Both involved government officials blocking members of the public on social media, but each led to a different result. The 9th Circuit found impermissible censorship, while the 6th Circuit did not. Due to the complexity of internet law, it’s unlikely Americans will feel good about the rule of law that will be articulated by the Supreme Court,” he said.
Still, if the NIH is “selectively listening to people online, then that’s hugely problematic,” Goldman said. In particular, the NIH could be denying the patients’ ability to learn and talk with each other. “Selective intervention by the NIH takes away that potential,” he said.
Advocates say the censorship has further eroded trust between the Long COVID community and the NIH. “It’s not just a one off,” Billy Hanlon, the director of advocacy and outreach for the Minnesota ME/CFS Alliance said, “It’s a pattern.” The agency fails to value the lived experience of patients with infection-associated illnesses, even though these illnesses have a quality of life worse than some advanced-stage cancers, Hanlon said.
“I can see why people were furious,” said JD Davids about the censorship “It’s an insult upon injury.” As the co-director of the advocacy group Long COVID Justice, Davids said that if the NIH wants to truly work and engage with patients, they need to work closely with people living with Long COVID and certainly not silence their lived experience.
“We need a government-wide response to Long COVID,” he said, describing the necessity for patients and complex chronic disease experts to be consulted on major decisions at the NIH and beyond. Tweeting that there is a treatment plan for a condition with no treatments or cures, Davids said, creates an illusion of a broader treatment plan for Long COVID, when there isn’t one. It confuses the public and creates doubt about people living with Long COVID. “It has huge unintended consequences,” Davids said.
Editor’s note: JD Davids has donated to the COVID-19 Data Dispatch. This had no influence on the article, as the author talked to him before the CDD decided to publish it.
Miles W. Griffis is an independent journalist based in Los Angeles, California. He’s written for High Country News, National Geographic, The New York Times, and many others.
If you are able to contribute a tip for this reporting, please Venmo @miles-griffis.
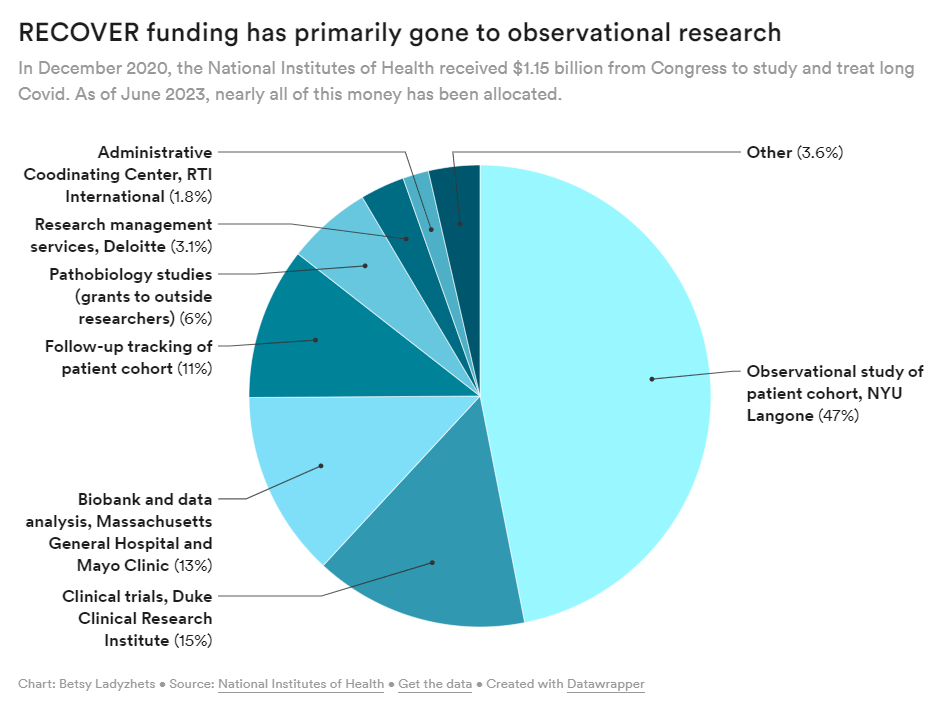
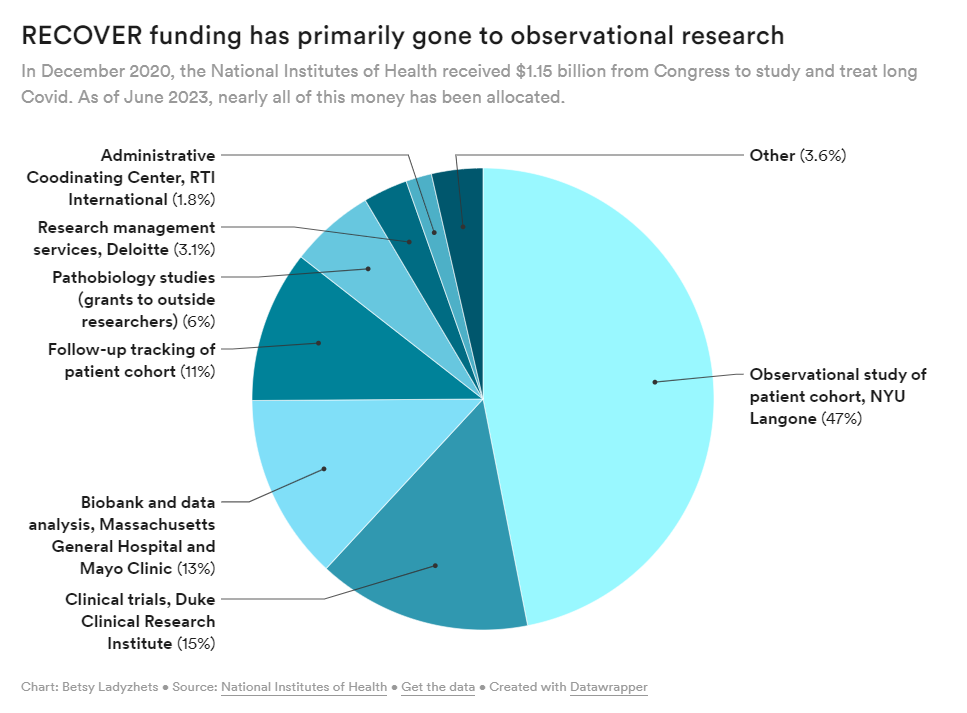
The NIH has primarily spent its funds for Long COVID research on observational studies rather than clinical trials, according to new data shared with my article this week.
Last week, the National Institutes of Health and Duke University announced five Long COVID clinical trials as part of the NIH’s RECOVER initiative. This might sound like an exciting milestone for the millions of people dealing with long-term symptoms—but in fact, experts and long-haulers are disappointed by the trials, I learned when covering this news for MuckRock and STAT News.
RECOVER is the largest Long COVID research effort in the world; the NIH received $1.15 billion for it, provided by Congress in late 2020. It’s also been plagued by delays and criticisms, as I’ve reported before. As we approach the three-year mark of the initial funding, long-haulers are becoming increasingly frustrated with RECOVER’s lack of results.
My latest story for MuckRock and STAT focuses on the clinical trials, but connects to larger issues with RECOVER and with the federal government’s response to Long COVID in general. Read it on STAT’s site here or on MuckRock’s here.
RECOVER is only testing a handful of drugs for Long COVID, instead focusing on behavioral interventions that outside experts say are unlikely to address underlying causes of symptoms. There are several lists of potential drugs that should be (and aren’t) prioritized, including one compiled by members of an advisory committee to RECOVER.
Looking more closely at the drug trials, experts shared concerns about the study designs, suggesting that RECOVER’s choices of controls, outcomes measures, and other aspects of the studies may lead to inaccurate results. For example, dysautonomia expert Lauren Stiles told me that the trial testing drugs for autonomic symptoms may fail to accurately capture whether those drugs help with Long COVID.
At this point, the NIH has no plans for further Long COVID trials or other research going beyond RECOVER. The initiative has almost fully allocated all of its $1.15 billion in funding, and NIH officials haven’t shared details about how they will continue Long COVID research after this study concludes (though they acknowledge more research will be necessary).
RECOVER failed to put much funding in clinical trials to begin with, focusing instead on observational studies aiming to track Long COVID symptoms over time. While such studies could be valuable for better understanding the condition, RECOVER has largely replicated other research and hasn’t contributed useful, new information to the field, experts have told me. In fact, over 40,000 people have petitioned the NIH to retract RECOVER’s first paper based on its observational research.
Many of RECOVER’s errors, such as choosing the wrong treatments to prioritize and focusing on observational studies over clinical trials, could’ve been avoided if the initiative had listened more to long-haulers and learned from experts in other post-infectious diseases. Long-haulers have done plenty of research themselves in the last three years, ranging from informal tests of different treatments to formal studies conducted by the Patient-Led Research Collaborative; yet these studies have not informed RECOVER.
Plus, scientists with expertise in ME/CFS, dysautonomia, HIV/AIDS, and many other similar diseases could share lessons with RECOVER—but they aren’t leading the initiative. I thought Todd Davenport, a rehabilitation expert at University of the Pacific who’s studied ME/CFS, put it well when he said that RECOVER scientists “have parachuted into post-infectious illness and are now trying these things for the first time, to them. But it’s clear they haven’t done the reading.”
I hope to continue covering RECOVER and other issues with Long COVID research in the U.S. If you have any tips or stories to share with me on this topic, please reach out.
Ed Yong, a widely-admired science journalist, recently announced that he’s leaving his position at The Atlanticafter eight years at the publication. He also published the latest in a series of articles explaining the challenges of Long COVID, a subject that he’s become well-known for covering.
I have been a big fan of Yong’s for a long time; reading his work when I was in college was one of my inspirations for getting into science writing. But his COVID-19 coverage has been especially informative and inspirational. In particular, he was one of the first journalists to write about Long COVID back in 2020 and has remained a leading writer on the topic since then. His work has brought wider recognition to the long-haulers seeking research and support.
His latest story, like his others, is a master class in weaving together patient experiences and scientific insights. It covers fatigue and post-exertional malaise, two of the most common—and most debilitating—symptoms of Long COVID and myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). As people with those conditions have shared the article on social media, I’ve seen many say that it offers poignant descriptions of these symptoms and insightful understanding of their experiences.
If you haven’t read this article yet, please check it out. (Feel free to email me if you have a hard time accessing it through the paywall.) And I think I can speak for many readers here when I express gratitude for Ed Yong’s COVID-19 work over the last three years, and excitement for what he’ll do next!
New papers show wastewater’s predictive value: This week, I noted three recently-published papers that all demonstrate wastewater surveillance’s value for flagging changes in COVID-19 trends before other metrics, such as hospitalizations. One paper, in Nature, found that wastewater trends preempted hospitalization trends by one to four weeks, in 150 U.S. counties. Another paper, in JAMA Network Open, found that wastewater trends tracked with case trends in 268 U.S. counties from January through September 2022; however, the correlation became weaker with reduced clinical testing over time. And a third paper, in PNAS, shares an algorithm that can flag community-level COVID-19 surges before they show up in other metrics, using data from North Carolina’s wastewater surveillance.
Long COVID’s impact on employment: The Urban Institute, a think tank focused on economic and social policy research, published a report exploring employment challenges and related hardships among people with Long COVID. The researchers (a group that included Lisa McCorkell from the Patient-Led Research Collaborative) analyzed results from Long COVID questions included in an Urban Institute survey, conducted among more than 7,500 American adults across the country in December 2022. Among the findings: 10% of adults with Long COVID stopped working for a period due to their symptoms while another 5% reduced their work hours; 24% limited activities outside of work; 42% reported food insecurity in the last year; 20% reported difficulty paying their rent or mortgage.
Characterizing potential Long COVID phenotypes: Another Long COVID study from this week, published in The Lancet: a research consortium including several medical centers across Europe tracked patients over time, seeking to better understand different subtypes of the condition. The study included about 1,000 people with at least one Long COVID symptom, tracked over one year from their initial COVID-19 diagnosis. Researchers found four potential subtypes: one similar to ME/CFS (including fatigue and cognitive symptoms), one with respiratory symptoms, one with chronic pain, and one with changes to taste and smell. The researchers also noted some patient characteristics and aspects of acute illness that may contribute to increased risk of different subtypes.
Outdoor transmission at a night market: One more notable new paper: researchers at local health agencies in China’s Zhejiang province reported on coronavirus transmission at an outdoor night market, in Frontiers in Public Health. In one day at the night market, three infected visitors led to 131 secondary cases, the researchers found. Based on samples from both people at the market and surfaces, the researchers estimated that particles of an Omicron BA.5 strain could linger for over an hour and still be contagious. The study suggests that, even in outdoor settings, transmission is still possible when other precautions aren’t taken.
Acute Hospital at Home data: The Data Liberation Project, which collects and shares data from public records requests, recently published a dataset from a COVID-era program by the Centers for Medicare and Medicaid Services (CMS) which allowed hospitals to treat patients in their homes. Early this year, the project filed a FOIA request for data indicating which hospitals applied to participate in the program and how their patients fared. CMS completed the request in June, and DLP is working to process and understand the resulting data. If you’re interested in using the data, you can check out the documentation and sign up for updates.
Diagnosis challenges with alpha-gal syndrome: Finally, a bit of non-COVID public health news: the CDC recently released some data showing challenges with diagnosing alpha-gal syndrome—a disease transmitted by tick bites that leads to new allergies—despite recent increases in its spread. The CDC estimates that up to 450,000 people in the U.S. may have been impacted by this disease, potentially developing new allergies to meat and other animal products. Yet in one CDC study, the majority of health providers surveyed were not confident in their ability to diagnose the syndrome. This trend reflects similar challenges for other chronic diseases that might be new or unfamiliar to providers, such as Long COVID.
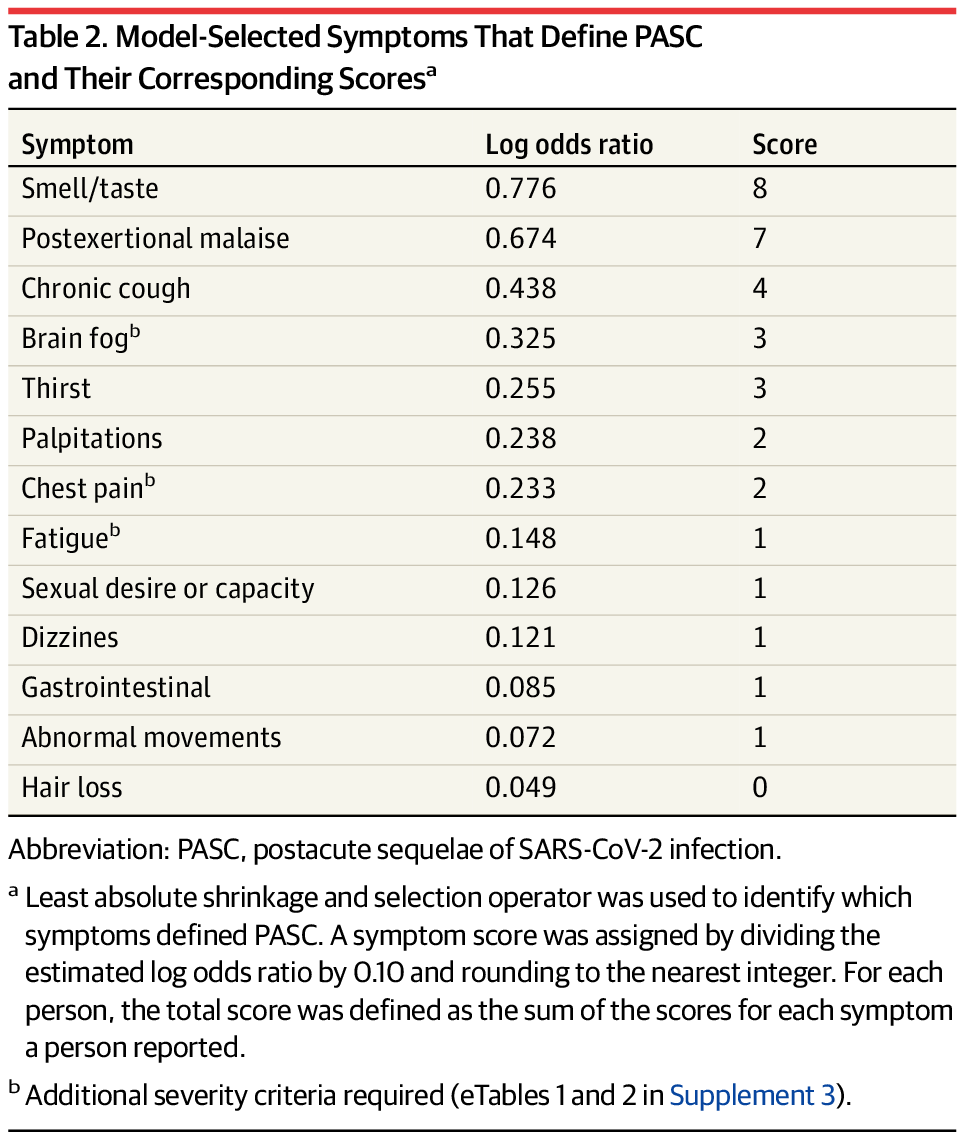
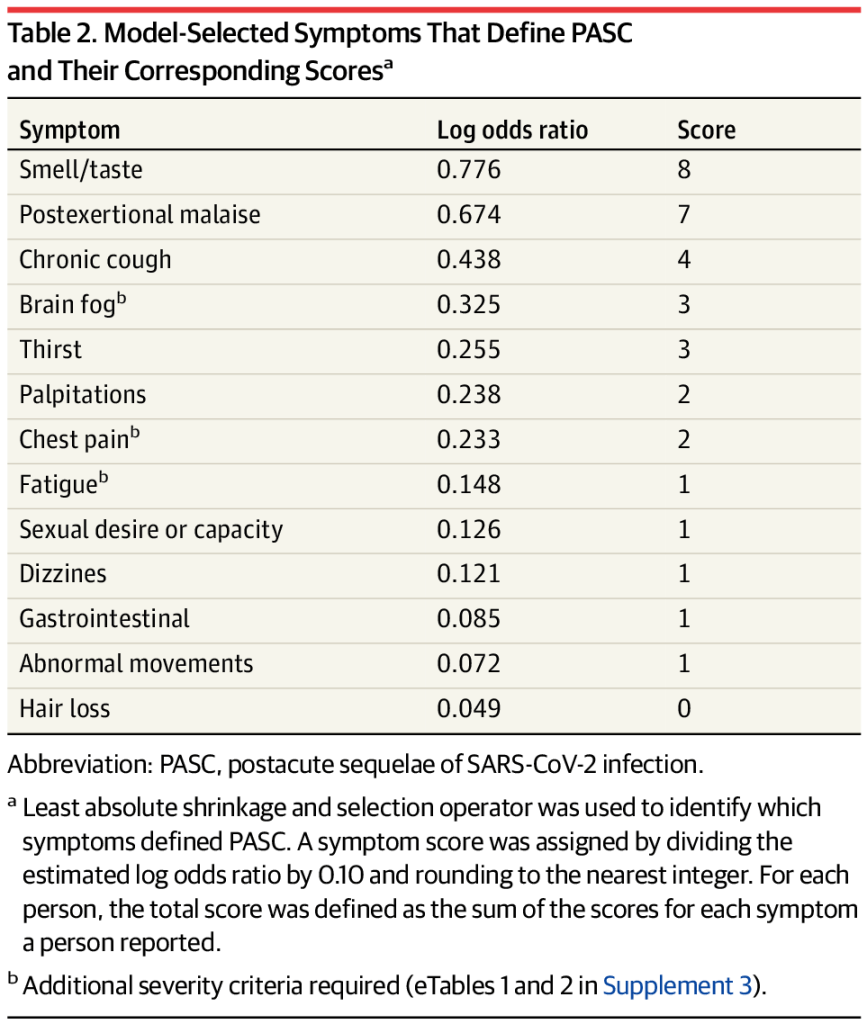
The new RECOVER paper identifies 12 major Long COVID symptoms, but this is far from an exhaustive list defining the condition.
RECOVER, the U.S.’s largest initiative to understand Long COVID, published a major scientific study this week in JAMA. The paper goes over key Long COVID symptoms and other findings from nearly 10,000 adults who have joined the project’s research cohort. Its authors propose a new, more specific definition for Long COVID, which will be used in future studies from this project.
This is a big milestone for RECOVER; it’s the first paper to actually share data from the study’s patient cohort, rather than from electronic health records. While the paper doesn’t provide any truly novel, previously unreported information about Long COVID, it confirms findings from smaller studies and validates patient experiences. It’ll certainly be valuable for thousands of scientists around the country struggling to understand this debilitating condition, though patients have expressed some concerns about the paper’s central framework.
This study is also a rather late milestone, considering that the National Institutes of Health received $1 billion in funding from Congress for this initiative in December 2020 (two and a half years ago), and started enrolling patients in fall 2021. For more details on RECOVER’s delays—and many criticisms it’s faced from patients and experts—please check out this investigation by me and Rachel Cohrs, at STAT News and MuckRock.
Here are a few key things you should know about the paper, and that you should watch out for while reading other articles about it:
The authors’ main goal was to determine which symptoms can specifically be used to diagnose long-term symptoms following a coronavirus infection.Using survey data from RECOVER’s participants, the researchers developed a framework that sorts patients into three categories: definitely having symptoms due to a past coronavirus infection (or “infected”), not having symptoms due to a past infection (“uninfected”), and possibly having symptoms due to a past infection (“unspecified”). This framework prioritizes symptoms unique to Long COVID, such as the loss of smell or taste, over those symptoms that are actually more debilitating for patients, such as chest pain or chronic fatigue. Also, as patient-expert Lisa McCorkell pointed out on Twitter, the unspecified category includes people with Long COVID.
The paper highlights 12 Long COVID-specific symptoms; there are a lot more. I’ve seen some articles covering this study frame it as, “these are the 12 definitive symptoms of Long COVID.” That’s a misrepresentation of the results. In fact, the authors selected 12 common symptoms that are helpful for their framework (i.e. determining who had a coronavirus infection); we know from other research that Long COVID can include up to 200 different symptoms. RECOVER leader Leora Horwitz even acknowledged in a Twitter thread describing the paper that “these are not the ONLY symptoms that people have, nor are they necessarily the most important to patients, the most common, the most severe or most burdensome.”
Long COVID is a spectrum, with different clusters of symptoms. This paper adds more evidence to support a hypothesis I’ve heard from many experts, that Long COVID is not one condition but a variety of overlapping conditions all caused by SARS-CoV-2. Different symptoms might be caused by different biological processes, and different patient groups could require different treatments. RECOVER has identified potential patient groups, which the researchers will study further (including through clinical trials, projected to start this summer).
Long COVID has a wide variety of impacts on day-to-day life, but the most severe patients might not have the best proof. Using this paper’s framework, long-haulers can give themselves a “Long COVID score” reflecting how likely they are to have symptoms caused by a past coronavirus infection. But, as patient-expert Chris Maddison explained, a higher score doesn’t necessarily mean Long COVID has more drastically impacted the patient’s day-to-day life. “I would prefer to flip this, i.e., a def. that centers folks who are suffering regardless of whether we can accurately predict prior infection,” he wrote.
Infection post-vaccination or with Omicron can lead to lower—but still significant—Long COVID risk, compared to earlier in the pandemic. Since RECOVER started recruiting in fall 2021, the study includes some people who were first infected during the first Omicron wave, then developed Long COVID symptoms afterward. About 10% of the patients infected during Omicron later developed symptoms, which pretty close to the study’s overall estimate of Long COVID prevalence (also about 10%). Vaccination or infection with an Omicron variant may make you less likely to get Long COVID, this study suggests, but the risk is still very present.
Repeat infections may increase Long COVID risk. RECOVER was able to follow 2,150 people who got infected during the Omicron wave, including 81 who had multiple infections. Of those with multiple infections, 16 people—or one in five—had Long COVID symptoms within six months. That’s double the prevalence rate of those who just had one infection in the same timeframe (10%). While these are small numbers, the finding is certainly worth further study; see this thread from patient-expert Hannah Davis for more details.
This is not a prevalence paper, and it does not provide a clinical definition of Long COVID. Some media coverage might suggest that this paper has “defined Long COVID,” which is a misrepresentation of the study. While the authors do propose a new framework for evaluating potential Long COVID patients, they make it clear that a lot more research and iteration will be needed before any RECOVER findings should be used in the doctor’s office. The paper also doesn’t provide a definitive answer on how many people get Long COVID, since it includes a relatively small number of people who were uninfected when they joined the study. Quoting Lisa McCorkell again: “It is very clear throughout the paper that in order for this to be actionable at all, iterative refinement is needed.”
This won’t be the last paper sharing findings from the RECOVER cohort. This study presented data from patients’ symptom surveys, which is just one small part of the RECOVER cohort’s activities. The enrolled patients have also undergone extensive medical testing and symptom tracking over time, which will be the subject of future studies—and will be used to refine RECOVER’s Long COVID framework. Clinical trials will (eventually) provide more data as well.
To my fellow journalists covering this study: I highly encourage you to present this paper as a small part of a complicated, iterative research process, rather than a definitive answer to long-standing questions about Long COVID. I also encourage you to talk to patient-experts and ask for their criticisms of the study (like those I’ve cited here), rather than just letting the RECOVER leadership go unchallenged.
In December 2020, Congress gave the National Institutes of Health $1.2 billion to study Long COVID. That money was used to fund the RECOVER initiative, billed as a thorough study of this condition and an effort to help patients actually recover from the often-debilitating long-term effects of COVID-19.
But it’s been more than two years, and the RECOVER initiative doesn’t have much to show for that money—besides a growing number of frustrated people in the Long COVID community. Clinical trials haven’t started yet, very limited research findings have been published, and some long-haulers involved with the initiative are losing faith in its ability to find answers.
I collaborated with Rachel Cohrs, a reporter at STAT News, on a thorough investigation into RECOVER’s problems. We combed through documents and data, talked to a number of people involved with the initiative, and researched the broader context around RECOVER.
This project was a collaboration between STAT and MuckRock, and you can read the full story on STAT’s websiteor on MuckRock’s. I also wrote a Twitter thread with some highlights:
As I wrote on Twitter, I want to keep reporting on RECOVER, as I know there are other problems with the initiative that weren’t captured in this story. If anyone reading this has additional information to share, please shoot me an email or reach out on social media. (You can also reach out to ask for my number on Signal, a secure messaging platform.)
Here’s the story’s introduction, to give you an idea of what we found:
The federal government has burned through more than $1 billion to study long Covid, an effort to help the millions of Americans who experience brain fog, fatigue, and other symptoms after recovering from a coronavirus infection.
There’s basically nothing to show for it.
The National Institutes of Health hasn’t signed up a single patient to test any potential treatments — despite a clear mandate from Congress to study them. And the few trials it is planning have already drawn a firestorm of criticism, especially one intervention that experts and advocates say may actually make some patients’ long Covid symptoms worse.
Instead, the NIH spent the majority of its money on broader, observational research that won’t directly bring relief to patients. But it still hasn’t published any findings from the patients who joined that study, almost two years after it started.
There’s no sense of urgency to do more or to speed things up, either. The agency isn’t asking Congress for any more funding for long Covid research, and STAT and MuckRock obtained documents showing the NIH refuses to use its own money to change course.
“So far, I don’t think we’ve gotten anything for a billion dollars,” said Ezekiel Emanuel, a physician, vice provost for global initiatives, and co-director of the Healthcare Transformation Institute at the University of Pennsylvania. “That is just unacceptable, and it’s a serious dysfunction.”
Eric Topol, the founder and director of the Scripps Research Translational Institute, said he expected the NIH would have launched many large-scale trials by now, and that testing treatments should have been an urgent priority when Congress first gave the agency money in late 2020.
“I don’t know that they’ve contributed anything except more confusion,” Topol said.
Patients and researchers have already raised alarms about the glacial pace of the NIH’s early long Covid efforts. But a new investigation from STAT and the nonprofit news organization MuckRock, based on interviews with nearly two dozen government officials, experts, patients, and advocates, and internal NIH correspondence, letters, and public documents, underscores that the NIH hasn’t picked up the pace — instead, the delays have compounded.
It’s difficult to pinpoint exactly why progress is so stalled, experts and patients involved in the project emphasized, because the NIH has obscured both who is in charge of the long Covid efforts and how it spent the money. The broader Biden administration has also missed opportunities for oversight and accountability of the effort — despite the president’s lofty promises to focus on the disease.
The NIH’s blunders have massive ramifications for the more than 16 million Americans suffering from long Covid, in addition to those with other, similar chronic diseases. As the biggest government-funded study on this topic, the NIH initiative, dubbed RECOVER, sets precedents for future research and clinical guidelines. It will dictate how doctors across the country treat their patients — and, in turn, impact people’s ability to access work accommodations, disability benefits, and more.
“The NIH RECOVER study is pointless,” said Jenn Cole, a long Covid patient based in Brooklyn, N.Y., who wanted to enroll in the study but found the process inaccessible. The research is “a waste of time and resources,” she said, and fails to use patients’ tax dollars for their benefit.
In response to STAT and MuckRock’s questions, the NIH and an institute at Duke University managing the clinical trials defended the initiative, without providing a clear explanation for the delays.
The NIH said it chose to fund a large-scale research program instead of small-scale studies to make sure data and processes could be shared across different groups of patients, adding that clinical trials will be launching soon. In these trials, standardized study designs will allow the agency to test multiple treatments across multiple sites. If there are signals a drug works, the agency said it can pivot to devote more resources there.
A Department of Health and Human Services spokesperson said the agency has made progress over the last year in responding to long Covid, and that there are research efforts underway in addition to the RECOVER program.
“The Administration remains committed to addressing the longer-term impacts of the worst public health crisis in a century,” HHS said.
Long COVID care access challenges: A new paper, published this week in JAMA Network Open, shares the results of a survey by the Urban Institute think tank. The researchers surveyed about 9,500 adults, including 800 with self-reported Long COVID, about their experiences accessing medical care. The long-haulers were more likely to report difficulties with accessing and paying for care, compared to adults who don’t have the condition. To address this issue, the healthcare system needs to develop clinical guidelines for Long COVID, train workers about it, address insurance barriers, and more, the researchers said.
PolyBio announces Long COVID research agenda: Speaking of Long COVID: the PolyBio Research Foundation, a nonprofit devoted to Long COVID, ME/CFS, and other chronic conditions, has announced several research projects that it’s supporting. The projects will evaluate potential biological mechanisms underlying Long COVID symptoms, such as virus persisting in different parts of the body, changes in T cell activity, microclots, and more. PolyBio has a great reputation for pushing ahead post-viral disease research, and I’m looking forward to seeing the results of these studies.
Bivalent boosters hold up against XBB variants: Another new study that caught my attention this week: researchers at the University of North Carolina and North Carolina state health department reported on how well the bivalent, Omicron-specific boosters worked, based on the agency’s surveillance data. The study examined data from September 2022 through February 2023, a period when the BQ and XBB subvariants were dominating coronavirus spread. North Carolina residents who received the bivalent boosters were significantly less likely to experience severe COVID-19 symptoms, the researchers found, but their protection started to wane within a month after receiving the shots.
Resources on indoor air quality in schools: Journalist’s Resource recently updated this list of research and resources for journalists interested in covering indoor air quality in K-12 schools. The update follows a CDC report showing that many public schools across the U.S. have failed to upgrade their ventilation, despite federal funding to do so (which I covered last week). School air quality is a topic that deserves more reporting, especially from local journalists who can dig into how their school districts are doing.
Arizona county starts monitoring for a fungus in wastewater: I’m always on the lookout for new uses of wastewater surveillance, and one promising application could be tracking Candida auris, a fungal pathogen that’s resistant to common drugs and spreads quickly in healthcare settings. The Arizona state health department and a lab at the University of Arizona recently launched a pilot program to track this fungus through Yuma County’s wastewater. Arizona and neighboring southwest states have been a hotbed for C. auris; if this pilot is successful, other states could start similar efforts.
Second Omicron boosters for high-risk adults: The FDA and CDC are planning to authorize a second round of bivalent, Omicron-specific vaccines for high-risk adults, the Washington Post reported this week. This decision will apply to Americans over age 65 and those who have compromised immune systems, with these groups becoming eligible four months after their initial bivalent boosters. It’s unclear exactly when the decision will become official; the FDA and CDC will make authorizations sometime “in the next few weeks,” according to WaPo.
HHS announces (underwhelming) Long COVID progress: This week marks one year since Biden issued a presidential memo kicking off a “whole-of-government response” to Long COVID. The Department of Health and Human Services (HHS) commemorated the occasion with a fact sheet sharing the federal government’s progress so far. Unfortunately, that progress has been fairly minor, mostly consisting of reports and guidance that largely summarize existing government programs or build on existing systems (such as Veterans Affairs hospitals). Many of the Long COVID programs that Biden previously proposed have not received funding from Congress; meanwhile, the National Institutes of Health’s RECOVER initiative, the one program that has been funded, has faced a lot of criticism.
RECOVER PIs recommend action on treatment: Speaking of RECOVER: this week, a group of scientists leading research hubs within the national study called for federal funding that would support treatment. The principal investigators (PIs) of these hubs have developed expertise in Long COVID through recruiting and studying patients, leading them to identify gaps in available medical care for long-haulers. To respond, the PIs recommend that Congress allocate $37.5 million to support Long COVID medical care at the RECOVER research sites. Their proposed budget includes patient outreach, telehealth support, educating healthcare workers on Long COVID, and more.
Ventilation improvements in K-12 schools: The CDC released a new study this week in its Morbidity and Mortality Weekly Report, sharing results of a survey (conducted last fall) including about 8,400 school districts representing 62% of public school students in the U.S. Research company MCH Strategic Data asked the districts about how they’d improved ventilation in their school buildings, along with other COVID-19 safety measures. About half of the districts reported “maintaining continuous airflow in classrooms,” one-third reported HVAC improvements, 28% reported using HEPA filters, and 8% reported using UV disinfectants. The results indicate that many districts have a long way to go in upgrading their indoor air quality.
Flu vs. COVID-19 mortality risk: Ziyad Al-Aly and his colleagues at the VA healthcare system in St. Louis have published another paper analyzing COVID-19 through the VA’s electronic health records. This study, published in JAMA Network, describes the mortality risk of COVID-19 compared to seasonal flu for patients hospitalized during the 2022-2023 winter season. The researchers evaluated about 9,000 COVID-19 patients and 2,400 flu patients, finding that risk of death for COVID-19 patients in the 30 days following hospitalization was about 1.6 times as high as the risk of death for flu patients. Despite great advances in vaccines and treatments, COVID-19 remains more dangerous than other seasonal viruses, the study suggests.
Biobot launches mpox dashboard: This week, leading wastewater surveillance company Biobot Analytics launched a new dashboard displaying its mpox (formerly monkeypox) monitoring. Biobot tests for mpox at hundreds of sewage sites across the U.S., largely through its partnership with the CDC, and will continue this monitoring through at least summer 2023. The new dashboard shows mpox detections nationally over time and monitoring sites by state; it also includes some information on how mpox surveillance differs from COVID-19 surveillance.