Since BA.2.86 emerged a couple of weeks ago, scientists around the world have been racing to evaluate this variant. Several teams posted data in the last week, and the news is promising: while BA.2.86 does have an advantage over past variants, the lab findings suggest that vaccines (including the upcoming boosters) and past infections provide protection against it.
The new studies come from research groups in the U.S., China, Japan, Switzerland, and South Africa. These scientists studied BA.2.86 by growing the variant in petri dishes and evaluating it against antibodies from blood samples. Overall, they found that BA.2.86 can infect people who were recently infected with XBB.1.5 and its relatives, but this variant isn’t as successful at getting into human cells as XBB.1.5.
Another notable study came from researchers at Moderna, who evaluated how the company’s upcoming booster shot performs against BA.2.86. This team found that the booster—which is designed from XBB.1.5—helps the immune system prepare for XBB variants as well as BA.2.86. While lab studies like this one don’t translate perfectly to real-world effectiveness, the data do suggest that Moderna’s booster should protect well against BA.2.86 infection for a few weeks after vaccination, and against severe disease for longer.
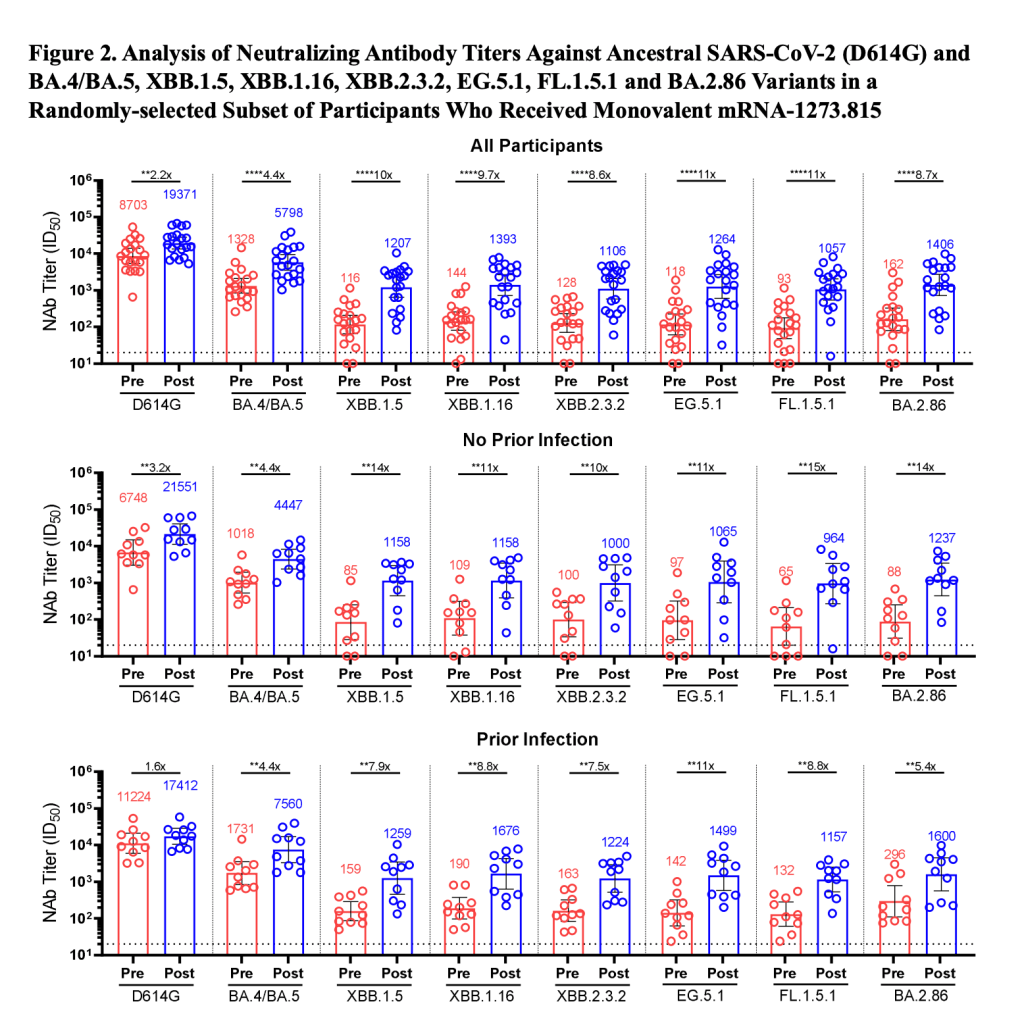
You might have seen the figure below shared around on social media in the last few days. This chart, from the Moderna team, shows how the new booster improves immunity toward several variants. For example, patients who received the booster had 8.7 times more neutralizing antibodies against BA.2.86 and 10 times more neutralizing antibodies against XBB.1.5 than those who had not received it.
This figure, from a preprint by Moderna scientists, shows how the company’s upcoming fall booster performs against different variants.
Pfizer has also tested their new booster against BA.2.86 and found similar results, according to a report from Reuters. This company’s results have yet to be shared in a scientific paper, though.
The studies I’ve discussed here are all preprints, meaning the results have yet to be peer-reviewed (outside of the informal review process that happens on social media for this type of urgent research). It’s also worth noting that lab studies look at immune system signals, rather than actually tracking who’s getting this new variant and their disease outcomes.
Even if BA.2.86 is not “the next Omicron,” as some scientists suggested based on its mutations, it could still contribute to a new uptick in cases this fall. And all cases carry the risk of severe illness, Long COVID, and other poor outcomes. The new boosters are likely to help reduce risk (which is good news), but other measures are still needed.
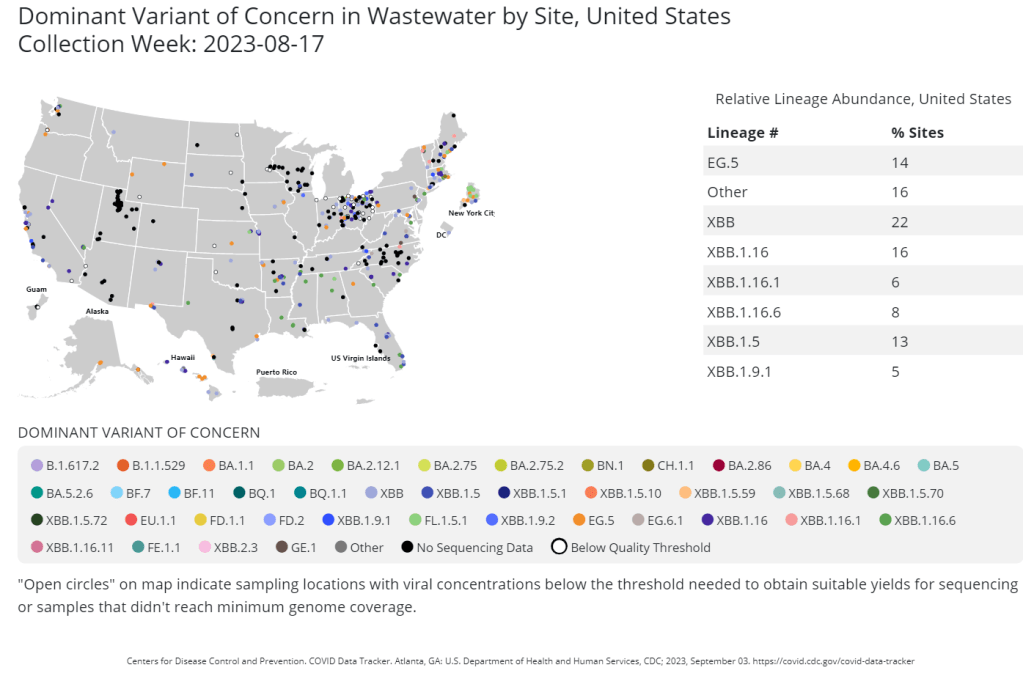
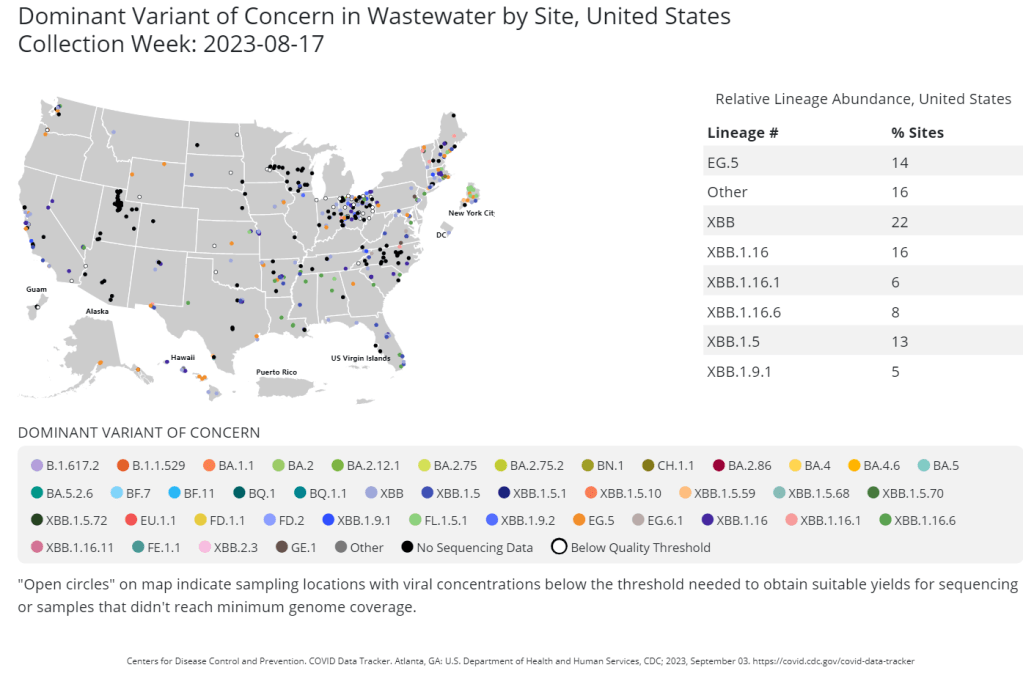
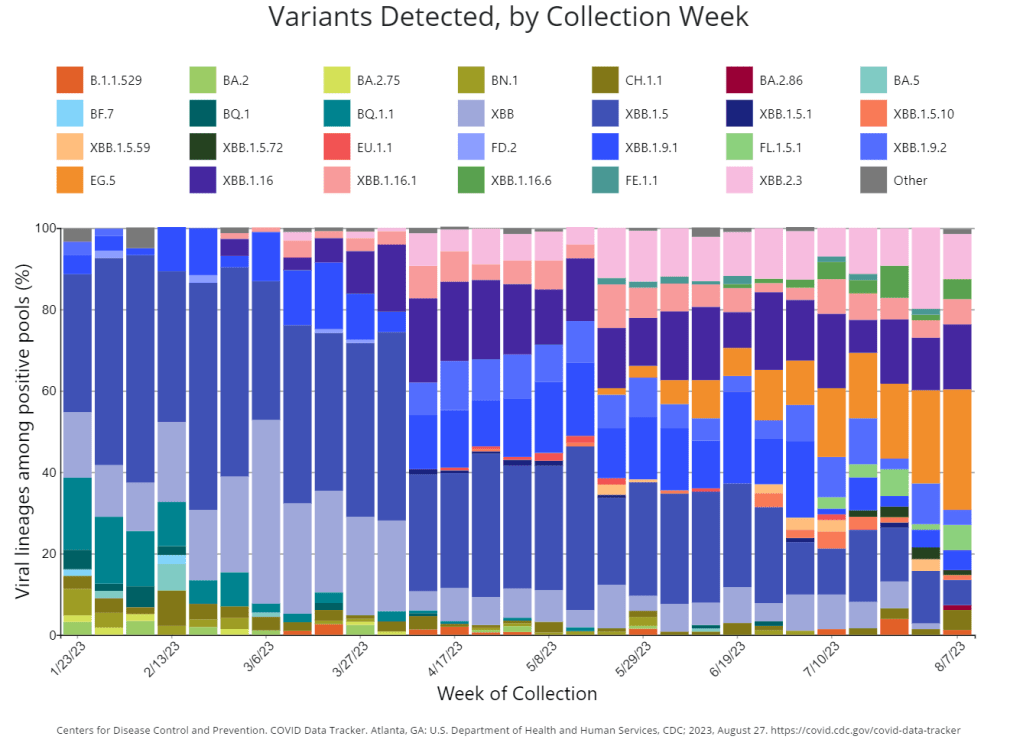
The CDC publishes data from about 400 wastewater testing sites that are sequencing their samples. Chart shows data from the week of August 17.
This week, the health department in New York City, where I live, announced that they’d identified new variant BA.2.86 in the city’s wastewater. (For more details about BA.2.86, see last week’s Q&A post.)
I covered the news for local outlet Gothamist/WNYC, and the story got me thinking about how important wastewater surveillance has become for tracking variants. With less clinical testing, sewage is now a crucial source for understanding how the coronavirus is mutating and what impacts those mutations have. But there are continued barriers to obtaining and interpreting wastewater data.
Quoting from the story:
The declaration of the end of the public health emergency in May made COVID-19 tests less available in health care settings, and sewage monitoring has since emerged as an important way to identify new variants.
“As the wastewater testing has gotten better, the patient surveillance has decreased,” [said Marc Johnson, a virologist at the University of Missouri]. Several variants have been found in sewage before cases were confirmed, he said.
Wastewater surveillance has some distinct advantages, when it comes to variant monitoring:
It covers thousands of people—the entire population of a sewershed—with one sample. In big cities like NYC, one sample can include data from more than one million residents.
Through sewage samples, scientists can look for multiple variants at once, rather than compiling data over many PCR test results. They can also track population-level trends over time.
Unlike traditional case data, wastewater data don’t rely on how many people are getting tested or where. This lack of testing bias is important, as people typically use rapid tests—which are not reported to health systems—over PCR these days (rapid tests are easier to access, PCR sites have closed following the end of the federal public health emergency, etc.).
But there are also some problems, as the NYC detection this week demonstrated:
Public health officials are still getting used to using and sharing wastewater data, as this is a relatively novel source with novel pipelines for transmitting data. While the CDC and other organizations are working to compile these data in a standardized way, it’s still a work in progress.
Discrepancies and delays can sometimes occur as a result. For example, in New York, the governor’s office put out a press release on Tuesday morning claiming that BA.2.86 hadn’t been detected in the state yet—then, just hours later, the city health department announced they’d found it. State health officials weren’t aware of the detection before the city made its public announcement, I learned for my news story.
Health officials are also still learning how to interpret and act on wastewater data. The NYC health department failed to answer my questions about in which sewershed or from which sampling date they found BA.2.86; it’s unclear if they’re using the detection to take any specific actions, besides simply warning the public that this variant is present.
As wastewater surveillance captures such broad samples, it’s difficult to tie new variant detections to clinical data, such as whether an infected person went to the hospital due to their symptoms. Officials can’t contact trace from these detections, making it hard to answer questions like whether BA.2.86 causes more severe symptoms.
During the most recent week of data available (August 13-19), the U.S. reported about 15,100 new COVID-19 patients admitted to hospitals, according to the CDC. This amounts to:
An average of 2,200 new admissions each day
4.6 total admissions for every 100,000 Americans
19% more new admissions than the prior week (August 6-12)
Additionally, the U.S. reported:
14.9% of tests in the CDC’s surveillance network came back positive
A 3% higher concentration of SARS-CoV-2 in wastewater than last week (as of August 30, per Biobot’s dashboard)
23% of new cases are caused by Omicron XBB.1.6; 22% by EG.5; 15% by FL.1.5.1 (as of September 2)
The late-summer COVID-19 surge is still in full swing, with all major metrics showing further increases in disease spread this week. BA.2.86 isn’t spreading widely yet but is worth continued surveillance.
Last week, I wrote that wastewater data from Biobot Analytics showed a potential plateau—but cautioned those data were tentative. Unfortunately, further updates this week suggest that COVID-19 transmission is still increasing, albeit not as dramatically as it was in July.
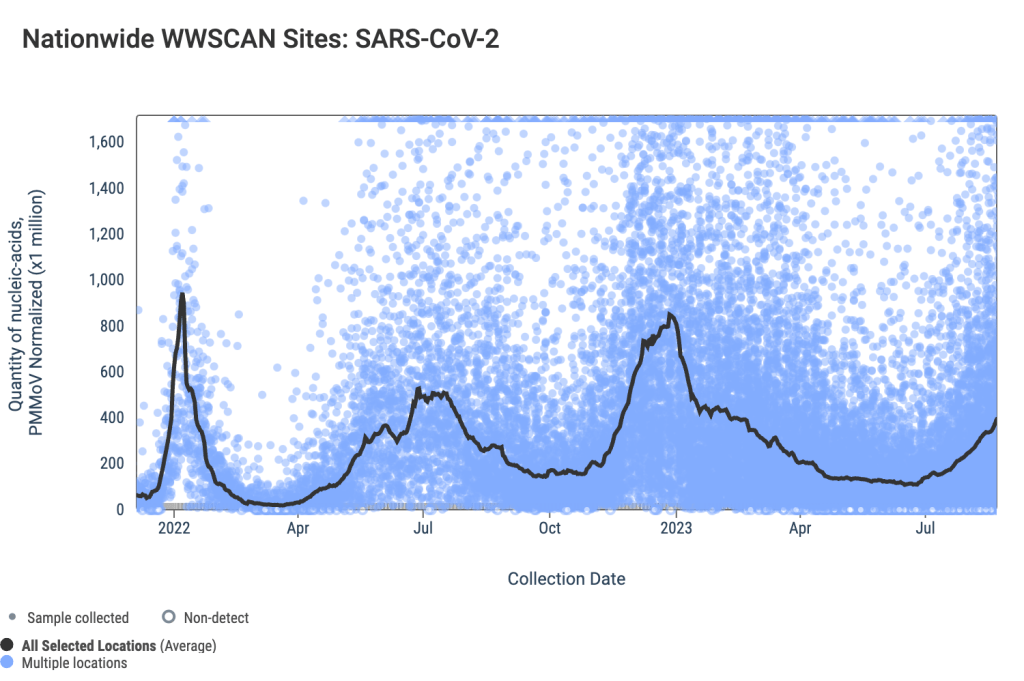
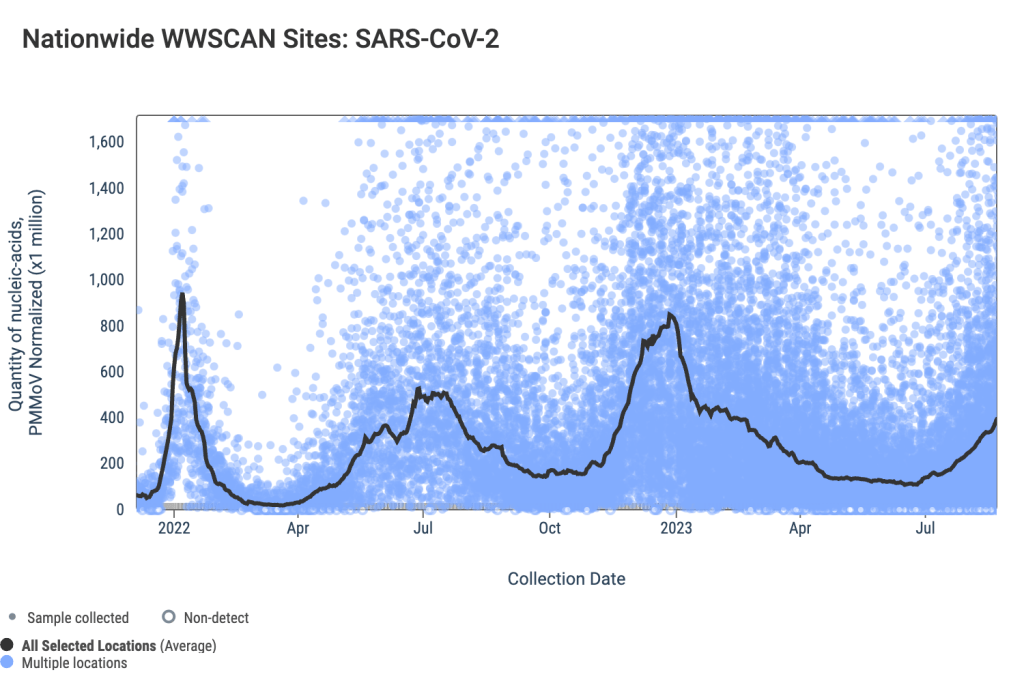
Data from WastewaterSCAN show a similar pattern: a sharp increase in COVID-19 spread from late June through July, followed by a slight leveling off, and then followed by further increase. This could be caused by a newer variant entering the picture, driven by behaviors, or (most likely) some combination of the two.
Regional data from both Biobot and WastewaterSCAN indicate that COVID-19 transmission might be approaching plateaus in the South and Midwest, but is going up sharply in the Northeast and West coast. The Midwest, after showing decreases in Biobot’s data over recent weeks, is now trending up again.
The CDC’s test positivity and hospitalization numbers continue to rise as well. New hospital admissions for COVID-19 reached 2,000 per day during the week ending August 19, and are likely still higher now. Test positivity is up to 15%, the highest this metric has been since last winter’s holiday surge.
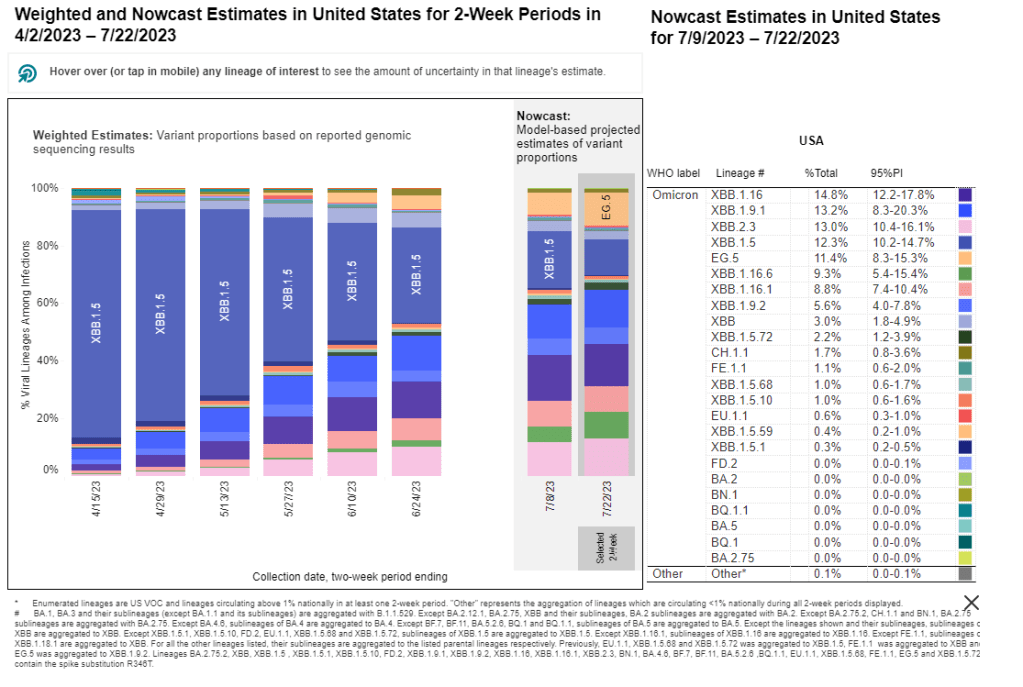
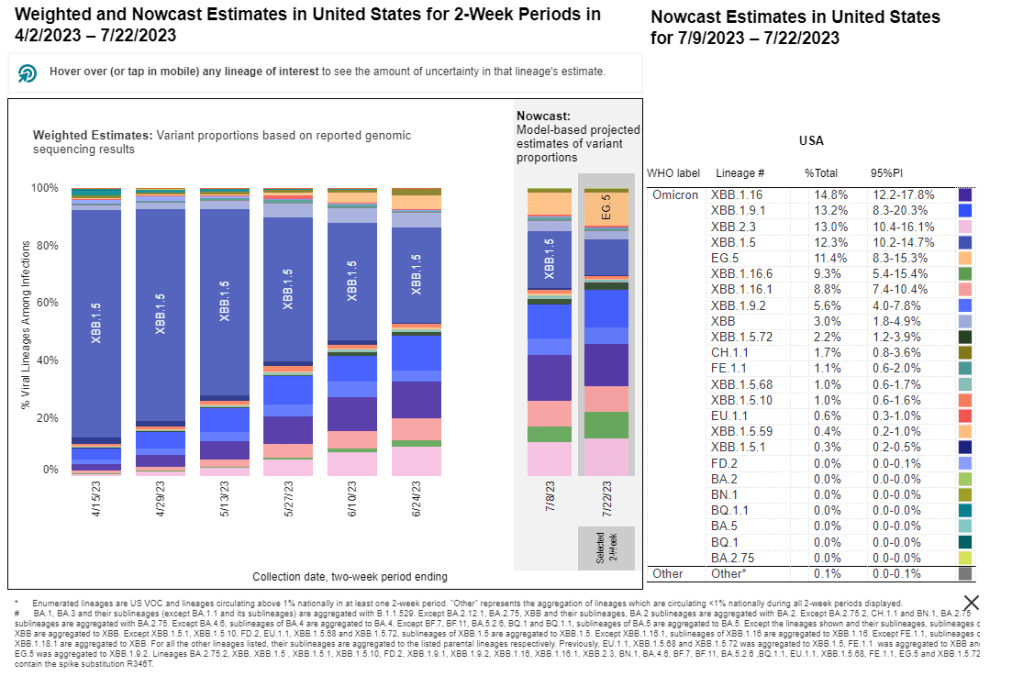
In the CDC’s latest variant estimates (posted on Saturday), EG.5 and XBB.1.6 continue to dominate in a crowded landscape of Omicron XBB relatives. The agency hasn’t yet found enough BA.2.86 for this new variant to be included in the update. However, this could indicate low testing rather than an actual low prevalence of BA.2.86.
The CDC often takes COVID-19 reporting breaks over holiday weekends, and this one is no exception: the agency will not update its dashboard on Monday, according to a note posted at the top of the page. Hospitalizations, test positivity, and other metrics will be updated later in the week.
Of course, the coronavirus doesn’t care about holidays—in fact, it usually spreads more widely when people travel and gather. Fully understanding this Labor Day weekend’s impact could take several weeks, at our current pace of data reporting.
The CDC’s Traveler Surveillance program, which offers free PCR tests to international travelers entering the U.S., was one of the first surveillance programs to pick up BA.2.86, pictured in dark red on the right-most bar of this chart.
Last week, I introduced you to BA.2.86, a new Omicron variant that’s garnered attention among COVID-19 experts due to its significant mutations. We’ve learned a lot about BA.2.86 since last Sunday, though there are many unanswered questions to be answered as more research is conducted.
Here’s my summary of what we know so far—and what scientists are still working to understand. Overall, this variant has some concerning properties, but more data are needed before we know what kind of impact it will have on disease transmission and severity.
Where did BA.2.86 come from?
BA.2.86 was first identified in Israel earlier this month. Scientists then picked it up in Denmark, the U.S., U.K., and several other countries across multiple continents (and in people without recent travel history), suggesting that it has been spreading under the radar for a while.
However, as I’ve noted with past variants, the country where BA.2.86 was first identified is not necessarily the country where it developed. Many countries around the world are doing fairly limited COVID-19 testing and sequencing these days, so nations like Israel and the U.S. (which have more robust surveillance, relatively speaking) are likely to catch new variants.
Why are scientists concerned about BA.2.86?
BA.2.86 worries experts because it has a number of mutations: about 30 in its spike protein, compared to BA.2, its closest relative. The spike protein is the part of the coronavirus that binds to and enters human cells, so mutations tend to accumulate here, enabling the virus to cause new infections in people who have already been infected or vaccinated.
BA.2, you might remember, was a dominant variant in early 2022, so it’s unexpected to see a descendant of this lineage pop up now. Scientists hypothesize that BA.2.86 might have evolved in a single person with a persistent infection; the virus could have multiplied and mutated over the course of several months or a year in someone originally infected with BA.2. This evolution also could have occurred in an animal population, then transferred back to humans.
Scientists have similar hypotheses about the original Omicron variant, which was also very different from circulating strains when it emerged. In fact, BA.2.86 is about as different from XBB.1.5 (a recently dominant variant globally) as Omicron BA.1 was from Delta.
Where has BA.2.86 been identified so far?
Surveillance efforts in many countries have now found BA.2.86, ranging from Thailand to South Africa. This variant is evidently already spreading globally; unlike Omicron’s initial emergence, however, we don’t have a singular country to watch for signals of how BA.2.86 may impact transmission trends.
In the U.S., researchers have found BA.2.86 in three different states:
One case in Michigan, from a person tested in early August
One traveler returning to a D.C.-area airport from Japan, their infection caught through the CDC’s travel surveillance program
Wastewater from a sewershed in Elyria, Ohio
As surveillance is currently fairly uneven across the U.S., we can likely assume that BA.2.86 is present in other states already. Continued testing in the next few weeks will provide a clearer picture of the situation.
How does BA.2.86 impact transmission and disease severity?
This is one question that we can’t answer yet, though scientists are concerned about its potential. In a risk assessment report published this past Wednesday, the CDC said that mutations present in BA.2.86 suggest that this variant may have greater capacity to “escape from existing immunity from vaccines and previous infections” when compared to recent variants.
However, this is just a hypothesis based on genomic sequences. The CDC report cautions that it’s too soon to know how transmissible BA.2.86 is or any impact it may have on symptom severity. To answer this question, scientists will need to identify more cases caused by this variant, then track their severity and spread.
Will our new booster shots work against BA.2.86?
The FDA and CDC are planning to distribute booster shots this fall, based on the XBB.1.5 variant that dominated COVID-19 spread in the U.S. this spring and earlier in the summer. As Eric Topol points out in a recent Substack post, this booster choice made sense a couple of months ago, but it’s unlikely to work well against BA.2.86 if that variant takes off.
More research is needed on this topic, of course, but the existing genomic data is concerning. Having an XBB.1.5 booster this fall, if we see a BA.2.86-driven surge, would be like having a booster based on Delta, when Omicron is spreading: better than no booster, but unlikely to provide full protection.
“The strategy of picking a spike variant for the mRNA booster at one point in time and making that at scale, going through regulatory approval, and then for it to be given 3 or more months later is far from optimal,” Topol writes. “We desperately need to pursue a variant-proof vaccine and there are over 50 candidate templates from broad neutralizing antibodies that academic labs have published over the last couple of years.”
Will current COVID-19 tests and treatments work for BA.2.86?
According to the CDC’s risk assessment, current tests should still detect BA.2.86 and treatments should work against it, based on early studies of the variant’s genomic sequences. More research (from health agencies and companies) will provide further data on any changes to test or treatment effectiveness.
Mara Aspinall points out in her testing-focused Substack that rapid tests, in particular, tend to be unaffected by variants because they test for the N protein, a different part of the coronavirus from the spike protein (which is the main area of viral evolution). However, if you’re taking a rapid test, it’s always a good idea to follow best practices for higher accuracy—testing multiple times, swabbing your throat, etc.—and get a PCR if available.
How are scientists tracking the coronavirus’ continued evolution?
BA.2.86 has arrived in an era of far less COVID-19 surveillance, compared to what we had available a year or two ago. Most people rely on rapid tests (if they test at all), which are rarely reported to the public health system and can’t be used for genomic surveillance. As a result, it might take longer to identify BA.2.86 cases even as this variant spreads more widely.
However, there are still some surveillance systems tracking the virus—and all are now attuned to BA.2.86. A couple worth highlighting in the U.S.:
Wastewater surveillance increasingly includes testing for variants. The CDC has a dashboard showing variant testing results from sewage; this is happening in about 400 sewersheds now and will likely increase in the future.
The CDC also supports a travel surveillance program at major international airports, in partnership with Concentric by Ginkgo and XpressCheck. This program caught one of the first BA.2.86 cases in the U.S. (the traveler from Japan mentioned above).
Several major testing companies and projects continue virus surveillance, via both limited PCR samples and wastewater. These include Helix, Biobot, and WastewaterSCAN.
What will BA.2.86 mean for COVID-19 spread this fall and winter?
While BA.2.86 is similar to Omicron BA.1 in its level of mutations, it’s not yet driving significant disease spread at the same level that we saw from Omicron when that variant first emerged in late 2021. All warnings at this point are tentative, based on very limited data.
It could “fizzle,” or fail to outcompete currently-circulating variants and spread widely despite its concerning array of mutations.
It could “displace” the current variants and contribute to increased transmission, but not cause a huge wave on the same level as Omicron BA.1 in late 2021.
It could cause a major wave, comparable to the initial Omicron spread.
Based on analysis from Johnson and other experts I follow, the second scenario seems most likely. But if the U.S. and other countries had meaningful public health protections in place, we could actually contribute to those odds, rather than leaving things up to evolutionary chance. Remember: variants don’t just evolve in a vacuum. We create them, by letting the virus spread.
Last week, several variant experts that I follow on Twitter (which I refuse to call by its new name, thanks) started posting about a new SARS-CoV-2 variant, first detected in Israel. They initially called it Omicron BA.X while waiting for more details to emerge about the sequence; it’s now been named BA.2.86.
Scientists and health officials are concerned about BA.2.86 because it has many mutations on its spike protein, showing significant deviation from other versions of Omicron. This variant evolved from an earlier Omicron strain (BA.2) rather than XBB, which is the primary lineage spreading across the world right now—and is the primary focus of booster development for this fall.
Here are two relevant threads with more info (the first for a more general audience, the second going into more details about mutations):
Quick summary of the "BA.X" variant that trackers are watching closely. Bear in mind, there are only a few sequences of it so far and it may not be able to compete with currently dominant variants and may not take off. But it's interesting and *potentially* concerning.
Virologists hypothesize that BA.2.86 may have evolved in someone with a chronic infection—essentially gaining more and more mutations as the same person stayed sick for many months. Similar hypotheses apply to Delta and Omicron, though it’s hard to get definitive answers without actually finding those patients.
Another reason for concern: as of today, BA.2.86 has been detected on three different continents. In addition to Israel, scientists have found it in Denmark and the U.S. Since most countries are not doing rigorous genomic surveillance these days, the cases found so far suggest that this variant is actually far more widespread; it just went undetected until now.
I’m keeping today’s post about BA.2.86 short due to the limited information we have so far. But I’d like to dive into it more next week. So, send me your questions about this variant or about genomic surveillance more broadly, and I will answer them in next Sunday’s newsletter.
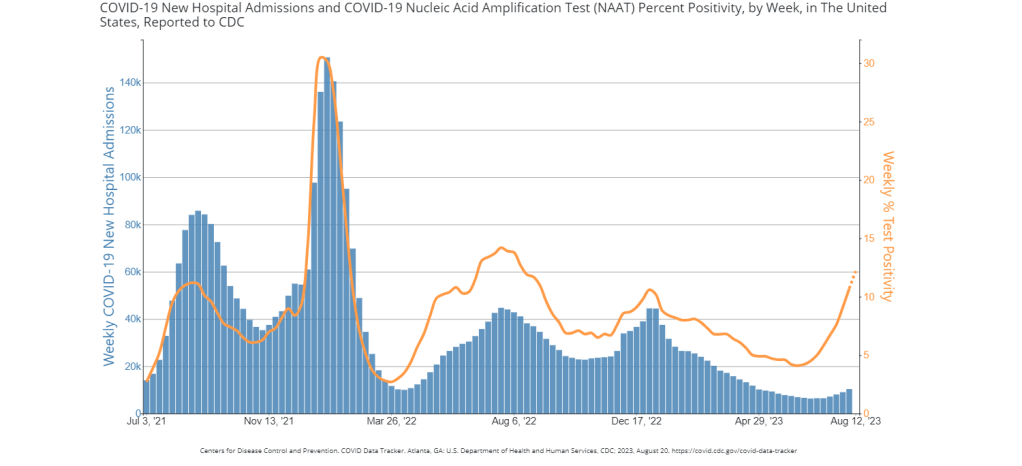
While the rise in hospitalizations has been modest, test positivity is on a similar level to the last couple of surges, per the CDC. Data as of August 18.
During the most recent week of data available (July 30 through August 5), the U.S. reported about 10,300 new COVID-19 patients admitted to hospitals, according to the CDC. This amounts to:
An average of 1,500 new admissions each day
3.1 total admissions for every 100,000 Americans
14% more new admissions than the prior week (July 23-29)
Additionally, the U.S. reported:
12.2% of tests in the CDC’s surveillance network came back positive
A 10% higher concentration of SARS-CoV-2 in wastewater than last week (as of August 16, per Biobot’s dashboard)
25% of new cases are caused by Omicron XBB.1.6; 21% by EG.5; 11% by XBB.2.3; 13% by FL.1.5.1 (as of August 19)
The summer COVID-19 surge continues. While wastewater surveillance data suggest that transmission trends may be turning around in some places, the virus is largely still increasing across the U.S. New variants are on the horizon, too.
Nationally, coronavirus levels in wastewater are the highest they’ve been since last winter’s holiday surge, according to data from Biobot Analytics. Viral concentrations have tripled since mid-June, and continue to follow a similar pattern to the Delta surge that we experienced at about the same time in summer 2021.
Biobot’s regional data suggest that the Midwest—which reported a serious spike last week—may have turned a corner in this surge, with viral levels going into a plateau. This pattern is based on just one week of data, though, so we’ll have to see what next week’s numbers show.
Wastewater data from the CDC and WastewaterSCAN similarly show continued increases in COVID-19 spread. Some counties in Southern states, such as Florida, Georgia, and Alabama, are reporting particularly large upticks. Hawaii may be a state to watch, too, as residents face health access challenges following the recent wildfires.
Test positivity also continues to increase, with the CDC reporting that about 12% of COVID-19 tests reported to its respiratory network returned positive results in the week ending August 16. Hospital admissions and emergency department visits are still going up as well, though these metrics are reported with two-week delays.
The CDC updated its variant data this week, reporting that Omicron EG.5 continues to outcompete other XBB lineages. EG.5 doesn’t have a huge advantage in transmission, though, so it’s increasing relatively slowly amid a sea of other similar variants.
But a new variant, called BA.2.86, may be one to watch more closely. Health officials are on the alert after seeing just a few cases in the U.S., Israel, and Denmark due to a number of mutations in this variant’s spike protein, which diverge significantly from other strains. (More on this variant later in today’s issue.)
While the CDC says it’s monitoring this new variant, the agency’s genomic surveillance is far sparser than it was a year or two ago. The agency and its research partners are now sequencing under 5,000 coronavirus samples a week, compared to almost 100,000 a week at the height of Omicron. With this small sample pool, the CDC is less equipped to catch BA.2.86, or any other variants that may arise.
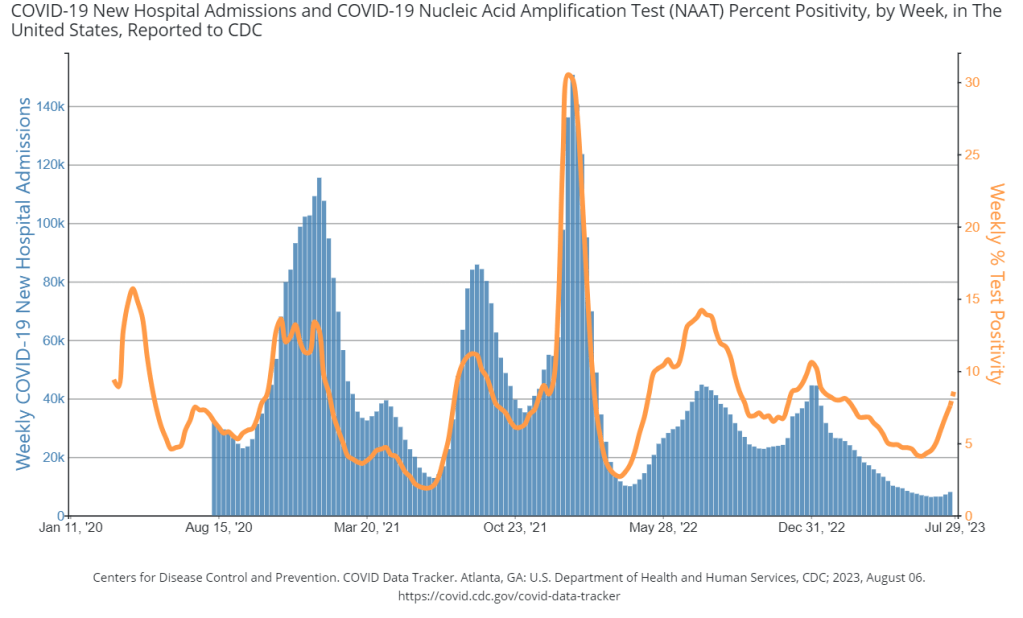
Test positivity is way up in the U.S., while hospitalizations are starting to follow this trend. Chart via the CDC.
During the most recent week of data available (July 16 through 22), the U.S. reported about 8,000 new COVID-19 patients admitted to hospitals, according to the CDC. This amounts to:
An average of 1,150 new admissions each day
2.4 total admissions for every 100,000 Americans
12% more new admissions than the prior week (July 9-15)
Additionally, the U.S. reported:
8.9% of tests in the CDC’s surveillance network came back positive
A 10% higher concentration of SARS-CoV-2 in wastewater than last week (as of August 2, per Biobot’s dashboard)
31% of new cases are caused by Omicron XBB.1.6; 17% by EG.5; 11% by XBB.2.3; 10% by XBB.1.9 (as of August 5)
Over the last few weeks, the signals of a summer COVID-19 surge in the U.S. have grown steadily clearer. Viral levels in wastewater, test positivity, and hospitalizations are all climbing across the country.
Wastewater surveillance data from Biobot suggest that coronavirus levels have doubled nationally in the last month. The surge is impacting all major regions of the country; the Northeast and South saw earlier increases, but the Midwest and West Coast are now catching up.
The CDC’s wastewater surveillance network also points to increasing COVID-19 spread, with sites across the country reporting higher viral levels. While wastewater surveillance remains uneven (some states are testing in every county, others in just a handful of locations), it still gives us enough information to identify a widespread surge.
Test positivity from the CDC’s lab testing network shows continued increases as well. About 8.9% of COVID-19 tests reported to the agency returned positive results in the week ending July 29, compared to 4.5% in the week ending June 24. This increase, too, is consistent across regions.
Hospitalizations for COVID-19 are also going up, according to the CDC. These data are significantly delayed, with the most recent numbers dating to about two weeks ago. So, while overall patient numbers remain low right now, I expect they will continue to rise as the surge goes on.
The coronavirus’ continued evolution is likely playing a role in this summer’s increased spread, as are summer travel and waning immunity from past vaccinations. Omicron EG.5, a descendant of the XBB.1.9 lineage, is the latest variant to spread widely, according to the CDC’s estimates.
No one version of XBB has yet shown a significant ability to spread much faster or cause more severe symptoms than other variants. Rather, many iterations of this Omicron lineage are spreading in tandem, continuing to mutate with every infection. And with fewer PCR tests happening, it’s harder for health agencies to keep track.
This summer’s surge may be less visible than ever. But wastewater data suggest we’re seeing similar levels of COVID-19 spread as we saw with Delta in summer 2021. Precautions are still important!
During the most recent week of data available (July 2 through 8), the U.S. reported about 6,200 new COVID-19 patients admitted to hospitals, according to the CDC. This amounts to:
An average of 900 new admissions each day
1.9 total admissions for every 100,000 Americans
1% fewer new admissions than the prior week (June 25-July 1)
Additionally, the U.S. reported:
6.3% of tests in the CDC’s surveillance network came back positive
A 9% higher concentration of SARS-CoV-2 in wastewater than last week (as of July 19, per Biobot’s dashboard)
24% of new cases are caused by Omicron XBB.1.6; 19% by XBB.1.9; 13% by XBB.2.3 (as of July 22)
COVID-19 data in the U.S. is showing increasingly clear signs of a summer surge, with infections rising across the country. However, thanks to the federal public health emergency’s end, we have less and less data to track this trend.
Wastewater data from Biobot Analytics show that national coronavirus levels have gone up by about 68% in the last month. Current levels are far below this time last year (when the Omicron BA.4/BA.5 surge was in full swing), but still at their highest in several months.
Biobot’s regional data suggest that the COVID-19 uptick is hitting all major regions. But the increases have been most pronounced in the Northeast and South; coronavirus levels have doubled in both regions in the last month, per Biobot.
The CDC’s wastewater surveillance network has picked up these increases as well, with more than half of testing sites in this network (with recent data) reporting coronavirus upticks in the last two weeks. Some major cities, such as Boston and Los Angeles, are also reflecting the increase.
Test positivity data from the CDC also show the increasing COVID-19 spread: nationally, test positivity from the labs in the agency’s surveillance network has gone up from 4.3% one month ago to 6.3% in the most recent week of data. The most prominent increases for this metric are similarly in the Northeast and South, and in the health region including Oregon, Washington, Idaho, and Alaska.
One metric not yet showing an increase is the CDC’s hospital admissions data. But the agency has continued to report these data with a lag: as of today, the most recent hospitalization numbers are as of July 8, two weeks ago. The CDC has yet to provide a clear explanation for this reporting lag.
Either way, the data we do have give us sufficient warnings about this summer’s uptick in COVID-19 spread. One likely culprit is the continued evolution of Omicron XBB: about 15 different subvariants are currently competing, according to the CDC’s latest data. No variant seems to be a clear winner yet.
Regardless of which variant comes to dominate next, the same safety measures continue to work against COVID-19.
In the past week (May 28 through June 3), the U.S. reported about 7,200 new COVID-19 patients admitted to hospitals, according to the CDC. This amounts to:
An average of 1,000 new admissions each day
2.2 total admissions for every 100,000 Americans
6% fewer new admissions than last week (May 21-27)
Additionally, the U.S. reported:
4.2% of tests in the CDC’s surveillance network came back positive (an 8% decrease from last week)
40% of new cases are caused by Omicron XBB.1.5; 26% by XBB.1.16; 21% by XBB.1.9 (as of June 10)
(Biobot update delayed)
Nationally, the COVID-19 situation in the U.S. is similar to where we’ve been for the last few weeks. Major metrics (such as we have them) show an overall plateau in disease spread. Wastewater trends in a few places suggest a summer surge might be coming, but it’s hard to say for sure.
Hospital admissions and test positivity (from the specific network of labs reporting to the CDC) are trending slightly down at the national level. But there are still about 1,000 people being hospitalized with COVID-19 every day.
Biobot Analytics, my usual go-to source for wastewater surveillance data, did not update their dashboard this week due to a tech issue. The company’s most recent data, as of May 29, show plateaus in all four major regions.
The CDC’s National Wastewater Surveillance System (NWSS) shows a similar picture. Among about 1,100 sewage testing sites that recently reported to the CDC, 60% reported decreases in coronavirus levels in the last two weeks while 40% reported increases.
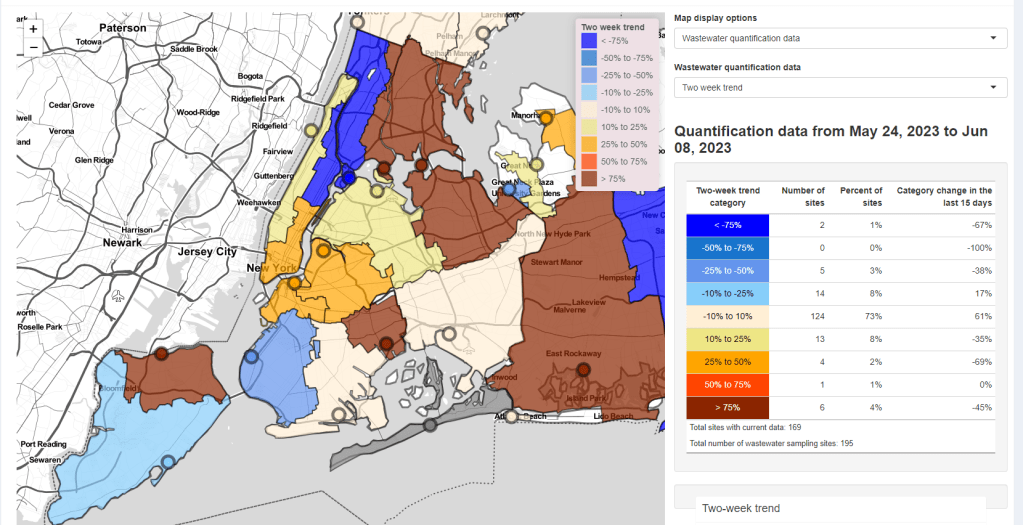
New York City is one of the places seeing wastewater increases, as I noted last week. Patterns differ somewhat across the city’s fourteen sewersheds, with some reporting more than 1000% increases in wastewater levels in recent weeks while others are still in plateaus.
Both the New York/New Jersey and New England regions are reporting slight upticks in their test positivity, according to the CDC’s surveillance network. This (along with the trends in NYC’s sewage) could be a precursor of more COVID-19 spread this summer, but it’s currently hard to say for sure.
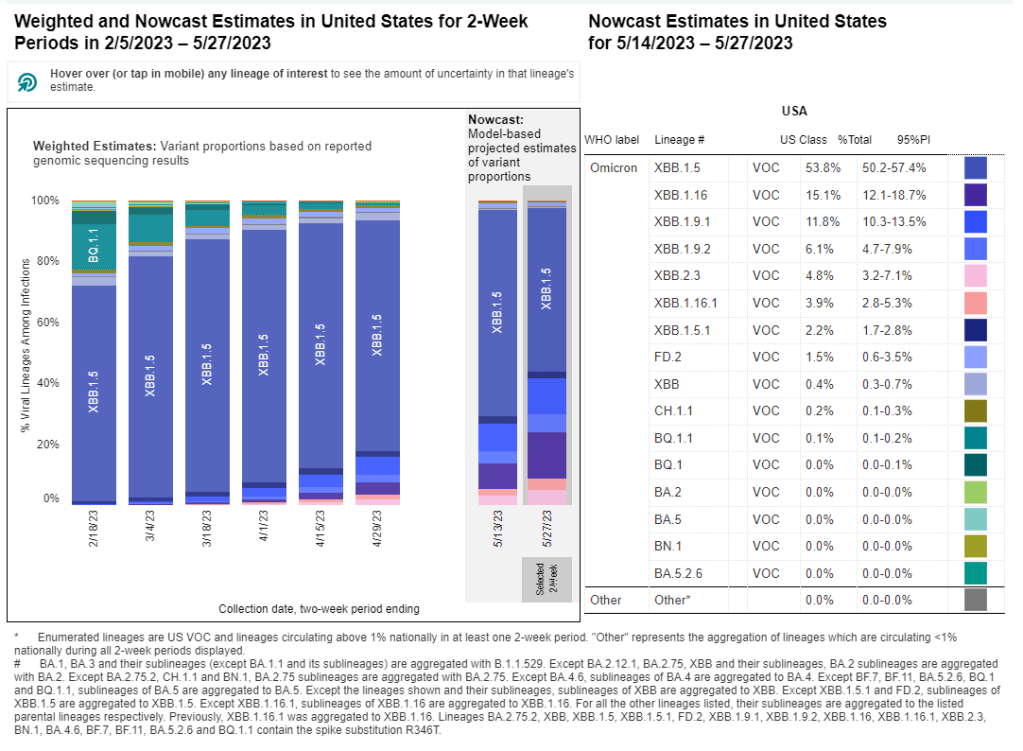
The CDC updated its variant estimates (now reported every other week) this past Friday. XBB.1.5 is still the most common lineage, causing an estimated 40% of cases, the CDC reports. XBB.1.16 and XBB.1.9 continue to outcompete it, causing about 26% and 21% of cases respectively.
These newer lineages have yet to contribute to a significant shift in transmission, from what I can tell. We have yet to see if past immunity in the U.S. can hold off against the ever-evolving Omicron variants this summer.
In the past week (May 14 through 20), the U.S. reported about 8,300 new COVID-19 patients admitted to hospitals, according to the CDC. This amounts to:
An average of 1,200 new admissions each day
2.5 total admissions for every 100,000 Americans
11% fewer new admissions than last week (May 7-13)
Additionally, the U.S. reported:
A 16% lower concentration of SARS-CoV-2 in wastewater than last week (as of May 24, per Biobot’s dashboard)
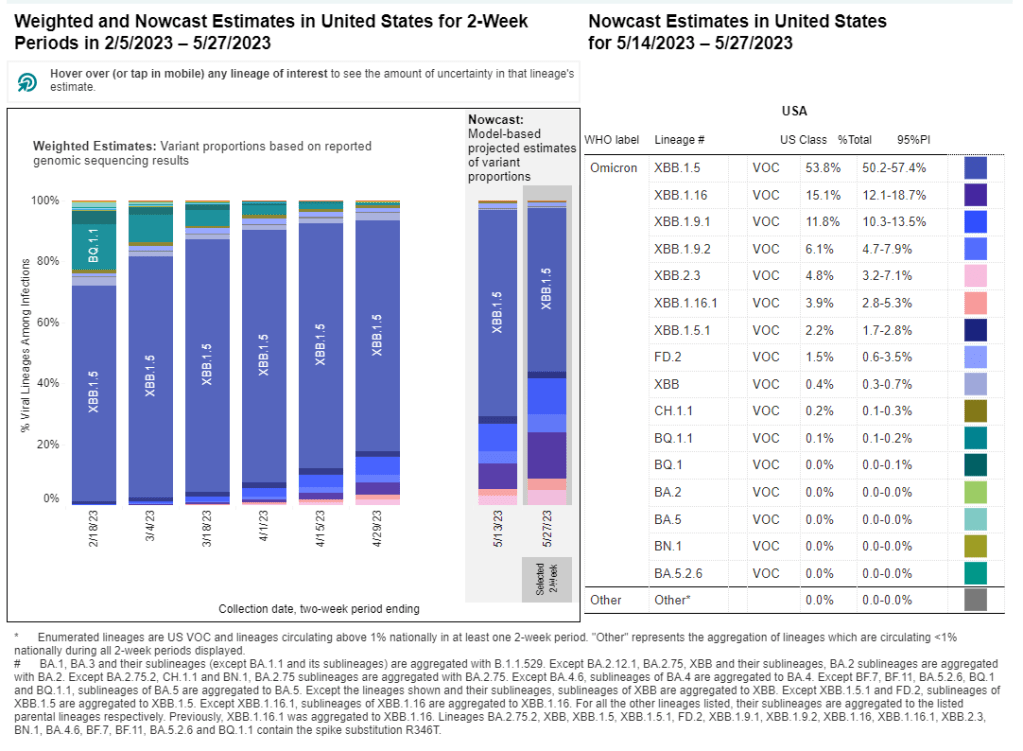
54% of new cases are caused by Omicron XBB.1.5; 19% by XBB.1.16; 18% by XBB.1.9 (as of May 27)
The COVID-19 plateau continues, with hospital admissions and viral levels in wastewater (the two main metrics I’m looking at these days) both trending slightly down at the national level. Newer Omicron variants are still on the rise, but don’t seem to be impacting transmission much yet.
Hospitalizations continue to trend slightly down across the board, though hospitals are still reporting more than 1,000 new COVID-19 patients each day. The vast majority of U.S. counties have low hospitalization levels, according to the CDC, with just 14 counties in the medium or high categories.
Coronavirus levels in wastewater are following a similar pattern: trending down very slightly, continuing the middling plateau of the last couple of months. All four major regions are still in this holding pattern, according to Biobot’s data.
We have new variant data this week, as the CDC is now on a biweekly schedule for updates. XBB.1.5 caused just over half of new cases in the U.S. in the two weeks ending May 27, as it slowly gets outcompeted by newer versions of Omicron. XBB.1.16 and XBB.1.9 continue to rise, causing 19% and 18% of hew cases respectively.
XBB.1.16 is most prevalent on the West Coast, the Northeast, and the Gulf Coast states, while XBB.1.9 is most prevalent in the Midwest, according to the CDC—though these estimates are becoming less reliable over time, since so few COVID-19 samples are sequenced.
The CDC has also recently added national and regional COVID-19 test positivity data back to its dashboard, representing tests conducted by labs in the CDC’s National Respiratory and Enteric Virus Surveillance System.
Nationally, test positivity is trending down, at just under 5% of COVID-19 tests (in this lab network) returning positive results in the most recent week of data. Test positivity is trending up slightly in the Northeast and New York/New Jersey regions; I’ll be following to see if this continues in the coming weeks.
Finally, a bit of good news: excess deaths in the U.S. have returned to baseline in the last couple of months. While hundreds are still dying from COVID-19 every day, the excess death trend suggests that the disease is currently not causing a significant ripple effect on overall mortality the way that it did in earlier stages of the pandemic. (Of course, this could change with a new surge.)