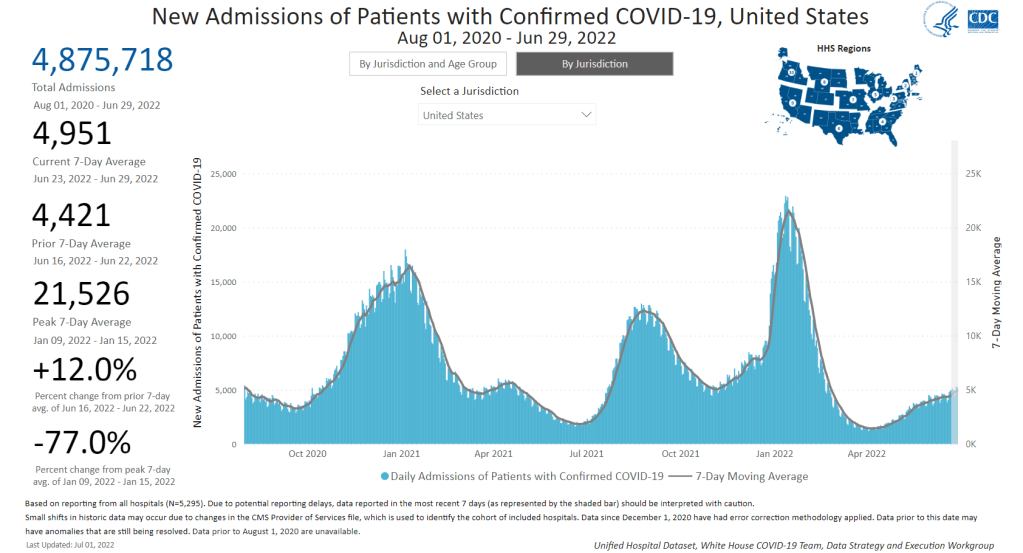
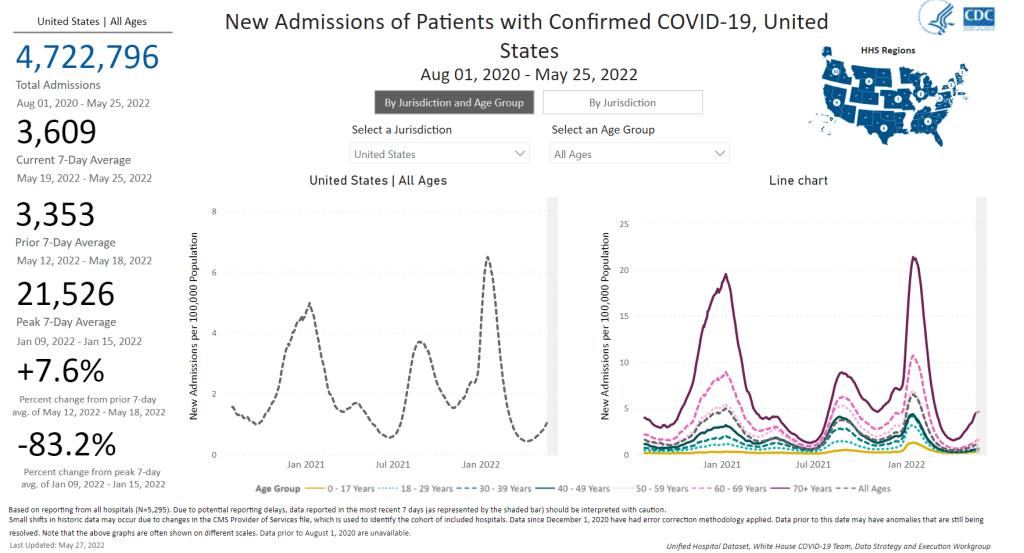
New hospital admissions for COVID-19 increased 12% last week over the week prior, a signal of the continued surge. Chart via the CDC.
In the past week (June 25 through July 1), the U.S. reported about 800,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 110,000 new cases each day
234 total new cases for every 100,000 Americans
11% more new cases than last week (June 18-24)
In the past week, the U.S. also reported about 35,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 5,000 new admissions each day
10.6 total admissions for every 100,000 Americans
12% more new admissions than last week
Additionally, the U.S. reported:
2,200 new COVID-19 deaths (0.7 for every 100,000 people)
48% of new cases are Omicron BA.2.12.1-caused; 52% BA.4/BA.5-caused (as of June 25)
An average of 150,000 vaccinations per day (per Bloomberg)
BA.4 and BA.5 are now the dominant coronavirus lineages in the U.S., and they’re reviving our recent surge: from the plateau of recent weeks, national COVID-19 cases are clearly going up again. Reported cases rose 11% last week from the week prior. And, as always, this number is a significant undercount of true infections.
New hospital admissions also went up last week: about 5,000 Americans were admitted to hospitals with COVID-19 each day, up 12% from the week prior. While the vast majority of COVID-19 cases may now be mild—thanks to vaccinations, prior infections, and treatments—this is a reminder that severe symptoms are still very possible.
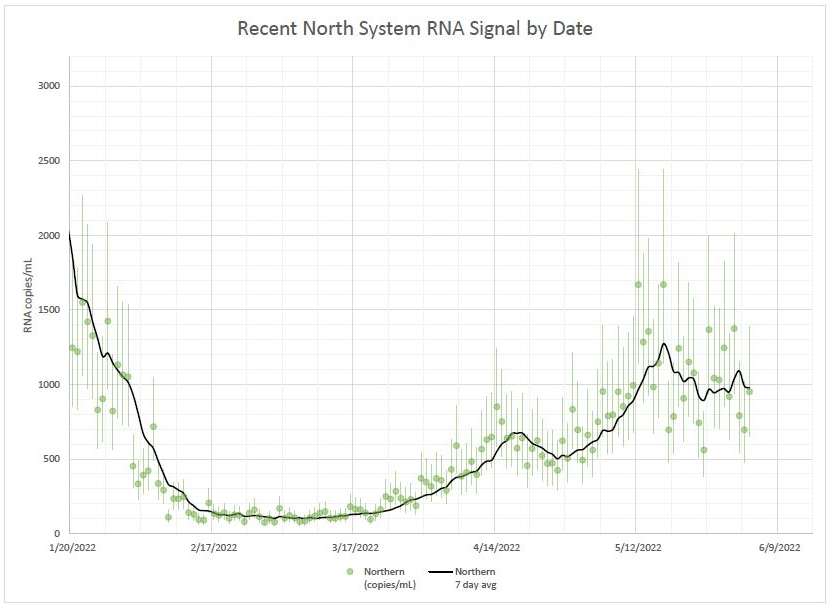
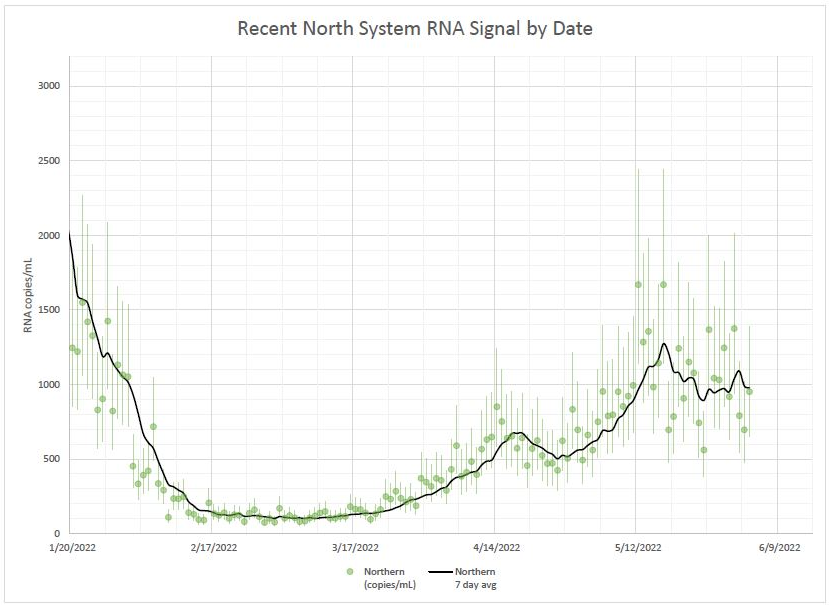
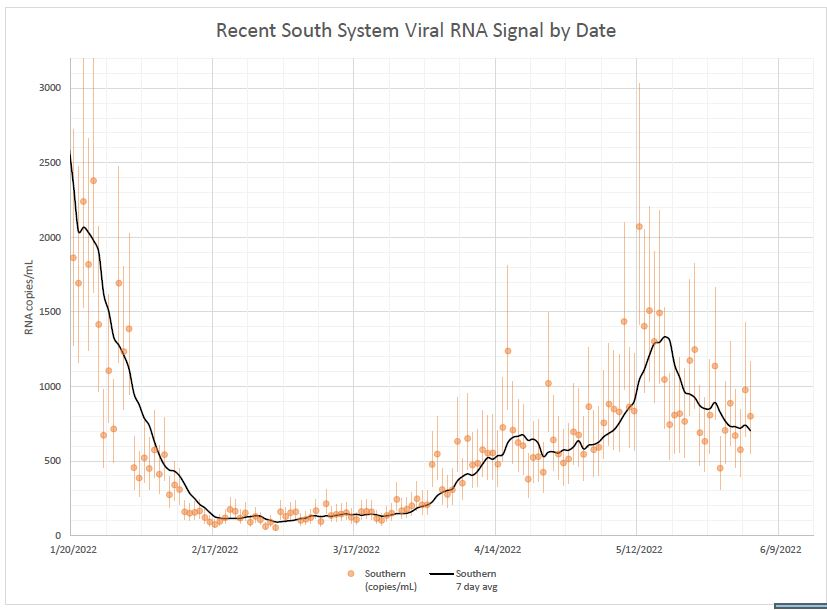
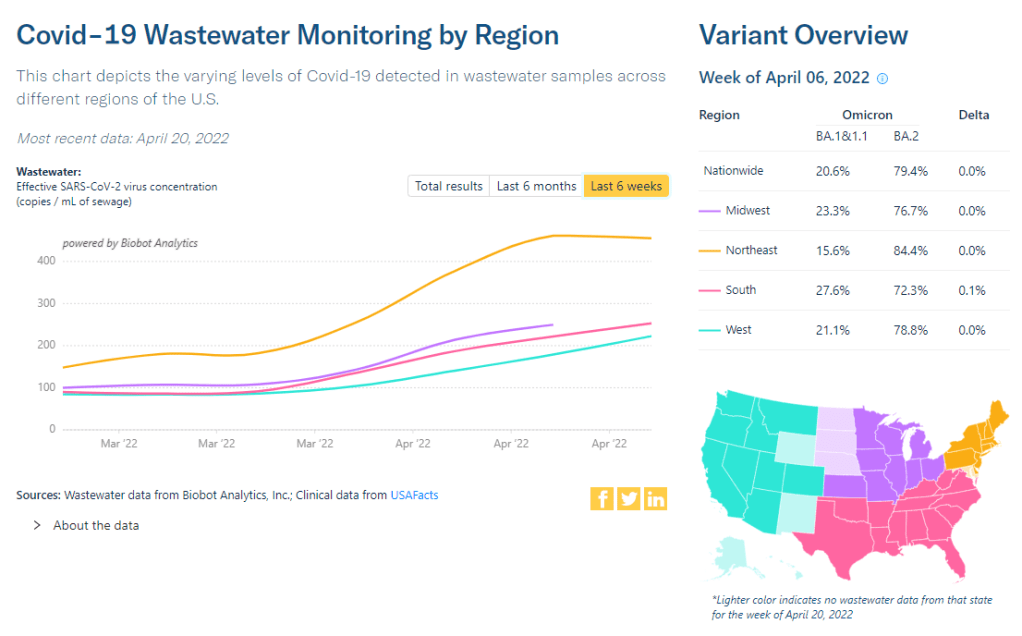
Wastewater data from Biobot indicate a continued plateau in transmission at the national level. At the regional level, COVID-19 levels are trending down in the West and South, but ticking up again in the Northeast, likely as BA.4 and BA.5 take over from BA.2.12.1 in these areas.
In my FAQ post last month ago, I wrote that scientists weren’t yet sure whether BA.4 and BA.5 would be able to outcompete BA.2.12.1, the offshoot of BA.2 first identified in New York. Now, it seems clear that BA.4 and BA.5 are capable of dominating: these two subvariants caused over half of new cases nationwide in the week ending June 25, as well as in most regions.
Missouri wastewater update. Numbers up again slightly from last week. BA.4/5 has overtaken BA.2.12.1 by a nose. The other Omicron sub-variants are holding steady. Still no sign of BA.2.75. This is the cumulative data from 61 sewersheds. pic.twitter.com/z9MUYkRylC
Even places like New York City, which saw a major BA.2/BA.2.12.1 wave, is now reporting another uptick in cases, according to data from the local health department. The city’s test positivity rate went over 10% on Thursday for the first time since January, a signal of the underreporting in recent weeks as PCR testing becomes less popular. And yet, city leadership is not interested in implementing any new safety precautions.
Remember, the problem with these subvariants is that they’re built for reinfection. Even if you had Omicron BA.1 in the winter, or even had BA.2 this spring, you could easily get BA.4 or BA.5. These infections are, at best, a week-long inconvenience, and at worst, could turn into Long COVID.
The holiday tomorrow will interrupt COVID-19 reporting, as holidays always do. Stay safe this weekend, and don’t be fooled if you see a brief downturn in case numbers.
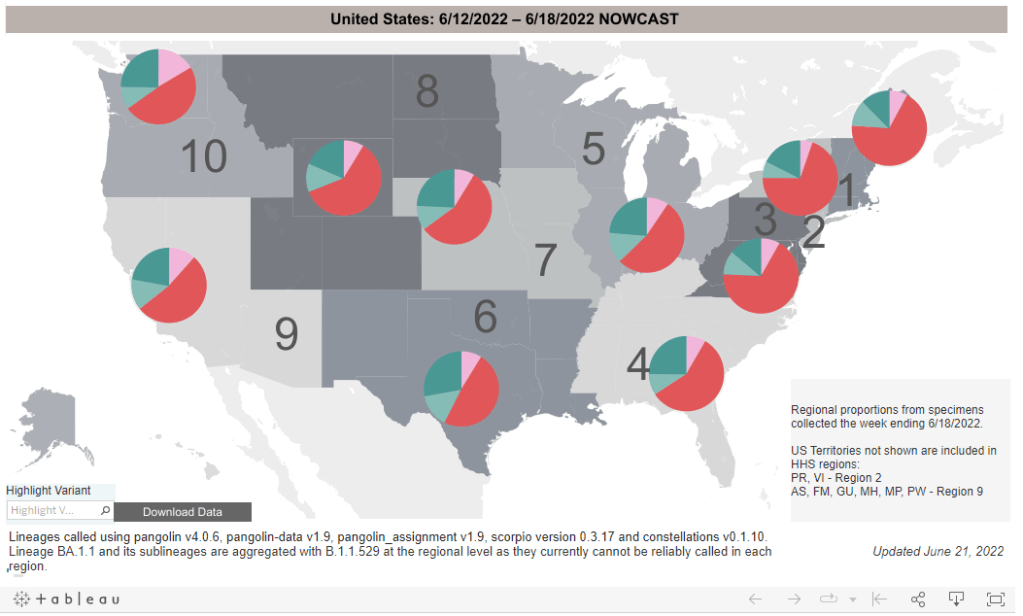
BA.4 and BA.5 (teal) are competing with BA.2.12.1 (red), with different lineages dominating in different parts of the country. CDC estimates reflect the week from June 12 to June 18.
In the past week (June 18 through 24), the U.S. reported about 680,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 100,000 new cases each day
208 total new cases for every 100,000 Americans
6% fewer new cases than last week (June 11-17)
In the past week, the U.S. also reported about 31,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 4,400 new admissions each day
9.3 total admissions for every 100,000 Americans
1% more new admissions than last week
Additionally, the U.S. reported:
1,800 new COVID-19 deaths (0.5 for every 100,000 people)
56% of new cases are Omicron BA.2.12.1-caused; 35% BA.4/BA.5-caused (as of June 18)
An average of 50,000 vaccinations per day (per Bloomberg)
America’s Omicron subvariant surge continues to be in a plateau this week, with national COVID-19 case rates, hospitalization rates, and wastewater trends remaining fairly level or showing slight declines.
The U.S. has reported a weekly average between 100,000 and 110,000 new cases a day since mid-May, according to the CDC. These numbers are massive undercounts, as about five times more rapid antigen tests are being conducted in the U.S. than PCR tests, so the true trend is difficult to discern—but we can safely say that there is a lot of coronavirus circulating throughout the country.
New hospital admissions, the number of COVID-19 patients who sought treatment, rose slightly in the last week: about 4,400 patients were admitted each day nationwide, compared to 4,300 last week. Wastewater data from Biobot shows a national plateau, as coronavirus levels drop in the Northeast and West while rising in the South and remaining stagnant in the Midwest.
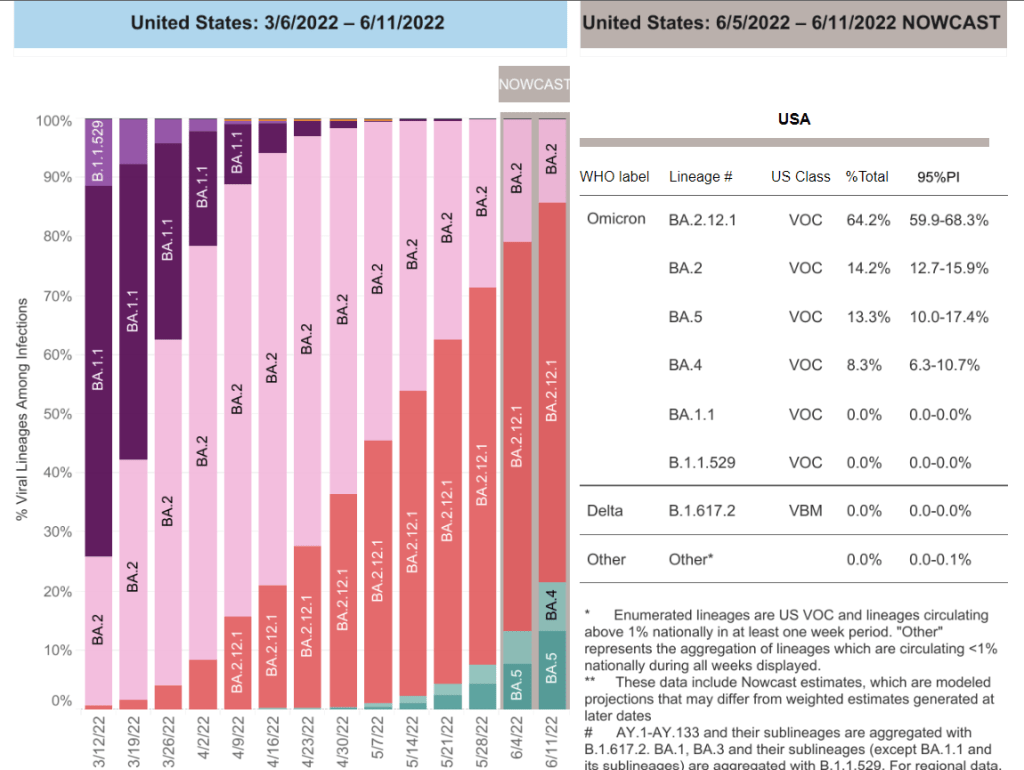
Why this prolonged plateau? Most likely, the rise of immune-evading Omicron subvariants BA.4 and BA.5 is preventing a BA.2-initiated wave from truly dipping back down. Estimates from the CDC suggest that BA.4 and BA.5 may even be outcompeting BA.2.12.1: the share of U.S. cases caused by BA.2.12.1 dropped for the first time in the CDC’s latest variant prevalence update, from 63% in the week ending June 11 to 56% in the week ending June 18.
Regions with a higher share of BA.4 and BA.5—namely, Gulf Coast states, the Midwest, and the West Coast—are also reporting case increases. A few state hotspots that stick out in the (admittedly, poor) official case counts: Hawaii, Florida, New Mexico, Alaska, and California all reported more than 250 new cases per 100,000 people in the week ending June 22.
In the Northeast, BA.2.12.1 is still causing a majority of cases, but BA.4 and BA.5 are gaining some ground. This may explain why places like New York City are seeing case trends that simply refuse to go down as quickly as we’ve observed in past waves, though a lack of new safety measures is likely also playing a role.
NYC this plateau is stressing me out*
*the usual caveats about underreporting, antigen tests not included, etc apply pic.twitter.com/6wKgebObOn
Meanwhile, vaccination rates remain the lowest they’ve been since late 2020. Fewer than 25,000 people received a first vaccine dose in the week ending June 21, according to the CDC. I was expecting to see a bump from children under five finally becoming eligible for vaccination, but it has not shown up in the data yet—likely another signal of current apathy towards COVID-19 safety.
BA.4 and BA.5 caused more than 20% of new COVID-19 cases nationwide in the week ending June 11, according to CDC estimates.
This week, I had a new story published at TIME’s online news site, explaining what Omicron BA.4 and BA.5 could mean for COVID-19 trends in the U.S.
The story makes similar points to my FAQ post on these subvariants from earlier in June: basically, BA.4 and BA.5 have evolved to get around antibodies from a prior coronavirus infection or vaccination, and the U.S. is likely to see a lot of reinfections from these subvariants—even among people who already had BA.1 or BA.2 earlier this year. BA.2.12.1 has mutated in a similar way, leading experts to suspect that one of these subvariants (or all three) will dominate the next phase of the pandemic.
When I talked to variant experts for my TIME story, I asked them for their thoughts on surveillance. “Is it getting harder to identify and track new linages like BA.4 and BA.5 as fewer people use PCR tests and more use at-home tests?” I asked. “What improvements or shifts would you like to see in surveillance?”
All three experts I spoke to had different perspectives, which I found interesting—and worth sharing in the COVID-19 Data Dispatch, since I wasn’t able to include this (somewhat wonkier) information in my TIME story.
Here’s what they said:
Marc Johnson, a microbiology and immunology professor at the University of Missouri who leads the state’s wastewater surveillance program, thinks that expanding wastewater monitoring is the way to go (though he admitted his bias, as someone who works in this area). “Sewershed monitoring is a really good way to track variants going forward,” he said. “It gives you a comprehensive view without costing you hundreds of thousands of dollars… or without having to sequence a thousand people.”
Shishi Luo, associate director of bioinformatics and infectious diseases at Helix (a genomics and viral surveillance company), is thinking about how to ensure her company consistently receives enough PCR test samples to get useful data from sequencing. At the moment, pharmacies and community testing sites are still providing enough samples that Helix has sufficient information to track variants, she said. But, anticipating that those numbers may dwindle, Helix is connecting with urgent care clinics and hospitals that do diagnostic testing. “I think those places will continue to collect samples and perform qPCR tests,” she said.
Paul Bieniasz, a professor at Rockefeller University who studies viral evolution, thinks that the current levels of surveillance are sufficient—at least, when it comes to policymaking and updating vaccines. “I would like to keep surveillance at a level such that such that we can have a pretty accurate picture about what’s going on,” he said. But he wants to prioritize “the really important things”: namely, understanding changes to vaccine effectiveness, which treatments to use, and identifying a new “major antigenic shift” like the one that produced Omicron as soon as it occurs.
“But it can always be better,” he said. “The more intense the surveillance, the more sensitive it is, and the earlier you detect things that might be of concern in the future.”
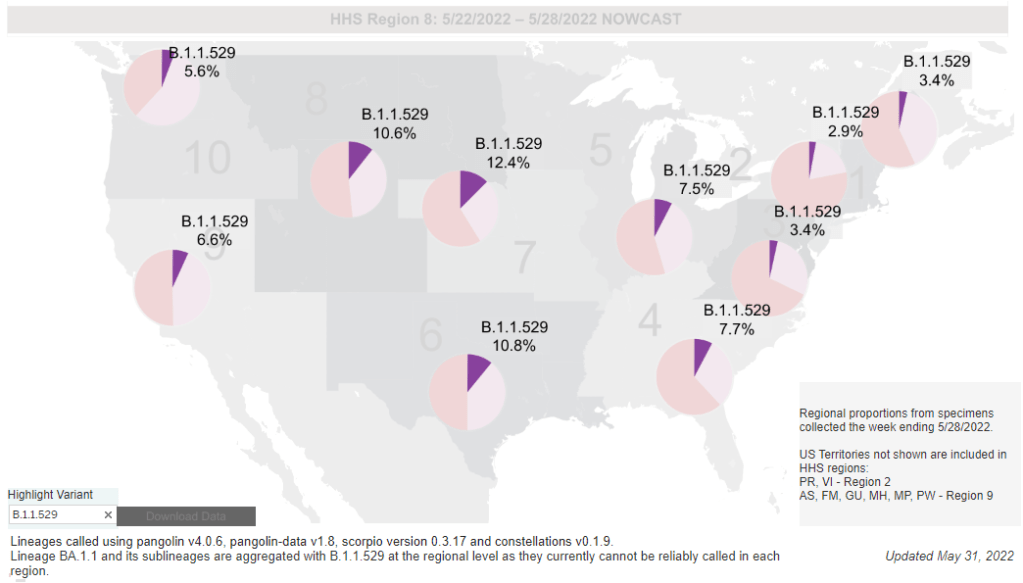
While the CDC is not yet reporting BA.4 and BA.5 separately, the subvariants are included in B.1.1.529; this grouping is driving increased transmission in some Midwestern and Southern states. Chart via the CDC variant dashboard.
America’s current COVID-19 surge is being driven by BA.2 and its sublineage BA.2.12.1. But there are other versions of Omicron out there to which we need to pay attention—namely, BA.4 and BA.5. Here’s a brief FAQ on these two subvariants, including why scientists are concerned about them and where they’re spreading in the U.S.
What are BA.4 and BA.5?
Remember how, when South African scientists first sounded the alarm about Omicron in November, they identified three subvariants—BA.1, BA.2, and BA.3? BA.1 first spread rapidly around the world, followed by BA.2.
Then, in the winter, South African scientists again identified new Omicron subvariants, called BA.4 and BA.5. These two variations split from the original Omicron lineage, and tend to be discussed together because they have similar mutations. (Specifically, they have identical spike protein mutations; this article discusses the mutations in more detail).
It’s important to note that, while South African scientists characterized these subvariants, they likely didn’t originate in the country. South Africa has a better variant surveillance system than many other countries, particularly compared to its neighbors, allowing the country’s scientists to quickly identify variants of concern. BA.4 and BA.5 also caused a new surge in South Africa, allowing for study of the subvariants’ performance.
Why are scientists concerned about these subvariants?
Early studies of BA.4 and BA.5 indicate that not only are these subvariants more transmissible than other forms of Omicron, they’re also more capable of bypassing immunity from prior infection or vaccination.
While the differences between BA.4/BA.5 and BA.1/BA.2 are less dramatic than the differences between the Omicron family and Delta, scientists hypothesize that there is still enough distinction between these two Omicron sub-groups that people who already had Omicron BA.1 or BA.2/BA.2.12.1 could potentially get reinfected by BA.4 or BA.5.
My guess based on this: BA.4/BA.5 escape, while not as dramatic as Omicron escape from vaccine or Delta immunity, is enough to cause trouble and lead to an infection wave. But not likely to cause much more severe disease than the previous wave, especially in vaccinated.
What are BA.4 and BA.5 doing in South Africa and other countries?
BA.4 and BA.5 have been detected in over 30 countries, according to CNN. But scientists have again focused on South Africa, as this country has better surveillance than many others—particularly as PCR testing declines around the world.
In South Africa, the BA.4/BA.5 wave that started in April has peaked and is now on the decline. Hospital admissions and deaths were lower in this recent wave than in the Omicron BA.1 wave in November and Decenter, largely thanks to high levels of immunity in the country. Still, the continued Omicron infections suggest that reinfection is a real concern for these subvariants.
Brief trip back into Covid data today:
Promising news from South Africa, where the BA.4 / BA.5 variant wave has passed quietly, with high levels of immunity meaning this wave has had little impact on rates of severe illness or death pic.twitter.com/C5W6iZzDLK
South Africa never really had a BA.2 wave, so BA.4 and BA.5 mostly competed with other Omicron lineages in that country. But in the U.K., which did face BA.2, recent data suggest that BA.4 and BA.5 have a growth advantage over even BA.2.12.1. In other words, BA.4 and BA.5 could potentially outcompete BA.2.12.1 to become the most transmissible Omicron subvariants yet.
What are BA.4 and BA.5 doing in the U.S.?
The subvariants are definitely here and spreading, but we have limited visibility into where and how much thanks to declined testing and surveillance. The CDC has yet to separate out BA.4 and BA.5 on its variant dashboard; according to White House COVID-19 Data Director Cyrus Shahpar, this is because the CDC has yet to identify these subvariants as causing 1% or more of new national cases in a given week.
Updated variant proportions just posted. BA.2.12.1 now estimated to be ~59% of specimens sequenced last week. BA.4 and BA.5 not yet meeting the 1%+ threshold to be listed separately https://t.co/YIeQkH8YmEpic.twitter.com/SsSyoVO5Gh
— Dr. Cyrus Shahpar Archived (@cyrusshahpar46) May 31, 2022
But the CDC does include BA.4 and BA.5 in its Omicron B.1.1.529 category, which has grown from causing 1% of new cases in the first week of May to causing 6% of new cases in the last week of the month. The number of cases sequenced in a week has dropped this spring compared to the first Omicron surge, leading me to wonder: are BA.4/BA.5 really causing fewer than 1% of new cases each, or do we just not have the data to detect them yet?
CDC data do show that the B.1.1.529 group (which includes BA.4/BA.5) is causing over 10% of new cases in the Plain States, Gulf Coast, and Mountain West—compared to under 5% in the Northeast, where BA.2.12.1 is more dominant. This data aligns with local reports of BA.4 and BA.5 spreading in wastewater in some Midwestern states that track variants in their sewage. For example, scientists at the Metropolitan Council in the Twin Cities recently said they expect BA.4 and BA.5 to “replace BA.2.12.1 as the dominant variants” in the next few weeks.
What could BA.4 and BA.5 mean for future COVID-19 trends in the U.S.?
As I noted above, data from the U.K. suggest that BA.4 and BA.5 could outcompete BA.2—and even BA.2.12.1—to become the dominant Omicron subvariants in the U.S. Early data from U.S. Omicron sequences are showing a similar pattern, reported variant expert Trevor Bedford in a recent Twitter thread.
“Focusing on the US, we see that BA.2.12.1 currently has a logistic growth rate of 0.05 per day, while BA.4 and BA.5 have logistic growth rates of 0.09 and 0.14 per day,” Bedford wrote. The country’s rising case counts can be mostly attributed to BA.2.12.1, he said, but BA.4 and BA.5 are clearly gaining ground. And, he noted, these two subvariants may be able to reinfect many people who already had BA.1 or BA.2.
Thus, we expect at least some portion of the BA.4 / BA.5 epidemics to be driven by increased vaccine breakthrough and increased reinfection relative to current BA.2 circulation. 12/12
In short: even more Omicron breakthrough infections and reinfections could be coming our way. Even if BA.2.12.1 transmission dips (as it seems to be doing in the Northeast), we could quickly see new outbreaks driven by BA.4 and BA.5—leading overall case numbers to plateau or rise again.
“For the summer, going into the winter, I expect these viruses to be out there at relatively high levels,” Dr. Alex Greninger from the University of Washington’s clinical virology lab told CNN. “Just the number of cases, the sheer disruptions of the workforce — It’s just a very high, high burden of disease.”
In the past week (May 28 through June 3), the U.S. reported about 700,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 100,000 new cases each day
215 total new cases for every 100,000 Americans
9% fewer new cases than last week (May 21-27)
In the past week, the U.S. also reported about 27,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 3,800 new admissions each day
8.1 total admissions for every 100,000 Americans
5% more new admissions than last week
Additionally, the U.S. reported:
1,700 new COVID-19 deaths (0.5 for every 100,000 people)
94% of new cases are Omicron BA.2-caused; 59% BA.2.12.1-caused (as of May 28)
An average of 70,000 vaccinations per day (per Bloomberg)
The BA.2/BA.2.12.1 surge continues. According to the CDC, the number of new cases reported nationwide dropped last week, compared to the prior week; but this drop is more likely a result of the Memorial Day holiday than of an actual slowdown in transmission. (As I frequently note in these updates, holidays always result in case reporting dips as public health workers take time off.)
Despite the holiday, the country reported over 100,000 new cases a day last week. And, of course, this is a massive undercount. A new preprint from researchers at the City University of New York suggests that actual coronavirus infections during the BA.2/BA.2.12.1 surge may be 30 times as high as reported case counts—and that’s in New York City, which has better PCR infrastructure than most. (More on this study later in the issue.)
Unlike official case counts, the number of COVID-19 patients newly admitted to hospitals across the country rose last week: an average of 3,800 patients were admitted each day, a 5% increase from the prior week. Hospital admissions are more reliable than case counts, especially after a holiday, suggesting that we are indeed still on the upswing of this surge.
Similarly, coronavirus levels in the country’s wastewater keep rising. Biobot’s dashboard shows a continued national increase, as well as increases in the Midwest, West, and South regions. In the Northeast, virus levels dipped last week and now appear to be at a plateau.
Has the Northeast peaked? Optimistically, I would like to say yes, but a combination of spotty data and the Memorial Day holiday makes it tough to say for sure. In New York City, case rates dropped last week—but so did testing. In Boston, coronavirus concentrations in wastewater seem to be on a downturn—but the data are noisy.
And even if the Northeast is coming out of its BA.2/BA.2.12.1 surge, the rest of the country is on the opposite side of the wave. Reported case numbers in Southern and Midwest states like Missouri, Wyoming, Alabama, Utah, Mississippi, and Texas shot up by over 20% last week, while Hawaii and Florida now have the highest reported case rates, according to the June 2 Community Profile Report.
Even the CDC’s highly lenient Community Levels are beginning to light up yellow and orange, suggesting that counties from Florida to central California should reinstate indoor mask requirements. But are any leaders actually putting these measures in place? It seems unlikely, leaving the increasingly-smaller COVID-concerned minority to fend for ourselves.
It’s not all mild cases: new COVID-19 hospital admissions have been rising at a similar rate to cases in the last couple of weeks. Chart via the CDC.
In the past week (May 21 through 27), the U.S. reported about 770,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 110,000 new cases each day
234 total new cases for every 100,000 Americans
8% more new cases than last week (May 14-20)
In the past week, the U.S. also reported about 25,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 3,600 new admissions each day
7.7 total admissions for every 100,000 Americans
8% more new admissions than last week
Additionally, the U.S. reported:
2,200 new COVID-19 deaths (0.7 for every 100,000 people)
97% of new cases are Omicron BA.2-caused; 58% BA.2.12.1-caused (as of May 21)
An average of 70,000 vaccinations per day (per Bloomberg)
America’s largely-ignored BA.2 surge continues: the U.S. reported over 100,000 new cases a day last week, while an average of 3,600 new COVID-19 patients were admitted to hospitals each day. Both of these metrics rose about 8% from the week prior.
Of course, as I am frequently reminding everyone these days, current case numbers are a drastic undercount of actual infections, thanks to at-home testing and increasingly-fractured PCR access. Our current surge might actually be the country’s “second-largest wave of COVID-19 infections since the pandemic began,” Wall Street Journal reporter Josh Zumbrun wrote last week.
The culprits for this wave of infections are BA.2 and its sublineage BA.2.12.1; the latter is now causing more than half of new cases in the U.S., according to CDC estimates. Northeast states, which have been BA.2.12.1 hotspots for a few weeks now, continue to report the highest case rates: these include Rhode Island, Delaware, New Jersey, Massachusetts, D.C., and New York.
There are some promising signs that the BA.2 wave in these Northeast states may soon be on a downturn, if it isn’t already. Data from Biobot show that coronavirus levels in wastewater are dropping in this region, with reports from Bostonand from Maine contributing to this pattern. New York City, where I live, has reported a case plateau for the last week or so, but I’m hopeful that it could turn into a downturn soon.
what's up with COVID-19 in NYC right now? official case numbers have plateaued, and I think we could see a downturn soon. a cautiously optimistic thread: (1/9) pic.twitter.com/3T96FagCts
— betsy ladyzhets 📊 (@betsyladyzhets) May 26, 2022
But will this encouraging pattern in the Northeast withstand the holiday weekend of largely-unmasked travel and gatherings? It may be a couple of weeks before we know for sure, because the holiday will interrupt data reporting (as holidays always do). The CDC itself is taking a long weekend off, with no Weekly Review this past Friday and no data updates at all Saturday, Sunday, and Monday.
Meanwhile, COVID-19 deaths—the most lagging pandemic metric—are going up once again. More than 300 Americans died of the disease each day last week, in a 13% increase from the week prior. These are the consequences of our country’s continued failure to protect the vulnerable.
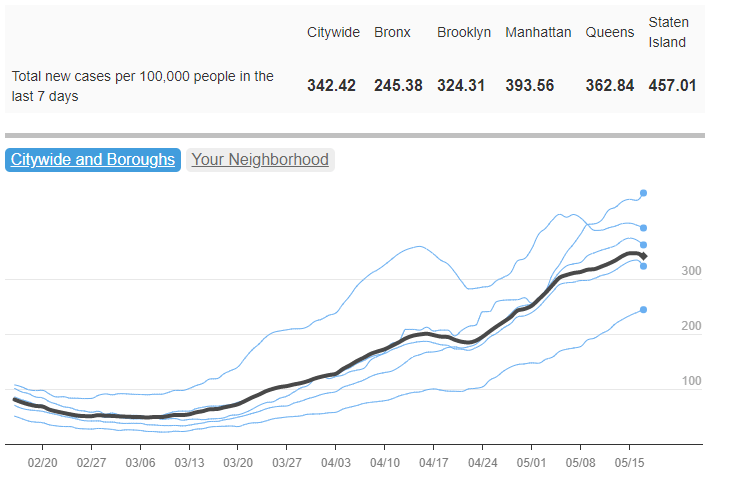
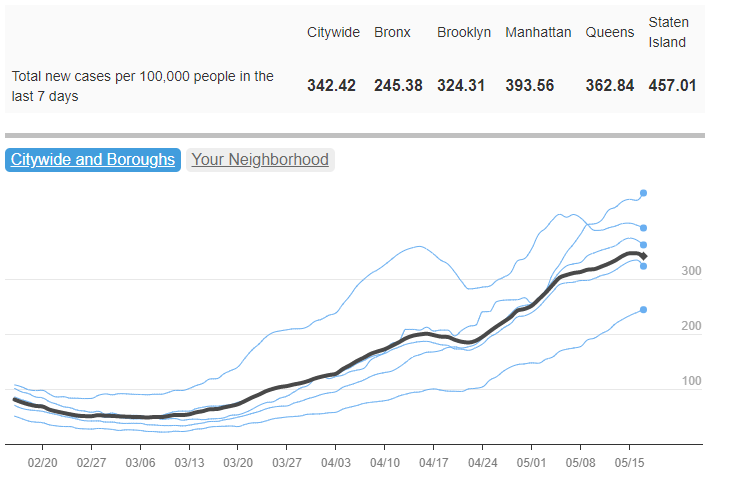
After appearing to peak in mid-April, COVID-19 case rates in New York City began going up again as BA.2.12.1 took over. Chart from NYC Health.
In the past week (May 14 through 20), the U.S. reported about 710,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 101,000 new cases each day
216 total new cases for every 100,000 Americans
19% more new cases than last week (May 7-13)
In the past week, the U.S. also reported about 23,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 3,300 new admissions each day
6.9 total admissions for every 100,000 Americans
24% more new admissions than last week
Additionally, the U.S. reported:
2,000 new COVID-19 deaths (0.6 for every 100,000 people)
98% of new cases are Omicron BA.2-caused; 48% BA.2.12.1-caused (as of May 14)
An average of 140,000 vaccinations per day (per Bloomberg)
The Omicron BA.2 surge continues in the U.S., with a 19% increase in officially-reported COVID-19 cases in the past week to over 100,000 new cases a day. Of course, the official case numbers severely underestimate true infections, as PCR testing sites close and more people use rapid tests; actual case counts may be five or more times higher.
New hospital admissions are also increasing: about 23,000 COVID-19 patients were admitted for care nationwide last week, up from 11,000 one month ago. While millions of Americans have some protection against severe disease from vaccination and/or prior Omicron infections, many are still susceptible. Hospitals are beginning to fill up again in almost every state, and as Ed Yong points out, the numbers don’t capture continued burnout among healthcare workers.
🚨I wrote about how the health-care system is faring. In many places, things are better than the winter's surge. But that's scant comfort. The system is now locked in a chronic, cumulative crisis that exerts a toll regardless of what COVID is doing. 1/ https://t.co/zZItleYRg5
BA.2.12.1, the most transmissible version of Omicron BA.2 now spreading in the U.S., accounted for almost half of new cases in the week ending May 14, according to CDC estimates. Northeast states remain hotspots: BA.2.12.1 caused about three in four new cases in New York and New Jersey last week.
One thing I’ve been wondering, in recent weeks, is when we might see cases peak in the Northeast. In New York City, where I live, case trends seemed to turn downward in mid-April; but then after about a week, the numbers went up again — perhaps a consequence of BA.2.12.1 taking over from BA.2.
COVID-19 trends from wastewater surveillance for the Northeast look similar to the case trends in NYC: a slow increase through March and April, followed by a potential plateau or further increases in May.
And other regions are catching up, according to Biobot’s tracker: states in the Midwest and South continue to see their coronavirus levels increase as the Northeast stagnates. Official case data from the latest Community Profile Report suggest that states such as Nebraska, Montana, Missouri, Kansas, and Kentucky reported the sharpest increases over the last week.
One piece of good news: new COVID-19 vaccinations rose slightly over the last week, going above 100,000 new shots administered daily for the first time in several months. Second booster shots in older adults and those with severe medical conditions are likely driving this increase, though, rather than shots for the previously unvaccinated.
As local leaders like NYC mayor Eric Adams refuse to institute new mask mandates and the country overall seems apathetic to this COVID-19 surge, it’s unclear how long we’ll be dealing with these Omciron subvariants — or how much we’ll invite the virus to keep mutating.
The US’s second Omicron surge is fully here.
At the end of Jan / beginning of Feb, my hypothesis was that if there wasnt a clear national surge by the end of March we would be basically surge-free until the fall.
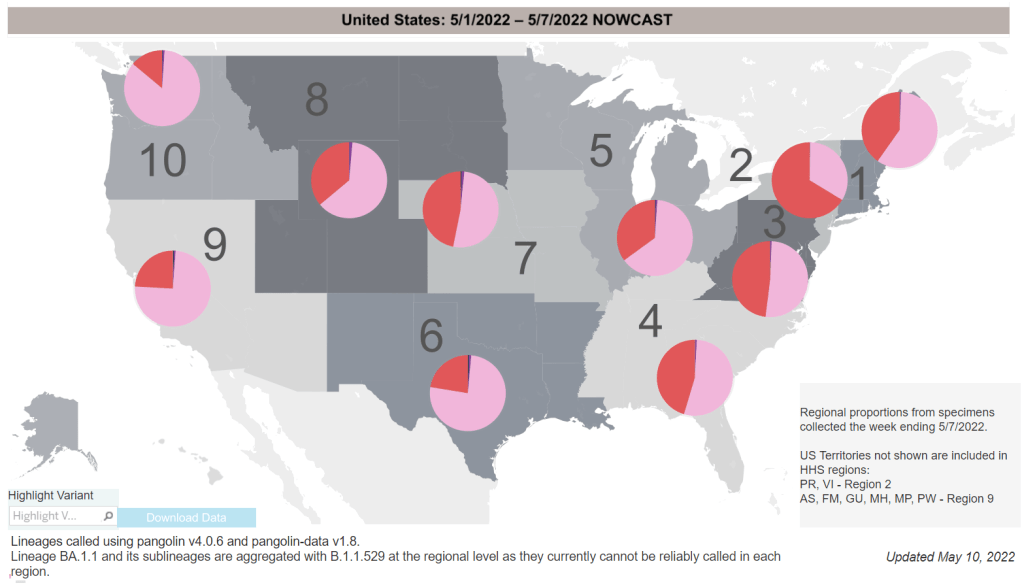
Omicron BA.2.12.1 (shown here in red) is taking over from BA.2 (pink) in much of the country, with the Northeast in the lead. Chart via the CDC, data as of May 7.
In the past week (May 7 through 13), the U.S. reported about 590,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 85,000 new cases each day
181 total new cases for every 100,000 Americans
31% more new cases than last week (April 30-May 6)
In the past week, the U.S. also reported about 18,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 2,600 new admissions each day
5.6 total admissions for every 100,000 Americans
18% more new admissions than last week
Additionally, the U.S. reported:
1,900 new COVID-19 deaths (0.6 for every 100,000 people)
99% of new cases are Omicron BA.2-caused; 43% BA.2.12.1-caused (as of May 7)
An average of 80,000 vaccinations per day (per Bloomberg)
New COVID-19 cases continue to rise in the U.S., with an average of 85,000 cases reported nationally each day last week—double the daily average from three weeks ago. This is a significant undercount, of course, as the majority of COVID-19 tests conducted these days are done at home.
The country is also reporting more COVID-19 patients admitted to hospitals: about 18,400 people were admitted last week, an 18% increase from the prior week. While this is far lower than the numbers reported during the peak of the Omicron wave (and includes some incidental hospitalizations), it’s still a concerning signal: even as immunity from prior vaccinations and infections protects many Americans from severe disease, plenty of people remain vulnerable.
This current increase is largely driven by the Omicron subvariant BA.2 and its offshoot BA.2.12.1, which is the most transmissible version of this lineage yet. BA.2.12.1 caused about 43% of new cases nationwide in the week ending May 7, according to CDC estimates; in parts of the Northeast, Midwest, and South, that ratio is over 50%.
The Northeast, which has the most BA.2.12.1, also continues to report the highest coronavirus levels in wastewater regionally, according to Biobot. After a potential plateau in recent weeks, the Northeast is now continuing to show a clear uptick; wastewater data from other parts of the country also indicate a slow increase in coronavirus transmission.
The CDC’s wastewater data somewhat reaffirm these trends, but are currently difficult to interpret as a number of sites have gone offline recently. (More on that later in the issue.)
States with the highest COVID-19 case rates continue to include Northeast states: Rhode Island, Massachusetts, New York, Maine, Vermont, New Jersey, and Washington, D.C. But some Midwest states (Illinois, Michigan, Wisconsin) as well as Hawaii are also reporting over 250 new cases per 100,000 people in the last week, showing how this BA.2 surge is spreading to other regions.
If you look at the CDC’s Community Level guidance, you may think that, even if you live in one of these surging Northeast states, you can go out in public without a mask. But other metrics, such as the agency’s old Community Transmission levels (which are based more on cases than hospitalizations), suggest otherwise.
1. Based on this week's @CDCgov transmission levels, 89% of the US population lives in a county classified as "substantial" or "high".
— Jason L. Salemi, PhD, FACE (@JasonSalemi) May 13, 2022
In short: if you want to protect yourself and others in your community, especially if you live in the Northeast, now is a good time to mask up, test often, and avoid large indoor gatherings.
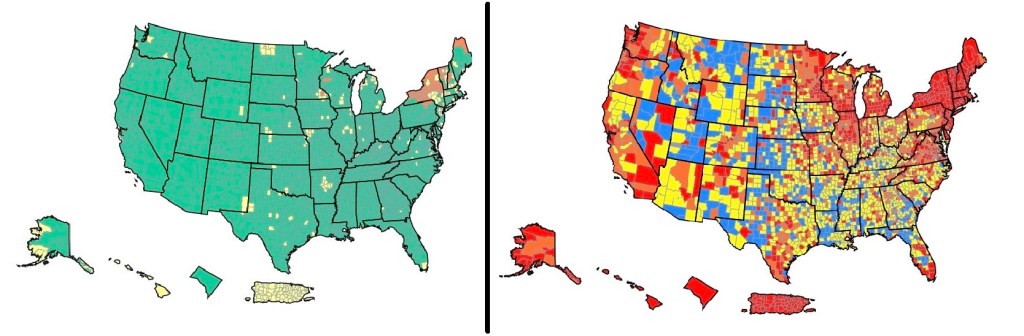
On the left, the CDC’s current Community Levels indicate that 90% of the U.S. is in a “low risk” region. On the right, the CDC’s old Transmission Levels indicate that only 15% of the country is in a “low risk” region.
In the past week (April 23 through 29), the U.S. reported about 370,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 53,000 new cases each day
113 total new cases for every 100,000 Americans
25% more new cases than last week (April 16-22)
In the past week, the U.S. also reported about 13,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 1,900 new admissions each day
4.0 total admissions for every 100,000 Americans
19% more new admissions than last week
Additionally, the U.S. reported:
2,300 new COVID-19 deaths (0.7 for every 100,000 people)
97% of new cases are Omicron BA.2-caused; 29% BA.2.12.1-caused (as of April 23)
An average of 80,000 vaccinations per day (per Bloomberg)
Nationwide, new COVID-19 cases have increased in the U.S. for the fourth week in a row. The daily case average has doubled since early April, and that’s just the cases that we’re reporting; with less PCR testing availability and more people using at-home tests, we have very limited visibility into this current uptick.
New hospital admissions, a more reliable metric than cases, have also continued to rise this week. U.S. hospitals reported about 13,200 COVID-19 patients admitted this week, up from under 10,000 in the first week of April.
Wastewater data similarly continue to indicate increased coronavirus spread. The Northeast is still in a high plateau, according to Biobot’s dashboard, while other parts of the country are reporting upticks.
This mirrors the reported case data: Northeast states Vermont, Rhode Island, New York, and Massachusetts reported the highest case rates in the week ending April 27, according to the latest Community Profile Report. But states in the South and West, such as North Carolina and Nebraska, reported the sharpest increases.
Almost one-third of new cases were caused by the BA.2.12.1 subvariant in the week ending April 23, according to the CDC’s latest estimates. This version of Omicron, first identified by the New York state health department, is even more transmissible than BA.2. It’s causing more than half of cases in the New York and New Jersey region, the CDC estimates.
Despite all of these concerning signals, the vast majority of the country seems unaware that we are in a new COVID-19 spike. Indeed, I’m writing this from the plane back to New York City, on which I’m one of few mask-wearers.
And I can’t really blame my fellow travelers for their lack of awareness: if you just look at the CDC’s Community Level map—as the agency recommends people do—you’d think that the whole country is in a green, low-risk zone. The agency’s old guidance, with more stringent, case-based thresholds, paints a very different picture.
Here are the 2 CDC COVID maps. The one on the left is the community level map which suggests 90% of the US has low risk. The map on the right of actual virus transmission levels shows a different story where only 15% of the country is low risk. pic.twitter.com/gf2NyF9OKf
The U.S. has “reached the choose-your-own-adventure stage of the pandemic,” as Maryn McKenna put it in a recent WIRED article. We’re taking “individual responsibility” to a whole new level.
Coronavirus levels in wastewater may be plateauing in the Northeast, while the remaining regions of the country catch up. Chart via Biobot, retrieved on April 24.
In the past week (April 16 through 22), the U.S. reported about 300,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 43,000 new cases each day
91 total new cases for every 100,000 Americans
35% more new cases than last week (April 9-15)
In the past week, the U.S. also reported about 11,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 1,600 new admissions each day
3.4 total admissions for every 100,000 Americans
8% more new admissions than last week
Additionally, the U.S. reported:
2,600 new COVID-19 deaths (0.8 for every 100,000 people)
93% of new cases are Omicron BA.2-caused; 19% BA.2.12.1-caused (as of April 16)
An average of 100,000 vaccinations per day (per Bloomberg)
After weeks of me warning about it, a BA.2 surge is upon us. Nationwide, new COVID-19 cases have gone up for the third week in a row; we’ve seen a 68% increase since the last week of March.
And that’s just the reported cases: Americans may be doing about four times more at-home tests than they’re doing lab-based PCR tests, according to Mara Aspinall, a COVID-19 testing expert (who cowrites a testing-focused newsletter). The vast majority of these at-home tests are never reported to public health officials and don’t make it into our trends analysis.
But there are other metrics that similarly indicate a national rise in coronavirus transmission. Viral levels in wastewater are going up, according to both Biobot’s tracker and the CDC’s national monitoring system; the CDC’s COVID-19 data team noted in this Friday’s Weekly Review that “more than half of all sites reporting wastewater data are experiencing a modest increase in SARS-CoV-2 levels.” Some of these increases are going from very low to still low, but they’re still worth watching.
The U.S. is also reporting an increase in new COVID-19 patients admitted to hospitals: about 11,000 people this week, up from 10,000 last week. New hospitalizations lag behind cases slightly, but they are a more reliable metric, as anyone with symptoms severe enough to require hospitalization generally will seek care (so, underreporting is less of a concern.)
At the regional level, the Northeast is still seeing the highest case rates: leading jurisdictions include Vermont, Washington D.C., New York, Rhode Island, and Massachusetts, according to the April 21 Community Profile Report. The Northeast—particularly New York and New Jersey—is also a hotspot for the Omicron sub-subvariant, BA.2.12.1.
To borrow an analogy from my sister (an engineering student): the emergence of these new Omicron sublineages feels like when you’re trying to do a problem set that claims to have five problems, but then each problem has several sub-problems, and those sub-problems themselves have more sub-problems. In the coming weeks, we’ll see just how much more transmissible Omicron can get.
There’s some good news, though: cases in some parts of the Northeast might be plateauing. It’s hard to tell for sure because of the aforementioned unreliable data, but wastewater data for the region (as well as for individual cities like Boston) seem to be leveling off; we’ll see next week if this trend continues.