In the last week of December, I had a major story published at MuckRock, USA TODAY, and local newsrooms in Arizona, Oregon, and Texas. The story explains that official COVID-19 statistics underestimate the pandemic’s true toll—particularly on people of color, who are more likely to have their deaths inaccurately represented in mortality data.
We already knew that the COVID-19 pandemic widened existing health disparities in the US. But the official statistics only show a piece of COVID-19's true toll.
This story was part of Uncounted, MuckRock’s broader project to investigate death certificate errors and other death reporting issues uncovered by looking at all excess deaths during the pandemic, not just those deaths officially marked as COVID-19. It relies on data from the CDC’s provisional mortality statistics and excess death estimates by a team of demography researchers at Boston University led by Andrew Stokes.
I’ve copied the introductory section of the story here, because I don’t think anything else I write would do a better job at summarizing it. I encourage you to read the full piece; it is the biggest (and likely most important) story that I wrote in 2022.
It’s not always easy to identify a COVID-19 death.
If someone dies at home, if they have symptoms not typically associated with the disease or if they die when local health systems are overwhelmed, their death certificate might say “heart disease” or “natural causes” when COVID-19 is, in fact, at fault.
New research shows such inaccuracies also are more likely for Americans who are Black, Hispanic, Asian or Native.
The true toll of the COVID-19 pandemic on many communities of color – from Portland, Oregon, to Navajo Nation tribal lands in Arizona, New Mexico and Utah, to sparsely populated rural Texas towns – is worse than previously known.
Incorrect death certificates add to the racial and ethnic health disparities exacerbated by the pandemic, which stem from long-entrenched barriers to medical care, employment, education, housing and other factors. Mortality data from the Centers for Disease Control and Prevention point to COVID-19’s disastrous impacts, in a new analysis by the Documenting COVID-19 Project at Columbia University’s Brown Institute for Media Innovation and MuckRock, in collaboration with Boston University’s School of Global Public Health; the USA TODAY Network; the Arizona Center for Investigative Reporting; Willamette Week in Portland; and the Texas Observer.
The data shows that deaths from causes the CDC and physicians routinely link to COVID– including heart disease, respiratory illnesses, diabetes and hypertension–have soared and remained high for certain racial and ethnic groups.
In Arizona’s Navajo and Apache counties, which share territory with Navajo Nation, COVID deaths among Native Americans drove nation-leading excess death rates in 2020 and 2021. While COVID death rates among Natives dropped during the second year of the pandemic thanks to local health efforts, other causes of death such as car accidents and alcohol poisoning increased significantly from 2020 to 2021.
In Portland, deaths from causes indirectly related to the pandemic went up in 2021 even as official COVID deaths remained relatively constant. Black residents were disproportionately impacted by some of these causes, such as heart disease and overdose deaths – despite a county-wide commitment to addressing racism as a public health threat.
In Texas, smaller, rural counties served by Justices of the Peace were more likely to report potential undercounting of COVID deaths than larger, urban counties served by medical examiners. Justices of the Peace receive limited training in filling out death certificates and often do not have sufficient access to postmortem COVID testing, local experts say.
Experts point to several reasons for increased inaccurate death certificates among non-white Americans. These include resources available for death investigations, the use of general or unknown causes on death certificates, and how the race and ethnicity fields of these certificates are filled out.
Such barriers to accurate death reporting add on to existing health disparities that made non-white Americans more susceptible to COVID in 2021, despite widespread vaccination campaigns and health equity efforts.
“Even if you try to level the playing field, from the jump, certain populations are dealing with things that put them at greater risk,” said Enrique Neblett, a health equity expert at the University of Michigan’s School of Public Health. These issues include higher exposure to COVID, as people of color are overrepresented among essential workers, as well as higher rates of chronic conditions that confer risk for severe disease. “Those things aren’t eliminated just by increasing access to a vaccine,” Neblett said.
It is critical to improve data collection and reporting for deaths beyond those officially labeled as COVID because data is a “major political determinant of health,” said Daniel Dawes, executive director of the Satcher Health Leadership Institute at the Morehouse School of Medicine. Information on how people are dying in a particular community can shape priorities for local public health departments and funding for health initiatives.
“If there is no data, there is no problem,” Dawes said.
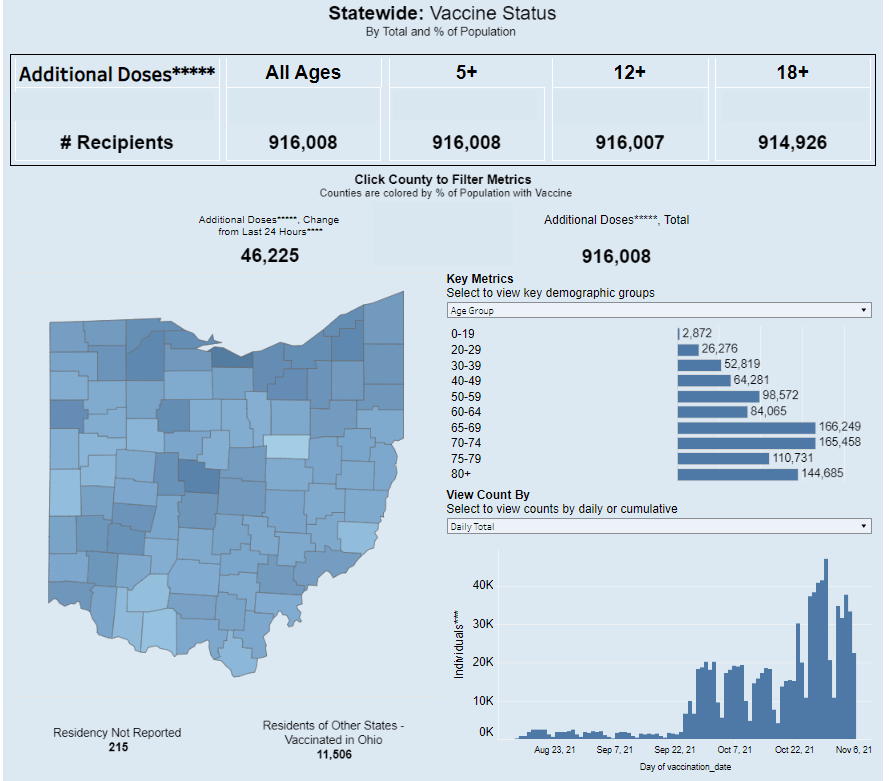
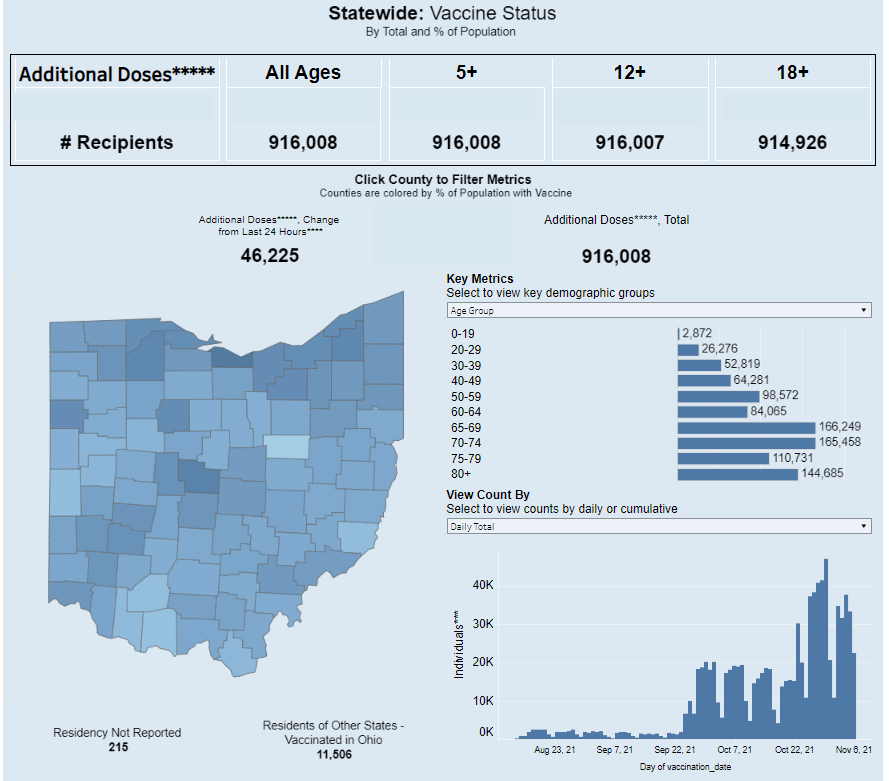
Ohio is one of just eight states reporting demographic data for booster shots administered in the state. Screenshot taken on November 7.
It’s now been over a month since the FDA and the CDC authorized third doses of Pfizer’s COVID-19 vaccine for a large swath of the U.S. population, and a couple of weeks since the agencies did the same thing for additional doses of Moderna and Johnson & Johnson’s vaccines. In that time, over 20 million Americans have received their boosters.
This weekend, I set out to see what data are now available on these booster shots. I updated my vaccination data in the U.S. resource page, which includes detailed annotations on every state’s vaccine reporting along with several national and international sources.
The majority of states (and national dashboards) are now including booster shots in their vaccine reporting, I found. But in most cases, the reporting stops at just one statistic: the total number of residents who have received an additional dose. A few states are reporting time series information—i.e. booster shots administered by day—and a few are reporting demographics—i.e. booster shot recipients by age, gender, race, and ethnicity—but these metrics are lacking across most dashboards.
Demographic information, particularly race and ethnicity, should be a priority for booster shot data, as it should be for numerous other COVID-19 metrics. At the beginning of the U.S.’s vaccine rollout, Black and Hispanic/Latino Americans lagged behind white Americans in getting their shots, but limited data hindered the public health system’s ability to respond to this trend. (Now, the trends have evened out somewhat, though Black vaccination rates still lag white rates in some states.)
Will we see the same pattern with booster shots? Considering the immense confusion that has surrounded America’s booster shot rollout in the last couple of months, it would not be surprising if disadvantaged communities are less likely to know about their potential need for a booster, or where and how to get those shots.
But so far, we don’t have enough data to tell us whether this pattern is playing out. The CDC has yet to report booster shot data by race or ethnicity, though the agency is now reporting some figures by age and by state. Note: the CDC still has yet to report detailed vaccination data by race and ethnicity, period; the agency just reports national figures, nothing by state or other smaller geographies.
At the state level, just eight states are reporting booster shots by race and ethnicity. 13 states are reporting some kind of time series (boosters administered by day or week), and three are reporting doses administered by vaccine manufacturer.
Here are all the states that I found reporting booster shot data, with links to their dashboards:
Wyoming: Total boosters and doses administered by manufacturer.
Local reporters: If your state is reporting demographic data, I recommend taking a look at those numbers. How does the population receiving booster shots compare to the overall population of your state, or to the population that’s received one or two doses? And if your state is not reporting demographic data (or any booster data at all), ask your public health department for these numbers!
I recently had the opportunity to discuss data equity with Dr. Debra Furr-Holden, a public health expert at Michigan State University. Dr. Furr-Holden is the university’s Associate Dean for Public Health Integration and Director of the Flint Center for Health Equity Solutions, a health research center focused on Flint, Michigan, where she is based.
At one of my National Science-Health-Environment Reporting Fellowship training sessions, Dr. Furr-Holden spoke about the Flint water crisis and other health equity issues. Her comments made me think about continued issues in COVID-19 data collection and reporting, so I asked her to discuss COVID-19 data further in an interview for the CDD.
We talked about the ongoing challenges of collecting and reporting COVID-19 race data, how data gaps fuel vaccine hesitancy, the equity challenges inherent in vaccine mandates, and more.
The interview below has been lightly edited and condensed for clarity.
Betsy Ladyzhets: First, I’m curious about your backstory, how you got involved in doing this kind of [health equity] work.
Dr. Debra Furr-Holden: I think it probably was born out of my own lived experience. My dad died at 37, of a complication from hypertension. My mom died at 56 of an asthma attack.
It wasn’t until I went to college that I realized that my peers had very different experiences. I went to college with no living grandparents and one living parent, and I just assumed everybody had relatives with, you know, amputated limbs and with diabetes and heart disease. And I realized that’s not the case.
As I networked with the very small cohort of African-American students in my class, I noticed despite our socioeconomic backgrounds—because I came from sort of more humble beginnings than some of my Black and brown peers—I was like, Oh, [these health conditions are] over-represented in black and brown people.
BL: How has that informed the work that you’ve been doing with COVID? I saw that you’ve been advocating for better vaccine access and stuff like that?.
DFH: What I’ve realized is, a lot of what we do around disparities, we do to people, and for people, and on their behalf. But the populations most affected very rarely have a voice, and the solutions that get created and implemented and employed—and we saw it with COVID, we’re seeing it now.
The President has made a national declaration, give everybody $100 for the newly vaccinated. And that doesn’t make sense to a lot of people. People who are having trouble paying for their hypertension medication or their other things are now being told, we’ll give you $100 to get this COVID vaccine. When earlier in the pandemic, those same people couldn’t get access to a COVID test.
BL: And in some cases, probably still can’t get access to a COVID test.
DFH: Yeah. And I’ve just realized, like, my own lived experience that is ongoing still informs my work, but it elevated my authentic and deep appreciation for how important the voice of community and affected populations is in the work. It’s not just about the data. It’s not just about the science… You can only glean but so much from a data table. You need more wind underneath that. And that wind is the voice of community, and the voice of the people that you’re trying to impact and serve.
So, the big gap to me in our work around how to bridge this gap among the unvaccinated is: we are quantifying who is unvaccinated, but we’re not asking the question of, what is needed to bridge that gap for you to get the vaccine? Instead, I think we’ve got a lot of well-meaning people who are coming up with solutions, but those solutions are not mapping onto people’s concerns. And it’s not moving the needle.
In Ohio, they offered this big lottery, it did not cause a big boom in vaccination. Same thing is happening in Michigan right now. It did not rapidly accelerate the pace of newly vaccinated people. And because my work is so community engaged, when I talk to people and they tell me the reasons underneath [their vaccination choice], it’s not about the money.
I call the money the carrot. We’ve tried to dangle the carrot in front of people. That didn’t produce much. Now we’re using the stick.
BL: The mandates.
DFH: The mandates, yeah. That will likely produce more [vaccination] than the carrot did, because people will have their hands forced. But that will likely elevate resentment and give way to—any negative consequences or outcomes that come from people being forced into vaccination will likely only further fuel their mistrust of the healthcare system, and our government overall. I just feel like the solutions are not being informed by the people that we’re trying to get on board.
BL: Yeah. What kind of information do we need to actually inform better solutions, do you think?
DFH: We need to hear from the very large and diverse pool of unvaccinated people. Because there’s no one solution here.
Now, I do believe fundamentally, as a public health professional, I think of public health big population-level interventions that make health choices easy. So things like fluoride in drinking water. We don’t [remember] the time when the cavities and dental cavities were contributing to all of this excess death and morbidity. Why, because we got fluoride in drinking water. So it’s just a non-starter for us now. Same thing for standardized childhood immunizations, which were transformative for eradicating diseases that took millions of lives before we not only developed those vaccines, but made them a part of the standard immunization protocol for children.
We’ve now got to do the work to figure out how to implement and integrate these COVID protections into our system of care, and have them be more normative. I think all of the mistakes around how the whole pandemic has been handled in the US—how the resources, not just the vaccine, but other resources, like payroll protection, enhanced unemployment, support for essential workers.
You know, we weren’t providing PPE to essential workers in the beginning. We had national leaders saying you don’t have to wear a mask. All of these things now conflict with, “Oh, we care so much, and everybody has to get vaccinated. Everybody needs to take one for the team.” People just aren’t buying into that.
BL: They think there’s something else going on, I guess. So, I know, when we were closer to the start of the vaccine rollout, like earlier in 2021, I saw a lot of press attention on the lack of demographic data on vaccinations. A couple of my colleagues at the COVID Tracking Project wrote an article in The Atlantic and there was other kind-of big name publication stuff. But now we still don’t have good data. And it seems like no one is really drawing attention to that. I’m wondering if you have any thoughts on this, and if there’s anything we can do to continue that pressure, because we still do need this information.
DFH: Yeah, it’s unfortunate, because I always say a lack of data continues to fuel the debate. And the lack of quality data around COVID resources is only fueling the problem. It is an unnecessary and unacceptable omission for providers to administer COVID tests and not collect basic demographic data on the people that they’re testing. It dampens our ability to quantify who is most impacted and what should be the targets of our outreach, engagement, and intervention efforts. And it’s unnecessary and unacceptable.
In Michigan, the system that we use is called MICR… It would take a programmer about eight seconds to make race, and ZIP code, and gender, and age category a required field to be entered. And we just simply haven’t done it. And so as a result, it’s hard for us to quantify the extent of a problem.
Because, remember, COVID cases are only a function of COVID testing. You can only get identified as a COVID case as a function of having a COVID test. If you’re in a household, and there’s a known case in the household, and all of the other [household] members display classic COVID symptoms, if they don’t get a test, they don’t get counted anywhere. So we know that we’ve greatly underestimated the extent of the problem.
BL: When I asked you about this at the SHERF session, you mentioned that there’s a provision in the CARES Act that requires providers to do this [data collection]. Can you talk more about that? And what we can do to actually have some accountability there?
DFH: Yes. There is a provision in the CARES Act that all COVID testing providers have to collect these core demographic variables. And then there was follow up guidance that was issued. And when the new administration took office, they haven’t enforced that [guidance].
So COVID testing providers continue to receive these resources to provide COVID testing, with no quality assurance or quality control, to ensure that they’re actually collecting and entering that demographic data. It then shifts the responsibility to backfill that information to local health departments and other providers, to try to link insurance records or electronic health records. Or even worse to do outreach and contact tracing and actually contact cases, by phone or by email to try to backfill that information. When there are so many other competing demands, it’s an unfair and undue burden to place on an already overstressed segment of our healthcare system.
What it’s akin to is gums without teeth. We have the law, but there’s no enforcement or compliance checks to ensure that that law is being honored. And I think a simple solution is compliance checks. We need compliance checks, and we need enforcement.
BL: Do you have any thoughts on other stories that we should be telling? Like, what should I tell my journalist friends to cover around COVID and health equity?
DFH: One thing is probably already on your radar, which is the fact that we’re not doing systematic genetic sequencing on current strains of COVID. So it’s hard to estimate, you know—people keep talking about the Delta variant, but we have thousands of variants of SARS-CoV-2 now. And we just don’t have a good system for genomic surveillance to understand them.
And the CDC a few weeks ago said, we’re just going to stop doing the genomic sequencing on any kind of systematic level and reporting. It’s a problem, because with breakthrough cases, and
the vaccinated now showing up in hospitals and emerging data saying that even if you’re vaccinated, you can still spread and transmit… I just had a conversation with somebody who works in our building who said, I don’t want to get vaccinated, because if I get COVID, I want to have symptoms, so I’ll know, so I can protect my nine-year-old who’s got asthma. Like, I want to know. A lot of people now feel like the vaccine increases the chances of them being an asymptomatic carrier.
We just really have to collect data. Instead of mandating shots in arms, we should be mandating the data so that we have better information and can do more credible and transparent information dissemination to communities.
BL: Yeah, so that we can actually answer people’s questions on these things.
DFH: Yeah.
BL: I was also wondering if you had any recommendations, either of good stories that do a good job of covering these issues we’ve been talking about, or data sources or resources that myself and other journalists in this space should be paying attention to.
DFH: We should be putting the press on the CDC to collect and compile the data. Like, the data on cases, all of that data should be disaggregated by race. And the percentage of cases with unknown race or unknown gender or unknown geography should also be reported. Because I don’t know if people notice this, but a lot of times [the CDC is] presenting data only on cases with complete information. But the missing information points to something important as well.
BL: I think it’s something like they have maybe 50% or 60% of cases with known race. But where’s that other share of cases? [Editor’s note: It’s 63%, as of August 14.]
DFH: The assumption is that the distribution of these variables in the unknown is similar to that of the known. But it is a major assumption. And it’s not an assumption that we should be making.
BL: I see. Yeah. Anything else [you’d recommend as a story idea]?
DFH: I do like this carrot stick analogy. The carrot is not working, the dangling the big incentive is not working. The stick will likely work. If you tell people, “You can’t get on a plane, if you’re unvaccinated,” there will be a lot of people who are unvaccinated right now who will get vaccinated because they’ll not want to lose the opportunity to travel.
Think about the media. If you are chasing a story, or if you’ve got to be on site for something… If you’re in New York and you’ve got a story in California, you’re not going to drive to California, you will likely get off the fence and get vaccinated.
I feel like a larger problem is, we have to engage experts in the work to make sure that we’re not furthering inequity [with mandates]. Because if we use, now, the stick, and start to mandate it…. [Michigan State University] has now mandated vaccination for all faculty, staff and students who want to return to campus by September 7. I know that that will likely produce greater increases in vaccination than did the incentives of cash payments, or lotteries or other things.
But we have to keep an eye toward equity, and make sure—what if there’s disproportionality and then who does that impact? Are we going to see an increase in Black and brown people, or people with disabilities, or people with chronic health conditions, losing their jobs, or dropping out of school, or some of these other things? There just needs to be more thoughtfulness to how we apply these policy interventions to make sure that it’s not furthering inequity.
BL: Have you seen any examples of where that’s been done successfully?
DFH: No, because it’s all just coming out now.
BL: I know there are some places, like in New York, they’re giving you an option, saying, “You can get vaccinated or you have to be tested once a week.” Is that effective? Or does that still fit into what you’re talking about?
DFH: I think we’re gonna figure that out. And if that’s the case, then again, we gotta deal with the access issue, and people need to have fair and equitable access—and affordable access—to COVID testing.
BL: Yeah, totally. And the last kind of big question I had for you: one thing I think a lot about as a journalist who is still rather early-career and has been covering COVID very intensely is that this is probably just the beginning of us dealing with major public health crises. You know, continued climate disasters and all that stuff.
And I’m wondering how you think about preparing for the next COVID, or the next whatever it’s going to be. What lessons do we take from these past couple of years?
DFH: Well, I think we’ve learned there is a business case for preparedness, and a business case for equity. Our lack of preparation for this pandemic will have cost our country tremendously. There’s going to be tremendous financial toll. So, there’s a business case to be made for preparedness.
We learned that with the Flint water crisis. Not having the million-dollar investment in the water treatment system, not spending the 150 bucks a day on anticorrosives, those things will have cost us hundreds of millions of dollars to now replace and repair the whole water infrastructure system and pay settlements from the Flint water crisis.
And then there’s also a business case for equity. Not doing a better job of equitably rolling out the vaccine early on caused a lot of people who were a “yes” to sort of say, “why bother?” And now many of them are a “no.” These are people who earlier on [were amenable], but then all these reports come out and get sensationalized by the media of side effects and blood clots and heart inflammation. And so a lot of people who were in line, trying to move through the line to get vaccinated are now an absolute “no.”
That’s going to cost us as well, because we have fallen well short of that 70% goal. And new vaccinations are moving at a snail’s pace. So I think what we’ve learned—and we’ll really know, the impact of it in the next few years—is not being prepared and not practicing equity will have a tremendous financial toll on the country.
Screenshot of the Health Equity Tracker showing which states are missing race and ethnicity data for COVID-19 cases.
Two weeks ago, a major new COVID-19 data source came on the scene: the Health Equity Tracker, developed by the Satcher Health Leadership Institute at Morehouse School of Medicine.
This tracker incorporates data from the CDC, the Census, and other sources to provide comprehensive information on which communities have been hit hardest by COVID-19—and why they are more vulnerable. Notably, it is currently the only place where you can find COVID-19 race/ethnicity case data at the county level.
I featured this tracker in the CDD the week it launched, but I wanted to dig more into this unique, highly valuable resource. A couple of days ago, I got to do that by talking to Josh Zarrabi, senior software engineer at the Satcher Health Leadership Institute—and a fellow former volunteer with yours truly at the COVID Tracking Project.
Zarrabi has only been working on the Health Equity Tracker for a couple of months, but he was able to share many insights into how the tracker was designed and how journalists and researchers might use it to look for stories. We talked about the challenges of obtaining good health data broken out by race/ethnicity, communicating data gaps, and more.
The interview below has been lightly edited and condensed for clarity.
Betsy Ladyzhets:Give me the backstory on the Health Equity Tracker, like how it got started, how the different stakeholders got involved.
Josh Zarrabi: At the beginning of the pandemic, the Satcher Health Leadership Institute at Morehouse School of Medicine saw the lack of good COVID data in the country, and especially the lack of racial data. The COVID Tracking Project kind-of tried to solve that as well with the Racial Data Tracker.
Morehouse wanted to do something similar. And so they applied for a Google.org grant… After about nine months, the tracker just got released. It went through a couple of different iterations, but what it is now is, it’s a general health equity tracker, so it tracks a couple of different determinants of health. And it really has a focus on equity between races and amplifying marginalized races as much as possible.
Probably the most innovative thing it does is, it shows COVID rates by race down to the county level. We think that’s relatively hard to find anywhere else. (Editor’s note: It is basically impossible to find anywhere else.) So that’s probably like the main feature that it has that people care about, but it does track other health metrics. We also have poverty, health insurance, and we try to track diabetes and COPD, but there’s not great data on that, unfortunately, in the United States. We’re planning to add more metrics in the future.
BL: How does this project build on the COVID Racial Data Tracker? And I know, like APM has a tracker for COVID deaths by race. And there are a couple other similar projects. So what is this one doing that is taking it to the next level?
JZ: A couple of things. We’re using the CDC restricted dataset. Basically what the dataset looks like is, it’s like a very large CSV file where every single line is an individual COVID case. So we’re able to break it down basically however we want. So we were able to break that down to the county level, state level and national level.
And what we do is we allow you to compare that [COVID rates] to rates of poverty, and rates of health insurance in different counties. We think that’s pretty innovative, and we’re gonna allow you to compare it to other things in the future. So that’s one thing that we do. And I mean, the second thing that I would say is like, probably makes us stand out the most I would say is our real focus on racial equity, and showing where the data gaps are and how that affects health equity. So what you’ll notice, if you go to our website, we very prominently display the amount of unknown…
BL: Yeah, I was gonna ask you about that, because I know the COVID Racial Data Project had similar unknown displays. Why is it so important to be highlighting those unknowns? And what do you want people to really be taking away from those red flag notes?
JZ: We really try to do our best to display the data in context as much as possible. First of all, the most important thing, I think, is just showing the high percentage of unknown race and ethnicity of COVID cases in the United States. For something like 40% of cases, we don’t know the race and ethnicity of the person who had COVID.
We want people to really think about that when they look at, for example, you’ll notice that it looks like Black Americans are affected to the exact level of their population. Black Americans look like 12% of the population and 11% of cases. But we don’t know the race of 40% of people who have COVID. And so we really wanted people to think about that when they look at these numbers. And it’s the same for American Indian/Alaskan Native populations. It doesn’t look like they’re that heavily affected in the United States. But that’s why we allow you to break down into the county level, where race is not being reported. And so we really want people to look and say, like, oh, wow, like in Atlanta, 60% of cases are not being counted for race and ethnicity.
We’re not doing any extrapolation. We’re not multiplying, we’re not like trying to guess the races of unknowns, or anything like that. We really want people to think about that, when they’re saying like, oh, wow, it looks like Native American people are not really heavily affected by COVID. It’s like, no, we just don’t know. We don’t know their races, or those people are just not being reported properly by the health agencies.
And if you look at places that have high percentages of Black Americans and high percentages of American Indian/Alaskan Natives, you’ll see that those places are the same places that are not reporting the race and ethnicity of the people who had COVID.
We had a team of about 20 health equity experts advising us throughout the entire project. That’s where those red flags that you see come from. It’s explaining, for example, if you look into deaths for Native American and Alaska Natives, there’s an article about how a lot of American Indian/Alaskan Native people who died are not, are improperly categorized racially, and they’re often categorized as white. And so we have that kind of stuff to really try to put the numbers in context.
We were only able to do that, because we had this large team of racial equity experts and health equity experts advising us throughout the entire time. And so we really had diverse representation on the project as we were building it, and people who really knew what they were talking about.
BL: What can public health agencies and also researchers and journalists do to push for better data in this area?
JZ: The good thing is we are seeing [data completion] get better over time. And so we’ve seen, for example, the percentage of race and ethnicity for cases improved from about 50% to about 60% over the last couple of months.
And, I mean, really, all you can do is—it’s really a thing that goes down to the county level. So, everybody’s just got to call their county representatives. I’d be like, hey, could you please report the race and ethnicity of the county’s COVID cases to the CDC? Unfortunately, a lot of that work might be too late, because [data were submitted months ago]. But we have seen it get better. And so we’re hoping that, you know, these health agencies are able to do the work and really, like, properly report these cases to the CDC…
BL: ‘Cause a lot of it comes from the case identification point, where if you’re not asking on your testing form, what race are you, then you just might not have that information. Or you might be, like, guessing and getting it wrong or something, right?
JZ: Yeah, there’s guessing. There’s two different categories of unknown cases—there’s unknown and there’s missing. The vast majority of these cases have filled out unknown [in the line file], which means that the person who’s filling out the data form literally puts “unknown” as the race. We don’t really know exactly what that means in every case. But it could be they didn’t ask, it could be the person didn’t feel comfortable saying it, just said, “I don’t want to tell you my race.” Or it could just be that they just didn’t make an effort to figure out what their race is.
BL: Do you have a sense of how that 60% known cases compares to what the COVID Racial Data Tracker had in compiling from the states?
JZ: Yeah, I think the COVID Racial Data Tracker was a bit higher [in how many cases had known race/ethnicity]. But the thing is, as far as I understand, the COVID Racial Data Tracker was using aggregate numbers.
BL: We were looking at the states and then kind-of like, synthesizing their data to the best of our ability, which was pretty challenging because every state had slightly different race and ethnicity categories. There were some states that had almost no unknown cases, but there were some where almost all cases or almost all deaths were unknown. New York, I don’t know if they ever started reporting COVID cases by race.
JZ: They do to the CDC, I don’t think they report—
BL: They don’t report it on their own, state public health site.
JZ: Let me actually check that… Yeah, so New York is not great. They have a 60% unknown rate. [Race and ethnicity is only reported to the CDC for 40% of cases.] Not great. Actually, New York City is pretty good. But the rest of New York State is not doing a good job reporting the race and ethnicity of cases.
BL: Because I’ve gotten tested here, I know that New York City is good about collecting that [race and ethnicity] from everybody.
JZ: I was one of those cases in New York City, actually. When [I got called by a contact tracer], I was kind of chatting with them about this. They asked me about my race—I actually became a probable case for COVID, like, the day after I started this job. And [NYC Health] called me, they were like, “What’s your race?” I was like, “Oh, that’s kind of funny, I just started working on this racial data project.” And—this is totally anecdotal. But she told me, most people just refuse to report their race.
And then for deaths… 40% of COVID deaths in New York state, they don’t know the race, which is not great. New York is not good compared to the rest of the states. It’s one of the worst states for unknowns.
JZ: The process of getting it’s not that hard. You just apply, and then they give you access to a GitHub repo, and then you can just use it. Using the data itself is pretty hard because the data files are so large. We were lucky enough to have a team of Google engineers working on this project, they wrote a bunch of Python scripts that analyze the data and aggregate it in a way that the CDC isn’t doing.
The reason why they restrict the use is because it’s line-by-line data. [Each line is a case.] And the CDC does suppress some of the data because they think it would make those cases identifiable. Still, you’re not allowed to just, like, release the data into the wild, because they want to know who else has track of it. So, we wrote some Python to aggregate the data, in exactly the way you see on the website. We aggregate it to the amount of cases, deaths and hospitalizations per county, per race, essentially.
The CDC has been extremely helpful, like, we’ve had a couple of meetings with them. We think we were one of the heaviest users of the data at the beginning, because we pointed out a couple of problems with the data that they actually fixed. So, that’s cool.
BL: That’s good to hear that they were responsive.
JZ: Yeah, definitely. We meet with them every couple of weeks. They’re really good partners in this.
BL: And they update that [case surveillance] dataset once a month?
JZ: They started doing it every two weeks now. Every other Monday, they update the dataset.
BL: Could you talk more about the feature of the tracker that lets you compare COVID to other health conditions and insurance rates? I thought that was really unique and worth highlighting.
JZ: We wanted to really provide the [COVID] numbers in context. And so that’s one way that we thought that we could do that and really show how… These numbers don’t happen, like a high rate of COVID for race doesn’t happen in a vacuum. There are political determinants of health.
For example, you’ll see everywhere that Hispanic Americans are just by far the most impacted by COVID case-wise. In California especially. And we provide those numbers in context—Hispanic Americans are also much less likely to be insured than white Americans, for example, and much more likely to be in poverty. And, you know, it’s not a crazy surprise that they would also be more likely to have contracted COVID at some point.
[The comparison feature] was a way that we thought, we would just allow people to really view numbers in context and get a better understanding of what the political situation is on the ground with where these high numbers are happening.
BL: What are the next conditions that you want to add to the tracker?
JZ: I want to be careful, because we can’t make any promises. But we’re talking about adding smoking rates, maybe. [The challenge is] where we can find data that we can aggregate correctly.
BL: Right. Are you looking specifically for data that’s county level as opposed to state level?
JZ: Hopefully… It depends. I was pretty surprised by the lack of quality in, for example, COPD and diabetes data, where like, if you look at [the dataset], like it’s state level—but in most states, there’s not a statistical significance for most races.
BL: Wow.
JZ: For example, we use the BRFSS survey. [The Behavioral Risk Factor Surveillance System.] It’s a CDC survey. And as far as we can tell, it’s the gold standard for diabetes [data] in the country.
And if you look at, say, diabetes, for most states… There’s only, like, four states where Asian people are statistically significant in the survey to make any sort of guess about how many people have diabetes, which is pretty atrocious. But that [data source] is the best we could do, you know. Ideally, we would like to find places that do go down to the county level, but it’s hard.
For as paltry as the COVID data is, it’s much better than—as far as I’ve seen, like, the fact that there’s like a line-by-line database that the CDC provides, that you can really make all these breakdowns of, is a huge step ahead [compared to other health data]. I’m not like a data expert on this kind of stuff, I’ve just been working on this project for two and a half months. But as far as I’ve seen, that’s what the situation is.
BL: Yeah, I mean, that kind of lines up with what I have seen as well. And I bet a lot of it is a case where, like, a journalist could FOIA [the data] from a county or from a state. But that’s not the same as getting something that is comprehensive, line-by-line, from the CDC.
JZ: And we [the Satcher institute] don’t want to be a data collection agency, like the COVID Tracking Project or the New York Times is. I mean, we want this to be a sustainable project. And the COVID Tracking Project was not a sustainable project.
BL: Yeah, totally. I was there doing the [data entry] shifts twice a week, that’s not something we could have done forever.
JZ: Yeah, I was there, too. I always think, like, the COVID Tracking Project could only exist when there’s an army of unemployed people who are too afraid to leave their house.
BL: And volunteers who were like, yeah, sure, I’ll do this on my evenings and weekends.
JZ: Who, you know, you don’t want to leave, you’re too afraid to go, like talk to people. You want to stay home in front of your computer all day, and feel useful.
I’m sure you could find all the diabetes data by going to county and state health department websites, but it’s too much work. So we really want everything to come from federal sources, basically, that’s our goal.
BL: How are you finding that people have used the tracker so far? Like, do you know of any research projects that folks are doing?
JZ: We released it a couple weeks ago, and we haven’t really heard of any yet… But we hope people are looking at it. And we have a couple of meetings lined up with some interesting research groups and stuff like that. So hopefully, they’ll like it.
BL: Are there any specific statistics or comparisons or anything else you found in working on it that you would want to see explored further? Are there any stories that you want to see come out of it?
JZ: The high rates of unknown data in a lot of places, that really needs to be looked into. Because it’s just hard to make any conclusions about what’s going on if—I mean, in some states like New York, over 50% of cases are unknown. That’s a huge problem. And that’s definitely something that needs to be looked into, like, why that’s happening. And if there’s anything that can be done to change that [unknown rate.] The reason why I do think that it can get better is because the COVID Tracking Project racial data had higher completeness rates. And so they [the states] probably do know the races of people who got sick, but they’re just not reporting it for whatever reason.
And for me, something that’s really stuck out was the extremely high rates of COVID for Hispanic and Latino people, especially in California. If you look at them and compare them to white rates, it’s, like, the exact opposite pattern. So it kind of does look like Hispanic and Latino people were kind-of shielding white people from getting COVID, if you compare the numbers. That’s something I would look into, too, like, why that happened.
(Editor’s note: This story from The Mercury News goes into how the Bay Area’s COVID-19 response heightened disparities for the region’s Hispanic/Latino population.)
BL: And another question along the same lines, is there a specific function or aspect of the tracker that you would encourage people to check out?
JZ: The unknowns. Just, like, look into your county and see what percentage of cases in your county have reported race and ethnicity at all. I think you can really see how good of a job your county has done at reporting that data. I know I was kind-of shocked by that rate for the county like I grew up in, like, I know that they have the resources to [report more data], but they’re just not doing a very good job.
BL: How would you say this experience with tracking COVID cases might impact the world of public health data going forward, specifically health equity data, and how do you see the tracker project playing a role in that?
JZ: We really want this project to show the importance of tracking racial health data down to the county level or even lower than that. County is the best we can do right now, but we’d love to see city level or something like that. And again, I kind-of said this before—as much as was missing for the COVID data, it’s still better than the data that there is for most other diseases and other determinants of health. So we would like to see, like, more things able to be filled out on the tracker. We would like to be able to get more granular on more different determinants of health, so that we can see, for example, how poverty impacts health, or a lack of health insurance, or how diabetes and COVID are related down to the county level. You can’t really do that right now…
We want people to see that, A, there’s a lot of data missing. But B, even with the data that we have, we can see that there’s like a huge problem. And so we would like to be able to fill out the data more to really get a better picture of what’s going on. If we can see there’s a problem, we can make better policy to help and make these disparities not as stark.
For months, I’ve been calling on the CDC to release state-by-state demographic data on who is getting vaccinated. While the vast majority of states report this information themselves, the state data are completely unstandardized—making it difficult to perform comprehensive analyses or compare one state to another.
“The vaccine data that individual states are publishing replicate the patchwork nature of the other state-level COVID-19 data our teams have been compiling,” COVID Tracking Project leaders Alice Goldfarb and Erin Kissane wrote in The Atlantic in January.
While many more states are reporting vaccination demographics now than in January—Montana and Wyoming are the only two states that now fail to report vaccinations by race—the data continue to be patchwork and hard to analyze.
Bloomberg has devoted a small team to analyzing and presenting these data in the publication’s U.S. Vaccine Demographics Tracker. But Bloomberg isn’t making their underlying data public, so other journalists and researchers are unable to build on this work. And really, it shouldn’t be on journalists to standardize from a fragmented state-by-state landscape—it should be the work of the CDC.
That’s why I was thrilled when, this week, we finally got that data from the CDC. Well… sort-of.
The data indicate that, despite promises from the White House to prioritize vulnerable communities in the vaccination campaign, a lot of inequities persist: “KHN’s analysis shows that only 22% of Black Americans have gotten a shot, and Black rates still trail those of whites in almost every state.”
!function(){“use strict”;window.addEventListener(“message”,(function(a){if(void 0!==a.data[“datawrapper-height”])for(var e in a.data[“datawrapper-height”]){var t=document.getElementById(“datawrapper-chart-“+e)||document.querySelector(“iframe[src*=’”+e+”‘]”);t&&(t.style.height=a.data[“datawrapper-height”][e]+”px”)}}))}();
In some states, white residents have been vaccinated at almost twice the rate of Black residents. In Iowa, for example, 15% of the Black population has received at least one dose—compared with 37% of the white population. Other states with high disparities include Florida, New Hampshire, Maine, Wisconsin, New Jersey, New York, Hawaii, and Connecticut.
Hispanic/Latino vaccination rates also lag behind the rates for white residents in some states, but the disparities are not as drastic as those for the Black population. Nationwide, 22% of Black Americans have received at least one dose, compared to 33% of white Americans.
Both Native Americans and Asian Americans have higher vaccination rates than the white population. Many tribes, in particular, have made dedicated efforts to promote vaccination.
And another hopeful caveat: vaccination rates for minorities have improved in recent weeks as the rate for white Americans goes down. In the last two weeks, about half of first doses administered in the U.S. have gone to people of color. This includes about 24% of doses going to Hispanic/Latino Americans, 10% going to Black Americans, and 8% going to Asian Americans.
The day after KHN’s analysis was published, Victoria Knight (another KHN reporter) asked CDC Director Dr. Rochelle Walensky whether the agency would add state-level race and ethnicity vaccination data to its dashboard.
“We have been updating our website,” Dr. Walensky said in response. “I can’t say that it’s daily; I believe that it’s weekly.”
And yet as of Sunday morning, May 23, state-by-state demographic data are nowhere to be found on the CDC’s site.
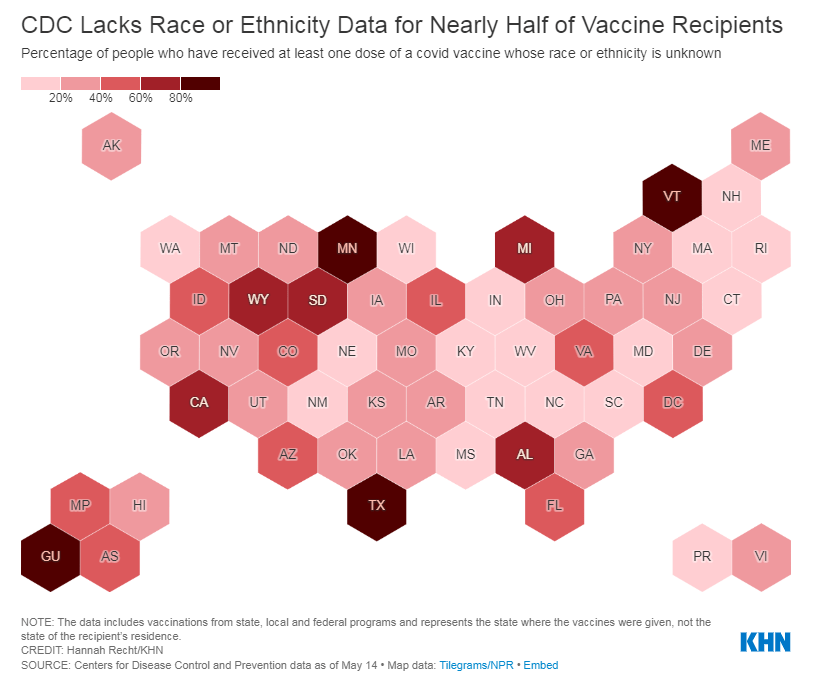
Knight also asked what the CDC is doing to address the high number of vaccinations for which demographic details are unknown. Race/ethnicity data are missing for about 44% of vaccinated Americans, meaning that true disparities may be even starker.
!function(){“use strict”;window.addEventListener(“message”,(function(a){if(void 0!==a.data[“datawrapper-height”])for(var e in a.data[“datawrapper-height”]){var t=document.getElementById(“datawrapper-chart-“+e)||document.querySelector(“iframe[src*=’”+e+”‘]”);t&&(t.style.height=a.data[“datawrapper-height”][e]+”px”)}}))}();
In some states, that unknown percentage is much higher than 44%. Eight states “either refuse to provide race and ethnicity details to the CDC or are missing that information for more than 60% of people vaccinated,” according to KHN. These states are excluded from KHN’s analysis as a result: they are Alabama, California, Michigan, Minnesota, South Dakota, Texas, Vermont and Wyoming.
Dr. Walensky told reporters the CDC is working with state and local public health departments to improve demographic reporting, but didn’t provide specifics.
In order to continue improving vaccination rates for minority communities, the CDC needs to actually make all of the agency’s data public. If state-by-state demographic data were easily available, researchers and reporters like me could more easily identify both the success stories and the disappointments—and help the states that are lagging catch up.
As Hannah Recht put it on Twitter: “we should not have to keep FOIAing for CDC state-level data that they could just put online if they wanted to.”
Following the end of the federal public health emergency in May, the CDC has lost its authority to collect vaccination data from all state and local health agencies that keep immunization records. As a result, the CDC is no longer providing comprehensive vaccination numbers on its COVID-19 dashboards. But we still have some information about this year’s vaccination campaign, thanks to continued CDC efforts as well as reporting by other health agencies and research organizations.
This week, the FDA authorized Novavax’s updated COVID-19 vaccine. Here’s why some people are excited to get Novavax’s vaccine this fall, as opposed to Pfizer’s or Moderna’s.
Last week, I asked you, COVID-19 Data Dispatch readers, to send me your stories of challenges you experienced when trying to get this fall’s COVID-19 vaccines. I received 35 responses from readers across the country, demonstrating issues with insurance coverage, pharmacy logistics, and more.
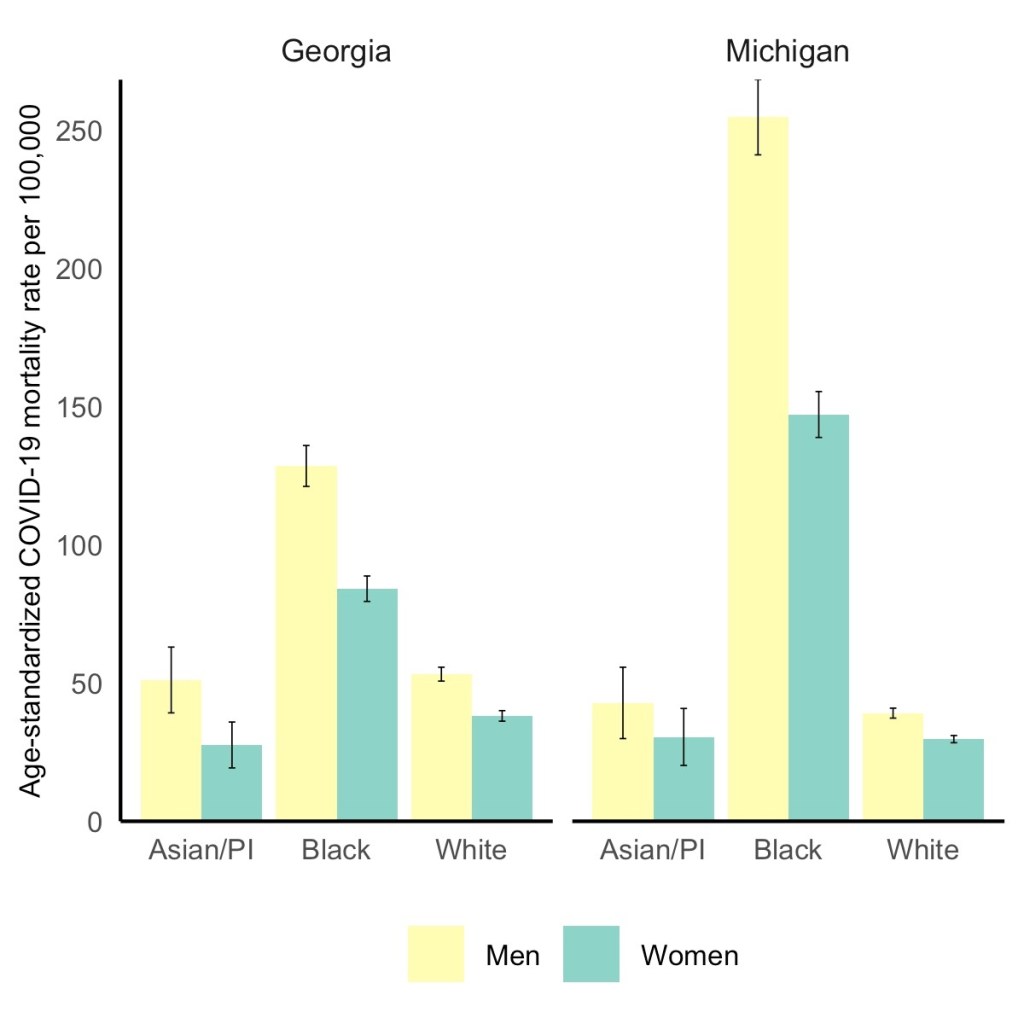
Black men have the highest COVID-19 death rate, but Black women die at higher rates than white or Asian men. Via the GenderSci Lab.
We’ve spent a lot of time in the COVID-19 Data Dispatch discussing how the COVID-19 pandemic has disproportionately impacted racial and ethnic minorities in the U.S., along with gaps and problems in the available data on this issue. (You can find past coverage here.)
A new study from the GenderSci Lab at Harvard sheds light on a more underreported side of the issue: how race and sex intersect in COVID-19 death rates. The lab has been tracking gender/sex and COVID-19 since April 2020, compiling data from states through a similar methodology to what the COVID Tracking Project did. And, similarly to the COVID Tracking Project, the GenderSci Lab faces challenges in producing a standardized dataset from 50 states that each have their own data definitions and reporting practices.
One of those challenges: very few states report COVID-19 data by both sex and other demographic factors, such as age and race/ethnicity. Such intersectional data are useful because they can provide more detailed information on who is most at risk from the disease, which may be tied to comorbidities and other social determinants of health.
For their recent study, GenderSci Lab researchers Tamara Rushovich et al. used data from the only two states that provide COVID-19 mortality data on sex, race, and age: Georgia and Michigan. The patterns they found in both states complicate the well-known trend that men are more likely to die of COVID-19 than women.
Black men have the highest death rate overall in Georgia and Michigan, significantly higher than white men. In Michigan, 254 out of every 100,000 Black men have died, compared to 39 out of every 100,000 white men. But the data also show that Black men and women both have significantly higher death rates compared with white and Asian men.
As the GenderSci Lab researchers note in a Twitter thread sharing this study, these data demonstrate that the sex difference in COVID-19 deaths is driven by comorbidities and social factors, not by some intrinsic, biological difference between men and women that makes men more vulnerable. Men may be less likely to wear masks or adhere to social distancing precautions, for example, and Black Americans are disproportionately represented in essential jobs and in incarcerated populations.
The researchers say that more data on this topic are needed (hello, other 48 states!) as well as more intersectional analysis:
There is an urgent need to understand why some men (often Black, Indig., and Latino) are so vulnerable to COVID, but we must recognize that many women (Black, Indig., and Latina) are much more vulnerable to COVID than many men (especially white men). @BlackFeministHS
Editor’s note, April 11, 6 PM: My friend (and CDD reader) Charlotte Minsky, who works on the COVID Racial Data Tracker, has pointed out that three states in addition to the two used in the GenderSci Lab’s analysis report COVID-19 mortality data by sex and race. Georgia and Michigan are the only two states to report by sex, race, and age; the researchers used age stratifications to calculate age-adjusted mortality rates. I’ve edited the post for clarification.
The CDC made two major updates to its COVID-19 data this week.
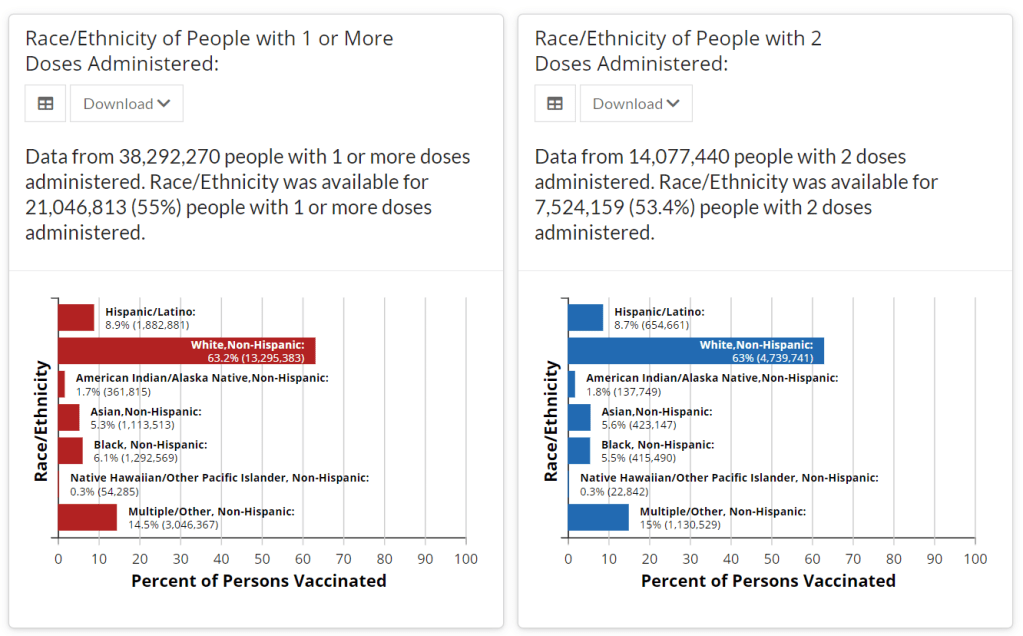
First: On Tuesday, the agency published a new dataset with more granular information on COVID-19 cases. Like previous case surveillance datasets, this new source compiles cases shared with the CDC, along with anonymized information on their symptoms, underlying medical conditions, race/ethnicity, and other variables. The new dataset is notable because it includes detailed geographic data, going down to the county level.
After months of no state-by-state demographic data from the federal government, we now have county-by-county demographic data. This is a pretty big deal! It’s also a pretty big dataset; it includes about 22 million cases (out of a total 30 million U.S. cases to date).
Of those 22 million cases, race is available for about 13 million cases (58%) and ethnicity is available for about 10 million cases (47%). The dataset will be updated monthly, so we may see better completion with further updates. I haven’t had time to do much detailed analysis of the new dataset yet (hell, I haven’t even managed to get it to load on my computer), but I’m excited to dive into it for future issues.
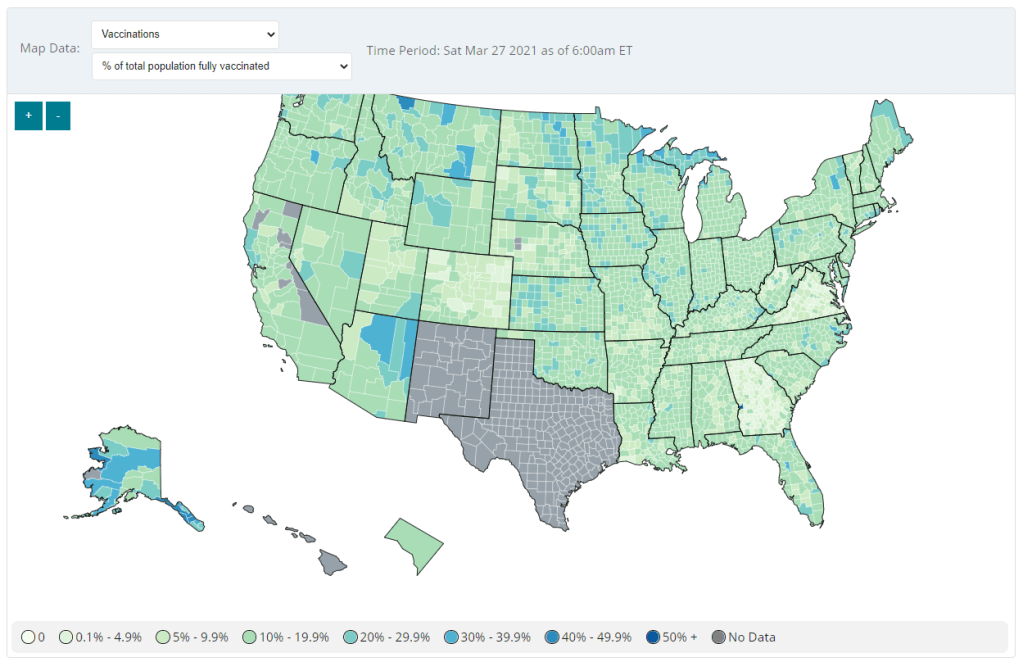
Second: Vaccination data at the county level are now available on the CDC’s COVID Data Tracker, as of Friday. No, not in the vaccinations section—you need to go to the County View section, then select “Vaccinations” in the dropdown menu. Click on a specific county (or select it using dropdown menus), and you’ll be able to see data for that county.
County-level vaccination data from the CDC. Screenshot taken on March 27.
At the moment, only three data points are available: total fully vaccinated population, fully vaccinated population over age 18, and fully vaccinated population over age 65. Also, data are missing for Texas, New Mexico, and select other counties. Still, this a great start for more standardized vaccination data at the national level. (Can we get more demographic data next?)
These county-level vaccination data aren’t downloadable directly from the CDC’s tracker, but the COVID Tracking Project is archiving the data at the Project’s public GitHub. The New York TImes has also built an interactive map with the data, which you can find on their vaccine tracker.
It’s worth noting that I found out about both of these updates via tweets from the White House COVID-19 Data Director, Cyrus Shahpar. I’m on both the CDC’s press list and the White House press list, and I watch nearly every White House COVID-19 press briefing, so it seems a little odd that I’m getting the news from Twitter.
(Not that I don’t love Cyrus’ daily tweets! I just wonder about the PR strategy here. Also, Cyrus, if you’re reading this, that interview request I sent back in January still stands.)
Drew Armstrong, Bloomberg News‘s senior editor for health care, talked about his work on the publication’s Vaccine Tracker; and Arielle Levin Becker, director of communications and strategic initiatives for the Connecticut Health Foundation, discussed how to navigate COVID-19 race and ethnicity data. Thank you to everyone who attended—we had a great turnout!
For those who couldn’t make it live, you can watch the recording of the session below. You can also check out the slides here. I’m also sharing a brief recap of the workshop in today’s issue.
In next Wednesday’s workshop, we’ll discuss engaging COVID-19 data providers, featuring Liz Essley Whyte (Center for Public Integrity), Tom Meagher (The Marshall Project), and Erica Hensley (independent reporter from Mississippi). If you aren’t registered for the series yet, you can sign up here.
The Bloomberg Vaccine Tracker
In his presentation, Drew Armstrong provided a behind-the-scenes look at Bloomberg’s tracker and shared some advice on analyzing vaccine data more broadly.
“We attempt to capture every vaccine dose that’s reported for COVID-19, every single day, around the world,” he said. In addition to the tracker’s daily updates on vaccine doses distributed and administered, the site also includes information on vaccine contracts between companies and countries—allowing a window into future distribution.
All of the data on the tracker comes from public sources, largely national and state public health departments that share figures via their own dashboards, press conferences, and social media. Like other aspects of pandemic data, these figures can be pretty messy. Every country, and even every state, may have its own definition of an “administered dose” or a “vaccinated individual”—and these definitions are evolving as the rollout progresses.
Armstrong provided one example: Tennessee reports “number of people with 1 dose only” vs. “2 doses,” and moves people from the first category to the second after they receive that second dose. Maryland, on the other hand, reports total people who have received one and two doses; both totals are always growing. It’s difficult to make apples-to-apples comparisons when every jurisdiction is doing something different. If you can, Armstrong said, actually get on the phone with your local official and make sure you understand precisely what the terms on their vaccine reports mean. When the Johnson & Johnson vaccine (which only requires one dose) starts rolling out, this definitional landscape will only get more complicated.
As a result of this messy data landscape, figures for the Bloomberg Vaccine Tracker are compiled manually by a huge team, including reporters from every bureau of the publication. “You have to really get your hands dirty with this data to understand it,” Armstrong said.
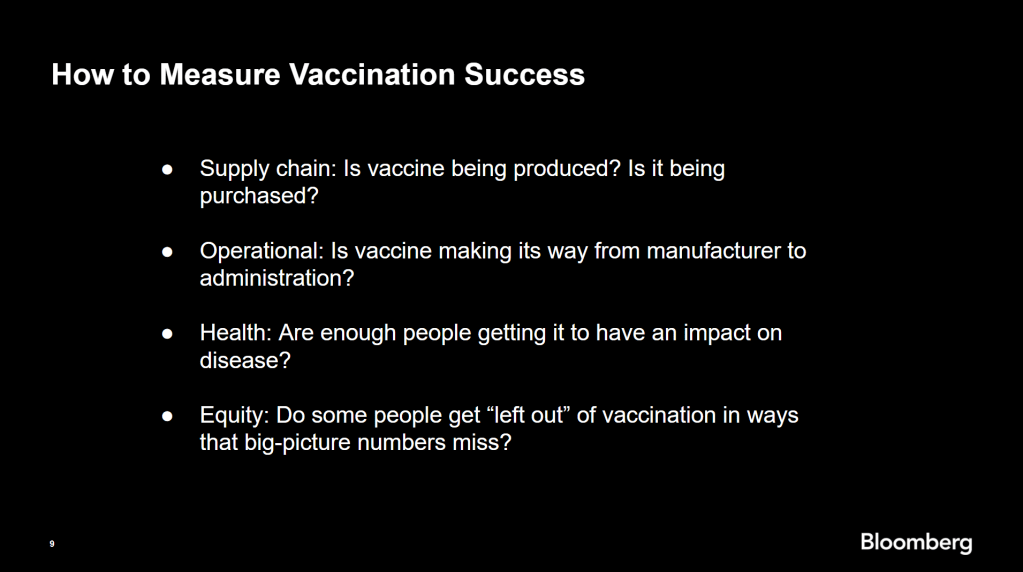
Armstrong also provided four ways for reporters to measure vaccination success. I’m including his slide here because I think it provides a good look at the multifaceted nature of vaccine data analysis and communication; your state might be vaccinating residents at a quick pace, but if the most vulnerable members of your community have been left out, you can’t fully call that rollout a success.
Slide from Drew Armstrong’s talk discussing the Bloomberg Vaccine Tracker.
On the equity front: Armstrong announced that the Bloomberg tracker now includes a demographic vertical. This tracker currently includes data from 27 states and two cities which are reporting vaccinations by race and/or ethnicity—you can check it out here. Bloomberg’s team is planning to update this tracker weekly, adding more states as their data become available.
Armstrong emphasized that he and his colleagues want their tracker to be a resource for other journalists, civic engagement, and other public health communication. “All of our DMs are open,” he said. (Or you can send feedback to the team through a public form.)
He also noted that reporting on these data—or even @-ing your governor on Twitter and asking them why the numbers aren’t better—is a useful way of actually making the data better. By letting public officials know that we’re looking at these numbers and noticing the gaps, we can put the pressure on for changes to be made.
Analyzing sources of race and ethnicity data
In her presentation, Arielle Levin Becker shared some strategies and resources for navigating a new data source—with a focus on demographic data.
“Data is incredibly important—and easy to misuse,” she said at the start of her talk. Vetting a source properly, she explained, can help you understand both how to properly use this source and how to address its limitations in your reporting.
Vetting questions to consider:
Who’s compiling this source?
Who’s funding it?
How transparent are they about their methods? Can you identify how it was compiled, or even track the chain of their methodology?
Do they disclose the limitations of the data?
Similarly to Armstrong, Levin Becker recommended reaching out to a source directly when you have questions. People who compile public data are often “very welcoming” about explaining their work, she said, and may be excited to help you better use their data.
Once you get to the analysis stage, Levin Becker suggested asking another round of questions, such as, “Do the numbers in this source match other numbers from similar sources?” and “How could I explain these numbers in plain English?” One particularly important question, she said, is: “What’s the denominator?” Does this analysis apply to everyone in a state or to a particular subset, like the over-65 population? As we’ve discussed before, denominators can be a particular challenge for COVID-19 school data—without enrollment numbers or clear data definitions, case numbers associated with schools are difficult to interpret.
Levin Becker honed in on age adjustment, a process that’s commonly used in health data analysis to compare outcomes for different populations. It’s kind-of a complicated statistical process, she said, but the basic idea is, you weight your data by the age distribution of a population. White populations tend to skew older than Black and Hispanic/Latino populations, for example; to compare these groups in a more equivalent way, a researcher might calculate what their disease rates would be if the different populations had the same age distribution.
Before the state of Connecticut started age-adjusting its COVID-19 death rates, Levin Becker said, the public health department was boasting that Hispanic/Latino residents of the state were less likely to die from the disease than white residents. But after doing an age adjustment, the state revealed that residents of color were actually at higher risk.
Slide from Arielle Levin Becker’s talk, showing how age adjustment can reveal health disparities. Chart is from the CT health department.
“The median age for a non-Hispanic white resident is 47 years,” Levin Becker said. “For a non-Hispanic Black resident, the median age is 34 years, and for a Hispanic resident, it’s 29 years.”
Finally, of course, there are many instances in which the lack of data is the story. There’s been a big focus on race and ethnicity data for COVID-19 vaccinations, but we’re also still missing data on other pandemic impacts. For example, the federal government and the vast majority of states don’t report COVID-19 tests by race and ethnicity. In a lot of cases, Levin Becker said, healthcare providers simply aren’t required to record the race and ethnicity of their patients—“it hasn’t been prioritized in health systems.”
When the COVID-19 pandemic is no longer an imminent crisis, she said, “keep poking at the questions of what’s being collected and how it’s used.” Continued advocacy by journalists and other communicators can keep the pressure on to improve our race and ethnicity healthcare data—and use it to reveal the disparities that must be fixed.
Related resources
A few links shared in the chat during this session:
The CDC continues to improve its vaccination reporting. The agency is now regularly reporting demographic data on its dashboard—including race, ethnicity, age, and sex. You can see counts for both U.S. residents who have received one and two doses. Like the rest of the CDC’s dashboard, the agency is updating these figures every day.
But when it comes to tracking who’s getting vaccinated in America, we still have a long way to go. Now that demographic data are becoming more available at the federal and state levels, equity advocates are pushing for more local data—vaccinations by county, by town, by ZIP code.
New York City data reporter Ann Choi, for example, pointed out on Friday that this city has lagged behind cities such as Chicago and D.C. in releasing ZIP code-level vaccination data, which would allow researchers and journalists to see precisely which neighborhoods are getting more shots. And NYC ZIP codes are precise—I’m literally moving two blocks, but my ZIP code is changing.
Reminder @NYCMayor still has not released vaccination rate at ZIP code level, keeping New Yorkers in the dark. NYC once again lags behind major cities in publishing public health data. https://t.co/m93m4d8JbU
(P.S. Ann will be speaking at the third workshop in the Diving into COVID-19 data series, on March 3, about her work at THE CITY!)
The Biden administration will soon start sending doses directly to Community Vaccination Centers, sites operated in partnership with existing community health clinics in an attempt to capitalize on existing connections that these clinics have in their neighborhoods. In order to judge the success of these clinics, we need data about their communities. Local data, demographic data, occupation data… the more complete picture that we can get, the better.
With more local data, we can do more stories like these:
Following the end of the federal public health emergency in May, the CDC has lost its authority to collect vaccination data from all state and local health agencies that keep immunization records. As a result, the CDC is no longer providing comprehensive vaccination numbers on its COVID-19 dashboards. But we still have some information about this year’s vaccination campaign, thanks to continued CDC efforts as well as reporting by other health agencies and research organizations.
This week, the FDA authorized Novavax’s updated COVID-19 vaccine. Here’s why some people are excited to get Novavax’s vaccine this fall, as opposed to Pfizer’s or Moderna’s.
Two weeks ago, I wrote that only 19 states were reporting vaccinations by race and/or ethnicity. This demographic information is key to evaluating the vaccine rollout: both government officials and watchdogs should be able to see how well this process is serving vulnerable populations. Without good data, we can’t see the true picture—making it harder to advocate for a more equitable system.
Demographic vaccine data has improved since then, but not by much. The federal government is still not reporting these data on a national level. 23 states are reporting some form of vaccinations by race and ethnicity—but the data are difficult to standardize, as every state is reporting slightly different demographic categories. Several states are reporting in percentages, rather than whole numbers, which makes the data less precise.
And a lack of federal standards for these data means it’s easy for states to change things up: Indiana, which started reporting vaccinations by race/ethnicity early in January, is now only reporting vaccinations by age and gender. New York City also reported demographic data for vaccinations in December, then removed the figures after disparities were revealed, according to Gothamist. (NYC’s demographic data are back, as of this morning, but they still show white residents getting vaccinated at disproportionately high rates compared to the city’s population.)
Meanwhile, the data we have so far continue to show significant disparities. In 23 states with available data, white Americans are being vaccinated at higher rates than Black Americans, a recent analysis by Kaiser Health News’ Hannah Recht and Lauren Weber found. This analysis followed a similar study that I cited two weeks ago—Recht and Weber write that “disparities haven’t significantly changed” with two more weeks and several more states reporting.
In all but six of the states Recht and Weber analysed, white residents had been vaccinated at double (or more) the rate of Black residents. In Pennsylvania, this rate rises to 4.2 times. Indiana reported white residents vaccinated at 2.6 times the rate of Black residents—before the state took these data off its dashboard. Polling from the Kaiser Family Foundation continues to show that Black Americans are more hesitant; 42% of those surveyed said they want to “wait and see” how the vaccines are working for others before getting a shot.
This vaccination news builds on the continued, deep strain that COVID-19 has placed on Black communities. Alice Goldfarb provided an update this week in an analysis post for the COVID Tracking Project. While the piece maps out disparities in COVID-19 cases for Black, Hispanic or Latino, and Indigenous populations in every state, Goldfarb also provides a stark comparison for the toll this pandemic has taken:
More Black Americans have died of COVID-19 since the pandemic began than there are names on the Vietnam Memorial. More Black or Latinx people have died than the number of people commemorated on the AIDS Memorial Quilt.
The urgency of fixing our vaccine system is clear. And politicians are starting to take note: Massachusetts Representative Ayanna Pressley and Senators Elizabeth Warren and Edward Markey called for better demographic data in a letter to the Department of Health and Human Services this week. They urged the department to better work with states, local public health departments, and labs to collect more data and publish it publicly.
In a statement to the Associated Press, Pressley says:
That which gets measured gets done, and the first step towards ensuring we are able to effectively address these disparities and direct lifesaving resources to our hardest-hit communities is for our government to collect and publish anonymized demographic data, including race and ethnicity, of vaccine recipients.
White Massachusetts residents are getting vaccinated at 1.4 times the rate of Black residents, according to KHN.
Dr. Marcella Nunez-Smith, the chair of Biden’s new COVID-19 equity task force, similarly discussed the need for better data and equitable vaccination at briefings this week. She mentioned leveraging existing data sources, removing barriers to vaccination in underserved communities, sharing ideas between states, and generally making vaccines more accessible, along with a vaccine communications campaign. But she didn’t go into many specifics.
The federal government may be able to make vaccine distribution more equitable, if it can provide the funding that state and local public health departments—along with health clinics, community centers, churches, and so many other possible vaccine providers—need right now. But one thing it can do is require race and ethnicity data, and make it standardized. We need that, like, a month ago.
More vaccination data updates
There were a couple of great features this week on problems with America’s vaccine data system(s), as well as updates to major sources. Here are the highlights:
STAT’s Nicholas St. Fleur wrote about the struggle to find a vaccine appointment, highlighting a viral Twitter thread from intensive care physician Dr. Arghavan Salles. Convoluted online systems are simply not working for seniors and many other vulnerable populations.
In another STAT piece, Mario Aguilar described vaccination data challenges in Utah as a microcosm of similar issues across the country. Even within this single state, he writes, some counties with robust IT already in place were able to adapt their tech for COVID-19 vaccination, while in others, exhausted healthcare workers must enter every data point by hand.
KHN’s Rachana Pradhan and Fred Schulte describe how a lack of standards for race and ethnicity data collection have led some states to leave this field optional, while others aren’t tracking it at all. Similar problems persist for occupation data, which should be crucial when we’re supposedly prioritizing essential workers for earlier vaccination!
Cat Ferguson at MIT Technology Review gives the full picture of Vaccine Administration Management System, or VAMS, a brand-new vaccine data system that the CDC commissioned for COVID-19 vaccination—and that is completely failing to do its job. Most states in the country have chosen not to use this free system, as it is difficult to use, arbitrarily cancels appointments, and confuses patients.
A team from POLITICO laid out Biden’s journey to locate 20 million vaccine doses. The White House briefings were “short on details,” these authors claim, because behind the scenes, the Biden team was still struggling to get their hands on basic information that should’ve been communicated during the transition. Once doses are delivered to states, the state public health systems are fully responsible for tracking these doses until they are officially recorded as “administered”; this makes it difficult for the federal government to track the overall vaccine rollout.
KFF has a new dashboard for its COVID-19 Vaccine Monitor, which is tracking public opinions of and responses to vaccines. The organization is also running a dashboard of state COVID-19 vaccine priorities, which makes it easy to compare strategies across states.
Vaccine Finder, a tool developed at Boston Children’s Hospital which makes it easy for Americans to find vaccine providers in their communities, is partnering with Google Maps to “bring wider awareness and access to COVID-19 vaccines,” according to John Brownstein, Chief Innovation Officer at the hospital.
Following the end of the federal public health emergency in May, the CDC has lost its authority to collect vaccination data from all state and local health agencies that keep immunization records. As a result, the CDC is no longer providing comprehensive vaccination numbers on its COVID-19 dashboards. But we still have some information about this year’s vaccination campaign, thanks to continued CDC efforts as well as reporting by other health agencies and research organizations.
This week, the FDA authorized Novavax’s updated COVID-19 vaccine. Here’s why some people are excited to get Novavax’s vaccine this fall, as opposed to Pfizer’s or Moderna’s.