In the past week (October 8 through 14), the U.S. reported about 270,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 39,000 new cases each day
83 total new cases for every 100,000 Americans
12% fewer new cases than last week (October 1-7)
In the past week, the U.S. also reported about 23,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 3,300 new admissions each day
7.0 total admissions for every 100,000 Americans
4% fewer new admissions than last week
Additionally, the U.S. reported:
2,300 new COVID-19 deaths (330 per day)
12% of new cases are caused by Omicron BA.4.6; 11% by BQ.1 and BQ.1.1; 5% by BF.7; 3% by BA.2.75 and BA.2.75.2 (as of October 15)
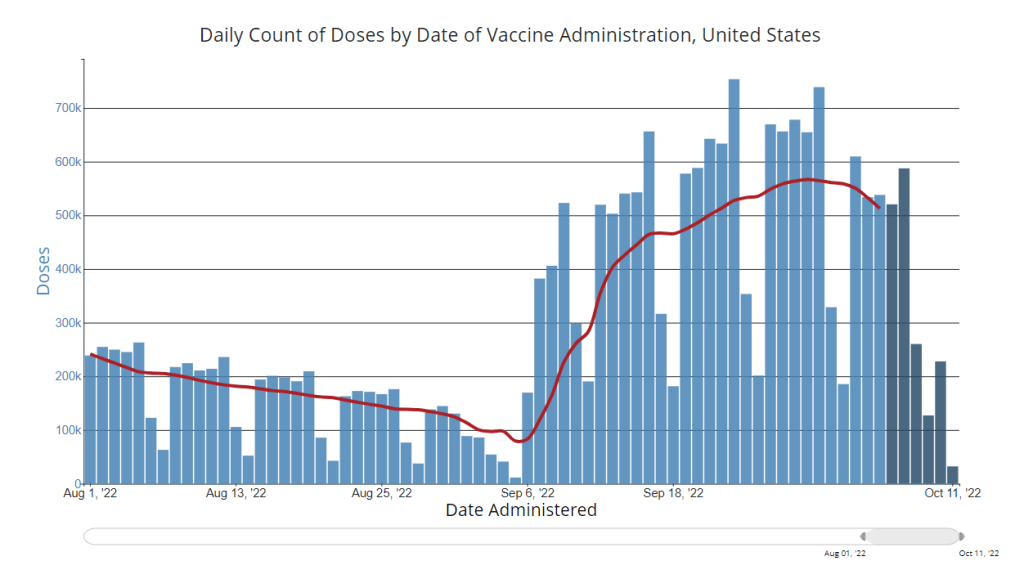
An average of 400,000 vaccinations per day
While official case numbers remain low compared to past fall seasons—both national cases and hospital admissions dropped again this week—signals of a coming fall surge are accumulating from wastewater and local data.
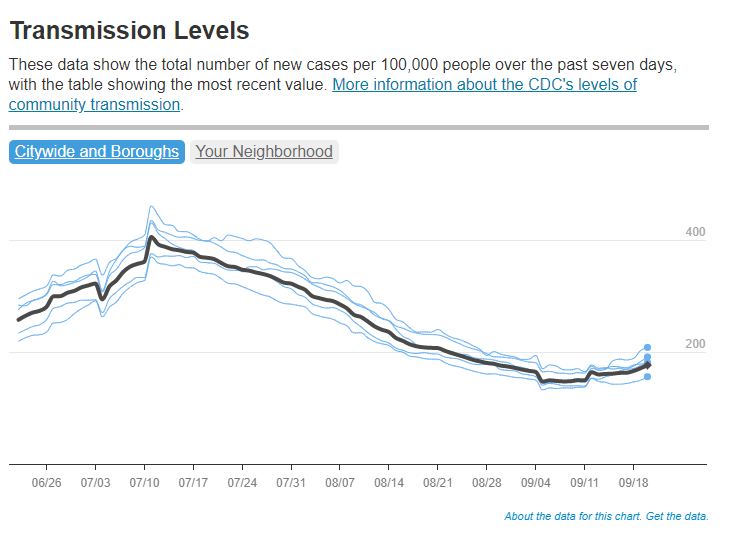
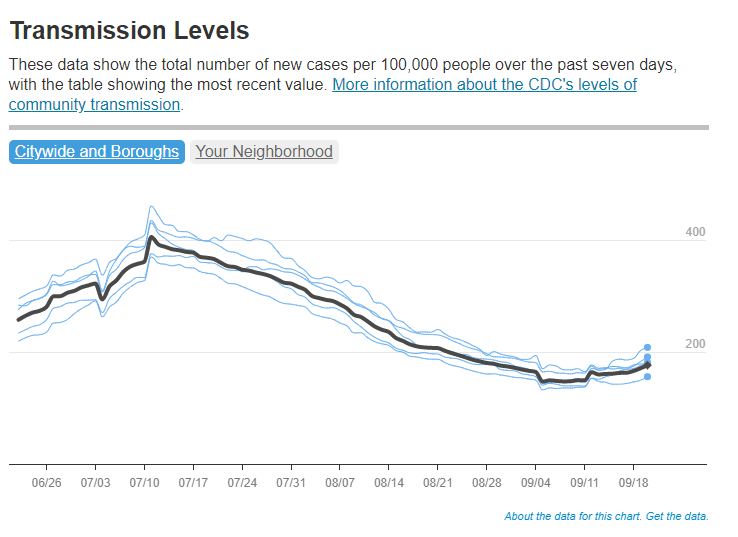
According to Biobot’s dashboard, the coronavirus continues to spread in the Northeast at higher levels than the rest of the country with a new uptick this week. In places like Franklin County, Massachusetts, Fairfield County, Connecticut, and Middlesex County, New Jersey, coronavirus levels are higher now than they have been at any point in the last six months.
Similar patterns are starting to show up in clinical data: Northeast states including Vermont, Maine, Connecticut, New Hampshire, Massachusetts, New York, and New Jersey reported increased COVID-19 patients this past week, according to the October 13 Community Profile Report.
Along with colder weather and behavior patterns, new Omicron lineages could contribute to the increased transmission—if they aren’t contributing already. BQ.1 and BQ.1.1, two sublineages from BA.5, are now causing about 11% of new cases nationwide, according to the CDC’s most recent variant prevalence update. In the northeast, their prevalence is approaching to 20%. (More on the new subvariants in the next post.)
As many of the sublineages now circulating are descended from BA.5 or BA.4, the bivalent booster shots designed to protect against these variants should still help protect against newer strains. In fact, the FDA and CDC recently expanded eligibility for these new shots to younger age groups, going down to kids ages five to eleven.
But uptake of the new boosters remains low—in part because public communication has been so limited, many Americans don’t know they qualify for these shots. Only 15 million people have received the boosters as of October 12, a tiny fraction of the eligible population.
Drew Armstrong, senior health care editor and leader of the tracking effort, provided the motivations for this decision in an update post. New rounds of booster shots around the world, including bivalent shots in some countries, have made it harder to track and present data: “There are more categories of data to collect and fewer simple comparisons among the more than 100 countries we’ve been tracking,” Armstrong wrote.
Armstrong also explained that the vaccine tracker has been a huge lift for Bloomberg, and the company is only able to put so many resources into a dashboard that really should be provided by government or academic institutions. (The COVID Tracking Project’s leaders said something similar when that project stopped data collection in spring 2021.)
While I’m sad to see this tracker go, I understand the decision and remain very grateful for all the work that’s gone into it since vaccination campaigns started in winter 2020. Congratulations to all of the Bloomberg journalists who contributed to this valuable resource!
New, Omicron-specific booster shots are publicly available for all American adults who’ve been previously vaccinated. This is the first time our shots actually match the dominant coronavirus variant (BA.5), and possibly the last time that the shots will be covered for free by the federal government.
So… why does it feel like almost nobody knows about them? Since the CDC and FDA authorized these shots, I’ve had multiple conversations with friends and acquaintances who had no idea they were eligible for a new booster. My own booster happened in a small, cramped room of a public hospital—a far cry from the mass vaccination sites that New York City has offered in past campaigns.
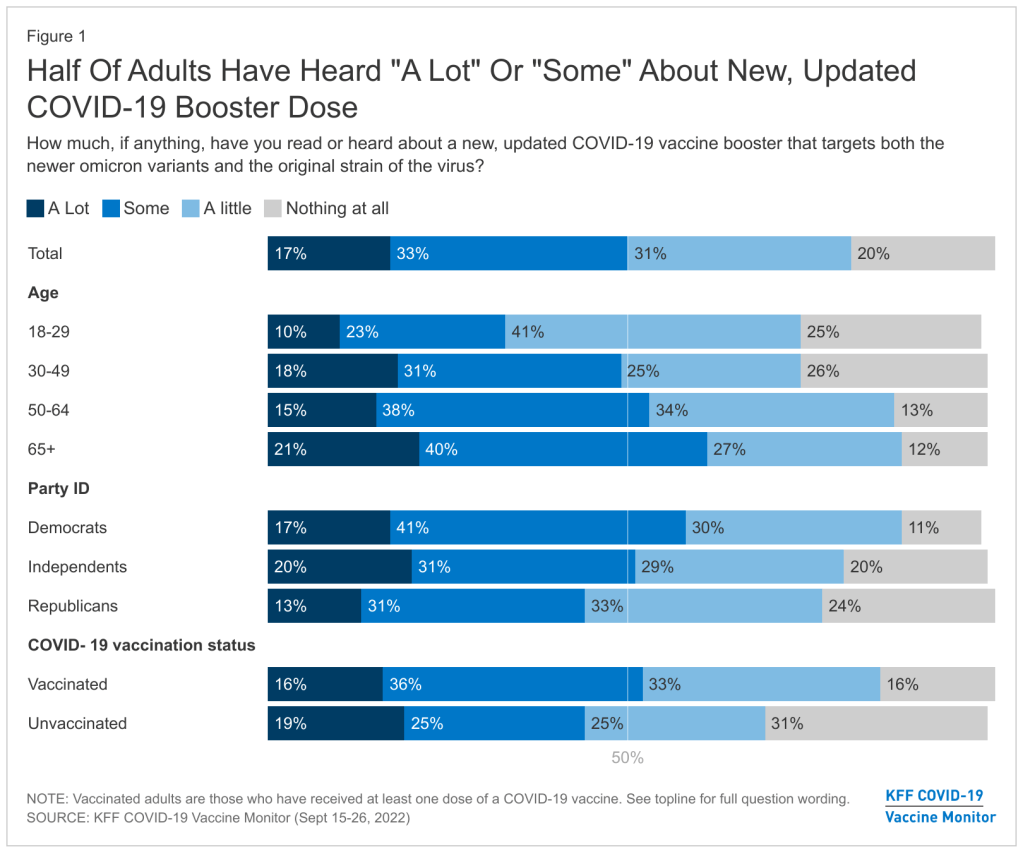
This week, the Kaiser Family Foundation (KFF) provided some data to back up such anecdotal evidence. According to the September iteration of KFF’s Vaccine Monitor survey, about half of U.S. adults have heard only “a little” or “nothing at all” about the new boosters. That includes more than half of adults who have been previously vaccinated.
Moreover, the KFF survey found that 40% of previously vaccinated adults (who received the full primary series) are “not sure” if the updated booster is recommended for them. Another 11% said the new booster is not recommended for them—which is not true! The CDC has recommended these boosters for everyone who previously got vaccinated.
Booster eligibility knowledge is even lower in certain demographics, KFF found. That includes: 55% of previously vaccinated Black adults and 57% of Hispanic adults don’t know that they’re eligible for boosters. Same thing for 57% of vaccinated adults with less than a college education and 58% of those living in rural areas.
As of September 28, only 7.6 million Americans have received an updated booster shot, the CDC reports.
Overall, the CDC reports that about 7.6 million Americans have received an updated booster shot as of September 28, including 4.9 million who received a Pfizer shot and 2.7 million who received a Moderna shot. This represents less than 4% of all fully vaccinated adults who are eligible for the new boosters. And we don’t have demographic data yet, but I expect the patterns will fall among similar lines to what KFF’s survey found.
“Clear and consistent messaging accompanied by strategies to deliver boosters is needed to narrow these gaps,” said public health expert Anne Sosin, sharing the KFF findings on Twitter. We need big, public campaigns for the new boosters in line with what we got for the original vaccines in 2021—or else the new shots won’t be very helpful in an inevitable fall/winter surge.
In the past week (September 17 through 23), the U.S. reported about 380,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 54,000 new cases each day
116 total new cases for every 100,000 Americans
11% fewer new cases than last week (September 10-16)
In the past week, the U.S. also reported about 28,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 4,000 new admissions each day
8.5 total admissions for every 100,000 Americans
10% fewer new admissions than last week
Additionally, the U.S. reported:
2,400 new COVID-19 deaths (350 per day)
83% of new cases are caused by Omicron BA.5; 12% by BA.4.6; 2% by BF.7; 1% by BA.2.75 (as of September 24)
An average of 300,000 vaccinations per day
Nationally, official COVID-19 case counts continue to decline: reported cases are down about 11% last week compared to the prior week, while new COVID-19 patients in hospitals are down 10%. But signals from wastewater and variants suggest a fall surge may be starting soon.
“Currently, most of the country is reporting moderate to high SARS-CoV-2 levels in wastewater,” CDC officials noted in this Friday’s COVID Data Tracker Weekly Review. For almost 20% of sites, these coronavirus levels are the highest seen since December 2021, the CDC reports. About half the wastewater sites in the CDC’s network are reporting an increase in coronavirus levels and half are reporting a decrease.
Notably, many of the wastewater sites reporting increased coronavirus spread are in the Northeast, a region that’s also a hotspot for Omicron subvariants BA.2.75 and BF.7. BF.7, a new sublineage that evolved from BA.5, is particularly worth watching (more on that below). Overall, the U.S.’s variant composition is slowly shifting from BA.5 to these two subvariants, along with BA.4.6—which caused 12% of new cases nationwide in the week ending September 24.
According to the latest Community Profile Report, states reporting significant increases in cases from week to week include Nevada, California, New Hampshire, Kentucky, Massachusetts, New Jersey, New York, and Oregon. In New York City—often a bellwether for new surges—cases have started to tick up slightly, according to the city’s health department, after a long (and slow) decline from July’s summer peak.
Meanwhile, other common respiratory viruses might make a comeback this fall, report Dr. Katelyn Jetelina and Dr. Caitlin Rivers in a joint issue of their newsletters. Data so far on the flu, RSV, rhinovirus, and other viruses we consider part of a normal fall season suggest that children in the U.S. might have a particularly virus-heavy fall and winter—putting more pressure on the healthcare system.
One of the best ways to protect yourself from COVID-19 this fall is by receiving one of the new, Omicron-specific booster shots. According to the CDC, about 4.4 million Americans have received one so far, as of September 21. The new shots have brought our vaccine administration counts to over 300,000 new doses given a day, but that still pales in comparison to the millions administered daily during the spring 2021 campaign.
I received my own booster on Friday at a NYC Health + Hospitals site. Unlike my primary series doses, for which my girlfriend and I had to wait in long lines with hundreds of other New Yorkers, we got our new shots in a small, hard-to-find room tucked away in a small corner of a south Brooklyn hospital campus. This vaccination campaign seems to be almost an afterthought when it deserves primetime attention.
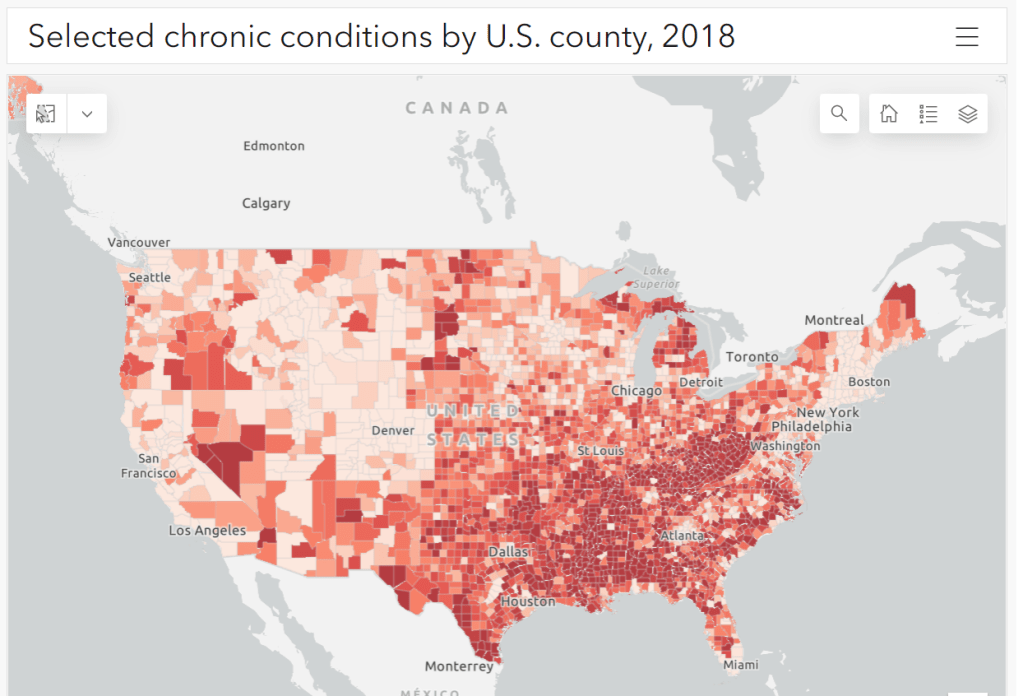
Parts of the South and Midwest have higher rates of chronic conditions (colored darker red on the map) that confer higher risk for severe COVID-19. Chart via the CDC.
The U.S. has started a new booster shot campaign, this time using vaccines designed to specifically target super-contagious subvariants Omicron BA.4 and BA.5. (For more details on the shots themselves, see last week’s post.)
Unlike previous vaccination campaigns, these boosters are available to all adults across the country who have been previously inoculated. There was no prioritization for seniors, healthcare workers, or other higher-risk adults. The official guidance from the federal government is actually pretty straightforward, for once: everyone should get the new booster. And get a flu shot soon, too, possibly even at the same time as your COVID-19 shot.
But all previously-vaccinated Americans are not facing similar levels of COVID-19 risk. Many of the same qualifications that might have warranted you an earlier dose in spring 2021 should now lead you to prioritize your Omicron booster, even if you might have been infected recently. At the same time, people who fall in these groups (or who share their households) have a good reason to continue using other safety measures after their boosters.
Here are the major qualifications for higher risk, with data to back them up:
Seniors, especially those over age 70: More than 90% of Americans over age 65 have received at least their primary vaccine series, according to the CDC, while over 70% have received at least one booster. Yet older Americans continue to have the highest rates of hospitalizations and deaths. For example, those older than 70 have consistently been hospitalized at several times the rate of younger adults (when adjusted for population). The same pattern is true for deaths among adults over age 75. Seniors who receive the new booster shots will face a lower risk of severe COVID-19 this fall and winter.
Black, Indigenous, and other Americans of color, especially seniors: Despite dedicated vaccination campaigns and other health equity efforts, Americans of color have continued to be hit harder by the pandemic than white Americans. Higher rates of chronic conditions in minority populations combined with other socioeconomic factors (POC are more likely to work essential jobs, to lack healthcare, etc.) have led to disproportionately high hospitalization and death rates. And the U.S.’s booster shot campaigns so far have been inequitable, as shown in a recent study by demography experts. Reaching these populations should be a priority for the new Omicron boosters.
Immunocompromised people: National estimates consider about 3% of Americans to be moderately or severely immunocompromised, meaning that their immune systems have limited capacity to respond to infections without medical assistance. This group includes cancer patients, organ transplant recipients, people with autoimmune diseases, and more. (This Yale Medicine article provides more information.) Immunocompromised people might have already had multiple booster shots but are still eligible to receive an Omicron booster as soon as possible, the CDC recommends.
People with Long COVID and related conditions: While there isn’t as much established data in this area, I have seen a lot of anecdotal reports from Long COVID patients who work hard to avoid new coronavirus infections—concerned about reinfection’s possibility to worsen their symptoms. On the flip side, vaccination might lead to improvement in Long COVID patients, as the shot boosts a patient’s immune system in responding to lingering reservoirs of virus. The Atlantic covered this possibility when Long COVID patients were first eligible for vaccination in early 2021, and other studies since then have backed it up. More research is needed, but at the very least, Long COVID patients receiving a new booster will have lower risk of a new severe case.
People with other preexisting health conditions: The CDC has an extensive list of medical conditions that can confer additional risk for severe COVID-19, with plenty of links to other CDC pages and medical sites where you can learn more about relevant evidence. I won’t go through them all here (that’s a topic for another week’s issue), but I do recommend checking out the CDC’s information and linked sources if you have a condition on the list. You can also explore this map of chronic condition rates by county.
This week, the FDA and CDC authorized new booster shots from both Pfizer and Moderna that are tweaked to specifically target Omicron BA.4 and BA.5. The vaccines will start becoming available at pharmacies and doctors’ offices across the country in the coming days.
Much of the media coverage of these new boosters has focused on the fact that they’re the first COVID-19 vaccines derived from a newer variant, as opposed to the original Wuhan strain. BA.5 and BA.4.6, a sublineage of BA.4, are causing almost all COVID-19 cases in the country right now; some experts hope that a booster campaign targeted to these versions of the coronavirus will lead to actual decreases in transmission, not just severe disease.
While this is an important milestone, I’d like to focus on a couple of reasons these shots are notable from a data perspective. First, the Omicron boosters are the first COVID-19 vaccines authorized in the U.S. without data from human trials. During vaccine development, companies typically start with lab studies, then test the vaccine in animal models, then in humans. Because the BA.4/BA.5 shots were designed so recently, Pfizer and Moderna haven’t had time to test them in humans yet.
From a safety and efficacy perspective, this lack of data isn’t a huge concern because the new vaccines are very close to BA.1 versions that have been tested in humans. As Katelyn Jetelina explained in a Your Local Epidemiologist post about the new vaccines:
Literally the difference of a few amino acids—like a few letter edits on a Word document. We aren’t changing the number of words in the paper (like dosage of RNA), or the content of the paper, or the platform (like Word to Excel). Because of the minimal change, we are confident that BA.1 bivalent safety data will accurately reflect BA.5 safety.
Another important piece of context here is that flu vaccines—which are updated each year to reflect currently circulating versions of the virus—are typically not tested in humans before they’re rolled out in annual flu campaigns. So, the new COVID-19 shots are following an existing process; future vaccine adjustments for new variants going forward will likely happen in a similar way.
Second, the Omicron boosters are the first COVID-19 vaccines authorized in the U.S. before they’ve been tested in other countries. For previous booster campaigns, effectiveness data from countries with better-organized health systems that started using new rounds of shots before we did (such as the U.K. and Israel) have been key for U.S. regulators making authorization decisions.
But the BA.4/BA.5 boosters haven’t been rolled out anywhere else yet. Several other countries (the E.U., the U.K., Canada, Switzerland, Australia) have authorized Omicron BA.1 boosters—those that have gone through more clinical testing. The U.S. is the first to try the BA.4/BA.5 option. It will be interesting to see whether there are significant differences in how these countries’ fall booster campaigns mitigate potential surges.
And third, these boosters are likely to be the last COVID-19 vaccines authorized while they’re still covered by federal funding.Recent announcements from officials like Ashish Jha have suggested that, in 2023, the government will stop buying vaccine supplies in large quantities to distribute for free. Instead, COVID-19 vaccines will start to be privately-purchased, health insurance-mediated products like other vaccines.
While some local governments and large health institutions will likely still organize free vaccine distributions for future rounds of shots, the lack of federal supplies will be a major shift. It will make COVID-19 vaccination harder to access, especially among people without health insurance—likely leading to even lower uptake. We need to make this last free booster campaign count.
Going forward, here are a few questions I’ll be tracking as these boosters get rolled out:
How will public health agencies track the effectiveness of these new vaccines? We’ll want to see how the BA.4/BA.5 shots compare to prior boosters at preventing infections, hospitalizations, and deaths. Data on breakthrough cases is already pretty limited in the U.S., so we may have to rely on specific local health departments and health systems that have better infrastructure for this.
What additional boosters might be needed in the future? As we examine how well these Omicron-specific boosters work, we will need to keep track of the potential need for more shots. Will immunocompromised people or older adults need second rounds of Omicron shots, for example?
What new variants will come on the scene? Also impacting the potential need for further vaccine shots: the arrival of new variants, either continued Omicron mutations or something else entirely. Wastewater surveillance may be particularly helpful for variant tracking as PCR testing continues to be less available.
How will the privatization of vaccines impact tracking? If COVID-19 vaccines are no longer purchased and distributed by the federal government after 2022, will this impact the CDC’s ability to track vaccinations? We’re already seeing more vaccine distribution at private pharmacies and doctors’ offices as opposed to publicly-run clinics; I wonder how this trend may continue.
For more information on the new boosters, check out:
KFF poll shows low vaccine uptake for young kids: This week, the Kaiser Family Foundation released an update from their COVID-19 Vaccine Monitor, an ongoing project tracking U.S. attitudes towards vaccines. This latest update focuses on children under age five, and the results are worrying: about 43% of parents with kids in this age group say they will “definitely not” get their child vaccinated, citing concerns about vaccine safety. Conservative parents and those who are unvaccinated themselves were particularly likely to be against vaccinating their young kids, KFF found.
Vaccine side effects less common for second boosters: A new CDC study, published in this week’s Morbidity and Mortality Weekly Report, tracked reactions to COVID-19 boosters among Americans over age 50 using CDC monitoring systems. Among over 200,000 people who received third and fourth doses from the same vaccine manufacturer, side effects like a sore arm and fatigue were less common after the fourth dose compared to the third dose. Still, uptake for second boosters has been slow and potentially inequitable; the CDC recently published data on second boosters by race/ethnicity, showing that white Americans over age 50 are more likely to get this extra protection than non-white people in this age group.
White House summit on next-generation COVID-19 vaccines: And one more piece of vaccine news for this week: the White House brought together federal officials, scientists, and pharmaceutical executives for a summit discussing next-generation COVID-19 vaccines. The summit highlighted vaccine candidates designed to work against many potential coronavirus variants, as well as those that would be delivered through the nose—potentially producing more protection against coronavirus infection and transmission. Either option would require a lot of funding from a Congress that has been hesitant to support COVID-19 efforts.
States are letting health emergency declarations expire: While the federal declaration of COVID-19 as a public health emergency will remain in place at least through this fall, many states have let their declarations expire in recent months. These expirations impact the resources states are able to allocate for tracking and responding to COVID-19—ranging from data collection to telehealth access. The ending emergencies are certainly contributing to less frequent COVID-19 data updates in many states.
New studies on COVID-19’s origins: Two major studies have conclusively linked the coronavirus’ early spread to the Huanan Seafood Market in Wuhan, China. These studies, both published in Science, were produced by an international group of virologists and evolutionary biologists at the Scripps Research Institute, the University of Arizona, the University of Sydney, the University of Edinburgh, and many other institutions. The experts traced early cases in the seafood market, finding evidence of spillover from animals to humans. The precise origins of COVID-19 are still unknown, but these studies go a long way in demonstrating early spread tied to animals, not a lab leak.
This week, the FDA’s vaccine advisory committee met to discuss fall booster shots, in anticipation of another COVID-19 surge next winter. The discussion demonstrated the U.S.’s continued failure to provide the data that are really needed to make these decisions.
I have written a lot about this topic in the past, so to avoid being too repetitive, I’ll link to a couple of past articles:
But here’s the TL;DR: due to the fractured nature of America’s public health system, it’s difficult for researchers to connect data on different health metrics. For example, a state might have one database with vaccination records and another database with case records, and the databases might not easily link to answer questions about breakthrough cases.
Some state health departments have figured out how to make these links, but the process is not uniform. And the breakthrough case data we do have generally aren’t linked to information on variants, or demographic data, or outcomes like Long COVID.
The more specific the vaccine effectiveness question, the more complicated it becomes to answer. This is a bigger problem now as the FDA considers fall boosters, because the agency needs to determine the best vaccine candidate and identify priority populations for shots—while operating in a politcal climate where vaccine funding is less popular than it was a year ago.
Should the fall booster be a monovalent vaccine, meaning it only includes Omicron-specific genetic material? Or should it be bivalent, meaning it includes both Omicron and the original, Wuhan strain? Pfizer and Moderna presented different options; some experts say a bivalent vaccine may provide more long-term protection.
Should the booster shot be specific to BA.4 and BA.5? The panel agreed that it should, as these strains are now dominant in the U.S., but there’s a timing trade-off as vaccine companies have yet to do clinical trials (or provide substantial data) for a subvariant-specific vaccine.
Should the booster shot be another type of vaccine entirely? In addition to Pfizer and Moderna, the FDA panel also heard from Novavax. This company has developed a protein-based vaccine that hasn’t yet received FDA authorization, but panelists were impressed by its potential for long-term protection.
How well do the vaccines provide non-antibody-based protection? As in past advisory committee meetings, the vaccine companies primarily presented data based on antibodies generated from their shots. Experts wanted to see more data about T cells and other aspects of immunity which are harder to measure, but may be more important in the long term.
Who would most benefit from another booster? If the federal government isn’t able to buy enough shots for everyone, priortization will need to happen. Will Omicron-specific boosters be most useful for seniors, or for people with certain health conditions? These groups will likely get priority again, though we could still be collecting more data on how the vaccines fare for them.
Of course, despite the dearth of data and cautions from some members of the FDA advisory committee, the U.S. government seems to be going full-speed ahead with fall boosters. The Biden administration has placed a $3.2 billion order from Pfizer for 105 million doses of whichever Omicron-specific vaccine the FDA chooses to authorize.
CDC adds second boosters to its vaccine dashboard: In the latest update to the CDC’s COVID Data Tracker, you can now find a national tally of Americans who have received second booster shots on the “COVID-19 Vaccinations in the United States” page. About 10 million people have received these additional shots as May 6, about one-tenth the number of first booster recipients. The CDC has yet to add state-by-state or demographic data for second boosters.
KFF updates COVID-19 Vaccine Monitor: This week, the Kaiser Family Foundation published the latest update of its Vaccine Monitor, a long-running project tracking Americans’ attitudes towards COVID-19 vaccines and related issues. One notable finding from the April update: just 18% of parents with children under age five are “eager to get their child vaccinated right away,” compared to 27% who say they will “definitely not” get their child vaccinated. This report also includes survey findings on mask-wearing, COVID-19 in the workplace and in schools, and future booster shots.
Biobot on GitHub: I recently learned that Biobot Analytics, the leading COVID-19 wastewater surveillance company, publishes its underlying data on GitHub. This repository includes coronavirus concentrations in wastewater treatment plants monitored by Biobot across the country, along with regional wastewater data, national data, and COVID-19 case numbers for comparison.
TON’s Guide to Tracking Source Diversity: Not directly COVID-related, but a resource that I thought readers may find useful: The Open Notebook (TON) has published a detailed guide for journalists seeking to track the diversity of sources interviewed for their stories. While TON is geared towards science writers, this guide is broadly applicable to any reporter who spends a lot of time seeking out and talking to experts.
Last fall, I wrote—both in the COVID-19 Data Dispatchand for FiveThirtyEight—that the U.S. did not have the data we needed to make informed decisions about booster shots. Several months later, we still don’t have the data we need, as questions about a potential BA.2 wave and other future variants abound. Discussions at a recent FDA advisory committee meeting made these data gaps clear.
Our country has a fractured public health system: every state health department has its own data systems for COVID-19 cases, vaccinations, and other metrics, and these data systems are often very difficult to link up with each other. This can make it difficult to answer questions about vaccine effectiveness, especially when you want to get specific about different age groups, preexisting conditions, or variants.
To quote from my November FiveThirtyEight story:
In the U.S., vaccine research is far more complicated. Rather than one singular, standardized system housing health care data, 50 different states have their own systems, along with hundreds of local health departments and thousands of hospitals. “In the U.S., everything is incredibly fragmented,” said Zoë McLaren, a health economist at the University of Maryland Baltimore County. “And so you get a very fragmented view of what’s going on in the country.”
For example, a database on who’s tested positive in a particular city might not be connected to a database that would reveal which of those patients was vaccinated. And that database, in turn, is probably not connected to health records showing which patients have a history of diabetes, heart disease or other conditions that make people more vulnerable to COVID-19.
Each database has its own data fields and definitions, making it difficult for researchers to integrate records from different sources. Even basic demographics such as age, sex, race and ethnicity may be logged differently from one database to the next, or they may simply be missing. The Centers for Disease Control and Prevention, for instance, is missing race and ethnicity information for 35 percent of COVID-19 cases as of Nov. 7.*
*As of April 9, the CDC is still missing race and ethnicity information for 35% of COVID-19 cases.
This past Wednesday, the FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) met to discuss the future of COVID-19 booster shots. Notably, this committee didn’t actually need to vote on anything, since the FDA and CDC had already authorized a second round of boosters for Americans over age 50 and immunocompromised people the week before.
When asked why the FDA hadn’t waited to hear from its advisory committee before making this authorization decision, vaccine regulator Peter Marks said that the agency had relied on data from the U.K. and Israel to demonstrate the need for more boosters—combined with concerns about a potential BA.2 wave. The FDA relied on data from the U.K. and Israel when making its booster decision in the fall, too; these countries, with centralized health systems and better-organized data, are much more equipped to track vaccine effectiveness than we are.
With that authorization of second boosters for certain groups already a done deal, the VRBPAC meeting this past Wednesday focused more on the information we need to make future booster decisions. Should we expect annual COVID-19 shots, like we do for the flu? What about shots that are designed to combat specific variants? A lot of this is up in the air right now, the meeting discussion indicated.
Also up in the air: will the FDA ever host a virtual VRBPAC meeting without intensive technical difficulties? The meeting had to pause for more than half an hour to sort out a livestream issue.
we can pull together extraordinary vaccines in under a year we can cook up oral antivirals that slash hospitalization and death rates by 90% we can manufacture great masks, and detect viral infections with 15-minute tests
we cannot get VRBPAC livestreams to work
— Katherine J. Wu, Ph.D. (@KatherineJWu) April 6, 2022
Here are some vaccine data questions that came up on Wednesday, drawing from my own notes on the meeting and the STAT News liveblog:
How much does protection from a booster shot wane over time? We know that booster shots increase an individual’s protection from a coronavirus infection, symptoms, hospitalization, and other severe outcomes; CDC data presented during the VRBPAC meeting showed that, during the Omicron surge, Americans who were boosted were much more protected than those with fewer doses. But we don’t have a great sense of how long these different types of protection last.
How much does booster shot protection wane for different age groups? Waning immunity has been a bigger problem among seniors and immunocompromised people, leading to the FDA’s decision on fourth doses for these groups. But what about other age groups? What about people with other conditions that make them vulnerable to COVID-19, like diabetes or kidney disease? This is less clear.
To what degree is waning immunity caused by new variants as opposed to fewer antibodies over time? This has been a big question during the Delta and Omicron surges, and it can be hard to answer because of all the confounding variables involved. In the U.S., it’s difficult to link up vaccine data and case data; tacking on metrics like which variant someone was infected with or how long ago they were vaccinated often isn’t possible—or if it is possible, it’s very complicated. (The U.K. does a better job of this.)
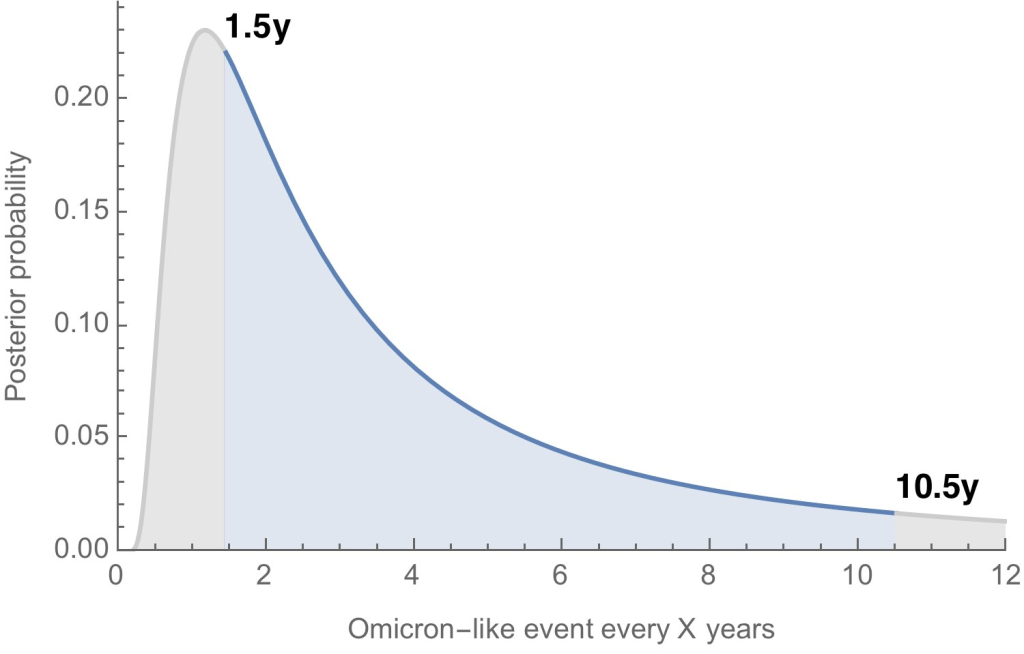
Where will the next variant of concern come from, and how much will it differ from past variants? Computational biologist Trevor Bedford gave a presentation to VRBPAC that attempted to answer this question. The short answer is, it’s hard to predict how often we’ll see new events like Omicron’s emergence, in which a new variant comes in that is extremely different from the variants that preceded it. Bedford’s analysis suggests that we could see “Omicron-like” events anywhere from every 1.5 years to every 10.5 years, and we should be prepared for anything on that spectrum. The coronavirus has evolved quite quickly in the last two years, Bedford said, and will likely continue to do so; though he expects some version of Omicron will be the main variant we’re dealing with for a while.
What will the seasonality of COVID-19 be? The global public health system has a well-established process for developing new flu vaccines, based on monitoring circulating flu strains in the lead-up to flu seasons in different parts of the world. Eventually, we will likely get to a similar place with COVID-19 (if annual vaccines become necessary! also an open question at the moment). But right now, the waxing and waning of surges caused by new variants and human behavior makes it difficult to identify the actual seasonality of COVID-19.
At what point do we say the vaccine isn’t working well enough? This question was asked by VRBPAC committee member Cody Meissner of Tufts University, during the discussion portion of the meeting. So far, the most common way to measure COVID-19 vaccine effectiveness in the lab is by testing antibodies generated by a vaccine against different forms of the coronavirus. But these studies don’t account for other parts of the immune system, like T cells, that garner more long-term protection than antibodies. We need a unified method for measuring vaccine effectiveness that takes different parts of the immune system into account, along with real-world data.
How might vaccine safety change over time? This question was brought up by Hayley Ganz of Stanford, another VRBPAC committee member. The CDC does have an extensive system for monitoring vaccine safety; data from that system should be readily available to the experts making booster shot decisions.
Today, I presented to @US_FDA VRBPAC with an overview of SARS-CoV-2 evolution up to this point and a brief perspective for what to expect going forward. Slides are here: https://t.co/QnzOctVCSN and my slot in the full recording is viewable here: https://t.co/n5rlgOvtEg. 1/13
Another thing I’m wondering about right now, personally, is how the U.S.’s shifting focus away from case data might make all of this more complicated. As public health agencies scale down case investigations and contact tracing—and more people test positive on at-home, rapid tests that are never reported to these agencies—we’re losing track of how many Americans are actually getting COVID-19. And breakthrough cases, which are more likely to be mild or asymptomatic, might also be more likely to go unreported.
So, how does the U.S. public health system study vaccine effectiveness in a comprehensive way if we simply aren’t logging many of our cases? Programs such as randomized surveillance testing and cohort studies might help, but outside of a few articles and Twitter conversations, I’m not seeing much discussion of these solutions.
Finally: a few friends and relatives over age 50 have asked me about when (or whether) to get another booster shot, given all of the uncertainties I laid out above. If you’re in the same position, here are a couple of resources that might help: