Two House Democrats called on the CDC to release more Long COVID data. This week, Rep. Ayanna Pressley (from Massachusetts) and Rep. Don Beyer (from Virginia) sent the CDC a letter insisting that the agency report estimates of Long COVID infection numbers, including demographic breakdowns by race, gender, and age. “Collecting and publishing robust, disaggregated demographic data will help us better understand this illness and ensure that we are targeting lifesaving resources to those who need them most,” said Rep. Pressley in a statement tothe Washington Post. While studies that may, theoretically, help provide such data are in the works via the National Institutes of Health’s RECOVER consortium, the consortium has yet to release any results. Long COVID continues to represent one of the biggest COVID-19 data gaps in the U.S.
We don’t know yet whether cannabis can treat COVID-19, despite promising early studies. Recent studies have shown that CBD, along with other products containing marijuana and hemp, has some capacity to block coronavirus spread in the body in lab-grown cells and in mice. The studies were quickly turned into sensationalist headlines, even though it’s too early to say whether these products could actually be used to treat COVID-19. An excellent STAT News article by Nicholas Florko and Andrew Joseph describes the studies and their limitations, as well as how these early reports of COVID-19 treatment potential are “adding to the FDA’s existing CBD headache” when it comes to regulating these products.
Have you received your free at-home rapid tests from the USPS yet? Last week, I described the federal government’s effort to distribute at-home rapid tests to Americans free of charge, along with the equity issues that have come with this initiative so far. This week, I saw some reports on social media indicating that people have started receiving their tests! Have you gotten your tests yet? If you have, I would love to hear from you—in absence of formal data from the USPS, maybe we can do some informal data collection on test shipping times within the COVID-19 Data Dispatch community.
CDC dashboard adds booster shots to key pages: This week, the CDC added booster shot status to its COVID-19 dashboard page detailing the rates of lab-confirmed COVID-19 hospitalizations by vaccination status. According to the new chart (at the bottom of this page), in December, hospitalization rates were 49 times higher in unvaccinated adults over age 65 than in fully vaccinated and boosted adults in that age group. The CDC also added booster shot status to its COVID-19 Vaccination Equity page, with a chart showing booster shot rates according to race and ethnicity. Unsurprisingly, white and Asian Americans have the highest booster rates.
KFF: How Are Private Insurers Covering At-Home Rapid COVID Tests? A new report from the Kaiser Family Foundation compares rapid at-home test reimbursement policies for 13 major private insurers, as of mid-January 2022. According to the report, six insurers are currently offering direct coverage (meaning users don’t need to pay out of pocket for the tests), while seven offer reimbursement online, by mail, or by fax.
QCovid® risk calculator: This tool, commissioned by England’s Chief Medical Officer for use in the U.K. national healthcare system, helps potential COVID-19 patients estimate their risk for severe symptoms. The tool is meant for use by doctors and other medical professionals who are actively evaluating patients, but the website allows anyone to go through the risk questionnaire and see their status. (You just can’t use the results for anything beyond gaining information.)
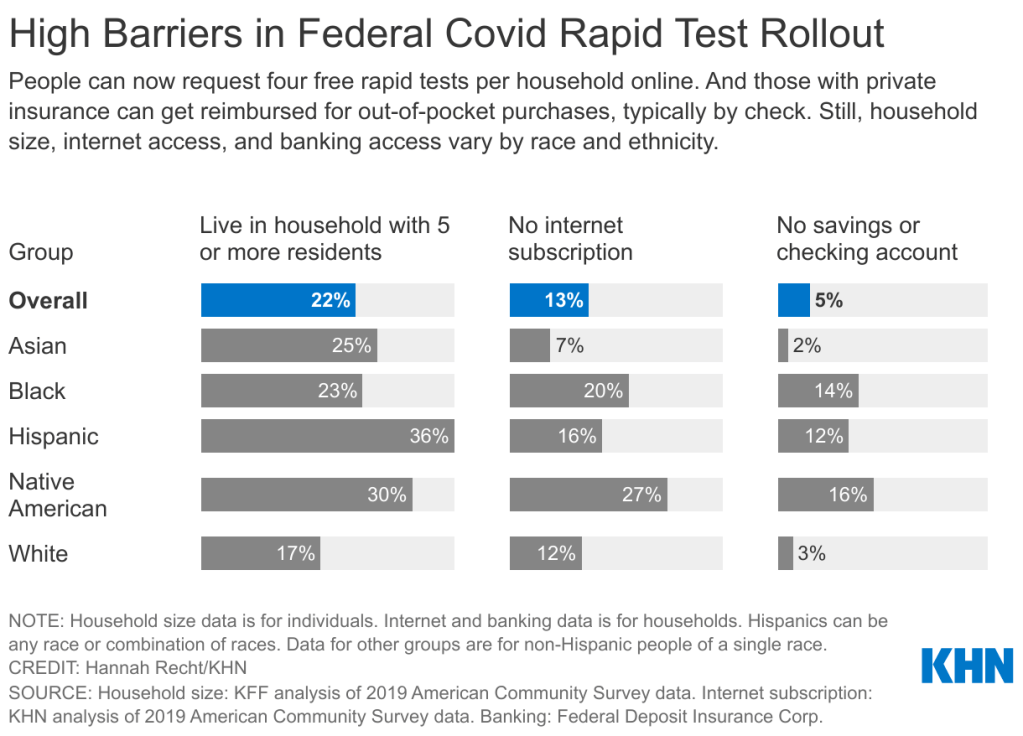
The federal government’s policies aimed at helping Americans get free rapid tests are insufficient for many households including people of color. Graphic via KHN.
On Tuesday, the site went live early in “beta test” form before its formal launch on Wednesday. Within hours of it going live, public health experts were already raising equity concerns about the free test distribution program. To address these concerns, the federal government should release data on where the free tests go—including breakdowns by state, county, ZIP code, race and ethnicity, the tests’ delivery dates, and more.
As the link to the testing order site was shared widely on social media, one thing quickly became clear: people who lived in high-density settings were at a disadvantage. Americans in traditional apartment buildings, houses split into multiple living spaces, dormitories, and other multi-unit dwellings attempted to order tests—only to get an error message stating someone at their address had ordered tests already.
The USPS ordering page is set up to allow just one test order per address, to prevent people from abusing the free test program. But, despite having literally every address in the U.S. on file, the USPS apparently failed to account for many apartment buildings. Some apartment-dwellers were able to get around this issue by placing their apartment number on the first address line, removing “Apt” from the address, or otherwise adjusting how they filled out the form, but these tricks didn’t work for everyone.
I myself ordered the free tests before I learned about these issues on Twitter; I later sheepishly texted the groupchat for my Brooklyn, seven-unit apartment building, preemptively apologizing in case I’d fucked up my neighbors’ chances of obtaining free tests. (Luckily, my building seemed to be unaffected by the USPS issue—one of my neighbors responded saying that she was able to order the tests without a problem.)
Still, a “small percentage of orders” could add up to millions of people living in multi-unit housing who were unable to obtain free tests, or would have to share just four tests among an apartment building’s worth of residents. Without more precise data, it’s hard to understand the scope of this problem.
All the Twitter discourse about apartment buildings obscures another group that shouldn’t have to share a small number of tests among many people: large households. The USPS is sending just four tests in each order—not four testing kits, four individual tests. That’s not enough for a family of four to test themselves according to FDA recommendations (i.e. twice within two days) after a potential exposure; it’s certainly not enough for large families including five or more people.
And minority communities are more likely to include such large households. According to a Kaiser Family Foundation analysis of Census data: “More than a third of Hispanic Americans plus about a quarter of Asian and Black Americans live in households with at least five residents…Only 17% of white Americans live in these larger groups.”
Households in West coast states are also more likely to include five or more residents, according to a similar analysis from the University of North Carolina Chapel Hill’s Carolina Demography center. States with the highest shares of five or more resident households are: Utah (18.8%), California (13.7%), Hawaii (13.5%), Idaho (13.2%), and Alaska (12.9%). On the other hand, in some East coast states, under 7% of households include five or more residents.
!function(){“use strict”;window.addEventListener(“message”,(function(e){if(void 0!==e.data[“datawrapper-height”]){var t=document.querySelectorAll(“iframe”);for(var a in e.data[“datawrapper-height”])for(var r=0;r<t.length;r++){if(t[r].contentWindow===e.source)t[r].style.height=e.data["datawrapper-height"][a]+"px"}}}))}();
The USPS test distribution system also gave an advantage to Americans with internet access. At one point on Tuesday afternoon, the USPS order site was drawing more than half of all government website traffic, demonstrating its popularity with internet users—while people without internet were not yet able to order tests.
As of Friday, those without internet access can order the free tests over the phone, at 1-800-232-0233. This phone line is open daily from 8 AM to midnight Eastern Time, according to NPR, and Americans can order in over 150 languages. The USPS website itself is available in English, Spanish, and Chinese.
While this phone line is very helpful now, the delay between the website’s release (on Tuesday) and the phone line’s release (on Friday) means that Americans without internet may be behind in the queue for actually receiving their tests. Already, the federal government has said that people who ordered their tests may need to wait for weeks to receive their tests.
Of course, as analysis from KHN has shown, Americans of color are less likely to have internet access than their white neighbors. 27% of Native Americans, 20% of Black Americans, and 16% of Hispanic Americans have no internet subscription, compared to 12% of white Americans.
Finally, the USPS test distribution system leaves out one major group of vulnerable Americans: those who don’t have an address at all. Homeless people are particularly vulnerable to COVID-19: many outbreaks have occurred in shelters, and many of these people have health conditions that increase their risk of severe symptoms. The impact of COVID-19 among homeless Americans is not well understood due to a lack of data collection; still, we know enough to indicate free tests should be a priority for this group.
The White House has said that equity will be a priority for the free rapid test rollout: each day, 20% of test shipments will go to people who live in highly vulnerable communities, as determined by the CDC’s Social Vulnerability Index. This index ranks ZIP codes according to the communities’ ability to recover from adverse health events, based on a number of social, environmental, and economic factors.
This priority is nice to hear. But without data on the test rollout, it’ll be difficult to evaluate how well the federal government is living up to its promise of equitable test distribution. I’d like to see data on the free test distribution that goes to the same level of detail as the data on our vaccine distribution, if not even more granular.
The data could include: tests distributed by state, county, and ZIP code; tests distributed to ZIP codes that rank highly on the Social Vulnerability Index; tests distributed by race, ethnicity, age, gender, and household size; dates that tests were ordered and delivered; tests delivered to single- and multi-unit buildings; and more.
Unlike other COVID-19 metrics that are difficult to collect and report at the federal level, the federal government literally has all of this information already—they’re collecting the address of every person that orders tests! There is no excuse for the government not to make these data public.
In short: USPS, where is your free rapid test distribution dashboard? I’m waiting.
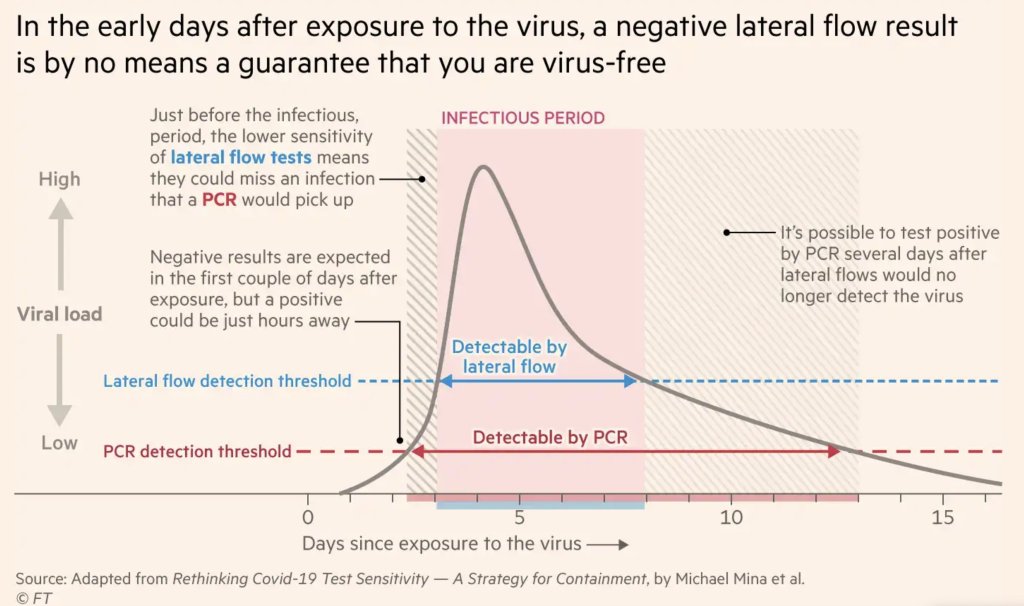
After exposure to the coronavirus, someone may test negative on rapid antigen tests for multiple days before their viral load becomes high enough for such a test to detect their infection. Chart by Michael Mina, adapted by the Financial Times.
As Omicron spreads rapidly through the U.S., this variant is driving record case numbers—and record demand for testing, including both PCR and rapid at-home tests. In other words, it feels harder than ever to get tested for COVID-19, largely because more people currently need a test due to recent exposure to the virus than at any other time during the pandemic.
Also this week, the CDC changed its guidance for people infected with the coronavirus: rather than isolating for 10 days after a positive test, Americans are now advised to isolate for only five days, if they are asymptomatic. Then, for the following five days, people should wear a mask in all public settings. This guidance change has prompted further discussion (and general confusion) about who needs to get tested for COVID-19, when, and how.
Here’s a brief FAQ, to help navigate this complicated testing-and-isolation landscape. In addition to the CDC guidance, it’s inspired by a recent question from a reader about testing and isolation following a positive PCR result in her family.
What’s the difference between being infected and being contagious?
As we think about interpreting COVID-19 test results in the Omicron era, it’s key to distinguish between being infected with the coronavirus and being actively contagious.
Infected: The virus is present in your body.
Contagious: The virus is present in your body at high enough levels that you can potentially spread it to other people.
In a typical coronavirus infection, it takes a couple of days after you encounter the virus—i.e. breathe the same air as someone who was contagious—for the coronavirus to build up enough presence in your body that tests can begin detecting it. PCR tests can typically detect the virus within one to three days after an infection begins, while rapid tests may take longer.
How do you use testing to tell if you’re infected and/or contagious?
Timing is extremely important with coronavirus tests, and has become even more so with Omicron. If you learn about a recent exposure to the virus, you don’t want to get tested immediately after that exposure, since the test would not pick up a potential infection yet. Say you had dinner with a friend on Wednesday, and they tell you on Thursday that they just tested positive; you should wait until Friday or Saturday to get tested with PCR, or until Saturday or Sunday to get tested with a rapid at-home test. (And ideally, you would avoid interacting with other people while you wait to get tested.)
PCR tests can detect the virus within a couple of days of infection. Rapid tests, which are less precise, generally can’t detect the virus until it’s at high enough levels for someone to be contagious. This can take time—though Omicron may have shortened the window between infection and becoming contagious to just three days, according to some early studies. A new CDC study released this week provides additional evidence here.
This chart, an adaptation of a figure by rapid test expert Michael Mina published in the Financial Times, shows how someone could potentially test negative on rapid tests for multiple days after a coronavirus exposure, even though they are infected:
When this person tests positive on a rapid test, the result indicates that they’ve become contagious with the virus. Then, it’s possible that the person may continue testing positive on PCR tests after they stop testing positive with antigen tests, because they are no longer contagious but continue to carry enough virus genetic material that a PCR test can pick it up.
How do you get ahold of rapid tests, in the first place?
In order to use rapid tests to tell whether you’re contagious with the coronavirus, you need to get some rapid tests! Here are a couple of suggestions:
Order online from Walmart: If you look at this website right now, Walmart will probably say that Abbott BinaxNOW rapid tests are out of stock. But if you leave the page open and refresh often, you may be able to snag some rapid tests right after Walmart restocks (which happens roughly once a day, I think). I like ordering from Walmart because they’re cheaper than other BinaxNOW vendors and ship quickly, usually within a week.
Order online from iHealth Labs: iHealth Labs is one rapid test manufacturer that’s grown in popularity recently, as an alternative to BinaxNOW. You can order up to 10 packs (with two tests each) directly from the manufacturer, and report test results in an app. In my experience, though, iHealth Labs is slower to ship than other distributors; an order I placed on December 22 is due to arrive two weeks later, on January 5.
Use NowInStock to see availability: This website tracks rapid test availability at a number of websites, including CVS, Walgreens, Walmart, Amazon, and others. It’s helpful to see your options for a number of different tests, but bear in mind that tests sold by third-party vendors (like Amazon) may be less reliable than those sold directly by pharmacies.
Follow local news: A lot of city and state governments have recently started making rapid tests available to the public for free, from D.C. libraries to Connecticut towns. I recommend keeping an eye on local news and government websites in your area to look for similar initiatives—or, if your area isn’t making rapid tests available, call your local representative and ask that they do!
Why did the CDC change its guidance for isolation?
As I mentioned above, the CDC recently changed its guidance for people who test positive for the coronavirus. If someone has no symptoms five days after their positive test result, they can stop isolating from others—but they need to wear a mask in all public settings.
According to the CDC, the new guidance is “motivated by science demonstrating that the majority of SARS-CoV-2 transmission occurs early in the course of illness, generally in the 1-2 days prior to onset of symptoms and the 2-3 days after.” In other words, the CDC is saying that people are generally contagious for a few days after their symptoms start. After that, they’re less likely to infect others, so isolation may be less necessary—and good mask-wearing may be sufficient to prevent further coronavirus spread.
Many experts are attributing the guidance chance to economic needs: as Omicron causes flight cancellations, closed restaurants, and other business disruptions, a shorter isolation period can help people get back to work more quickly. The recent isolation change follows a similar guidance change the previous week, which said healthcare workers could shorten their isolation periods if their facilities were experiencing staffing shortages.
Generally, it does seem that most people—particularly vaccinated people—are no longer contagious five days after their symptoms start. (Reminder: five days after symptoms start could be seven to nine days into the infection period, since it takes time for the virus to build up in your body and cause symptoms.) But this is by no means guaranteed for everyone, as each person infected with the coronavirus has a unique COVID-19 experience.
As a result, many experts have said that the CDC should have required negative rapid tests for people to leave isolation after five days. A negative rapid test would indicate that someone is no longer contagious, the argument goes, and they can then go back into the world. In the U.K., two negative rapid test results are required to shorten isolation from ten to seven days.
CDC’s new guidance to drop isolation of positives to 5 days without a negative test is reckless
Some ppl stay infectious 3 days,Some 12
I absolutely don’t want to sit next to someone who turned Pos 5 days ago and hasnt tested Neg
However, for everyone in the U.S. to be able to rapid test out of isolation, the country would need a far greater supply of those tests than we currently have available. This Twitter thread, by epidemiologist Matt Ferrari, explains the challenges posed by limited rapid testing:
There’s a lot to unpack here. One thing I’ve heard from clinicians throughout the pandemic is “don’t order at test you won’t act on”. Here that is married with “don’t order a test that you can’t offer”. There is a lot here that makes sense to me, even if I’m not 100% on board 1/ pic.twitter.com/wE5w32dQKj
— The Ferrari Lab: @TheFerrariLab.bsky.social (@TheFerrariLab) December 30, 2021
Ferrari argues that the CDC guidance makes sense, given the information and resources currently available in the U.S., as well as the fact that simpler rules are easier to follow. Still, I personally would say that, if you have the rapid tests available to test out of isolation, you should.
This past Monday, President Biden gave a speech about the Omicron variant. He told America that Omicron is “cause for concern, not a cause for panic,” and thanked the South African scientists who alerted the world to this variant. (Though a travel ban is not a great way to thank those scientists!)
Towards the end of the speech, he said: “We’re throwing everything we can at this virus, tracking it from every angle.” Which I, personally, found laughable. As I’ve pointed out in a previous post about booster shots, the U.S.’s anti-COVID strategy basically revolves around vaccines, and has for most of 2021.
wild to hear Biden say "we are throwing everything we can at this virus" … like, sir, no we aren't. we are throwing ONE THING (vaccines) at this virus.
My Tweet about Biden’s vaccine-only strategy got more attention than I’m used to receiving on the platform, so I thought it was a worthwhile topic to expand upon in the COVID-19 Data Dispatch. Why aren’t vaccines enough to address Omicron—or our current surge, for that matter—and what else could the Biden administration be doing to slow the coronavirus’ spread?
Why aren’t vaccines enough?
Prior to Delta’s spread, there was some talk of reaching herd immunity: perhaps if 70% or 80% of Americans got fully vaccinated, it would be sufficient to tamp down on the coronavirus. But Delta’s increased capacity to spread quickly, combined with the vaccines’ decreased capacity to protect against infection and transmission, have shown that vaccines are not enough to eradicate the virus.
Here, then, is the current pandemic dilemma: Vaccines remain the best way for individuals to protect themselves, but societies cannot treat vaccines as their only defense. And for now, unvaccinated pockets are still large enough to sustain Delta surges, which can overwhelm hospitals, shut down schools, and create more chances for even worse variants to emerge. To prevent those outcomes, “we need to take advantage of every single tool we have at our disposal,” [Shweta Bansal of Georgetown University] said. These should include better ventilation to reduce the spread of the virus, rapid tests to catch early infections, and forms of social support such as paid sick leave, eviction moratoriums, and free isolation sites that allow infected people to stay away from others.
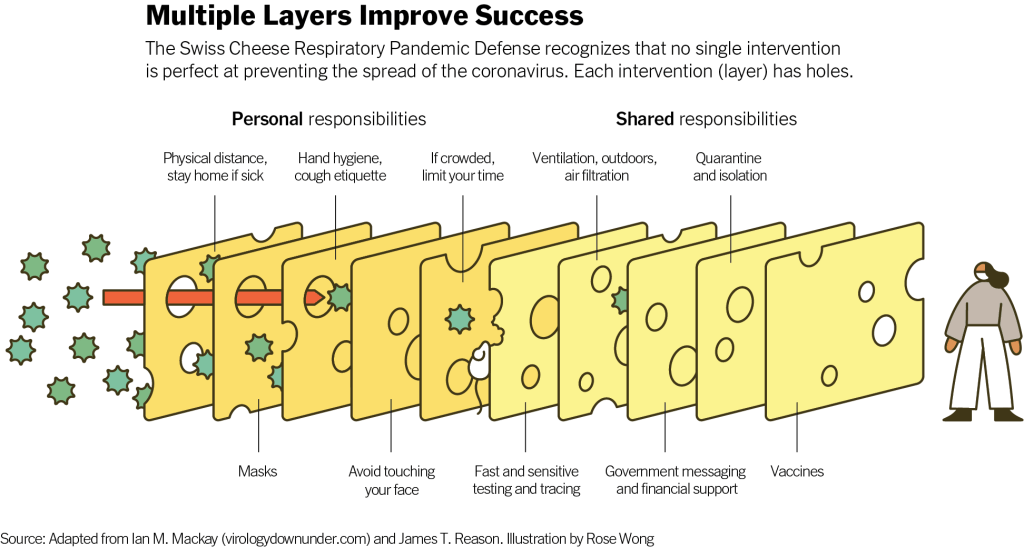
Remember that Swiss cheese model of pandemic interventions? Vaccines may be the best protection we have against the coronavirus, but they’re still just one layer of protection. All the other layers—masks, testing, ventilation, etc.—are still necessary, too. Especially when we’re dealing with a new variant that might not respond as well to our vaccines.
Re-upping this brilliant image from last year as a reminder on how mitigation measures work together to prevent the spread of coronavirus. pic.twitter.com/p7Z8u7fS2w
One strategy that we could employ against Omicron, as well as against the current Delta surge, is better masks. While cloth masks certainly make it less likely for the coronavirus to spread from one person to another, their efficacy varies greatly depending on the type of material, the number of layers, and the mask’s fit.
N95 masks do the best job at stopping the coronavirus from spreading, followed by KN95 masks. Surgical masks do a better job than cloth masks, but making sure these masks fit properly can be a challenge for some people (including yours truly, who has a very narrow face!). Layering a surgical mask and cloth mask may be a safer option to get both good fit and protection, though two layers of mask can be challenging to wear for long periods of time.
Some experts have recommended that the U.S. mail N95 or KN95 masks to all Americans, or at least require these masks in high-risk areas, such as on flights. Germany and other European countries established similar requirements last summer.
Given how transmissible Delta is—and the likelihood that Omicron is also highly transmissible—consider upgrading to an N95/KN95 mask or equivalent when indoors and around others, especially if you're elderly or immunocompromised.
In many countries—including the U.K., Germany, India, and others—rapid tests are freely available. Here in the U.S., on the other hand, the tests are quite expensive (often upwards of $10 for one test) and difficult to find, with pharmacies often limiting the number of packages that people can buy at once.
Biden has attempted to increase rapid testing access as part of his latest COVID-19 plan: in January, private insurance companies will be required to cover the cost of rapid tests. But this doesn’t solve the supply issue, and it doesn’t really make the tests more accessible, either. The measure would still require people to buy tests out of pocket, then fill out insurance reimbursement forms to maybe get their money back. Can you imagine anyone actually doing this?
In addition, as some experts have pointed out, the people most likely to need rapid tests—essential workers and others in high-risk environments—are also those less likely to have insurance. Biden is also distributing some rapid tests to community health centers, but that’s not enough to meet the need here.
This part of Biden’s omicron plan is also short-sighted.
Sure reimbursement by private health insurance of rapid test costs is a nice thing to have, but the people who MOST need rapid tests are the same people who DONT have private health care. What’s the plan for helping them? pic.twitter.com/tnlC8T0PDk
Ideally, the Biden administration would mail every American a pack of, like, 20 rapid tests, along with that pack of N95 or KN95 masks I mentioned above. Free of charge.
And at the same time, of course, we need more readily available PCR testing. Even in New York City, which has a better testing infrastructure than most other parts of the country, the lines at free testing sites are getting long again as cases go up. Any American who wants to get tested should be able to easily make an appointment within a day or two, and get their results within another day after that.
Increased testing is not only important for identifying Omicron cases (and cases of any other new variant); it’s also key for the Merck and Pfizer antiviral treatments due to be approved in the U.S. soon. Without efficient testing, patients won’t be able to start these treatments within days of their symptoms starting.
What we could do: improve genetic surveillance
The U.S. is doing a lot more coronavirus sequencing than we were in early 2021: we’ve gone from under 5,000 cases sequenced a week to over 80,000. The CDC worked with state and local health agencies, as well as research organizations and private companies, to increase sequencing capacity across the country.
Urban centers close to large academic centers tend to be well covered, while rural areas are less so. That means public health departments in large parts of the country are still flying blind, even as they are figuring out ways to prioritize Omicron-suspicious samples.
A lack of testing compounds this problem. If someone doesn’t confirm their COVID-19 case with a PCR test, their genetic information will never make it to a testing lab, much less a sequencing lab. While rapid tests are very useful for quickly finding out if you’re infected with the coronavirus, you need a PCR test for your information to actually be entered into the public health system.
In addition, even where the U.S. is sequencing a lot of samples, the process can take weeks. Vox’s Umair Irfan writes:
Still, it takes the US a median time of 28 days to sequence these genomes and upload the results to international databases. Contrast that with the United Kingdom, which sequences 112 genomes per 1,000 cases, taking a median of 10 days to deposit their results. A delay of only a few days in detection can give variants time to silently spread within communities and across borders.
Despite sequencing shortfalls in the U.S., we’re still doing much more surveillance than the majority of countries. Many nations in Africa, Asia, South America, and other parts of the world are sequencing fewer than 10 cases per 1,000, Irfan reports. As the U.S. should be doing more to get the world vaccinated, the U.S. should also do more to help other countries increase their sequencing capacity—monitoring for the variants that will inevitably follow Omicron.
What we could do: stricter domestic travel requirements
Starting on Monday, all international travelers coming into the U.S. by air will need to show a negative COVID-19 test, taken no more than one day before their flight. This includes all travelers regardless of nationality or vaccination status. At the same time, any non-U.S. citizens traveling into the country must provide proof of their vaccination against COVID-19.
But travelers flying domestically don’t face any such requirements. There are mask mandates on airplanes, true, but people can wear cloth masks, often pulled down below their noses, and airports tend to have limited enforcement of any mask rules.
Both experts and polls have supported requiring vaccination for domestic air travel, though the Biden administration seems very hesitant to put this requirement in place. Speaking for myself, I felt very unsafe the last time I flew domestically. A vaccine mandate for air travel would make me much more likely to fly again.
What we could do: more social support
In the U.S., a positive COVID-19 test usually means that you’re in isolation for 10 to 14 days, along with everyone else in your household. This can pull kids out of school, and pull income from families. As has been the case throughout the pandemic, support is needed for people who test positive, whether that’s a safe place to isolate for two weeks, grocery delivery, or rapid tests for the rest of the household.
This type of support could make people actually want to get tested when they have symptoms or an exposure risk, rather than avoiding the public health system entirely.
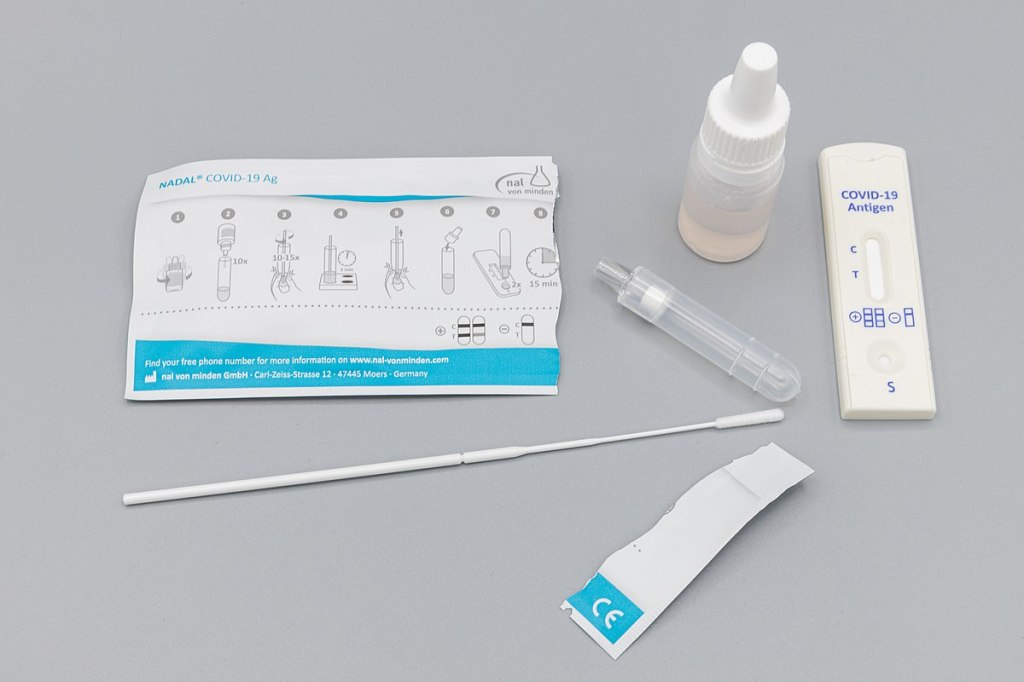
Two Abbott BinaxNOW antigen tests used by Betsy and her sister during their trip, demonstrating single-line negative results.
As I mentioned in last week’s newsletter, I went on vacation during the last week of August. I traveled to California to visit my younger sister, who was living there over the summer for an internship. We spent a couple of days in the Bay Area, then drove to Southern California, hit a few different destinations, and finally flew out of Los Angeles International Airport (LAX).
Both my sister and I are fully vaccinated, of course, but we still took a number of precautions to make our trip as safe as possible in light of the current COVID-19 surge. I wanted to share what we did in case it’s useful for others thinking about travel right now.
Key precautions included:
Limited exposure and tests before traveling: For ten days before my flight out to California, I avoided all unmasked indoor activities, including small gatherings with fully vaccinated friends. Closer to my flight, I also avoided other activities outside my home (grocery shopping, taking the subway, and the like). I got a PCR test at a NYC Health site two days before my flight, and didn’t leave my apartment between that test and heading out to the airport.
Rapid testing every two days during the trip: I carried three packs’ worth of Abbott BinaxNOW rapid antigen tests in my suitcase, and bought a couple more packs in California. Starting two days after I arrived, my sister and I tested ourselves every other day. While antigen tests like these are more likely to give you a false negative than PCR tests, testing frequently increases your chances of catching a case—and catching it early in your disease progression, when you’re most likely to infect others. The tests were easy to incorporate into our routines, especially once we got used to the swabbing process.
Sticking to outdoor activities: Our trip included a lot of outside time: hiking in a redwood forest, hitting up Southern California beaches, camping for a night at Joshua Tree National Park, and lots of outdoor dining. The riskiest two activities of the week, we agreed, were an afternoon at Monterey Bay Aquarium and a day at Universal Studios in LA. But both of those establishments did a great job of reminding all patrons (including the vaccinated) to keep their masks on inside—following current mask regulations in the Bay Area and LA County.
Double-masking indoors: On both my flights and whenever I needed to be inside for a longer period of time, I wore two masks: a surgical mask and a fitted, multi-layer cloth mask. Studies suggest that cloth masks on their own are not the best option for protecting against Delta, but layering a cloth and surgical mask can increase protection. I especially like to layer masks because surgical masks typically don’t fit well on my face; when I add a cloth mask on top, the fit becomes much more snug.
Precautions when visiting relatives: My sister and I visited a few relatives over the course of our trip. For these visits, we basically followed the precautions that health experts recommended last Thanksgiving: eat outside whenever possible, mask up in common areas inside, open windows for extra ventilation, etc. We also organized the trip so that no visits occurred after Universal Studios, which we had deemed the riskiest activity of the week.
Extra testing after traveling: Flying out of LAX proved to be incredibly stressful, as neither the airport nor our airline put in effort to enforce mask guidance. My sister and I even gave extra masks to two fellow travelers at the check-in desk, because the airline apparently did not have any extras available. Because of this extra COVID-19 exposure risk, I did some extra testing upon my return to the East coast: daily rapid tests for two days in a row, followed by a PCR test.
hi @JetBlue! your mask availability and enforcement is apparently so bad that my sister and I had to literally GIVE TWO OF OUR OWN EXTRA MASKS to fellow travelers at the (very crowded) LAX check-in desk. this is extremely irresponsible in the face of the current covid surge.
Personally, this will probably be my last major trip for a while. Conferences that I’d planned to attend in the fall have been moved to all-virtual formats, and I’m lucky to live close enough to my parents that I don’t need a flight to see them for the holidays. If I were to travel again, though, I’d likely follow these same precautions—with adjustments based on COVID-19 infection rates at my destination. Also, I would probably avoid LAX.
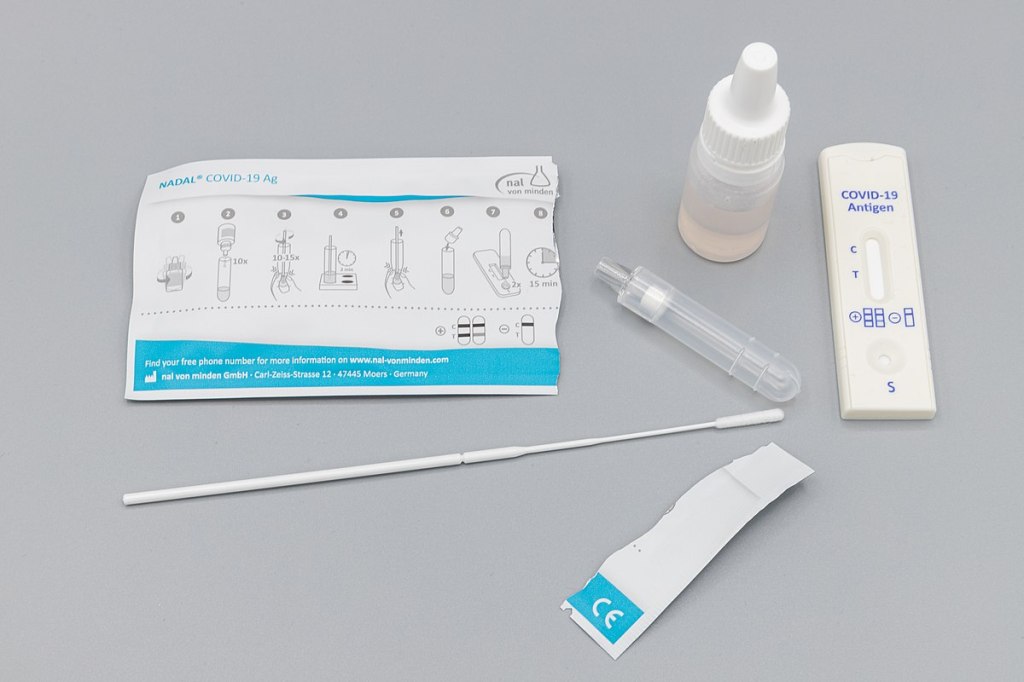
Antigen test kit image via Dronepicr // Wikimedia Commons.
This week, I had a story on COVID-19 testing published in Slate’s Future Tense vertical. The piece explores how testing will change in the next few months as more Americans become vaccinated and rapid tests become more widely available, with a practical focus: how should you interpret the test numbers on your local COVID-19 dashboard?
Overall, I found, we will need to keep getting tested even post-vaccination. But the purpose of testing may shift, for many of us in the U.S., from diagnostic testing—a test to figure out if you are currently sick with COVID-19—to more screening and surveillance testing—tests to identify case trends and stomp out outbreaks in a broader community. This shift may be aided by the rise of rapid, at-home tests, which are becoming much more widely available thanks to investment from the federal government. Just this week, USA Today reported that at-home tests will soon be sold at national pharmacies CVS, Walgreens, and Walmart.
In the CDD today, I’m excited to share one of the interviews I conducted for the piece, with Dan Larremore, a statistician at the University of Colorado and long-time advocate for the potential of rapid tests. We talked on April 2, just days after two major developments in the testing space: the FDA gave Emergency Use Authorization to several rapid tests for over-the-counter use, and the CDC and NIH announced a massive study to investigate how well these tests work for population-level screening. (One more piece of context: when we talked, case numbers were rising at a more concerning rate than they are now.)
Larremore and I talked about his reaction to the rapid test news, how to interpret testing numbers, other new test types that may come on the market, and more.
The interview below has been lightly edited and condensed for clarity.
Betsy Ladyzhets: First question is, since a lot of this piece is meant to be about the numbers of testing, what would you consider the most useful metric or metrics right now to how successful testing is, whether that’s test positivity or other things?
Dan Larremore: I think about testing for three different reasons. One reason is information about the trajectory of the pandemic, which is things like test positivity rates, number of new cases. We test to kind-of get our bearings in the movement of the pandemic. The second reason that we test is more at the individual level, but it’s still that [same] information. And that is, I would test because I want to know, am I sick? Might I give the disease to somebody else? Or, can my current symptoms be explained by being infected? So the first two are informational.
The third reason that we might test is specifically just to break transmission chains, which is more like testing as an answer, not as a question. And so, for at-home testing, for serial testing, for the regular kind of testing that we have to do to be on campus here [at the University of Colorado]… To me, that’s much more about an intervention to slow down transmission than it is about gaining information.
So, that’s a roundabout way of answering your question. But I think, in terms of what numbers to look at, it really matters what the intention of the testing is. So if people continue to take the pandemic seriously, and continue to, like, get tested regularly, or get tested when they feel sick, then those sort of daily case numbers will remain useful and interesting. And therefore the test positivity rate information will continue to tell us something about the trajectory of the pandemic. Does that answer your question?
BL: Yeah, I think that does answer my question. Because I think that was one of the big kind of questions I had going into this story is like, is test positivity still useful if maybe, as people get vaccinated, they stopped thinking they need to get tested or as other dynamics change. But yeah, I had another person who I’ve interviewed for this story also had kind of a hierarchy description [of testing], so that definitely is a useful thing to think about.
DL: Knowing why people come in to get tested just gives you so much more interpretability of like, what the numbers mean. Here on campus, if I want to be here on campus, I need to get tested weekly. I’ve been vaccinated, one dose, dose number two soon. But nevertheless, I still need to spit in the tube every week, and they test it. So, the test positivity rates here on campus are minuscule. Because with high compliance, everybody gets tested, so the denominator in that positivity rate is huge. At a drive up site, or at a doctor’s office, where people are coming in because they feel sick, the test positivity rates are going to be a lot higher.
And I think, as people get more and more vaccinated—regardless of the case counts—as the pandemic feels like it’s winding down, I think people may be less likely to get tested. And so you can imagine test positivity rate being driven by, not just what the virus is doing, but a lot of the human behavior as well… I guess, the way that you can put it is, that you can see changes in the test positivity that are driven entirely by human behavior with respect to getting tested at all. And not so much about changes in the virus.
BL: That makes sense. And I think it’s also about access, right? Are people able to go and get tested if they feel sick? Or if you’re thinking about schools and workplaces, is their employer having everyone get tested once a week? Is that something we’re going to see more of now that we have—like, literally earlier this week, the FDA gave EUA to a bunch of antigen tests, right?
DL: Yeah, for at-home use.
BL: Right. Do you think we’re gonna finally see that massive use of rapid tests that experts have wanted to see since, like, the summer?
DL: A lot of people, myself included, have been excited about the possibility of at-home repeated antigen testing, as a way to really take community transmission levels and push them down. Because we know that asymptomatic transmission occurs, we know that getting people results rapidly is absolutely critical. Because four-day-old information is totally useless if you have infected people in those four days.
I don’t know how useful those test kits are going to be right away, like, right now, given that we just now have an EUA for that kind of at home use that we’ve been hoping for for a long time. But at the same time, cases are shooting up due to these new variants around the U.S. and more importantly, around the world. So, I think these tools are still going to be useful, especially this fall, as we get a lot more kids in school. And we start bringing people together, temperatures starting to cool off, more people are indoors. I think that having the rapid test as a screening tool will still be valuable, particularly if we see limited uptake of the vaccine.
BL: That makes sense… Another question around rapid tests is, that I know in the U.S., it’s really hard to get comprehensive data on them. I volunteered at the COVID Tracking Project, and I wrote [a blog post] about the problem of antigen test data. So I was curious as to how we will know how well the tests are working. And if there are any specific studies that you’re watching or data sources that you recommend, in terms of, like, knowing if people are actually using these at home tests.
DL: I am excited about… On the 30th, there was a press release about the NIH and CDC rolling out at-home testing to two cities.
BL: I saw that, yeah!
DL: The work that Michael Mina and I did last year was showing that, at the individual level, the trade off between test sensitivity and turnaround time, should really tell us that turnaround time is critical. Like, theoretically, at the individual person level, the rapid test idea is really, really good. What we’ve not yet seen—outside of Slovakia—is the ability to flood the zone with tests, as Fauci put it, and just catch as many positives as possible and drive the epi curve downward, just because of the rapid tests.
My feeling is that, really, the proof is in the pudding. If people can, at a community level, use a boatload of rapid tests regularly for a few weeks, and we can watch the new cases spike as we find those positives and then crash as we break all the transmission chains. That’s the key thing. That’s the key thing that I’m looking out for in these new trials.
The Slovakia folks showed some of the limitations of this [strategy]. There’s a paper in Science where they wrote up their results. And basically what they found was the rapid testing worked really well, but the problem was on the isolation side. [Not everyone who tests positive can truly and effectively isolate.] In the short term, while they still had the supplies, these three waves of everybody in the country getting tested, worked like they were supposed to work, worked like the theory said. However, once you stop testing, you take your foot off the brakes, things re-accelerate. The second thing is that a lot of folks in particularly rural areas were like, okay, well, I’m positive, but I live with my family. How am I going to isolate? So unlike on a college campus here, where when somebody tests positive, we have a separate dorm set up for them for two weeks—in real life, that isolation stuff is going to be harder.
BL: So it’s kind-of like, you need to pair it with the social services aspect, or some other way to help people out. I know, in New York, there’s a hotel room program, where if you test positive, you can contact the City Department of Health, and they’ll like, put you up in a hotel for two weeks. I don’t know how much it gets used, but it definitely seems like something that should be around in more places.
DL: I mean, even if it’s just supporting people, by telling them like, this is gonna be awkward, but wear your mask at home, and don’t hang out with your family. Go watch TV in the basement, or, you know, otherwise keep distance from people. Whatever these interventions are, they can help. And we know that what we call the secondary attack rate is actually not that high. So, even among people who live in the same household, even among spouses, if one person is sick, that doesn’t mean that the other person definitely gets it. It’s only [around 20%] chance that they do. We looked at pairs of roommates here on campus, and studied [transmission between] them. And even among roommates, the secondary attack rate is not that high [20-28%].
BL: Well, that brings me to another question I wanted to ask you, which is how public health communication around testing either is changing or should be changing in order to express like, okay, maybe you’ve been vaccinated, but you still need to get tested, or what needs to be communicated about these at home tests, or any other messages that you think are important to be conveying.
DL: One thing that’s important is that we know that we need to keep our eye on the variants. And evidence is emerging… that there are some breakthrough variants, they are less well handled by the vaccine, even though the vaccine works really well… So, testing is going to remain important, even as, more broadly, the vaccine protects people from the most severe disease.
We’re seeing a really interesting split right now, right? Where like, cases are going up, and we expect hospitalizations to then go up, and then mortality to go up. But I wonder if we’re gonna see that in the U.S. this time. Like, week on week, mortality continues to go down. And the question is, are we gonna get it again?
BL: Is it gonna go up again?
DL: Or did we vaccinate enough of the high-risk people that the mortality stays flat even while cases go up?
BL: I definitely think there’s going to be kind-of a demographic aspect of it. Like,I’ve seen charts where people do, with the HHS hospitalization data, they publish it by age. So, you can see that hospitalizations are going way up in people ages, like, 18 to 30, but not so much in seniors. Although, kind-of tangentially, one data gap that I get annoyed by is that there’s very little demographic data for testing. Like, if you look at race data, for example, there are maybe five states that publish testing data by race and ethnicity. And there’s not a lot of it by age. So it’s kind-of hard to track patterns there.
DL: I mean, I don’t know what the right messaging is around testing, other than, [if you feel like you’re sick], if you have the symptoms, you’ve got to go get tested. It doesn’t matter if you’re vaccinated or not. If you feel sick, you should go get tested. If you are going to be around somebody who you know is really vulnerable, if testing is available, go get tested.
I still think it’s a valuable intervention, especially in places where vaccine uptake is low or vaccine availability is low. But I think the question is, like, really, how long is—what’s the expiration date on recommendations about testing? If 70% of the US is vaccinated by July, let’s say, does it still make sense to recommend a huge amount of testing? And I don’t know the answer to that. What I would like to see is people equipped for this fall, if there are spikes in cases, or if there are variants that are circulating even among vaccinated people, it would be amazing if, like, a local public health authority could tell everybody, this Sunday, I want everybody to use your rapid at-home test. Report your results anonymously to this number. And, if you test positive, take it seriously, take precautions. Measures like that could preserve privacy, while still collecting that key surveillance data and crashing the epidemic curve.
BL: Right, that would be really cool to see. Are there any other types of COVID tests or surveillance methods that you think might become more useful and more prevalent in the next few months or heading into the fall?
DL: Yeah, there are two kinds. So, one key point about at-home tests is that privacy-preserving aspect. Like, I trust local public health here. But I tend to vote left of center and generally trust the government. I live in Colorado, and not everybody feels that way. There’s definitely a strong libertarian independent streak. And I feel like one of the key advantages of at-home tests is that they appeal to that kind of person. They empower a person and their family to make health decisions, and they give you the information. But they don’t necessarily get recorded by something like COVID Tracking Project or HHS.
BL: Yeah.
DL: There’s less visibility for authorities, but for some folks who want information that they can act on to protect themselves and others, then that’s going to be fine. And so, as much as I would like to know exactly what is happening with the pandemic, if the trade-off for lower cases is that we don’t know about a lot of cases among folks who would rather not report their data, I think that’s a fair trade-off.
BL: Yeah, that makes sense.
DL: But it’s sort of like uncomfortable for me, who likes the data to say that. You know what I mean?
BL: It reminds me of the conversation around exposure notification apps. I talked to someone who works on those apps recently, and she kind-of said the same thing, that she would rather have everyone using the app than really good data from a tiny subset of the population that’s okay with their privacy being violated.
DL: A big thing to me is that, we know that the pandemic has been political. And I don’t see any reason why we can’t have solutions that work for the person who votes left of center, the person who votes in the middle, and the person who votes right of center.
But the other kind of tests that I’m excited about, only because they’re extremely cheap and really easy, are anosmia screens. We know that loss of sense of smell is highly specific to COVID. If you don’t have a stuffy nose, and you [suddenly] can’t smell things, you probably have COVID. So, there are companies that produce, like, a little card with a scratch-and-sniff quiz. You don’t know what’s behind the panel, but you scratch, pull up a smartphone app, and then say what you think the smell is from a multiple choice test.
One of the cool things is that anosmia only occurs in around 40% of people [with COVID] if you ask them to self-report. But if you give them one of these objective quizzes, the prevalence of anosmia as a symptom goes up to [around 75 or 80%], depending on which study you look at. The important thing is that those cards cost 25 cents apiece, and multiple people can use the same card. It’s literally a scratch-and-sniff with an online quiz.
BL: That’s incredible. Do you know if there are tests like that that are up for EUA?
DL: Yeah. Roy Parker, Michael Mina, and I collaborated with a great team to write this paper last year on typical COVID testing [PCR, LAMP, and antigen testing], test sensitivity and frequency and turnaround time. Then, Roy and I teamed up with Derek Toomre at Yale School of Medicine, and took the same idea and said, well, what if we use frequent, repeated anosmia screening tests?
One of the things that I like about those is that they’re cheap. But another thing that I like about them is that nobody thinks that [a smell test is] the same thing as a proper COVID test. You can’t get them confused. [This is important because one of the questions with rapid tests is how people may interpret a negative test—they might be infected, but the virus is at a low level. So if they get a negative rapid test and then go to the gym, the test could actually have an unintended effect. But if an anosmia test tells you that you still have your sense of smell… People understand that just because you still have your sense of smell doesn’t mean that you’re COVID-free. There’s lower risk of unintended consequences.]
Anyway, I think the messaging around those [anosmia] tests is easy. They’re easy to use, you can do them at home. And they can print them for, like, a quarter apiece. So the modeling suggests that they could be pretty effective and really cheap. You could literally mail somebody a stack of 10 of these things to everybody in the U.S.
BL: And do it once a week!
DL: Yeah, do it once a week. So, that’s another kind of test that I would like to see out there. The company that Derek started, that makes those [tests], just won one of the XPRIZEs for COVID testing. So, I think that’s cool. It’s a more creative kind of test, and it’s inexpensive.
BL: Sweet. So, that was all the questions that I had. Is there anything you think is important on this topic that I should know for this article?
DL: I just think it’s really important to keep a global perspective… As with vaccines, we know there are inequities within the U.S. But there are definitely global inequities. And while we might feel like we’re on a glide path to herd immunity through vaccination here in the States, things look very different in the rest of the world. And so, the use of these tests may become more important this fall, we may get more variants globally, even as the U.S. cases go down. I think it’s an ongoing story, even if hospitalizations and deaths continue to drop here in the States.
BL: And those tests you’re talking about that are cheaper and easier to use are useful in many places, not just here.
DL: Yeah, that’s the hope… I feel generally optimistic about [the state of the pandemic], but like, hesitant.
BL: I feel you. It’s definitely weird to see everyone getting very excited about the summer when I’m kind-of sitting here in my COVID reporting bubble, like, ahhh, not there yet.
DL: Well, one of the hardest parts, I think, for public health officials is going to be, if cases are going up, but mortality and hospitalizations are flat or going down. If COVID is only making people sick, but it’s not hospitalizing and killing them. Then, like, do we just reopen everything? Do we open up the schools? That’s tough when we’ve been acclimated to keep our foot on the brakes as much as possible.
Abbott ID NOW tests, pictured at a health clinic in Williamsburg (my photo).
Two weeks ago, I went to my COVID-19 testing site of choice for a post-Maine trip screening. I walked the now-familiar ten blocks to the site, a private clinic in Williamsburg, and waited at the now-familiar counter for one of the receptionists to be available to check me in.
“Do you want a rapid test?” the receptionist asked.
“No, PCR, please,” I replied.
I had assumed that the “rapid test” she offered was an antigen test. Antigen tests, as I’ve described in this newsletter before, have a low sensitivity, meaning that they may miss identifying people who are actually infected with the novel coronavirus. (These missed cases are called false negatives.) Evidence also suggests that antigen tests will return more false negatives for patients who are asymptomatic. As I was not exhibiting COVID-19 symptoms, and rather wanted to get tested because I had recently traveled out of the state, I was interested in receiving a more accurate test.
But confusion quickly ensued: the rapid test that my clinic offered, as it turned out, was not an antigen test. It was a nucleic acid amplification test—a model manufactured by Abbott called the ID NOW. Like PCR (polymerase chain reaction) tests, this test uses gene amplification to identify genetic material associated with the novel coronavirus in a patient’s mucus sample. But unlike PCR tests, the ID NOW test does not require clinics to send samples out to faraway labs for processing. This test is distributed with small, in-house DNA amplification machines that can provide patients with their results in 15 minutes. I got the result of my ID NOW test later that same afternoon. (And then I got the results of a second test, this one a PCR test which I had asked the clinic to request at a lab, several days later. Both tests were negative.)
I hadn’t heard of Abbott ID NOW tests before last week. But they’re in the news now, connected to what has become America’s most infamous COVID-19 outbreak: President Trump’s White House relied on Abbott ID NOW tests. And they used these tests incorrectly.
No test type specification in molecular testing data
Rapid testing has been the White House’s defense against critiques of COVID-19 carelessness, explains Slate reporter Daniel Politi. Each day, staffers would get tested with Abbott ID NOW tests. Upon receiving negative results, staffers would be cleared to take off their mask and act without consideration for social distancing. Boxes of the ID NOW tests used for this screening have been pictured at the White House since March.
But how accurate are those negative results? If you’re asymptomatic: not very. The ID NOW test is only authorized for use in people with symptoms. A guidance from the Food and Drug Administration (FDA), updated on September 17, specifies:
The ID NOW COVID-19 is authorized for use with respiratory specimens collected from individuals who are suspected of COVID-19 by their healthcare provider within the first seven days of the onset of symptoms.
The majority of White House staffers who were tested with these tests had not been coughing and wheezing, nor had they been suspected of COVID-19 by a healthcare provider. In asymptomatic patients like these, as many as one-third of negatives returned by the ID NOW test may be false negatives. It’s no surprise, then, that the virus spread quickly through an indoor environment where staffers were using rapid tests—but doing little else.
White House staff are not the only people who used the wrong type of test to check their COVID-19 status. I shouldn’t have gotten an Abbott ID NOW test either. But when a nurse at my local clinic, which I saw as a site of trusted health expertise, offered one to me, I didn’t ask too many questions. It’s PCR, I thought. It’ll be accurate.
But first of all: the Abbott ID NOW test is not a PCR test. It’s in the same family as PCR tests (molecular-based, DNA amplification), but it operates on a different paradigm. And second of all, the health care workers at my clinic gave me no indication of how accurate this rapid test was, especially for my asymptomatic self. (Note: I have no hard feelings toward this clinic or any of the workers there. I’m simply using my own experience as an example of how poorly information about test types is conveyed to the public in general.)
What if my PCR test, sent out to a lab, had returned a positive result? I would have traversed Brooklyn, gotten groceries, grabbed coffee at a neighborhood cafe, and attended a protest in Queens that weekend, buoyed by a negative result yet unknowingly spreading the coronavirus to my fellow New Yorkers. And both of my tests would have been accounted for on New York’s testing dashboard in one single tick mark. New York reports tests in encounters, so my two specimens would have been deduplicated as simply “one person tested on September 30.”
I say “would have been” because I am not, in fact, sure that my Abbott ID NOW test made it into the New York Public Health Department’s database at all.
Here’s a line from the press release that Abbott put out on October 2, the day that Trump tested positive:
While we don’t know the details on who was tested and on which devices, we know that more than 11 million Americans have taken the ID NOW test, helping to stop the spread of the virus.
11 million is a pretty big number: if these tests were all included in the national count reported by the COVID Tracking Project, they would make up about 10% of the total. But are the ID NOW tests included in the COVID Tracking Project’s count? It is difficult to say. The majority of state public health departments, the sources for the COVID Tracking Project’s data, simply report total counts of nucleic acid-based tests, if they specify their test type at all.
State COVID-19 dashboards fail to separate out test counts by method or manufacturer. Some states, such as Maine and Illinois, acknowledge that their test counts include all “nucleic acid-based tests,” not only the PCR tests which fall into this category. Other states, such as Oklahoma and Florida, report detailed data about the testing capacity of individual labs and point-of-care facilities, but fail to supply the testing models used at each location. South Carolina acknowledges a small number of “unknown” tests, for which the public health department is investigating possible categorizations. The Department of Health and Human Services, meanwhile, only reports PCR tests, absent counts of any other molecular test type.
And, returning to Abbott’s press release: the manufacturer admits that they “don’t know the details on who was tested and on which devices.” This leaves a lot of open questions about how rapid testing data are being collected; Abbott seems to imply that even the manufacturer itself does not have access to specific information about where and how their tests are in use. If I had to guess, I’d say that 11 million figure comes from bulk test orders sent out by facilities like my local clinic.
It’s great for healthcare responses that Abbott tests can be processed quickly on-site, in facilities like a healthcare clinic or a major political site. But public health departments don’t have relationships with clinics—they have relationships with testing laboratories. When tests aren’t sent out to a lab, it’s easy for them to fall through gaps in a data pipeline which relies on complex electronic reporting systems. (This is also a problem for antigen tests.)
So, the problem stands: Abbott ID NOW tests are in use across the country. 11 million of them have been distributed since March. But where are the tests being used, how many of them have returned positive results, and are they being used correctly—to quickly diagnose patients with COVID-19 symptoms? Without these data, it is difficult to determine whether Abbott’s test should be part of America’s testing strategy going forward.
Conflating antigen and PCR tests
I can’t discuss the data pitfalls of rapid COVID-19 testing without devoting a few paragraphs to antigen tests.
Five days before his positive COVID-19 test was made public, President Trump announced a plan to deploy 150 million antigen tests across the country. 100 million tests will go to state and territory public health departments, while the remaining 50 million will go to facilities supporting vulnerable populations such as nursing homes, hospice care facilities, and historically Black colleges. Trump discussed how useful antigen tests could be for screening, suggesting that teachers could be tested regularly.
The tests Trump praised are rapid antigen tests manufactured by Abbott, which received FDA Emergency Use Authorization at the end of August. Abbott’s antigen tests are cheap—each one costs $5. And, like the ID NOW tests, they’re fast—patients receive results in 15 minutes. But, also like the ID NOW tests, antigen tests are more effective for symptomatic people.
Here is how Alexis Madrigal and Rob Meyer explain it, in an article for The Atlantic published this past week:
If distributed en masse and used to screen asymptomatic people, these antigen tests will deliver hundreds of thousands—if not millions—of false results, they say. False negatives could lead to reckless behavior by people who don’t know they’re sick. False positives can also put people at risk: If a virus-free nursing-home resident with a false positive is placed in a COVID-19 ward, that person could become infected.
This is not to say that antigen tests are useless; their utility is still being debated in epidemiological and public health circles. The advantages of these cheap, fast tests may outweigh the dangers of their low sensitivity. But to truly understand this problem, we need access to better antigen test data—not just 60 tests from Nevada nursing homes (the sample size upon which that state’s decision was made).
If 11 million Abbott ID NOW tests are a data concern, 150 million Abbott antigen tests are a data minefield. For the past month, I’ve been working on an analysis for the COVID Tracking Project which covers how states are reporting—and failing to report—antigen test results. This analysis is set to be released in the next week, in all its detailed glory. But I can tell you now that the majority of states are not reporting antigen tests in separate counts from DNA-based tests, just as the majority of states are not reporting other types of DNA-based tests as separate from PCR tests. In fact, several states now specifically report that their testing counts combine PCR and antigen tests in one figure.
When two different test types are conflated in a single total figure, it is difficult to analyze the progression of how either test is being used. I can’t tell you how many antigen tests are being put to use across the country, or how effective they are at containing COVID-19 in a given community, if these test numbers are lumped in with another test type. Test lumping also presents a(nother) challenge for test positivity calculations, as antigen and PCR tests have very different sensitivity levels.
And even the few separate antigen test counts that states do report are likely significant undercounts of the actual scale of antigen testing going on in the U.S. As I mentioned earlier, no data reporting pipelines are set up for tests that occur rapidly in point-of-care settings. The Center for Medicare & Medicaid Services (CMS) does not report the number of antigen tests that have occurred in nursing homes, for example.
So far, it appears that state and federal public health agencies alike are unprepared to report the results of antigen tests. Before the White House deploys its 150 million Abbott antigen tests, I hope to see that change.