It’s now been almost two months since the CDC approved third vaccine doses for patients with weakened immune systems—and over two weeks since the agency approved third Pfizer doses for patients with increased breakthrough case risk. Since August 13, the CDC’s dashboard says, about 7.3 million Americans have received a third dose.
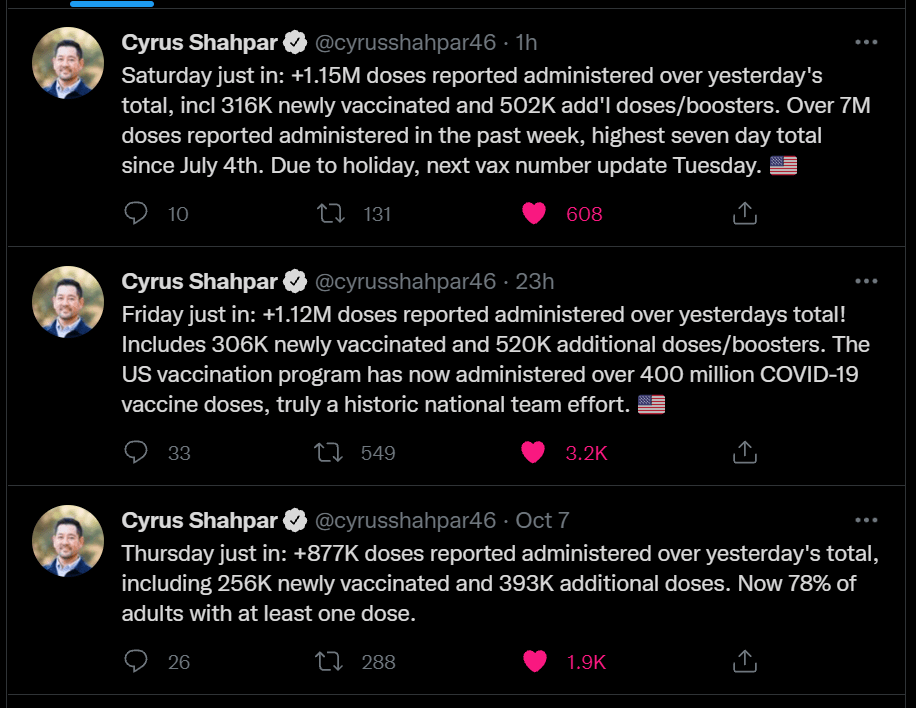
As I mentioned in today’s National Numbers post, these booster shots are obfuscating the country’s vaccination trends. Over one million people have been vaccinated every day for the past week, but roughly half of those people were getting their booster shots.
One might think I am sourcing that daily booster shot number from the CDC dashboard, but no: it comes, as many key COVID-19 data updates do these days, from the Twitter account of White House COVID-19 Data Director Cyrus Shahpar. The CDC has yet to add any booster shot data to its dashboard beyond a total count of doses administered.
Much as I appreciate Shahpar’s daily updates, I would like to see the agency add those daily booster shot counts to its dashboard. And why stop there? The CDC should also provide information on the demographics of those getting booster shots, such as age and race/ethnicity, as well as geographic trends.
Notably, the New York Times has added a booster shot trendline to its vaccination dashboard; see the chart titled “New reported people vaccinated.” As I noted last week, 15 states have added booster shots to their vaccine dashboards and reports as well, including three states that are reporting demographic breakdowns. The CDC is behind the data reporting curve, as usual.
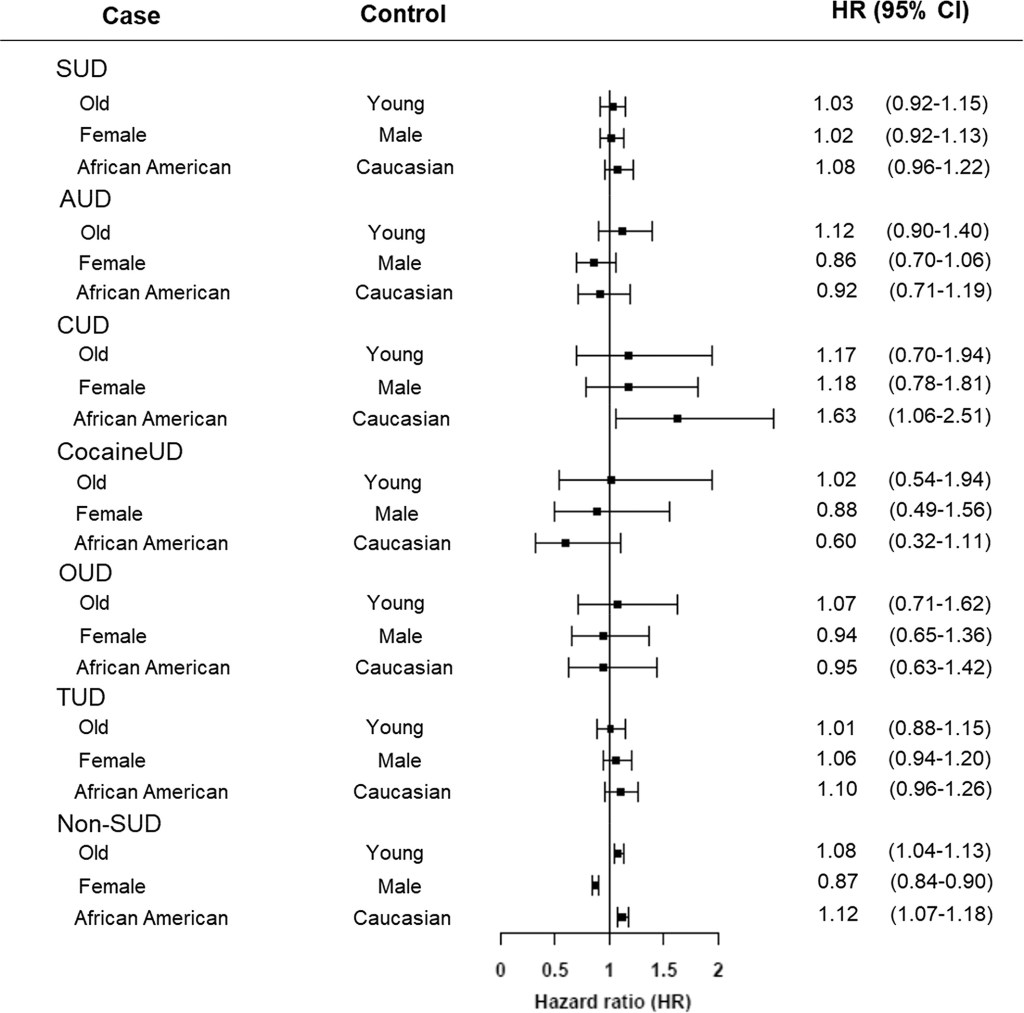
Adults with substance use disorders have an increased risk of breakthrough cases, according to a new study published this week in the journal World Psychiatry. Though the chances of a COVID-19 case after vaccination were very low in this group, these patients’ odds of a breakthrough case were about twice as high as the odds for adults without substance use disorders, researchers from the National Institutes of Health (NIH) found.
This study is the first I’ve seen to delineate breakthrough case risk in a specific, vulnerable population—besides studies demonstrating higher risk for older adults. As I wrote two weeks ago, a lack of specific data on breakthrough cases has contributed to confusion and debate surrounding who should be eligible for a booster shot in the U.S.
So, how did these NIH researchers determine the risk for people with substance abuse? They used anonymous, electronic health records from 63 healthcare organizations across the U.S., compiled in the TriNetX Analytics platform. The study included health records from about 30,000 patients with substance use disorders, compared with 550,000 patients without these disorders. From this large pool of anonymous data, the researchers were able to determine breakthrough case risk among different patient demographics, different substance use disorders, and more.
I got a chance to talk to Dr. Nora Volkow, director of the NIH’s National Institute on Drug Abuse and one of the study’s lead authors, about this methodology, as I covered the paper for DailyMail.com. I asked her if she expected to see similar studies examining breakthrough case risk for other health risks and occupations.
“Absolutely,” Dr. Volkow said. She told me she’s already seen other papers comparing the risk of a breakthrough with Delta compared to other variants, and that more research looking at specific patient groups may be ongoing. Still, using electronic health records has its drawbacks.
“We are basically basing [the analysis] on the electronic health records,” she said. “But it could be useful to complement this with studies that actually are genotyping, getting information about, what was the virus that is responsible?” In other words: health records from hospitals and clinics typically are not matched with genetic sequencing information, making it difficult to link specific variants with breakthrough case risk.
As for why patients struggling with substance abuse have a higher risk of breakthrough COVID-19: Dr. Volkow said this is largely due to socioeconomic factors, such as lack of access to healthcare, low income, and homelessness. Drugs and alcohol are also capable of weakening patients’ immune systems, though; marijuana in particular can hinder immune system regulation.
Last week, one of the reader questions I answered addressed Long COVID, the condition in which people have COVID-related symptoms for weeks or months after their initial coronavirus infection. One reader had asked about monitoring for Long COVID patients (also called long-haulers); I later received another question about the risks of Long COVID after vaccination.
These questions made me realize that I’ve devoted very little space to Long COVID in the COVID-19 Data Dispatch—even though I consider it one of the biggest COVID-19 data gaps in the U.S. Though it’s now been well over a year since the first Long COVID patients were infected, there is still so much we don’t know about the condition.
For example, we don’t know a very rudimentary number: how many people in the U.S. are struggling with Long COVID. We also don’t have a clear, detailed picture of Long COVID symptoms, or how these symptoms arise from a coronavirus infection, or how they impact the daily lives of Long COVID patients.
Why does this massive data gap exist? Long COVID studies are challenged by the lack of standardized patient data in the U.S., making it difficult to identify symptom patterns across large groups of people. We face a similar problem in tracking breakthrough cases, demographic information, and other COVID-19 trends.
Plus, thanks to limited COVID-19 testing in the U.S. throughout the pandemic (and restrictions on who could get tested, back in spring 2020), a lot of Long COVID patients never had a positive test result—making it difficult for them to get a formal diagnosis. And many of the Long COVID studies that have been conducted focus on patients who had a positive COVID-19 test or were hospitalized for the disease, thus narrowing much of our clinical data to a small subset of the actual Long COVID population.
As I noted last week, the National Institutes of Health (NIH) has set up a major research initiative to study Long COVID. This initiative, called RECOVER, is poised to become our best source for Long COVID data in the future. But it’s in early stages right now, beginning to distribute funding to different research groups and recruit Long COVID patients for study. It could be years before we get results.
All of that said, there are still a few things we know about Long COVID based on research thus far. Here’s a roundup of twelve key statistics.
Between 10% and 30% of coronavirus infections lead to Long COVID. This statistic comes from the NIH’s RECOVER Initiative website; it summarizes findings from past studies. Consider: 30% of the 44.2 million Americans with a documented COVID-19 case amounts to 13.3 million people with Long COVID. Even 10% of those 44.2 million would amount to 4.4 million people.
Some studies suggest that as many as one-third of COVID-19 patients may have persistent or returning symptoms. A recent study of electronic health records in the U.S. and U.K., run by scientists at the University of Oxford, suggests that the true share of COVID-19 patients who contract Long COVID is on the higher end of that 10%-30% estimate that the NIH provides. This new study found that 36% of COVID-19 patients (among a sample size of 270,000) had symptoms three and six months after their diagnosis.
Long COVID may manifest with over 100 different potential symptoms. There is a Long COVID paper that I personally come back to, whenever I want to see a clear picture of the many ways that this condition can impact patients. The paper, published in The Lancet in July, reports results from a survey of over 3,000 Long COVID patients conducted by the Patient-Led Research Collaborative. According to this survey, Long COVID patients may suffer from about 100 possible symptoms, including systemic, reproductive, cardiovascular, musculoskeletal, immunologic/autoimmune, head/eyes/ears/nose/throat, pulmonary, gastrointestinal, and dermatologic symptoms.
Long COVID symptoms may change over time. The Patient-Led Research Collaborative survey found that some patients may have changing symptoms, or relapses brought on by different activities. One very common Long COVID symptom is Post-Exertional Malaise, a condition in which patients experience a relapse after physical or mental exertion, even if that exertion is relatively minor.
Some Long COVID patients have been sick for over 18 months. The Patient-Led Research Collaborative survey covers symptoms over a course of seven months, but some Long COVID patients have been suffering for far longer. Some patients who initially contracted the coronavirus in spring 2020, during the first wave in the U.S., have now been sick for 18 months or more.
Many Long COVID patients are unable to work. According to the Patient-Led Research Collaborative survey, almost half of the Long COVID patients who responded (45%) “required a reduced work schedule, compared to pre-illness.” Another 22% were not working at the time of the survey because of Long COVID. Other studies have backed up the findings from this survey. At this point in the pandemic, some Long COVID patients are struggling to receive accommodations from their employers, even though the condition is recognized as a disability at the federal level.
Long COVID can occur at all age ranges, but is documented most in younger and middle-age adults. Among respondents to the Patient-Led Research Collaborative survey, about 24% were in their thirties, 31% in their forties, and 25% in their fifties—though patients ranged in ages from 18 to over 80. This survey and others have also found that Long COVID seems to be more common for women; this pattern aligns with other post-infectious conditions, like chronic fatigue syndrome and chronic Lyme disease.
Long COVID may lead to long-term neurological issues. This past summer at the Alzheimer’s Association International Conference, a few researchers presented findings on Long COVID and Alzheimer’s. Brain scans of COVID-19 patients, along with observations of patients’ prolonged symptoms, suggest that adults who suffer from Long COVID may have an increased risk of Alzheimer’s later in life. Severe COVID-19 patients in their sixties and seventies are already starting to see symptoms matching early-onset Alzheimer’s, one researcher told NPR.
Autoimmune response may be one cause for Long COVID symptoms. While scientists are still working to determine exactly how a coronavirus infection may lead to numerous symptoms, research thus far suggests that overreaction of the immune system could be a major player. Some clinicians who work with Long COVID patients have developed treatments based on dysautonomia, medical conditions caused by immune and autonomic nervous system issues.
About 5,200 children in the U.S. have been diagnosed with MIS-C, and 46 have died. MIS-C stands for Multisystem Inflammatory Syndrome in Children. The condition follows a COVID-19 infection in rare cases, leading to inflammation of different parts of the body. While this condition is not directly comparable to Long COVID, scientists think it may have similar causes. The condition has disproportionately impacted children of color in the U.S.: out of 5,200 cases, 61% are Black or Hispanic/Latino.
The risk of Long COVID is dramatically lower after a breakthrough infection, even if you contract the coronavirus. A recent study published in The Lancet found that vaccinated patients who later had a breakthrough COVID-19 case were about half as likely to report symptoms after four weeks, compared to unvaccinated patients who had a non-breakthrough COVID-19 case. Plus, vaccinated people are already far less likely to contract the coronavirus in the first place, because vaccination reduces risk of infection. Commenting on the study, NIH Director Dr. Francis Collins called it “encouraging news,” though he cautioned that more research is needed on this topic.
Vaccination may help alleviate COVID-19 symptoms for Long COVID patients. In addition to reducing one’s risk of developing Long COVID, vaccination can alleviate symptoms for Long COVID patients. A recent preprint, posted online at the end of September, found that Long COVID patients who got vaccinated were about twice as likely to completely recover, compared to unvaccinated patients. “Overall, this study adds to growing evidence that vaccines can improve symptoms and lessen the disease impact in Long COVID,” wrote Long COVID researcher Dr. Akiko Iwasaki, sharing the study on Twitter.
To me, these Long COVID statistics—along with everything we still don’t know about the condition—provide a strong argument for vaccination. Long COVID can impact people who were young and healthy before they were infected, completely messing up their lives for months or even years. It surprises me that public health and political leaders don’t discuss this condition more when they tell people to get vaccinated.
As for continued research: the NIH’s RECOVER Initiative has received over $1 billion in funding from Congress, and it’s just getting started on setting up studies. If you’re interested in learning more about the research—or signing up to participate in a RECOVER study—you can sign up for email alerts on the NIH website.
The Delta surge is waning. Will this be the last big surge in the U.S., or will we see more? This question and more, answered below; chart from the CDC.
Last week, I asked readers to fill out a survey designed to help me reflect on the COVID-19 Data Dispatch’s future. Though the Delta surge—and the pandemic as a whole—is far from over, I’m considering how this publication may evolve in a “post-COVID” era. Specifically, I’m thinking about how to continue serving readers and other journalists as we prepare for future public health crises.
Thank you to everyone who’s filled out the survey so far! I really appreciate all of your feedback. If you haven’t filled it out yet, you can do so here.
Besides some broader questions about the CDD’s format and topics we may explore in the future, the survey asked readers to submit questions that they have about COVID-19 in the U.S. right now. In the absence of other major headlines this week, I’m devoting this week’s issue to answering a few of those questions.
Should I get a booster shot? If so, should it be a different one from the first vaccine I got? When will my kids (5-11) likely be eligible?
I am not a doctor, and I’m definitely not qualified to give medical advice. So, the main thing I will say here is: identify a doctor that you trust, and talk to them about booster shots. I understand that a lot of Americans don’t have a primary care provider or other ways to easily access medical advice, though, so I will offer some more thoughts here.
As I wrote last week, we do not have a lot of data on who’s most vulnerable to breakthrough COVID-19 cases. We do know that seniors are more vulnerable—this is one point where most experts agree. We know that adults with the same health conditions that make them more likely to have a severe COVID-19 case without a vaccine (autoimmune conditions, diabetes, kidney disease, etc.) are also more vulnerable to breakthrough cases, though we don’t have as much data here. And we know that vaccinated adults working in higher-risk locations like hospitals, nursing homes, and prisons are more likely to encounter the coronavirus, even if they may not necessarily be more likely to have a severe breakthrough case.
The FDA and CDC’s booster shot guidance is intentionally broad, allowing many Americans to receive a booster even if it is not necessarily needed. So, consider: what benefits would a booster shot bring you? Are you a senior or someone with a health condition that makes you more likely to have a severe COVID-19 case? Do you want to protect the people you work or live with from potentially encountering the coronavirus?
If you answered “yes” to one of those questions, a booster shot may make sense for you. And, while you may be angry about global vaccine inequity, one individual refusal of a booster shot would not have a significant impact on the situation. Rather, many vaccine doses in the U.S. may go to waste if not used for boosters. But again: talk to your doctor, if you’re able to, about this decision.
Currently, Pfizer booster shots are available for people who previously got vaccinated with Pfizer. The FDA’s vaccine advisory committee is meeting soon to discuss Moderna and Johnson & Johnson boosters: they’ll discuss Moderna on October 14 and J&J on October 15. Vaccine approval in the U.S. depends upon data submission from vaccine manufacturers—and vaccine manufacturers have not been studying mix-and-match booster regimens—so coming approvals will likely require Americans to get a booster of the same vaccine that they received initially. We will likely see more discussion of mix-and-match vaccinations in the future, though, as more outside studies are completed.
As for when your kids will likely be eligible: FDA’s advisory committee is meeting to discuss Pfizer shots for kids ages 5 through 11 on October 26. If that meeting—and a subsequent CDC meeting—goes well, kids may be able to get vaccinated within a week of that meeting. (Potentially even on Halloween!)
Why don’t people get vaccinated and how can we make them?
I got a couple of questions along these lines, asking about vaccination motivations. To answer, I’m turning to KFF’s COVID-19 Vaccine Monitor, a source of survey data on vaccination that I (and many other journalists) have relied on since early 2021.
KFF released the latest round of data from its vaccine monitor this week. Here are a few key takeaways:
The racial gap in vaccinations appears to be closing. KFF found that 71% of white adults have been vaccinated, compared to 70% of Black adults and 73% of Hispanic adults. Data from the CDC and Bloomberg (compiling data from states) similarly show this gap closing, though some parts of the country are more equitably vaccinated than others.
A massive partisan gap in vaccinations remains. According to KFF, 90% of Democrats are vaccinated compared to just 58% of Republicans. This demonstrates the pervasiveness of anti-vaccine misinformation and political rhetoric among conservatives.
Rural and younger uninsured Americans also have low vaccination rates (62% and 54%, respectively). Both rural and uninsured people have been neglected by the U.S. healthcare system and face access barriers; for more on this topic, I recommend this Undark article by Timothy Delizza.
Delta was a big vaccination motivator. KFF specifically asked people who had gotten their shots after June 1 why they chose to get vaccinated. The most popular reasons were, in order: the increase in cases due to Delta (39%), concern about reports of local hospitals and ICUs filling with COVID-19 patients (38%), and knowing someone who got seriously ill or died from COVID-19 (36%).
Mandates and social pressures were also vaccination motivators. 35% of KFF’s recently vaccinated survey respondents said that a big reason for their choice was a desire to participate in activities that require vaccination, like going to the gym, a big event, or traveling. 19% cited an employer requirement and 19% cited social pressure from family and friends.
The second part of this question, “how can we make them?”, reflects a dangerous attitude that has permeated vaccine conversations in recent months. Yes, it’s understandable to be frustrated with the Americans who have refused vaccination. But we can’t “make” the unvaccinated do anything, and such a forceful attitude may put off people who still have questions about the vaccines or who have faced discrimination in the healthcare system. To increase vaccinations among people who are still hesitant, it’s important to remain open-minded, not condescending. For more: read Ed Yong’s interview with Dr. Rhea Boyd.
That said, we’re now getting a sense of which strategies can increase vaccination: employer mandates, vaccination requirements for public life, and personal experience with the coronavirus. As the Delta surge wanes, it will take more vaccination requirements and careful, open-minded conversations to continue motivating people to get their shots.
What are some things I might say to convince people of Delta’s severity and the need to not relax on masking, distancing, etc?
To answer this, I’ll refer you to the article I wrote about Delta on August 1, as the findings that I discuss there have been backed up by further research.
Personally, there are two statistics that I use to express Delta’s dangers to people:
Delta causes a viral load 1,000 times higher than the original coronavirus strain. This number comes from a study in Guangzhou, China, posted as a preprint in late July. While viral load does not correspond precisely to infectiousness (there are other viral and immune system factors at play), I find that this “1,000 times higher” statistic is a good way to convey just how contagious Delta is, compared to past variants.
An interaction of one second is enough time for Delta to spread from one person to another. Remember the 15-minute rule? In spring 2020, being indoors with someone, unmasked, for 15 minutes or more was considered “close contact.” Delta’s increased transmissibility means that an interaction of one second is now enough to be a “close contact.” The risk is lower if you’re vaccinated, but still—Delta is capable of spreading very quickly in enclosed spaces.
You may also find it helpful to discuss rising numbers of breakthrough cases in the U.S. While vaccinated people continue to be incredibly well protected against severe disease and death caused by Delta, the vaccines are not as protective against coronavirus infection and transmission. (They are protective to some degree, though! Notably, coronavirus infections in vaccinated people tend to be significantly shorter than they are in the unvaccinated, since immune systems can quickly respond to the threat.)
It’s true that rising breakthrough case numbers are, in a way, expected—as more people get vaccinated, breakthrough cases will naturally become more common, because the virus has fewer and fewer unvaccinated people to infect. But considering the risks of spreading the coronavirus to others, plus the risks of Long COVID from a breakthrough case… I personally don’t want a breakthrough case, and so I continue masking up and following other safety protocols.
What monitoring do we have in place for COVID “longhaulers” and their symptoms/health implications?
This is a great question, and one I wish I could answer in more detail. Unlike COVID-19 cases, hospitalizations, and other major metrics, we do not have a comprehensive national monitoring system to tell us how many people are facing long-term symptoms from a coronavirus infection, much less how they’re faring. I consider this one of the country’s biggest COVID-19 data gaps, leaving us relatively unprepared to help the thousands, if not millions, of people left newly disabled by the pandemic.
In February, the National Institutes of Health (NIH) announced a major research initiative to study Long COVID. Congress has provided over $1 billion in funding for the research. This initiative will likely be our best source for Long COVID information in the future, but it’s still in early stages right now. Just two weeks ago, the NIH awarded a large share of its funding to New York University’s Langone Medical Center; NYU is now setting up long-term studies and distributing funding to other research institutions.
As I wrote in the September 19 issue, the NIH’s RECOVER website currently reports that between 10% and 30% of people infected with the coronavirus will go on to develop Long COVID; hopefully research at NYU and elsewhere will lead to some more precise numbers.
While we wait for the NIH research to progress, I personally find the Patient-Led Research Collaborative (PLRC) to be a great source for Long COVID research and data. The PLRC consists of Long COVID patients who research their own condition; it was founded out of Body Politic’s Long COVID support group. This group produced one of the most comprehensive papers on Long COVID to date, based on an international survey including thousands of patients, and has more research currently ongoing.
If you have the means to support Long COVID patients—many of whom are unable to work and facing homelessness—please see the responses to this tweet by PLRC researcher Hannah Davis:
As others have mentioned, people with Long COVID are unable to work & are becoming homeless.
If you have #LongCovid & are struggling, drop your venmo/cashapp/paypal/etc in this thread & I'll retweet.
If you have $ to spare, please support patients in this thread.
Why is the CDC not doing comprehensive high volumes of sequencing on all breakthrough cases at the very least?
I wish I knew! As I wrote last week (and in several other past issues), the lack of comprehensive breakthrough case data in the U.S. has contributed to a lack of clarity on booster shots, as well as a lack of preparedness for the next variants that may become threats after Delta. The CDC’s inability to track and sequence all breakthrough cases—not just the severe ones—is dangerous.
That said, it is very difficult to track breakthrough cases in a country like the U.S. Consider: the U.S. does not have a comprehensive, national electronic records system for patients admitted to hospitals, much less those who receive COVID-19 tests and other care at outpatient clinics. This lack of comprehensive records makes it difficult to match people who’ve been vaccinated with those who have received a positive COVID-19 test. Thousands, if not millions of Americans are now relying on rapid tests for their personal COVID-19 information—and most rapid tests don’t get entered into the public health records system at all.
Plus, local public health departments are chronically underfunded, understaffed, and burned out after almost two years of working in a pandemic; they have little bandwidth to track breakthrough cases. Many Americans refuse to participate in contact tracing, which hinders the public health system’s ability to collect key information about their cases. And there are other logistical challenges around genomic sequencing; despite new investments in this area, many parts of the country don’t have sequencing capacity, or the information infrastructure needed to send sequencing results to the CDC.
So, if the CDC were tracking non-severe breakthrough cases, they’d likely miss a lot of the cases. But that doesn’t mean they shouldn’t be trying, in my opinion.
How safe is it to visit my family for the holidays?
This is another place where I don’t feel qualified to give advice, but I can offer some thoughts. If I were you, I would think about the different ways in which holiday travel might pose risk to me and to the people at the other end of my trip. I would consider:
Quarantining beforehand. Do your occupation and living circumstances allow you to quarantine for a week, or at least limit your exposure to settings where you might be at risk of catching the coronavirus, before you travel? Can you get a test before traveling?
Types of travel. Can you make the trip in a car or on public transportation, or do you need to fly? If you need to fly, can you select an airline that has stricter COVID-19 safety requirements? (United recently reported that over 96% of its employees are now vaccinated, for example.) Can you wear a high-quality mask for the flight?
Quarantining and/or testing upon arrival. Can you spend a couple of days in quarantine once you get to your destination? Would you have access to testing (with results in under 24 hours) upon your arrival, or would you be able to bring rapid tests with you?
Who you’re spending time with. Among the family you’d be visiting, is everyone vaccinated (besides young children)? If anyone is not vaccinated, could your potential travel be a motivator to help convince them to get vaccinated? Does the group include seniors or people with health conditions that put them at high risk for COVID-19, and if so, can they get booster shots?
Activities that you do at your destination. Would you be able to have large gatherings outside, or in a well-ventilated space? What else can you do to reduce the risk of these activities?
Like other activities, travel can be relatively safe or fairly dangerous depending on the precautions that you’re able to take, and depending on COVID-19 case rates where you live and at your destination. And, like other activities, your choice to travel or not travel depends a lot on your personal risk tolerance. Nothing is zero-risk right now; each person has a threshold that determines what level of COVID-19 risk they are and are not comfortable taking. Through some self-reflection, you can determine if travel is above or below your risk threshold.
Why are policies so different now than they were at this time last year?
Public health tends to go through cycles of “panic” and “neglect.” Ed Yong’s latest feature goes into the history of this phenomenon:
Almost 20 years ago, the historians of medicine Elizabeth Fee and Theodore Brown lamented that the U.S. had “failed to sustain progress in any coherent manner” in its capacity to handle infectious diseases. With every new pathogen—cholera in the 1830s, HIV in the 1980s—Americans rediscover the weaknesses in the country’s health system, briefly attempt to address the problem, and then “let our interest lapse when the immediate crisis seems to be over,” Fee and Brown wrote. The result is a Sisyphean cycle of panic and neglect that is now spinning in its third century. Progress is always undone; promise, always unfulfilled. Fee died in 2018, two years before SARS-CoV-2 arose. But in documenting America’s past, she foresaw its pandemic present—and its likely future.
During the COVID-19 pandemic, the U.S. took a nosedive into the “neglect” cycle before we were even finished with the “panic” cycle. Congress has already slashed its funding for future pandemic preparedness, while state and local governments across the country restrict the powers of public health officials. As a result, we’re seeing an “everyone for themselves” attitude at a time when we should be seeing new mask mandates, restrictions on public activities, and other safety measures.
Basically, America decided the pandemic was over and acted accordingly—and if you get COVID-19 now, it’s “your fault for not being vaccinated.” This phenomenon has been especially pronounced in rural areas, which struggled a lot (but saw few cases) during spring 2020 lockdowns and are extremely hesitant to do anything approaching a “lockdown” again.
We need an attitude shift—and more investment in public health—to actually end this pandemic and prepare for the next health crisis. Yong’s feature goes into this in more detail; definitely give that a read if you haven’t yet.
When is this going to be over?!?
Unfortunately, this is very hard to predict—even for the expert epidemiologists and computational biologists who make the models. Check out the CDC’s compilation of COVID-19 case models: most of them agree that cases will keep going down in the coming weeks, but they’re kind of all over the place.
Last week, I summarized two stories—from The Atlantic and STAT News—that discuss the coming winter, and kind of get at this question. It’s possible that cases keep declining from their present numbers, and that the Delta surge we just faced is the last major surge in the U.S. It’s also possible that a new variant arises out of Delta and sends us into yet another new surge. If that happens, more people will be protected by vaccination and prior infection, but healthcare systems could come under strain once again.
As long as the coronavirus continues spreading somewhere in the world, it will continue to pose risk to everyone—able to cause new outbreaks and mutate into new variants. This will continue until the vast majority of the world is vaccinated. And then, at some point, the coronavirus will probably become endemic, meaning it persists in the population at some kind of “acceptable” threshold. Just like the flu.
Dr. Ellie Murray, epidemiologist at Boston University’s School of Public Health, explained how a pandemic becomes endemic in a recent Twitter thread:
Everyone keeps talking about covid becoming endemic, but as I listen to the conversation, it’s becoming more & more clear to me that very few of you know what “endemic” means.
Dr. Murray points out that, even when a disease reaches endemic status, tons of scientists and public health workers will still continue to monitor it. This is the case for the flu—think about all of the effort that goes into a given year’s flu shot!—and it will likely be the case for COVID-19.
In short, public health leaders need to figure out what level of COVID-19 transmission is “acceptable” and how we will continue to monitor it. This needs to happen at both U.S. and global levels. And, thanks to our vaccine-rich status, it’ll likely happen in the U.S. long before it happens globally.
So, yes, our only viable choice left is covid becoming endemic. It didn’t have to be this way, but our leaders MADE a choice.
And now they need to make another choice: They need to choose an “acceptable” level of COVID death & disease.
This week, two of the outlets that I consider to be among the most reliable COVID-19 news sources published stories on our coming pandemic winter. Obviously, you should read both pieces in full, but here are my takeaways.
This piece focuses on the changing role of vaccination in protecting the U.S. from COVID-19. After a few months of encouraging data, suggesting that vaccines could protect us against coronavirus infection and transmission, we are now back to using COVID-19 vaccines for their initial purpose: preventing severe disease and death. As we see higher numbers of breakthrough cases, we can take comfort in the fact that those cases will rarely lead to hospitalization or death. (Though the risk of Long COVID after vaccination is less known.)
The Atlantic’s article also explains who is now most at risk of COVID-19, and how that risk may shift in the coming months. Right now, unvaccinated children face high risk, especially if they live in communities where most of the adults aren’t vaccinated. But that won’t always be the case:
Relative risk will keep shifting, even if the virus somehow stops mutating and becomes a static threat. (It won’t.) Our immune systems’ memories of the coronavirus, for instance, could wane—possibly over the course of years, if immunization against similar viruses is a guide. People who are currently fully vaccinated may eventually need boosters. Infants who have never encountered the coronavirus will be born into the population, while people with immunity die. Even the vaccinated won’t all look the same: Some, including people who are moderately or severely immunocompromised, might never respond to the shots as well as others.
At the end of the article, the writers touch on variants. Delta is now the world’s major concern, but future variants might develop new mutations and pose new dangers. Yet the writers say that any variant “can be stopped through the combined measures of vaccines, masks, distancing, and other measures that cut the conduits they need to travel.”
The second “pandemic winter” story comes from ace STAT News reporter Helen Branswell. Branswell goes into more detail about potential variant scenarios, outlining what Delta may do and how other mutations may arise as the weather gets colder.
Some modeling efforts suggest that COVID-19 case numbers may stay low once the Delta wave ends, Branswell reports, because the majority of Americans are now fully vaccinated or have some immunity from a prior infection. But if another dangerous variant comes along, we could be in trouble. Still, if cases go up again, we won’t see as many hospitalizations or deaths as we did last winter, thanks to the vaccines.
I personally take comfort in this quotation from computational biologist Trevor Bedford:
“It is likely that we’ll see some wave,” Bedford said. “I would like to think it’s very unlikely to be as big as it was last year.”
Because Delta is causing the vast majority of the world’s COVID-19 cases right now, Branswell reports, future variants would likely arise from Delta. That could mean even more transmissibility or challenges to the human immune system. There’s a lot of uncertainty involved in trying to predict mutations, though. Branswell points out:
Early in the pandemic, coronavirus experts confidently opined that this family of viruses mutates far more slowly than, say, influenza, and major changes weren’t likely to undermine efforts to control SARS-2. But no one alive had watched a new coronavirus cycle its way through hundreds of millions of people before.
Branswell’s story also spends time explaining the potential pressures that COVID-19 could put on the healthcare system if combined with flu or other respiratory viruses. Healthcare workers may need to distinguish COVID-19 cases from flu cases, then treat both with similar equipment.
The story makes a pretty good argument for getting your flu shot now, if it’s available to you. I got mine last week.
had the fun experience today of getting my flu shot directly into my tattoo. (get your flu shots, everyone!!) pic.twitter.com/W7K6DeJ9so
This past Thursday, an advisory committee to the CDC recommended that booster doses of the Pfizer vaccine be authorized for seniors and individuals with high-risk health conditions. The committee’s recommendation, notably, did not include individuals who worked in high-risk settings, such as healthcare workers—whom the FDA had included in its own Emergency Use Authorization, following an FDA advisory committee meeting last week.
Then, very early on Friday morning, CDC Director Rochelle Walensky announced that she was overruling the advisory committee—but agreeing with the FDA. Americans who work in high-risk settings can get booster shots. (At least, they can get booster shots if they previously received two doses of Pfizer’s vaccine.)
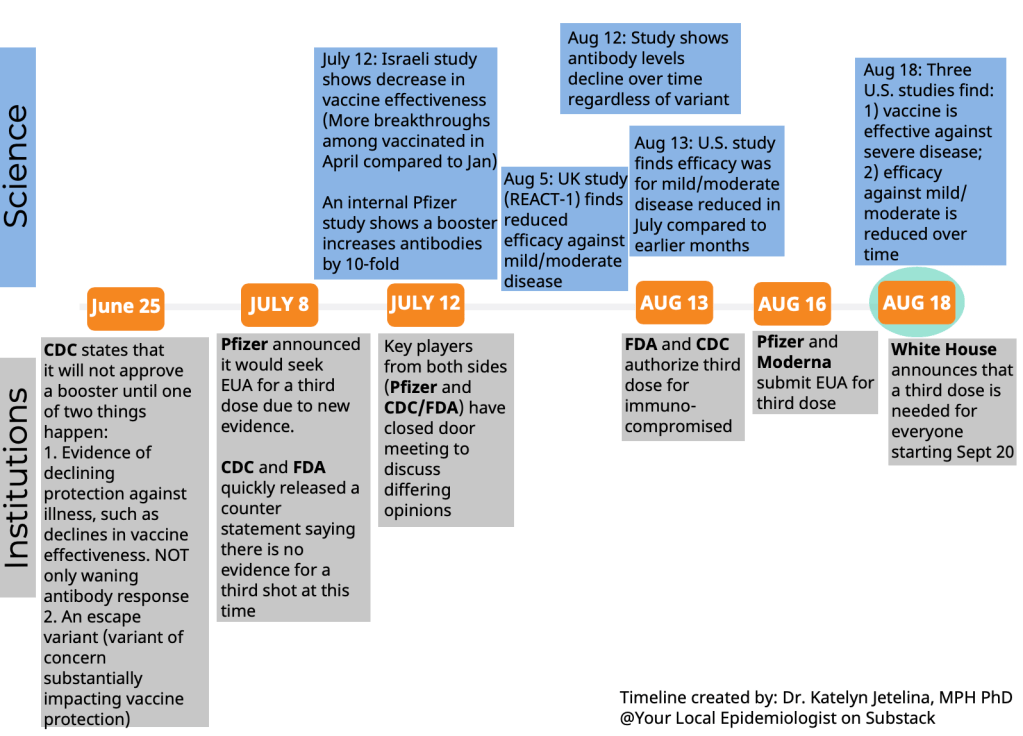
This week’s developments have been just the latest in a rather confusing booster shot timeline:
The US timeline for boosters. You'd have to work really hard to mess this up this badly and engender this much confusion. 😬 pic.twitter.com/KHNWEQJyLg
Why has this process been so confusing? Why don’t the experts agree on whether booster shots are necessary, or on who should get these extra shots? Part of the problem, of course, is that the Biden administration announced booster shots were coming in August, before the scientific agencies had a chance to review all the relevant evidence.
But from my (data journalist’s) perspective, the booster shot confusion largely stems from a lack of data on breakthrough cases.
Let’s go back in time—back four months, or about four years in pandemic time. In May, the CDC announced a major change in its tracking of breakthrough cases. The agency had previously investigated and published data on all breakthrough cases, including those that were mild. But starting in May, the CDC was only investigating and publishing data on those severe breakthrough cases, i.e. those which led to hospitalization or death.
At the time, I called this a lazy choice that would hinder the U.S.’s ability to track how well the vaccines are working. I continued to criticize this move, when researchers and journalists attempted to do the CDC’s job—but were unable to provide data as comprehensive as what the CDC might make available.
Think about what might have been possible if the CDC had continued tracking all breakthrough cases, or had even stepped up its investigation of these cases through increased testing and genomic sequencing. Imagine if we had data showing breakthrough cases by age group, by high-risk health condition, or by occupational setting—all broken out by their severity. What if we could compare the risk of someone with diabetes getting a breakthrough case, to the risk of someone who works in an elementary school?
If we had this kind of data, the FDA and CDC advisory committees would have information that they could use to determine the potential benefits of booster shots for specific subsets of the U.S. population. Instead, these committees had to make guesses. Their guesses didn’t come out of nowhere; they had scientific studies to review, data from Pfizer, and information from Israel and the U.K., two countries with better public health data systems than the U.S. But still, these guesses were much less informed than they might have been if the CDC had tracked breakthrough cases and outbreaks in a more comprehensive manner.
From that perspective, I can’t really fault the CDC and the FDA for casting their guesses with a fairly wide net—including the majority of Americans who received Pfizer shots in their authorization. There’s also a logistical component here; the U.S. has a lot of doses that are currently going unused (thanks to vaccine hesitancy), and may be wasted if they aren’t used as boosters.
But it is worth emphasizing how a lack of data on breakthrough cases has driven a booster shot decision based on fear of who might be at risk, rather than on hard evidence about who is actually at risk. Other than seniors; the risk for that group is fairly clear.
The booster shot decision casts a wide net. But at the same time, it creates a narrow band of booster eligibility: only people who got two doses of Pfizer earlier in 2021 are now eligible for a Pfizer booster. Recipients of the Moderna and Johnson & Johnson vaccines are still left in the dark, even though some of those people may need a booster more than many people who are now eligible for additional Pfizer shots. (Compare, say, a 25-year-old teacher who got Pfizer to a 80-year-old, living in a nursing home, with multiple health conditions who got Moderna.)
That Pfizer-only restriction also stems from a data issue. The federal government’s current model for approving vaccines is very specific: first a pharmaceutical company submits its data to the FDA, then the FDA reviews these data, then the FDA makes a decision, then the CDC reviews the data, then the CDC makes a decision.
By starting with the pharmaceutical company, the decision-making process is restricted to options presented by that company. As a result, we aren’t seeing much data on mixing-and-matching different vaccines, which likely wouldn’t be profitable for vaccine manufacturers. (Even though immunological evidence suggests that this could be a useful strategy, especially for Johnson & Johnson recipients.)
In short, the FDA and CDC’s booster shot decision is essentially both ahead of evidence on who may benefit most from a booster, but behind evidence for non-Pfizer vaccine recipients. It’s kind-of a mess.
I also can’t end this post without acknowledging that we need to vaccinate the whole world, not just the U.S. Global vaccination went largely undiscussed at the FDA and CDC meetings, even though it is a top concern for many public health experts outside these agencies.
48. An observation: There was zero discussion today about the global vaccine supply situation or how use of boosters in the United States might affect getting first doses to billions around the world. Not. One. Word. #ACIP
At an international summit this week, President Biden announced more U.S. donations to the global vaccine effort. His administration seems convinced that the U.S. can manage both boosters at home and donations abroad. But the White House only has so much political capital to spend. And right now, it’s pretty clearly getting spent on boosters, rather than, say, incentivizing the vaccine manufacturers to share their technology with the Global South.
Among the top vaccine donors: -13% of vaccines donated by US have been delivered – 49% of China's donations delivered – 34% of Japan's donations delivered – 4% of Germany's delivered – 8% of UK's delivered
This past Friday, the Food and Drug Administration (FDA)’s vaccine advisory committee voted to recommend booster shots of the Pfizer-BioNTech vaccine for all Americans over age 65 and those who are particularly vulnerable to the virus, due to their health conditions and/or work environments. This was a notable recommendation because it went against the FDA’s ask: booster shots for everyone over the age of 16.
Let’s walk through the data behind this decision.
How is the current two-dose vaccine regimen faring against severe COVID-19 disease?
Before we get into any numbers, it’s important to remember the initial goal of the COVID-19 vaccines: protect people against severe disease, hospitalization, and death, basically reducing the coronavirus’ power to cause deadly harm.
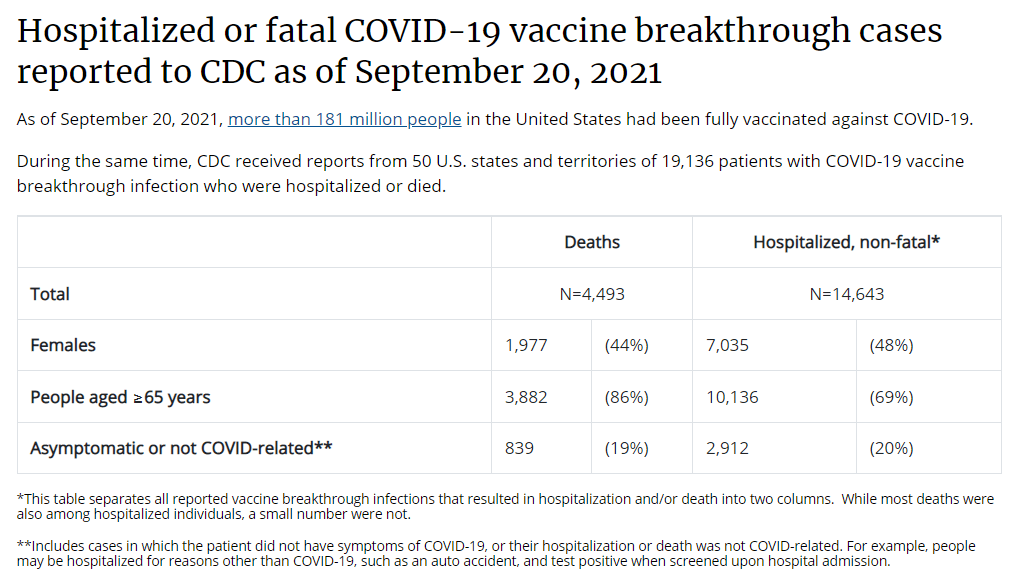
On this front, all of the vaccines are performing well. Numerous papers cited during the advisory meeting, as well as the U.S.’s breakthrough case data, suggest that vaccination protects against severe COVID-19 disease for the vast majority of recipients. Among over 178 million people who had been fully vaccinated in the U.S. by mid-September, just 3,000 have died following a positive COVID-19 test. Those 3,000 deaths account for just about 1% of all COVID-19 deaths in the U.S. since January 2021.
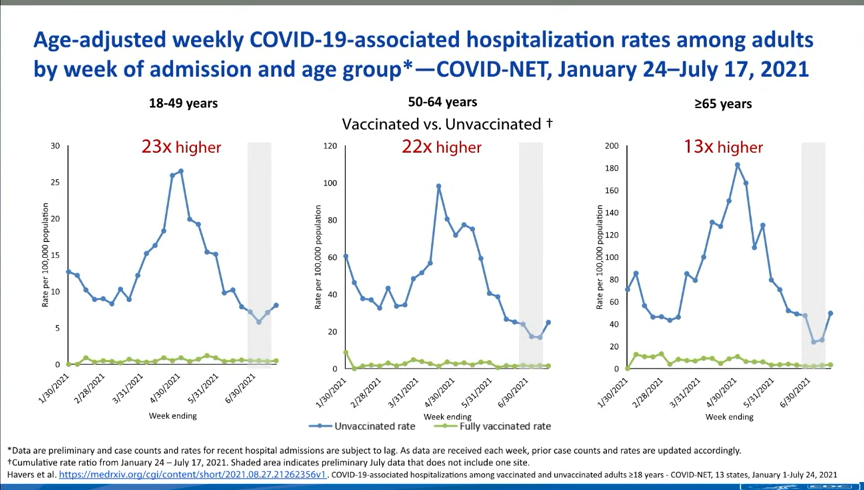
The numbers get a bit more complex, however, when you look at older adults and other vulnerable populations. Those who were more vulnerable to a severe COVID-19 case in the first place are also more vulnerable to having a severe breakthrough case, if they encounter the virus after vaccination. One chart, presented at the FDA meeting, provides a picture of this trend. From late January to mid-July, 2021, the hospitalization rate among younger adults (ages 18-49) was 23 times higher for the unvaccinated than for the vaccinated. For seniors (over age 65), however, the rate was 13 times higher for the unvaccinated.
Seniors are more likely to experience a severe breakthrough case than younger adults, CDC data suggest.
How is that current regimen faring against coronavirus infection?
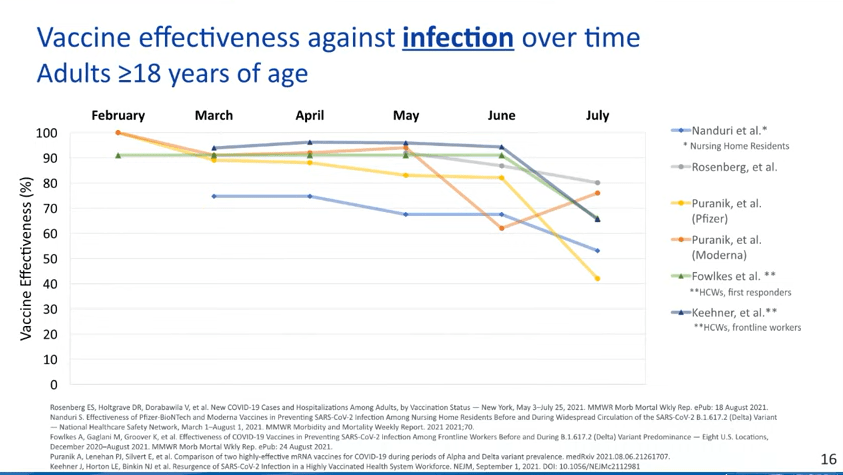
This is where we see a bigger drop in efficacy. Multiple studies point to the Pfizer and Moderna vaccines becoming less capable of protecting recipients against infection, over time; in other words, if you got your two shots in April 2021, you’re more likely to get a positive test result now, in September, than you were in May. (Though your case will likely be mild or asymptomatic!)
While the vaccines are still highly effective against severe disease, their effectiveness against coronavirus infection appears to be waning.
We can also see this in breakthrough case numbers when we look at all infections, as opposed to only those cases that lead to severe disease or death. This type of analysis is difficult to do in the U.S., as the CDC is only systematically tracking those severe cases, but we can see patterns in the data from local jurisdictions that are reporting their breakthrough cases more comprehensively.
For example, let’s look at Washington, DC, which reports breakthrough cases in extensive detail:
Washington, D.C. is seeing many more breakthrough cases now than it was earlier in 2021.
During the week of March 8, DC reported 14 breakthrough cases. The district reported about 800 cases overall that week, meaning that breakthroughs accounted for 2% of all cases.
During the week of August 23, however, the district reported almost 500 breakthrough cases. In that week, the district reported about 1,400 cases overall—meaning that breakthrough cases have jumped from 2% of all weekly DC cases to 35% of all weekly DC cases.
DC also reports a breakdown of breakthrough cases according to the time it’s been since residents were fully vaccinated. This reveals that most breakthroughs occur at least two months after an individual completed their dose series, with the highest number of breakthroughs in people who’d been vaccinated three to four months ago. We can assume that similar patterns are occurring elsewhere in the country.
It’s also worth noting that we don’t have a great sense of how well the vaccines protect against Long COVID—though data thus far suggest that post-vaccination Long COVID cases are much rarer than non-breakthrough cases.
Why are the vaccines appearing to lose their effectiveness?
This was a big point of discussion for the FDA advisory committee. Are the Pfizer and Moderna vaccines appearing to lose their ability to protect us against coronavirus infection because Delta has a special ability to evade the vaccines or because the vaccines become less effective over time?
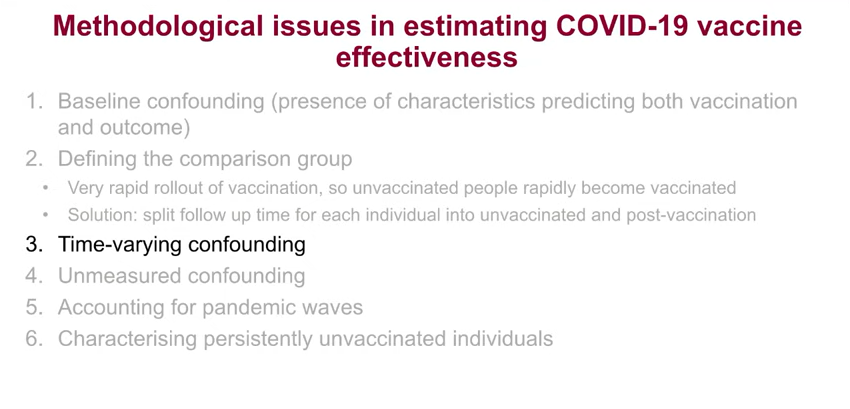
One early-morning presenter at the FDA meeting, medical statistician Jonathan Sterne from the University of Bristol, dove into this issue. His presentation focused on confounders, a statistical term for an outside force that influences the question a researcher is trying to study. In the case of vaccine effectiveness, Sterne said, there are a lot of confounders; these include vaccine recipients’ ages, how long ago they were vaccinated, and when they were vaccinated (i.e. in which phase of the pandemic?).
Sterne’s presentation focused on the confounders that make it difficult to estimate vaccine effectiveness.
Sterne and other British researchers have taken advantage of the U.K.’s extensive electronic health records to analyze how well the vaccines are working, attempting to take these confounders into consideration. Overall, he said, it’s very challenging to get trustworthy effectiveness numbers—though the U.K. has approved boosters for residents over age 50, so it’s clear that the country’s public health agency does see some need for the additional shots.
Sterne’s presentation, as did a presentation from Israeli public health officials, also underscored the need for the U.S. to collect more standardized data on breakthrough cases, among other things.
This current discussion from the CDC on collecting data about the vaccines just reveals how terrible the U.S. collection of health data are. All of it goes back to our fragmented IT infrastructure. Compare it to the data coming from the U.K.'s NHS.
Why did the FDA advisory committee vote against booster shots for everyone, ages 16 and over?
When this advisory committee votes on a question regarding vaccines or another biological product, the committee is specifically asked to consider whether the benefits of the product outweigh the risks. In this case, do the benefits of widespread boosters outweigh the risks of potential side effects from those additional doses?
When it comes to those risks of potential side effects, the committee had strikingly little data to evaluate. Pfizer did conduct a clinical trial of booster shots, but it only included 306 participants—an incredibly small number, when compared to the massive trials of the vaccine’s original two-dose regimen. The trial didn’t include any participants under age 18 or over age 55, which some advisory committee members found problematic, as they were being asked to consider approval for all Americans over age 16.
Israel—which has now administered booster shots to over 2.8 million residents—provided some data on side effects, but their utility is limited. The country started giving boosters to older adults before moving to younger adults, limiting Israeli health officials’ ability to identify potential risk for myocarditis or other severe side effects that might be more common in the younger population.
Israel has only identified 19 serious vaccine side effects from its booster shot rollout thus far, but the majority of the country’s young adults have yet to be vaccinated.
While data from Israel do suggest that booster shots can bring down infection numbers in an overall population, the FDA advisory committee did not find that a sufficient argument to recommend boosters for all Americans. Not at this time, anyway.
Why did the committee vote to support boosters for seniors and other vulnerable populations?
The risks of booster shots may not be clear for younger adults, but the risks of a breakthrough COVID-19 case are clear for older adults and others with health conditions that make them more vulnerable to severe COVID-19 case. The committee’s vote to recommend boosters for vulnerable groups aligns with a growing scientific consensus: that the U.S. should protect seniors, nursing home residents, and others who are at higher risk for serious COVID-19 cases.
What happens next?
It’s important to underscore here that this booster shot recommendation came from a committee that advises the FDA, not from the FDA itself. The agency typically follows its committee’s recommendations, but it doesn’t have to. We can expect the FDA’s decision—approval of booster shots for vulnerable groups, for everyone over age 16, or something else—within a couple of days.
Next week, on Wednesday and Thursday, a CDC advisory committee is set to meet to further discuss booster shots. If both the FDA and CDC approve boosters, health departments across the country are prepared to begin administering them to eligible Americans; this will likely include seniors and other vulnerable adults who previously got two shots of the Pfizer vaccine.
What about everyone who got the Moderna or Johnson & Johnson vaccines?
Again, this decision focused on the Pfizer vaccine, so Moderna and J&J recipients will need to wait for more data and more deliberation. Moderna has formally applied to the FDA for authorization of its booster shot, so we may see a similar series of meetings about that vaccine in the coming weeks.
J&J vaccine recipients will likely experience a longer wait as researchers collect data on the effectiveness of this one-shot vaccine. CNET has a good explainer of the situation.
Also: If you’d like to read a more detailed breakdown of everything that happened at Friday’s advisory committee meeting, I highly recommend the STAT News liveblog by Helen Branswell and Matthew Herper, which I drew upon heavily in writing this post.
This week, the federal government announced that the U.S. intends to provide third vaccine doses to all Americans who received the Pfizer or Moderna vaccines. This booster shot distribution will start in September, with adults becoming eligible once they hit eight months after their second shot.
While the booster shot regimen still must be approved by the FDA and CDC, federal officials are making it sound like a pretty sure thing—President Biden himself announced the decision at a press conference on Wednesday. However, many epidemiologists, vaccine experts, global health experts, and other scientists have criticized the decision.
Here are three main criticisms I’ve seen in the past few days.
First: Scientific evidence is lacking. As the booster shot decision was announced on Wednesday, the CDC published threenewstudies that appear to show a decline in the Pfizer and Moderna vaccines’ ability to stave off symptomatic COVID-19 infection after several months. One of these reports, from a network of U.S. nursing homes, suggests that efficacy among nursing home residents fell to just 53% by June and July 2021, many months after this vulnerable population was vaccinated. The other two reports show similar declines, though the CDC found that vaccination remains effective against severe disease, hospitalization, and death.
The federal government—and others arguing in favor of booster shots—have also pointed to data from Israel, which appear to similarly demonstrate that the vaccines lose their effectiveness after several months. In Israel, where almost 80% of residents over age 12 are vaccinated, the majority of those hospitalized with COVID-19 are now fully vaccinated individuals.
But the act of interpreting these data is more complicated than it first appears. In a blog post at COVID-19 Data Science, biostatistics professor Jeffrey Morris explains that, when the majority of a population is vaccinated, vaccination numbers will go up in this population simply because they are the majority. But the risk remains far higher for the unvaccinated. Plus, Morris explains, stratifying hospitalization numbers by age reveals that older adults are more likely to have a severe COVID-19 case regardless of vaccination status, while younger adults are less likely to be vaccinated (and thus have a non-breakthrough case).
Simply put, the vaccines do still work well against severe COVID-19—you just need to be precise in calculating effectiveness. And yet, the U.S. government is saying that vaccine efficacy wanes so much, everyone’s going to need a third shot in the fall or early next year. This suggests that the federal government has more data that it is not sharing publicly, which leads us to the second criticism.
Second: Transparency is also lacking. Typically, when the government makes a decision about approving a new medical product, this decision follows a series of prescribed steps: data submission from the company behind the product, review by FDA scientists, FDA approval, followed by more review by other agencies (such as the CDC or the Centers for Medicare & Medicaid Services) as needed. Review meetings are typically open to the public, with data shared in advance of a decision. In the case of these booster shots, however, the president has announced a specific rollout plan before full scientific review has taken place.
To many experts, including Baylor, the sequencing of the decisions being made is also out of whack. While U.S. health officials said booster shots could start being offered the week of Sept. 20, the Food and Drug Administration has not even ruled yet on Pfizer’s application for approval of a third shot; it was filed only Monday. Moderna hasn’t yet asked the agency to authorize a third shot at all.
The FDA and CDC will certainly still be reviewing the need for booster shots, but the experts cited in Branswell’s piece are skeptical that any decision other than, “Yes, go ahead” will be considered. I, for one, will be very curious to see how the discussions proceed—and what data get cited—at the FDA and CDC committee meetings.
Third: We need to vaccinate the world. As I’ve explained in the CDD before, getting vaccines to the low-income nations that have yet to start their rollouts is not just a humanitarian priority. It also protects us, here in the U.S., because the longer the coronavirus circulates, the more opportunities it has to mutate into increasingly-dangerous variants.
By moving to provide booster shots to everyone—not just the immunocompromised, the elderly, or the otherwise extra-vulnerable—the U.S. is likely delaying shots to other countries, prolonging the pandemic overall.
As Dr. Michael Ryan, emergencies chief at the World Health Organization, told reporters last week: “We’re planning to hand out extra life jackets to people who already have life jackets, while we’re leaving other people to drown without a single life jacket.”
Following the end of the federal public health emergency in May, the CDC has lost its authority to collect vaccination data from all state and local health agencies that keep immunization records. As a result, the CDC is no longer providing comprehensive vaccination numbers on its COVID-19 dashboards. But we still have some information about this year’s vaccination campaign, thanks to continued CDC efforts as well as reporting by other health agencies and research organizations.
This week, the FDA authorized Novavax’s updated COVID-19 vaccine. Here’s why some people are excited to get Novavax’s vaccine this fall, as opposed to Pfizer’s or Moderna’s.
Last week, I asked you, COVID-19 Data Dispatch readers, to send me your stories of challenges you experienced when trying to get this fall’s COVID-19 vaccines. I received 35 responses from readers across the country, demonstrating issues with insurance coverage, pharmacy logistics, and more.
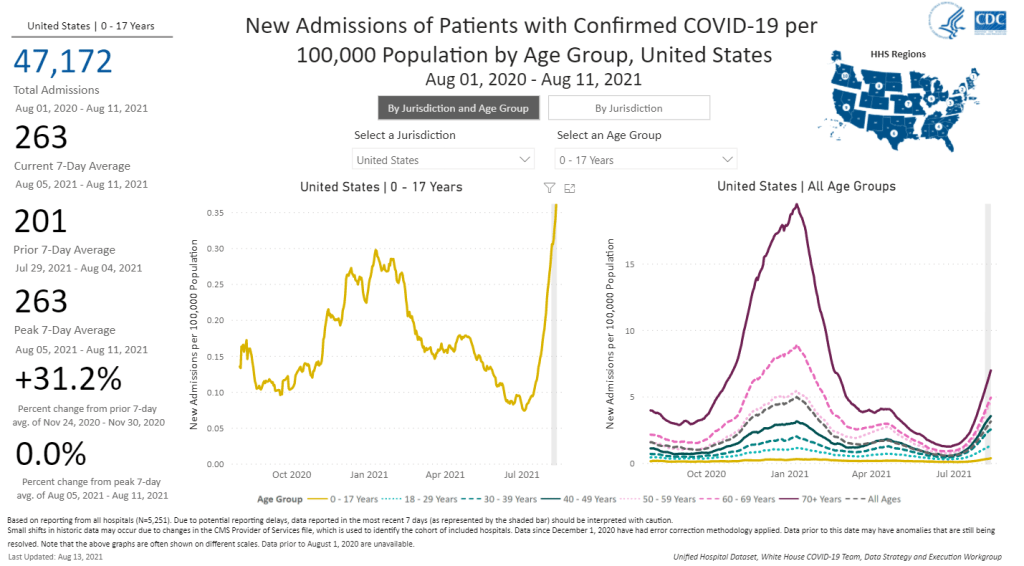
The number of children hospitalized with COVID-19 has shot up in recent weeks. Chart from the CDC COVID Data Tracker.
A couple of additional items from this week’s COVID-19 headlines:
1,900 children now hospitalized with COVID-19 in the U.S.: More kids are now seriously ill with COVID-19 than at any other time in the pandemic. The national total hit 1,902 on Saturday, according to HHS data. Asked about this trend at a press briefing on Thursday, Dr. Anthony Fauci explained that, thanks to Delta’s highly contagious properties, we’re now seeing more children get sick with COVID-19 just as we are seeing more adults get it. The vast majority of kids who contract the virus have mild cases, but this is still a worrying trend as schools reopen with, in many cases, limited safety measures. For more on this issue, I recommend Katherine J. Wu’s recent article in The Atlantic.
2.7% of Americans now eligible for a third vaccine dose: Both the FDA and the CDC have now given the go-ahead for cancer patients, organ transplant recipients, and other immunocompromised Americans to get additional vaccine doses. There are about 7 million Americans eligible, comprising 2.7% of the population. Studies have shown that two Pfizer or Moderna doses do not provide these patients with sufficient COVID-19 antibodies to protect against the virus, while three doses bring the patients up to the same immune system readiness that a non-immunocompromised person would get out of two dioses. Still, this move goes against the World Health Organization’s push for wealthy nations to stop giving out boosters until the rest of the world has received more shots.
203 cases so far linked to Lollapalooza, out of 385,000 attendees: Chicago residents and public health experts worried that Lollapalooza, a massive music festival held in the city in late July, would become a superspreader event. Two weeks out from the festival, however, local public health officials are seeing no evidence of superspreading, with a low number of cases identified in attendees. Lollapalooza may thus be an indicator that large events can still be held safely during the Delta surge—if events are held outdoors and the vast majority of attendees are vaccinated. (Officials estimated that 90% of the Lollapalooza crowd had gotten their shots.)
This week, the World Health Organization (WHO) called for wealthy nations to stop giving out booster shots in a push towards global vaccine equity.
These nations should stall any booster shots until at least September, said WHO Director-General Tedros Adhanom Ghebreyesus at a press conference on Wednesday. Instead, excess vaccines should be donated to COVAX, the international vaccine distributor that aims to mitigate COVID-19 in low-income countries. When 10% of the population in every country has been vaccinated, then wealthy countries could resume administering boosters, Tedros said.
I understand the concern of all governments to protect their people from the Delta variant. But we cannot and we should not accept countries that have already used most of the global supply of vaccine using even more of it while the world’s most vulnerable people remain unprotected.
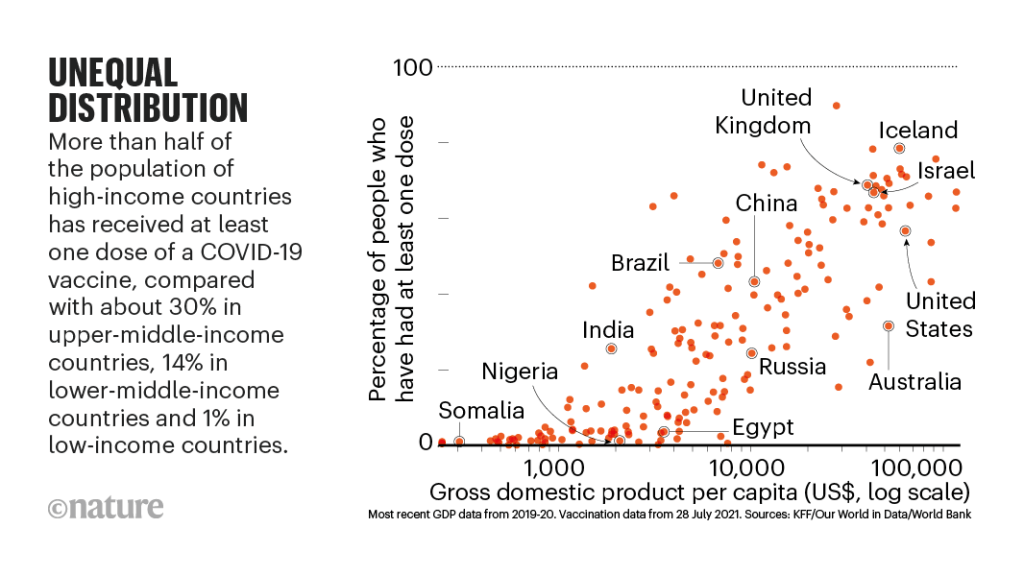
It may seem counterintuitive for a country to not provide its citizens with extra protection when it has the means to do so. But the global numbers are staggering. About 50% of the U.S. population has now been fully vaccinated, and we have doses to spare (some of which are going to waste). Meanwhile, in most African countries, 1% or less of the population is vaccinated. This is even though vaccine demand is actually far higher in low-income nations than in the U.S.
An internal analysis from the World Health Organization (WHO) estimates that if the 11 rich countries that are either rolling out boosters or considering it this year were to give the shots to everyone over 50 years old, they would use up roughly 440 million doses of the global supply. If all high-income and upper-middle-income nations were to do the same, the estimate doubles.
About 3.5 billion people in low- and lower-middle-income countries have yet to be vaccinated, Maxmen estimates. Give one dose to 10% of that number, and you use 350 million doses—less than the 440 million that rich nations would use up with boosters.
The longer that these low-income countries go without widespread vaccination, the more likely it is that new variants will emerge from their outbreaks. This is because, with every new COVID-19 case, the virus has a new opportunity to mutate. We’re already seeing Delta adapt to become even more transmissible and monitoring other potentially-concerning variants, like Lambda.
It’s unclear how much power the WHO has to enforce a booster shot moratorium, especially now that some countries (like Israel) have already gotten started on administering these extra shots. And it’s also worth noting that public health officials in the U.S. are shifting away from using “booster” to describe third shots for immunocompromised people or second shots who for those who received the one-and-done Johnson & Johnson vaccine; they say that these shots rather bring patients up to the same immunity levels as those who received two mRNA doses.
Following the end of the federal public health emergency in May, the CDC has lost its authority to collect vaccination data from all state and local health agencies that keep immunization records. As a result, the CDC is no longer providing comprehensive vaccination numbers on its COVID-19 dashboards. But we still have some information about this year’s vaccination campaign, thanks to continued CDC efforts as well as reporting by other health agencies and research organizations.
This week, the FDA authorized Novavax’s updated COVID-19 vaccine. Here’s why some people are excited to get Novavax’s vaccine this fall, as opposed to Pfizer’s or Moderna’s.
Last week, I asked you, COVID-19 Data Dispatch readers, to send me your stories of challenges you experienced when trying to get this fall’s COVID-19 vaccines. I received 35 responses from readers across the country, demonstrating issues with insurance coverage, pharmacy logistics, and more.