This past week, two outlets published major investigations of the Centers for Disease Control & Prevention (CDC). The first story, by Science’s Charles Piller, focuses on White House Coronavirus Task Force Coordinator Dr. Deborah Birx and her role in the hospitalization data switch from the CDC to the Department of Health and Human Services (HHS). The second story, by ProPublica’s James Bandler, Patricia Callahan, Sebastian Rotella, and Kristen Berg, provides a broader view of internal CDC dynamics and challenges since the start of the pandemic.
These stories do not focus on data specifically, but I wanted to foreground them this week as crucial insights into how the work of science and public health experts is endangered when powerful leaders prioritize their own narratives. Both stories describe how Dr. Birx disrespected and overrode CDC experts. She wanted data from every hospital in the country, every day, and failed to understand why the CDC could not deliver. The ProPublica story quotes an anonymous CDC scientist:
Birx expected “every hospital to report every piece of data every day, which is in complete defiance of statistics,” a CDC data scientist said. “We have 60% [of hospitals] reporting, which was certainly good enough for us to have reliable estimates. If we got to 80%, even better. A hundred percent is unnecessary, unrealistic, but that’s part of Birx’s dogma.”
As I explained in this newsletter’s very first issue, in July, the CDC’s hospital data reporting system was undercut in favor of a new system, built by the software company TeleTracking and managed by the HHS. Hospitals were told to stop reporting to the CDC’s system and start using TeleTracking instead. The two features published this week tie that data switch inexorably to Dr. Birx’s frustration with the CDC and her demand for more frequent data at any cost.
Public health experts across the country worried that already-overworked hospital staff would face significant challenges in switching to a new data system, from navigating bureaucracy to, in some cases, manually entering numbers into a form with 91 categories. Initial data reported by the new HHS system in July were fraught with errors—such as a report of 118% hospital beds occupied in Rhode Island—and inconsistencies when compared to the hospital data reported out by state public health departments. I co-wrote an analysis of these issues for the COVID Tracking Project.
But at least, I thought at the time, the HHS system was getting more complete data. The HHS system quickly increased the number of hospitals reporting to the federal government by about 1,500, and by October 6, Dr. Birx bragged at a press briefing that 98% of hospitals were reporting at least weekly. As Piller’s story in Science describes, however, such claims fail to mention that the bar for a hospital to be included in that 98% is very low:
At a 6 October press briefing, Birx said 98% of hospitals were reporting at least weekly and 86% daily. In its reply to Science, HHS pegged the daily number at 95%. To achieve that, the bar for “compliance” was set very low, as a single data item during the prior week. A 23 September CDC report, obtained by Science, shows that as of that date only about 24% of hospitals reported all requested data, including protective equipment supplies in hand. In five states or territories, not a single hospital provided complete data.
Piller goes on to describe how HHS’s TeleTracking data system allows errors—such as typos entered by overworked hospital staff—to “flow into [the] system” and then (theoretically) be fixed later. This method further makes HHS’s data untrustworthy for the public health researchers using it to track the pandemic. The agency is working on improvements, certainly, and public callouts of the hospital capacity numbers have slowed since TeleTracking’s rollout in July. Still, the initial political media storm created by this hospitalization data switch, combined with the details about the switch revealed by these two new features, has led me to be much warier of future data releases by both the HHS and the CDC than I was before 2020.
Just as the White House boasted, “Our staffers get tested every day,” in response to critiques of President Trump’s flaunting of public health measures, the head of the White House Coronavirus Task Force wanted to boast, “We collect data every day,” in response to critiques of the country’s overburdened healthcare system. But testing and collecting data should both be only small parts of the national response to COVID-19. When scientists see their expertise ignored in favor of recommendations that will fit a chosen political narrative, public trust is lost in the very institutions they represent. And rebuilding that trust will take a long time.
On October 1, a little over two weeks ago, I received an email from New York Governor Andrew Cuomo’s office.
The email invited me to download a new COVID-19 phone application, developed by the New York State Department of Health along with Google and Apple. The app, called COVID Alert NY, is intended to help New Yorkers contact trace themselves. (Side note: I am not entirely sure how Cuomo’s office got my email, but I suspect it has something to do with the complaints I left about his budget back in June.)
Here’s how Cuomo’s office describes the app:
COVID Alert NY is New York State’s official Exposure Notification App. This is a free smartphone app available to anyone 18+ who lives and/or works in New York. The app uses Bluetooth technology—not location data—to quickly alert users if they have been in close contact with someone who has tested positive for COVID-19. Once alerted, users can quickly protect themselves and others by self-quarantining, contacting their physician and getting tested.
The app is intended to fit into New York’s contact tracing efforts by automatically informing app users that they have been exposed to COVID-19 and prompting them to take the necessary precautions. It also features a sypmtom checker, which asks users to note if they have exhibited a fever, cough, or other common COVID-19 symptoms, and a page with the latest case and testing data for every county in New York.
Contact tracing, or the practice of limiting disease spread by personally informing people that they have been exposed, has been a major method for controlling COVID-19 spread in other countries, such as South Korea. But in the U.S. the strategy is—like every other part of our nation’s COVID-19 response—incredibly patchwork. We have no national contact tracing app, much less a national contact tracing workforce, leaving states to set up these systems on their own.
Back in May, I researched and wrote an article for Stacker about this problem. I compared contact tracing targets, calculated by researchers at George Washington University, with the actual numbers of contact tracers employed in every state, compiled by the public health data project Test and Trace. GWU’s estimates started at a baseline 15 contact tracers per 100,000 people, then were adjusted based on COVID-19 trends in every state. Now, this story should be seen as a historical snapshot (the summer’s Sun Belt outbreaks hadn’t yet started when I wrote it), but it is telling to scroll through and see that, even several months into America’s COVID-19 outbreak, the majority of states had tiny fractions of the contact tracing workforces they needed to effectively trace new cases. New York, for example, had a reported 575 contact tracers employed, compared to an estimated need of over 15,000 contact tracers.
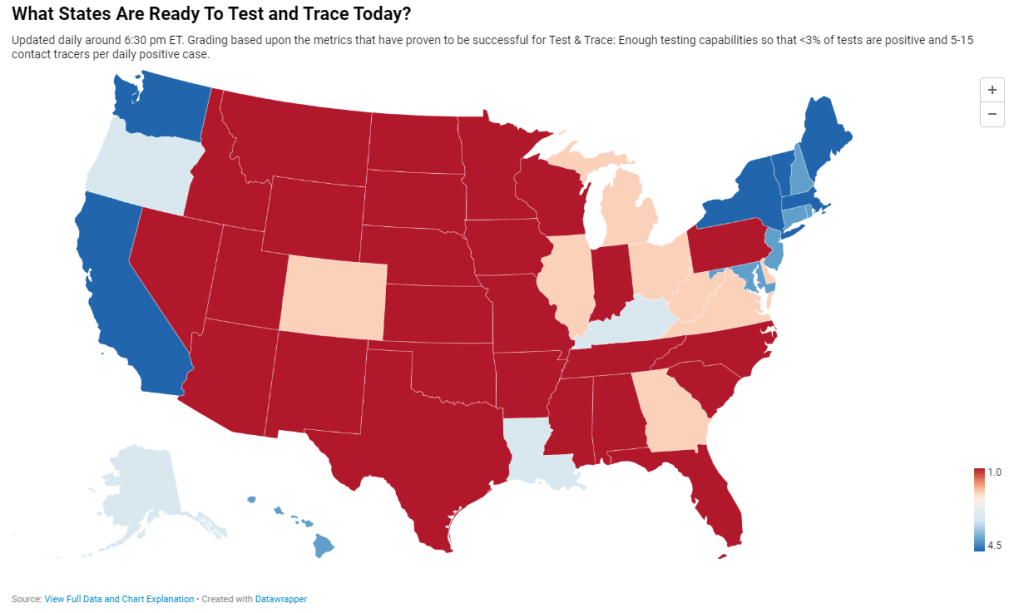
Today, many states are doing better. New York is up to 9,600 contact tracers, according to Test and Trace’s latset counts, and has planned to hire thousands more. This state, along with Massachusetts, New Hampshire, New Jersey, Connecticut, Vermont, and Washington D.C., has received high marks from Test and Trace’s scoring system, with 5 to 15 tracers employed for every new positive COVID-19 case. But all of these high-scoring states are in the Northeast, where COVID-19 outbreaks peaked in the spring. The Midwestern states currently seeing spikes, such as Wisconsin and Missouri, all rank far lower on their preparedness to trace new cases. (See the screenshot above.)
Meanwhile, actual data on the efficacy of these contact tracers are difficult to come by. To continue using New York as an example: since the application’s release on October 1, New York’s Department of Health has not released any data on how many people have downloaded the application, much less how many positive cases have been logged or how many contacts have been traced. Data have neither been mentioned in Cuomo’s press releases nor have they appeared on the state’s COVID-19 dashboard.
According to tech website 9to5Mac, as of October 1, 11 states had registered contact tracing apps with Google and Apple’s exposure notification technology. These states include Alabama, Arizona, Delaware, Nevada, New Jersey, North Carolina, North Dakota, Pennsylvania, Virginia, and Wyoming, as well as New York. Six more states have apps in development.
A brief analysis by yours truly found that, of those 11 states with contact tracing apps, only four post contact tracing data: Delaware, New Jersey, North Dakota, and Wyoming. Delaware and New Jersey both have dedicated data pages detailing the share of COVID-19 cases which have successfully participated in the state’s contact tracing efforts (57% and 71%, respectively). North Dakota and Wyoming both post statistics on their cases’ source of COVID-19 exposure, including such categories as “contact with a known case,” “community spread,” and “travel”; these data must be sourced from contact tracing investigations. 11.1% of North Dakota’s cases and 27.1% of Wyoming’s cases have an exposure source listed as “unknown” or “under investigation,” as of October 18. Meanwhile, Pennsylvania and North Carolina have both posted statistics on their contact tracing workforces, but no data on the results of these workforces’ efforts.
Other states without registered apps may also be posting contact tracing data. But it is still a notable discrepancy that, among the states that have systematic contact tracing technology, tracing results are lacking. Compare these states to South Korea, which at the height of its outbreak publicly posted demographic information and travel histories for individual COVID-19 cases in alerts to surrounding communities. South Korea’s approach has faced criticism, however, for reporting private information about people who tested positive.
And that brings me to the biggest weakness for American contact tracing: lack of public trust. Americans, more than residents of other nations, tend to be concerned about personal privacy and, as a result, are more wary of speaking to strangers on the phone or using an application that sends their data to the government, even if all those data are anonymized. Olga Khazan explained this issue in an article for The Atlantic, published in late August:
Still, contract tracing depends on trust, and many Americans don’t trust the government enough to give up their contacts or follow quarantine orders. Of the 121 agencies Reuters surveyed, more than three dozen said they had been hindered by peoples’ failure to answer their phone or provide their contacts. About half of the people whom contact tracers call don’t answer the phone, because they don’t want to talk with government representatives, Anthony Fauci, the director of the National Institute of Allergy and Infectious Diseases, said during a June news conference.
Black and Hispanic or Latino communities are particularly likely to distrust the government and avoid contact tracers’ calls. This attitude makes sense, given how both America’s government and medical systems are inexorably tied to racist histories. But for the public tracers hoping to help these communities—which have been disproportionately impacted COVID-19—it’s another barrier to stopping the virus’ spread.
Even I, as someone who understands more about the need for contact tracing than the average American, am wary about using New York’s COVID Alert app. The app asks me to turn on both Bluetooth and location data, and even though COVID Alert purports to be anonymous, Twitter, Instagram, and other applications have made no such promises. So far, I have been using the application when I go to the park, grocery shop, or ride the subway, but for the vast majority of my days it sits dormant on my phone.
And of course, I have to wonder: where was this app in March, when the city shut down and my neighborhood filled with ambulance sirens? Like most other parts of America’s COVID-19 response, contact tracing has been scattered and difficult to evaluate, but the data we do have indicate that most states are doing too little, too late.
I’m doing a shout-out instead of a callout this week, because sometimes even I tire of finding data issues to upon which I can focus my tirades.
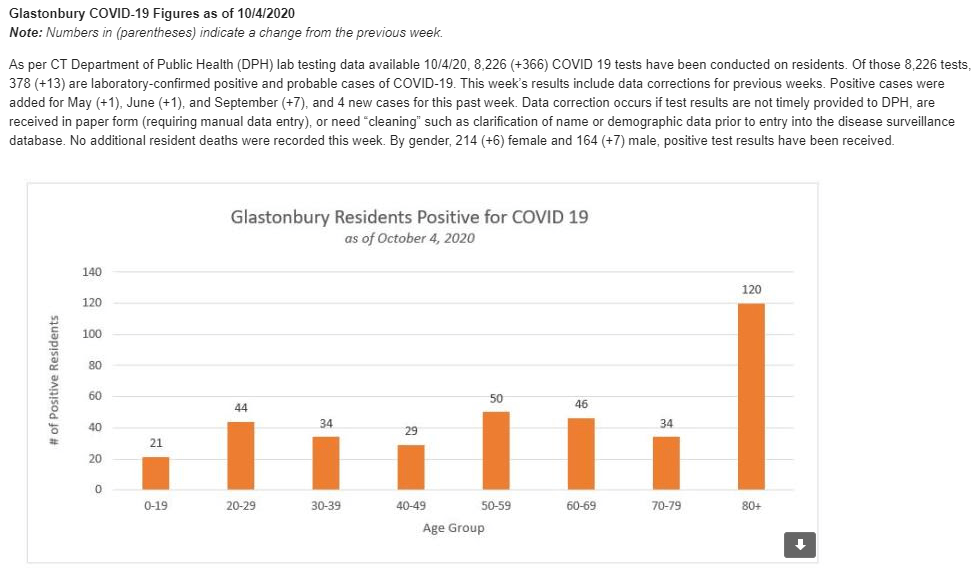
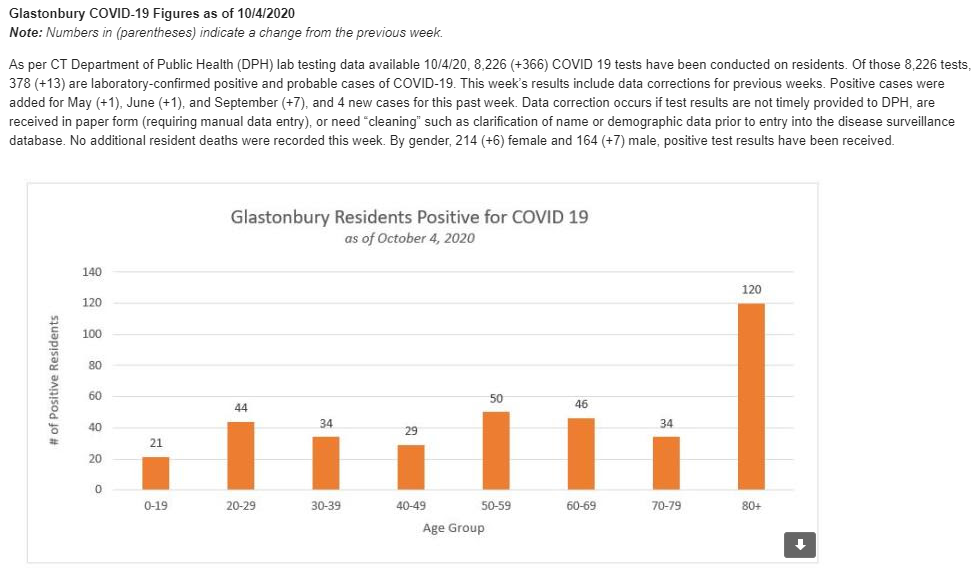
Every few weeks, my mom forwards me an email from the Town Manager in my hometown, Glastonbury, Connecticut. This email comprises the Town Manager’s Weekly COVID-19 update, including data for the town, updates for the state, and the occasional public service announcements. The most recent email, sent on October 7, includes Halloween best practices, information on flu clinics, and absentee ballot resources.
After peering at endlessly complicated state dashboards during COVID Tracking Project shifts, it’s refreshing to see a COVID-19 update which presents data as simply as possible—no hovering or scrolling required. And yeah, they clearly made that chart in Microsoft Excel, but it does its job!
The Human Mortality Database: This database includes detailed population and mortality data for 41 countries. In response to the COVID-19 pandemic, the team behind the database has started compiling weekly death counts, which can be used for excess death calculations; they have compiled counts for 34 countries so far.
SARS-CoV-2 Superspreading Events: Superspreading events, or instances in which many people are infected with the novel coronavirus at once, have been identified as a major force behind the spread of COVID-19. This database includes over 1,400 superspreading events from around the world, with information on each event’s timing, location, inside/outside setting, and more.
COVID-19 Risk Levels Dashboard: A new map from the Harvard Global Health Institute and other public health institutions allows users to see the COVID-19 risk for every U.S. county. These risk levels are calculated based on daily cases per 100,000 population (7-day rolling average).
This newsletter is about to step up its game in a big way. I am absolutely honored and thrilled to announce that I’ve been selected for the inaugural cohort of the Entrepreneurial Journalism Creators Program.
This program is a new 100-day course from the Craig Newmark Graduate School of Journalism at the City University of New York. Starting this coming week, I will learn how to better understand the needs of my audience (that’s you!) and develop a sustainable journalism project. The other 19 students in my cohort include journalists from around the world, working on projects ranging from local news to global health reporting. You can read more about the program and its participants here.
I’m incredibly grateful to all of the readers who have supported this project so far, whether you subscribed to my first issue or just found this newsletter last week. Thank you for your support and feedback on how I can best make COVID-19 data accessible. I’m excited to share what I learn in my course with you, and to grow the scope and resources offered by this project.
The county-level testing dataset published by CMS has become a regular topic for this newsletter since it was released in early September. As a refresher for newer readers: CMS publishes both total PCR tests and test positivity rates for every county in the country; the dataset is intended as a resource for nursing home administrators, who are required to test their residents and staff at regular intervals based on the status of their county.
This past Monday, October 5, I was pleasantly surprised to find a new update posted on CMS’ COVID-19 data page. I say “surprised” because I had been led to believe, both by past dataset updates and by reporting when the dataset was first published, that this source would be updated once every two weeks. And yet, here was a new update, with only one week’s delay (the last update before this was on Monday, September 28). CMS is also now posting weekly updates on an Archive page which goes back to August 19; some of these updates are older, while others were posted or edited in the past week.
I always appreciate more frequent data, even when the data provider in question is not particularly transparent about their update strategy. Frequent updates are particularly useful for testing data; the nursing home administrators monitoring testing in their counties will be able to see information that better reflects the level of COVID-19 risk around them.
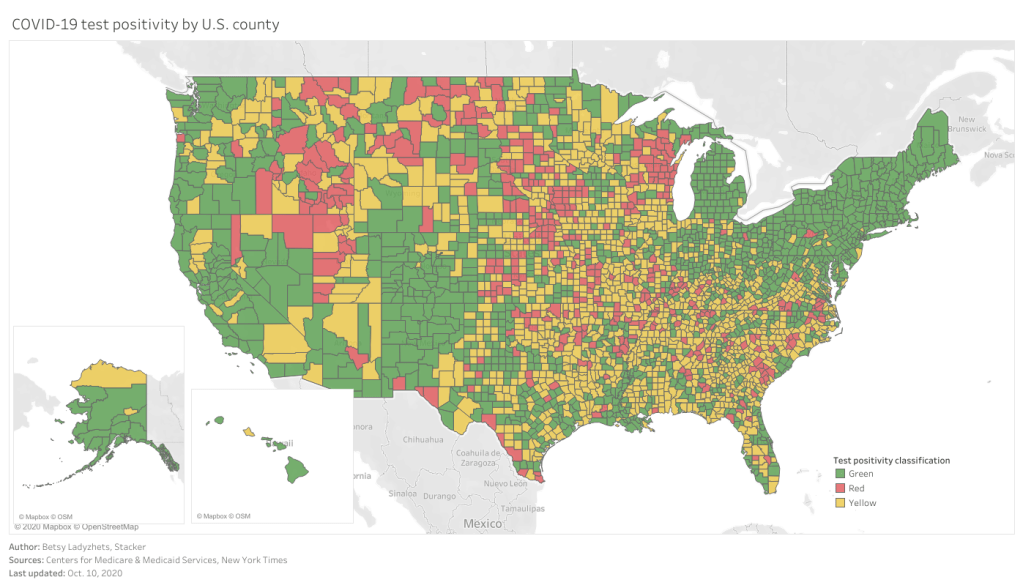
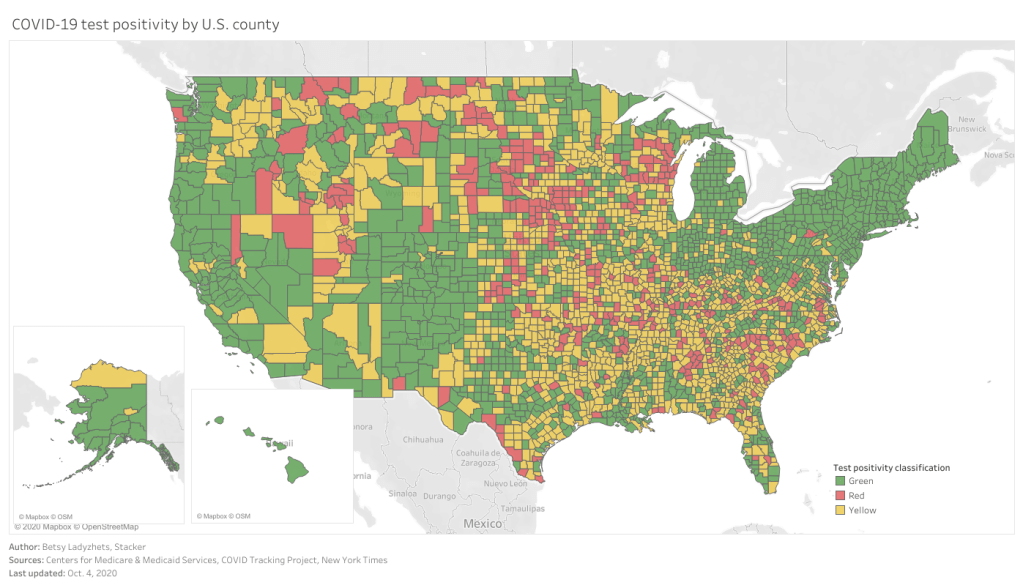
As you can see, the majority of the Northeast and much of the West Coast continues to be in the green (positivity rates under 5%), while areas in the South and Midwest are not faring so well. Twelve counties have extremely high positivity rates (over 30%), eleven of which are in Midwestern states. This table allows you to rank and sort the test positivity rates by state.
Also, a note on my methodology for this dashboard: in earlier iterations, I used state-level data from the COVID Tracking Project to calculate state test positivity rates for the same time period as the CMS has provided county-level rates. I then compared the county-level rates against state-level rates; this was the source of the “[x]% above state positivity rate” tooltips on the dashboard. After reading a new COVID Tracking Project blog post about the challenges of calculating and standardizing positivity rates, however, I realized that combining positivity rates from two different sources might misrepresent the COVID-19 status in those counties. So, I switched my method: the county-to-state comparisons are now based on averages of all the CMS-reported county-level positivity rates in each state.
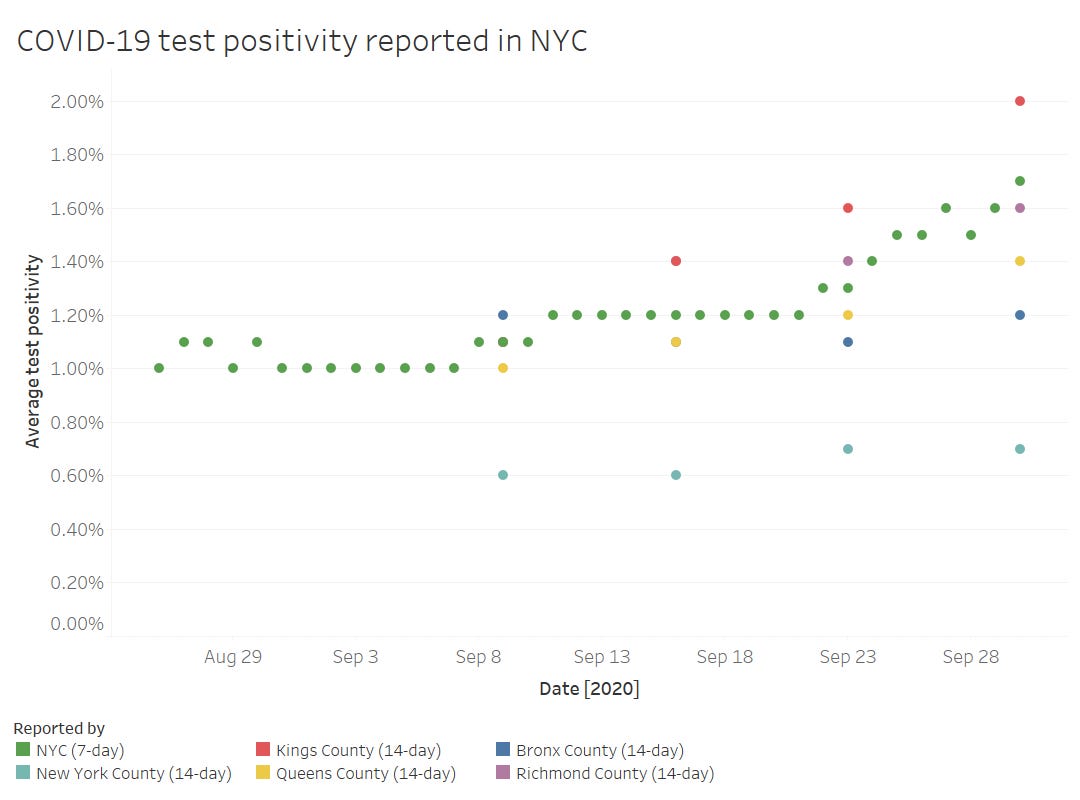
Finally, out of curiosity (and to practice my Tableau skills), I compared the CMS-reported test positivity rates for the five counties of New York City to the city-level rate reported by the NYC Department of Health.
The positivity rates reported by the two sources follow the same general direction, but it’s interesting to see how the rates diverge when the five counties split up. Manhattan remaining far below 1% while Brooklyn surges up to 2%? Not surprising.
Meanwhile, CMS is cracking down on COVID-19 reporting from hospitals: NPR reported this week that hospitals which fail to report complete, daily data to HHS can lose money from Medicare and Medicaid, starting this coming January.
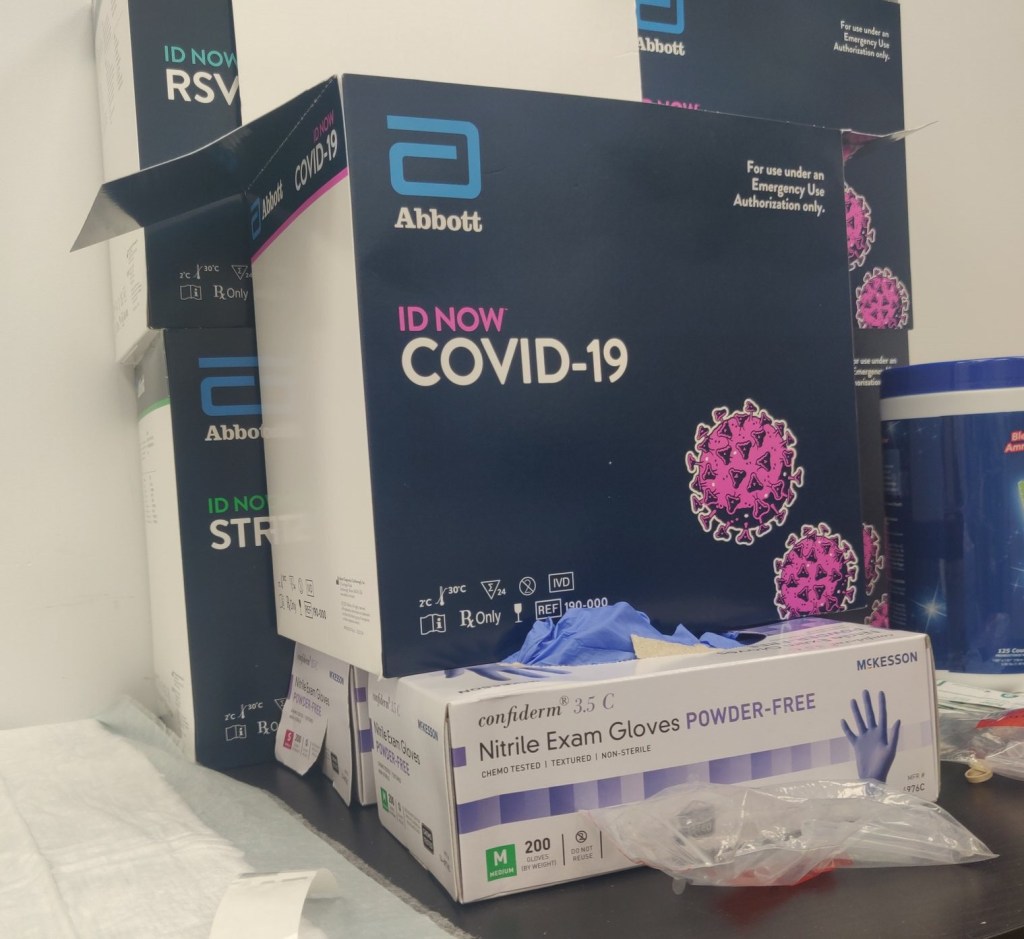
Abbott ID NOW tests, pictured at a health clinic in Williamsburg (my photo).
Two weeks ago, I went to my COVID-19 testing site of choice for a post-Maine trip screening. I walked the now-familiar ten blocks to the site, a private clinic in Williamsburg, and waited at the now-familiar counter for one of the receptionists to be available to check me in.
“Do you want a rapid test?” the receptionist asked.
“No, PCR, please,” I replied.
I had assumed that the “rapid test” she offered was an antigen test. Antigen tests, as I’ve described in this newsletter before, have a low sensitivity, meaning that they may miss identifying people who are actually infected with the novel coronavirus. (These missed cases are called false negatives.) Evidence also suggests that antigen tests will return more false negatives for patients who are asymptomatic. As I was not exhibiting COVID-19 symptoms, and rather wanted to get tested because I had recently traveled out of the state, I was interested in receiving a more accurate test.
But confusion quickly ensued: the rapid test that my clinic offered, as it turned out, was not an antigen test. It was a nucleic acid amplification test—a model manufactured by Abbott called the ID NOW. Like PCR (polymerase chain reaction) tests, this test uses gene amplification to identify genetic material associated with the novel coronavirus in a patient’s mucus sample. But unlike PCR tests, the ID NOW test does not require clinics to send samples out to faraway labs for processing. This test is distributed with small, in-house DNA amplification machines that can provide patients with their results in 15 minutes. I got the result of my ID NOW test later that same afternoon. (And then I got the results of a second test, this one a PCR test which I had asked the clinic to request at a lab, several days later. Both tests were negative.)
I hadn’t heard of Abbott ID NOW tests before last week. But they’re in the news now, connected to what has become America’s most infamous COVID-19 outbreak: President Trump’s White House relied on Abbott ID NOW tests. And they used these tests incorrectly.
No test type specification in molecular testing data
Rapid testing has been the White House’s defense against critiques of COVID-19 carelessness, explains Slate reporter Daniel Politi. Each day, staffers would get tested with Abbott ID NOW tests. Upon receiving negative results, staffers would be cleared to take off their mask and act without consideration for social distancing. Boxes of the ID NOW tests used for this screening have been pictured at the White House since March.
But how accurate are those negative results? If you’re asymptomatic: not very. The ID NOW test is only authorized for use in people with symptoms. A guidance from the Food and Drug Administration (FDA), updated on September 17, specifies:
The ID NOW COVID-19 is authorized for use with respiratory specimens collected from individuals who are suspected of COVID-19 by their healthcare provider within the first seven days of the onset of symptoms.
The majority of White House staffers who were tested with these tests had not been coughing and wheezing, nor had they been suspected of COVID-19 by a healthcare provider. In asymptomatic patients like these, as many as one-third of negatives returned by the ID NOW test may be false negatives. It’s no surprise, then, that the virus spread quickly through an indoor environment where staffers were using rapid tests—but doing little else.
White House staff are not the only people who used the wrong type of test to check their COVID-19 status. I shouldn’t have gotten an Abbott ID NOW test either. But when a nurse at my local clinic, which I saw as a site of trusted health expertise, offered one to me, I didn’t ask too many questions. It’s PCR, I thought. It’ll be accurate.
But first of all: the Abbott ID NOW test is not a PCR test. It’s in the same family as PCR tests (molecular-based, DNA amplification), but it operates on a different paradigm. And second of all, the health care workers at my clinic gave me no indication of how accurate this rapid test was, especially for my asymptomatic self. (Note: I have no hard feelings toward this clinic or any of the workers there. I’m simply using my own experience as an example of how poorly information about test types is conveyed to the public in general.)
What if my PCR test, sent out to a lab, had returned a positive result? I would have traversed Brooklyn, gotten groceries, grabbed coffee at a neighborhood cafe, and attended a protest in Queens that weekend, buoyed by a negative result yet unknowingly spreading the coronavirus to my fellow New Yorkers. And both of my tests would have been accounted for on New York’s testing dashboard in one single tick mark. New York reports tests in encounters, so my two specimens would have been deduplicated as simply “one person tested on September 30.”
I say “would have been” because I am not, in fact, sure that my Abbott ID NOW test made it into the New York Public Health Department’s database at all.
Here’s a line from the press release that Abbott put out on October 2, the day that Trump tested positive:
While we don’t know the details on who was tested and on which devices, we know that more than 11 million Americans have taken the ID NOW test, helping to stop the spread of the virus.
11 million is a pretty big number: if these tests were all included in the national count reported by the COVID Tracking Project, they would make up about 10% of the total. But are the ID NOW tests included in the COVID Tracking Project’s count? It is difficult to say. The majority of state public health departments, the sources for the COVID Tracking Project’s data, simply report total counts of nucleic acid-based tests, if they specify their test type at all.
State COVID-19 dashboards fail to separate out test counts by method or manufacturer. Some states, such as Maine and Illinois, acknowledge that their test counts include all “nucleic acid-based tests,” not only the PCR tests which fall into this category. Other states, such as Oklahoma and Florida, report detailed data about the testing capacity of individual labs and point-of-care facilities, but fail to supply the testing models used at each location. South Carolina acknowledges a small number of “unknown” tests, for which the public health department is investigating possible categorizations. The Department of Health and Human Services, meanwhile, only reports PCR tests, absent counts of any other molecular test type.
And, returning to Abbott’s press release: the manufacturer admits that they “don’t know the details on who was tested and on which devices.” This leaves a lot of open questions about how rapid testing data are being collected; Abbott seems to imply that even the manufacturer itself does not have access to specific information about where and how their tests are in use. If I had to guess, I’d say that 11 million figure comes from bulk test orders sent out by facilities like my local clinic.
It’s great for healthcare responses that Abbott tests can be processed quickly on-site, in facilities like a healthcare clinic or a major political site. But public health departments don’t have relationships with clinics—they have relationships with testing laboratories. When tests aren’t sent out to a lab, it’s easy for them to fall through gaps in a data pipeline which relies on complex electronic reporting systems. (This is also a problem for antigen tests.)
So, the problem stands: Abbott ID NOW tests are in use across the country. 11 million of them have been distributed since March. But where are the tests being used, how many of them have returned positive results, and are they being used correctly—to quickly diagnose patients with COVID-19 symptoms? Without these data, it is difficult to determine whether Abbott’s test should be part of America’s testing strategy going forward.
Conflating antigen and PCR tests
I can’t discuss the data pitfalls of rapid COVID-19 testing without devoting a few paragraphs to antigen tests.
Five days before his positive COVID-19 test was made public, President Trump announced a plan to deploy 150 million antigen tests across the country. 100 million tests will go to state and territory public health departments, while the remaining 50 million will go to facilities supporting vulnerable populations such as nursing homes, hospice care facilities, and historically Black colleges. Trump discussed how useful antigen tests could be for screening, suggesting that teachers could be tested regularly.
The tests Trump praised are rapid antigen tests manufactured by Abbott, which received FDA Emergency Use Authorization at the end of August. Abbott’s antigen tests are cheap—each one costs $5. And, like the ID NOW tests, they’re fast—patients receive results in 15 minutes. But, also like the ID NOW tests, antigen tests are more effective for symptomatic people.
Here is how Alexis Madrigal and Rob Meyer explain it, in an article for The Atlantic published this past week:
If distributed en masse and used to screen asymptomatic people, these antigen tests will deliver hundreds of thousands—if not millions—of false results, they say. False negatives could lead to reckless behavior by people who don’t know they’re sick. False positives can also put people at risk: If a virus-free nursing-home resident with a false positive is placed in a COVID-19 ward, that person could become infected.
This is not to say that antigen tests are useless; their utility is still being debated in epidemiological and public health circles. The advantages of these cheap, fast tests may outweigh the dangers of their low sensitivity. But to truly understand this problem, we need access to better antigen test data—not just 60 tests from Nevada nursing homes (the sample size upon which that state’s decision was made).
If 11 million Abbott ID NOW tests are a data concern, 150 million Abbott antigen tests are a data minefield. For the past month, I’ve been working on an analysis for the COVID Tracking Project which covers how states are reporting—and failing to report—antigen test results. This analysis is set to be released in the next week, in all its detailed glory. But I can tell you now that the majority of states are not reporting antigen tests in separate counts from DNA-based tests, just as the majority of states are not reporting other types of DNA-based tests as separate from PCR tests. In fact, several states now specifically report that their testing counts combine PCR and antigen tests in one figure.
When two different test types are conflated in a single total figure, it is difficult to analyze the progression of how either test is being used. I can’t tell you how many antigen tests are being put to use across the country, or how effective they are at containing COVID-19 in a given community, if these test numbers are lumped in with another test type. Test lumping also presents a(nother) challenge for test positivity calculations, as antigen and PCR tests have very different sensitivity levels.
And even the few separate antigen test counts that states do report are likely significant undercounts of the actual scale of antigen testing going on in the U.S. As I mentioned earlier, no data reporting pipelines are set up for tests that occur rapidly in point-of-care settings. The Center for Medicare & Medicaid Services (CMS) does not report the number of antigen tests that have occurred in nursing homes, for example.
So far, it appears that state and federal public health agencies alike are unprepared to report the results of antigen tests. Before the White House deploys its 150 million Abbott antigen tests, I hope to see that change.
Search trends on COVID-19 symptoms: Researchers can now access a Google Search dataset of search trends related to over 400 COVID-19 symptoms and related health conditions, such as fever, cough, and difficulty breathing.
FAQs on Protecting Yourself from COVID-19 Aerosol Transmission: This pubic document was compiled by a group of scientists and engineers who study aerosol transmission. Answered questions range from “How long can the virus stay in the air indoors?” to “What is the best type of mask?”
MIT COVID-19 Indoor Safety Guideline: Another air transmission resource allows users to calculate the risk levels for different indoor spaces, based on a model by MIT researchers Martin Bazant and John Bush.
Open States COVID-19 Legislation: Open States, a public civic engagement project, is compiling a list of legislation related to the COVID-19 pandemic in the U.S. The database currently tracks over 3,000 bills in 46 states.
This past Monday, September 28, the Centers for Medicare & Medicaid Services (CMS) updated the county-level testing dataset which the agency is publishing as a resource for nursing home administrators.
I’ve discussed this dataset in detail in two past issues: after it was published in early September, and when it was first updated two weeks ago. The most recent update includes data from September 10 to September 23; CMS is continuing to analyze two weeks’ worth of testing data at a time, in order to improve the stability of these values. And this update came on a Monday, rather than a Thursday, decreasing the data lag from one week to five days.
A CMS press release from this past Tuesday describes one update to how CMS assigns test positivity categories, which nursing home administrators look at to determine how often they are required to test their patients and staff:
Counties with 20 or fewer tests over 14 days will now move to “green” in the color-coded system of assessing COVID-19 community prevalence. Counties with both fewer than 500 tests and fewer than 2,000 tests per 100,000 residents, and greater than 10 percent positivity over 14 days – which would have been “red” under the previous methodology – will move to “yellow.”
This change intends to address the concerns of rural states which are not doing much testing due to their small populations.
I’ve updated my Tableau visualization with the most recent county data. The majority of the Northeast continues to be in the green, while areas in the South and Midwest pose higher concerns.
President Trump and the First Lady tested positive for COVID-19 in the early morning on Friday, October 2. As I draft this newsletter on Sunday morning, at least 15 other people connected to the President have tested positive, ranging from Bill Stepien, Trump’s campaign manager, to New York Times Washington correspondent Michael Shear.
You might expect me to source this number and these names from a federal public health agency, which is conducting all of these tests and making their results public. Not in this pandemic! My source is, of course, a dashboard compiled by volunteer journalists and science communicators.
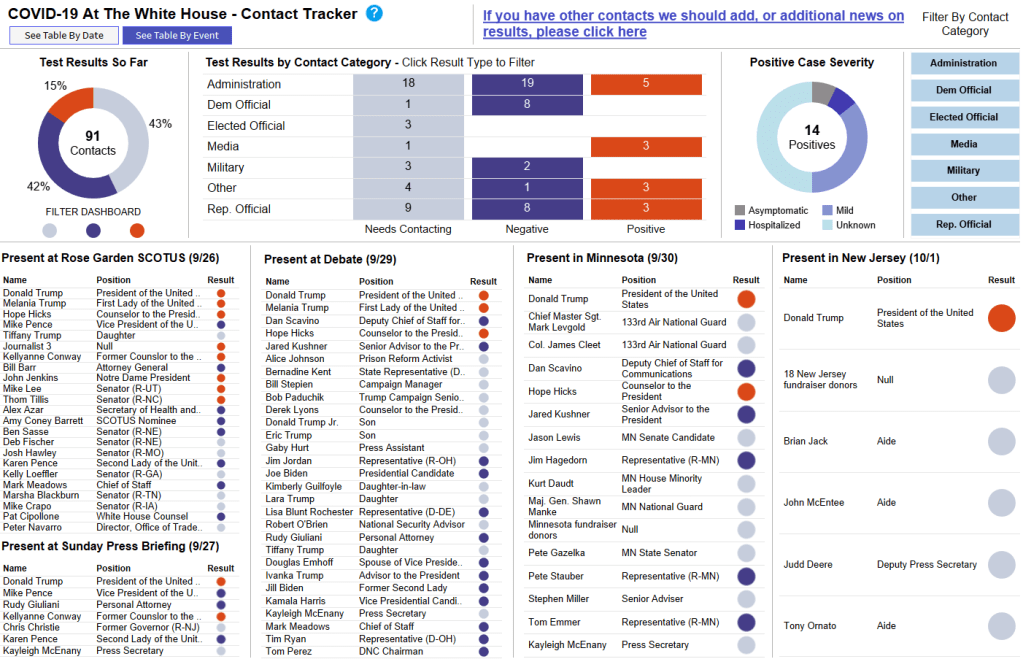
This dashboard, called the COVID-19 At The White House Contact Tracker, is attempting to trace over 200 contacts in connection with the President and his staff. The team behind it includes Benjy Renton, independent reporter on COVID-19 in higher education, Peter Walker, data visualization lead at the COVID Tracking Project, and Jesse O’Shea, MD, infectious disease expert at Emory University.
The Contact Tracker is an incredible public service. In its current form, the dashboard lists 235 White House contacts who should get tested for COVID-19, along with their positions, test results (if known), symptoms (if they test positive), and the date of their most recent test. You can also view the data as a timeline, based on each person’s last contact with the President, and as a map based on the Rose Garden ceremony, the debate, and two other potential spreading events.
It is not surprising, after months of poor data reporting from the federal government that, instead of the CDC or the HHS, the best source of data on this high-profile outbreak is—as Dr. O’Shea puts it— “three awesome dudes [contact tracing] from our homes.” But it is worth emphasizing.
we are seeing a super spreader event of high-profile politicians driven by a supreme court ceremony, & the best source of data on the outbreak is a tableau dashboard thrown together by a couple of independent journalists!!! not surprising at this point but it has to be said!!!!
What are federal public health agencies prioritizing right now, you might ask? The HHS is planning a $300 million-plus ad campaign with the goal of “defeating despair” about the coronavirus. And this money came out of the CDC’s budget. I was planning to devote a bigger section to this campaign before COVID-19 hit the White House, but instead, I will direct you to an excellent (and terrifying) POLITICO feature on the subject. Dan Diamond also discusses his investigation of the campaign on his podcast, POLITICO’s Pulse Check.