This is the last week of Pride Month for 2021, and it’s also officially Pride weekend in NYC, where I live. (As the newsletter goes out, I’ll likely be marching with the Stonewall Protests, a group that advocates for Black trans women.)
So, it felt appropriate for me to take this issue to highlight a couple of lessons that the U.S. response to COVID-19 has taken from our response to another pandemic—one that is still ongoing.
HIV, the virus that causes AIDS, infects over one million new people every year. The HHS estimates that there were about 38 million people living with this virus around the world in 2020, including 1.2 million in the U.S. While many of us might associate HIV/AIDS with American outbreaks in the 1980s and 90s, it continues to disproportionately impact people of color and queer people in the U.S. and globally.
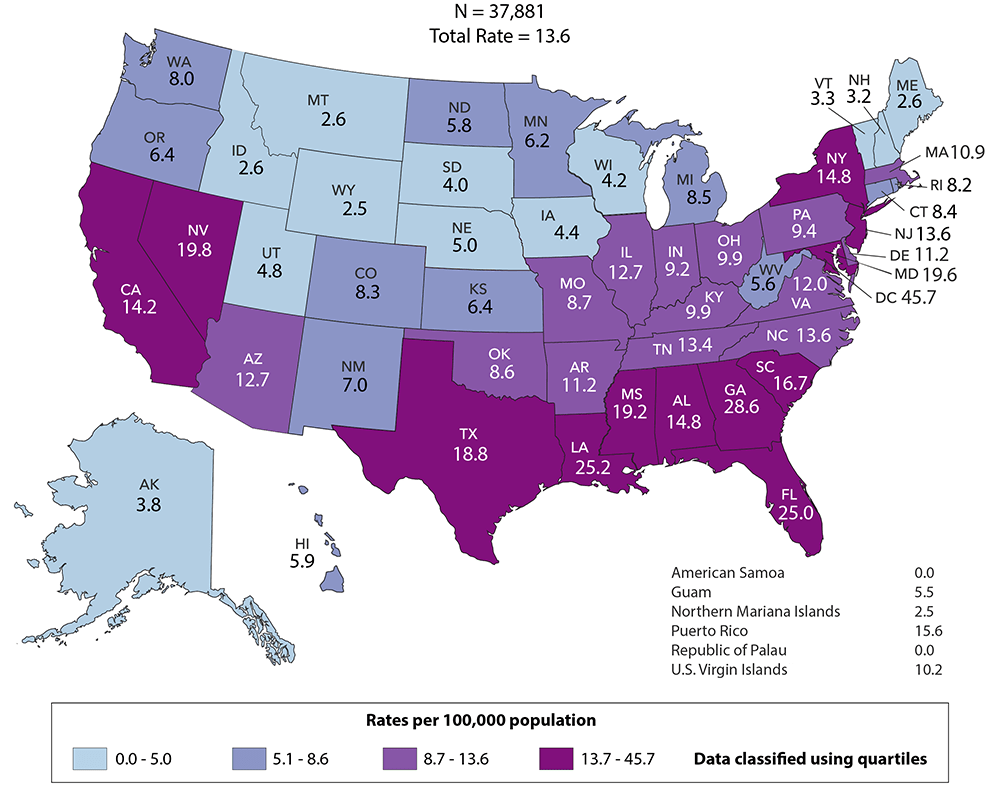
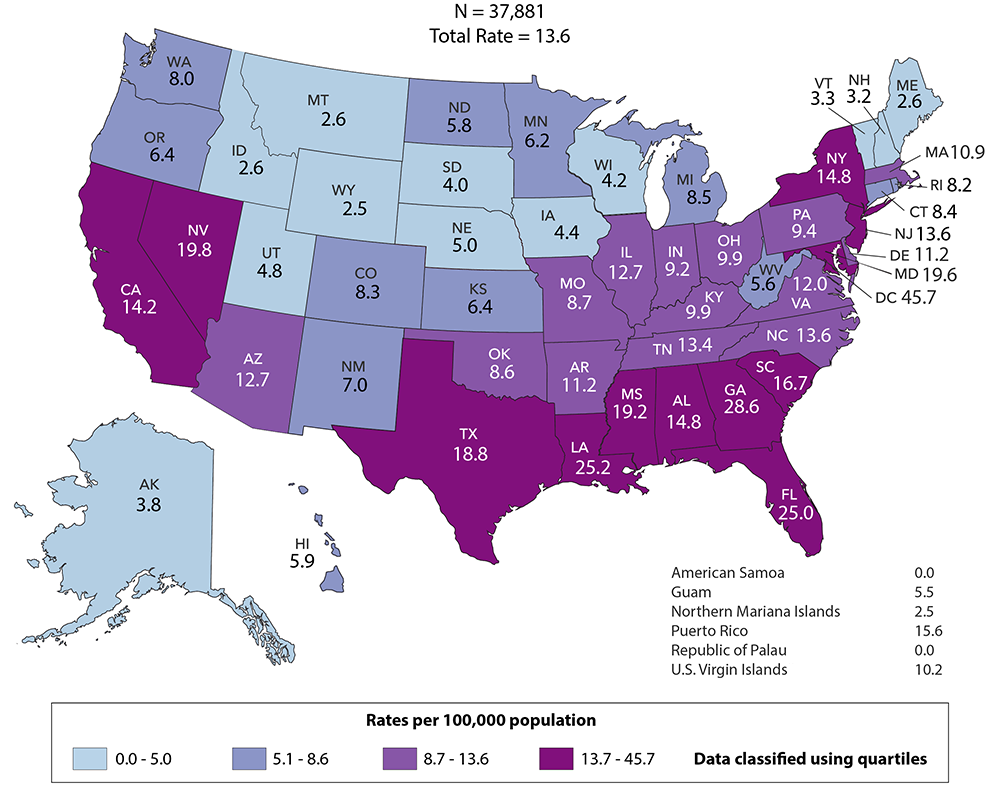
In the U.S., the South has higher HIV infection rates than any other part of the country. Black Americans are diagnosed with the virus at rates almost ten times higher than white Americans, according to CDC data from 2014 to 2018. At a global scale, the virus disproportionately impacts African nations; Swaziland has the highest infection rate, at 27%.
Treatments do exist for HIV, a virus that attacks the body’s immune system, and AIDS, the immunodeficiency condition that this virus causes. The most common treatment is antiretroviral therapy (or ART), which allows people with HIV infections to live long, healthy lives and avoid transmitting the virus to sexual partners. The HHS estimates that about 16% of the global population with HIV (or about 6 million people) does not know they’re infected, and still needs access to tests and treatment.
This is a pandemic that demands continued focus even after urgency around COVID-19 wanes. But the responses to HIV/AIDS—both scientific and political—can show us how an understanding of intersectionality and local community focus may contribute to pandemic response.
Understanding disparities and comorbidities
People living with HIV are more vulnerable to severe COVID-19. One study of HIV patients in New York state found that, if diagnosed with COVID-19, these patients were more likely to go to the hospital and more likely to die from the disease compared to non-HIV patients.
An HIV diagnosis, like a case of diabetes or asthma, is a disease that hits people of color harder and may contribute to their worse COVID-19 rates. Public health efforts around COVID-19 can learn from clinicians focused on HIV/AIDS, who are already used to connecting with vulnerable communities and understanding the intersectional socioeconomic factors that contribute to their health.
It takes a long time to learn disease origins
This page on the evolution of HIV may give you an idea of the many steps that typically go into finding a disease’s source. When the page was first written, in 2008, scientists had found ties between the virus and chimpanzees in west-central Africa, but they didn’t know all the details of its first jump to humans. News updates in 2010, 2015, and 2020 provide more information, reflecting updates in scientific knowledge: newer research suggests that the virus spread to humans in the early 20th century and went undetected for decades.
These updates remind us that scientists cannot pinpoint biological disease origins overnight. Scientists are still working to understand the evolution of HIV, decades after we first became aware of the disease. There are other outbreaks, not as old as HIV but older than COVID-19, that we still don’t understand:
Regulatory pathways need to prioritize patients
In the 1980s, AIDS activists led by the AIDS Coalition to Unleash Power (or ACTUP) protested the FDA and other public health officials. They saw the agency’s drug approval process as a barrier, keeping them from accessing potentially life-saving treatments; while small numbers of patients received new drugs in clinical trials, the vast majority of HIV-positive Americans had to wait for data to come out. Even Dr. Anthony Fauci was involved: AIDS activist Larry Kramer called him a killer and an idiot in a 1988 letter. Fauci later credited Kramer with pushing for change in the medical establishment.
As a result, we can thank those AIDS activists who advocated for processes that allow faster drug development and patient treatment in times of crisis. This includes faster vaccine trials and the hundreds of Emergency Use Authorizations provided to COVID-19 tests and treatments over the past year.
Neighborhood-level healthcare provides critical services
People living with HIV in the U.S. often were not able to access support from the government or healthcare insurance, especially earlier in the 1980s. As a result, many queer communities organized locally to provide their own support. Neighborhoods like the Castro district in San Francisco and Greenwich Village in New York saw healthcare clinics, free testing, information-sharing about virus prevention, and more. These local institutions built trust in their communities.
Such trust was also key in the COVID-19 pandemic, when government agencies from the federal to the county level weren’t ready to serve their residents. In an article for The Conversation, Daniel Baldwin Hess and Alex Bitterman describe how some of the same community groups that started to provide HIV testing decades ago added COVID-19 testing to their repertoire this year:
For example, in New York, the Erie County Department of Health requested that Evergreen Health – an LGBTQ community group originally established in the 1980s as a volunteer effort to fight HIV – assume responsibility for HIV testing during the COVID-19 pandemic so that the county government could focus on COVID-19 testing. Evergreen also opened a drive-though COVID-19 testing center in the spring of 2020 – four decades after it had introduced HIV testing to the Buffalo region.
These local institutions have also helped build vaccine trust and administer doses.
Finally, there’s one lesson we may take from COVID-19 back to the continued fight against HIV/AIDS: mRNA vaccines! Moderna is currently partnering with International AIDS Vaccine Initiative to develop a potential mRNA vaccine for HIV.

Leave a comment