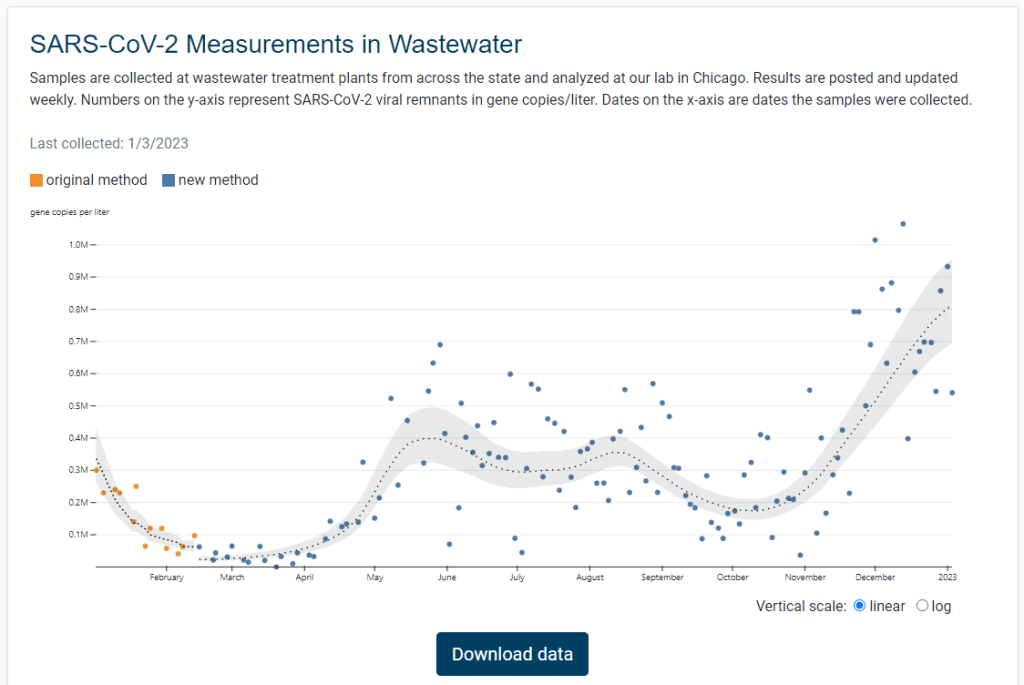
Illinois is the latest state to get its own dashboard for COVID-19 wastewater surveillance, with a new website that launched earlier this week. It includes data for 75 sites across the state.
The new dashboard—like the state’s wastewater surveillance program itself—is a collaboration between the Illinois Department of Public Health and the Discovery Partners Institute, a research center at the University of Illinois. Illinois’ agency received more than $6.5 million in federal grants to fund wastewater testing, according to local TV station WTTW.
I poked around a bit on the new dashboard, and I’m a fan: it includes a map of sampling locations, charts showing COVID-19 trends over time, easily-downloadable data, and ample information on how to interpret results. Nice work, Illinois!
New Long COVID review from PLRC and Scripps: Leading Long COVID researchers from the Patient-Led Research Collaborative and the Scripps Research Translational Institute collaborated on a review paper published this week in Nature, summarizing major findings from the literature so far. The paper includes summaries of major symptoms (ranging from cardiac damage to cognitive impairment), correlations between Long COVID and other chronic diseases (ME/CFS, POTS, etc.), treatment options for specific symptoms and/or biological mechanisms, and much more. I haven’t had a chance to read the paper in full yet, but I anticipate that it will be a valuable resource for future research.
Vaccines still reduce risk of transmission: Another recent paper in Nature reports on the impact of vaccination among inmates in the California state prison system. Researchers at the University of California San Francisco analyzed COVID-19 surveillance data from 35 prisons during the early months of Omicron (December 2021 to May 2022). They found patients infected with Omicron after vaccination and/or a prior infection had lower risks of transmitting the virus to others. The study suggests that vaccination (and prior infection) is still helpful in reducing COVID-19 spread in addition to reducing severe symptoms, even at this point in the pandemic. (H/t Your Local Epidemiologist.)
Coronavirus found in airplane wastewater on international flights: In a small study, researchers at the National Public Health Laboratory of Malaysia tested wastewater samples from 29 flights that arrived at Kuala Lumpur from outside the country. The researchers found that SARS-CoV-2 was present on 28 of the 29 flights—and testing for the remaining flight wasn’t yet complete, according to a local news outlet that covered the study. While this is a relatively small sample, the results suggest that COVID-19 is very prevalent in travel settings. The study also serves as a helpful example for future plane wastewater testing.
New report highlights nursing home issues: A recent report from the American Health Care Association shares results from a survey of 524 nursing homes across the U.S. The findings show challenges with staffing and economic challenges; for example, 84% of the nursing homes surveyed reported “moderate to high levels of staffing shortages,” and 67% of the homes surveyed reported concerns that they may need to close their facilities due to staffing problems. (H/t POLITICO Pulse.)
End of Ebola outbreak in Uganda: Finally, a bit of (non-COVID-19) good news: this week, health officials in Uganda declared the end of the country’s recent Ebola outbreak. The outbreak started in September 2022, and included a total of 164 cases and 55 deaths. The final patient of this outbreak was released from healthcare on November 30, according to the World Health Organization; Uganda successfully curbed the disease’s spread despite a lack of vaccines and treatments approved against the strain of Ebola that was spreading.
China is currently facing a massive COVID-19 surge, after ending many of its stringent “zero COVID” policies in December. Some estimates suggest that the country is experiencing over a million new cases each day, and widespread travel over the Lunar New Year later this month will likely prolong the surge.
Among U.S. media outlets covering the situation, a common topic is China’s lack of reliable COVID-19 data. For example: “The country no longer tallies asymptomatic infections or reliably reports COVID deaths—employing not the distortion of statistics but their omission,” writes Dhruv Khullar in The New Yorker.
Articles like Khullar’s accurately describe how difficult it is to understand the scale of COVID-19’s impact on a country without accurate data. But they fail to explain that this is far from a uniquely Chinese problem. In fact, many of the same claims that writers and health experts have made about China could also apply to the U.S., albeit on a different scale.
Some examples:
Without widespread PCR testing, officially-reported case counts are likely significant underestimates of true infections.
Public health agencies are no longer doing widespread contact tracing or attempting to track asymptomatic cases.
Unchecked spread of the virus could contribute to the development of new variants that evade prior infections and/or vaccinations, but such variants will be hard to quickly identify due to low testing rates.
This Twitter thread, from the writer and podcast host Artie Vierkant, shows the similarities pretty clearly:
Brief thread of how basically every article about covid in China right now (left) exceptionalizes things that are also existing, huge problems in the US and internationally (right) pic.twitter.com/hnaCBTf6G0
Don’t get me wrong—the current surge in China is an immense tragedy. But we can’t talk about it in a vacuum, or ignore the very similar problems plaguing the U.S. and many other countries. Poor COVID-19 data is, unfortunately, a global issue right now.
It’s the fourth year of the pandemic. I’ve written this statement in a few pitches and planning documents recently, and was struck by how it feels simultaneously unbelievable—wasn’t March 2020, like, yesterday?—and not believable enough—haven’t we been doing this pandemic thing for an eternity already?
As someone who’s been reporting on COVID-19 since the beginning, a new year is a good opportunity to parse out that feels-like-eternity. So this week, I reflected on the major trends and topics I hope to cover in 2023—both building on my work from prior years and taking it in new directions.
(Note: I actually planned to do this post last week, but then XBB.1.5 took higher priority. Hence its arrival two weeks into the new year.)
Expansions of wastewater, and other new forms of disease surveillance
As 2022 brought on the decline of large-scale PCR testing, wastewater surveillance has proven itself as a way to more accurately track COVID-19 at the population level—even as some health departments remain wary of its utility. We also saw the technology’s use for tracking monkeypox, polio, and other conditions: the WastewaterSCAN project, for example, now reports on six different diseases.
This year, I expect that wastewater researchers and public agencies will continue expanding their use of this surveillance technology. That will likely mean more diseases as well as more specific testing locations, in addition to entire sewersheds. For example, we’re already seeing wastewater testing on airplanes. I’m also interested in following other, newer methods for tracking diseases, such as air quality monitors and wearable devices.
At the same time, these surveillance technologies will continue to face challenges around standardization and public buy-in. The CDC’s big contract with Biobot expires this month, and I’ve already noticed a decline in sites with recent data on the agency’s dashboard—will CDC officials and local agencies step in to fill gaps, or will wastewater testing become even more sporadic?
New variants, and how we track them
For scientists who track the coronavirus’ continued evolution, 2022 was the year of Omicron. We didn’t see all-new virus lineages sweeping the world; instead, Omicron just kept mutating, and mutating, and mutating. It seems likely that this pattern will continue in 2023, but experts need to continue watching the mutation landscape and preparing for anything truly concerning.
With declining PCR testing, public agencies and companies that track variants have fewer samples to sequence. (This led to challenges for the CDC team tracking XBB.1.5 over the holidays.) As a result, I believe 2023 will see increased creativity in how we keep an eye on these variants—whether that’s sequencing wastewater samples, taking samples directly from healthcare settings, increased focus on travel surveillance, or other methods.
Public health experts—and journalists like myself—also need to rethink how we communicate about variants. It’s no longer true that every new, somewhat-more-contagious variant warrants alarm bells: variants can take off in some countries or regions while having relatively little impact in others, thanks to differences in prior immunity, seasonality, behavior, etc. But new variants still contribute to continued reinfections, severe symptoms, Long COVID, and other impacts of COVID-19. Grid’s Jonathan Lambert recently wrote a helpful article exploring these communication challenges.
Long COVID and related chronic diseases
As regular readers likely know, Long COVID has been an increased topic of interest for me over the last two years. I’ve covered everything from disability benefits to mental health challenges, and am now leading a major project at MuckRock that will focus on government accountability for the Long COVID crisis.
Long COVID is the epidemic following the pandemic. Millions of Americans are disabled by this condition, whether they’ve been pushed out of work or are managing milder lingering symptoms. Some people are approaching their three-year anniversary of first getting sick, yet they’ve received a fraction of the government response that acute COVID-19 got. Major research projects are going in the wrong directions, while major media publications often publish articles with incorrect science.
For me, seeing poor Long COVID coverage elsewhere is great motivation to continue reporting on this topic myself, at MuckRock and other outlets. I’m also planning to spend more time reading about (and hopefully covering) other chronic diseases that are co-diagnosed with Long COVID, like ME/CFS and dysautonomia.
Ending the federal public health emergency.
Last year, we saw many state and local health agencies transition from treating COVID-19 as a health emergency to treating it as an endemic disease, like the many others that they respond to on a routine basis. This transition often accompanied changes in data reporting, such as shifts from daily to weekly COVID-19 updates.
This year, the federal government will likely do the same thing. POLITICO reported this week that the Biden administration is renewing the federal public health emergency in January, but will likely allow it to expire in the spring or summer. The Department of Health and Human Services has committed to telling state leaders about this expiration 60 days before it happens.
I previously wrote about what the end of the federal emergency could mean for COVID-19 data: changes will include less authority for the CDC, less funding for state and local health departments, and vaccines and treatments controlled by private markets rather than the federal government. I anticipate following up on this reporting when the emergency actually ends.
Transforming the U.S. public health system
Finally, I intend to follow how public health agencies learn from—or fail to learn from—the pandemic. COVID-19 exposed so many cracks in America’s public health system, from out-of-date electronic records systems to communication and trust issues. The pandemic should be a wakeup call for agencies to get their act together, before a new crisis hits.
But will that actually happen? Rachel Cohrs has a great piece in STAT this week about the challenges that systemic public health reform faces, including a lack of funding from Congress and disagreements among experts on what changes are necessary. Still, the window for change is open right now, and it may not be at this point in 2024.
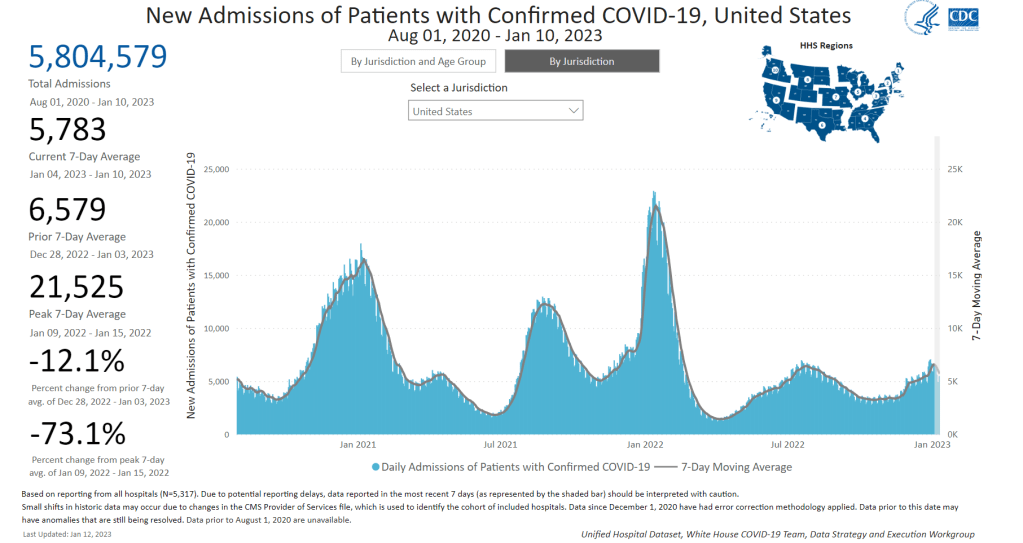
New hospital admissions for COVID-19 are starting to trend down, according to the CDC, though we’ll need more data to see if this trend persists.
In the past week (January 5 through 11), the U.S. officially reported about 420,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 59,000 new cases each day
126 total new cases for every 100,000 Americans
13% fewer new cases than last week (December 29-January 4)
In the past week, the U.S. also reported about 40,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 5,800 new admissions each day
12.3 total admissions for every 100,000 Americans
12% fewer new admissions than last week
Additionally, the U.S. reported:
3,900 new COVID-19 deaths (560 per day)
43% of new cases are caused by Omicron XBB.1.5; 45% by BQ.1 and BQ.1.1 (as of January 14)
An average of 150,000 vaccinations per day (CDC link)
Last week, I wrote that a combination of holiday travel/gatherings and the latest Omicron subvariant, XBB.1.5, was driving a winter surge. This week, COVID-19 metrics suggest that the surge may have peaked, though we’ll need more data to say for sure—and XBB.1.5 remains a concern.
After reporting a significant increase in coronavirus levels through the end of December, Biobot’s wastewater dashboard is now showing downturns nationally and for all four U.S. regions. The CDC’s wastewater dashboard similarly shows that about two-thirds of sites in the National Wastewater Surveillance System have reported decreasing COVID-19 levels in the last two weeks, as of January 10.
“Importantly, this data is subject to change as we update 2x weekly,” Biobot’s Twitter shared on Thursday, when the company’s dashboard was most recently updated. “Stay tuned for Tuesday’s update.”
📣Our #Covid ww dashboard has been updated—https://t.co/GBL4twvGGT. We’re seeing a drop in concentrations in all regions, which may indicate the passing of the holiday surge. Importantly, this data is subject to change as we update 2x weekly. Stay tuned for Tuesday’s update.
Official COVID-19 cases and hospital admissions are also trending down, according to CDC data: new cases dropped by 13% from the week ending January 4 to the week ending January 11, while newly hospitalized patients dropped by 12%. But this trend isn’t universal; five states and Washington D.C. reported increased hospitalizations this week, with the biggest upticks in Rhode Island, Louisiana, and Maine.
XBB.1.5, the latest and most contagious Omicron subvariant, caused an estimated 43% of new cases nationwide in the week ending January 14, per the CDC. It’s clearly outcompeting BQ.1 and BQ.1.1 as well as a number of other strains in the “Omicron soup” we currently face, but is not taking over as quickly as we saw the original Omicron do in late 2021.
This strain continues to dominate the Northeast—particularly New England and New York/New Jersey—where COVID-19 spread is trending down. But it’s just starting to pick up in other parts of the country; to me, it seems likely that the Northeast had a holidays-and-XBB.1.5 combined surge, while other areas may face a second COVID-19 increase as this variant spreads more widely.
Meanwhile, other respiratory viruses continue to place additional burden on our health system. For example, the CDC recently released estimates about this year’s flu season, finding that the flu may have caused up to 560,000 hospitalizations and 48,000 deaths since fall 2022.
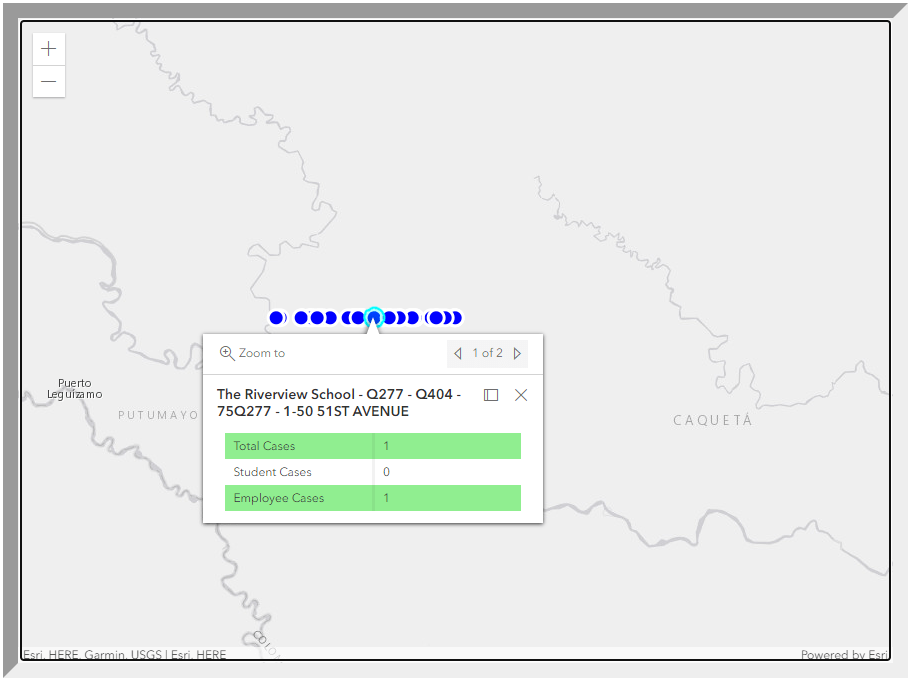
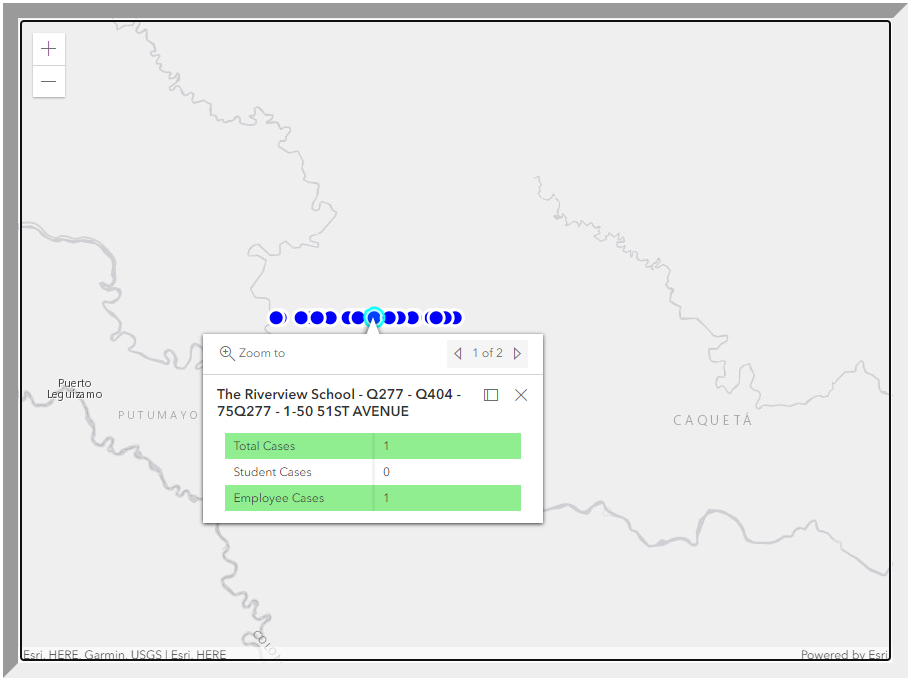
The error appears to be a problem with the dashboard’s geographical tagging, putting these schools in another continent instead of their correct NYC neighborhoods. But it’s a pretty big issue for parents and school staff who might be checking the map, looking for COVID-19 cases at their schools.
If these users didn’t know to zoom out and then scroll down a fair amount—which they probably wouldn’t, unless they got very creative or followed the right people on Twitter—they would think there were no cases. Which is far from the truth.
NIH launches at-home testing telehealth program: This week, the National Institutes of Health announced the first location for “Home Test to Treat,” a new program that will make it easier for people in vulnerable communities to receive Paxlovid after testing positive on at-home, rapid tests. The Biden administration first announced this program in September, but it’s formally launching now with Berks County, Pennsylvania as the first participating community. As Paxlovid shifts to a drug that must be privately purchased instead of provided for free by the federal government, more programs like this one will be needed to fill access gaps.
Study estimates global Long COVID prevalence: A large team of researchers, led by population health scientists at the University of Washington, conducted an extensive review of Long COVID symptoms. The analysis used 54 prior studies and two medical record databases, incorporating data from 1.2 million people in total. Overall, about 6% of patients reported at least one class of Long COVID symptoms three months after their initial infections, with the vast majority of cases occurring in people who had mild acute cases. The study was published in JAMA in October, but gained attention this week thanks to an article that its leading authors wrote in The Conversation.
China’s COVID-19 data are unreliable: It’s been about a month since China loosened its COVID-19 protocols in the wake of protests and contagious Omicron subvariants, and the country is now facing a massive surge—with as many as one million new cases a day according to some modeling estimates. Yet COVID-19 deaths reported in the country have been very low, fewer than five a day. This discrepancy suggests that China’s authorities are not correctly counting their COVID-19 deaths, while the country’s dismantled testing infrastructure has also led to less reliable case numbers. Officials from the World Health Organization have formally called on the country to “be more forthcoming with information” about its COVID-19 surge, reports Helen Branswell at STAT News.
CDC testing airplane wastewater on flights from China: In response to surveillance concerns, the CDC is working to test wastewater on flights arriving from China in select U.S. airports. This method is, of course, more efficient than testing every single traveler from the country in the interest of identifying any new variants that might arise. (Though it’s worth noting that some experts are skeptical about the potential of new variants arising in China.) Scientists from Concentric, a company that works with the CDC on traveler surveillance, previously talked about plane wastewater testing during our interview in November.
Race/ethnicity differences among child vaccination rates: Finally, a notable study in this week’s CDC Morbidity and Mortality Weekly Report: researchers at the CDC and collaborators examined vaccination rates among children ages five to 17 using data from the National Immunization Survey. They found vaccination coverage (with at least one dose) was highest among Asian children (at about 75%), followed by Hispanic or Latino children (49%), white children (45%), and Black children (43%). The researchers also noted differences among vaccination rates by other socioeconomic factors, and by parents’ mask-wearing habits.
In the last week of December, I had a major story published at MuckRock, USA TODAY, and local newsrooms in Arizona, Oregon, and Texas. The story explains that official COVID-19 statistics underestimate the pandemic’s true toll—particularly on people of color, who are more likely to have their deaths inaccurately represented in mortality data.
We already knew that the COVID-19 pandemic widened existing health disparities in the US. But the official statistics only show a piece of COVID-19's true toll.
This story was part of Uncounted, MuckRock’s broader project to investigate death certificate errors and other death reporting issues uncovered by looking at all excess deaths during the pandemic, not just those deaths officially marked as COVID-19. It relies on data from the CDC’s provisional mortality statistics and excess death estimates by a team of demography researchers at Boston University led by Andrew Stokes.
I’ve copied the introductory section of the story here, because I don’t think anything else I write would do a better job at summarizing it. I encourage you to read the full piece; it is the biggest (and likely most important) story that I wrote in 2022.
It’s not always easy to identify a COVID-19 death.
If someone dies at home, if they have symptoms not typically associated with the disease or if they die when local health systems are overwhelmed, their death certificate might say “heart disease” or “natural causes” when COVID-19 is, in fact, at fault.
New research shows such inaccuracies also are more likely for Americans who are Black, Hispanic, Asian or Native.
The true toll of the COVID-19 pandemic on many communities of color – from Portland, Oregon, to Navajo Nation tribal lands in Arizona, New Mexico and Utah, to sparsely populated rural Texas towns – is worse than previously known.
Incorrect death certificates add to the racial and ethnic health disparities exacerbated by the pandemic, which stem from long-entrenched barriers to medical care, employment, education, housing and other factors. Mortality data from the Centers for Disease Control and Prevention point to COVID-19’s disastrous impacts, in a new analysis by the Documenting COVID-19 Project at Columbia University’s Brown Institute for Media Innovation and MuckRock, in collaboration with Boston University’s School of Global Public Health; the USA TODAY Network; the Arizona Center for Investigative Reporting; Willamette Week in Portland; and the Texas Observer.
The data shows that deaths from causes the CDC and physicians routinely link to COVID– including heart disease, respiratory illnesses, diabetes and hypertension–have soared and remained high for certain racial and ethnic groups.
In Arizona’s Navajo and Apache counties, which share territory with Navajo Nation, COVID deaths among Native Americans drove nation-leading excess death rates in 2020 and 2021. While COVID death rates among Natives dropped during the second year of the pandemic thanks to local health efforts, other causes of death such as car accidents and alcohol poisoning increased significantly from 2020 to 2021.
In Portland, deaths from causes indirectly related to the pandemic went up in 2021 even as official COVID deaths remained relatively constant. Black residents were disproportionately impacted by some of these causes, such as heart disease and overdose deaths – despite a county-wide commitment to addressing racism as a public health threat.
In Texas, smaller, rural counties served by Justices of the Peace were more likely to report potential undercounting of COVID deaths than larger, urban counties served by medical examiners. Justices of the Peace receive limited training in filling out death certificates and often do not have sufficient access to postmortem COVID testing, local experts say.
Experts point to several reasons for increased inaccurate death certificates among non-white Americans. These include resources available for death investigations, the use of general or unknown causes on death certificates, and how the race and ethnicity fields of these certificates are filled out.
Such barriers to accurate death reporting add on to existing health disparities that made non-white Americans more susceptible to COVID in 2021, despite widespread vaccination campaigns and health equity efforts.
“Even if you try to level the playing field, from the jump, certain populations are dealing with things that put them at greater risk,” said Enrique Neblett, a health equity expert at the University of Michigan’s School of Public Health. These issues include higher exposure to COVID, as people of color are overrepresented among essential workers, as well as higher rates of chronic conditions that confer risk for severe disease. “Those things aren’t eliminated just by increasing access to a vaccine,” Neblett said.
It is critical to improve data collection and reporting for deaths beyond those officially labeled as COVID because data is a “major political determinant of health,” said Daniel Dawes, executive director of the Satcher Health Leadership Institute at the Morehouse School of Medicine. Information on how people are dying in a particular community can shape priorities for local public health departments and funding for health initiatives.
“If there is no data, there is no problem,” Dawes said.
XBB.1.5 caused about 28% of new cases in the week ending January 7 (confidence interval: 14% to 47%), according to the CDC’s estimates.
You’ve probably seen it in the news this week: XBB.1.5 is the latest Omicron subvariant to spread rapidly through the U.S.
It is, of course, more transmissible and more capable of evading immunity from past infections than other versions of Omicron that have gone before it, as this lineage continues mutating. Scientists are still learning about XBB.1.5; it emerged from the U.S. during the holiday season, which has posed surveillance challenges. But we know enough to say that this variant is bad news for an already overstretched healthcare system.
Here’s a brief FAQ post on XBB.1.5.
Where did XBB.1.5 come from?
XBB, the parent of this latest lineage, emerged in Asia in October 2022. It evolved from Omicron BA.2 via recombination, which basically means two different BA.2 subvariants fused—likely while the same person was infected with both—and formed this new strain. (See my variants post from October for more details on XBB.)
XBB started spreading and mutating in the U.S. a few weeks later, leading to XBB.1.5. This subvariant was first identified in New York State in mid-December, though it could have evolved elsewhere in the northeast (since New York has better variant surveillance than some other states). Eric Topol’s newsletter has more details about XBB evolution.
New variant to watch
XBB.1.5 really taking off in New York, where it appears to have evolved
BQ.1* in NY has been almost flat since dominance in Nov
What are XBB.1.5’s advantages compared to other variants?
It spreads faster, likely because it is more capable of evading immune system protections from past infection or vaccination than other Omicron subvariants. In the U.S., CDC data suggests that XBB.1.5 is starting to outcompete other lineages in the “Omicron variant soup” we currently have circulating.
BQ.1.1 and XBB (original) were already known to be the best-evolved subvariants in this area before XBB.1.5 came along, according to this December 2022 paper in Cell. XBB.1.5 has taken this immune escape further, as it evolved a mutation called F486P that’s tied to this property.
“It’s crazy infectious,” Paula Cannon, a virologist at the University of Southern California, told USA TODAY reporter Karen Weintraub. Cannon added that protections that have worked against other coronavirus strains for the last three years will likely be less effective against XBB.1.5 and other new variants.
What questions are scientists currently working to answer about XBB.1.5?
One major question that arises with any new subvariant is severity: will XBB.1.5 have a higher capacity to cause severe symptoms than other coronavirus lineages? (We now know, for example, that Delta was more severe compared to prior variants.)
The World Health Organization is currently working on a report about XBB.1.5’s severity, according to POLITICO. Scientists and public health officials will also study whether current COVID-19 treatments work against this subvariant. Antiviral treatments Paxlovid and Mulnopiravir likely won’t be impacted, but Omicron’s continued evolution has put a lot of restrictions on monoclonal antibodies.
Another important question will be how well our updated booster shots work against XBB.1.5. The shots used in the U.S. were primed for BA.4 and BA.5, while XBB is derived (albeit indirectly) from BA.2, so our shots are not the best match. Still, antibody neutralization studies have shown that the shots provide protection against XBB, meaning some impact on XBB.1.5 is likely. This is a great time to get your booster if you haven’t yet.
What impact is XBB.1.5 currently having in the U.S.?
The subvariant caused about 28% of new cases in the week ending January 7, according to CDC estimates. These estimates have a fairly wide confidence interval, though, meaning that XBB.1.5’s true prevalence could be between 14% and 47%; the CDC will improve these estimates in the coming weeks as it collects more XBB.1.5 samples.
But we know with more confidence that XBB.1.5 has already taken over in the Northeast. It’s causing the vast majority of cases in HHS Region 1 (New England) and Region 2 (New York and New Jersey). Other mid-Atlantic states are catching up.
Some experts have noted that New York and other Northeast states are currently reporting rising COVID-19 hospitalizations, which could be a sign that XBB.1.5 causes more severe disease. It’s currently unclear how much the increased hospitalizations may be attributed to XBB.1.5’s presence, though, as the entire country is seeing this trend already in the wake of the holidays.
Sam Scarpino, a disease surveillance expert at Northeastern University, has a helpful Twitter thread explaining this issue. “It’s clear that XBB.1.5 is correlated [to] an increase in hospitalizations in many highly vaccinated states,” he writes. “I suspect it will hit harder in states with lower bivalent booster rates.”
1/ For those concerned about #XBB15 and hospitalizations, I think the evidence is more mixed than many are admitting.
While it's true hospitalizations are up in states like MA where XBB.1.5 is common, they are up across the entire US, even in states w/ little-to-no #XBB15! pic.twitter.com/LVrYqjn44K
Why has XBB.1.5’s prevalence been harder to pin down than other subvariants?
Many of the news articles you might have read this week about XBB.1.5 cited that the subvariant’s prevalence more than doubled in about one week, according to CDC estimates. But then the CDC’s estimates were revised down this week, suggesting that XBB.1.5 actually caused 18% of new cases in the last week of December—not 41%.
Why did the estimate change so dramatically? Well, it actually didn’t: as the CDC itself pointed out in its Weekly Review newsletter this Friday, the 41% estimate had a big confidence interval (23% to 61%), so the revision down to 18% was not far outside the existing realm of possibility. The CDC revises its variant estimates constantly as new data come in; this might be a bigger shift than we’re used to seeing, but it’s still pretty unsurprising.
The CDC’s variant forecasting team is also facing a couple of challenges unique to XBB.1.5 right now. First, this is a homegrown, U.S.-derived variant, so they don’t have a wealth of international sequences to analyze in preparation for a U.S. surge. And second, XBB.1.5 arose during the holidays, when a lot of COVID-19 testing and sequencing organizations were taking time off. The CDC is currently working with very limited data, but it will continue to revise estimates—and make them more accurate—as more test results come in.
For more info on the CDC’s process here, I recommend this Twitter thread from epidemiologist Duncan MacCannell:
The variant surveillance dashboard on the CDC COVID Data Tracker was just updated to include projections up to 1/7/2022; this is a weekly update that posts like clockwork every Friday. https://t.co/rnE66MCoHSpic.twitter.com/WGtfHix8va
How will XBB.1.5 impact the next phase of the pandemic?
Scientists will be closely watching to see how quickly XBB.1.5 spreads in other parts of the U.S., as well as how it performs in other countries that recently had surges of other Omicron subvariants.
Overall, the data we have about this subvariant so far suggest that it’s not distinct enough from other versions of Omicron to drive a massive new surge on the level of Omicron BA.1 last winter. But it’s still arriving in the wake of holiday travel and gatherings—and in a country that has largely abandoned public health measures that stop the virus from spreading.
In New York, for example, XBB.1.5 might not be the main cause of rising hospitalizations. Yet it is undoubtedly making more people sick with COVID-19, at a time when this region also faces continued healthcare pressure from flu and RSV. And an impending nurses’ strike won’t help the situation either, to put it mildly.
I think this Twitter thread from T. Ryan Gregory, an evolutionary biology expert who tracks coronavirus variants, is helpful at putting XBB.1.5 into context. This latest lineage follows other versions of Omicron that have kept the U.S. and other countries at relatively high levels of COVID-19 transmission throughout the last year. While our current moment may not look as dire as January 2022, we are currently seeing COVID-19 go up from an already-unsustainable baseline.
“BA.1 was the highest peak,” he writes, referring to 2022 in Canada and the U.K., “but the area under the curve of the others was as bad or worse.”
That said, I don't think "not as bad as the first Omicron wave" should be the standard. As noted, Canada, the UK, etc. had their deadliest year in 2022 through multiple Omicron waves. BA.1 was the highest peak, but the area under the curve of the others was as bad or worse. pic.twitter.com/5JwU857oHo
In the past week (December 29 through January 4), the U.S. officially reported about 470,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 67,000 new cases each day
143 total new cases for every 100,000 Americans
16% more new cases than last week (December 22-28)
In the past week, the U.S. also reported about 46,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 6,500 new admissions each day
13.9 total admissions for every 100,000 Americans
16% more new admissions than last week
Additionally, the U.S. reported:
2,700 new COVID-19 deaths (390 per day)
28% of new cases are caused by Omicron XBB.1.5; 56% by BQ.1 and BQ.1.1; 5% by XBB (as of January 7)
An average of 150,000 vaccinations per day
Well, here we are: the winter COVID-19 surge. It may have happened later than some experts predicted, but the U.S. is clearly now experiencing an uptick in virus transmission as the latest, most contagious Omicron subvariants collide with holiday travel and gatherings.
You might notice that the CDC’s official case numbers didn’t rise too dramatically this week (though the national count is up 16% compared to last week). That’s unsurprising: case increases after holidays are always delayed, because many testing sites and public health officials take time off from processing new data. Christmas and New Year’s tend to deliver the worst of this trend—and in 2022, limited access to PCR testing made case numbers even less reliable.
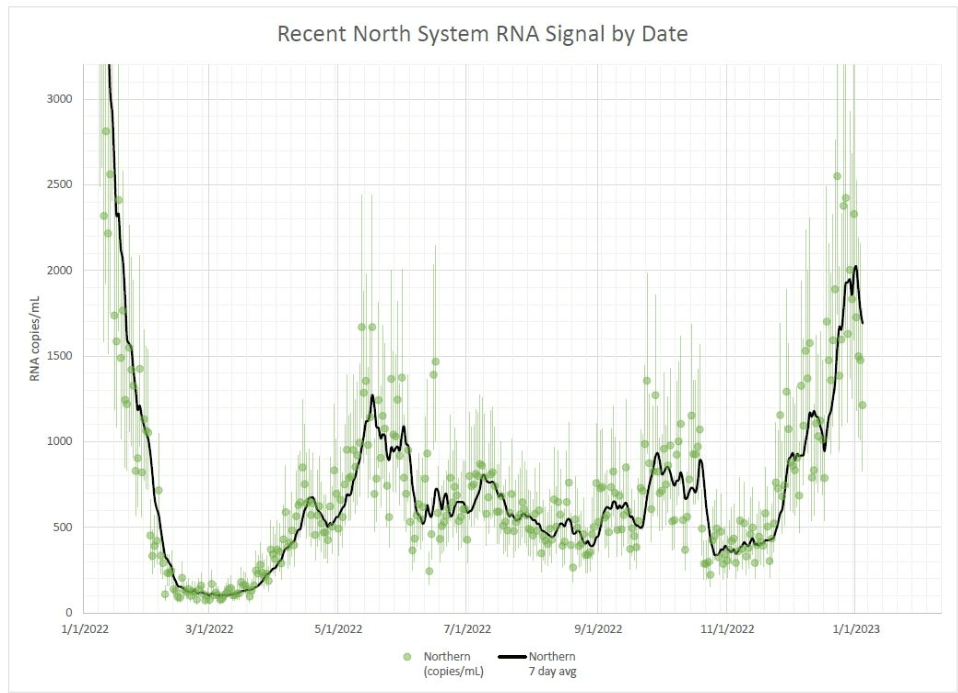
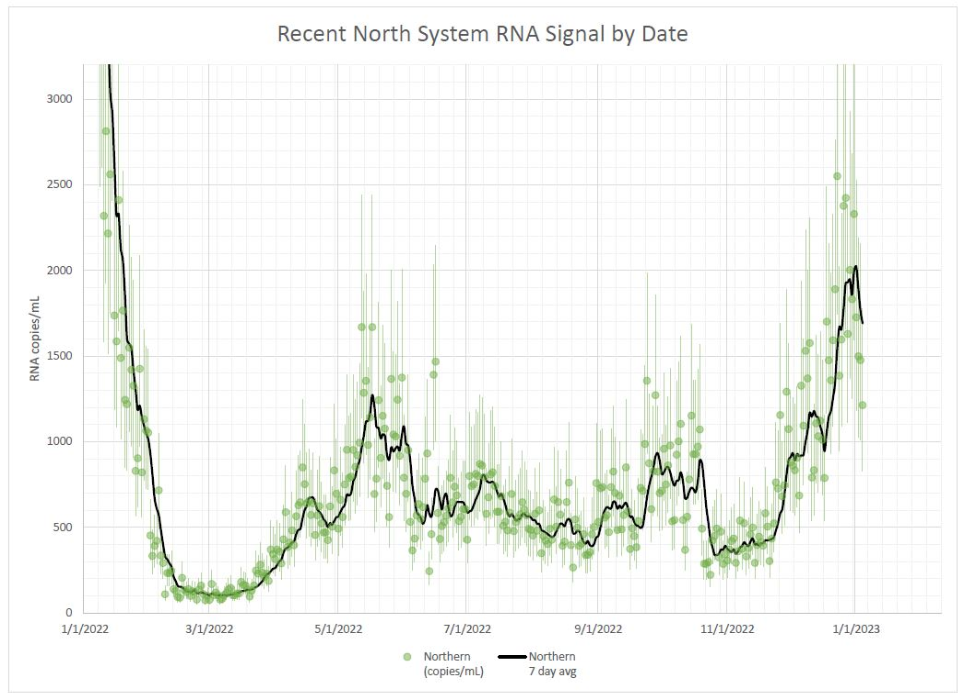
Wastewater surveillance, on the other hand, clearly shows a significant rise in coronavirus spread from early December through early January—building on another rise that followed Thanksgiving. Biobot’s dashboard suggests that the U.S. as a whole is seeing about as much COVID-19 transmission now as we saw at the peak of the summer BA.5 wave. In some places, transmission is the highest it’s been since last January (during the original Omicron surge.)
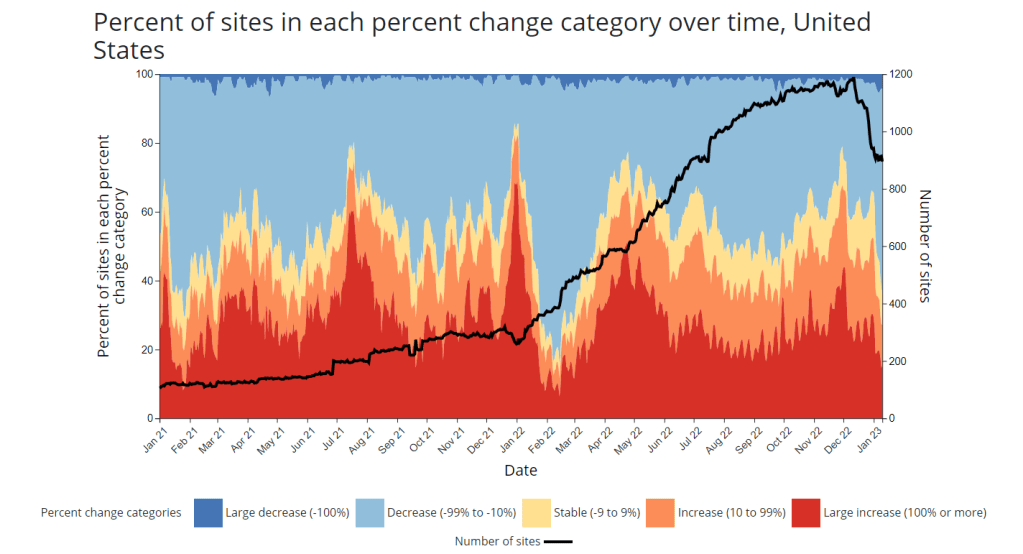
The CDC’s wastewater data similarly show increasing COVID-19: out of 600 sites with available recent data, more than half were reporting upticks in the two-week period ending January 2. 117 of those sites reported an increase between 100% and 999%, and 87 reported an increase over 1,000%.
Regionally, the Northeast has reported the biggest recent COVID-19 spike in wastewater, though the trend may already be turning around. We see this both in Biobot’s regional data and in individual cities and counties, like Boston and New York City. The Northeast is also a hotspot for XBB.1.5, a homegrown Omicron subvariant that’s spreading faster than other lineages. (More on that later in the issue.)
In addition to the wastewater surveillance, hospitalization data have remained uninterrupted by the holidays with clear increases in COVID-19 patients through December and into this week. This week, about 6,600 new COVID-19 patients were admitted to hospitals nationwide, a 16% increase from the prior week and about twice the number of people admitted during the week before Thanksgiving.
Washington D.C., Connecticut, Massachusetts, and West Virginia reported the highest rates of new COVID-19 patients in the week ending January 3, according to the latest Community Profile Report. They were followed by other Northeast states New Jersey, New York, and Delaware. But states reporting the highest increases in hospitalization are in the South: Louisiana, Mississippi, Florida, Texas.
Two pieces of good news for this week: the flu and RSV are both trending down after their surges earlier in the fall. High levels of influenza-like activity remain in the majority of states, though. And we may see a second flu peak driven by a second strain, as Katelyn Jetelina reports in Your Local Epidemiologist.
All the same safety measures we know and love—masks, testing, vaccinations, etc.—continue to help reduce the risk of COVID-19 and other viruses. But uptake of these measures remains low. As of January 5, only 15% of the eligible U.S. population has received an Omicron-specific booster dose, per the CDC.