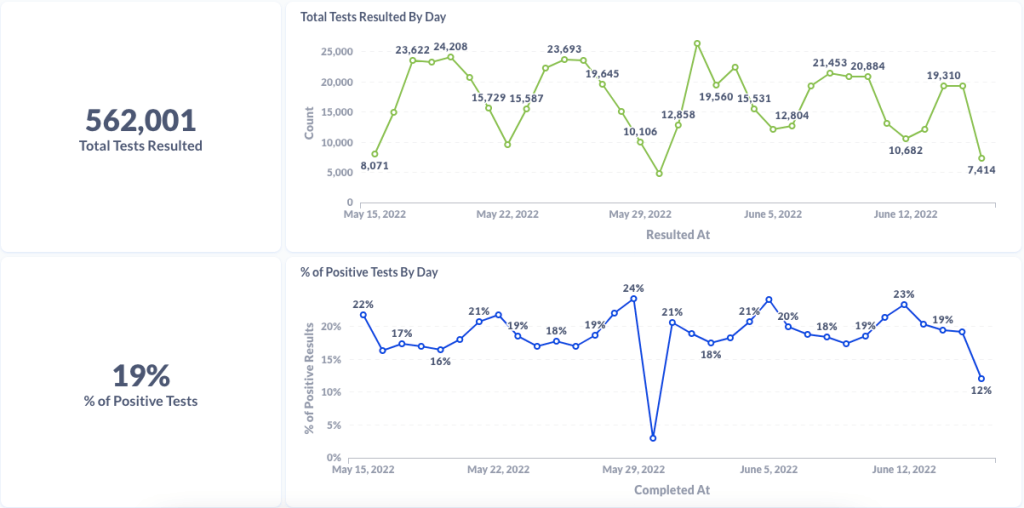
Chart from Curative showing test numbers and test positivity from their sitesChart from Curative showing testing data for Alexandria, Virginia (a current hotspot)Chart from Curative showing testing data for Houston, Texas (another current hotspot)
Curative provides testing trends and commentary to reporters: Last week, I talked to Isaac Turner, chief technology officer at Curative, a COVID-19 testing company with more than 15,000 locations across the country. Curative staff keep a close eye on trends in test positivity and cycle threshold values (a measure of how infectious someone with COVID-19 may be), and share this information with health agencies. While the company doesn’t have a public dashboard, they’re eager to share data with reporters on request and discuss testing trends. For example, Turner told me that in recent weeks, there has been “almost no surge in testing” even though COVID-19 cases have clearly risen across the country. To reach out, you can contact PIO Alana at alana.prisco@ketchum.com.
Walgreens COVID-19 testing dashboard: Another source for testing trends, as government sources become less reliable, is the Walgreens dashboard—incorporating data from COVID-19 PCR testing at more than 5,000 Walgreens locations across the country. In partnership with Aegis Services, many of these test samples are sequenced or identified as specific variants via S-gene target failure. The Walgreens dashboard has a shorter lag time than the CDC’s variant prevalence estimates, so it may be a useful way to see trends in advance.
Kids under 5 can finally get vaccinated: As of yesterday, the CDC has formally recommended versions of both Pfizer’s and Moderna’s COVID-19 vaccines for children under age 5 after they received emergency use authorization from the FDA. This youngest age group can finally get vaccinated! I usually like to watch the FDA advisory committee meetings where new vaccines are discussed, but didn’t have the bandwidth to watch or report on the meetings this week; if you’d like to read up on them, I recommend the Your Local Epidemiologist and STAT News recaps.
Estimating lives saved by universal healthcare: A major new paper this week, by researchers at the Yale School of Public Health, estimates that if the U.S. had a single-payer universal healthcare system, the country may have saved 212,000 lives during the first year of the pandemic. They arrived at this estimate by analyzing data on Americans who lost their health insurance in 2020 or were already uninsured, combined with the impact of being uninsured on COVID-19 mortality. A universal healthcare system would have also saved over $100 billion in healthcare costs in 2020, the researchers found. Read more at Scientific American.
Long COVID may be less likely after an Omicron case: Another new study that caught my attention this week: researchers at King’s College London used the U.K.’s excellent statistics on Long COVID prevalence to compare the risks of long-term symptoms after a Delta infection to the risks after an Omicron infection. They found that the risk of Long COVID after an Omicron infection was about half the risk after a Delta infection, which is potentially pretty good news! Still, it’s still concerning that so many people are at risk for Long COVID after an Omicron infection considering the high case numbers driven by this variant, some outside researchers told NPR.
CDC study on COVID-19 risk for people with disabilities: And one more notable study: CDC researchers examined COVID-19 hospitalization rates among Medicare beneficiaries, comparing those who were on this healthcare plan due to disability to those on the plan due to age. They found that disability beneficiaries had 50% higher hospitalization rates, with the risk for hospitalization increasing with age in both groups. Also: Native American Medicare beneficiaries had the highest hospitalization rate of any racial or ethnic group.
CDC investigating deaths from Long COVID: Researchers at the CDC’s National Center for Health Statistics are currently working to investigate potential deaths from Long COVID, according to a report from POLITICO. The researchers are reviewing death certificates from 2020 and 2021, looking for causes of death that may indicate a patient died from Long COVID symptoms rather than during the acute stage of the disease. There’s currently no death code associated with Long COVID and diagnoses can be highly variable, so the work is preliminary, but I’m really looking forward to seeing their results.
CDC reports on ventilation improvements in schools: And one notable CDC study that was published this week: researchers at the agency from COVID-19, occupational health, and other teams analyzed what K-12 public schools are doing to improve their ventilation. The report is based on a survey of 420 public schools in all 50 states and D.C., with results weighted to best represent all schools across the country. While a majority of schools have taken some measures to inspect their HVAC systems or increase ventilation by opening windows, holding activities outside, etc., only 39% of schools surveyed had actually replaced or upgraded their HVAC systems. A lot more work is needed in this area.
Results from the COVID-19 U.S. State Policy database: The Boston University team behind the COVID-19 U.S. State Policy database has published a paper in BMC Public Health sharing major findings from their work. The database (which I’ve shared in the CDD before) documents what states have done to curb COVID-19 spread and address economic hardship during the pandemic, as well as how states report COVID-19 data. In their new paper, the BU team explains how this database may be used to analyze the impacts of these policy measures on public health.
Promising news about Moderna’s bivalent vaccine: Moderna, like other vaccine companies, has been working on versions of its COVID-19 vaccine that can protect better against new variants like Omicron. This week, the company announced results (in a press release, as usual) from a trial of a bivalent vaccine, which includes both genetic elements of the original SARS-CoV-2 virus and of Omicron. The bivalent vaccine works much better than Moderna’s original vaccine at protecting against Omicron infection, Moderna said; still, scientists are skeptical about how the vaccine may fare against newer subvariants (BA.2.12.1, BA.4, BA.5).
Call center and survey from FYLPRO: A reader who works at the Filipino Young Leaders Program (FYLPRO) requested that I share two resources from their organization. First, the program has set up a call center aimed at helping vulnerable community members with their COVID-19 questions. The call center is available on weekdays from 9 A.M. to 5 P.M. Pacific time in both English and Tagalog; while it’s geared towards the Filipino community, anyone can call in. And second, FYLPRO has launched a nationwide survey to study vaccine attitudes among Filipinos; learn more about it here.
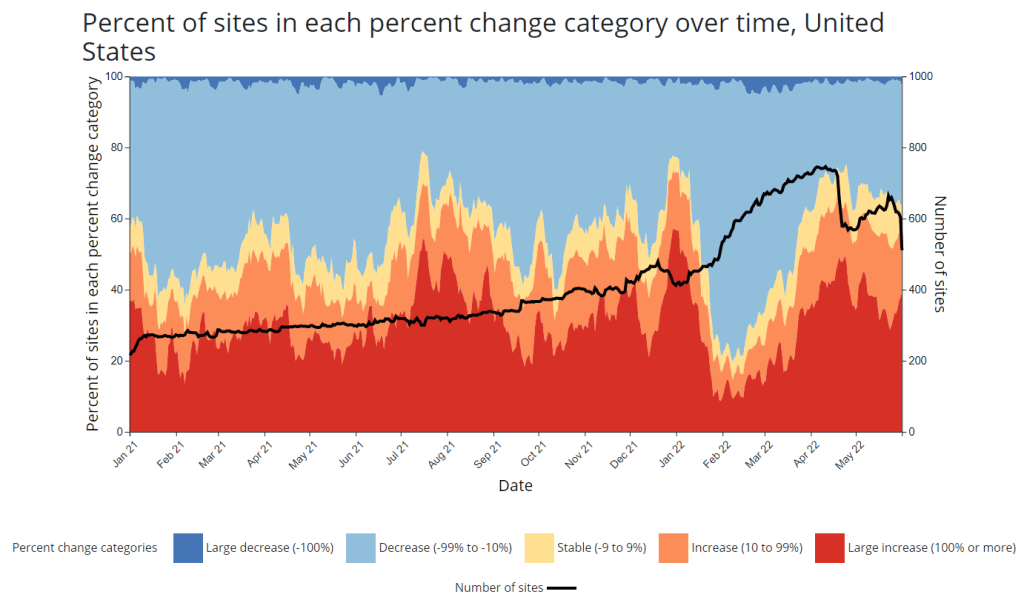
CDC adds new chart to wastewater dashboard: This week, the CDC updated its National Wastewater Surveillance System (NWSS) dashboard with a new chart that aims to summarize the overall picture of coronavirus trends in the country’s sewers. The chart shows the percentage of NWSS sites that have reported their coronavirus concentrations decreasing, staying stable, and increasing over two-week periods; it also shows the overall number of sites with recent data. (This number dropped when NWSS switched contractors, though it has ticked back up in recent weeks as Biobot onboards sites.) Of course, the sites included in NWSS represent a small fraction of the U.S. population, and different locations are using different analysis methods which may be difficult to summarize. But the new chart is still a helpful way to see national trends from the surveillance network.
Preprint suggests 30x scale of case underreporting: Last week, researchers from the City University of New York (CUNY) shared striking results from a study in which they’d surveyed about 1,000 New York City residents about their COVID-19 status during two weeks of the BA.2/BA.2.12.1 surge. The sample was designed to represent the broader city population, and residents could self-report positive test results on both PCR and at-home rapid tests as well as possible symptoms and contact with infected people. About 22% of the survey respondents had a coronavirus infection during the study period (April 23 to May 8), the researchers found. The study hasn’t been peer-reviewed and should be interpreted with caution, but still: it could indicate that one in five New Yorkers got COVID-19 within two weeks. Official case counts were 30 times lower, the researchers found, reflecting massive underreporting; and NYC has more access to PCR testing than many other places.
1. In our new (not yet peer reviewed) pre-print on NYC's BA.2/BA.2.12.1 surge, in a population-representative sample, we estimated SARS-CoV-2 prevalence to be 22.1% during April 23-May 8 (about 1.8M adults). About 31 times the official case count. https://t.co/Vr7PUWsWd7
CDC study demonstrates disproportionate COVID-19 impact on Native Americans: One study from the CDC’s Morbidity and Mortality Weekly Report (MMWR) that caught my attention this week: researchers in Alaska (at the state’s health agency and tribal health institutions) examined COVID-19 rates for the state’s indigenous population. They found that the age-adjusted COVID-19 case rate among Native Americans/Alaska Natives was about twice as high as the rate among white people living in Alaska, and the death rate was about three times higher. Many indigenous people in Alaska live in rural, remote areas, some inaccessible by car, which heightens the challenges of accessing healthcare.
Native American life expectancy fell during the pandemic: Another related preprint: researchers at Virginia Commonwealth University, the University of Colorado Boulder, and the Urban Institute have produced multiple studies examining how life expectancy changed during the pandemic. In general, COVID-19 led to massive decreases in life expectancy across the board; but the latest update from this group showed that Native Americans were particularly hard-hit. Native American life expectancy dropped by 4.7 years, compared to a 2.1 drop for the white American population. Steven Woolf, corresponding author, discussed the study in a Q&A with Virginia Commonwealth University. (H/t Andrew Stokes.)
Higher burden of COVID-19 in developing countries: And one more notable new study, published this week in BMJ Global Health: a group of researchers at institutions in the U.S., Australia, Brazil, and other countries conducted an in-depth review of global COVID-19 serology data to estimate the disease’s true infection and fatality rates across the world. The researchers found that infection fatality rates (i.e. the share of infected people who die of COVID-19) were much higher in developing/low-income countries than in developed/high-income countries, in some cases up to three times higher. “The results are, in a word, depressing,” lead author Gideon Meyerowitz-Katz wrote in a Twitter thread discussing the study.
New job posting at CDC forecasting center: The CDC’s new Center for Forecasting and Outbreak Analytics, formally launched in April, has posted a job opening for (at least one?) data scientist. Considering that the center plans to hire 100 scientists and science communicators, this singular posting is likely just one of many more opportunities to come.
New Surgeon General advisory on health worker burnout: This week, U.S. Surgeon General Dr. Vivek Murthy released a new advisory on COVID-19 burnout among health workers, summarizing research on the issue and highlighting it as a public health priority. The advisory discusses a variety of societal, cultural, structural, and organizational factors contributing to health worker burnout, while tying this burnout to growing shortages of doctors and other health professionals. From the one-page summary of the advisory: “If not addressed, the health worker burnout crisis will make it harder for patients to get care when they need it, cause health costs to rise, hinder our ability to prepare for the next public health emergency, and worsen health disparities.”
CDC may change COVID-19 reporting for hospitals: The CDC is planning a few changes to its reporting requirements for hospitals in order to simplify the reporting process and cut down on redundant information, according to a draft plan shared with Bloomberg. Among the changes: hospitals may no longer be required to report suspected COVID-19 cases (i.e. those cases not yet confirmed with a PCR test); with most hospitals testing all patients when they’re admitted, suspected cases are less common and the data are less useful than they had been at earlier points in the pandemic. The CDC may also stop requiring COVID-19 reporting from some types of facilities, such as mental health centers, and may change the frequency of required reporting.
New preprint about Omicron BA.4 and BA.5: While the U.S. mostly worries about BA.2.12.1, additional Omicron subvariants BA.4 and BA.5 have been spreading in South Africa and other countries. A new study from a highly-regarded consortium of Japanese researchers suggests that BA.4 and BA.5 are about 20% more transmissible than BA.2 (similarly to BA.2.12.1). Also, even more concerning: the researchers found that BA.4 and BA.5 are more capable of resisting protection from a prior Omicron infection than BA.1. While the study has not yet been peer-reviewed, it garnered a lot of attention on Twitter this week from scientists warning that we need to watch out for these subvariants.
U.S. gets closer to a vaccine for kids under five: The FDA has set new dates for its vaccine advisory committee to review data on COVID-19 vaccines for children under age five: the committee will discuss both Moderna’s and Pfizer’s under-five vaccines on June 15, after discussing Moderna’s vaccine for children ages six to 17 on June 14. This announcement came after Pfizer and BioNTech released new data on their under-five vaccine, saying that a series of three doses provided strong protection against severe disease. There are some caveats for the data (which were shared via press release), but this is great news for children under age five and their families.
NIH sharing some COVID-19 technology (but not patents): I missed this news from earlier in May: the National Institutes of Health has made a deal with the World Health Organization’s COVID-19 Technology Access Pool and the Medicines Patent Pool to lisense 11 technologies used in COVID-19 vaccines and therapeutics. This lisense will allow pharmaceutical manufacturers around the world to make the coronavirus spike protein, RNA virus tests, and other COVID-19 components, increasing access to these technologies in low- and middle-income countries. Of course, it would be better for these countries if the NIH had shared full vaccine patents, but apparently that’s asking too much.
HHS begins releasing Paxlovid data: This past week, the Department of Health and Human Services (HHS) published data on how many courses of Paxlovid and other major COVID-19 therapeutics have been ordered and administered nationwide. As KHN reporter Hannah Recht pointed out on Twitter: “This is still not the detailed, complete data that county health officials need to do their jobs but it’s a start.” (See Recht’s article on this data gap for more context.)
COVID-19 Local Action Tracker: Since early 2020, the National League of Cities has tracked how cities and other local municipalities have responded to COVID-19. The tracker includes 800 cities and almost 5,000 policies, impacting over 100 million people; it links out to policy documents for each item. (H/t Data Is Plural.)
FEMA funeral assistance: The Federal Emergency Management Agency (FEMA) has distributed over $2 billion in aid for COVID-19 funerals since the beginning of the pandemic, supporting more than 300,000 families, the agency announced in a press release this spring. The press release also includes data providing the number of applicants and total funds awarded in each state.
New Long COVID studies with electronic records: Two recent papers on Long COVID caught my attention this week. First, researchers at data nonprofit FAIR Health analyzed a cohort of 78,000 Long COVID patients using a new diagnostic code for the condition, leading to useful findings about potential demographics and risk factors. Second, researchers at the University of North Carolina, the University of Colorado, and other collaborators used machine learning techniques on health records to identify potential Long COVID patients. Both studies used electronic health records to include wider patient pools than typical U.S. Long COVID research.
Limited immunity after Omicron infection: Another notable paper, published this week in Nature: researchers at Gladstone Institutes, a research organization in San Francisco, examined immunity after Omicron infections by testing out potential immune responses to different variants in mice and analyzing human serological samples. Their results suggest people infected with Omicron after vaccination have more protection against variants other than Omicron compared to unvaccinated people, which may only be protected against future Omicron infections.
FDA authorizes combined at-home test for COVID-19, flu, RSV: And a piece of diagnostic news for this week: for the first time, the FDA has provided emergency use authorization to an at-home test that can distinguish between COVID-19, the flu, and RSV. Processing the test does involve mailing results of a nasal swab to the testing company, Labcorp, so it’s not as simple as the at-home COVID-only tests we’ve all grown used to. Still, this authorization is an important step for future testing.
COVID-19 deaths that could’ve been prevented with vaccines: A new analysis from the Brown University School of Public Health suggests that almost 319,000 U.S. COVID-19 deaths could have been avoided if all adults had gotten vaccinated against the disease. This number differs significantly by state; there were 29,000 preventable COVID-19 deaths in Florida, compared to under 300 in Vermont. For more context on the analysis, see this article in NPR.
CDC dashboard in Spanish: The CDC has translated its COVID-19 Data Tracker into Español. At a glance, the Spanish version appears to include all the major aspects of the tracker: cases, deaths, vaccinations, community transmission, variant prevalence, wastewater, etc. Of course, it would have been great if the agency could’ve devoted resources to this translation effort well below spring 2022, when the number of people looking to the agency for COVID-19 guidance is pretty low.
CDC may lose access to COVID-19 data:According to reporting from POLITICO, the CDC and other national health agencies may no longer have the authority to require COVID-19 data reporting from states and individual health institutions if the Biden administration allows the country’s federal pandemic health emergency to end this summer. Such a change in authority could lead to the CDC (and numerous other researchers across the country) losing standardized datasets for COVID-19 hospitalizations, transmission in nursing homes, PCR testing, and other key metrics. Considering that hospitalizations are considered the most reliable metric right now, this could be a major blow.
COVID-19 testing declines globally: Speaking of losing reliable data: this report from the Associated Press caught my eye. The story, by Laura Ungar, explains that the U.S. is not the only country to see a major decrease in reported COVID-19 tests (a.k.a. Lab-based PCR, not at-home rapid tests) in recent months. “Experts say testing has dropped by 70 to 90% worldwide from the first to the second quarter of this year,” Ungar writes, “the opposite of what they say should be happening with new omicron variants on the rise in places such as the United States and South Africa.”
More promising data on Moderna kids’ vaccine: While Pfizer’s vaccine for children under five remains in development, Moderna continues to release data suggesting that this company is further ahead in providing protection for the youngest age group. This week, Moderna announced a half-dose of its vaccine provides a “strong immune response” in children ages six to 11; the announcement was backed up by a scientific study published in the New England Journal of Medicine (so, more rigorous than your typical press release). The FDA is currently evaluating a version of Moderna’s vaccine for children between ages six months and six years.
CDC adds second boosters to its vaccine dashboard: In the latest update to the CDC’s COVID Data Tracker, you can now find a national tally of Americans who have received second booster shots on the “COVID-19 Vaccinations in the United States” page. About 10 million people have received these additional shots as May 6, about one-tenth the number of first booster recipients. The CDC has yet to add state-by-state or demographic data for second boosters.
KFF updates COVID-19 Vaccine Monitor: This week, the Kaiser Family Foundation published the latest update of its Vaccine Monitor, a long-running project tracking Americans’ attitudes towards COVID-19 vaccines and related issues. One notable finding from the April update: just 18% of parents with children under age five are “eager to get their child vaccinated right away,” compared to 27% who say they will “definitely not” get their child vaccinated. This report also includes survey findings on mask-wearing, COVID-19 in the workplace and in schools, and future booster shots.
Biobot on GitHub: I recently learned that Biobot Analytics, the leading COVID-19 wastewater surveillance company, publishes its underlying data on GitHub. This repository includes coronavirus concentrations in wastewater treatment plants monitored by Biobot across the country, along with regional wastewater data, national data, and COVID-19 case numbers for comparison.
TON’s Guide to Tracking Source Diversity: Not directly COVID-related, but a resource that I thought readers may find useful: The Open Notebook (TON) has published a detailed guide for journalists seeking to track the diversity of sources interviewed for their stories. While TON is geared towards science writers, this guide is broadly applicable to any reporter who spends a lot of time seeking out and talking to experts.
Nursing Home Inspect (ProPublica): ProPublica recently published a major investigation into medical exemptions to COVID-19 vaccines among nursing home workers, finding that high numbers of workers are claiming these exemptions even though the actual, medical reasons causing someone to be ineligible for vaccination are fairly limiting. Along with the investigation, the newsroom added staff COVID-19 vaccination data to its Nursing Home Inspect database, which allows users to compare nursing homes based on negative inspection reports and other deficiencies.
Neighborhood Atlas: One source I learned about at the health journalists’ conference this weekend is the Neighborhood Atlas tool from researchers at the University of Wisconsin School of Medicine and Public Health. The atlas maps out metrics that put neighborhoods—i.e. Census block groups, a geographical level much more granular than counties—at a health disadvantage, including income, education, employment, and housing.
Access to hospital services for minority groups: Another source from the AHCJ conference: this February 2022 paper and corresponding dataset, measuring how far different minority communities across the country have to go to access hospital services. Over half of rural Native American communities are more than 30 miles from the closest intensive care unit, said Dr. Mary-Katherine McNatt in a talk introducing this source.
KFF’s State Health Facts: Also at the conference, Juliette Cubanski from the Kaiser Family Foundation (KFF) gave a presentation on the organization’s data tools and resources for journalists, focusing on Medicare data. One broadly useful KFF tool is the State Health Facts dashboard, which enables journalists and researchers to search through over 800 health indicators at the state level. These indicators are frequently updated with the most recent data.
Nursing home staffing reports: COVID-19 revealed how unprepared America’s nursing homes were for a health crisis. In a panel discussing this issue, Richard Mollot from the Long Term Care Community Coalition (a nonprofit that advocates for better long-term care) shared some data from his organization, highlighting drops in staffing during the pandemic that have not yet been recovered.
This weekend, I spoke on a panel at the Association of Health Care Journalists (AHCJ) annual conference, held in person in Austin, Texas. (Yes, the irony of my first air travel post-end of the mask mandate being a trip to a health journalism conference is not lost on me.)
My session focused on COVID-19 data, particularly the data gaps left by the federal government—which, longtime readers know, is a topic I’ve reported on extensively. We provided attendees with a tipsheet, sharing some source suggestions and tips for reporting on this topic.
Derek Kravitz, my editor and project lead of the Documenting COVID-19 project, moderated the session; Nsikan Akman, health and science editor at Gothamist/WNYC, was another panelist. Dr. Katelyn Jetelina, author of the incredible Your Local Epidemiologist newsletter, was scheduled to be a panelist as well, but unfortunately couldn’t make it to the conference last minute. (Her contributions are still reflected in our slides and tipsheet, though.)
During the session, we discussed a range of COVID-19 data topics, including:
The lack of standardization for COVID-19 data collection and reporting in the U.S., exacerbated by our decentralized healthcare and public health systems;
Discrepancies between New York State and New York City data, as an example of this lack of standardization (a specialty for Nsikan);
Challenges around (and some recommendations for) communicating COVID-19 data to audiences;
One of the most challenging aspects of reporting on the pandemic has been accessing reliable, accurate data about COVID-19 and its impact on Americans. The need for trustworthy, real-time data has caused a few journalism and nonprofit groups to create repositories to pull together data from varying sources.
A Thursday session at Health Journalism 2022 in Austin, “The quest for COVID-19 data: Where “official sources” fell short and journalism stepped in,” focused on these efforts and provided journalists with a wealth of resources for up-to-date data related to the pandemic.
Most high-income countries have national health care systems, so data collection and collation is far more straightforward than in the federalized U.S. health care system, where a mix of private and public payers are governed by national and differing state laws. Without a national registry or centralized healthcare system, it’s been harder to track statistics on COVID cases, hospitalizations, deaths, vaccinations, and other relevant numbers.
The tipsheet from this session includes links and blurbs to a few of the panel’s favorite COVID-19 data sources, including:
CDC mortality data, cleaned and sorted by Documenting COVID-19
HHS Community Profile Reports
MCH Strategic Data’s COVID-19 in schools dashboard
COVIDPoops19 dashboard
Historical wastewater data from CDC NWSS
Long COVID Source List
Health Equity Tracker
Open Government Data
And the tipsheet also includes a few tips for communicating COVID-19 data, supplemented with stories that provide useful examples. Here are the tips:
Explain where data come from and how they’re collected – using as little jargon as possible.
Be clear about uncertainties and caveats; what can’t the data tell you?
Share how data points, trends or study results can be translated into actionable information for readers.
Use questions from readers to guide reporting.
Look for differences in how state and municipalities track their COVID-19 data.
Look for ways that data collection methods (or the lack of clear methods) may hide health inequities.
Use visuals/multimedia to communicate the pandemic’s immense tolls.
Provide larger context about the reasons why COVID-19 data in the U.S. are often fractured and difficult to interpret.
Hospitalizations of young children during Omicron: A major study released in the CDC’s Morbidity and Mortality Weekly Report (MMWR) this week describes hospitalization rates among children ages five to 11, focusing on the Omicron wave in December through February. Findings include: about nine in ten of the children hospitalized during this period were unvaccinated, and hospitalization rates were twice in high in unvaccinated children compared to vaccinated children, demonstrating the importance of vaccination in the five to 11 age group.
COVID-19 death rates by race and ethnicity: Another notable study published in MMWR this week: CDC researchers used provisional mortality data (based on death certificates) to study COVID-19 death rates among different racial and ethnic groups, comparing 2020 and 2021. Death rates for Hispanic, Black, and Native Americans were closer to the rates for white Americans in 2021 than they had been in 2020, the report found; this is likely tied to lower vaccination rates and, consequently, higher death rates in conservative and rural areas. For any reporters seeking to investigate these patterns in their regions, the Documenting COVID-19 project’s CDC mortality data repository includes county-level death data from the same source as this MMWR report.
New CMS data on hospital and nursing home ownership: Nursing homes and other long-term care facilities have been under increased scrutiny during the pandemic, as COVID-19 revealed major flaws in facilities’ ability to care for vulnerable seniors, A series of new datasets from the Centers of Medicare & Medicaid Services (CMS) aims to enable more scrutiny: the datasets include changes of ownership for skilled nursing facilitiesand for hospitals. CMS plans to update these datasets on a quarterly basis, according to a press release about the new data.
New funding for patient-led Long COVID research: The Patient-Led Research Collaborative (PLRC), a group of Long COVID patients that have produced leading research on their condition, announced this week that they’ve received $3 million in funding. This funding comes from Balvi, a fund for high-impact COVID-19 projects established by Ethereum co-creator Vitalik Buterin. PLRC announced that $2 million will go to start a pool of Long COVID research grants—to be awarded directly by patients—while the remaining $1 million will fund a series of PLRC-led studies. I look forward to reporting on the results of this research! (Also, related: this week, I updated the source list of Long COVID patients and experts willing to talk to reporters, which I compiled with Fiona Lowenstein.)
FDA authorizes breathalyzer for COVID-19: The latest new COVID-19 test is a breathalyzer: this machine, developed by Texas-based diagnostics company InspectIR, analyzes chemicals in a person’s breath to quickly detect compounds signifying a coronavirus infection. This test can deliver results in just three minutes—even faster than an antigen test—but it needs to be performed in a medical setting; InspectIR is working on a version that could be hand-held, like breathalyzers for alcohol. Impressive as the technology is, this data reporter is asking: how will those test results get reported to public health agencies?