Last week, the National Institutes of Health and Duke University announced five Long COVID clinical trials as part of the NIH’s RECOVER initiative. This might sound like an exciting milestone for the millions of people dealing with long-term symptoms—but in fact, experts and long-haulers are disappointed by the trials, I learned when covering this news for MuckRock and STAT News.
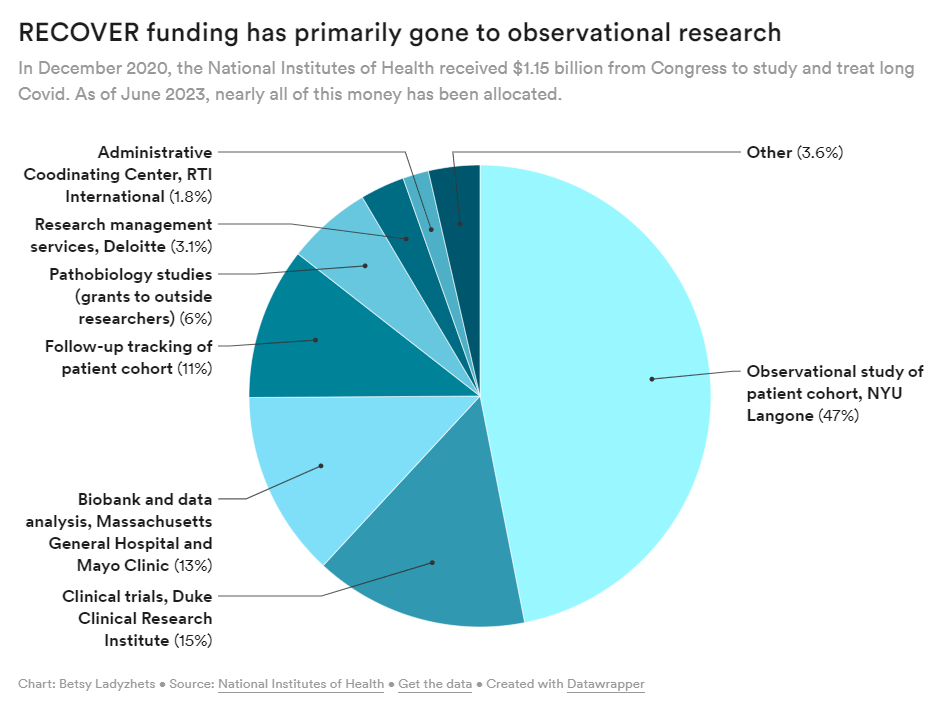
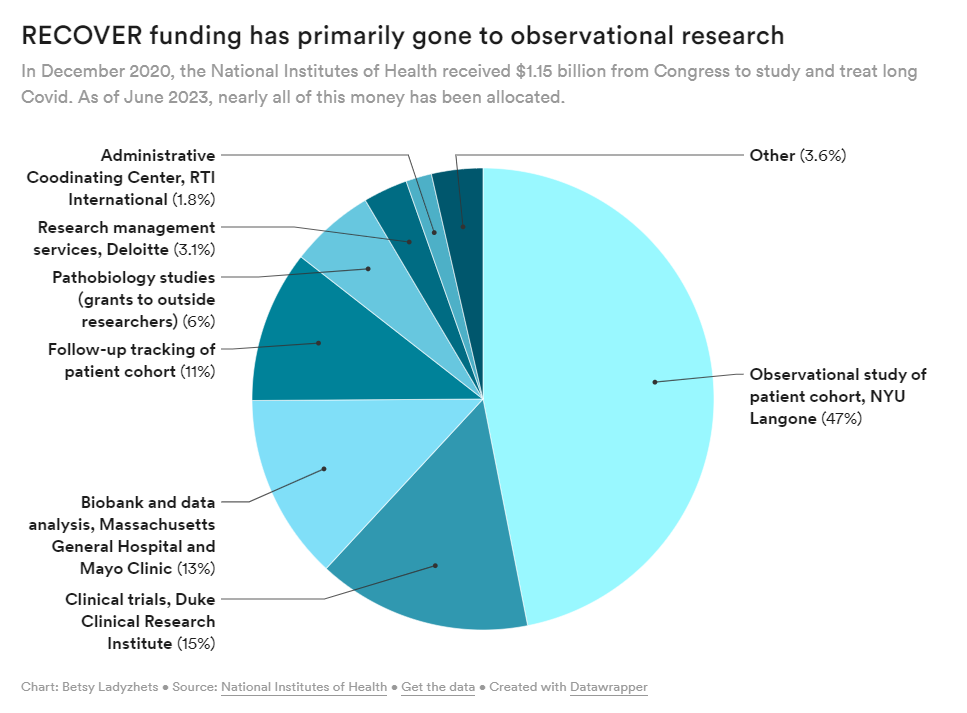
RECOVER is the largest Long COVID research effort in the world; the NIH received $1.15 billion for it, provided by Congress in late 2020. It’s also been plagued by delays and criticisms, as I’ve reported before. As we approach the three-year mark of the initial funding, long-haulers are becoming increasingly frustrated with RECOVER’s lack of results.
My latest story for MuckRock and STAT focuses on the clinical trials, but connects to larger issues with RECOVER and with the federal government’s response to Long COVID in general. Read it on STAT’s site here or on MuckRock’s here.
A few key points from the story:
- RECOVER is only testing a handful of drugs for Long COVID, instead focusing on behavioral interventions that outside experts say are unlikely to address underlying causes of symptoms. There are several lists of potential drugs that should be (and aren’t) prioritized, including one compiled by members of an advisory committee to RECOVER.
- Looking more closely at the drug trials, experts shared concerns about the study designs, suggesting that RECOVER’s choices of controls, outcomes measures, and other aspects of the studies may lead to inaccurate results. For example, dysautonomia expert Lauren Stiles told me that the trial testing drugs for autonomic symptoms may fail to accurately capture whether those drugs help with Long COVID.
- At this point, the NIH has no plans for further Long COVID trials or other research going beyond RECOVER. The initiative has almost fully allocated all of its $1.15 billion in funding, and NIH officials haven’t shared details about how they will continue Long COVID research after this study concludes (though they acknowledge more research will be necessary).
RECOVER failed to put much funding in clinical trials to begin with, focusing instead on observational studies aiming to track Long COVID symptoms over time. While such studies could be valuable for better understanding the condition, RECOVER has largely replicated other research and hasn’t contributed useful, new information to the field, experts have told me. In fact, over 40,000 people have petitioned the NIH to retract RECOVER’s first paper based on its observational research.
Many of RECOVER’s errors, such as choosing the wrong treatments to prioritize and focusing on observational studies over clinical trials, could’ve been avoided if the initiative had listened more to long-haulers and learned from experts in other post-infectious diseases. Long-haulers have done plenty of research themselves in the last three years, ranging from informal tests of different treatments to formal studies conducted by the Patient-Led Research Collaborative; yet these studies have not informed RECOVER.
Plus, scientists with expertise in ME/CFS, dysautonomia, HIV/AIDS, and many other similar diseases could share lessons with RECOVER—but they aren’t leading the initiative. I thought Todd Davenport, a rehabilitation expert at University of the Pacific who’s studied ME/CFS, put it well when he said that RECOVER scientists “have parachuted into post-infectious illness and are now trying these things for the first time, to them. But it’s clear they haven’t done the reading.”
I hope to continue covering RECOVER and other issues with Long COVID research in the U.S. If you have any tips or stories to share with me on this topic, please reach out.

Leave a comment