In May 2023, the Department of Health and Human Services (HHS), Walgreens, and Labcorp started offering free PCR tests at select pharmacy locations. The program appears to still be available following the end of the federal public health emergency.
Through the program, Americans can pick up a free kit to take a PCR test at home, then ship their sample to Labcorp for analysis. No insurance information is required. Results should be available within two days of the lab receiving the patient’s sample, according to Walgreens. About 1,000 Walgreens locations across the country are stocking these free tests, but they need to be picked up in person.
I learned about this Walgreens program from the People’s CDC, which included it in their Weather Report newsletter on July 10. The newsletter suggests this program is recent, though I haven’t been able to find any other news about it besides a press release from May 2022. So, either tests are still available from the original iteration of the program or Walgreens revamped it recently.
Either way, this Walgreens program is a helpful option for anyone looking to get a free PCR test—though it’s obviously far below the extensive, accessible PCR testing network that the U.S. continues to need. If any readers try this out, I would be curious to learn about your experience!
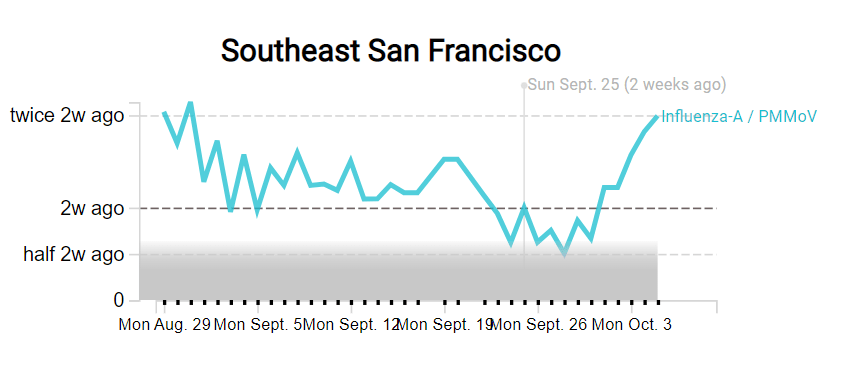
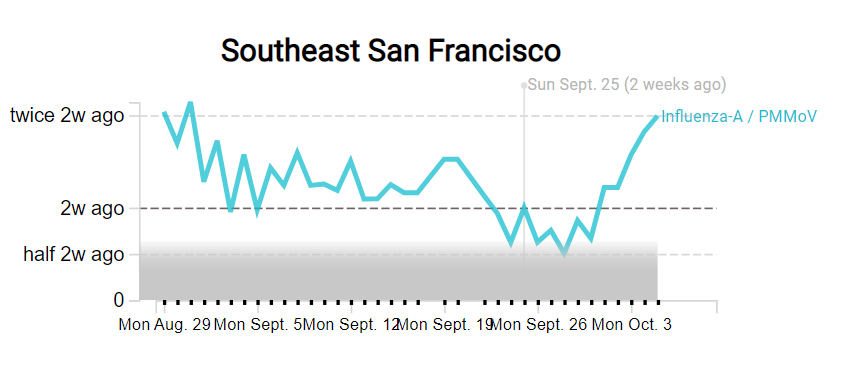
As you might have guessed from the last couple weeks of National numbers posts, I am anticipating that the U.S. will see a new COVID-19 surge this fall, along with potential surges of the flu and other respiratory diseases. And I’m not the only person making this prediction: in the last couple of weeks, this potential surge has been a major theme in news publications and health experts’ Twitter threads.
Yes, most of the U.S.’s major COVID-19 indicators appear to be at low levels right now (at least compared to earlier in the Omicron era). But rising numbers in Europe, as well as trends from some parts of the Northeast, provide reasons to worry. Here’s why it’s worth worrying, and some thoughts on better tracking these viruses in the future.
Why experts anticipate a fall surge
One likely reason for a fall surge, as writer Ewen Callaway explains in Nature, is an influx of new subvariants that have continued to evolve off of Omicron. While there are several lineages on the rise in various countries, researchers are finding that they tend to have similar mutations and capacities for reinfecting people, Callaway reports. Scientists call this “convergent evolution.”
From the story:
SARS-CoV-2-watchers are tracking an unprecedented menagerie of variants from a number of branches of the Omicron family tree, says Tom Peacock, a virologist at Imperial College London. Despite these variants’ distinct ancestries, they carry many of the same mutations to the SARS-CoV-2 spike protein (the part of the virus that immune systems target). “Clearly, there’s an optimal way for a variant to look going into this season,” says Peacock.
The new bivalent booster shots will help reduce severe disease from these newer Omicron iterations. But Americans are currently getting boosted in such small numbers that the shots might not help alleviate healthcare systems as much as experts might’ve hoped. And that brings me to another surge driver: behavior.
More than at any point in the pandemic, Americans are acting like COVID-19 is not worth a simple mask in public or test before a gathering—even though the coronavirus is still very capable of sending people to the hospital or giving them long-term symptoms. Indoor gatherings, holiday travel, fully opened schools, and all the behaviors that come with them will inevitably lead to outbreaks that are poorly tracked by our increasingly-less-resourced public health system (and that are largely ignored by leaders who encouraged the unsafe behavior).
So we can call this winter “post-pandemic” if we want. But given the policy failures and institutional dysfunctions that have accumulated over the past three years, it won’t be anything like a pre-pandemic winter, either. The more we resist that reality, the worse it will become. If we treat this winter as normal, it will be anything but.
In addition to COVID-19 and the flu, the U.S. is seeing increased transmission of other respiratory viruses particularly primed to spread among children, such as RSV, rhinoviruses and enteroviruses. Pediatricians and hospital directors told USA TODAY’s Adrianna Rodriguez that they’re seeing more sick kids, earlier in the school year than they would typically expect. Kids have less immunity to these viruses after limited spread in the last two winters, while minimal health precautions are making it easier for the viruses to infect more people.
Expanding COVID-19 surveillance to other viruses
In short, we could see a lot of respiratory virus cases in the next few months. These trends have got me thinking about how, in an ideal world, the U.S. public health system might expand our existing COVID-19 surveillance to better track all of the viruses that wreak havoc on our bodies during colder weather. (As I pointed out last month, our flu tracking is pretty terrible right now.)
Here are a few suggestions:
Expand wastewater surveillance to other respiratory viruses. Some pilot programs, such as the SCAN network based at Stanford and Emory Universities, have already started to monitor the flu, RSV, and other viruses in wastewater. But we need this type of tracking on a much broader scale, and we need it to be funded by the CDC and other major health institutions. (Biobot and the CDC’s expansion into monkeypox surveillance is a good first step here.)
Make multipurpose PCR tests widely available. My favorite place to get a COVID-19 test is one of the NYC health department’s express PCR sites. These public labs conduct PCR analysis on-site, so I get my test results in a few hours. And the results don’t just include COVID-19: the lab also tests for flu and RSV, so I can immediately rule out several explanations as to why my throat might be sore. We need many more labs doing this type of multi-virus testing.
Conduct population surveys for multiple respiratory diseases. I frequently reference the work of epidemiologist Denis Nash and his team at the City University of New York, who have surveyed New Yorkers and nationally to understand true COVID-19 infection rates. This type of work should be expanded to other diseases, in order to develop better, closer-to-real-time estimates of multiple conditions.
Add more diseases to hospital surveillance systems. Did you know that the HHS’s hospital utilization dataset includes hospitalizations for flu? While facilities have the opportunity to submit their flu patient numbers through the same system that they report on COVID-19 patients, flu reporting is optional—and therefore not very useful for analysis. A future iteration of the HHS’s hospital surveillance system should include mandatory flu reporting as well as other diseases, so that we can track severe cases more closely.
Incorporate respiratory virus tracking into school systems. For the first couple of pandemic-era semesters, many K-12 school systems maintained detailed records of their COVID-19 cases. This process has largely disappeared along with other COVID-19 measures—and while it lasted, it was incredibly burdensome for the school officials doing the tracking (many of them already-overworked school nurses). Still, in a future with more resources devoted to health in public schools, I’d like to see them become sites for tracking a variety of diseases and health conditions. The more collaboration between public schools and public health, the better.
If you know of researchers or organizations working on any of these surveillance mechanisms—or anything I haven’t included on this list—please reach out! I am always on the lookout for solutions story ideas.
New York City has been closing PCR testing sites, even as the city faced a major Omicron resurgence this spring. This was the main finding from a story I wrote for Gothamist and WNYC (New York Public Radio), based on my analysis of public information on city-run testing sites.
While this was a local story, I think the trends I found—and the pushback that the piece received from city health officials—are pretty indicative of the national state of COVID-19 testing right now. Since the federal government ran out of funding to cover testing for Americans without health insurance in late March, private testing companies have started requiring insurance information and, in many cases, raising their prices.
At the same time, state and local health departments have closed their public PCR testing sites and directed people to use at-home rapid tests instead. New York City still has more accessible testing than most of the country, but my story showed how even here, getting tested is becoming more difficult—and less popular.
NYC has faced a major COVID-19 surge this spring — yet the city closed public testing sites and made it harder to get PCR results.
— betsy ladyzhets 📊 (@betsyladyzhets) July 5, 2022
Here are a few key statistics from the piece:
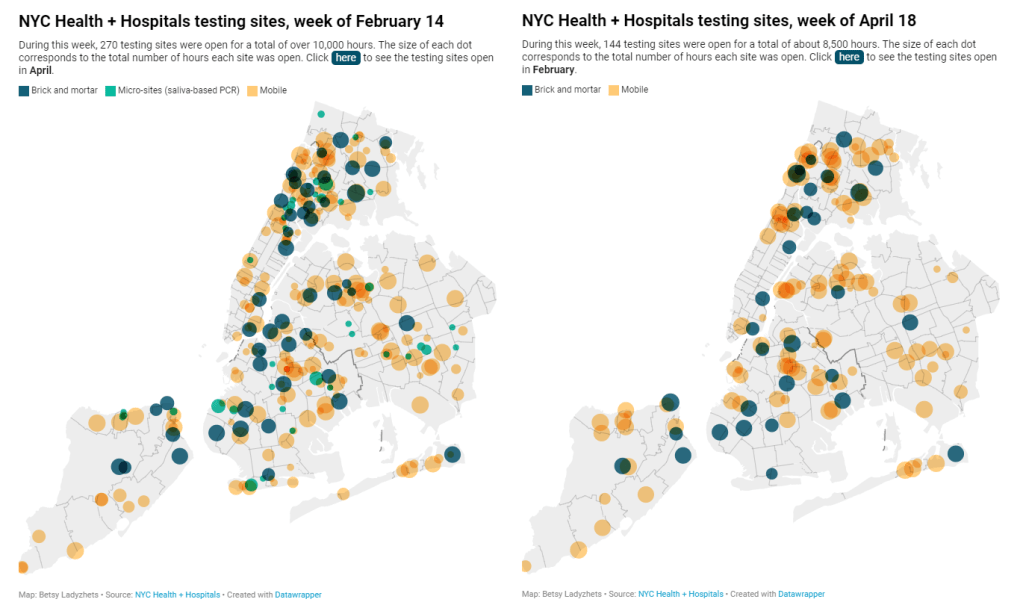
The number of public PCR testing sites run by NYC Health + Hospitals was cut in half between mid-February and mid-April.
The total hours that public testing sites were open decreased from over 10,000 during a week in February, to 8,500 during a week in April, to 7,500 in the last week of June.
Manhattan testing hours remained relatively constant (about 1,500 in each of the weeks I analyzed), while hours were cut in other boroughs.
The numbers of New Yorkers getting tested on a daily basis were similar in June 2021 and June 2022—even though reported case rates were about ten times higher this year.
New York City’s test positivity rate recently shot above 10%, and is now over 15%. It was closer to 1% at this time last year.
The NYC health department had some issues with my story. In fact, city health commissioner Dr. Ashwin Vasan posted a Twitter thread stating that it was “missing key information” and that the city actually has “more testing resources than ever.” But the “testing resources” he cites here are mostly at-home tests; PCR testing in NYC is both less accessible and less popular. A follow-up story that I coauthored with Nsikan Akpan, my editor at Gothamist/WNYC, further explains the situation in the city.
The decline in PCR testing is making it harder to understand where and how fast the coronavirus is spreading, both in the city and around the U.S. To explain the implications of this trend, here’s a short FAQ on how to think about testing during our current surge.
Why is PCR testing still important for individuals?
One of the city officials’ main responses to my story was that NYC has made it easy for people to get free at-home rapid tests, in place of PCR testing. The city has distributed more than 35 million at-home tests at hundreds of libraries and other community sites.
At-home tests certainly have advantages: they’re more convenient, with results back in 15 minutes. Turnaround times for PCR tests are generally pretty fast right now thanks to limited demand (usually under 48 hours, if not under 24 hours, in NYC), but that’s still a long wait compared to a rapid test. Rapid, at-home tests also provide a better indicator of contagiousness.
Still, PCR tests have continued utility because they remain the gold standard of accuracy: they’re able to identify a COVID-19 case with much smaller amounts of coronavirus present in someone’s respiratory tract than a rapid test. As a result, if you were recently exposed or are showing some mild symptoms—but testing negative on rapid tests—a PCR test could be valuable to provide a more reliable COVID-19 status.
PCR tests can also be helpful for documenting a COVID-19 case. While many doctors will take a rapid test positive as a clear indicator of an infection, some settings may require a PCR test—in which results are verified by the lab that processes the test. This can be particularly true for Long COVID clinics, health advocate JD Davids told me. So, if you tested positive on a rapid test but are concerned about Long COVID symptoms, a PCR test may be a helpful verification step.
Why is PCR testing still important for communities?
Rapid, at-home test results generally do not travel further than your trashcan, or maybe your phone camera. They don’t get reported to testing companies, or local public health departments, or the CDC—unlike PCR tests, which have established data pipelines for such reporting. Some jurisdictions do have options for residents to self-report rapid test results, but this self-reporting is generally a small fraction of the total tests conducted.
As a result, public health experts generally rely upon PCR testing data to understand patterns in COVID-19 spread. When less PCR testing takes place, these patterns become more difficult to interpret. For example, in the U.S. as a whole, around 100,000 new cases a day have been reported for the last several weeks; but we know that the true trend would likely be a lot more variable if we had data from rapid tests.
Also, as Brown University epidemiologist Dr. Jennifer Nuzzo pointed out when my editor Nsikan interviewed her for our follow-up story, PCR tests are necessary for tracking variants. A selection of PCR test samples get genetically sequenced; this doesn’t happen for rapid tests.
“It’s really important for us to stay ahead of what variants are circulating in our communities,” Nuzzo said, citing what society has already learned about different variants to date. “Some are more transmissible. Some have been more severe. We need to stay ahead of the virus, so that we can know when and how and if to change our strategy about how to control it.”
What’s the value of abundant local testing sites?
If PCR testing is less popular in this current phase of the pandemic, you might ask, why not just have a few central testing hubs in a place like NYC, and maintain testing capacity in a more efficient way? This seems to be the city’s response, to some extent: officials explained that some brick-and-mortar testing sites (mostly at NYC hospitals) are staying open, while the city’s fleet of mobile testing vans can move around as needed.
But for a lot of people, traveling outside their neighborhood to get a test or tracking down the right mobile van can be a major barrier to getting tested. This is especially true for essential workers and low-income New Yorkers—who are the people most in need of testing. Maintaining public testing throughout the city is a health equity issue.
And even if the testing capacity is technically maintained, location is important. Consider a region like South Brooklyn: Four brick-and-mortar testing sites scheduled to close in mid-July are all located in this area: 4002 Fort Hamilton, Bay Ridge, Bensonhurst and Midwood Pre-K.
It’s unclear whether mobile sites will move to South Brooklyn in response. Shrier said each closing site has “dedicated at-home test distribution sites” within one mile. But residents of Bay Ridge, Bensonhurst and other nearby neighborhoods may need to travel further to get a PCR test — or face high costs at private sites.
What data sources could replace information from PCR tests?
Dr. Denis Nash, an epidemiologist at the City University of New York whom I interviewed for the first NYC story, talked about two types of data that may be collected by a health agency tracking disease spread.
“There’s active surveillance and passive surveillance,” he said. “In active surveillance, the health department staff are actively going out and trying to ascertain how many cases there might be. They’re going to hospitals and to homes, looking for cases. And when you do that, you’re more likely to exhaustively find a high proportion of cases.” One example of active surveillance: a survey conducted by Nash and his team at CUNY in April and May, which indicated about 20% of New Yorkers may have had COVID-19 within a two-week period.
Meanwhile, passive surveillance “relies on healthcare providers and laboratories to voluntarily report their tests and cases to the health department,” Nash said. NYC and other health departments which receive much of their COVID-19 data—PCR test results, hospital admissions, etc.—from healthcare providers are exemplifying this passive approach.
As COVID-19 becomes less of a public concern and testing is less popular, health agencies should step up their active surveillance, Nash said. Wastewater can be another source of data that’s more active than PCR test results, since it reflects COVID-19 spread across a large population. (Unfortunately, in NYC, wastewater data is pretty inaccessible; that’s a topic for another time.)
What’s the best way to use at-home rapid tests?
Rapid test use can fall into three different categories. First, if you are trying to determine whether you’re actively contagious right before a gathering or seeing a high-risk person: take one test, as close in time to the event as possible. (For example, if I’m going to a large march in NYC, I plan to test myself a few minutes before heading to the subway.)
Second, if you had a recent COVID-19 exposure (or attended a high-risk event), test multiple times in succession—ideally at least twice in 48 hours. This testing process should start a couple of days after the exposure, because rapid tests aren’t accurate enough to pick up the infection right away. You could also use a single PCR test to serve the same purpose as multiple rapid tests.
And third, if you are isolating after a positive COVID-19 test, rapid tests can help identify when you’re no longer contagious and able to return to society. As I wrote in an earlier post, the CDC’s five-day isolation guidance is not actually backed up by data; testing out of isolation is much safer.
As always, if you have questions about testing or any other COVID-19 topic, my inbox is open.