As the Omicron surge continues, we are still learning more about this variant. Here are the major updates from this week:
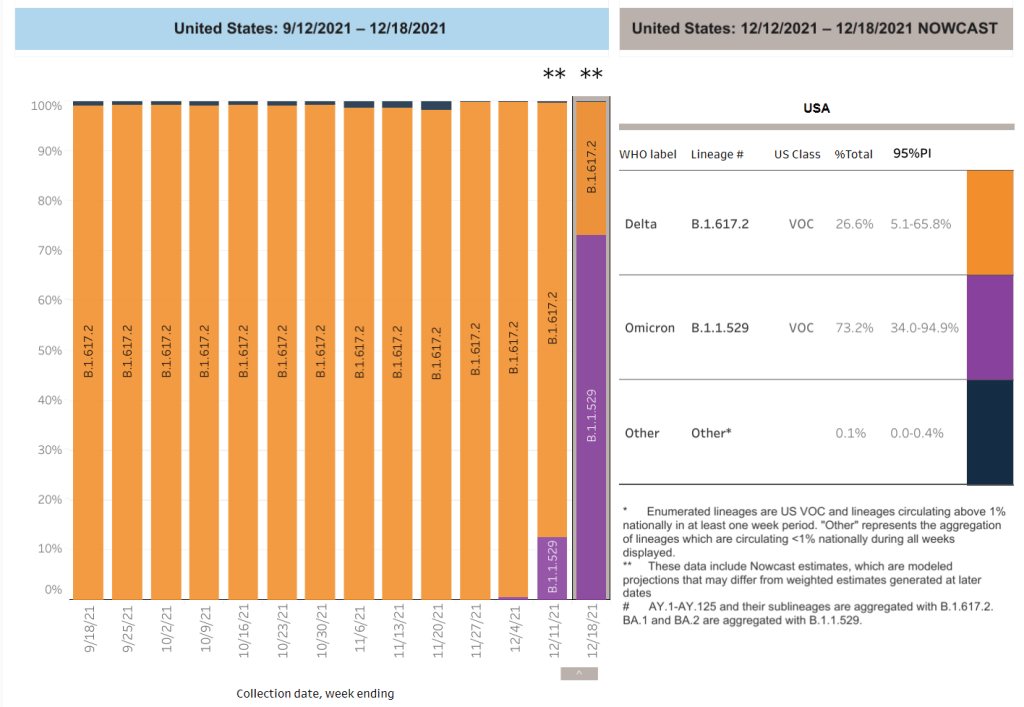
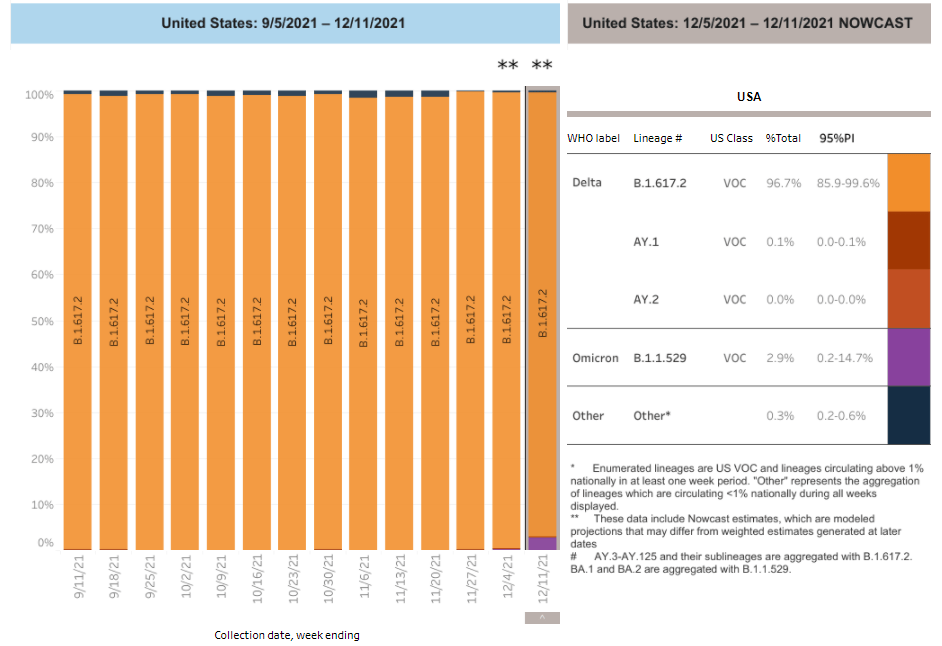
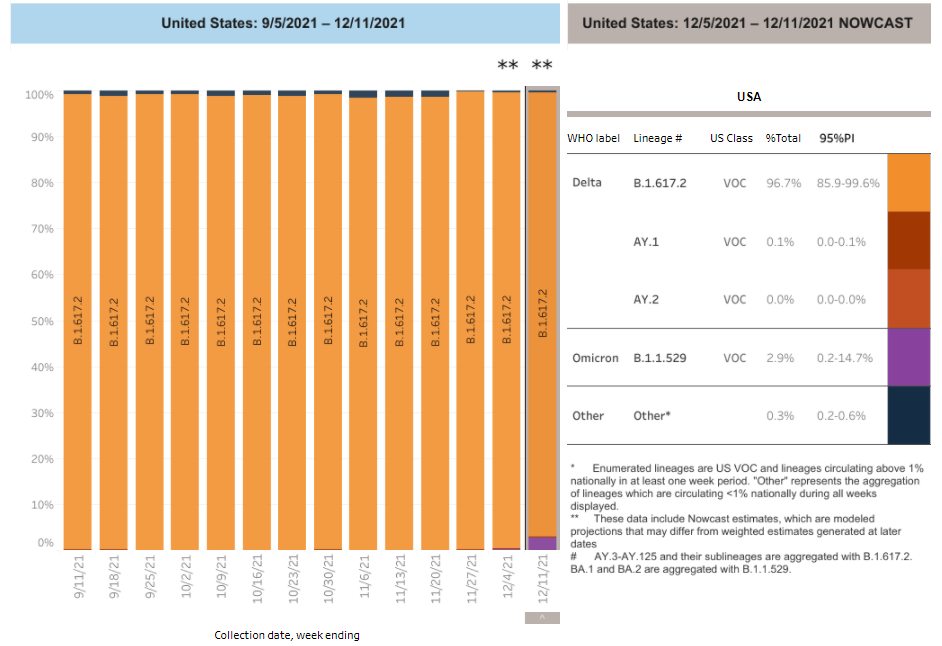
- Omicron is now causing more than 90% of new cases in the U.S. In the latest update of the CDC’s variant proportions estimates, the agency found that Omicron caused 95% of new COVID-19 cases nationwide in the week ending January 1. The CDC also revised estimates for previous weeks, bringing us to 77% Omicron for the week ending December 25 and 38% Omicron for the week ending December 18. While these estimates continue to be based on weeks-old data, it the CDC now has enough sequencing information to make Omicron estimates with lower confidence intervals than it did a few weeks ago—suggesting that these numbers are closer to reality than the estimates we saw in December.
- Omicron is causing the vast majority of cases in every state. Also included in the CDC’s variant proportions estimates: regional numbers. The latest figures estimate that, as of January 1, Omicron prevalence across the country ranges from 82% in the Northeast to 98% in New York/New Jersey and the Gulf states region (Texas, Louisiana, Arkansas, Oklahoma, and New Mexico). These numbers align with recent calculations from computational biologist Trevor Bedford based on sequences posed to the public repository GISAID. In short: Omicron is everywhere.
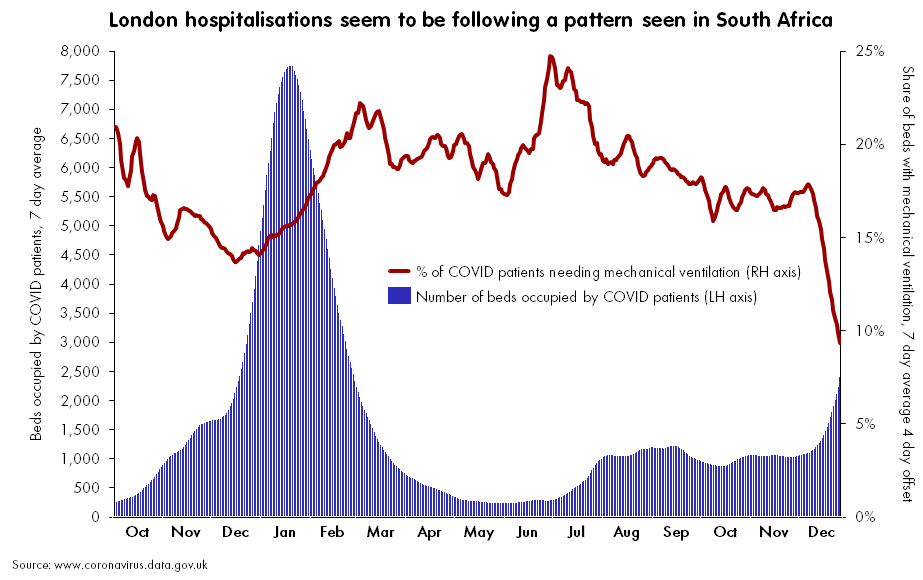
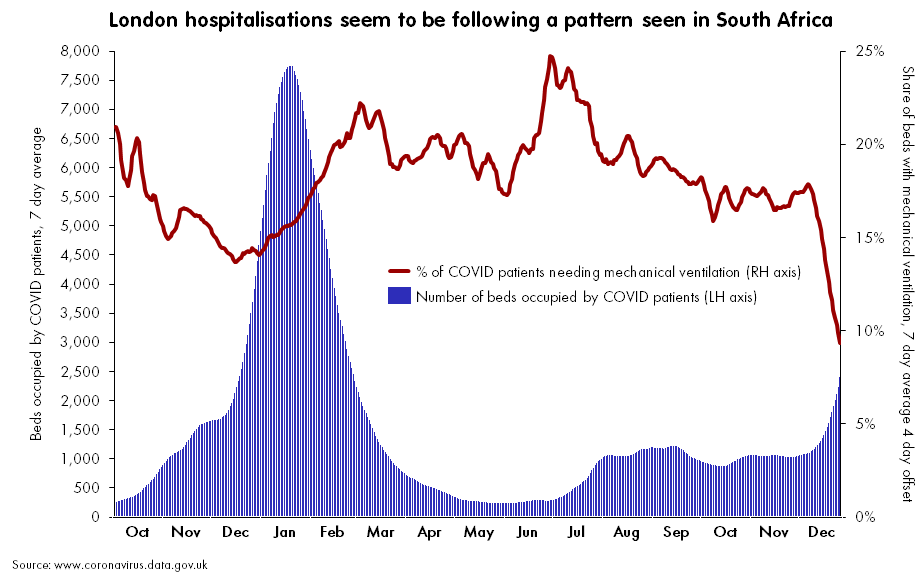
- Evidence that Omicron is less likely to cause severe symptoms continues to mount. A combination of real-world hospitalization and lab data continue to suggest that Omicron is less likely to cause severe COVID-19 symptoms than past coronavirus variants. The hospitalization data: in Omicron hotspots, hospitalization numbers are not rising at the same rate as case numbers, nor are the numbers of patients who require intensive care or ventilators. “Despite steep rises in cases and patients, the number on ventilators has barely risen,” wrote Financial Times data journalist John Burn-Murdoch in a recent thread about U.K. data.
- And the lab data: a growing number of studies show that Omicron is less capable of infecting patients’ lungs compared to past variants—meaning the worst respiratory symptoms are rarer. At the same time, people who catch Omicron after gaining immunity from vaccination and/or prior infection are protected against severe symptoms thanks to T cells and other aspects of immune system memory. Note that, however, we still don’t know about the risk of Long COVID following an Omicron case.
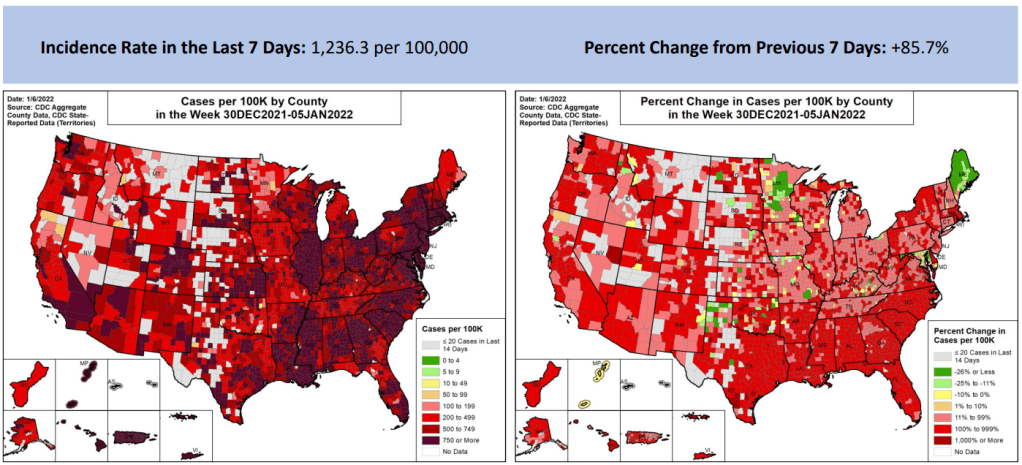
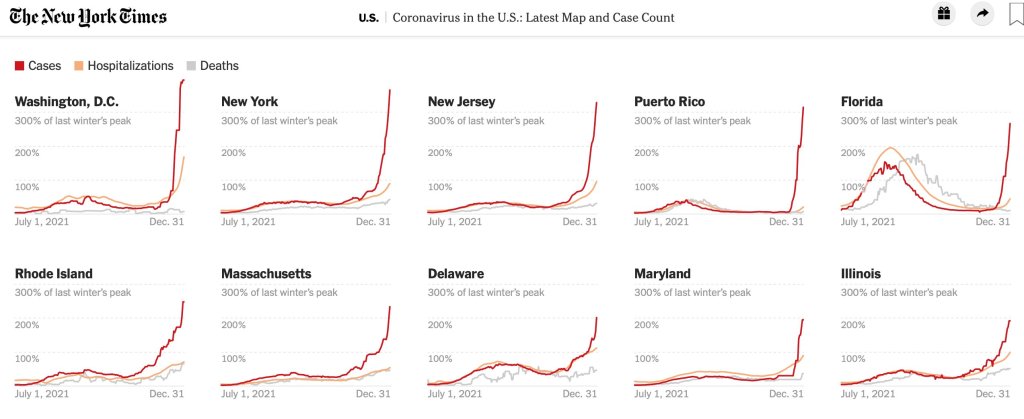
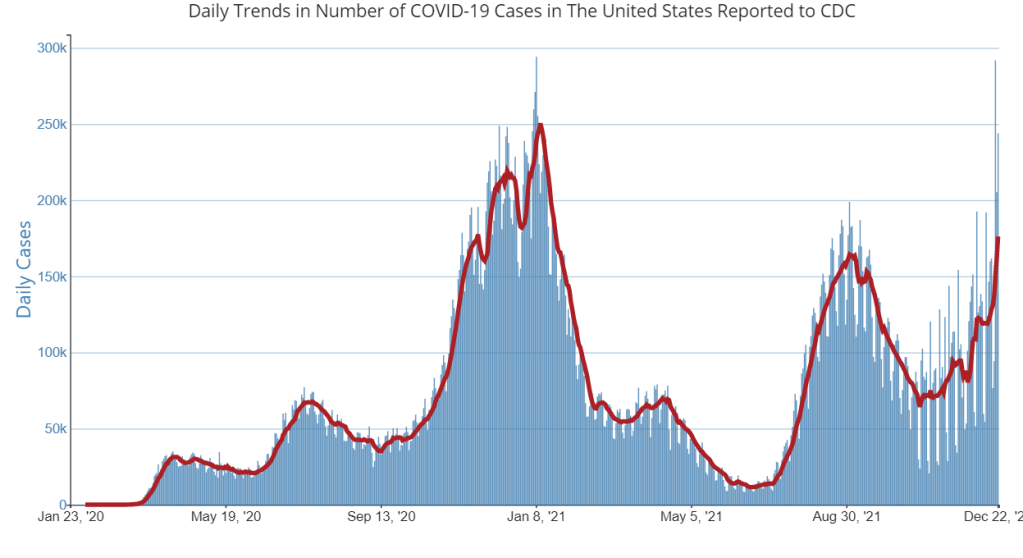
- Still: U.S. Hospitals are now incredibly overwhelmed with Omicron and Delta cases. In the U.S. so far, the “decoupling” phenomenon (in which hospitalizations and ICU admissions don’t rise as fast as cases) has been less visible than in other countries hit by Omicron. Several states have already set hospitalization and/or ICU records during the Omicron surge. This is likely because many parts of the U.S. have lower vaccination rates than other countries like the U.K. At the same time, accounts from hospital workers show the toll that this surge is taking: “Thankfully the Covid patients aren’t as sick. BUT there’s SO many of them,” wrote NYC ER doctor Dr. Craig Spencer in a recent Twitter thread.
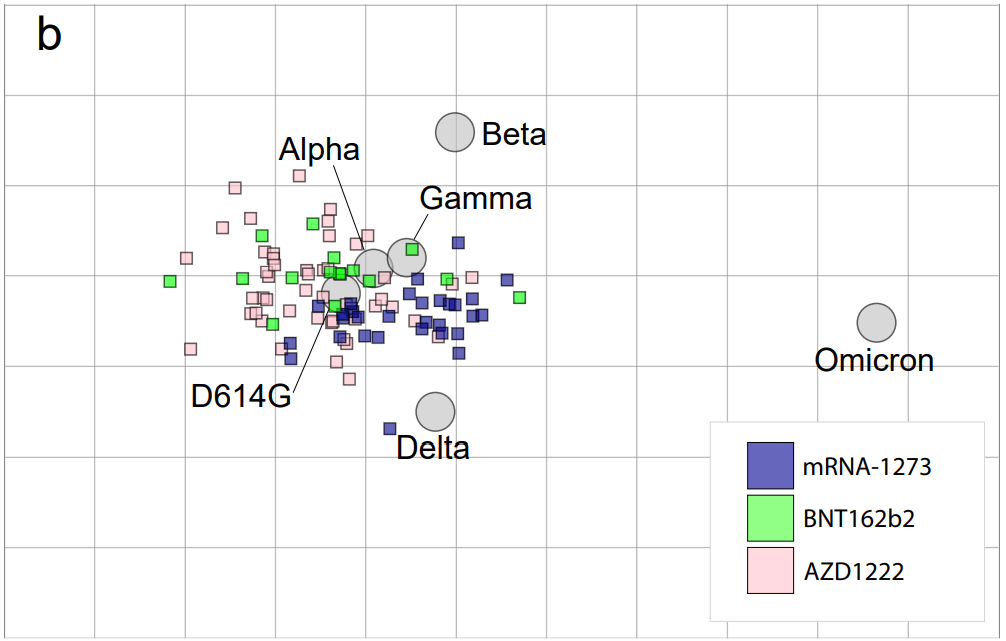
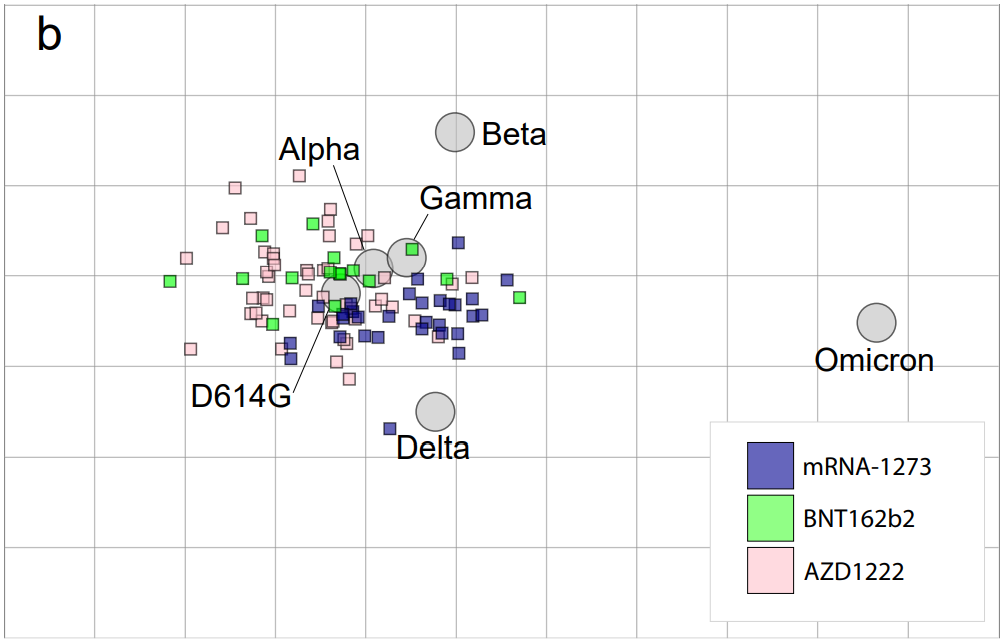
- Omicron has more antigenic drift than any other variant. “Antigenic drift” is a virology term referring to the small mutations in virus genetic material that cause these viruses to change slowly over time. As I noted in early Omicron updates, this variant didn’t evolve out of Delta (as many experts were expecting) but rather showed up seemingly out of nowhere; it might have emerged from a part of the world with limited variant surveillance, an immunocompromised person, or even an animal host. We don’t know Omicron’s origin yet, but we now know that it is further apart, genetically speaking, from the original coronavirus than any other variant so far.
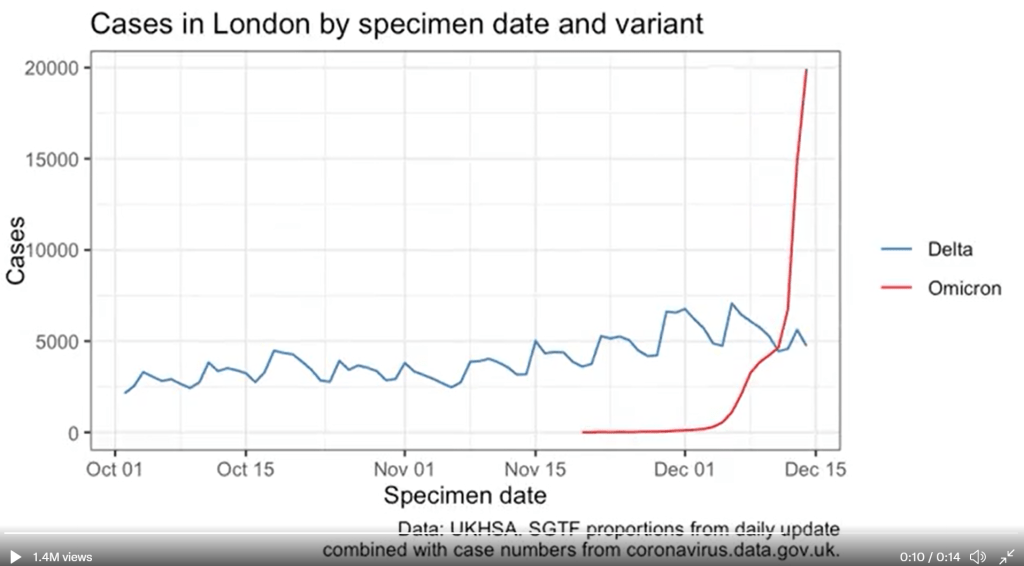
- London’s Omicron surge may have peaked. According to U.K. data, both case numbers and hospital admission numbers have slowed in their increases, the Washington Post reports. “For the moment, we can probably say London appears to be over the worst,” U.K. hospital executive Chris Hopson said last week. Other U.K. health officials are more skeptical though, according to the Post: while case numbers are falling for teenagers and younger adults, London is still reporting increasing cases among seniors.
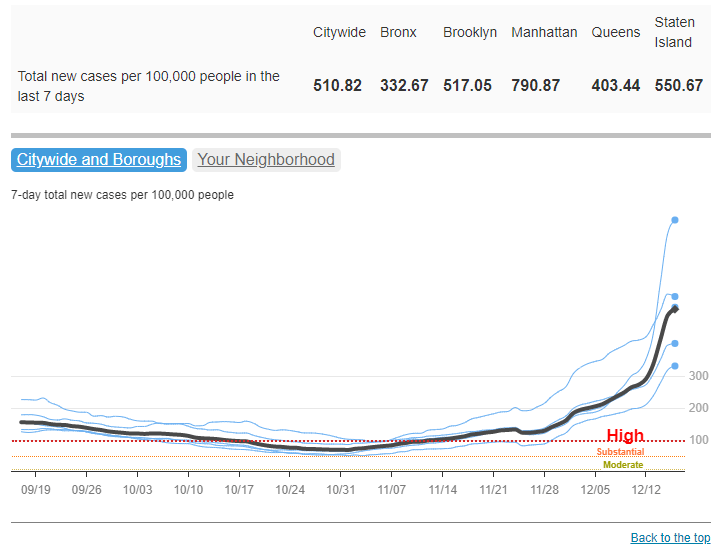
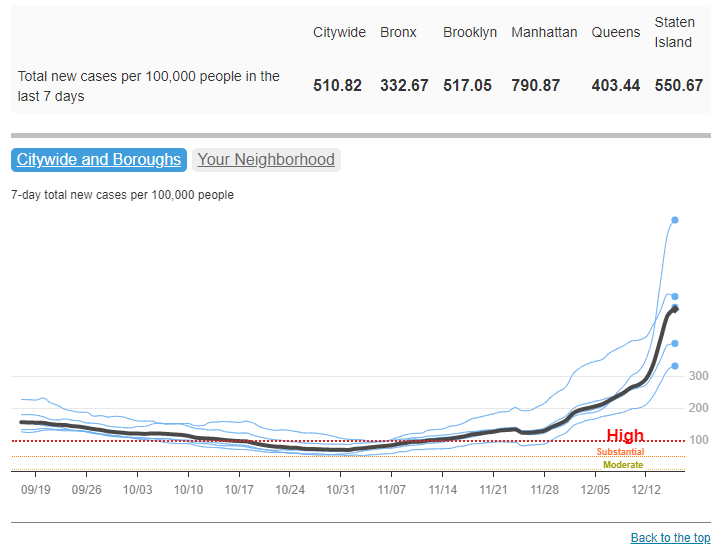
- New York City also might be on the verge of peaking. Another tentative peak report: data from NYC’s health department suggest that case numbers might be starting to fall in the city. The citywide seven-day average for new cases fell from 3,261 per 100,000 people on January 2 to 2,754 per 100,000 on January 4, and NYC’s positivity rate is also trending down. Reduced COVID-19 testing over New Years and other reporting uncertainties are likely playing a role here, but still—NYC cases jumped right back up after Christmas, but haven’t yet jumped up after New Years. I am cautiously optimistic!
- New research maps out South Africa’s intense Omicron wave. This recent study caught my eye when it was published in Nature this week through accelerated approval. Nearly 100 scientists in South Africa, Botswana, the U.S., Switzerland, the U.K., and other countries collaborated to analyze Omicron’s genetic makeup and the variant’s rapid spread through South Africa, including its ability to cause breakthrough cases and reinfect people who’ve previously had COVID-19. The paper is just one example of the immense collaboration that has taken place over the past month as scientists work to quickly understand this variant. Thank you, scientists!