As you might have guessed from the last couple weeks of National numbers posts, I am anticipating that the U.S. will see a new COVID-19 surge this fall, along with potential surges of the flu and other respiratory diseases. And I’m not the only person making this prediction: in the last couple of weeks, this potential surge has been a major theme in news publications and health experts’ Twitter threads.
Yes, most of the U.S.’s major COVID-19 indicators appear to be at low levels right now (at least compared to earlier in the Omicron era). But rising numbers in Europe, as well as trends from some parts of the Northeast, provide reasons to worry. Here’s why it’s worth worrying, and some thoughts on better tracking these viruses in the future.
Why experts anticipate a fall surge
One likely reason for a fall surge, as writer Ewen Callaway explains in Nature, is an influx of new subvariants that have continued to evolve off of Omicron. While there are several lineages on the rise in various countries, researchers are finding that they tend to have similar mutations and capacities for reinfecting people, Callaway reports. Scientists call this “convergent evolution.”
From the story:
SARS-CoV-2-watchers are tracking an unprecedented menagerie of variants from a number of branches of the Omicron family tree, says Tom Peacock, a virologist at Imperial College London. Despite these variants’ distinct ancestries, they carry many of the same mutations to the SARS-CoV-2 spike protein (the part of the virus that immune systems target). “Clearly, there’s an optimal way for a variant to look going into this season,” says Peacock.
The new bivalent booster shots will help reduce severe disease from these newer Omicron iterations. But Americans are currently getting boosted in such small numbers that the shots might not help alleviate healthcare systems as much as experts might’ve hoped. And that brings me to another surge driver: behavior.
More than at any point in the pandemic, Americans are acting like COVID-19 is not worth a simple mask in public or test before a gathering—even though the coronavirus is still very capable of sending people to the hospital or giving them long-term symptoms. Indoor gatherings, holiday travel, fully opened schools, and all the behaviors that come with them will inevitably lead to outbreaks that are poorly tracked by our increasingly-less-resourced public health system (and that are largely ignored by leaders who encouraged the unsafe behavior).
Katherine Wu summarized this situation well in a recent article for the Atlantic, writing:
So we can call this winter “post-pandemic” if we want. But given the policy failures and institutional dysfunctions that have accumulated over the past three years, it won’t be anything like a pre-pandemic winter, either. The more we resist that reality, the worse it will become. If we treat this winter as normal, it will be anything but.
At the same time, the behaviors contributing to more COVID-19 spread will also help other respiratory viruses. Experts are anticipating that the U.S. could have a bad flu winter, based on trends from the Southern hemisphere—which faces the flu a few months before we do. (For journalists interested in following flu patterns this fall and winter, the Association of Health Care Journalists has a new tipsheet on the subject.)
In addition to COVID-19 and the flu, the U.S. is seeing increased transmission of other respiratory viruses particularly primed to spread among children, such as RSV, rhinoviruses and enteroviruses. Pediatricians and hospital directors told USA TODAY’s Adrianna Rodriguez that they’re seeing more sick kids, earlier in the school year than they would typically expect. Kids have less immunity to these viruses after limited spread in the last two winters, while minimal health precautions are making it easier for the viruses to infect more people.
Expanding COVID-19 surveillance to other viruses
In short, we could see a lot of respiratory virus cases in the next few months. These trends have got me thinking about how, in an ideal world, the U.S. public health system might expand our existing COVID-19 surveillance to better track all of the viruses that wreak havoc on our bodies during colder weather. (As I pointed out last month, our flu tracking is pretty terrible right now.)
Here are a few suggestions:
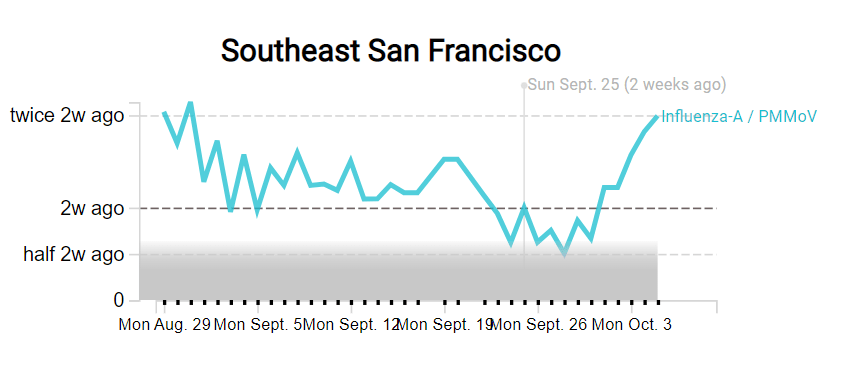
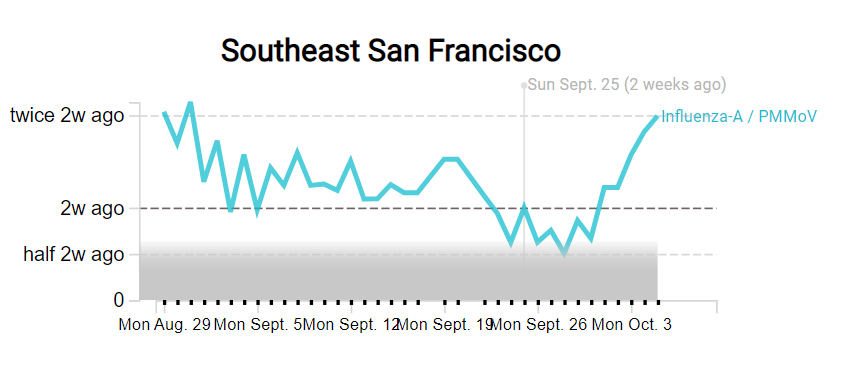
- Expand wastewater surveillance to other respiratory viruses. Some pilot programs, such as the SCAN network based at Stanford and Emory Universities, have already started to monitor the flu, RSV, and other viruses in wastewater. But we need this type of tracking on a much broader scale, and we need it to be funded by the CDC and other major health institutions. (Biobot and the CDC’s expansion into monkeypox surveillance is a good first step here.)
- Make multipurpose PCR tests widely available. My favorite place to get a COVID-19 test is one of the NYC health department’s express PCR sites. These public labs conduct PCR analysis on-site, so I get my test results in a few hours. And the results don’t just include COVID-19: the lab also tests for flu and RSV, so I can immediately rule out several explanations as to why my throat might be sore. We need many more labs doing this type of multi-virus testing.
- Conduct population surveys for multiple respiratory diseases. I frequently reference the work of epidemiologist Denis Nash and his team at the City University of New York, who have surveyed New Yorkers and nationally to understand true COVID-19 infection rates. This type of work should be expanded to other diseases, in order to develop better, closer-to-real-time estimates of multiple conditions.
- Add more diseases to hospital surveillance systems. Did you know that the HHS’s hospital utilization dataset includes hospitalizations for flu? While facilities have the opportunity to submit their flu patient numbers through the same system that they report on COVID-19 patients, flu reporting is optional—and therefore not very useful for analysis. A future iteration of the HHS’s hospital surveillance system should include mandatory flu reporting as well as other diseases, so that we can track severe cases more closely.
- Incorporate respiratory virus tracking into school systems. For the first couple of pandemic-era semesters, many K-12 school systems maintained detailed records of their COVID-19 cases. This process has largely disappeared along with other COVID-19 measures—and while it lasted, it was incredibly burdensome for the school officials doing the tracking (many of them already-overworked school nurses). Still, in a future with more resources devoted to health in public schools, I’d like to see them become sites for tracking a variety of diseases and health conditions. The more collaboration between public schools and public health, the better.
If you know of researchers or organizations working on any of these surveillance mechanisms—or anything I haven’t included on this list—please reach out! I am always on the lookout for solutions story ideas.

Leave a comment