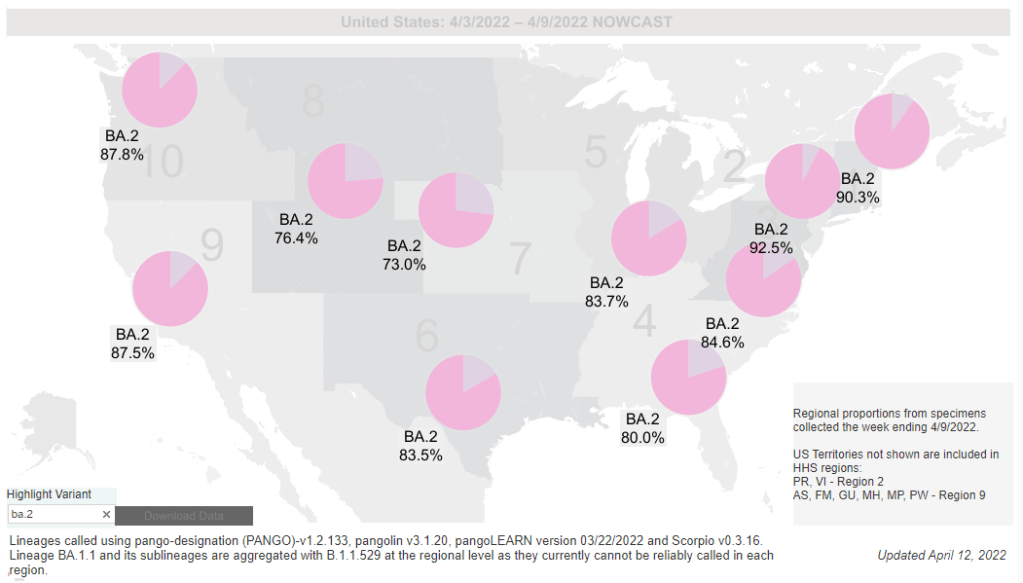
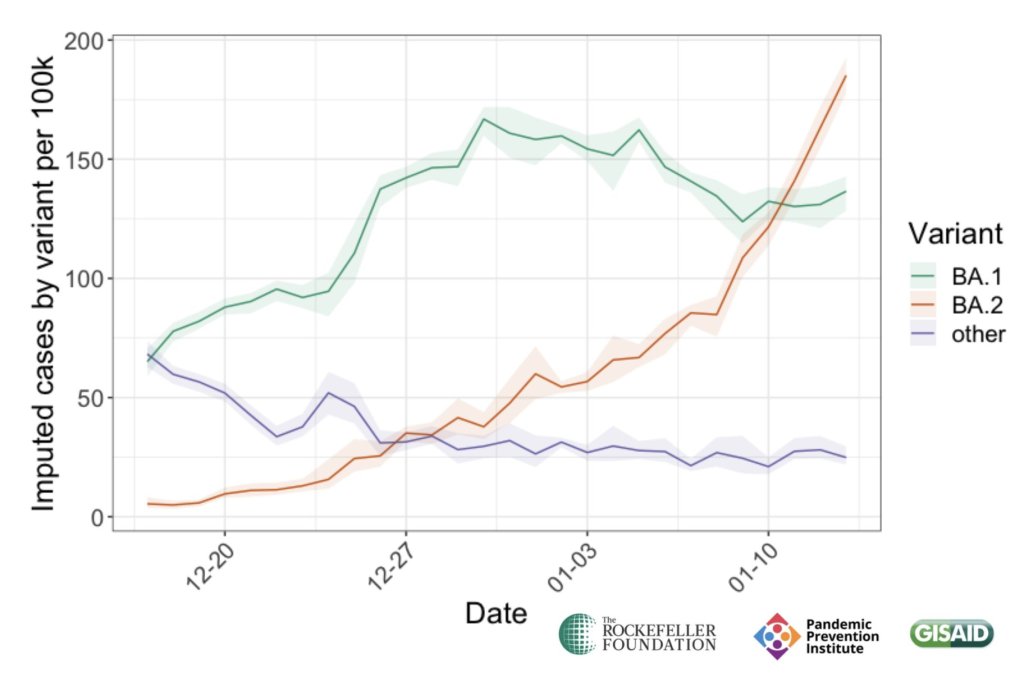
BA.2 levels are particularly high (93% prevalence) in the New York/New Jersey region, and new sublineages have recently been identified in New York. Chart via the CDC.
As though it’s not already confusing enough to distinguish between Omicron BA.1 and BA.2, more sublineages have popped up in recent weeks as Omicron continues to spread and mutate. Here are two that I’m watching, though they don’t seem to be major causes for concern at this time.
BA.2 sublineages in New York
Last week, the New York State Department of Health announced that it has identified new sub-variants of BA.2, called BA.2.12 and BA.2.12.1, through testing and sequencing. The BA.2 lineage overall accounts for the vast majority of cases in New York, and these two new strains are causing over 90% of new cases in the central part of the state.
These two sublineages seem to be spreading even faster than original BA.2 in New York, with a growth advantage of about 25%—perhaps explaining in part why the state is once again seeing higher case rates than other parts of the country. It’s unclear so far whether these BA.2 offshoots will have any impact on severity or vaccine effectiveness; the health department is looking into this.
Also worth noting: New York has a more robust variant surveillance system than a lot of other states. It’s very possible that Omicron is mutating elsewhere in the country, too; but those potential sublineages haven’t been identified yet.
The number of cases so far may seem to be insignificant compared with the steep Omicron peak of the winter, but “we’re essentially back at levels of case rates back to the Delta wave,” said Eli Rosenberg, deputy director for science at the New York State Department of Health. “This would have been a very significant wave already by last year’s standards.”
XE recombinant in the U.K. and other countries
This new offshoot hasn’t been identified in the U.S. yet, but it deserves some attention. Essentially, BA.1 and BA.2 have combined—likely in regions or even in individual people that are experiencing simultaneous infections of both strains—and formed what scientists call a “recombinant” variant, with some genetic material from both. The BA.1/BA.2 conglomerate has been labeled XE.
According to research so far, XE may have a slight growth advantage over BA.2. The World Health Organization (WHO) estimated that XE is about 10% more transmissible than BA.2, but further study is needed to confirm this number. Over 600 XE cases have been identified in the U.K., according to TIME, along with smaller numbers in India, Thailand, and other countries.
Scientists aren’t particularly concerned about XE at this point because it hasn’t been spreading rapidly and outcompeting other variants, like the original Omicron did in the winter. But agencies like the U.K.’s Health Security Agency and the WHO are monitoring for any worrying signals.
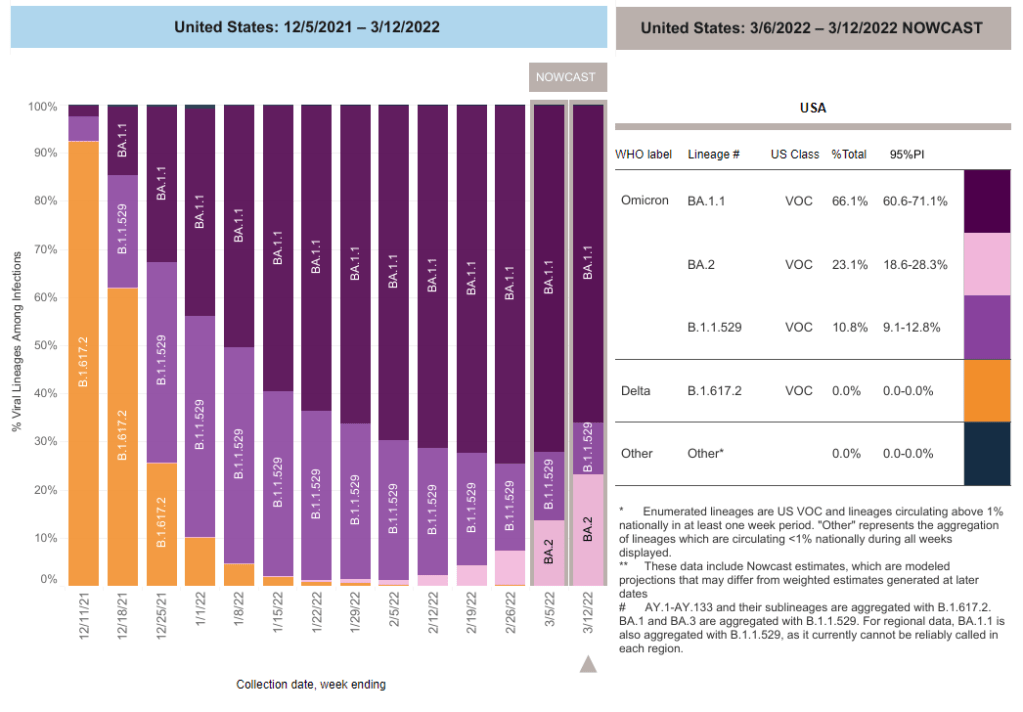
BA.2 caused about one in four U.S. COVID-19 cases in the week ending March 12, according to CDC estimates.
Two years into the pandemic, we now know some basic truisms about the coronavirus. For example: outdoor events are always safer than indoor events; older age is the most significant risk factor for severe symptoms; hospitalization trends typically follow case trends by a couple of weeks; and whenever Europe has a new surge, the U.S. is likely to also see a surge in the next month or so.
That last truism is particularly relevant right now, because Europe is experiencing a new surge. Cases are increasing in the U.K., Germany, the Netherlands, and many other countries. The new surge is likely due to European leaders’ decisions to end all COVID-19 safety measures in their countries, combined with the rise of Omicron sublineage BA.2.
As BA.2 prevalence increases here in the U.S.—and our leaders also end safety measures—we seem poised to follow in Europe’s footsteps once again. But a BA.2 surge is likely to look different from the intense Omicron surge that we experienced in December and January, in part because of leftover immunity from that Omicron surge.
Let’s go over what we know about BA.2, and what might happen in the next few weeks.
What is BA.2?
It’s important to note that this isn’t a new variant, at least not compared to the original Omicron strain. As I noted in a FAQ post about this strain back in January, South African scientists who originally characterized Omicron in November 2021 identified three sub-lineages: BA.1, BA.2, and BA.3.
BA.1 spread rapidly through the world, driving the surge that we experienced here in the U.S. in December through February. But BA.2, it turns out, is actually more transmissible than BA.1—allowing it to now outcompete that strain and contribute to case increases in countries that already faced major BA.1 surges.
How does BA.2 differ from BA.1, or original Omicron?
The main difference between these two strains is that BA.2 is more contagious: scientists estimate that BA.2 is about 30% more transmissible than other Omicron strains, if not more. (Note that this is a smaller difference than Omicron’s advantage over Delta and other earlier variants.)
In a recent report, the U.K. Health Security Agency estimated that someone infected with BA.2 would infect about 13.6% of their households and 5.3% of contacts outside of their households, compared to 10.7% of households and 4.2% outside contacts for other Omicron strains. The modest difference between these rates demonstrates why BA.2 is not outcompeting other Omicron strains as quickly as Omicron outcompeted Delta a couple of months ago.
Another notable feature of BA.2 is that, unlike BA.1, it can’t be identified with a PCR test. BA.1 has a mutation called S drop-out, which causes a special signal in PCR test results, allowing the variant to be flagged without sequencing; BA.2 doesn’t have this mutation. To be clear, a PCR test will still return a positive result for someone who is infected with BA.2—it’ll just take an additional sequencing step to identify that they have this particular strain.
Finally, one major challenge during the Omicron BA.1 surge has been that two of the three monoclonal antibody treatments used in the U.S. did not work well for people infected with Omicron. BA.2 may exacerbate this challenge, as some studies have suggested that the third treatment—called sotrovimab—continued working against BA.1, but may not hold up against BA.2. Luckily though, Eli Lilly (which developed one of the treatments that failed for BA.1) has produced an updated monoclonal antibody cocktail that does work for both Omicron strains.
How is BA.2 similar to BA.1, or original Omicron?
Two major pieces of good news here: 1) our existing COVID-19 vaccines work similarly well against BA.2 as they do against BA.1, and 2) prior infection with BA.1 seems to be protective against infection with BA.2.
Essentially, studies are showing that the two strains are close enough in their genetic profiles that antibodies from a BA.1 infection will provide some immunity against a BA.2 infection. And the same thing goes for vaccination, at least when it comes to protection against severe disease. A recent CDC study showed that, even during the Omicron surge, COVID-19 patients who had received three vaccine doses were far less likely to require mechanical ventilation or die from the disease than those who weren’t vaccinated.
There’s a flip side to this, though: for both BA.1 and BA.2, prior infection with a previous variant is not very protective against an Omicron infection. CDC seroprevalence data suggest that between 40% and 45% of Americans got infected with BA.1 during the winter surge; this means the remaining 55% to 60% of the population is susceptible to BA.2. Vaccines protect against severe disease and death from BA.2, but they don’t protect against BA.2 infection to the degree that they did against past variants.
This means that in terms of protection against infection, populations with high rates of vaccination or prior infection remain essentially naive to it. Though vaccines and prior infections still protect from severe disease and death (thanks to T-cell protection). 3/ pic.twitter.com/gmwlk2l7ZV
— Prof Francois Balloux (@BallouxFrancois) March 19, 2022
BA.2 and BA.1 are also similar in their severity. Both strains are less likely to cause severe disease than Delta; BA.1 had a 59% lower risk of hospital admission and 69% lower risk of death than Delta in the U.K., according to a new paper published this week in the Lancet.
It’s important to remember, however, that Delta was actually more severe than other variants that preceded it. As a result, “Omicron is about as mild/severe as early 2020 SARSCoV2,” wrote computational biologist Francois Balloux in his Twitter thread (referring to both BA.1 and BA.2).
What are the warning signs for a BA.2 surge in the U.S.?
First of all, many U.S. experts consider case increases in Europe to be an early indicator of increases in the U.S. As I said at the top of the post, Europe is seeing a surge right now, and many of the countries reporting case increases have estimated over 50% of their cases are caused by BA.2.
In the U.S., our BA.2 levels are lower: the CDC’s most recent estimates suggested that BA.2 was causing about 23% of new cases nationwide as of March 12. If BA.2 continues growing at the same rate we’ve seen in recent weeks, we have one or two more weeks before this variant hits 50% prevalence in the U.S.
“The tipping point seems to be right around 50%,” Keri Althoff, an epidemiologist at Johns Hopkins Bloomberg School of Public Health, told CNN. “That’s when we really start to see that variant flex its power in the population” as far as showing its severity.
At the same time, several Asian countries are also seeing major BA.2 surges at the moment. For example, Hong Kong was able to deal with early Omicron cases earlier in the winter, former COVID Tracking Project lead Erin Kissane pointed out in her Calm Covid newsletter; but now, the territory is facing a terrible BA.2 wave, driving what is now the world’s highest case fatality rate.
NEW: I’m not sure people appreciate quite how bad the Covid situation is in Hong Kong, nor what might be around the corner.
First, an astonishing chart.
After keeping Covid at bay for two years, Omicron has hit HK and New Zealand, but the outcomes could not be more different. pic.twitter.com/1Ol4HHs9kT
Here in the U.S., we’re also seeing warning signals in the form of rising coronavirus levels in wastewater. (Wastewater is considered an early indicator for surges, because coronavirus material often shows up in sewer systems before people begin to experience symptoms or get tested.) About one-third of sewershed collection sites in the CDC’s wastewater monitoring network are reporting increased virus prevalence in the two-week period ending March 15.
The CDC wastewater data must be interpreted cautiously, however, as this surveillance network is biased towards states like Missouri and Ohio, which have over 50 collection sites included in the national network. 12 states still do not have any collection sites in the network at all, while 23 states have fewer than 10. This recent Bloomberg article includes more context on interpreting wastewater data.
New York City is one place that’s reporting increased viral levels in wastewater, at the same time as the city health department reports that case numbers have plateaued—or may even be ticking up. An excellent time to loosen all mask and vaccination requirements, am I right?
What might a BA.2 surge in the U.S. look like?
Between the warning signals from Europe and the newly-lax safety measures throughout the U.S., it seems very likely that we will see a BA.2 surge in the coming weeks. The bigger question, though, is this surge’s severity: to what extent will it cause severe disease and death?
As I mentioned above, estimates suggest that about 40% to 45% of Americans have some Omicron antibodies from an infection earlier in the winter. At the same time, about 65% of the population is fully vaccinated and 45% of those fully vaccinated have received a booster shot, according to the CDC.
That’s a lot of people who are protected against severe COVID-19 symptoms, if they get infected with BA.2. But the U.S. has lower vaccination coverage than other countries, particularly when it comes to boosters. For example, in the U.K., 86% of eligible people are fully vaccinated and 67% are boosted, according to CNN. These lower vaccination rates contributed to the U.S.’s high mortality rate during the Omicron surge compared to other wealthy countries.
While the vaccines offer great protection, the U.S. appears to have given up on many other COVID-19 safety measures, like masks, social distancing, and limits on in-person gatherings. Without reinstating some of these measures, we would essentially be left without any tools to slow down the spread of BA.2; and even if some states and cities put safety measures in place, they’ll likely face more pushback now than they did in earlier surges.
To quote from Kissane’s newsletter:
In practical terms, with work and school happening in-person and without high-filtration (or any) masks or serious ventilation requirements in the US and most of Europe, governments in North America and Europe have made increased covid exposure essentially mandatory for most citizens.
I want to emphasize that for most vaccinated people, this increased risk probably won’t be a huge deal even if BA.2 causes a new case surge—they’ve either already racked up enough immunity to fight off BA.2 or they’ll be sick for a week.
One big caveat to this, though: we don’t have great data yet on how Omicron (or BA.2 specifically) might contribute to Long COVID rates; collecting data on this condition is very challenging and takes a lot of time. Studies suggest that vaccination reduces an individual’s risk of long-term symptoms if they get infected, but it does not eliminate this risk.
What can you do to prepare for this potential surge?
Here are a few things that I’m doing to prepare for a potential BA.2 surge in the coming weeks:
Promoting vaccination—particularly booster shots—to family members and friends.
Stocking up on good-quality masks (i.e. N95s and KN95s) and rapid tests. (Reminder, order a new round of free tests from covidtests.gov if you haven’t yet!)
Researching my options for COVID-19 treatments (antiviral pills and monoclonal antibodies) in the event that I get infected.
Getting tested frequently, particularly before attending indoor events (such as gathering with a few other friends, or going out to a movie theater.)
Watching wastewater and case trends in my area, and preparing to cut down on riskier behaviors if(/when) cases start rising.
I don’t know what BA.2 will mean for the US.
I do know this:
It hinges on vaccination/booster rates *now*.
So: 👆+
4th doses & Evusheld for immunocompromised ASAP, if not done.
Know where you’d get Paxlovid & Sotrovimab.
Order rapids now.
Get N95s or best possible now.
— Jeremy Faust MD MS (ER physician) (@jeremyfaust) March 16, 2022
As always, if you have any COVID-19 questions (about BA.2 or otherwise) that you’d like me to address, please reach out.
In the past week (February 19 through 25), the U.S. reported about 526,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 75,000 new cases each day
160 total new cases for every 100,000 Americans
38% fewer new cases than last week (February 12-18)
Last week, America also saw:
42,000 new COVID-19 patients admitted to hospitals (13 for every 100,000 people)
12,000 new COVID-19 deaths (3.6 for every 100,000 people)
100% of new cases are Omicron-caused (as of February 19)
An average of 200,000 vaccinations per day (per Bloomberg)
The U.S. is now on week six of falling COVID-19 case numbers nationwide. New cases fell 38% from last week to this week, and are down 87% from one month ago. This is also the first week that the country has reported a daily new case average under 100,000 since early December.
Hospitalizations also continue to fall, with about 30% fewer new COVID-19 patients entering U.S. hospitals this week compared to last week. And death numbers have also begun to come down—though they are still high, with over 1,500 people dying of COVID-19 each day.
Case numbers are falling in every single U.S. state; five states and D.C. reported fewer than 100 new cases for every 100,000 residents in the past week, according to the latest Community Profile Report: Washington, Nebraska, Maryland, Nevada, and Ohio. Last week, Maryland was the first state to report case numbers below the CDC’s old high transmission threshold. (The new threshold is higher, which I’ll get into later this issue.)
To quote prolific COVID-19 data commentator (and my former COVID Tracking Project colleague) Conor Kelly, whose chart is featured above: “There’s not all that much interesting to report on with COVID data right now. Things are getting better fast everywhere. It’s just a question of how long it continues.”
That continuation depends largely on variants. As the Omicron surge recedes, how long will we see these decreases (or a plateau at low numbers) before a new variant drives another surge?
One key factor here is BA.2, the Omicron sub-lineage that has been slowly gaining ground in the U.S. over the past month as it is more transmissible than original Omicron. And I do mean slowly: according to CDC estimates, BA.2 went from causing an estimated 2% of new cases in the week ending February 12 to 4% in the week ending February 19. It seems to be having a limited impact on the country’s case decrease right now, but we’ll see if that changes in the coming weeks.
Meanwhile, America’s vaccination campaign is stalling. According to the Associated Press: “The average number of Americans getting their first shot is down to about 90,000 a day, the lowest point since the first few days of the U.S. vaccination campaign, in December 2020.” More investment into reaching people who remain unvaccinated (and unboosted) is necessary if we want to be prepared for potential future surges.
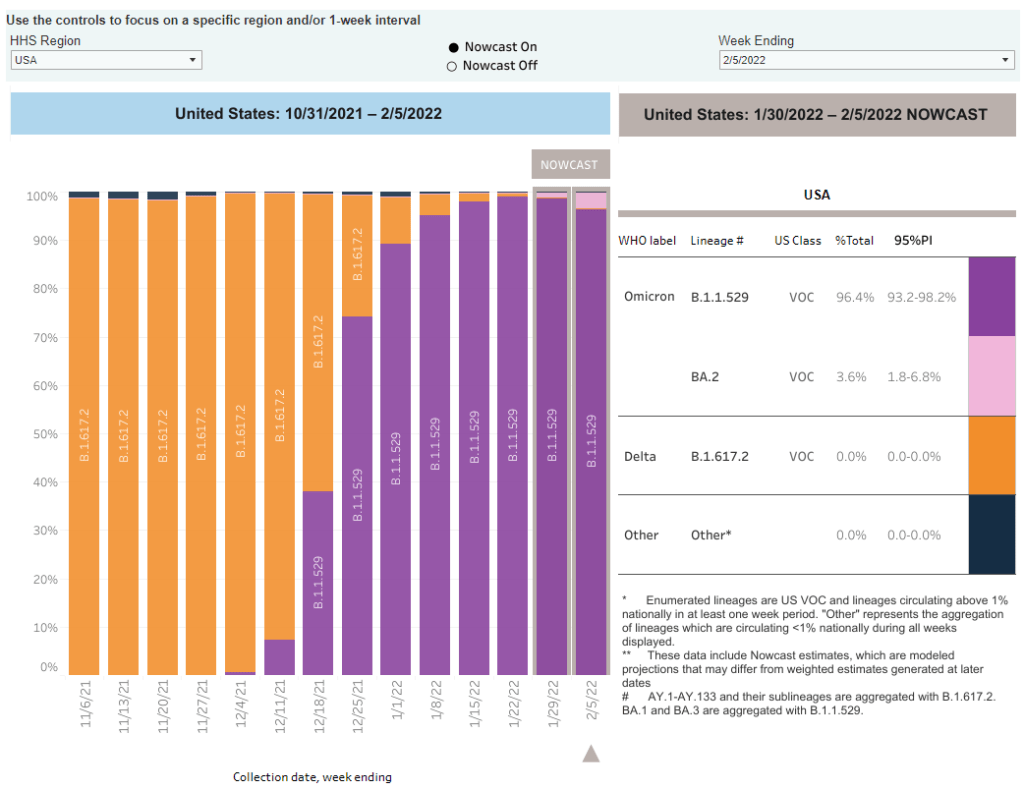
The CDC added BA.2 to its variant prevalence estimates. As I mentioned in today’s National Numbers post, the CDC is now splitting out its estimates of Omicron prevalence in the U.S. into original Omicron, also called B.1.1.529 or BA.1, and BA.2—a sister strain that’s capable of spreading faster than original Omicron. BA.2 has become the dominant variant in some parts of Europe and Asia, but seems to be present in the U.S. in fairly low numbers so far: the CDC estimates it caused about 3.6% of new cases nationwide in the week ending February 5, with a 95% confidence interval of 1.8% to 6.8%. The remainder of new cases last week were caused by original Omicron.
CDC describes its expanded genomic surveillance efforts in an MMWR study released this week. Between June 2021 and January 2022, the agency has extended its ability to monitor new variants spreading in the U.S., incorporating public repositories like GISAID into CDC data collection and developing modeling techniques that can produce more timely estimates of variant prevalence. (Remember: all variant data are weeks old, so the CDC uses modeling to predict the present.) According to the MMWR study, genomic sequencing capacity in the U.S. tripled from early 2021 to the second half of the year.
Vaccine effectiveness from a booster shot wanes several months after vaccination. In another MMWR study released this week, the CDC reports on mRNA vaccine effectiveness after two and three doses, based on data from a hospital network including hundreds of thousands of patients in 10 states. During the U.S.’s Omicron surge, researchers found, vaccine effectiveness against COVID-19 hospitalization was 91% two months after a third dose—but declined to 78% four months afterward. It’s unclear whether this declining effectiveness is a direct result of Omicron getting past the vaccine’s defenses, or whether we’d see similar declines with other variants. Also, the CDC’s findings are not stratified by age or other factors that make people more vulnerable to severe COVID-19.
Updated monoclonal antibody treatment from Eli Lilly gets FDA authorization. During the Omicron surge, one challenge for healthcare providers has been that, out of three monoclonal antibody treatments authorized by the FDA, only one retained effectiveness against this variant. (Monoclonal antibody treatments provide a boost to the immune system for vulnerable patients.) This week, however, the FDA authorized an updated version of Eli Lilly’s treatment that does work against Omicron, including against the BA.2 lineage. The federal government has purchased 600,000 courses of this new treatment.
More data released on South Africa’s mild Omicron wave. A new paper published in JAMA this week, from researchers at a healthcare provider in South Africa, compares COVID-19 hospitalizations during the Omicron surge to past surges. Among patients who visited the 49 hospitals in this provider’s network, about 41% of those who went to an emergency department with a positive COVID-19 test were admitted to the hospital during the Omicron surge—compared to almost 70% during South Africa’s prior surges. The paper provides additional evidence that Omicron is less likely to cause severe COVID-19 than past variants, though this likelihood is tied in part to high levels of vaccination and past infection in South Africa and other countries.
Omicron has been identified in white-tailed deer. New York City was an early Omicron hotspot in the U.S.; and the variant has been passed onto white-tailed deer in Staten Island, according to a new preprint posted this week (and not yet peer-reviewed). Scientists have previously identified coronavirus infections in 13 states, but finding Omicron is particularly concerning for researchers. “The circulation of the virus in deer provides opportunities for it to adapt and evolve,” Vivek Kapur, a veterinary microbiologist who was involved in the Staten Island study, told the New York Times.
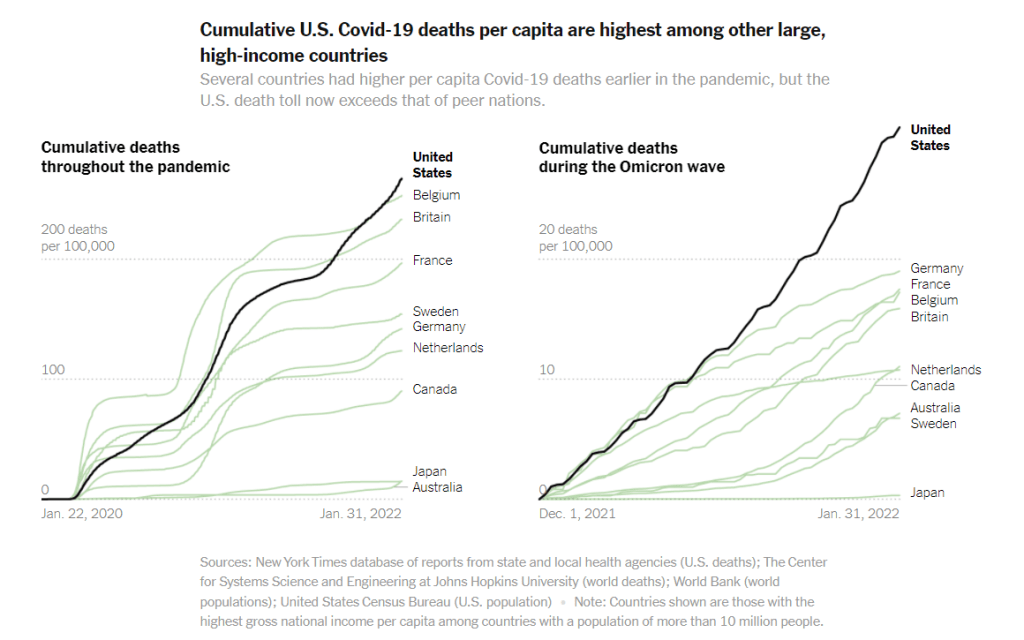
COVID-19 deaths during the Omicron wave have been much higher in the U.S. than in other similarly wealthy countries, according to a New York Times analysis.
Just a few updates for this week:
Scientists are still learning about BA.2, the more-transmissible Omicron offshoot. There haven’t been many major updates about BA.2 since last week, when I wrote this FAQ post; but this STAT News article by Andrew Joseph provides a helpful summary of what we know so far. The article explains that BA.2 clearly has a transmission advantage over BA.1 (and has now become the dominant variant in a few countries), but BA.1 may have spread around the world due to chance and some well-placed superspreading events. Notably, the CDC is not yet splitting out its Omicron prevalence estimates into BA.1 and BA.2, so we don’t have a great sense of how much this sub-lineage is spreading in the U.S.
More data indicates immune system memory remains strong against Omicron. In previous Omicron update posts, I’ve noted that, while vaccinated people are more likely to have a breakthrough case with Omicron than with past variants, vaccination is still highly protective against severe symptoms. A new study published in Nature this week further affirms this protection; researchers found that 70% to 80% of T cell response to Omicron was retained in people who were vaccinated or tested positive on antibody tests, compared to past variants. (T cells are key pieces of immune system memory response.)
Similarly, more data backs up the importance of vaccination to protect against severe disease during the Omicron era. The CDC released more MMWR studies this week showing that fully vaccinated and boosted Americans were less likely to require hospitalization or intensive care during the Omicron surge compared to the unvaccinated. For example, in Los Angeles County, California, hospitalization rates among unvaccinated people were 23 times higher than rates among those fully vaccinated with a booster, and five times higher than those vaccinated without a booster.
Omicron is too transmissible for school testing programs to keep up. I’ve previously reported on the challenges of K-12 COVID-19 testing programs, including the difficulty of setting up public health logistics, getting enough tests, and increasing polarization of testing. During the Omicron surge, these challenges have been magnified—to the point that some states, including Utah, Vermont, and Massachusetts, have suspended testing programs, POLITICO reported this week. I hope to see some of these programs resume after the surge is over.
The U.S.’s death toll during the Omicron surge has been far higher than in similarly wealthy nations. A new analysis from the New York Timescompares the death toll in the U.S. from December 2021 through January 2022, adjusted for population, to death tolls in peer wealthy nations like Germany, Canada, Australia, and Japan. The comparison is striking: “the share of Americans who have been killed by the coronavirus is at least 63 percent higher than in any of these other large, wealthy nations,” the NYT reports. This difference is largely because the U.S. is less vaccinated than these other countries, particularly when it comes to booster shots and vaccinations among seniors.
Globally, cases during the Omicron surge surpassed all of 2020. “In the 10 weeks since Omicron was discovered, there have been 90 million COVID-19 cases reported — more than in all of 2020,” said Tedros Adhanom Ghebreyesus, Director-General of the World Health Organization, at a press conference last week. In a Twitter thread reporting from the press conference, STAT’s Helen Branswell noted that the WHO is concerned about countries “opening up” and lifting COVID-19 restrictions before their case numbers are actually low enough to warrant these measures.
1. Amazing statistic: In the 10 weeks since Omicron was discovered, there have been 90M #Covid cases reported — more than in all of 2020, says @drtedros at today's @WHO press conference.
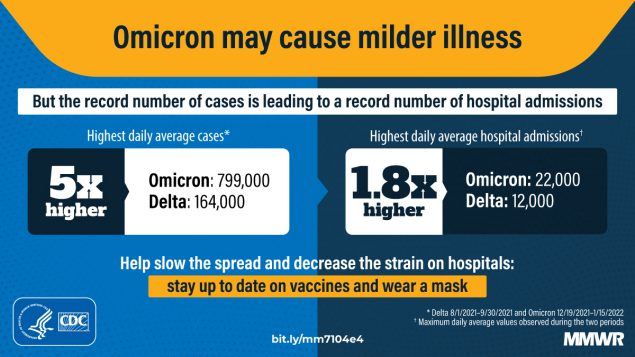
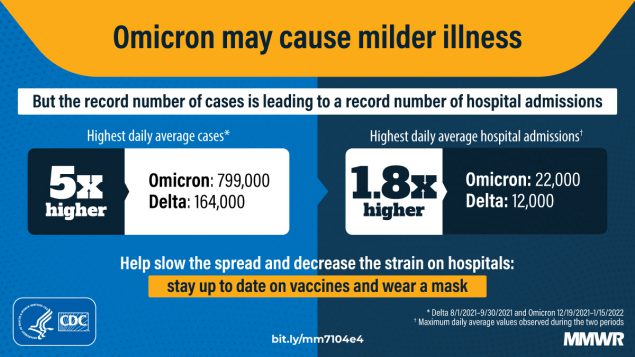
A new CDC analysis found that Omicron led to record hospitalizations, but lower levels of ICU admissions and other indicators of the most severe disease compared to past surges. Chart via CDC MMWR.
While BA.2 has dominated the news cycle this week, we’re still learning more about—and seeing policy shifts due to—the original Omicron strain, BA.1. Here are a few major updates:
Omicron is causing 100% of new COVID-19 cases in the U.S. According to the CDC’s latest update of its variant prevalence estimates, Omicron caused more than 99% of new COVID-19 cases in the country for the second week in a row: there was a slight increase from 99.4% of new cases in the week ending January 15 to 99.9% in the week ending January 22. The remaining 0.1% of cases are caused by Delta. The CDC is not yet distinguishing between BA.1 and BA.2 in its estimates, but will likely start doing so in the coming weeks.
ICU admissions and other indicators of severe COVID-19 symptoms were lower during the Omicron surge than during previous surges in the U.S. The CDC released another round of studies presenting Omicron’s impact on the healthcare system last week, including this report focusing on disease severity. CDC researchers analyzed data from three hospital surveillance systems and an additional large database; while the peak of new COVID-19 cases was five times higher during the Omicron surge than the Delta surge, they found, the peak of hospital admissions was only 1.8 times higher. And ICU admissions, the average stay length for hospitalized COVID-19 patients, and death rates were all lower during the Omicron surge than in the Delta and winter 2020-2021 surges.
Pfizer and BioNTech have started a clinical trial of an Omicron-specific vaccine. Quickly after Omicron was identified, both Pfizer and Moderna started updating their vaccines for this variant and investigating whether such Omicron-specific shots would be necessary. Pfizer is now entering a new clinical trial with its Omicron-specific shot, along with its vaccine development partner BioNTech, according to Reuters. Trial participants will include about 1,400 people who received third doses from Pfizer’s current COVID-19 vaccine regimen three to six months earlier. Pfizer intends to study the Omicron-specific shot’s safety and effectiveness against this variant.
The FDA recommends that U.S. facilities stop using monoclonal antibody treatments that don’t work well against Omicron. Speaking of Omicron-specific drugs: the Food and Drug Administration (FDA) announced this week that the agency is limiting use of two monoclonal antibody treatments, made by Regeneron and Eli Lilly. Both treatments, which boost patients’ immune systems by providing them with lab-made antibodies, worked well at reducing severe symptoms for past variants but have less of an impact on Omicron infections. As a result, healthcare providers should “ limit their use to only when the patient is likely to have been infected with or exposed to a variant that is susceptible to these treatments,” the FDA says. A third monoclonal antibody treatment, along with other drugs (including Pfizer’s hard-to-find pill), do work well against Omicron.
Omicron has a short incubation period, so test timing is key. As I’ve written in the past, Omicron infections tend to move more quickly than infections with past variants: people can go from an exposure to symptoms within three days, rather than four or five. As a result, there’s less time to catch an infection before becoming contagious; but at the same time, rapid tests may give negative results in those early days of an infection, before patients have built up enough of a viral load for an antigen test to identify the infection. A recent New York Times article summarizes the science on how Omicron infections compare to past variants and provides recommendations on testing. For instance: “many experts now recommend taking a rapid test two to four days after a potential exposure,” and ideally testing twice about a day apart.
Some experts are optimistic that we could see a COVID-19 lull after Omicron surges.Last week, I shared a STAT News article explaining that, thanks to high levels of population immunity, the U.S. might have “a bit of a break from the Covid roller coaster” after our Omicron surge ends in the coming weeks. Despite BA.2 concerns, Dr. Hans Henri Kluge, WHO’s regional director for Europe, shared a similarly optimistic view in a statement last week. “The pandemic is far from over, but I am hopeful we can end the emergency phase in 2022 and address other health threats that urgently require our attention,” he said.
Although deadly new Covid variants could emerge, I'm more optimistic today than at any point since the pandemic began. Here’s why. 1/thread
An offshoot strain of the Omicron variant has been making headlines this week as it spreads rapidly in some European and Asian countries. While the strain, called BA.2 by virologists, has not yet been identified in the U.S. in large numbers, it’s already spreading here, too: scientists have picked it up in wastewater samples in some parts of the country.
This strain clearly has a growth advantage over the original Omicron strain (also called BA.1), but it’s not cause for major concern at this point. Scientists are working to identify whether BA.2 has a higher capacity for breaking through immunity from past infection or vaccination; so far, early data suggest that it does not significantly differ from BA.1 on this front, though it may have a slight advantage.
Here’s a brief FAQ on what we know about the strain so far.
When and where did BA.2 emerge?
I’ve been careful not to call BA.2 a “new strain” or a “new variant” here because it’s not actually new—at least, it’s not any newer than Omicron BA.1. When South African scientists first sounded the alarm about Omicron in late November 2021, BA.2 was already present among the country’s cases of this variant.
In fact, a paper from South African scientists describing the Omicron wave in their country, published in Nature in early January, specifies that the earliest specimen of BA.2 was sampled on November 17; the earliest specimen of BA.1 was sampled on November 8. Around the same time, South African scientists also identified a third lineage, called BA.3—this one hasn’t yet become a cause for concern.
Why are scientists concerned about BA.2?
In the past couple of weeks, epidemiologists have identified that BA.2 is spreading faster in some countries than BA.1, the original Omicron strain. This means BA.2 has what scientists call a “transmission advantage” over BA.1: it is capable of getting from person to person fast enough that it may be able to outcompete BA.1.
For example, in Denmark, BA.2 became the dominant strain in mid-January, taking over from BA.1. The takeover has coincided with an additional increase in COVID-19 cases in the country after Denmark’s Omicron wave initially appeared to peak a couple of weeks ago—but it’s hard to determine whether this second increase is solely due to BA.2 or also connected to an announcement that Denmark will end its COVID-19 restrictions on February 1.
This past week, the World Health Organization (WHO) announced that investigations into BA.2, including its potential virulence and ability to escape prior immunity, “should be prioritized independently (and comparatively) to BA.1.” The WHO has yet to designate BA.2 as a separate variant of concern from BA.1, however; at the moment, both strains are still included under the Omicron label.
How does BA.2 compare to BA.1, the original Omicron strain?
As I’ve explained in previous posts about the variant, Omicron has the most antigenic drift of any coronavirus variant identified thus far—meaning that it’s the most genetically different from the initial Wuhan version of the virus. Omicron BA.1 has about 60 mutations compared to the Wuhan strain, but BA.2 has even more: about 85 mutations, according to a recent Your Epidemiologist post.
BA.2 is clearly more transmissible than BA.1, as we’ve seen from its rapid spread in countries including Denmark, the U.K., France, the Netherlands, India, and the Philippines. Scientists estimate that “BA.2 may be 30% to 35% more transmissible than BA.1,” STAT News reports.
3/ In Denmark, BA.2 is spreading rapidly, despite BA.1 leveling off. This worrying trend is why scientists, including analysts at PPI like @ZacharySusswein & @KaitEJohnson9, are investigating. pic.twitter.com/ItsoO5jcJh
— Pandemic Prevention Initiative (@PPI_Insights) January 26, 2022
The question scientists hope to answer, then, is why BA.2 has this transmission advantage over BA.1. Do BA.2’s additional mutations lend it some adaptation in how it interacts with human cells, enabling faster spread? Or is BA.2 more capable of evading protection from past infection or vaccination compared to BA.1, leading it to cause more reinfections and breakthrough cases?
While we don’t know the answers to these questions yet, early data are indicating that there’s no major difference in disease severity between BA.1 and BA.2. In other words, BA.2 isn’t more likely to cause severe symptoms.
“There is no evidence that the BA.2 variant causes more disease, but it must be more contagious,” Danish Health Minister Magnus Heunicke said at a news conference last week, Reuters reported.
Why do some articles call BA.2 a “stealth variant?”
You might have seen some headlines referring to BA.2 as a “stealth variant” or a “stealth version of Omicron.” This is because of one major difference between BA.2 and BA.1: while BA.1 can be identified with a PCR test due to a key mutation that’s visible on PCR test results, BA.2 does not have this mutation.
As a result, BA.2 can be more time-consuming for COVID-19 testing labs to identify: labs need to sequence a sample’s genome to identify this strain rather than simply look out for an indicator on a PCR test. It’s unclear how much of a difference this will make in the U.S.’s ability to track BA.2, however, as many labs across the country are already performing routine full-genome sequencing of coronavirus samples.
How well do vaccines work against BA.2?
So far, it seems like there is no significant difference in vaccine protection between BA.1 and BA.2, at least when it comes to severe symptoms—which makes sense, scientists say, given how well vaccines have worked against every major variant to emerge thus far.
Early findings in this area come from the U.K., which designated BA.2 as a “Variant Under Investigation” (separate from BA.1) about a week and a half ago. This past Friday, the U.K.’s Health Security Agency released a report with information on BA.2, including how it compares to BA.1 or original Omicron.
Overall, U.K. epidemiologist Meaghan Kall wrote in a Twitter thread summarizing the report, early evidence suggests that “BA.2 is no more immune evasive than Omicron,” though confidence in this statement is low. The report found that, for Brits who had received booster shots, vaccine effectiveness against symptomatic COVID-19 disease was 70% for BA.2 and 63% for BA.1. The confidence intervals on these effectiveness estimates overlapped, indicating that vaccines perform similarly against BA.2 and BA.1.
• Transmissibility: 🟥 risk LOW confidence advantage due to being more infectious
• Immune evasion: 🟧 risk LOW confidence BA.2 is no more immune evasive than Omicron pic.twitter.com/kaEYFbIbP7
— Meaghan Kall has moved to Bluesky (@kallmemeg) January 28, 2022
When it comes to disease severity, Kall wrote, the U.K. doesn’t have enough data to compare BA.2 and BA.1; early data on this topic (suggesting BA.2 is not more severe) have come from Denmark and India.
How will BA.2 impact the U.S.’s COVID-19 trajectory?
BA.2 has already outcompeted BA.1 in some parts of Europe and Asia, and epidemiologists expect that countries like the U.K. and the U.S. could also follow this pattern—though it will likely be a longer, slower replacement process compared to the intense way Omicron pushed out Delta. A bigger unknown here is what effect this strain may have on case numbers, hospitalizations, and deaths.
17/ BUT wastewater testing from Marc Johnson's lab at @mumedicine shows that BA.2 is in the US, and spreading fast. This aligns with what we would expect given trends in other countries.
— Pandemic Prevention Initiative (@PPI_Insights) January 26, 2022
Countries and regions now passing the peaks of their Omicron BA.1 waves have extremely high levels of population immunity. As a result, people who are fully vaccinated with boosters and/or recently infected with Omicron BA.1 likely will have a lot of immune system protection against BA.2, though we don’t yet have good data on exactly how robust this protection is.
So, could BA.2 cause the current downturn in U.S. COVID-19 cases to reverse? It’s possible, explains Andrew Joseph in a recent STAT News article. However, thanks to our high immunity levels, a further spike in cases could be “broadly limited to infections” rather than causing major increases in hospitalizations and deaths. In the coming weeks, we’ll get a better sense of how well prior Omicron infections protect against BA.2 and other key information that will inform our understanding of how this strain may change the country’s COVID-19 trajectory.
Right now, COVID-19 experts are closely monitoring BA.2, but they’re not hugely concerned. As Dr. Jetelina put it in a recent Your Local Epidemiologist post, the bigger worry right now is that another variant could “pop out of nowhere” like Omicron did in November.
Major news items for this week include the potential peak of the U.S.’s Omicron surge and real-world data from the CDC on how well booster shots work against this variant.
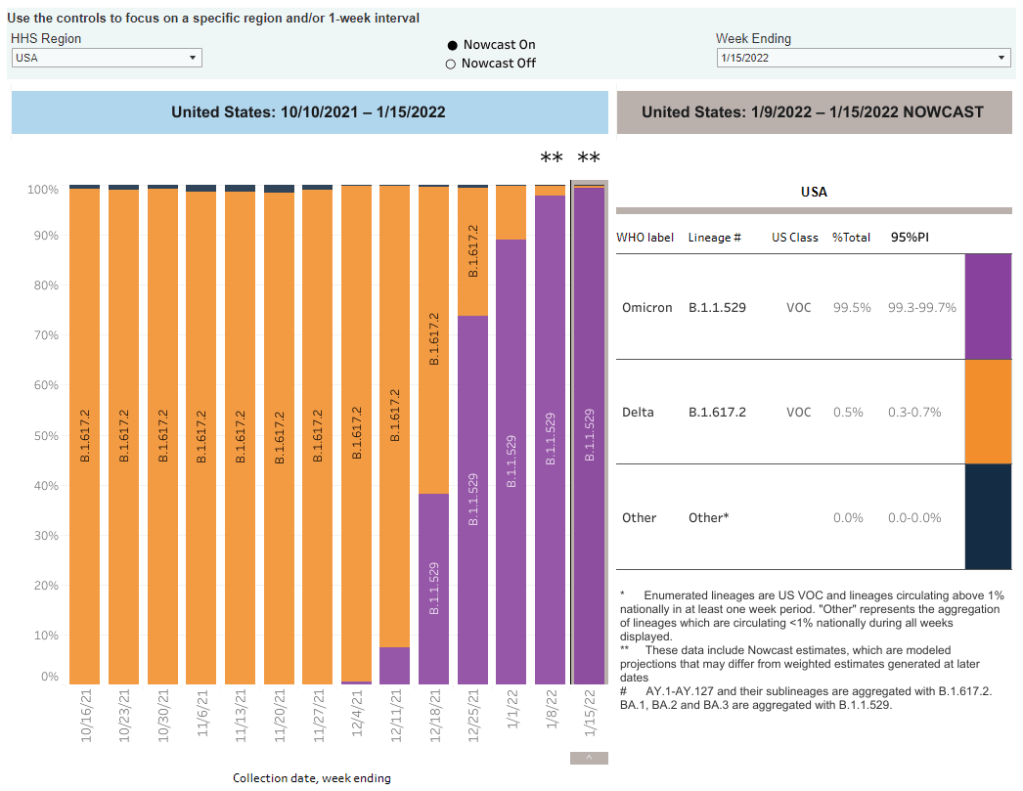
Omicron is now causing nearly 100% of new COVID-19 cases in the U.S. The latest CDC estimates of variant prevalence put Omicron at 99.5% of new cases in the U.S. as of January 15, with Delta causing the remaining 0.5% of cases. I have to say, it’s incredibly striking not only how quickly Omicron outcompeted Delta (it went from 1% of new cases to nearly 100% in just six weeks), but also how both of these highly contagious variants have dominated the country so thoroughly that they’re now the only two variants present here at all. For comparison, Alpha only got to 70% of cases at its peak. These trends show how drastically both Delta and Omicron changed the trajectory of the pandemic.
While the U.S. may be peaking, massive numbers of people are getting infected. As I noted in today’s National Numbers, America’s Omicron wave may have peaked this week, with the country’s massive case growth appearing to turn around. Computational biologist Trevor Bedford wrote a recent Twitter thread about this peak, pointing out that a huge share of the U.S. population was infected with Omicron in the past month: “between 18% and 23% of the country was infected by Omicron by Jan 17, with the large majority infected in a span of just ~4 weeks,” he hypothesized. By mid-February, Bedford says, this number could be “36%-46%.”
Case counts for the US appear to have peaked at a 7-day average of 806k on Jan 14. Omicron grew from approximately 35k daily cases on Dec 14 to ~800k daily cases in ~4 weeks. 1/9 pic.twitter.com/D1Y6R58SjN
The high infection numbers may give us “a bit of a break from the Covid roller coaster.” With so many people infected in such a short time, Omicron will have a huge impact on the “immunological landscape” of the U.S, Helen Branswell explains in a recent article for STAT News. Millions will have immunity from a recent infection, vaccination, or both; and Omicron’s unique biology may mean that people who caught this variant will be protected from other strains. As a result, the end of this wave may lead into “a bit of a break” from COVID-19, Branswell writes, with low case numbers for a few weeks or months. It’s hard to say whether this “break” will constitute the end of the pandemic, though—we don’t know how long post-Omicron immunity lasts.
Rapid at-home tests work well at detecting Omicron, though they’re far from perfect.As I’ve noted in past issues, there have been some questions recently about how well rapid antigen tests work at identifying Omicron infections. In a recent Your Local Epidemiologist post, Dr. Katelyn Jetelina walked through the data from several recent studies on this topic. The highlights: rapid tests likely won’t work well in the very beginning of an infection, so wait to test until five days after an exposure; if you test positive, trust the result; test repeatedly for higher accuracy; and, if you have the tests, wait for two negative results before coming out of isolation.
New CDC wastewater report shows how early Omicron was spreading in the U.S. The CDC published a report this week sharing findings from wastewater surveillance systems in a few states and localities. (Wastewater surveillance means the states are regularly testing samples from sewage to identify coronavirus levels coming from residents’, well, waste.) In New York City, Omicron was first detected in wastewater on November 21, the weekend before Thanksgiving. In California, Colorado, and Houston, Texas, the variant was detected in late November or early December.
An additional booster shot may not be enough to completely prevent Omicron infection, a small Israeli study suggests. Israel was one of the first countries to offer third vaccine doses to its residents, and now it’s also one of the first countries offering fourth doses. A new study presents the impact of these shots among about 270 healthcare workers. The additional doses produced more antibodies in the patients, but “this is probably not enough for the Omicron,” one of the study’s authors told Reuters—at least when it comes to completely preventing infection.
But: booster shots still reduce chances of infection significantly, compared to people who are unvaccinated. Another new CDC report published this week compares COVID-19 cases among vaccinated, boosted, and unvaccinated people in 25 U.S. jurisdictions. In late December, after Omicron started spreading widely, adults who were unvaccinated had a five times higher risk of COVID-19 infection compared to those who were fully vaccinated with a booster shot, the CDC found.
Booster shots also have a huge impact on risks of severe symptoms and hospitalization. One more CDC report released this week: scientists analyzed the impact of booster shots on emergency department visits and other hospitalization metrics in ten states. When both Delta and Omicron were the dominant variants in the U.S., the CDC researchers found, third doses had 94% efficacy rates in protecting people against COVID-related emergency department visits, and 82% efficacy rates in protecting against urgent care visits. Efficacy against hospitalization was also over 90%. In short: if you’re eligible for your booster, go get it!
Booster shots of Pfizer and Moderna vaccines could be critical for countries that used other brands.Last week, I shared a report that found 22 million mRNA vaccine doses are needed as booster shots in low-income countries, to protect the world against Omicron. This past week, a new study in Nature supported this report: a group of scientists in Hong Kong found that Pfizer doses are safe and highly effective booster shots for people who initially received the Chinese CoronaVac vaccine. The authors suggest that mRNA vaccines should be used as boosters in countries that originally distributed CoronaVac.
New research identifies a mutation that may contribute to Omicron’s super-contagiousness. A new study from the National Institutes of Health (NIH) found that a mutation present in the Alpha and Delta variants allows the coronavirus to more easily bind to human cells. When the coronavirus binds more easily, it can spread faster within the body; this rapid multiplication helps the virus quickly spread outside the body as well, increasing contagiousness. Though this study was done before the Omicron variant emerged, Omicron has this same mutation, explained lead author Dr. Lawrence Tabak in a post for the NIH Director’s Blog.
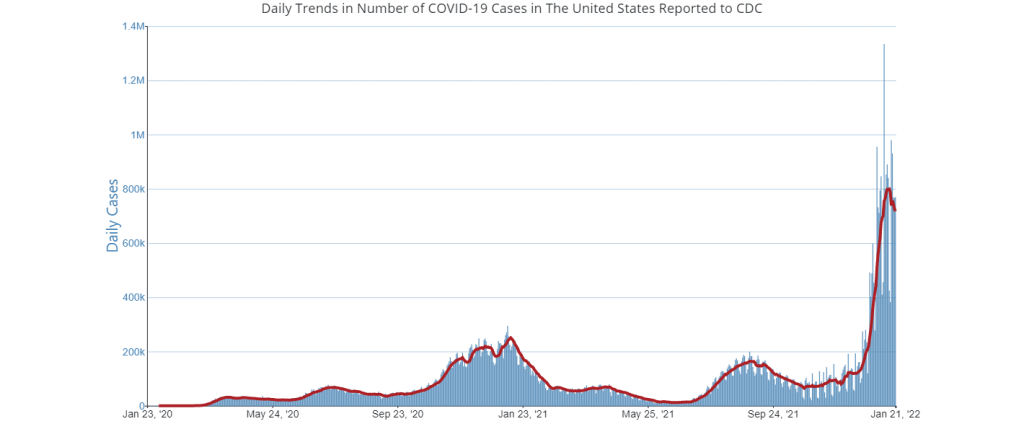
Has Omicron peaked in the U.S.? Nationally, it seems possible, but the situation is more complicated at the state and local level. Chart via the CDC, retrieved on January 23.
In the past week (January 15 through 21), the U.S. reported about 5.2 million new cases, according to the CDC. This amounts to:
An average of 745,000 new cases each day
1,588 total new cases for every 100,000 Americans
One in 63 Americans testing positive for COVID-19
5% fewer new cases than last week (January 8-14)
Last week, America also saw:
147,000 new COVID-19 patients admitted to hospitals (45 for every 100,000 people)
12,200 new COVID-19 deaths (3.7 for every 100,000 people)
100% of new cases are Omicron-caused (as of January 15)
An average of 300,000 vaccinations per day (per Bloomberg)
Has Omicron peaked in the U.S.? Looking at the national data, you might think so: new COVID-19 cases in the U.S. have dropped 5% from 5.5 million last week to 5.2 million this past week. While those numbers are astronomically high compared to past pandemic waves, it’s encouraging to think that they might not get higher.
Hospitalization data also seem to have reached a peak; while about 150,000 Americans are currently hospitalized with COVID-19, according to the HHS, this number is no longer rapidly increasing. Patient numbers are starting to decline in the states and cities that were first hit by Omicron.
It’s too soon to say that we’re actually coming down on the other side of the Omicron curve, though. For one thing, as Dr. Katelyn Jetelina pointed out in a recent issue of Your Local Epidemiologist, holiday reporting and test capacity could be playing a role here.
Last Monday was Martin Luther King Jr. Day, a federal holiday that many health agencies and test providers took off—though not a holiday on the reporting disruption level of Christmas or New Year’s. And tests are incredibly hard to find in some parts of the country, meaning that our current system simply isn’t catching a large number of COVID-19 cases. (Remember: most COVID-19 case counts do not include cases identified with at-home antigen tests.) In short, the current trend is encouraging, but we’ll have to see next week if it continues.
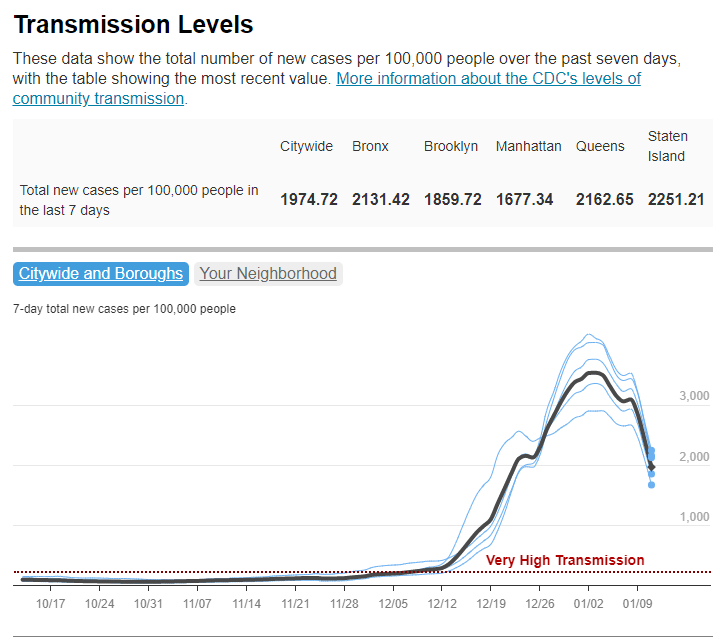
While the national picture is hard to interpret, it’s clear that the Northeast states that dealt with Omicron first are now on the decline. In New York City, the case rate has been reduced by over a third, from 3,500 new cases per 100,000 in a week at the beginning of January to 1,000 new cases per 100,000 in the last week. Case rates are also going down in New Jersey, Maryland, D.C., Connecticut, and Massachusetts.
NYC COVID transmission levels have fallen more than 3x from the city's peak on January 3 🙏 pic.twitter.com/k76lP7vl4I
At the same time, other parts of the country are still in the first half of their Omicron surges. Cases rose by over 40% from last week to this week in Wisconsin, Wyoming, Oklahoma, Idaho, Ohio, and New Mexico, according to the latest Community Profile Report. In fact, Wisconsin now has one of the highest per capita case rates in the country, at 2,800 new cases per 100,000 in the week ending January 19.
A recent NBC News article explains that the urban regions first exposed to Omicron have higher vaccination rates and more available hospital beds, making them more prepared to weather the variant. But now, Omicron is beginning to reach rural parts of the country that are less vaccinated, less capable of taking on patients, and still reeling from Delta. For these communities, the next few weeks are bound to be rough.
These update posts are getting shorter as time goes on, but we’re still learning about this variant! A few news items from this week:
Omicron is now causing almost 100% of new COVID-19 cases in the U.S. In the CDC’s latest variant proportions update, the agency estimated that 98% of new COVID-19 cases were caused by Omicron in the week ending January 8. The CDC also revised estimates for previous weeks, though the revisions were not as significant as they have been in the past—suggesting that the numbers are now fairly close to accurate, but will continue to be tweaked as more sequencing data come in.
Major Northeast hotspots appear to be peaking.Last week, I wrote that New York City’s Omicron wave seemed to have reached its peak. The trend has continued into this week: the new case rate and test positivity rate have both fallen consistently since peaking on January 3. Similarly, in Boston, the Omicron levels detected in the city’s wastewater have declined steeply since early January. The daily case rate is also going down in Washington, D.C., and in the Northeast region overall. Still, hospitals are still overwhelmed throughout the region, and it’s unlikely that cases will go down as quickly or as decisively as they went up.
We knew it was happening, but *reported* cases are now showing a strong decline in the northeast pic.twitter.com/sGrNiSReRs
New NYC report provides data on the city’s Omicron wave. Speaking of NYC: the city’s public health department recently put out a new report detailing the variant’s impact. The variant “has accounted for nearly all coronavirus samples sequenced in NYC” since Christmas, the report’s authors write. Also, while a smaller share of Omicron cases led to hospitalization compared to the Delta wave, more people have been hospitalized overall because of sheer case numbers. Unvaccinated New Yorkers, Black New Yorkers, and those over age 75 have been most likely to require hospitalization.
Real-world study suggests rapid at-home tests work well at detecting Omicron. A new study from the University of California, San Francisco, released this week as a preprint, analyzed rapid antigen tests’ capacity to detect Omicron by comparing rapid test results to PCR test results. The results: antigen tests correctly identified 95% of cases with high viral loads and 98% of symptomatic cases. In about one-third of the cases identified through PCR, patients tested negative on antigen tests; but this is in line with the tests’ accuracy for other variants.
Data from the NBA suggest Omicron’s viral load is pretty variable. Another new study posted as a preprint this week analyzed data from the National Basketball Association (NBA). The league’s regular testing policy allowed Harvard researchers to study viral loads in Omicron-positive patients, revealing that this variant had “lower peak viral load and more variable early viral growth durations than Delta,” according to one of the authors. In other words, some of the basketball players were highly contagious early into their Omicron infections, while others were less so; and the players had less virus in their bodies overall at the peak of their infections than in previous Delta infections. Also, a large number of the players were still contagious five days after they were diagnosed—which doesn’t bode well for the CDC’s new isolation guidance.
We get the longitudinal data we need on the viral load trajectory of Omicron… from the NBA. I’ll take it.
Takeaway: even in this vaccinated, highly-boosted group, ~50% of individuals have high viral loads (Ct<30) at five days post detection. https://t.co/nIgYUaucEs
More confirmation that vaccinated people are protected from severe disease from Omicron. Another new study, this one published in Nature through the journal’s advance preview system for COVID-19 reports, confirms previous research about T cell response to Omicron. T cells are a key part of the immune system’s long-term memory apparatus; they help protect against severe symptoms and death. The study found that, in patients who were fully vaccinated (or, to a lesser degree, had a previous infection), T cells could recognize Omicron and protect people against its worst impacts.
Omicron adds urgency to the need to vaccinate the world—ideally, with mRNA vaccines. A report from advocacy groups PrEP4All and Partners In Health, written with scientists at Harvard, Columbia, and other institutions, found that 22 billion additional mRNA vaccine doses are needed to control the pandemic, now that Omicron has become the dominant variant in the world. The report specifies that mRNA vaccines are needed because other vaccine types are not capable of preventing Omicron infection, and likely are less effective against severe disease. “Future viral variants may become even more transmissible, immune evasive, and virulent than Delta or Omicron,” the report cautions.