Editor’s note: Sarah Braner originally titled this post, “So long, farewell, I kinda hope this newsletter isn’t as necessary in the nearish future but also I hope we meet again.” While this is a very good title, I didn’t want anyone to see it and think that I, Betsy, am ending the publication (which I am not). Sarah has been an invaluable help these past few months—staying on top of COVID-19 data news, brainstorming post ideas, working on the K-12 data annotations, and more. I’m excited to watch her kill it at CNN and beyond!
This will be my last week writing for the CDD. I’m so incredibly grateful to everyone who has read my posts, to Betsy for literallyeverything, and to Dr. Ashish Jha for being the only one allowed to tweet from here on out. (Honorable mention to AstraZeneca for giving me an excuse to put a Simpsons meme in the newsletter.)
If you, for some reason, want to read more of my work this summer, you can catch me pumping out some Content for CNN Health after I figure out how their Slack channel works. When the school year starts up, I’ll be resuming my work as Bwog’s Science Editor with hopefully much less COVID-19 to write about. If my hopes pan out, I will fill that void by writing a weird amount of posts about Barnard laundry.
B.1.1.7. B.1.351. P1. B.1.671.2. It’s exhausting trying to keep up with emerging SARS-CoV-2 variants with names as inscrutable as these.
But thankfully, we finally have a straightforward naming system: on May 31, the WHO announced a system using letters of the Greek alphabet. B.1.1.7 (first identified in the U.K. is now Alpha, B.1.351 (first identified in South Africa) is now Beta, and so on. You can find the complete list (so far) here. While there are an innumerable amount of SARS-CoV-2 variants, so far the WHO naming system only applies to “variants of concern” and “variants of interest.”
While there have been non-place-related names for these variants for a while, colloquially they have been called things like “the U.K. variant” and “the South African variant” because most people won’t just toss “B.1.1.7” around in conversation. (I tried, and no one knew what I was talking about.) However, this is problematic for a few reasons. First, we don’t know for sure that B.1.1.7. originated in the United Kingdom — that’s just where they found it first. And for other countries, naming a coronavirus variant after them associates a dangerous stigma with that country (like how nicknaming the coronavirus “the China virus” earlier in the pandemic contributed to a rise in anti-Asian hate). According to WHO coronavirus lead Maria Van Kerkhove in an interview with STAT News, a country will be more likely to report a variant if the name of the variant will not be associated with the country name.
The WHO naming system is nice for now, but it’s not clear if it’ll catch on and become the norm or if it’ll just be yet another naming system in a crowded patchwork. It’s also unclear what will happen if we run out of Greek letters, but we certainly hope it doesn’t come to that. (Making this yet another reason to vaccinate the world.)
Good news for kids hoping for jabs in arms (which used to sound like an oxymoron before this spring): Moderna has announced promising results for its trial in adolescent-aged children. In around 4,000 adolescents, the vaccine proved to be 94.1% effective in preventing disease. No cases in the vaccinated group were found two weeks after the second shot, while 4 cases were found in the unvaccinated control group.
On Tuesday, May 25, Moderna showed in a clinical trial that its mRNA vaccine is safe and effective in people ages 12 to 17. The company will apply for FDA emergency use authorization in June. This follows the semi-recent authorization of the Pfizer-Biontech vaccine for the same age group, which happened at the end of March.
While children tend to have less severe complications from COVID-19 on the whole, serious illness is still quite possible. And even though rates across the country are falling due to more widespread vaccination, it’s still important that kids get vaccinated as herd immunity is not quite in our grasp yet.
The availability of another vaccine may help more people in this age group get protected; however, the rest of the world has nowhere near the access to vaccines that U.S. citizens over age 12 do right now. In April, health policy experts estimated that the United States might have an excess of up to 300,000 extra vaccines.
That being said, adolescents should still get vaccinated if it is available to them. This problem isn’t the fault of citizens wanting to get protection; it’s about the failures of governments and systems to provide vaccine equity.
Following the end of the federal public health emergency in May, the CDC has lost its authority to collect vaccination data from all state and local health agencies that keep immunization records. As a result, the CDC is no longer providing comprehensive vaccination numbers on its COVID-19 dashboards. But we still have some information about this year’s vaccination campaign, thanks to continued CDC efforts as well as reporting by other health agencies and research organizations.
This week, the FDA authorized Novavax’s updated COVID-19 vaccine. Here’s why some people are excited to get Novavax’s vaccine this fall, as opposed to Pfizer’s or Moderna’s.
Last week, I asked you, COVID-19 Data Dispatch readers, to send me your stories of challenges you experienced when trying to get this fall’s COVID-19 vaccines. I received 35 responses from readers across the country, demonstrating issues with insurance coverage, pharmacy logistics, and more.
Some good global vaccine news this week: it looks like vaccine cocktails may be a promising option.
A clinical trial based in Spain of around 600 participants (aged 18-59) reported encouraging results regarding mix-and-match vaccines (or “heterologous prime-and-boost,” if you want the jargon) meaning one shot of one vaccine and the second shot of another. In this study, the first dose given was AstraZeneca, and the second was Pfizer.
The study found that protective IgG antibodies were 30-40 times higher in the treatment group than the control group (those who had only received the first dose of the AstraZeneca vaccine). Neutralizing antibodies were also seven times higher after the Pfizer dose compared to the control, while usually they double in number after the second AstraZeneca shot.
As some people familiar with Covid vaccines may note, these vaccines use two different mechanisms to stimulate the immune system: the AstraZeneca shot uses an adenovirus vector modified with the SARS-CoV-2 spike protein while the Pfizer vaccine uses messenger RNA to coax cells into making the spike protein themselves. This early success demonstrates that vaccines with different mechanisms can be combined to induce a strong immune response.
In the wake of the AstraZeneca blood clot news, it’s reasonable to expect that some may be hesitant to get the second shot if they have received the first AstraZeneca shot. Some authorities have advised people who have gotten the first dose of AstraZeneca to get an alternative for the second shot. Having an alternative that hasn’t been linked to blood clots might persuade those hesitant to get the second AstraZeneca shot to complete a vaccination regimen, especially if it might stimulate even more of an immune response than the regular AstraZeneca regimen.
There’s currently another heterologous prime-and-boost trial in place in the United Kingdom with a slightly more complicated experimental setup (the four groups were AstraZeneca for both shots, Pfizer for both shots, Pfizer for the first and AstraZeneca for the second, or vice versa), with all participants over 50.
This study hasn’t reported results regarding immune responses yet, but they have reported some preliminary reactogenicity results. On May 12, researchers reported that mild side effects like fever or fatigue were more common in people who had received mixed vaccines. However, there were no severe side effects, and the mild ones subsided after a few days. The Spanish study did not find this, and instead found that mild side effects were about as common as they were with a regular vaccine regimen.
The UK study is expected to report immune response data soon, so it’ll be interesting to see if it matches the results found by the Spanish study. We’ll keep you updated when those results come out.
Following the end of the federal public health emergency in May, the CDC has lost its authority to collect vaccination data from all state and local health agencies that keep immunization records. As a result, the CDC is no longer providing comprehensive vaccination numbers on its COVID-19 dashboards. But we still have some information about this year’s vaccination campaign, thanks to continued CDC efforts as well as reporting by other health agencies and research organizations.
This week, the FDA authorized Novavax’s updated COVID-19 vaccine. Here’s why some people are excited to get Novavax’s vaccine this fall, as opposed to Pfizer’s or Moderna’s.
Last week, I asked you, COVID-19 Data Dispatch readers, to send me your stories of challenges you experienced when trying to get this fall’s COVID-19 vaccines. I received 35 responses from readers across the country, demonstrating issues with insurance coverage, pharmacy logistics, and more.
So long, farewell, I hope we never have to meet again: the sun is setting for the incredibly hardworking bot Turbovax.info. (As of May 15 it is still operational, and it is not clear when the bot will be retired for good.) New York City has opened more walk-in vaccine centers and as more people get vaccinated, and the bot’s creator, Huge Ma, tweeted that “It’s been a real honor to serve all of you but the need for TurboVax has come and gone.” The site has seen decreasing traffic since at least mid-April, as Ma tweeted on April 15 that there had been a 70% drop in bot traffic from the week before.
The bot (and its creator) became somewhat of a local legend when vaccine appointments in NYC were harder to find than an under-$900k Brooklyn brownstone. They drew attention from outlets ranging fromThe Guardian toThe New York Times to a particularly notable profile of Ma inThe Cut—making “Vax Daddy” (or “Vaddy”) a household name for many engrossed in COVID-19 news. Mayoral candidate Andrew Yang has even courted Ma’s endorsement. (To date, he has not endorsed a candidate, though he has endorsed more protected bike lanes.)
Ma has used his platform to advocate for AAPI folks and to denounce anti-Asian racism. On February 27, he suspended the bot as a form of protest as anti-Asian hate crimes rose across the country. (It was restored on March 1.) His continuing advocacy and fundraising for Welcome to Chinatown, a nonprofit providing resources for small businesses in the Chinatown area of Manhattan, has raised $200,000, according to his Twitter.
We here at the CDD salute Ma’s incredible work, and personally, I’m particularly grateful for Turbovax for getting one of my friends vaccinated, posting really cute pictures of his cat MaoMao, and getting Bowen Yang back on Twitter for a brief spell. And amidst the sentimentality, there’s a smidge of good news: while the actual bot is being retired, Ma will still be tweeting from the @Turbovax account “bc it’s fun.”
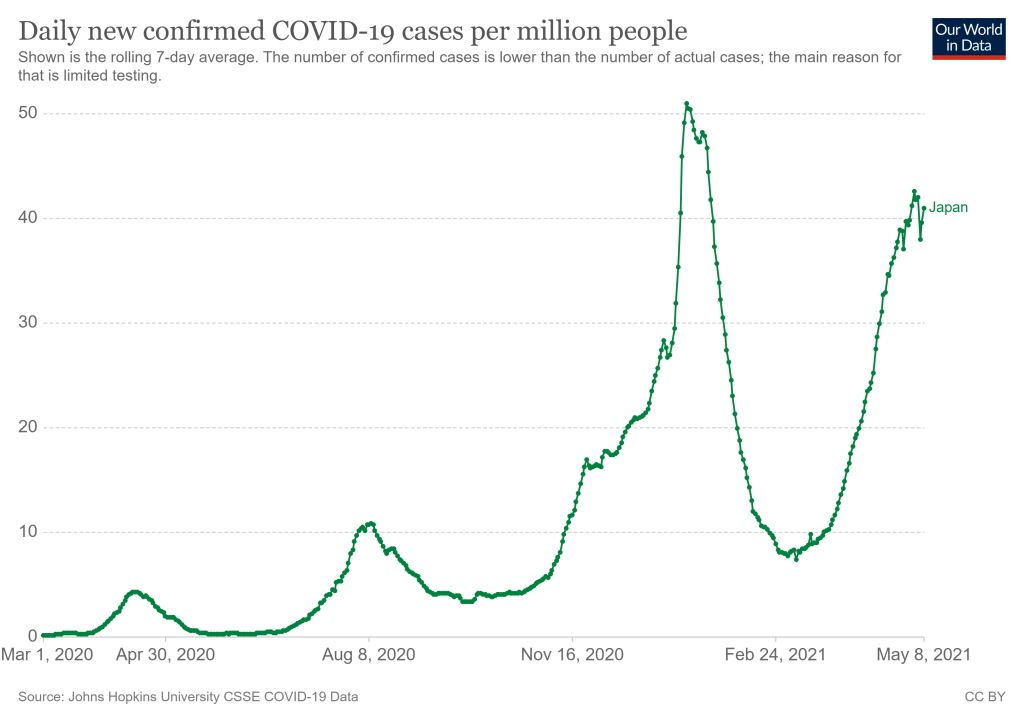
Japan’s new COVID-19 cases per million, as of May 8. Chart via Our World in Data.
They’re definitely not ready now. The Japanese government just announced it would extend an already-standing state of emergency through May 31 following a large spike in COVID-19 cases. After “Golden Week,” a sequence of Japanese Holidays lasting from late April to early May, Tokyo reported 907 new cases for the week. (New York City reported 985 cases just on May 7, for comparison.) A variant called N501Y has caused recent surges in cases, like in Osaka where hospitals struggled to treat the influx. N501Y is more infectious, and it has been correlated with more serious cases.
This surge comes as Japan struggles to roll out vaccinations. According to Our World in Data, as of May 6, 2.44% of the country’s population has received at least one dose of the vaccine. (In the United States, around 57% of the population has received at least one dose as of May 8.) So far, Japan has only approved the Pfizer-BioNTech vaccine for use, though it may approve the Moderna and AstraZeneca vaccines by May 20. Pfizer has also announced that the company will donate vaccines to athletes and staff, and the International Olympic Committee has said, “It is expected that a significant proportion of Games participants will have been vaccinated before arriving in Japan.”
An online campaign called Stop Tokyo Olympics has gained more than 200,000 signatures to an online petition, per Reuters. A Japanese poll in January showed that 80% of respondents said the games should be postponed or cancelled, and this trend has held true since.
Japan has been extremely successful in controlling the pandemic so far, but that has also led to a lack in urgency in vaccinating the population, and again, surges have happened. The Olympics are very difficult to do in an NBA-like bubble. The scale of the Olympics is much larger, and with case counts across the world as high as they are, it’s hard to imagine that someone won’t come down with COVID-19 during the games. As the New York Times points out, the chances of a COVID-19 free Olympics are slim—instead, the priority will be controlling cases as they come up.
Officials have repeatedly insisted that the games will go on as planned, and there is no sign that they will be cancelled or postponed. Will this current state of emergency crush the curve enough? We won’t know until July.
The academic year is coming to an end for most schools pretty soon (I’ve been off for about a week, but I’m a college student), so we thought it’d be appropriate to check in on the state of state K-12 COVID-19 data. We’ve been keeping track of the metrics reported by states throughout the fall and spring, and you can find our annotations of those sources here.
We had a few metrics that we looked for in a school tracker (if one exists for a state at all, which we’ll get to.) These include cases, hospitalizations, deaths, tests, test positivity rate, and in-person enrollment. We also wanted to know if trackers were separating student cases from staff cases. While we didn’t expect every state tracker to account for all of these, a robust tracker should include at least a few.
Turns out, no state trackers reported all of our wished-for metrics. Most trackers—37 of them—just reported cases and called it good, and 24 of them separated cases by students and staff. There are too many states in this vein to list them all, but a few include Alabama, Indiana, Idaho, the Dakotas, South Carolina, and Oregon (which is my home state so I’m a bit more disappointed.)
But when we narrow it down to slightly more granular metrics like hospitalizations, the number of trackers that report them drop significantly. Only five states reported deaths: Colorado, Illinois, Kansas, North Carolina, and Virginia. Three reported hospitalizations: Illinois, Kansas, and Georgia. Two reported tests: Georgia and New York. (One caveat for Georgia: they’re not actually reporting cases in schools, they’re reporting cases in school-aged children.)
To assess how robust a particular state’s tracker was, we assigned it an index number based on how many metrics it reported. (The methodology for doing so can be found here.) Essentially, a higher number indicates a more robust tracker. With this methodology, the top five states were New York (19), Kentucky (14), Texas (14), New Hampshire (14) and South Carolina (13). The bottom three were Utah, Arizona, and Kansas (all 7.) The average was between 8 and 9, with a median of 9.
However, so far we’ve been talking about states with school trackers at all. 11 states do not track school cases (at the very least, we couldn’t find their school tracker). I’ll actually list these out: Alaska, Arkansas, California, Iowa, Nebraska, Nevada, New Mexico, Oklahoma, Pennsylvania, Utah, and Wyoming.
In pointing this out, I’m not trying to shame the public health authorities in these states who are working very hard to get this pandemic under control. I’m trying to get the point across that statewide school data is still very fractured and very incomplete. And while we wait for a complete federal tracker, state data is really all we have. COVID-19 is still going to be a threat in schools as long as people under 16 can’t get vaccinated; we should at least know how much of a threat it’s turned out to be.
On November 18, New York City mayor Bill de Blasio announced that the city’s schools would close until further notice. The NYC schools discrepancy is indicative of an American education system that is still not collecting adequate data on how COVID-19 is impacting classrooms—much less using these data in a consistent manner.
After 10 days, the pause on the J&J vaccine has been lifted. According to CDC Director Rochelle Walensky, there have been about 1.9 cases of severe blood clotting per million people who had received the J&J vaccine. It has been re-authorized for use in people aged 18 and older, now with an addendum to the label and fact sheet warning of the risk of blood clots:
“We absolutely agree with the FDA on the implementation of a warning within our label and patient and physician factsheets describing this very rare event, including how it can be identified early and diagnosed and treated”. Here is the agreed on warning: pic.twitter.com/3dmKdVtATY
It’s important to note that at time of writing (April 24) only some states have already resumed its use. (These are Arizona, Colorado, Connecticut, Louisiana, Maine, Massachusetts, Michigan, Missouri, Nevada, New York, Tennessee, Texas, Indiana, and Virginia.) However, this is coinciding with a larger trend of states ordering fewer vaccine doses.
The J&J vaccine’s return is probably good news for the rest of the world as well. Combined with the AstraZeneca vaccine, the J&J vaccine was supposed to be one of the big players in the global fight against COVID-19. But the U.S. pause raised concerns for vaccine diplomacy and the global rollout—J&J had also paused its European distribution, South Africa announced they were putting J&J distribution on a temporary hiatus, and Australia said it wouldn’t purchase any J&J doses. Resuming distribution in the U.S., which can act as a bellwether for which vaccines are seen as desirable abroad, might allay concerns about safety abroad.
Following the end of the federal public health emergency in May, the CDC has lost its authority to collect vaccination data from all state and local health agencies that keep immunization records. As a result, the CDC is no longer providing comprehensive vaccination numbers on its COVID-19 dashboards. But we still have some information about this year’s vaccination campaign, thanks to continued CDC efforts as well as reporting by other health agencies and research organizations.
This week, the FDA authorized Novavax’s updated COVID-19 vaccine. Here’s why some people are excited to get Novavax’s vaccine this fall, as opposed to Pfizer’s or Moderna’s.
If you attended or read about the April 14 emergency ACIP (Advisory Committee on Immunization Practices) meeting discussing the pause, you probably heard “VAERS” a lot. VAERS stands for “Vaccine Adverse Event Reporting System.” It’s used as a “national early warning system to detect possible safety problems in U.S.-licensed vaccines,” it’s been around for much longer than the COVID-19 vaccines or even COVID-19, and it’s how regulators are examining the data about possible complications related to the Johnson & Johnson COVID-19 vaccine. And as the cherry on top, the data is open to the public through the WONDER search engine. So what’s there?
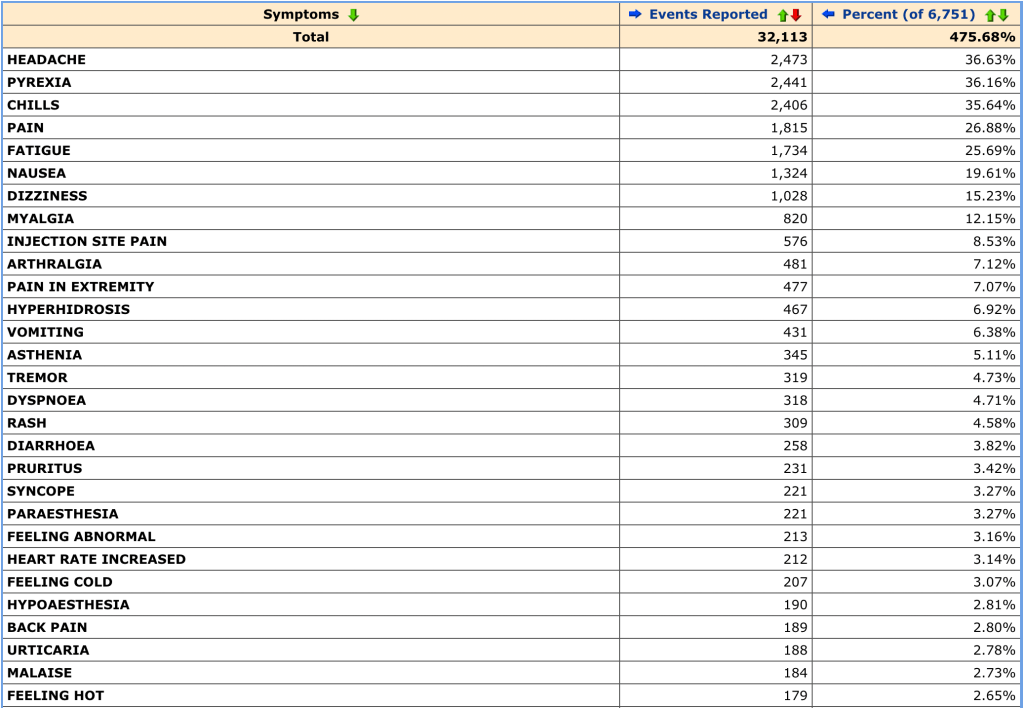
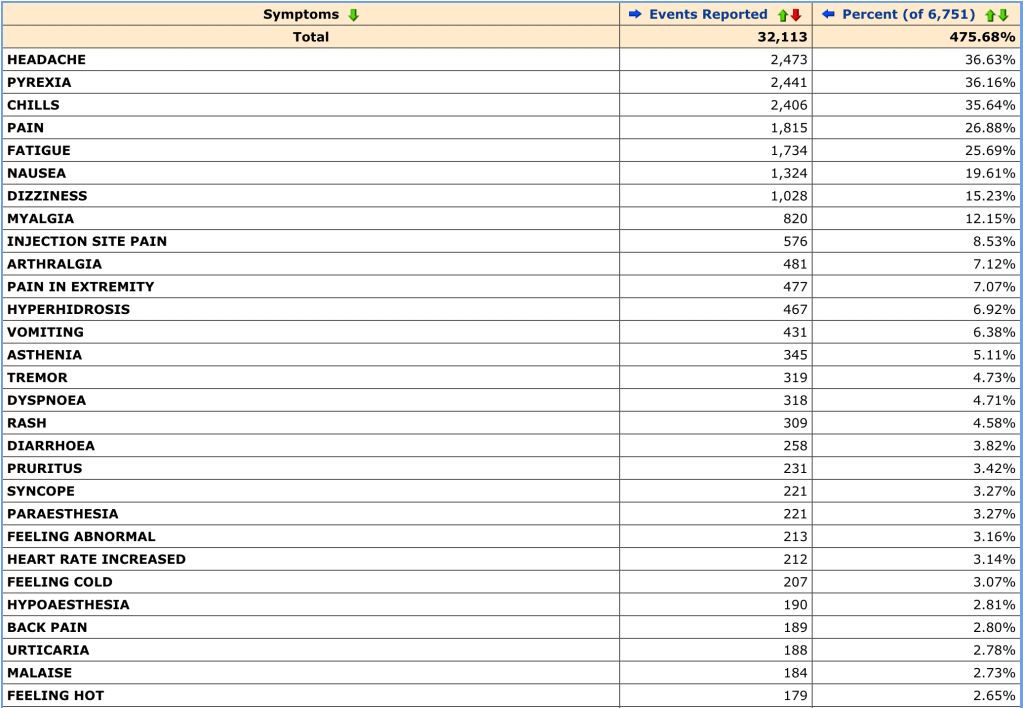
The search procedure is VERY customizable, and there’s even a video teaching you how to do it. You can narrow your search by symptoms, vaccine type, vaccine products, date that the event was reported, and more. For my cursory search, I, like a lot of people, was curious about the results for the Johnson & Johnson COVID-19 vaccine, so I just narrowed my search to “COVID-19 Vaccine Janssen.”
Here are my results, sorted by most common symptoms:
These are the most common results, but the list keeps going after that with rarer side effects as you go down. It quickly became clear that this is not a perfect system, with some slightly nonsensical reports and strange distinctions. I was certainly left wondering how “SARS-COV-2 test negative” ended up as an adverse effect. (Seems like that’s what you want? Either way, there were 59 of these reported. Good for those 59 people—or that one person with a very sore nose.)
Also notable were “Feeling abnormal” (213 reports), “Irritability” (10 reports) and my personal favorite, “No adverse event” (58 reports). It’s fairly obvious that not all of these adverse events were directly caused by the vaccine. Indeed, while the list can be fun to poke through and somewhat illuminating in what keeps popping up (headache, chills, pain, pyrexia/fever), finding the most common symptoms seems to be its main use.
J&J distribution is paused right now because there were 6 cases of cerebral venous sinus thrombosis (CVST) combined with low platelets in a group where that is not common, and symptoms manifested between 6 and 13 days after vaccination. However, you can’t see that from this dataset. It doesn’t even seem like this dataset is fully updated—right now, there’s only one case of CVST recorded. (It was last updated on April 10.) The dataset also doesn’t actually say when the person got vaccinated and when the event was reported—just frequency.
In the April 14 emergency ACIP meeting, Dr. Tom Shimabukuro of the CDC COVID-19 Vaccine Task Force cited the 6 reports as of April 12, so it looks like the public dataset hasn’t been updated while the people actually making decisions are working with updated data. It doesn’t mean that this dataset isn’t useful, it just means that one should act with caution before using it to draw any conclusions.
The CDC clearly agrees with me, as they make you check a box stating that you’ve read the disclaimers like “reports may include incomplete, inaccurate, coincidental and unverified information” and “the number of reports alone cannot be interpreted or used to reach conclusions about the existence, severity, frequency, or rates of problems associated with vaccines” before they show you the goods in WONDER.
There’s also a 17-page “VAERS Data Use Guide” which of course I found when I was almost done writing this up. Despite the limitations of the actual public dataset, I was extremely impressed by how much guidance that’s provided. I haven’t had my hand held this much while sifting through data in ages (I was very much on my own while going through the Global.Health database) and it really shows how much they want this data to be used with care. So I give serious props for solid and effective guidance on how to communicate this data—I just wish there was more data to communicate.
But WONDER isn’t the only way to sift through all the data. You can also download CSV files of every event reported (supposedly) back until 1990. That’d be a bit much for one post, but next week we might see what’s there.
Following the end of the federal public health emergency in May, the CDC has lost its authority to collect vaccination data from all state and local health agencies that keep immunization records. As a result, the CDC is no longer providing comprehensive vaccination numbers on its COVID-19 dashboards. But we still have some information about this year’s vaccination campaign, thanks to continued CDC efforts as well as reporting by other health agencies and research organizations.
This week, the FDA authorized Novavax’s updated COVID-19 vaccine. Here’s why some people are excited to get Novavax’s vaccine this fall, as opposed to Pfizer’s or Moderna’s.
On Friday, Collins posted a video of a “COVIDized” “Here Comes The Sun” to his NIH Director’s blog, in which he thanked “NIH-ers” and promised a way out of the “long, dark, COVID winter.” It’s best if you see for yourself:
The song was great of course but I loved the cat (her name is Zoe!) cameo the most.
Indeed, while numbers are looking a little worrying now, it’s pretty certain that we’re riding out the tail end, at least in the U.S.