It’s been a while since I did a formal request for reader questions. (And, gotta be honest, I am a little low on content for this week after spending the past few days at SEJ.)
So, here is a formal request: let me know what you’re wondering around COVID-19 in the U.S. We’re in a confusing period right now, as BA.2 prevalence increases and safety measures are dropped across the country. What do you want to know? I’m most qualified to answer data-specific questions, but I can do my best with other questions as well.
To send in a question, simply email me at betsy@coviddatadispatch.com or comment on the post below. You can also fill out this Typeform survey that I originally sent out in January, if you missed it at that time or if your perspectives have changed.
In January, I invited readers to fill out a survey asking what you’d like to see from the COVID-19 Data Dispatch in 2022. Thank you to everyone who responded—your feedback gave me some great ideas for topics to focus on and new CDD-related initiatives to pursue this year!
This week, though, I want to focus on a topic that multiple readers brought up in the survey: how individuals can impact COVID-19 policies. One reader asked, “What can I as an individual do to make better the lacking local, state, federal, and international societal responses to COVID-19?” Another reader asked, along the same lines, “What can I do to encourage policy changes that keep people safer?”
These questions feel particularly pertinent this week, as leaders of several states loosen up on mask mandates and other COVID-19 safety measures. Governors in New Jersey, Connecticut, Delaware, Oregon, and Massachusetts have all announced that they’re ending mask mandates in public schools, and in some cases, in other public spaces. New York Governor Kathy Hochul is keeping the state’s K-12 school mask mandate in place for now, but ending a mandate for New York businesses.
Policy changes like these go against long-standing guidance from the CDC. In summer 2021, the agency recommended that communities base their levels of COVID-19 safety measures on two primary metrics: new cases per 100,000 people in the last week, and the percent of PCR tests that returned positive results in the last week. A high case rate indicates a lot of COVID-19 in the community, while a high test positivity rate can indicate the community’s testing infrastructure is not picking up a large share of cases—both suggest that measures should be put in place to control the virus’ spread.
At the time, this guidance was instituted as a response to the CDC’s preemptive recommendation that vaccinated people could go maskless. The agency said that counties seeing “high” or “substantial” transmission, according to the CDC’s metrics, should mandate masks for all, while counties with lower transmission could allow vaccinated people to go maskless. Gotta be honest: I do not know of a single state or county that’s actually following this guidance. Still, this combination of metrics is, I find, a useful and simple way to evaluate community spread.
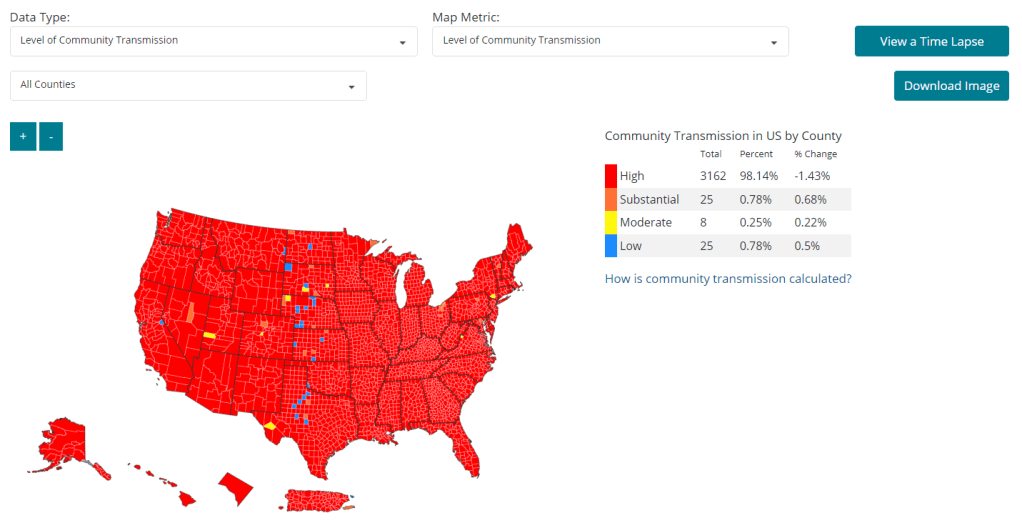
As I’ve pointed out in recent National Numbers updates, even though case numbers in the U.S. have dropped significantly since the Omicron peak in January, they are still at very high levels across the country. You can see on the CDC’s dashboard that, as of this week, about 98% of counties fall into the “high transmission” category—with over 100 new cases per 100,000 people and test positivity over 10%. And beyond the case numbers: many hospitals are currently recovering from record Omicron surges, while over 2,000 Americans are dying of COVID-19 each day.
According to the CDC’s own guidance, 98% of U.S. counties should have a mask mandate right now. But instead, among the small number of Democrat-led states that have retained mandates, safety measures are now being lifted. The CDC itself is having a hard time commenting on this situation, and is reportedly “considering updating its guidelines on the metrics states should use,” according to POLITICO.
During this time of “opening” the small number of places that were not already fully open, what can individuals do to make their voices heard—or at least improve COVID-19 safety in their own communities? I have three suggestions:
1. Call your political representatives and tell them how you feel.
If your state, city, or other local region is considering lifting some COVID-19 safety measures, you have a representative whose job literally includes listening to your complaints about this issue—whether that’s a state assembly member or city councilor.
In the last couple of years, conservative Americans have often been more politically active at the local level than more left-leaning Americans. Republicans often show up to school board meetings, call their representatives, and make their anger heard—sometimes supported by astroturfing campaigns. Anecdotal reports suggest that public health officials tend to hear more from community members who hate mandates than from those who actually want to see COVID-19 safety in their communities. You can push back against this trend.
I've talked to a lot of folks in disbelief that our government is ending mask mandates while we still have high #Covid19 transmission. I'm gutted too, but we can't be quiet. We need to BE LOUD & voice our outrage to our policymakers, governors, & leaders! Call them! Email them!
And if you want to do some additional phone-calling or emailing beyond political representatives, consider reaching out to your state or local public health department and offering some support! They can probably use it.
2. Volunteer for local organizations helping to provide vaccinations, masks, tests, and other resources.
About 80% of Americans ages five and up have received at least one COVID-19 vaccine dose, according to the CDC. This number may sound impressive, but’s more concerning when we look at the other side of the statistic: 20% of eligible Americans have not yet received at least one COVID-19 vaccine dose. Plus, among those Americans who have been fully vaccinated, more than half haven’t received a booster shot.
A lot of unvaccinated Americans are conservatives whose minds are very hard to change, this is true. But many of them are low-income workers with intense schedules, lingering health concerns, and other barriers to actually getting the shots that are surmountable, health policy expert Julia Raifman told me for a FiveThirtyEight story last month.
As a result, volunteer organizations around the country are still working to get their communities vaccinated and boosted. For example, Bed-Stuy Strong, a mutual aid group in my Brooklyn neighborhood, has hosted vaccination drives focused on local seniors and disseminated information on vaccinations and testing in the area.
Look for an effort like this that you might be able to join in your community! Or, if nothing like this currently exists, reach out to a local organization—like a public school, library, community center, etc.—and see if they might want to host a vaccine drive. Your local public health department could likely provide the supplies.
3. Educate your friends, family, and community members.
Beyond political and volunteer efforts, you can increase COVID-19 safety in your community simply by spreading the word about tools like high-quality masks and rapid tests. It might seem obvious, at this point in the pandemic, that we should all be stocking up on KN95s and testing kits, but many people do not have access to these tools—or simply don’t know why they’re useful.
You can send friends, family, and community members to websites like Project N95, which sells masks and other PPE, and Bona Fide Masks, a family business and leading KN95/N95 distributor. You can also tell them about antigen test distributors like iHealth Labs and Walmart, which are seeing fewer delays and supply crunches as the Omicron surge wanes.
In addition, if you have the resources, you can buy these masks and rapid tests in bulk and give them out. I recently gave out a couple of KN95 masks to contractors who were sent to look at a water issue in my apartment building, because I had the masks to spare. It’s that easy!
If you take any of these suggestions and see some impact, please email me (betsy@coviddatadispatch.com) and tell me about it!
Last January, as I relaunched the COVID-19 Data Dispatch on its own website, I also started a membership program. The membership, as I envisioned it, would allow readers to support my work while also getting access to an exclusive Slack server where they could network with each other and help shape the publication’s coverage.
I quickly learned, however, that while some people were willing to support my work, the Slack server was not very popular. Those who have kept up memberships over the past year have mostly done so because they like the COVID-19 Data Dispatch and want to help me keep it free for everyone.
This is awesome, obviously—and I’m very grateful to those donors, who have supported the CDD’s tech costs, payment for Intern Sarah Braner last spring, and a couple of guest articles. But in 2022, I would like to revamp readers’ options for donating in a way that aligns more closely with your interests.
The survey will help me figure that out, as well as give me an overall sense of what you all would like to see from the COVID-19 Data Dispatch in 2022. It should take under five minutes to complete, and can be done on a computer or smartphone.
I enjoyed compiling the list because it gave me a way to look back on COVID-19 news coverage throughout 2020, with a focus on those stories that dug into the numbers—whether that was visualizing pandemic trends or explaining an issue with data collection and reporting. (Also, it was a fairly straightforward issue to compile and send out two days after Christmas!)
This year, I’m planning to compile a similar list: the 21 best COVID-19 data stories of 2021.
And I need your help to pick these stories! Last year’s list was very U.S.-heavy, as I primarily read coverage from national and New York city-specific publications, and I would love to make this year’s list more geographically diverse. Please send me COVID-19 data stories you loved from your local news outlet, your favorite science journalist, or any other publication.
To submit ideas, you can comment below, email me at betsy@coviddatadispatch.com, or reach out on Twitter or Facebook. My full list will go out in next week’s issue, on December 26, and I’ll accept submissions until the 25th.
A couple of weeks ago, I received a reader question from a friend of mine who recently got engaged! He and his fiancée are planning a wedding in summer 2023, and he asked me: “How likely do you think it is that (1) the COVID-19 pandemic remains a serious danger to our safety in the summer of 2023 and (2) the government still has the energy to keep enforcing COVID-19 restrictions?” I’m going to tackle these questions one at a time.
Will the COVID-19 pandemic still be a serious danger to our safety in summer 2023?
I talked to an epidemiologist last week (for an upcoming story); he pointed out that COVID-19 is incredibly unpredictable—even for the most knowledgeable experts.
We don’t know why Delta surges appear to dip after two months, for example, or why cases might pick back up again after a decline. We can hypothesize (at least in the U.S.) that cold weather and more indoor gatherings are playing a role in the current beginnings-of-a-surge, but that’s a hypothesis. And there are plenty of other questions we’re still working to answer about the coronavirus, from why some people are superspreaders to how the virus can cause symptoms that last over a year.
So, it’s hard for me to say whether we’ll see more COVID-19 surges after the one that seems likely this winter, or what those surges will look like—whether we can stave off most severe infections with vaccinations (and booster shots), or whether hospitals will become overwhelmed yet again.
At the same time, we know that the vaccines are very good at protecting people from COVID-19. Three-dose series (and two-dose series with Johnson & Johnson) are especially good at protecting people, including from infection, transmission, severe disease, and Long COVID.
These incredible vaccines were developed based on early coronavirus strains, identified in China in early 2021. And they’re still working great against pretty much all variants. In the past couple of months, I’ve asked several experts what they think future variants might look like; and the consensus is that new mutations basically will arise from Delta at this point. The virus could get more contagious (as we saw with AY.4.2), but it seems unlikely that it would evolve to evade vaccine-induced immunity.
If we let infections hang around for too long without protecting people, without decreasing the burden of infection, it would not be surprising at all [if we see] newer variants. Will this be just a more concerning mutant of Delta? It’s possible. But it also could be something completely new that we’re not able to predict at the moment.
But I think it’s also very, very hard for us to get a new variant that will evade all vaccines. With the number of vaccines we have, we can really vaccinate many, many new people very, very quickly. I think no matter what variant comes, we will be able to bring it under control.
Of course, as far as I know, nobody saw a variant as contagious as Delta coming—so this could be overly optimistic. Again, there’s still a lot we don’t understand about this virus!
Will the government still enforce COVID-19 restrictions in summer 2023?
This second part of my friend’s question gets at a concept called “pandemic offramps,” which I’ve seen discussed a lot in COVID-19 scientist circles recently. The idea is, essentially, we need to decide how to get off the current freeway of COVID-19 safety and resume some kind of “normal life.”
The New York Times recently devoted its morning newsletter to this concept, asking when Americans will stop needing to “organize their lives around COVID-19.” The newsletter argued that vaccinated people already accept risk that’s comparable to COVID-19 in other ways, such as driving in cars.
But this piece drew criticism for suggesting that the U.S. loosen restrictions more when a new surge is approaching, more than 1,000 Americans are dying of COVID-19 every day, and billions around the world are still unvaccinated.
I really do think this kind of propaganda is more dangerous than even hard denialism. https://t.co/b1Bd19AHTV
We’re clearly not anywhere close to the “end of the pandemic” right now. But at some point, our leaders will need to answer some questions, such as: When are masks no longer necessary in public spaces? What about rigid vaccination checks, or regular testing for certain schools and businesses?
In a recent article for The Atlantic, Sarah Zhang argues that the U.S. needs to agree on a new COVID-19 goal. We’re no longer striving for 70% of adults to get vaccinated by July 4, so what are we striving for? Is there a vaccination threshold that we can label “herd immunity,” or a daily case threshold that would signify the ability to loosen restrictions?
Since public health systems in the U.S. are so fragmented, these questions likely won’t be answered all at once for everyone, but will be answered individually—by states, cities, school districts, businesses, and other institutions. New Mexico has already done this, to a certain extent, with a tiered system that helps counties add or remove COVID-19 safety measures based on outbreak levels.
And of course, in some states, it seems like leaders have already decided that any level of COVID-19 cases is acceptable, as long as businesses stay open. We can see other (less conservative) leaders go in this direction, too, with the popularization of booster shots rather than, say, implementing new mask mandates.
So, my TL;DR here is: I think serious restrictions on the level of wedding cancellation are pretty unlikely. Rather, the wedding venue might require vaccines, maybe including booster shots (possibly even multiple rounds of booster shots!). Maybe it will require COVID-19 tests or masks indoors, or the wedding planners might want to impose such precautions themselves for the safety of their guests.
Personally, I hope that by summer 2023, we can at least buy rapid tests in bulk at Costco.
I recently received a question from a COVID-19 Data Dispatch reader that followed a similar theme to many questions that readers, friends, and family members have asked me in the past few months. The question essentially outlined an event in the reader’s personal life that they’d been invited to attend, and asked for my advice: should they go? How risky was this event?
I have a hard time answering these types of questions directly, because I am no medical expert—I’m far from qualified to give direct advice. Instead, I like to outline my own attitudes towards risk at the pandemic’s current moment, and try to explain what I might do in that situation.
Right now, this type of decision-making feels harder than ever before. The majority of Americans are fully vaccinated, and we know how well the vaccines work. A growing number of Americans are getting booster shots, which we know are highly protective for seniors (and at least seem to reduce infection risk for others). So many of us are tired of the pandemic, and want to have a normal holiday season this year.
But at the same time, I feel an impetus to stay cautious—to protect the people around me as much as I can—as COVID-19 cases start to rise again in New York City, where I live, and in many other places around the country.
It’s also important to note here that everyone has a different risk comfort zone right now, partially as a product of a dearth of local and federal safety regulations at this point in the pandemic. If you’re fully vaccinated, and you’re comfortable hanging out inside with a large group of fully vaccinated people, there is evidence to suggest that is a largely safe situation for you. But if you’re not comfortable at such an event, there is also evidence to suggest that you may be able to pick up the coronavirus (even from a fully vaccinated crowd) and bring it back to someone who is more vulnerable than you are. Every choice comes with a calculation—what risk are you willing to bring to yourself and to those around you?
With all of that in mind, there are a few things I consider when I try to decide how “risky” an event might be. First of all, I still consider outdoor events to be very safe; the benefits of open air, wind, and sun far outweigh Delta’s high capacity for transmission. Then, for indoor events, I think about a few different layers of safety measures:
Will everyone be fully vaccinated?
Will negative COVID-19 tests be required before the event?
Will masks be required?
Will windows be open, or will ventilation in the space otherwise be high-quality?
What are the COVID-19 case numbers in the surrounding county; are they above or below the CDC’s “substantial transmission” threshold (50 total new cases for every 100,000 people in the past week)?
When at least three of these five conditions are met, I personally would consider an event safe for attendance. When fewer than three conditions are met, I tend to add additional layers of protection for myself and others in my immediate community by wearing a high-quality mask and getting tested before and after. (I might use an at-home rapid test or a PCR test, depending on how much security I want in that test result.
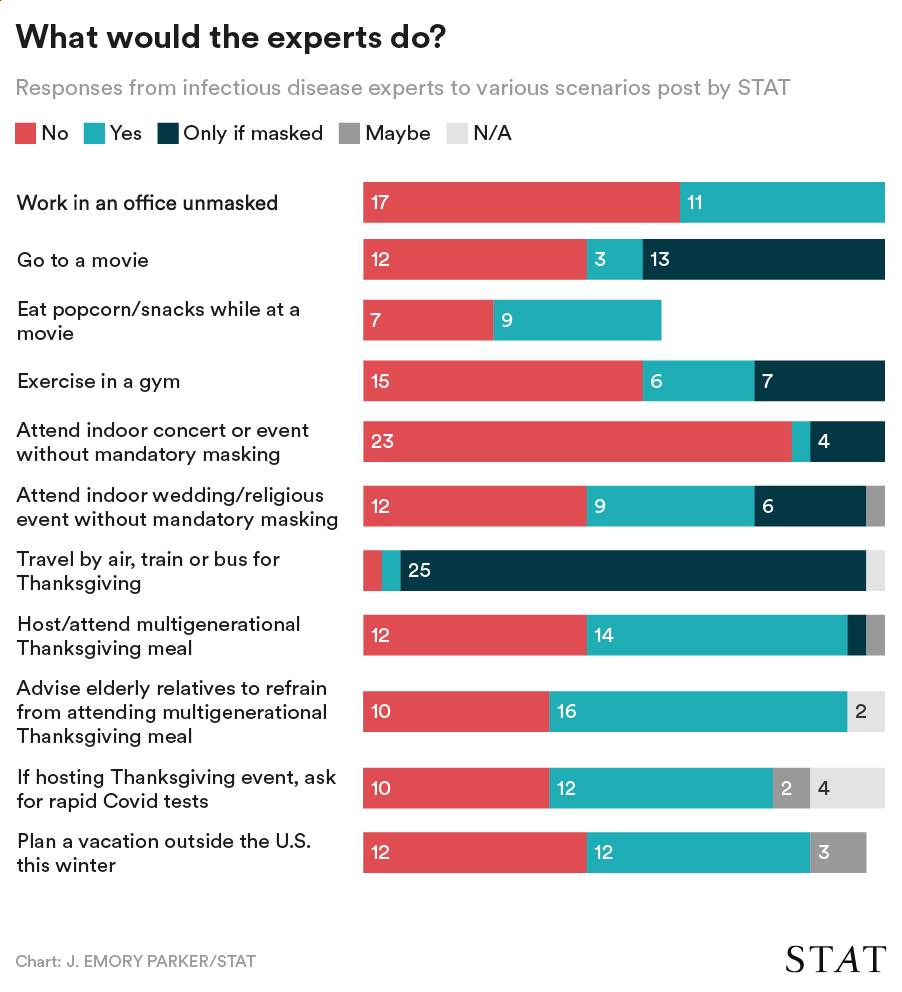
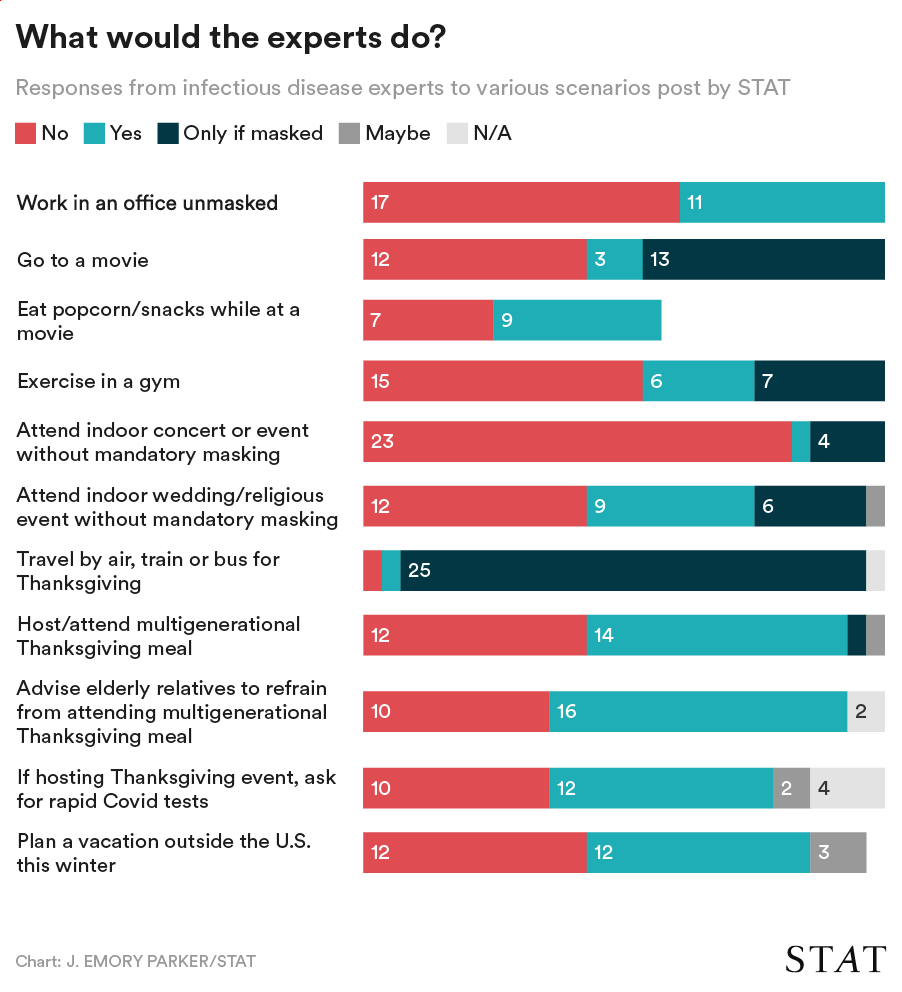
STAT News surveyed 28 infectious disease experts on activities they would currently feel comfortable doing. Chart via STAT.
Finally, if you’d rather listen to the insights of some high-profile COVID-19 experts than to me, I’ve got a source for you: STAT News recently surveyed 28 infectious disease experts on which activities they would feel comfortable doing right now. The responses to STAT’s survey reveal a diversity of risk comfort levels, even among people who are incredibly well-informed about the pandemic.
The vast majority of experts said they would travel by air, train, or bus for Thanksgiving (mostly with a mask on), and the majority said they would not attend an indoor concert or event without mandatory masks. Other than that, all the questions are fairly split. The article (which I recommend reading in full!) includes a number of insights from those experts explaining their survey responses.
It’s been about one year since I wrote the post, “Your Thanksgiving could be a superspreading event.” This post, inspired by a question I received from a reader, explained that a superspreading event occurs when one person infects many others with the coronavirus in a short period of time. I also went over how we identify these events and where they tend to occur—typically in crowded, indoor, poorly ventilated settings where people are packed together for long periods of time.
I ended the post by arguing that Thanksgiving celebrations, along with transportation and other activities along the way to those celebrations, could potentially become superspreading events. This year, the risk of spreading COVID-19 at a holiday gathering is still present—but for many gatherings, it’s much more manageable thanks to vaccines.
If you’re planning a holiday gathering this year, here are a couple of resources I’d recommend:
Upcoming holiday season (Your Local Epidemiologist): In this post, Dr. Katelyn Jetelina goes through a couple of different potential scenarios for holiday gatherings based on vaccine levels. If everyone is fully vaccinated, she writes, “approach the celebration like we did before the pandemic.” If not, more safety layers—such as encouraging new vaccinations, testing, and ventilation—may be useful.
Preparing for the holidays? Don’t forget rapid tests for COVID-19 (Harvard Health Publishing): This article, by Dr. Robert Shmerling, focuses more on the role of COVID-19 tests; Shmerling suggests that holiday hosts may offer rapid tests as guests arrive, or require a PCR test as a prerequesite to the gathering. He acknowledges, however, that rapid tests are currently pricey in the U.S. and come with other caveats.
What 5 health experts advise for holiday travel this year (Washington Post): For the unvaccinated, “your recommendations are identical to what they were last year,” Ohio State University’s Iahn Gonsenhauser told WaPo. But for the vaccinated, travel and gatherings are safer; the experts quoted in this article recommend asking about the vaccination status of other holiday guests, packing rapid tests, and making a backup plan in case someone tests positive.
But even the best resources cannot cover every possible scenario. So, I’d like to open this up for reader questions: What do you want to know about COVID-19 as we head into the 2021 holiday season?
Last week, one of the reader questions I answered addressed Long COVID, the condition in which people have COVID-related symptoms for weeks or months after their initial coronavirus infection. One reader had asked about monitoring for Long COVID patients (also called long-haulers); I later received another question about the risks of Long COVID after vaccination.
These questions made me realize that I’ve devoted very little space to Long COVID in the COVID-19 Data Dispatch—even though I consider it one of the biggest COVID-19 data gaps in the U.S. Though it’s now been well over a year since the first Long COVID patients were infected, there is still so much we don’t know about the condition.
For example, we don’t know a very rudimentary number: how many people in the U.S. are struggling with Long COVID. We also don’t have a clear, detailed picture of Long COVID symptoms, or how these symptoms arise from a coronavirus infection, or how they impact the daily lives of Long COVID patients.
Why does this massive data gap exist? Long COVID studies are challenged by the lack of standardized patient data in the U.S., making it difficult to identify symptom patterns across large groups of people. We face a similar problem in tracking breakthrough cases, demographic information, and other COVID-19 trends.
Plus, thanks to limited COVID-19 testing in the U.S. throughout the pandemic (and restrictions on who could get tested, back in spring 2020), a lot of Long COVID patients never had a positive test result—making it difficult for them to get a formal diagnosis. And many of the Long COVID studies that have been conducted focus on patients who had a positive COVID-19 test or were hospitalized for the disease, thus narrowing much of our clinical data to a small subset of the actual Long COVID population.
As I noted last week, the National Institutes of Health (NIH) has set up a major research initiative to study Long COVID. This initiative, called RECOVER, is poised to become our best source for Long COVID data in the future. But it’s in early stages right now, beginning to distribute funding to different research groups and recruit Long COVID patients for study. It could be years before we get results.
All of that said, there are still a few things we know about Long COVID based on research thus far. Here’s a roundup of twelve key statistics.
Between 10% and 30% of coronavirus infections lead to Long COVID. This statistic comes from the NIH’s RECOVER Initiative website; it summarizes findings from past studies. Consider: 30% of the 44.2 million Americans with a documented COVID-19 case amounts to 13.3 million people with Long COVID. Even 10% of those 44.2 million would amount to 4.4 million people.
Some studies suggest that as many as one-third of COVID-19 patients may have persistent or returning symptoms. A recent study of electronic health records in the U.S. and U.K., run by scientists at the University of Oxford, suggests that the true share of COVID-19 patients who contract Long COVID is on the higher end of that 10%-30% estimate that the NIH provides. This new study found that 36% of COVID-19 patients (among a sample size of 270,000) had symptoms three and six months after their diagnosis.
Long COVID may manifest with over 100 different potential symptoms. There is a Long COVID paper that I personally come back to, whenever I want to see a clear picture of the many ways that this condition can impact patients. The paper, published in The Lancet in July, reports results from a survey of over 3,000 Long COVID patients conducted by the Patient-Led Research Collaborative. According to this survey, Long COVID patients may suffer from about 100 possible symptoms, including systemic, reproductive, cardiovascular, musculoskeletal, immunologic/autoimmune, head/eyes/ears/nose/throat, pulmonary, gastrointestinal, and dermatologic symptoms.
Long COVID symptoms may change over time. The Patient-Led Research Collaborative survey found that some patients may have changing symptoms, or relapses brought on by different activities. One very common Long COVID symptom is Post-Exertional Malaise, a condition in which patients experience a relapse after physical or mental exertion, even if that exertion is relatively minor.
Some Long COVID patients have been sick for over 18 months. The Patient-Led Research Collaborative survey covers symptoms over a course of seven months, but some Long COVID patients have been suffering for far longer. Some patients who initially contracted the coronavirus in spring 2020, during the first wave in the U.S., have now been sick for 18 months or more.
Many Long COVID patients are unable to work. According to the Patient-Led Research Collaborative survey, almost half of the Long COVID patients who responded (45%) “required a reduced work schedule, compared to pre-illness.” Another 22% were not working at the time of the survey because of Long COVID. Other studies have backed up the findings from this survey. At this point in the pandemic, some Long COVID patients are struggling to receive accommodations from their employers, even though the condition is recognized as a disability at the federal level.
Long COVID can occur at all age ranges, but is documented most in younger and middle-age adults. Among respondents to the Patient-Led Research Collaborative survey, about 24% were in their thirties, 31% in their forties, and 25% in their fifties—though patients ranged in ages from 18 to over 80. This survey and others have also found that Long COVID seems to be more common for women; this pattern aligns with other post-infectious conditions, like chronic fatigue syndrome and chronic Lyme disease.
Long COVID may lead to long-term neurological issues. This past summer at the Alzheimer’s Association International Conference, a few researchers presented findings on Long COVID and Alzheimer’s. Brain scans of COVID-19 patients, along with observations of patients’ prolonged symptoms, suggest that adults who suffer from Long COVID may have an increased risk of Alzheimer’s later in life. Severe COVID-19 patients in their sixties and seventies are already starting to see symptoms matching early-onset Alzheimer’s, one researcher told NPR.
Autoimmune response may be one cause for Long COVID symptoms. While scientists are still working to determine exactly how a coronavirus infection may lead to numerous symptoms, research thus far suggests that overreaction of the immune system could be a major player. Some clinicians who work with Long COVID patients have developed treatments based on dysautonomia, medical conditions caused by immune and autonomic nervous system issues.
About 5,200 children in the U.S. have been diagnosed with MIS-C, and 46 have died. MIS-C stands for Multisystem Inflammatory Syndrome in Children. The condition follows a COVID-19 infection in rare cases, leading to inflammation of different parts of the body. While this condition is not directly comparable to Long COVID, scientists think it may have similar causes. The condition has disproportionately impacted children of color in the U.S.: out of 5,200 cases, 61% are Black or Hispanic/Latino.
The risk of Long COVID is dramatically lower after a breakthrough infection, even if you contract the coronavirus. A recent study published in The Lancet found that vaccinated patients who later had a breakthrough COVID-19 case were about half as likely to report symptoms after four weeks, compared to unvaccinated patients who had a non-breakthrough COVID-19 case. Plus, vaccinated people are already far less likely to contract the coronavirus in the first place, because vaccination reduces risk of infection. Commenting on the study, NIH Director Dr. Francis Collins called it “encouraging news,” though he cautioned that more research is needed on this topic.
Vaccination may help alleviate COVID-19 symptoms for Long COVID patients. In addition to reducing one’s risk of developing Long COVID, vaccination can alleviate symptoms for Long COVID patients. A recent preprint, posted online at the end of September, found that Long COVID patients who got vaccinated were about twice as likely to completely recover, compared to unvaccinated patients. “Overall, this study adds to growing evidence that vaccines can improve symptoms and lessen the disease impact in Long COVID,” wrote Long COVID researcher Dr. Akiko Iwasaki, sharing the study on Twitter.
To me, these Long COVID statistics—along with everything we still don’t know about the condition—provide a strong argument for vaccination. Long COVID can impact people who were young and healthy before they were infected, completely messing up their lives for months or even years. It surprises me that public health and political leaders don’t discuss this condition more when they tell people to get vaccinated.
As for continued research: the NIH’s RECOVER Initiative has received over $1 billion in funding from Congress, and it’s just getting started on setting up studies. If you’re interested in learning more about the research—or signing up to participate in a RECOVER study—you can sign up for email alerts on the NIH website.
The Delta surge is waning. Will this be the last big surge in the U.S., or will we see more? This question and more, answered below; chart from the CDC.
Last week, I asked readers to fill out a survey designed to help me reflect on the COVID-19 Data Dispatch’s future. Though the Delta surge—and the pandemic as a whole—is far from over, I’m considering how this publication may evolve in a “post-COVID” era. Specifically, I’m thinking about how to continue serving readers and other journalists as we prepare for future public health crises.
Thank you to everyone who’s filled out the survey so far! I really appreciate all of your feedback. If you haven’t filled it out yet, you can do so here.
Besides some broader questions about the CDD’s format and topics we may explore in the future, the survey asked readers to submit questions that they have about COVID-19 in the U.S. right now. In the absence of other major headlines this week, I’m devoting this week’s issue to answering a few of those questions.
Should I get a booster shot? If so, should it be a different one from the first vaccine I got? When will my kids (5-11) likely be eligible?
I am not a doctor, and I’m definitely not qualified to give medical advice. So, the main thing I will say here is: identify a doctor that you trust, and talk to them about booster shots. I understand that a lot of Americans don’t have a primary care provider or other ways to easily access medical advice, though, so I will offer some more thoughts here.
As I wrote last week, we do not have a lot of data on who’s most vulnerable to breakthrough COVID-19 cases. We do know that seniors are more vulnerable—this is one point where most experts agree. We know that adults with the same health conditions that make them more likely to have a severe COVID-19 case without a vaccine (autoimmune conditions, diabetes, kidney disease, etc.) are also more vulnerable to breakthrough cases, though we don’t have as much data here. And we know that vaccinated adults working in higher-risk locations like hospitals, nursing homes, and prisons are more likely to encounter the coronavirus, even if they may not necessarily be more likely to have a severe breakthrough case.
The FDA and CDC’s booster shot guidance is intentionally broad, allowing many Americans to receive a booster even if it is not necessarily needed. So, consider: what benefits would a booster shot bring you? Are you a senior or someone with a health condition that makes you more likely to have a severe COVID-19 case? Do you want to protect the people you work or live with from potentially encountering the coronavirus?
If you answered “yes” to one of those questions, a booster shot may make sense for you. And, while you may be angry about global vaccine inequity, one individual refusal of a booster shot would not have a significant impact on the situation. Rather, many vaccine doses in the U.S. may go to waste if not used for boosters. But again: talk to your doctor, if you’re able to, about this decision.
Currently, Pfizer booster shots are available for people who previously got vaccinated with Pfizer. The FDA’s vaccine advisory committee is meeting soon to discuss Moderna and Johnson & Johnson boosters: they’ll discuss Moderna on October 14 and J&J on October 15. Vaccine approval in the U.S. depends upon data submission from vaccine manufacturers—and vaccine manufacturers have not been studying mix-and-match booster regimens—so coming approvals will likely require Americans to get a booster of the same vaccine that they received initially. We will likely see more discussion of mix-and-match vaccinations in the future, though, as more outside studies are completed.
As for when your kids will likely be eligible: FDA’s advisory committee is meeting to discuss Pfizer shots for kids ages 5 through 11 on October 26. If that meeting—and a subsequent CDC meeting—goes well, kids may be able to get vaccinated within a week of that meeting. (Potentially even on Halloween!)
Why don’t people get vaccinated and how can we make them?
I got a couple of questions along these lines, asking about vaccination motivations. To answer, I’m turning to KFF’s COVID-19 Vaccine Monitor, a source of survey data on vaccination that I (and many other journalists) have relied on since early 2021.
KFF released the latest round of data from its vaccine monitor this week. Here are a few key takeaways:
The racial gap in vaccinations appears to be closing. KFF found that 71% of white adults have been vaccinated, compared to 70% of Black adults and 73% of Hispanic adults. Data from the CDC and Bloomberg (compiling data from states) similarly show this gap closing, though some parts of the country are more equitably vaccinated than others.
A massive partisan gap in vaccinations remains. According to KFF, 90% of Democrats are vaccinated compared to just 58% of Republicans. This demonstrates the pervasiveness of anti-vaccine misinformation and political rhetoric among conservatives.
Rural and younger uninsured Americans also have low vaccination rates (62% and 54%, respectively). Both rural and uninsured people have been neglected by the U.S. healthcare system and face access barriers; for more on this topic, I recommend this Undark article by Timothy Delizza.
Delta was a big vaccination motivator. KFF specifically asked people who had gotten their shots after June 1 why they chose to get vaccinated. The most popular reasons were, in order: the increase in cases due to Delta (39%), concern about reports of local hospitals and ICUs filling with COVID-19 patients (38%), and knowing someone who got seriously ill or died from COVID-19 (36%).
Mandates and social pressures were also vaccination motivators. 35% of KFF’s recently vaccinated survey respondents said that a big reason for their choice was a desire to participate in activities that require vaccination, like going to the gym, a big event, or traveling. 19% cited an employer requirement and 19% cited social pressure from family and friends.
The second part of this question, “how can we make them?”, reflects a dangerous attitude that has permeated vaccine conversations in recent months. Yes, it’s understandable to be frustrated with the Americans who have refused vaccination. But we can’t “make” the unvaccinated do anything, and such a forceful attitude may put off people who still have questions about the vaccines or who have faced discrimination in the healthcare system. To increase vaccinations among people who are still hesitant, it’s important to remain open-minded, not condescending. For more: read Ed Yong’s interview with Dr. Rhea Boyd.
That said, we’re now getting a sense of which strategies can increase vaccination: employer mandates, vaccination requirements for public life, and personal experience with the coronavirus. As the Delta surge wanes, it will take more vaccination requirements and careful, open-minded conversations to continue motivating people to get their shots.
What are some things I might say to convince people of Delta’s severity and the need to not relax on masking, distancing, etc?
To answer this, I’ll refer you to the article I wrote about Delta on August 1, as the findings that I discuss there have been backed up by further research.
Personally, there are two statistics that I use to express Delta’s dangers to people:
Delta causes a viral load 1,000 times higher than the original coronavirus strain. This number comes from a study in Guangzhou, China, posted as a preprint in late July. While viral load does not correspond precisely to infectiousness (there are other viral and immune system factors at play), I find that this “1,000 times higher” statistic is a good way to convey just how contagious Delta is, compared to past variants.
An interaction of one second is enough time for Delta to spread from one person to another. Remember the 15-minute rule? In spring 2020, being indoors with someone, unmasked, for 15 minutes or more was considered “close contact.” Delta’s increased transmissibility means that an interaction of one second is now enough to be a “close contact.” The risk is lower if you’re vaccinated, but still—Delta is capable of spreading very quickly in enclosed spaces.
You may also find it helpful to discuss rising numbers of breakthrough cases in the U.S. While vaccinated people continue to be incredibly well protected against severe disease and death caused by Delta, the vaccines are not as protective against coronavirus infection and transmission. (They are protective to some degree, though! Notably, coronavirus infections in vaccinated people tend to be significantly shorter than they are in the unvaccinated, since immune systems can quickly respond to the threat.)
It’s true that rising breakthrough case numbers are, in a way, expected—as more people get vaccinated, breakthrough cases will naturally become more common, because the virus has fewer and fewer unvaccinated people to infect. But considering the risks of spreading the coronavirus to others, plus the risks of Long COVID from a breakthrough case… I personally don’t want a breakthrough case, and so I continue masking up and following other safety protocols.
What monitoring do we have in place for COVID “longhaulers” and their symptoms/health implications?
This is a great question, and one I wish I could answer in more detail. Unlike COVID-19 cases, hospitalizations, and other major metrics, we do not have a comprehensive national monitoring system to tell us how many people are facing long-term symptoms from a coronavirus infection, much less how they’re faring. I consider this one of the country’s biggest COVID-19 data gaps, leaving us relatively unprepared to help the thousands, if not millions, of people left newly disabled by the pandemic.
In February, the National Institutes of Health (NIH) announced a major research initiative to study Long COVID. Congress has provided over $1 billion in funding for the research. This initiative will likely be our best source for Long COVID information in the future, but it’s still in early stages right now. Just two weeks ago, the NIH awarded a large share of its funding to New York University’s Langone Medical Center; NYU is now setting up long-term studies and distributing funding to other research institutions.
As I wrote in the September 19 issue, the NIH’s RECOVER website currently reports that between 10% and 30% of people infected with the coronavirus will go on to develop Long COVID; hopefully research at NYU and elsewhere will lead to some more precise numbers.
While we wait for the NIH research to progress, I personally find the Patient-Led Research Collaborative (PLRC) to be a great source for Long COVID research and data. The PLRC consists of Long COVID patients who research their own condition; it was founded out of Body Politic’s Long COVID support group. This group produced one of the most comprehensive papers on Long COVID to date, based on an international survey including thousands of patients, and has more research currently ongoing.
If you have the means to support Long COVID patients—many of whom are unable to work and facing homelessness—please see the responses to this tweet by PLRC researcher Hannah Davis:
As others have mentioned, people with Long COVID are unable to work & are becoming homeless.
If you have #LongCovid & are struggling, drop your venmo/cashapp/paypal/etc in this thread & I'll retweet.
If you have $ to spare, please support patients in this thread.
Why is the CDC not doing comprehensive high volumes of sequencing on all breakthrough cases at the very least?
I wish I knew! As I wrote last week (and in several other past issues), the lack of comprehensive breakthrough case data in the U.S. has contributed to a lack of clarity on booster shots, as well as a lack of preparedness for the next variants that may become threats after Delta. The CDC’s inability to track and sequence all breakthrough cases—not just the severe ones—is dangerous.
That said, it is very difficult to track breakthrough cases in a country like the U.S. Consider: the U.S. does not have a comprehensive, national electronic records system for patients admitted to hospitals, much less those who receive COVID-19 tests and other care at outpatient clinics. This lack of comprehensive records makes it difficult to match people who’ve been vaccinated with those who have received a positive COVID-19 test. Thousands, if not millions of Americans are now relying on rapid tests for their personal COVID-19 information—and most rapid tests don’t get entered into the public health records system at all.
Plus, local public health departments are chronically underfunded, understaffed, and burned out after almost two years of working in a pandemic; they have little bandwidth to track breakthrough cases. Many Americans refuse to participate in contact tracing, which hinders the public health system’s ability to collect key information about their cases. And there are other logistical challenges around genomic sequencing; despite new investments in this area, many parts of the country don’t have sequencing capacity, or the information infrastructure needed to send sequencing results to the CDC.
So, if the CDC were tracking non-severe breakthrough cases, they’d likely miss a lot of the cases. But that doesn’t mean they shouldn’t be trying, in my opinion.
How safe is it to visit my family for the holidays?
This is another place where I don’t feel qualified to give advice, but I can offer some thoughts. If I were you, I would think about the different ways in which holiday travel might pose risk to me and to the people at the other end of my trip. I would consider:
Quarantining beforehand. Do your occupation and living circumstances allow you to quarantine for a week, or at least limit your exposure to settings where you might be at risk of catching the coronavirus, before you travel? Can you get a test before traveling?
Types of travel. Can you make the trip in a car or on public transportation, or do you need to fly? If you need to fly, can you select an airline that has stricter COVID-19 safety requirements? (United recently reported that over 96% of its employees are now vaccinated, for example.) Can you wear a high-quality mask for the flight?
Quarantining and/or testing upon arrival. Can you spend a couple of days in quarantine once you get to your destination? Would you have access to testing (with results in under 24 hours) upon your arrival, or would you be able to bring rapid tests with you?
Who you’re spending time with. Among the family you’d be visiting, is everyone vaccinated (besides young children)? If anyone is not vaccinated, could your potential travel be a motivator to help convince them to get vaccinated? Does the group include seniors or people with health conditions that put them at high risk for COVID-19, and if so, can they get booster shots?
Activities that you do at your destination. Would you be able to have large gatherings outside, or in a well-ventilated space? What else can you do to reduce the risk of these activities?
Like other activities, travel can be relatively safe or fairly dangerous depending on the precautions that you’re able to take, and depending on COVID-19 case rates where you live and at your destination. And, like other activities, your choice to travel or not travel depends a lot on your personal risk tolerance. Nothing is zero-risk right now; each person has a threshold that determines what level of COVID-19 risk they are and are not comfortable taking. Through some self-reflection, you can determine if travel is above or below your risk threshold.
Why are policies so different now than they were at this time last year?
Public health tends to go through cycles of “panic” and “neglect.” Ed Yong’s latest feature goes into the history of this phenomenon:
Almost 20 years ago, the historians of medicine Elizabeth Fee and Theodore Brown lamented that the U.S. had “failed to sustain progress in any coherent manner” in its capacity to handle infectious diseases. With every new pathogen—cholera in the 1830s, HIV in the 1980s—Americans rediscover the weaknesses in the country’s health system, briefly attempt to address the problem, and then “let our interest lapse when the immediate crisis seems to be over,” Fee and Brown wrote. The result is a Sisyphean cycle of panic and neglect that is now spinning in its third century. Progress is always undone; promise, always unfulfilled. Fee died in 2018, two years before SARS-CoV-2 arose. But in documenting America’s past, she foresaw its pandemic present—and its likely future.
During the COVID-19 pandemic, the U.S. took a nosedive into the “neglect” cycle before we were even finished with the “panic” cycle. Congress has already slashed its funding for future pandemic preparedness, while state and local governments across the country restrict the powers of public health officials. As a result, we’re seeing an “everyone for themselves” attitude at a time when we should be seeing new mask mandates, restrictions on public activities, and other safety measures.
Basically, America decided the pandemic was over and acted accordingly—and if you get COVID-19 now, it’s “your fault for not being vaccinated.” This phenomenon has been especially pronounced in rural areas, which struggled a lot (but saw few cases) during spring 2020 lockdowns and are extremely hesitant to do anything approaching a “lockdown” again.
We need an attitude shift—and more investment in public health—to actually end this pandemic and prepare for the next health crisis. Yong’s feature goes into this in more detail; definitely give that a read if you haven’t yet.
When is this going to be over?!?
Unfortunately, this is very hard to predict—even for the expert epidemiologists and computational biologists who make the models. Check out the CDC’s compilation of COVID-19 case models: most of them agree that cases will keep going down in the coming weeks, but they’re kind of all over the place.
Last week, I summarized two stories—from The Atlantic and STAT News—that discuss the coming winter, and kind of get at this question. It’s possible that cases keep declining from their present numbers, and that the Delta surge we just faced is the last major surge in the U.S. It’s also possible that a new variant arises out of Delta and sends us into yet another new surge. If that happens, more people will be protected by vaccination and prior infection, but healthcare systems could come under strain once again.
As long as the coronavirus continues spreading somewhere in the world, it will continue to pose risk to everyone—able to cause new outbreaks and mutate into new variants. This will continue until the vast majority of the world is vaccinated. And then, at some point, the coronavirus will probably become endemic, meaning it persists in the population at some kind of “acceptable” threshold. Just like the flu.
Dr. Ellie Murray, epidemiologist at Boston University’s School of Public Health, explained how a pandemic becomes endemic in a recent Twitter thread:
Everyone keeps talking about covid becoming endemic, but as I listen to the conversation, it’s becoming more & more clear to me that very few of you know what “endemic” means.
Dr. Murray points out that, even when a disease reaches endemic status, tons of scientists and public health workers will still continue to monitor it. This is the case for the flu—think about all of the effort that goes into a given year’s flu shot!—and it will likely be the case for COVID-19.
In short, public health leaders need to figure out what level of COVID-19 transmission is “acceptable” and how we will continue to monitor it. This needs to happen at both U.S. and global levels. And, thanks to our vaccine-rich status, it’ll likely happen in the U.S. long before it happens globally.
So, yes, our only viable choice left is covid becoming endemic. It didn’t have to be this way, but our leaders MADE a choice.
And now they need to make another choice: They need to choose an “acceptable” level of COVID death & disease.
I recently wrapped up a big project over here at the COVID-19 Data Dispatch. (In case you missed it: I profiled five school communities that had successful reopenings in 2020-2021. Check out the project here!) Now that it’s done, I’ve been doing a bit of reflecting on the next steps for this publication—specifically, what I’d like it to look like one year from now.
My mission here is to provide you, my readers, with the information you need to understand what’s going on with COVID-19 in your community. I’m committed to covering the pandemic, for as long as it remains the number one health and science story in America.
But what happens when COVID-19 is no longer the number one health and science story in America? I started to consider this question early in summer 2021, before Delta came roaring in—and made many people realize that we were still pretty far away from the “end of the pandemic.” Delta allowed me to procrastinate, basically. But this is the kind of question one can only put off for so long, so here I am, considering it again.
As I think about the COVID-19 Data Dispatch’s future, I’m thinking about everything that this country needs to do in preparation for the next public health crisis. Because there will be a next public health crisis—in fact, climate change is already producing a never-ending stream of crises all around us. What information do we need, and what data-driven stories can we tell, to get ready? How can I serve my fellow journalists, scientists, health experts, and the other people in my community?
To help me figure this out, I’ve put together a survey for you, dear readers! It should be easy to fill out: 10 questions, mostly multiple choice. It can be done on a computer or a phone, and shouldn’t take you more than five minutes.








{kind=link}