Lessons learned from the non-superspreader Anime NYC convention: Last fall, one of the first Omicron cases detected in the U.S. was linked to the Anime NYC convention, a gathering of more than 50,000 fans. Many worried that the event had been a superspreader for this highly contagious variant, but an investigation from the CDC later found that, in fact, Omicron spread at the convention was minimal. My latest feature story for Science News unpacks what we can learn from this event about preventing infectious disease spread—not just COVID-19—at future large events. I am a big anime fan (and have actually attended previous iterations of Anime NYC!), so this was a very fun story for me; I hope you give it a read!
my latest @ScienceNews feature: despite Omicron's presence at the Anime NYC convention last fall, it turned out not to be a COVID-19 superspreader. what can we learn from Anime NYC about preventing disease spread at future large events? (1/5) https://t.co/MMzlyInTiypic.twitter.com/ZMOJ7EEvt9
States keep reducing their data reporting frequency: Last Sunday, I noted that Florida—one of the first states to shift from daily to weekly COVID-19 data updates—has now gone down to updating its data every other week. This is part of an increasing trend, writes Beth Blauer from the Johns Hopkins COVID-19 data team in a recent blog post. “As of March 30, only eight states and territories (AR, DE, MD, NJ, NY, PA, PR, and TX) report case data every day of the week,” Blauer says. And it seems unlikely that states will increase reporting frequencies again without a major change in public health funding or the state of the pandemic.
Biden administration announces Long COVID task force: This week, the Biden administration issued a memo addressing the millions of Americans living with Long COVID. The administration is creating a new, interagency task force, with the goal of developing a “national research action plan” on Long COVID, as well as a report laying out services and resources that can be directed to people experiencing this condition. It’s worth noting that recent estimates from the U.K. indicate 1.7 million people in that country (or one in every 37 residents) are living with Long COVID; current numbers in the U.S. are unknown due to data gaps, but are likely on a similar scale, if not higher.
Long COVID data just out from the ONS TL;DR -1.7 million people now living with long COVID (28 day definition) – that's 1 in 37 people in the commiunity -780,000 have had this for *more than a yr* -at least 334000 got this during the omicron wave (impact since Feb not felt yet)🧵
Study indicates continued utility for COVID-19 testing in schools: During the Omicron surge, testing programs in a lot of schools collapsed, simply because institutions didn’t have enough resources to handle all of the students and staff getting sick. The surge led some schools to consider whether school testing programs are worth continuing at all. But a new study, released last week in The Lancet, suggests that yes, surveillance testing can still reduce transmission—even when schools are dealing with highly contagious variants. (Note that this was a modeling study, not a real-world trial.)
Preprint shows interest in self-reporting antigen test results: Another interesting study released recently: researchers at the University of Massachusetts distributed three million free rapid, at-home antigen tests between April and October 2021, then studied how test recipients interacted with a digital app for ordering tests and logging results. About 8% of test recipients used the app, the researchers found; but more than 75% of those who used it did report their antigen test results to their state health agency. The results (which haven’t yet been peer-reviewed) suggest that, if institutions make it easy and accessible for people to self-report their test results, the reporting will happen.
Omicron has caused more U.S. COVID-19 deaths than Delta. Despite numerous headlines proclaiming the Omicron variant to be “milder” than previous versions of the coronavirus, this variant infected such a high number of Americans that it still caused more deaths than previous waves, a new analysis by the New York Times shows. Between the end of November and this past week, the U.S. has reported over 30 million new COVID-19 cases and over 154,000 new deaths, the NYT found, compared to 11 million cases and 132,000 deaths from August 1 through October 31 (a period covering the worst of the Delta surge).
124 countries are not on target to meet COVID-19 vaccination targets. The World Health Organization (WHO) set a target for all countries worldwide to have 70% of their populations fully vaccinated by mid-2022. As we approach the deadline, analysts at Our World in Data estimated how many countries have already met or are on track to meet the goal. They found: 124 countries are not on track to fully vaccinate 70% of their populations, including the U.S., Russia, Bangladesh, Egypt, Ethiopia, and other large nations.
Anime NYC was not an omicron superspreader event, CDC says. In early December, the Minnesota health department sounded the alarm about a Minnesotan whose COVID-19 case had been identified as Omicron—and who had recently traveled to New York City for the Anime NYC convention. The CDC investigated possible Omicron spread at this event, both by contact tracing the Minnesota case and by searching public health databases for cases connected to the event. Researchers found that this convention was not a superspreader for Omicron, despite what many feared; safety measures at the event likely played a role in preventing transmission, as did the convention’s timing at the very beginning of NYC’s Omicron wave. I covered the new findings for Science News.
ATTN WEEBS! two new reports, published today by the CDC, find that #AnimeNYC was not actually a superspreader event, despite Omicron's presence at the convention — but the situation is still complicated. I covered this for @ScienceNews: (1/11) pic.twitter.com/zSyCWl2t7H
Americans with lower socioeconomic status have more COVID-19 risk, new paper shows. Researchers at Brookings used large public databases to investigate the relationship between socioeconomic status and the risk of COVID-19 infections or death from the disease. Their paper, published this month in The ANNALS of the American Academy of Political and Social Science, found that education and income are major drivers of COVID-19 risk, as are race and ethnicity. The researchers also found that: “ socioeconomic status is not related to preventative behavior like mask use but is related to occupation-related exposure, which puts lower-socioeconomic-status households at risk.”
The federal government has failed to disclose how much taxpayers are spending for “free” COVID-19 tests. One month into the Biden administration’s distribution of free at-home COVID-19 tests to Americans who request them, millions have received those tests. But the government has not shared how much it spent for the tests, making it difficult for journalists and researchers to determine how much taxpayer money was paid for each testing kit. “The reluctance to share pricing details flies against basic notions of cost control and accountability,” writes KHN reporter Christine Spolar in an article about this issue. The government has also failed to share details about who requested these free tests or when they were delivered, making it difficult to evaluate how equitable this distribution has been.
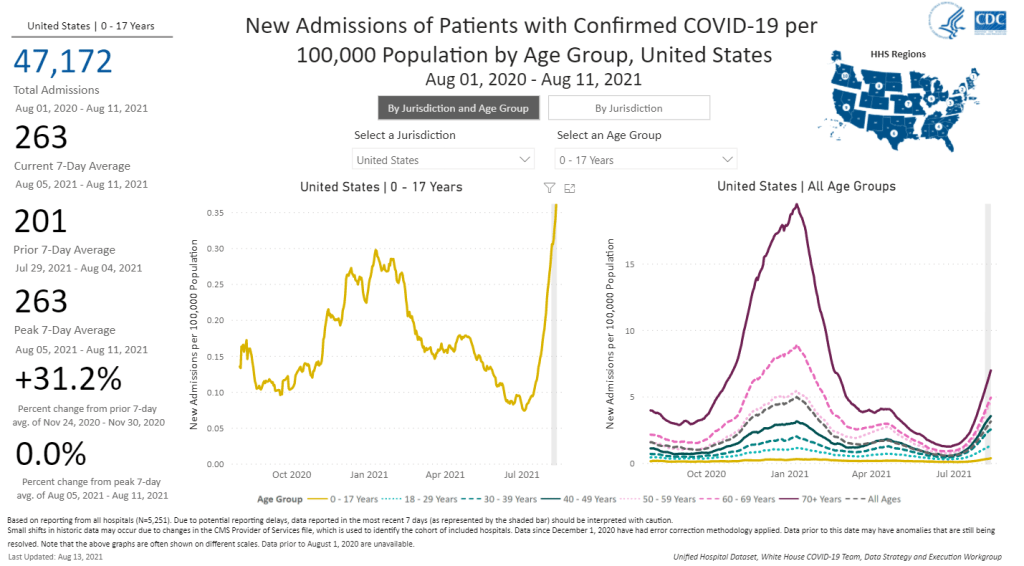
The number of children hospitalized with COVID-19 has shot up in recent weeks. Chart from the CDC COVID Data Tracker.
A couple of additional items from this week’s COVID-19 headlines:
1,900 children now hospitalized with COVID-19 in the U.S.: More kids are now seriously ill with COVID-19 than at any other time in the pandemic. The national total hit 1,902 on Saturday, according to HHS data. Asked about this trend at a press briefing on Thursday, Dr. Anthony Fauci explained that, thanks to Delta’s highly contagious properties, we’re now seeing more children get sick with COVID-19 just as we are seeing more adults get it. The vast majority of kids who contract the virus have mild cases, but this is still a worrying trend as schools reopen with, in many cases, limited safety measures. For more on this issue, I recommend Katherine J. Wu’s recent article in The Atlantic.
2.7% of Americans now eligible for a third vaccine dose: Both the FDA and the CDC have now given the go-ahead for cancer patients, organ transplant recipients, and other immunocompromised Americans to get additional vaccine doses. There are about 7 million Americans eligible, comprising 2.7% of the population. Studies have shown that two Pfizer or Moderna doses do not provide these patients with sufficient COVID-19 antibodies to protect against the virus, while three doses bring the patients up to the same immune system readiness that a non-immunocompromised person would get out of two dioses. Still, this move goes against the World Health Organization’s push for wealthy nations to stop giving out boosters until the rest of the world has received more shots.
203 cases so far linked to Lollapalooza, out of 385,000 attendees: Chicago residents and public health experts worried that Lollapalooza, a massive music festival held in the city in late July, would become a superspreader event. Two weeks out from the festival, however, local public health officials are seeing no evidence of superspreading, with a low number of cases identified in attendees. Lollapalooza may thus be an indicator that large events can still be held safely during the Delta surge—if events are held outdoors and the vast majority of attendees are vaccinated. (Officials estimated that 90% of the Lollapalooza crowd had gotten their shots.)
This week, I wrote a story for Popular Science that goes over what we know (and don’t know) about the most common settings for COVID-19 infection.
Most of the main points will probably be familiar to CDD readers, but it’s still useful to compile this info in one concise article. Here are the main points: Outside events are always safer. Surfaces are not a common transmission source. Communal living facilities and factories tend to be hotspots. Indoor dining and similar settings carry a lot of risk. Essential workers are called essential for a reason. And don’t rule out small gatherings, even though such events are safer for those of us who’ve been vaccinated.
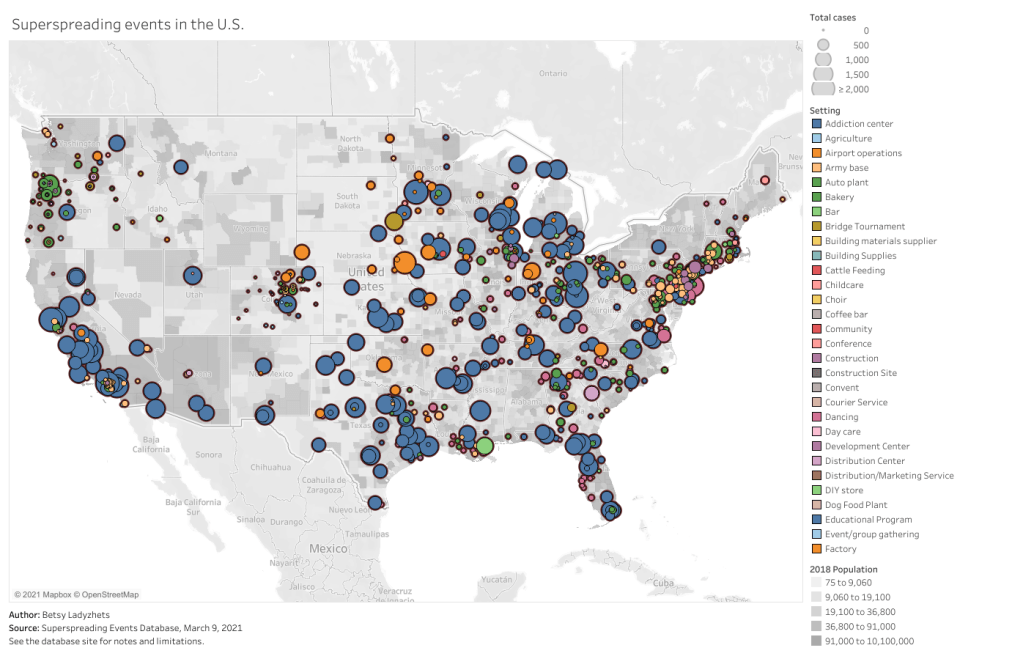
This story gave me an excuse to revisit one of my favorite COVID-19 datasets: the Superspreading Events Database, a project that compiles superspreading events from media reports, scientific papers, and public health dashboards. I interviewed Koen Swinkels, the project’s lead, for the CDD back in November.
At that time, the database had about 1,600 events; now, it includes over 2,000. All of the patterns I wrote about in November still hold true now, though. Notably, no event in the database took place solely outside (though Swinkels told me he’s seen some events with both an indoor and outdoor component). And the vast majority of events in the database took place in the U.S.
For those U.S. events, most common superspreading settings are prisons (166,000 cases), nursing homes (30,000 cases), rehabilitation/medical centers (24,000 cases), and meat processing plants (13,000 cases). By this database’s definition, a superspreading event may comprise a sustained outbreak at one location over a long period of time—and prisons have been continuous hotspots since last spring.
You can check out the U.S. superspreading events in the database below. I made this visualization in November and updated it this past week.
One of the reasons why I like the Superspreading Events Database is that Swinkels and his collaborators are extremely clear on the project’s limitations. If you load the database’s public Google sheet, you’ll see a prominent note at the top reading, “Note that the database is NOT a representative sample of superspreading events. Please read this article for more information about the limitations of the database.” The article, a post on Swinkels’ Medium blog, goes in-depth on the biases associated with the database. It’s easier to identify superspreading events in institutional settings, for example, since many of them employ frequent testing. Still, I think that—when carefully caveated—this database is an incredibly useful resource for identifying patterns in COVID-19 spread.
Swinkels additionally pointed me to another great source for exposure data: the state of Colorado publishes outbreak data in weekly reports. A few other states publish similar info, but Colorado’s data are highly detailed and complete. In this past week’s report, released on March 10, the state says that 6,900 out of a total 28,000 cases in active outbreaks are linked to state prisons. 3,900 more cases are linked to jails.
I’ve visualized the March 10 Colorado outbreak data below. As you may notice, the next-biggest outbreak setting after prisons and jails is higher education—colleges and universities represent 6,700 active outbreak cases. Colorado’s dataset does not specify how many of those cases are linked to the mask-less University of Colorado party that drew wide criticism last weekend… but we can assume that party was no small player.
Finally, this PopSci story also gave me an excuse to revisit one of my favorite COVID-19 data gripes: the lack of contact tracing info we have in the U.S. I’ve written about this issue in the CDD before; I surveyed state dashboards in October, and drew connections from the Capitol invasion in January. But it was still disheartening to find that now, in March, we continue to be largely in the dark about how many contact tracers are actively employed in most states and how many people they’re reaching.
Here’s a clip from the story:
In the US, though, the practice is done unevenly, if at all. Most states and local jurisdictions, struggling from years of underfunded public health departments leading up to the pandemic, have not been able to hire and train the contact tracers needed to keep tabs on every case.
Many states have attempted to supplement their limited contact tracing workforces with exposure notification apps, which are theoretically able to notify users when they’ve come into contact with someone who tested positive. Though these apps became more widespread in the US this past winter, they’re still not used widely enough to provide useful information. New Jersey, one state that provides data on its app use, reports that about 574,000 state residents have downloaded the app as of March 6—out of a population of 8.9 million.
This situation is not likely to improve much in the coming months as Americans aren’t about to change their perspectives on privacy any time soon. But if you have the opportunity to download an exposure notification app for your state, do it! The more data we have on where people are getting exposed to COVID-19, the better we can understand this virus.
The majority of states do not collect or report detailed information on how their residents became infected with COVID-19. This type of information would come from contact tracing, in which public health workers call up COVID-19 patients to ask about their activities and close contacts. Contact tracing has been notoriously lacking in the U.S. due to limited resources and cultural pushback.
Like everyone else, I spent Wednesday afternoon watching rioters attack the nation’s Capitol. I was horrified by the violence and the ease with which these extremists took over a seat of government, of course, but a couple of hours in, another question arose: did this coup spread COVID-19?
The rioters came to Washington D.C. from across the country. They invaded an indoor space in massive numbers. They pushed legislators, political staff, and many others to hide in small offices for hours. They inspired heated conversations. And, of course, none of them wore masks. These are all perfect conditions for what scientists call a superspreading event—a single gathering that causes a lot of infections.
My concerns were quickly echoed by many other COVID-19 scientists and journalists:
The harm caused by these domestic terrorists will not be limited to DC. They are actively committing biological warfare in what will no doubt be one of the largest superspreader events of this pandemic, and will be felt across the country.
The very next day, Apoorva Mandavilli published a story asking just this question in the New York Times. She quotes epidemiologists who point out that the event was ripe for superspreading among both rioters and Capitol Hill politicians. Many legislators were stuck together in small rooms, having arguments, while some of the Republican representatives refused to wear masks. POLITICO got a video of several Republicans refusing masks in a crowded safe room.
Punchbowl News: House lawmaker: "There's a severe covid outbreak coming among members. At the secure location yesterday at least 50 GOP members refused to wear masks. They were asked repeatedly. Older dem members pleaded. And they wouldn't do it."
By Friday, five Congressmembers had tested positive for COVID-19 in a week. It’s true, many of these legislators received vaccines in the first stage of the U.S. rollout in late December. But it takes several weeks for a vaccine to confer immunity, and we still don’t have strong evidence as to whether the Pfizer and Moderna vaccines prevent the coronavirus from spreading to other people. (They likely do, to some extent, but the evidence mainly shows that these vaccines prevent COVID-19 disease.)
Just this morning, Punchbowl News’ Jake Sherman reported that the attending physician for Congress sent a note to all legislators and staff, warning them that “people in the safe room during the riots may have been exposed to the coronavirus.” I will be carefully watching for more reports of legislators testing positive in the coming weeks. From our nation’s previous experience with COVID-19 outbreaks at the White House, it seems unlikely that the federal government will systematically track these cases—though the incoming administration may change this.
As for the rioters themselves, while the events of January 6 may well have been superspreading, we likely will never know the true extent of this day’s impact. As I’ve written previously, we identify superspreading events through contact tracing, the practice of calling up patients to quiz them on their activities and help identify others who may have gotten sick. When case numbers go up—as they are now—it becomes harder to call up every new patient. One county in Michigan is so understaffed right now, it’s telling COVID-19-positive residents to contact trace themselves.
But even if contact tracing were widely available in the communities to which those rioters are going home, can you really imagine them answering a phone call from a public health official? Much less admitting to an act of treason and risking arrest? No, these so-called patriots likely won’t even get tested in the first place.
It would take rigorous scientific study to actually tie the Capitol riot to COVID-19 spread to the homes of the rioters. (That said, if you see a study like that in the months to come: please send it my way.)
Finally, I have to acknowledge one more impact of the riot on D.C. at large: vaccine appointments were canceled after 4 PM that day. One of the most heinous aspects of that riot, to me, was how it pulled our collective attention away from the pandemic, precisely at a time when our collective health needs that attention most.