In the past week (January 26 through February 1), the U.S. officially reported about 280,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 40,000 new cases each day
86 total new cases for every 100,000 Americans
7% fewer new cases than last week (January 19-25)
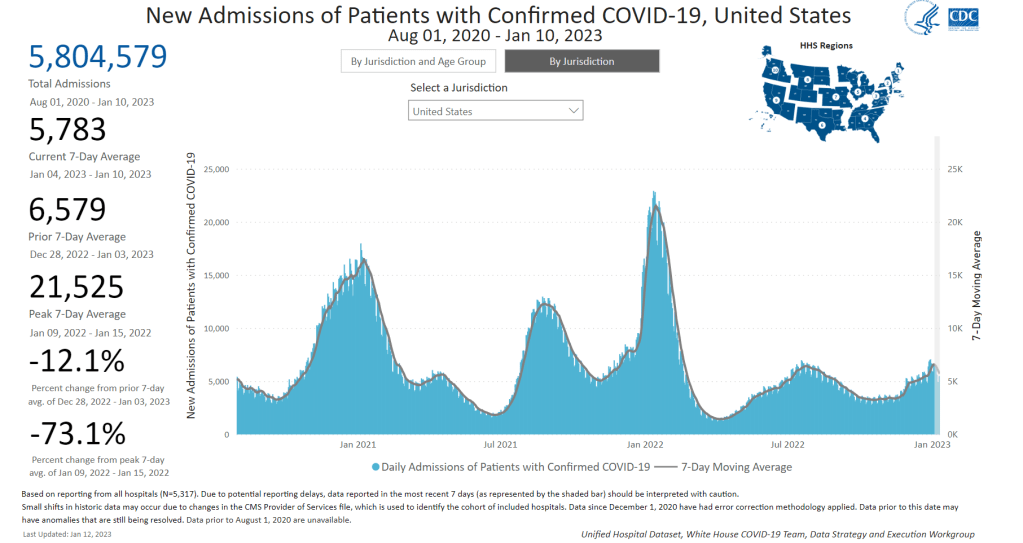
In the past week, the U.S. also reported about 27,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 3,900 new admissions each day
8.4 total admissions for every 100,000 Americans
8% fewer new admissions than last week
Additionally, the U.S. reported:
3,500 new COVID-19 deaths (500 per day)
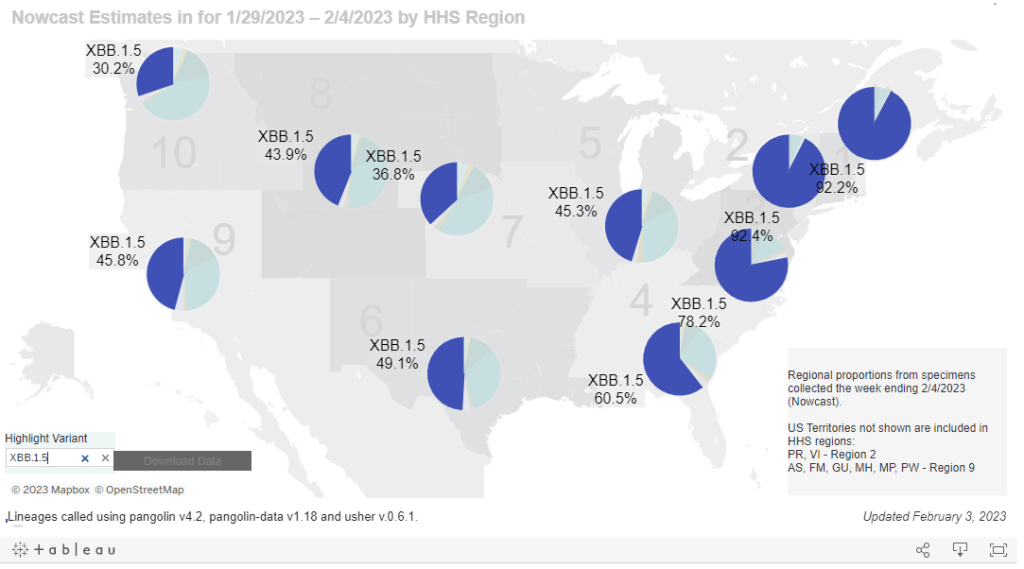
66% of new cases are caused by Omicron XBB.1.5; 27% by BQ.1 and BQ.1.1; 2% by CH.1.1 (as of February 4)
An average of 100,000 vaccinations per day
COVID-19 spread in the U.S. continues to decline—but the decline continues to get slower, following the trend that I wrote about last week. Official COVID-19 cases, hospital admissions, and wastewater surveillance all indicate decreased transmission, leading into potential plateaus.
New hospital admissions for COVID-19, for example, decreased by 8% this week (ending February 1) compared to the prior week (ending January 25). This is a smaller decrease than the prior two weeks, when admissions went down by 13% and 18%. Overall, new hospitalizations are at a similar level to what the U.S. faced in early summer 2022, as BA.5 started spreading across the country.
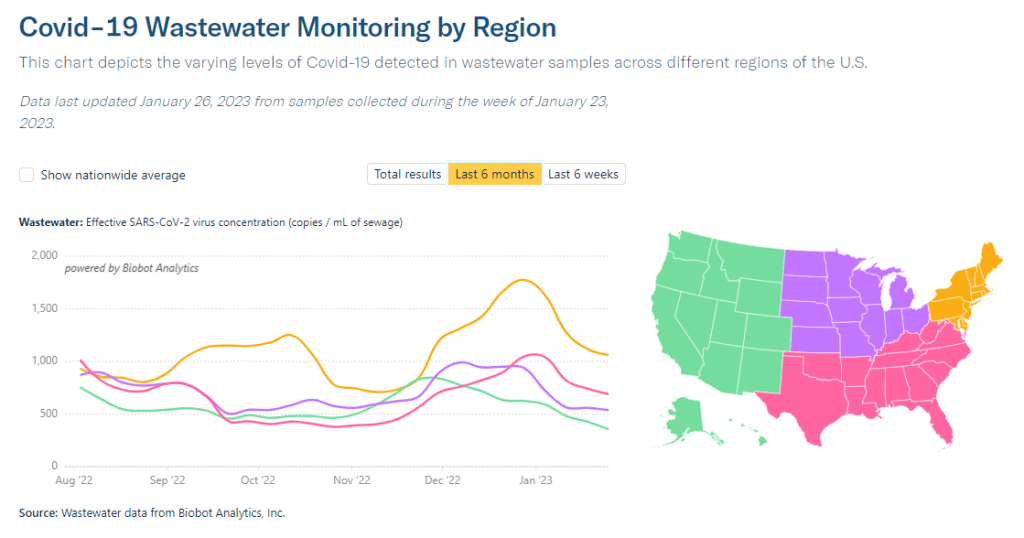
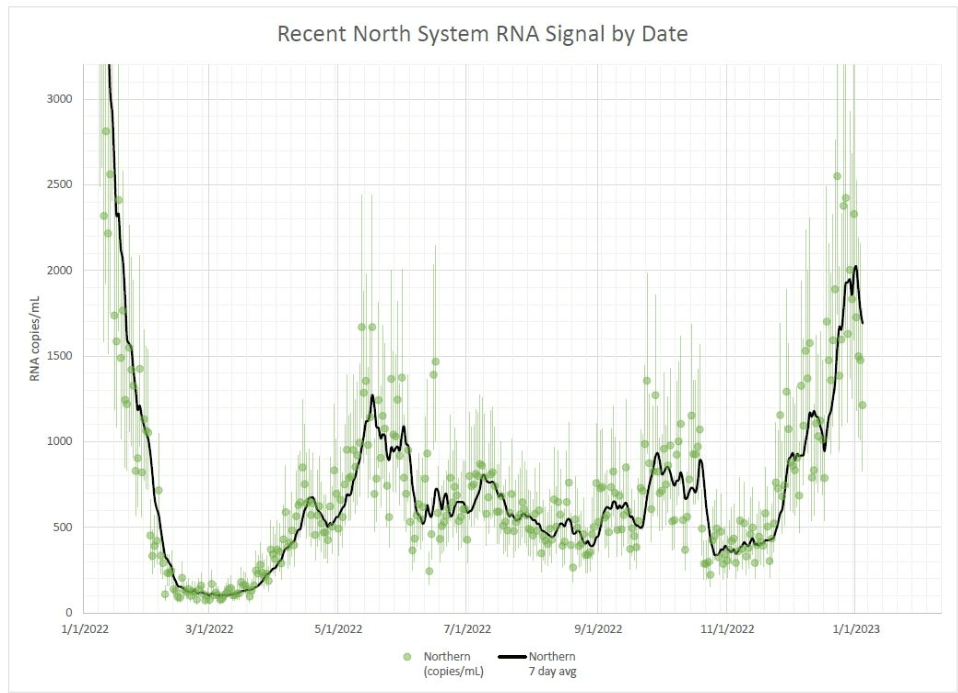
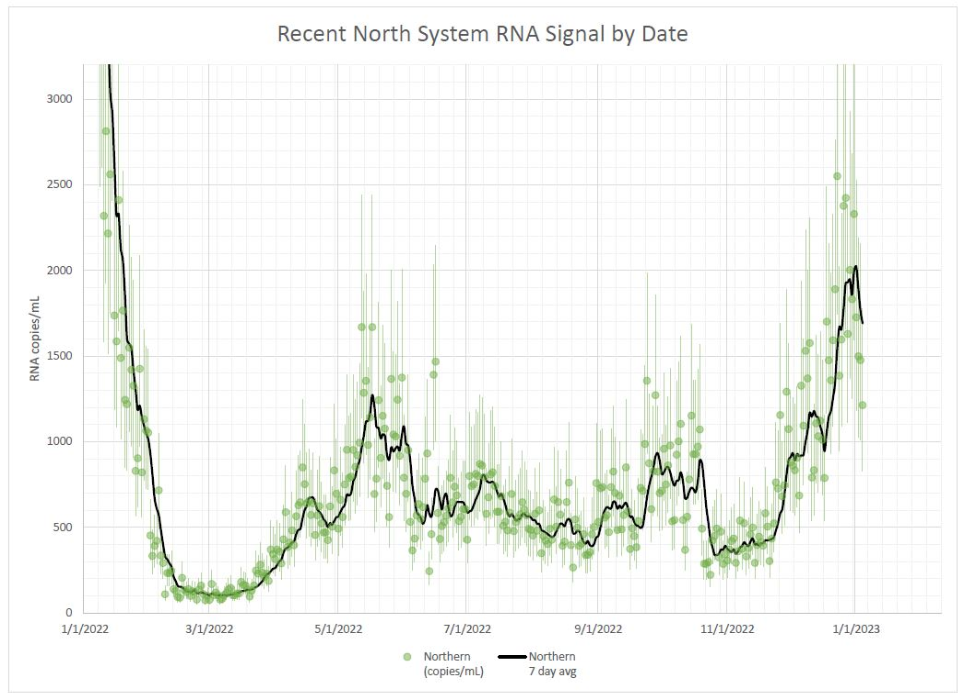
Wastewater surveillance from Biobot suggests that COVID-19 spread is decreasing in all four major regions. But the decrease is steeper in the Northeast and South than it is in the Midwest and West coast, suggesting potential plateaus in the latter regions. Wastewater data from the CDC continues to show decreased transmission in about half of sites reporting to the agency and increased transmission in the other half.
Where is COVID-19 spread increasing right now? Some northern Midwest states are reporting the most significant upticks. According to the latest Community Profile Report, new COVID-19 hospitalizations went up last week in South Dakota, Idaho, and Minnesota. Wastewater monitoring sites in Idaho and Minnesota also reported increased coronavirus concentrations, according to the WastewaterSCAN project.
In the Midwest and West coast, Omicron subvariant XBB.1.5 continues to outcompete other versions of the virus. Per the CDC’s estimates, it accounted for about 44% of new cases in the region including the Dakotas and Minnesota this week, compared to 32% last week. XBB.1.5 already dominates the East coast, so its rise in the rest of the country could be one reason why COVID-19 is starting to go up again.
Nationally, XBB.1.5 caused about two-thirds of new COVID-19 cases in the U.S. last week, according to the CDC’s estimates. It’s the only variant on the rise right now, as it drives out the BQ lineage and others. CH.1.1, the subvariant currently spreading fast in the U.K. and other countries, is less of a threat in the U.S. so far (at under 2% of new cases).
While XBB.1.5 contributes to new infections across the country, the number of Americans who’ve received an updated booster shot remains stubbornly low. Only 52 million people have received the Omicron-specific booster, representing just 20% of the eligible population, according to CDC data.
New York State expands wastewater surveillance program: This week, the New York State health department announced a major investment in the state’s wastewater surveillance program: the program has received a $6.6 million grant from the CDC and $15 million from the governor (over the next three years). With this investment, New York’s wastewater surveillance network will grow from 125 to 215 testing sites and will expand from COVID-19 to include flu, RSV, hepatitis, norovirus, and antimicrobial resistance. This is great news for New York—I hope to see other states make similar investments.
Bivalent boosters vs. XBB lineages: The bivalent, Omicron-specific booster shots provide some protection against XBB.1.5 and related Omicron subvariants, according to a new study published this week in the CDC’s Morbidity and Mortality Weekly Report. CDC researchers used data from COVID-19 testing at pharmacies to compare results among people who had received the new booster and those who hadn’t. Booster recipients were significantly less likely to have a symptomatic XBB/XBB.1.5 infection compared to people who hadn’t received the shot, the researchers found (with a vaccine effectiveness value of 48%). While the boosters work less well against XBB.1.5 than they did against BA.4/BA.5, they’re still a valuable protective measure.
CDC overhauling data communications: The CDC is creating new internal offices that will change how it processes, publishes, and communicates about data, according to POLITICO. The new offices include an Office of Health Equity and an Office of Public Health Data, Surveillance, and Technology—both of which have new acting directors as of this week. It’s currently unclear what the new offices will do, exactly, or how they will improve upon a fractured nationwide health data system (with decisions about how to store and share key data largely left up to state agencies and private companies). Still, it’s good to see movement on the CDC’s efforts.
WHO deliberates ending the global health emergency: On Friday, a World Health Organization committee met to discuss whether the official global health emergency over COVID-19 should be ended. The committee’s decision will be made public tomorrow, as a recommendation to WHO Director-General Tedros Adhanom Ghebreyesus; Tedros will ultimately decide whether or not to end the emergency. Global health experts who spoke to STAT reporter Helen Branswell suggested that the WHO likely isn’t ready to end this emergency yet, but it may happen later in 2023.
KFF compiles Long COVID data: A new report from the Kaiser Family Foundation compiles and provides context for Long COVID data reported by the Census and CDC’s Household Pulse Survey. The share of people who reported ever having Long COVID symptoms following a COVID-19 case has declined slightly over time, the KFF report finds; this number went from 35% in June 2022 to 28% in January 2023. However, the number is still high and Long COVID can be debilitating for many, as 79% of people with Long COVID report limitations to their day-to-day activities.
Health of Congressional Districts: Finally: a new dashboard, published this week by researchers at NYU Langone Health, provides detailed health metrics for all 435 Congressional districts in the U.S. (plus Washington, D.C.). The dashboard is a helpful source for researchers and policymakers looking to understand health patterns in specific districts. One of its key metrics is a “COVID Local Risk Index” that reflects the risk residents face for severe health, social, and economic outcomes of COVID-19.
Biobot’s regional data suggest that most of the country is seeing declining COVID-19 spread, but we’re heading into high plateaus.
In the past week (January 19 through 25), the U.S. officially reported about 300,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 42,000 new cases each day
90 total new cases for every 100,000 Americans
11% fewer new cases than last week (January 12-18)
In the past week, the U.S. also reported about 30,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 4,200 new admissions each day
9.0 total admissions for every 100,000 Americans
14% fewer new admissions than last week
Additionally, the U.S. reported:
3,800 new COVID-19 deaths (540 per day)
61% of new cases are caused by Omicron XBB.1.5; 31% by BQ.1 and BQ.1.1; 2% by CH.1.1 (as of January 28)
An average of 100,000 vaccinations per day
At the national level, COVID-19 spread appears to be approaching another plateau. New cases and hospitalizations (as reported by the CDC) are still in decline, but their descent is slowing: reported cases dropped by 11% this week, compared to 24% last week.
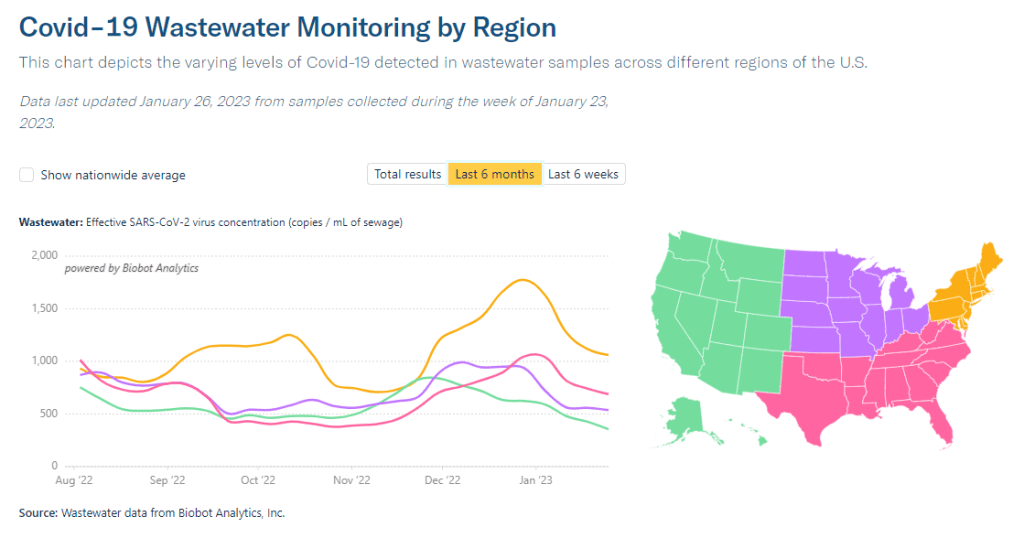
Wastewater surveillance presents the same trends. National data from Biobot suggest that COVID-19 transmission is leveling out in a similar place to where we were in October and November 2022, before the holiday surge drove up spread.
Biobot’s regional data show a slowing decline in the Northeast, plateaus in the Midwest and South, and a somewhat-more-pronounced decline in the West. And wastewater surveillance data from the CDC shows that COVID-19 spread is going up in some places, down in others: out of about 1,000 sites reporting data in the last two weeks, 48% reported decreases in coronavirus levels while 40% reported increases.
Unlike in recent weeks where every state has reported declines in COVID-19 cases and hospitalizations, a few places are now reporting definitive upticks, according to the latest Community Profile Report. These states include Alaska, Vermont, Maine, South Dakota, North Dakota, Nevada, Oklahoma, Minnesota, and Indiana.
Why might some states report COVID-19 upticks just after we emerged from a surge over the holidays? One explanation could be the XBB.1.5 variant, which continues to outcompete other Omicron lineages. XBB.1.5 now comprises about 60% of new cases nationwide (according to the CDC’s estimates); while it is most dominant in the Northeast, it’s growing—and likely reinfecting people—in other regions.
The CDC’s latest variant estimates also now include Omicron CH.1.1, which has been connected to rising cases in the U.K. and New Zealand in recent months. Per the CDC, CH.1.1 has been present in the U.S. at low levels (like, 1% or less) for a few weeks now, without posing a major challenge to XBB.1.5. But it is still a variant worth keeping an eye on.
As flu and RSV cases continue to trend down, the U.S. is confronted with the final weeks of a respiratory disease-heavy winter that was pretty rough on our healthcare system—but fell short of the mind-boggling case numbers that we saw in the prior two winters. Yes, we didn’t see a repeat of “the first Omicron wave”; but still, millions of people got sick, thousands died. Many will likely experience Long COVID as a consequence of their infections this winter.
In the past week (January 12 through 18), the U.S. officially reported about 330,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 47,000 new cases each day
101 total new cases for every 100,000 Americans
24% fewer new cases than last week (January 5-11)
In the past week, the U.S. also reported about 35,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 5,000 new admissions each day
10.7 total admissions for every 100,000 Americans
16% fewer new admissions than last week
Additionally, the U.S. reported:
4,000 new COVID-19 deaths (560 per day)
49% of new cases are caused by Omicron XBB.1.5; 40% by BQ.1 and BQ.1.1 (as of January 21)
An average of 150,000 vaccinations per day (CDC link)
National COVID-19 metrics continue to suggest that the U.S. is coming out of its holiday surge, though some parts of the country may face increased transmission as the Omicron variant XBB.1.5 spreads.
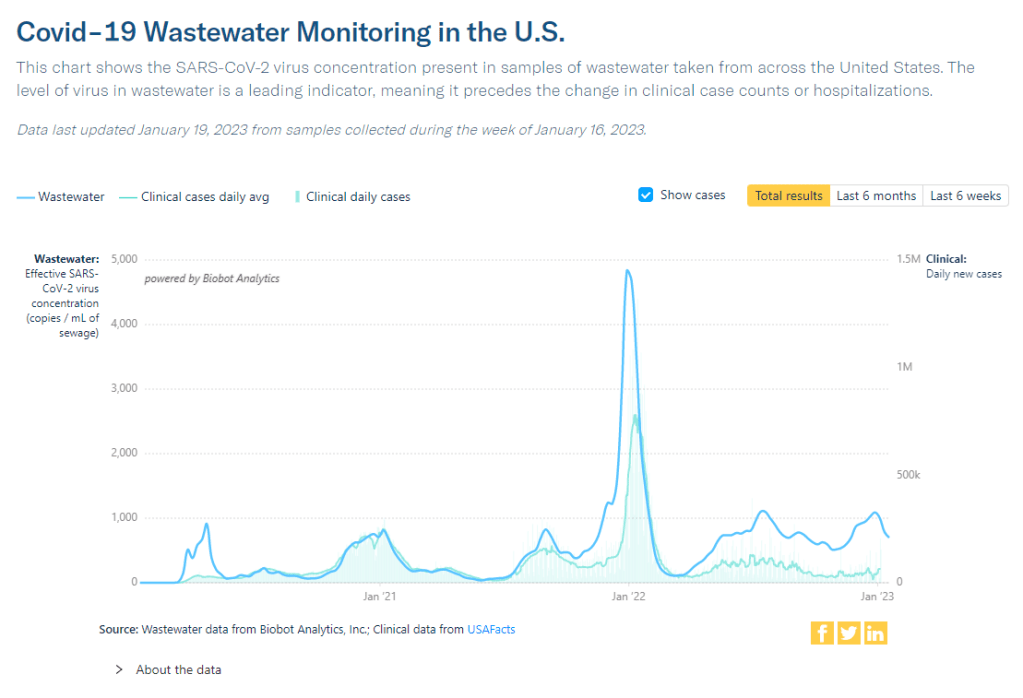
Official COVID-19 case numbers and new hospital admissions both reported declines this week, according to the CDC (of 24% and 16% respectively, compared to the prior week). Biobot’s wastewater surveillance data also show a decline, with coronavirus concentration at a similar level to mid-November 2022, just before Thanksgiving.
This trend is fairly consistent across states and regions, according to case and hospitalization data from the latest HHS Community Profile Report. However, Biobot’s regional and county-level data suggest that COVID-19 spread is in a plateau or even starting to increase in some parts of the South and Midwest regions.
Hospitalizations for the flu and RSV are following a similar pattern to COVID-19, according to a new CDC dashboard that reports on all three illnesses together. Almost all states reported moderate or low levels of influenza-like activity in the week ending January 14, very different from the patterns we were seeing a few weeks ago. The only areas still reporting high influenza-like activity are California, North Dakota, New Mexico, Texas, Puerto Rico, New York City, and Washington D.C.
All of this is good news, suggesting that the worst of this winter’s respiratory virus surges may be behind us. But COVID-19 is still spreading across the country at fairly high levels, reflecting the high baseline that the U.S. has faced ever since new Omicron subvariants started to hit in spring 2022.
We also need to continue watching XBB.1.5, the latest and most contagious version of Omicron. This subvariant caused about half of new cases in the U.S. in the last week, according to CDC estimates. It’s most prevalent in the Northeast but is quickly gaining ground in the Southeast and other regions. (And the BQ lineages that currently dominate these regions can spread quickly, too.)
In the coming weeks, we’ll see how much XBB.1.5 (and any other variants) contribute to increased transmission in these regions. Meanwhile, COVID-19 deaths went up recently as the holiday surge took its toll: more than 500 people have died from COVID-19 every day in the last two weeks. Deaths are always the most delayed—and the most tragic—metric.
New hospital admissions for COVID-19 are starting to trend down, according to the CDC, though we’ll need more data to see if this trend persists.
In the past week (January 5 through 11), the U.S. officially reported about 420,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 59,000 new cases each day
126 total new cases for every 100,000 Americans
13% fewer new cases than last week (December 29-January 4)
In the past week, the U.S. also reported about 40,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 5,800 new admissions each day
12.3 total admissions for every 100,000 Americans
12% fewer new admissions than last week
Additionally, the U.S. reported:
3,900 new COVID-19 deaths (560 per day)
43% of new cases are caused by Omicron XBB.1.5; 45% by BQ.1 and BQ.1.1 (as of January 14)
An average of 150,000 vaccinations per day (CDC link)
Last week, I wrote that a combination of holiday travel/gatherings and the latest Omicron subvariant, XBB.1.5, was driving a winter surge. This week, COVID-19 metrics suggest that the surge may have peaked, though we’ll need more data to say for sure—and XBB.1.5 remains a concern.
After reporting a significant increase in coronavirus levels through the end of December, Biobot’s wastewater dashboard is now showing downturns nationally and for all four U.S. regions. The CDC’s wastewater dashboard similarly shows that about two-thirds of sites in the National Wastewater Surveillance System have reported decreasing COVID-19 levels in the last two weeks, as of January 10.
“Importantly, this data is subject to change as we update 2x weekly,” Biobot’s Twitter shared on Thursday, when the company’s dashboard was most recently updated. “Stay tuned for Tuesday’s update.”
📣Our #Covid ww dashboard has been updated—https://t.co/GBL4twvGGT. We’re seeing a drop in concentrations in all regions, which may indicate the passing of the holiday surge. Importantly, this data is subject to change as we update 2x weekly. Stay tuned for Tuesday’s update.
Official COVID-19 cases and hospital admissions are also trending down, according to CDC data: new cases dropped by 13% from the week ending January 4 to the week ending January 11, while newly hospitalized patients dropped by 12%. But this trend isn’t universal; five states and Washington D.C. reported increased hospitalizations this week, with the biggest upticks in Rhode Island, Louisiana, and Maine.
XBB.1.5, the latest and most contagious Omicron subvariant, caused an estimated 43% of new cases nationwide in the week ending January 14, per the CDC. It’s clearly outcompeting BQ.1 and BQ.1.1 as well as a number of other strains in the “Omicron soup” we currently face, but is not taking over as quickly as we saw the original Omicron do in late 2021.
This strain continues to dominate the Northeast—particularly New England and New York/New Jersey—where COVID-19 spread is trending down. But it’s just starting to pick up in other parts of the country; to me, it seems likely that the Northeast had a holidays-and-XBB.1.5 combined surge, while other areas may face a second COVID-19 increase as this variant spreads more widely.
Meanwhile, other respiratory viruses continue to place additional burden on our health system. For example, the CDC recently released estimates about this year’s flu season, finding that the flu may have caused up to 560,000 hospitalizations and 48,000 deaths since fall 2022.
XBB.1.5 caused about 28% of new cases in the week ending January 7 (confidence interval: 14% to 47%), according to the CDC’s estimates.
You’ve probably seen it in the news this week: XBB.1.5 is the latest Omicron subvariant to spread rapidly through the U.S.
It is, of course, more transmissible and more capable of evading immunity from past infections than other versions of Omicron that have gone before it, as this lineage continues mutating. Scientists are still learning about XBB.1.5; it emerged from the U.S. during the holiday season, which has posed surveillance challenges. But we know enough to say that this variant is bad news for an already overstretched healthcare system.
Here’s a brief FAQ post on XBB.1.5.
Where did XBB.1.5 come from?
XBB, the parent of this latest lineage, emerged in Asia in October 2022. It evolved from Omicron BA.2 via recombination, which basically means two different BA.2 subvariants fused—likely while the same person was infected with both—and formed this new strain. (See my variants post from October for more details on XBB.)
XBB started spreading and mutating in the U.S. a few weeks later, leading to XBB.1.5. This subvariant was first identified in New York State in mid-December, though it could have evolved elsewhere in the northeast (since New York has better variant surveillance than some other states). Eric Topol’s newsletter has more details about XBB evolution.
New variant to watch
XBB.1.5 really taking off in New York, where it appears to have evolved
BQ.1* in NY has been almost flat since dominance in Nov
What are XBB.1.5’s advantages compared to other variants?
It spreads faster, likely because it is more capable of evading immune system protections from past infection or vaccination than other Omicron subvariants. In the U.S., CDC data suggests that XBB.1.5 is starting to outcompete other lineages in the “Omicron variant soup” we currently have circulating.
BQ.1.1 and XBB (original) were already known to be the best-evolved subvariants in this area before XBB.1.5 came along, according to this December 2022 paper in Cell. XBB.1.5 has taken this immune escape further, as it evolved a mutation called F486P that’s tied to this property.
“It’s crazy infectious,” Paula Cannon, a virologist at the University of Southern California, told USA TODAY reporter Karen Weintraub. Cannon added that protections that have worked against other coronavirus strains for the last three years will likely be less effective against XBB.1.5 and other new variants.
What questions are scientists currently working to answer about XBB.1.5?
One major question that arises with any new subvariant is severity: will XBB.1.5 have a higher capacity to cause severe symptoms than other coronavirus lineages? (We now know, for example, that Delta was more severe compared to prior variants.)
The World Health Organization is currently working on a report about XBB.1.5’s severity, according to POLITICO. Scientists and public health officials will also study whether current COVID-19 treatments work against this subvariant. Antiviral treatments Paxlovid and Mulnopiravir likely won’t be impacted, but Omicron’s continued evolution has put a lot of restrictions on monoclonal antibodies.
Another important question will be how well our updated booster shots work against XBB.1.5. The shots used in the U.S. were primed for BA.4 and BA.5, while XBB is derived (albeit indirectly) from BA.2, so our shots are not the best match. Still, antibody neutralization studies have shown that the shots provide protection against XBB, meaning some impact on XBB.1.5 is likely. This is a great time to get your booster if you haven’t yet.
What impact is XBB.1.5 currently having in the U.S.?
The subvariant caused about 28% of new cases in the week ending January 7, according to CDC estimates. These estimates have a fairly wide confidence interval, though, meaning that XBB.1.5’s true prevalence could be between 14% and 47%; the CDC will improve these estimates in the coming weeks as it collects more XBB.1.5 samples.
But we know with more confidence that XBB.1.5 has already taken over in the Northeast. It’s causing the vast majority of cases in HHS Region 1 (New England) and Region 2 (New York and New Jersey). Other mid-Atlantic states are catching up.
Some experts have noted that New York and other Northeast states are currently reporting rising COVID-19 hospitalizations, which could be a sign that XBB.1.5 causes more severe disease. It’s currently unclear how much the increased hospitalizations may be attributed to XBB.1.5’s presence, though, as the entire country is seeing this trend already in the wake of the holidays.
Sam Scarpino, a disease surveillance expert at Northeastern University, has a helpful Twitter thread explaining this issue. “It’s clear that XBB.1.5 is correlated [to] an increase in hospitalizations in many highly vaccinated states,” he writes. “I suspect it will hit harder in states with lower bivalent booster rates.”
1/ For those concerned about #XBB15 and hospitalizations, I think the evidence is more mixed than many are admitting.
While it's true hospitalizations are up in states like MA where XBB.1.5 is common, they are up across the entire US, even in states w/ little-to-no #XBB15! pic.twitter.com/LVrYqjn44K
Why has XBB.1.5’s prevalence been harder to pin down than other subvariants?
Many of the news articles you might have read this week about XBB.1.5 cited that the subvariant’s prevalence more than doubled in about one week, according to CDC estimates. But then the CDC’s estimates were revised down this week, suggesting that XBB.1.5 actually caused 18% of new cases in the last week of December—not 41%.
Why did the estimate change so dramatically? Well, it actually didn’t: as the CDC itself pointed out in its Weekly Review newsletter this Friday, the 41% estimate had a big confidence interval (23% to 61%), so the revision down to 18% was not far outside the existing realm of possibility. The CDC revises its variant estimates constantly as new data come in; this might be a bigger shift than we’re used to seeing, but it’s still pretty unsurprising.
The CDC’s variant forecasting team is also facing a couple of challenges unique to XBB.1.5 right now. First, this is a homegrown, U.S.-derived variant, so they don’t have a wealth of international sequences to analyze in preparation for a U.S. surge. And second, XBB.1.5 arose during the holidays, when a lot of COVID-19 testing and sequencing organizations were taking time off. The CDC is currently working with very limited data, but it will continue to revise estimates—and make them more accurate—as more test results come in.
For more info on the CDC’s process here, I recommend this Twitter thread from epidemiologist Duncan MacCannell:
The variant surveillance dashboard on the CDC COVID Data Tracker was just updated to include projections up to 1/7/2022; this is a weekly update that posts like clockwork every Friday. https://t.co/rnE66MCoHSpic.twitter.com/WGtfHix8va
How will XBB.1.5 impact the next phase of the pandemic?
Scientists will be closely watching to see how quickly XBB.1.5 spreads in other parts of the U.S., as well as how it performs in other countries that recently had surges of other Omicron subvariants.
Overall, the data we have about this subvariant so far suggest that it’s not distinct enough from other versions of Omicron to drive a massive new surge on the level of Omicron BA.1 last winter. But it’s still arriving in the wake of holiday travel and gatherings—and in a country that has largely abandoned public health measures that stop the virus from spreading.
In New York, for example, XBB.1.5 might not be the main cause of rising hospitalizations. Yet it is undoubtedly making more people sick with COVID-19, at a time when this region also faces continued healthcare pressure from flu and RSV. And an impending nurses’ strike won’t help the situation either, to put it mildly.
I think this Twitter thread from T. Ryan Gregory, an evolutionary biology expert who tracks coronavirus variants, is helpful at putting XBB.1.5 into context. This latest lineage follows other versions of Omicron that have kept the U.S. and other countries at relatively high levels of COVID-19 transmission throughout the last year. While our current moment may not look as dire as January 2022, we are currently seeing COVID-19 go up from an already-unsustainable baseline.
“BA.1 was the highest peak,” he writes, referring to 2022 in Canada and the U.K., “but the area under the curve of the others was as bad or worse.”
That said, I don't think "not as bad as the first Omicron wave" should be the standard. As noted, Canada, the UK, etc. had their deadliest year in 2022 through multiple Omicron waves. BA.1 was the highest peak, but the area under the curve of the others was as bad or worse. pic.twitter.com/5JwU857oHo
In the past week (December 29 through January 4), the U.S. officially reported about 470,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 67,000 new cases each day
143 total new cases for every 100,000 Americans
16% more new cases than last week (December 22-28)
In the past week, the U.S. also reported about 46,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 6,500 new admissions each day
13.9 total admissions for every 100,000 Americans
16% more new admissions than last week
Additionally, the U.S. reported:
2,700 new COVID-19 deaths (390 per day)
28% of new cases are caused by Omicron XBB.1.5; 56% by BQ.1 and BQ.1.1; 5% by XBB (as of January 7)
An average of 150,000 vaccinations per day
Well, here we are: the winter COVID-19 surge. It may have happened later than some experts predicted, but the U.S. is clearly now experiencing an uptick in virus transmission as the latest, most contagious Omicron subvariants collide with holiday travel and gatherings.
You might notice that the CDC’s official case numbers didn’t rise too dramatically this week (though the national count is up 16% compared to last week). That’s unsurprising: case increases after holidays are always delayed, because many testing sites and public health officials take time off from processing new data. Christmas and New Year’s tend to deliver the worst of this trend—and in 2022, limited access to PCR testing made case numbers even less reliable.
Wastewater surveillance, on the other hand, clearly shows a significant rise in coronavirus spread from early December through early January—building on another rise that followed Thanksgiving. Biobot’s dashboard suggests that the U.S. as a whole is seeing about as much COVID-19 transmission now as we saw at the peak of the summer BA.5 wave. In some places, transmission is the highest it’s been since last January (during the original Omicron surge.)
The CDC’s wastewater data similarly show increasing COVID-19: out of 600 sites with available recent data, more than half were reporting upticks in the two-week period ending January 2. 117 of those sites reported an increase between 100% and 999%, and 87 reported an increase over 1,000%.
Regionally, the Northeast has reported the biggest recent COVID-19 spike in wastewater, though the trend may already be turning around. We see this both in Biobot’s regional data and in individual cities and counties, like Boston and New York City. The Northeast is also a hotspot for XBB.1.5, a homegrown Omicron subvariant that’s spreading faster than other lineages. (More on that later in the issue.)
In addition to the wastewater surveillance, hospitalization data have remained uninterrupted by the holidays with clear increases in COVID-19 patients through December and into this week. This week, about 6,600 new COVID-19 patients were admitted to hospitals nationwide, a 16% increase from the prior week and about twice the number of people admitted during the week before Thanksgiving.
Washington D.C., Connecticut, Massachusetts, and West Virginia reported the highest rates of new COVID-19 patients in the week ending January 3, according to the latest Community Profile Report. They were followed by other Northeast states New Jersey, New York, and Delaware. But states reporting the highest increases in hospitalization are in the South: Louisiana, Mississippi, Florida, Texas.
Two pieces of good news for this week: the flu and RSV are both trending down after their surges earlier in the fall. High levels of influenza-like activity remain in the majority of states, though. And we may see a second flu peak driven by a second strain, as Katelyn Jetelina reports in Your Local Epidemiologist.
All the same safety measures we know and love—masks, testing, vaccinations, etc.—continue to help reduce the risk of COVID-19 and other viruses. But uptake of these measures remains low. As of January 5, only 15% of the eligible U.S. population has received an Omicron-specific booster dose, per the CDC.