Remember when I said “we’ll see if anything else happens” in last week’s article on AstraZeneca’s issues? Well, I accept full responsibility for manifesting the chaos that happened earlier this week and I promise I won’t tempt fate again this time around. If you’re confused, as I certainly was, here’s just what the hell happened.
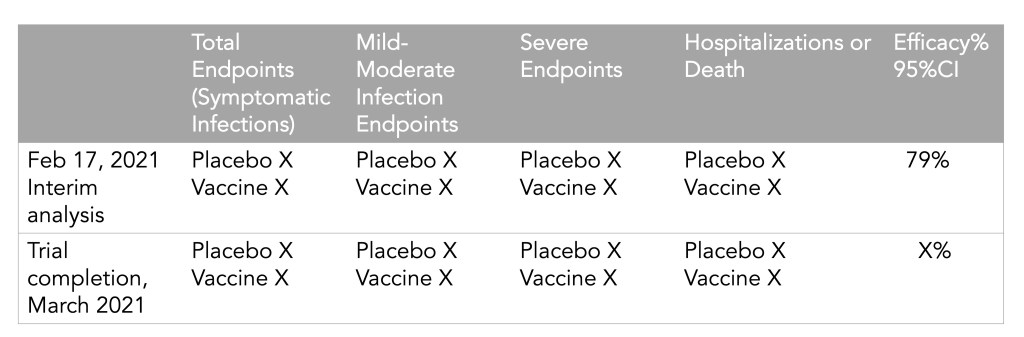
On Monday, AstraZeneca released results from their Phase 3 trials in the United States, and they looked good: 79% efficacy against symptomatic disease, 100% efficacy against hospitalizations and deaths. This was certainly a welcome result for the company which is continuing to grapple with fallout from rare cases of blood clots that have been reported in some people after they got the vaccine, and gears started to turn to get EUA approval in the United States. (Even though, again, the U.S. just promised most of their supply to Canada and Mexico. Everyone wants FDA clout, I guess.)
But on Tuesday, officials started to question the results. The results released on Monday had looked better than more recent results released elsewhere, one of which showed an overall efficacy of around 60%. Also, as Dr. Eric Topol pointed out, the data were fairly incomplete:
Independent reviewers from the data and safety monitoring board sent “a harsh note” to AstraZeneca, according to Anthony Fauci, and sure enough, it soon became clear that AstraZeneca had released outdated (better) numbers instead of the real results from the trial, obfuscating how efficacious the vaccine actually was in the U.S. trial.
#AstraZeneca saying its vaccine was 79% effective against symptomatic Covid when it is 76% effective is just like that guy on Hinge who says he is 5'11" when he is actually 5'9". Just why?
Following the end of the federal public health emergency in May, the CDC has lost its authority to collect vaccination data from all state and local health agencies that keep immunization records. As a result, the CDC is no longer providing comprehensive vaccination numbers on its COVID-19 dashboards. But we still have some information about this year’s vaccination campaign, thanks to continued CDC efforts as well as reporting by other health agencies and research organizations.
This week, the FDA authorized Novavax’s updated COVID-19 vaccine. Here’s why some people are excited to get Novavax’s vaccine this fall, as opposed to Pfizer’s or Moderna’s.
The problem child of COVID-19 vaccines was back in the news this week. After South Africa suspended the Oxford-AstraZeneca vaccine’s use when it failed to slow the spread of the predominant B.1.351 variant, vaccination using this vaccine has been suspended and then resumed in many European countries following reports of blood clots in some people who received it.
According to a release from AstraZeneca, there have been 15 cases of deep vein thrombosis and 22 cases of pulmonary embolism in people who have gotten the vaccine, as of March 8. These are serious complications—seven of those people died. Countries that suspended the vaccine’s use include Spain, Italy, France, and Germany, among others. (Europe tends to act as more of a bloc than North America when it comes to vaccines. Consider: Canada has authorized use of the AstraZeneca vaccine while the US has literal fridges full of the stuff just sitting there waiting for approval.)
Since the initial suspension, investigations have been launched and apparently concluded that there is no causative relationship between the vaccine and these symptoms. According to Emer Cooke, the executive director of the European Medicines Agency (EMA), in a press conference on March 18: “The committee… concluded that the vaccine is not associated with an increase in the overall risk of thromboembolic events or blood clots.”
And, according to the WHO on March 17: “At this time, WHO considers that the benefits of the AstraZeneca vaccine outweigh its risks and recommends that vaccinations continue.” Europe has since started to resume vaccinating with the Oxford-AstraZeneca vaccine, starting with France, Germany, and Italy. (Except not in Finland, where they just suspended it again after two people got similar blood clots.)
So all’s well that ends well right? Well, not necessarily. Besides that Finland wrinkle, some scientists and officials are concerned that this entire rigmarole could undermine public trust in the AstraZeneca vaccine. It’s worth noting that a tiny population experienced these effects out of the millions of people who have already gotten the vaccine. And blood clots are fairly common in the population; you’re going to expect some people to develop them just by sheer chance. But it’s also worth noting that these complications are serious, and rare among the age group that they were reported in. Not slowing down could have the same fear-inducing effect. As Shobita Parthasarathy says in her Slate column, “[T]his crisis isn’t about science at all. It’s about public trust, and scared citizens cannot be easily convinced by expertise that feels remote. Our solutions need to reflect that.”
We’ll see if anything else happens. But in the meantime, the US has since promised to share its stockpile of the Oxford-AstraZeneca vaccine with Canada and Mexico, so it looks like it’s at least medium-steam ahead for now.
Following the end of the federal public health emergency in May, the CDC has lost its authority to collect vaccination data from all state and local health agencies that keep immunization records. As a result, the CDC is no longer providing comprehensive vaccination numbers on its COVID-19 dashboards. But we still have some information about this year’s vaccination campaign, thanks to continued CDC efforts as well as reporting by other health agencies and research organizations.
This week, the FDA authorized Novavax’s updated COVID-19 vaccine. Here’s why some people are excited to get Novavax’s vaccine this fall, as opposed to Pfizer’s or Moderna’s.
More good vaccine news this week: Novavax, the current candidate using a recombinant protein method, released results from trials in the United Kingdom and South Africa, and they look good. Here’s the breakdown:
100% effective against hospitalization and death across all regions tested
96.4% effective against symptomatic disease in the “original strain”
86.3% effective against symptomatic B.1.1.7
48.6% effective against symptomatic Covid-19 in South Africa (where B.1.351 is the predominant strain)
It should be noted that the UK trial was a full phase 3, while the South African trial was a smaller phase 2b trial—so we have less information for South Africa. There’s also currently a 30,000-person trial happening in the United States and Mexico which should shed more light on what this vaccine can do. But for now, these results are super encouraging.
Yesterday, the FDA gave the Janssen—did you know it’s pronounced yahn-sen? I didn’t—vaccine Emergency Use Authorization, allowing it to join the likes of Pfizer and Moderna in the exclusive club of vaccines that may now be distributed in the U.S. Welcome, Janssen. (As a total coincidence I’m wearing my shirt that just says “Vaccines!” on it as I write this.) But the addition of a new vaccine in circulation also brings data reporting questions with few easy answers.
I got to hear the VRBPAC (Vaccines and Related Biological Products Advisory Committee) hold music for the first time on Friday. As I am a full-time student, I couldn’t watch the entire meeting; thus, a lot of this coverage is aided by Helen Branswell and Matthew Herper’s liveblog on STAT News—thank you guys for saving me hours of video to sift through.
The gist of the meeting is that of course it passed the committee vote. I’m pretty sure no one expected it wouldn’t. Katelyn Jetelina, who runs the Your Local Epidemiologist newsletter, certainly didn’t, especially because we knew beforehand that it was 100% effective in preventing hospitalizations and deaths.
However, I did find it interesting that the vote was unanimous—which I wasn’t expecting, given the pattern established by Pfizer and Moderna beforehand. Pfizer passed with 17 pro and 4 against (and 1 abstention); they did not explain their votes in that meeting but authorization for kids aged 16-17 was a sticking point. Moderna passed with 20 pro and 1 abstention; the question—“Based on the totality of scientific evidence available, do the benefits of the Moderna Covid-19 vaccine outweigh its risks for use in individuals 18 years of age and older?”—was worded too broadly, and the abstainer would have preferred to target authorization to high risk populations).
So what changed? Herper noted in the liveblog that the unanimous vote doesn’t necessarily mean this is a better vaccine than Pfizer or Moderna. It was more about panelists’ increased faith in the EUA process. Pfizer and Moderna have been EUA’d for a while and, per Patrick Moore of the University of Pittsburgh, “things are looking good.” Agreed! Now if we could just get it into more deltoids…
But we’re not here for deltoids, we’re here for data. The J&J presentation basically reiterated what we knew with some key statistics: The big Phase 3 study enrolled more than 44,000 participants globally. Across the entire study, the protection efficacy against severe disease was 85%, and that’s including the U.S. and South Africa (important because of variant prevalence in the latter country). No one who got the vaccine was hospitalized or died due to COVID-19. The efficacy against moderate to severe disease was 72% in the US, and 66% across all countries studied. These numbers were similar across ages, comorbidity statuses, sexes, races, and ethnicities. In short: it works.
There is a lack of data in people aged 75 or older. Only 755 people (3.8% of all participants) in this age group received the vaccine in the ENSEMBLE trial, and the FDA noted that it’s hard to interpret such low numbers. As Branswell says in the STAT liveblog, the trial didn’t prove that the vaccine works in older individuals. However, the VRBPAC committee barely touched on this. Either way, it’s been approved for adults 18 and over, and there’s nothing in the recent communications that indicates adults 60 and over aren’t advised to get it.
There are data questions beyond the VRBPAC committee meeting, though. Most vaccination dashboards are set up for a two-dose vaccine; they document how many people have gotten both shots and how many people have gotten just the first. So we don’t really know what’s going to happen when the Janssen vaccine becomes available—will that number factor into “people who have only gotten one dose?” Personally, I think the dashboards are going to have to change to “people who have partially completed dosing regimen” and “people who have completed the dosing regimen,” but knowing the states, it’ll likely be more complicated than that. Drew Armstrong, who runs Bloomberg’s Vaccine Tracker, mentioned in our CDD workshop last week that his team is already calling public health departments in order to discern how their reporting will change.
The question of how the dashboards will change gets more complicated when one considers a sticking point that actually was brought up in the committee meeting: just how many doses Janssen will eventually recommend. This particular petition was for a single dose vaccine. But Janssen has also been testing a two-dose regimen. Dr. Paul Offit, a member of the committee and a vaccine researcher, brought this up and raised a very important question: what if the two-dose regimen works better? What happens then? How is that going to be communicated to the public? How is that going to show up in the dashboards?
It’s tricky. The response, for now, is that the two-dose trial is still double-blinded, and that right now we’re concerned with granting EUA to a single-dose vaccine. The possibility was raised that the two-dose regimen might be what Janssen presents for true-blue FDA authorization. But we’re not there yet.
However, to go back to our dashboard question, let’s entertain for a minute that Janssen sees that the two-dose regimen works demonstrably better than the single-dose regimen. I find it hard to believe that this will come before the single-dose vaccines have started to be administered—and documented in dashboards. What happens to the dashboards then? Even if we assume it’s changed by then to “completed vaccine regimen” vs “partially completed vaccine regimen,” does that mean everyone who got the Janssen vaccine before – and would be counted under “completed regimen”—would have to be moved to “partially completed regimen?”
The ending sentiment seemed to be that the two-dose questions are a bridge we should cross when we get to it. While I sort of agree, I do think it’s worth considering now when it comes to data ramifications. States should be thinking about how they’re going to document this so we’re not blindsided if Janssen and the FDA decide that you need two shots for maximum COVID protection. We have enough data problems as it is, why add more?
Following the end of the federal public health emergency in May, the CDC has lost its authority to collect vaccination data from all state and local health agencies that keep immunization records. As a result, the CDC is no longer providing comprehensive vaccination numbers on its COVID-19 dashboards. But we still have some information about this year’s vaccination campaign, thanks to continued CDC efforts as well as reporting by other health agencies and research organizations.
This week, the FDA authorized Novavax’s updated COVID-19 vaccine. Here’s why some people are excited to get Novavax’s vaccine this fall, as opposed to Pfizer’s or Moderna’s.
Last week, Janssen, a pharmaceutical division owned by megacorp Johnson & Johnson, released results for its phase 3 ENSEMBLE study. The Janssen vaccine uses an adenovirus vector (a modified common cold virus that delivers the DNA necessary to make the coronavirus spike protein), can be stored at normal fridge temperatures, and only requires one dose. Here’s a table of the raw numbers from Dr. Akiko Iwasaki of Yale:
A single-shot J&J Janssen COVID19 vaccine phase 3 results summarized in one table. Great news! Imagine being 💯 protected from death 28 days after a single shot, and 💯 protected from severe disease after 49 days – against all variants. https://t.co/gGCcDbMglrpic.twitter.com/gPCDgG8oNJ
At first glance it does look like it’s “less effective” than the mRNA vaccines from Moderna and Pfizer. But, when you look at the severe disease, there’s a 100% decrease in deaths. No one who got the J&J vaccine died of coronavirus, no matter where they lived— including people who definitely were diagnosed with the South African B.1.351 variant. Here’s how that compares with the Moderna, AstraZeneca, Pfizer, and Novavax vaccines, per Dr. Ashish Jha of Brown:
Am often asked about different vaccines and their efficacy
Each trials tracks, reports efficacy differently
Currently, we have preliminary results for Novavax and J&J
But what numbers matter? What should you look for?
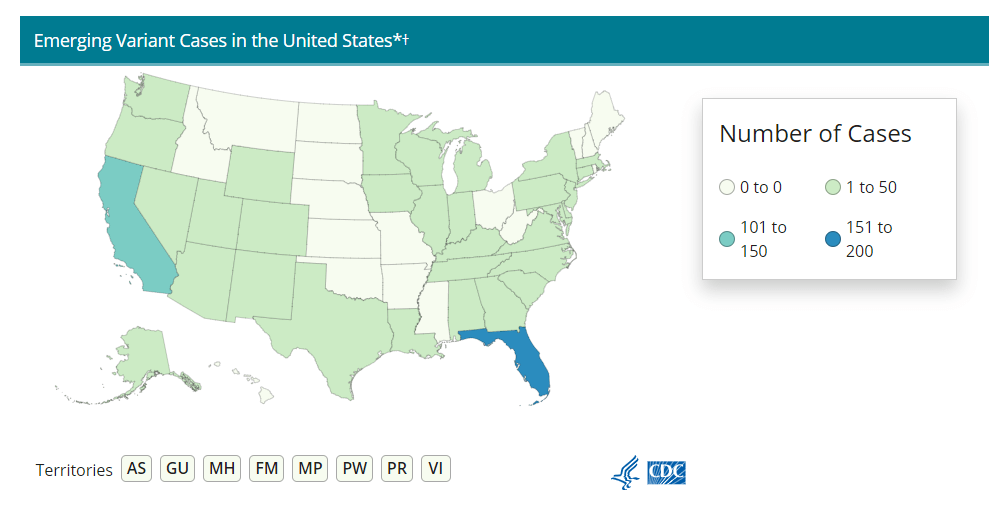
Nobody who got any of the vaccine candidates was hospitalized or died from COVID-19. That’s huge, especially as variants continue to spread across the U.S. (Here’s the updated CDC variant tracker.)
J&J’s numbers are especially promising when it comes to variant strains. Moderna and Pfizer released their results before the B.1.1.7 (U.K.) or B.1.351. (S.A.) variants reached their current notoriety, which makes J&J’s overall efficacy numbers look worse by comparison. But the fact that no one who got the J&J vaccine was hospitalized no matter which variant they were infectedwith is a cause for optimism. (B.1.351 is the variant raising alarms for possibly being able to circumvent a vaccine’s protection due to a helpful mutation called E484K. A Brazilian variant, P1, also has this mutation, though there’s not a lot of research on vaccine efficacy for this particular mutant.)
It also means that vaccination needs to step up. While it may seem counterintuitive to step up vaccinations against variants that can supposedly circumvent them, it’s important to note that there still was a significant decrease in COVID-19 cases in vaccinated patients from South Africa. A 57% drop compared with the 95% prevalence of the B.1.351 still suggests that vaccination can prevent these cases, and thus can seriously slow the spread of the variant.
What does all of this mean for COVID-19 rates? We can infer a few things. For starters, when vaccines are distributed to the general public around April or May, we may see hospitalization rates and death rates drop more than positive test rates. Positive test rates should obviously drop too, but they’ll probably stay at least a little higher than hospitalizations and death rates for a while.
Second, it means that we really need to ramp up sequencing efforts in the U.S.. We need more data to tell us just how well these vaccines can protect against the spreading variants, but we can’t collect that data if we don’t know which strain of SARS-CoV-2 someone gets. We here at the CDD have covered sequencing efforts – or lack thereof – before, but the rollout has still been painfully slow. CDC Director Rochelle Walensky stressed that “we should be treating every case as if it’s a variant during this pandemic right now,” during the January 29 White House coronavirus press briefing. But the6,000 sequences per week she’s pushing for as of the February 1 briefing should have been the benchmark months ago. We’re still largely flying blind until we can get our act together.
Some states in particular may be flying blinder than others. As Caroline Chen wrote in ProPublica yesterday, governors of New York, Michigan, Massachusetts, California, and Idaho are planning to relax more restrictions, including those on indoor dining. Such a plan is probably the perfect way to ensure these variants spread, so much that even Chen was surprised at how pessimistic the outlook was when she asked 10 scientists for the piece.
The B.1.1.7 variant is expected to become the dominant strain in the U.S. by March, according to the CDC. And on top of that, the B.1.1.7 variant seems to have picked up that helpful E484K mutation in some cases as well. Per Angela Rasmussen of Georgetown University, if these governors don’t realize how much they’re about to screw everything up, “the worst could be yet to come.” God help us.
Two weeks ago, after Pfizer announced its preliminary results, I posed a set of questions that can guide how you understand the details in COVID-19 vaccine press releases.
I’m revisiting those questions now in the wake of AstraZeneca and the University of Oxford’s news. The 70% effectiveness rate announced last Monday is promising at first glance, but details about this vaccine’s clinical trials have puzzled epidemiologists. Here’s what to consider as we await more details on AstraZeneca and Oxford’s findings, drawing on reports from STAT News, Nature, and the New York Times.
What is the sample size? Or, how many people were involved in the trial, and how many of them were diagnosed with COVID-19? AstraZeneca’s Monday announcement reported results from ongoing trials in the United Kingdom and Brazil, which include about 11,400 participants. 131 patients in the trial have tested positive for COVID-19. But here’s where things get tricky: out of those 11,400 participants, about 2,700 were given a lower dose of vaccine in their first shot due to an error in the U.K. trial. The other 8,900 trial participants received a standard two shots, i.e. two full doses of the vaccine. So, that 70% effectiveness rate is actually the average of results from two groups. In patients who received two full doses, the vaccine was 62% effective, while in patients who received a half dose and full dose, the vaccine was 90% effective.
Wait, the vaccine worked better in a lower dose? Yes—or at least, that’s what the data tell us so far. The researchers who made that dosing error may have gotten lucky by giving patients an initial dose which better stimulated their immune systems to act against the coronavirus. Nature’s Ewen Callaway quotes immunologists who say a lower dose might more effectively turn on T cells—immune cells that support antibody production—or more quickly activate the immune system’s memory of the virus. Still, the effectiveness rates we’ve seen for this vaccine so far may have been skewed by a small trial size; AstraZeneca has not reported how many patients among the 131 diagnosed with COVID-19 received a half-dose of the vaccine as compared to two full doses. AstraZeneca and Oxford will continue to study both the half-dose and full-dose regimens, and the scientific community eagerly awaits more data (and more details on how these trials are operating).
Astrazeneca/Oxford get a poor grade for transparency and rigor when it comes to the vaccine trial results they have reported. This is not like Pfizer or Moderna where we had the protocols in advance and a pre-specified primary analysis was reported. 1/5
Who is included in the sample size? Or, has this vaccine been tested on seniors, people of color, people with preexisting medical conditions that may garner worse COVID-19 outcomes, and other marginalized groups? In addition to their U.K. and Brazil trials, AstraZeneca and Oxford are conducting trials in the U.S., Japan, Russia, South Africa, Kenya, and Latin America with planned trials in other nations, including up to 60,000 total participants. AstraZeneca’s press release states that these global trials include “participants aged 18 years or over from diverse racial and geographic groups”; no further information on participant demographics is available.
Does the vaccine work for severe cases? Or, can this vaccine help reduce COVID-19’s severity by boosting immune system defenses for patients who may otherwise get seriously ill? So far, it seems possible: no patients in AstraZeneca and Oxford’s initial analysis group went to the hospital or otherwise reported severe illness. But more results are needed for a conclusion to be made.
Does the vaccine work for mild or asymptomatic cases? Or, can this vaccine prevent people from spreading COVID-19 even if they don’t cough, sneeze, or otherwise show symptoms? AstraZeneca and Oxford are more poised to answer this question than other potential vaccine makers because participants in the U.K. trial have routinely tested themselves for the coronavirus, regardless of if they exhibited any symptoms. Results so far show that yes, this vaccine may block COVID-19 transmission—but again, more data are needed from a wider study group.
Does the vaccine have any adverse effects? Or, what might happen to you when you get the shot? Pfizer has reported that a small number of patients got headaches or felt fatigued after receiving their shots; Moderna has reported similar side effects as well as fever and muscle pain. AstraZeneca and Oxford have yet to report side effects from their vaccine, but their ongoing global trials will give the researchers more opportunity to see and communicate possible small hazards of the vaccination experience.
What are the vaccine’s logistical needs? Like Pfizer and Moderna’s vaccine candidates, AstraZeneca and Oxford’s vaccine requires two doses given weeks apart. Unlike the other two candidates, this vaccine can be stored in a normal refrigerator for up to six months, making it much easier to distribute—particularly to remote and low-income areas. It’s also easier to mass-produce, and AstraZeneca will only be charging $3 to $4 a dose, making it cheaper for governments to buy in bulk. (The U.S. government has promised that COVID-19 vaccines will be free to all Americans.) More logistical needs for all three vaccine candidates will be finalized in the coming months.
Meanwhile, in Russia, vaccine trial results have been reported after only 39 documented COVID-19 cases:
Some new data came out today on the “other” #covid19 vaccine, Russia’s Sputnik V: Press release claims efficacy of 91,4% – 28 days after 1st shot 95% – 42 days after 1st shot
Apart from usual caveats it is important to note that this comes from analysis of just 39 infections: pic.twitter.com/8sMV8SRbRQ
This past Monday, pharmaceutical company Pfizer announced preliminary clinical trial results for its COVID-19 vaccine. In an interim analysis of the vaccine’s phase 3 study, the vaccine was shown to be 90% effective in preventing COVID-19. In other words, based on the people in Pfizer’s study who have become diagnosed with COVID-19 so far, those who got vaccinated were 90% less likely to get sick compared with the people who did not.
90% is an exciting number. The Food & Drug Administration (FDA) set a threshold of 50% effectiveness for COVID-19 vaccines to be authorized, and experts have been telling us for months that even a 60% or 70% effectiveness would still be incredibly useful in reducing infections across the population. Pfizer’s initial 90% rate blows those expectations out of the water.
Plus, this effectiveness value bodes well for other vaccine candidates. Pfizer’s vaccine, developed through a partnership with German biotech BioNTech, uses a new vaccine technology based on synthetic messenger RNA, or mRNA; so does the vaccine developed by Moderna, which is also currently in clinical trials. (For more backstory on mRNA, BioNTech, and Moderna, I highly recommend Damian Garde’s feature in STAT News.)
But we can’t get too excited. Pfizer reported its preliminary data not in a peer-reviewed scientific paper, but in a press release, and some key details about the company’s clinical trial are not yet public. I used information from STAT News, KHN, and SciLine to compile a few key questions that should be in all of our minds as we think about this and future vaccine data releases.
What is the sample size? Or, how many people were involved in the trial, and how many of them were diagnosed with COVID-19? For Pfizer’s trial, this is a question we can answer: about 44,000 people are enrolled in the study, and the 90% effectiveness rate is based on results from 94 people who contracted COVID-19, the majority of whom did not receive a vaccine dose. This may seem like a tiny fraction of the participants, but many experts are cautiously optimistic in hoping the 90% rate will hold up for a larger group.
Who is included in the sample size? COVID-19 has disproportionately impacted the elderly, people of color, people with certain medical conditions, and other marginalized groups. It is thus crucial that a vaccine is effective for people in these groups—in other words, these people must be represented in the vaccine trial. Pfizer reports that 42% of the overall study participants have “diverse backgrounds,” but the specific backgrounds of the patients who got sick are unknown.
Does the vaccine work for severe cases? While the majority of people diagnosed with COVID-19 are able to survive the disease with mild symptoms in their own homes, the minority of people who become seriously ill constitute the pandemic’s massive loss, as well as its burden on our nation’s healthcare system. A vaccine that reduces the disease’s severity through boosting immune system defenses may be incredibly valuable, even if it does not entirely prevent infection.
Does the vaccine work for mild or asymptomatic cases? A vaccine that prevents mild cases would help keep COVID-19 spread at bay, even if this vaccine does not reduce the disease’s severity. Pfizer’s press release does not include any specifics on the 94 patients who were diagnosed with COVID-19; experts are hoping that such details may be revealed in a forthcoming scientific paper.
Does the vaccine have any adverse effects? In other words, is the vaccine safe? We all know that flu vaccines make our arms sore, and other vaccines can give us mild colds. These types of common effects are usually nothing to worry about, but vaccines may pose a more severe danger to a small fraction of the population; for example, one in every ten thousand patients might have an allergic reaction that sends them to the hospital. So far, Pfizer has not reported any severe effects of its vaccine, but the current clinical trial gives the company a much wider pool of people in which dangerous reactions might be observed.
What are the vaccine’s logistical needs? One dose or two? At what temperature does the vaccine need to be stored? How long can it be at room temperature before it needs to be administered? How many doses can be manufactured in a day, a week, a year? What’s the price tag? Pfizer has given preliminary answers to some of these questions (two doses, -70 degrees Celsius) but the company is finalizing its manufacturing and distribution strategies as it completes its clinical trial.
Even when a vaccine is authorized by the FDA, distributing and tracking it poses a whole new set of questions. I’ve written about vaccine data before, and I expect that this will be a topic I cover in increasing detail during the months to come.