The Open Notebook has launched a new community program, called the Covering Science Slack, which could be a great opportunity for some journalist readers of the COVID-19 Data Dispatch. In this Slack server, general assignment and local journalists who are interested in improving their science reporting skills engage in discussions with experienced science journalists, who serve as mentors.
After a 12-week pilot program in 2022, the Covering Science Slack is now expanding: applications are open for a new cohort to join the Slack community. This iteration of the program has funding for regular discussions and activities through at least September 2023, and it’s free for participants.
Here’s how TON describes the program in their call for applications:
This community includes local and general-assignment reporters and editors, as well as a smaller number of experienced science journalists who serve as mentors within the group. Members are invited to seek (and offer) advice on any topic related to covering science, such as how to exchange ideas on topics such as finding suitable expert sources, refining story angles, evaluating scientific studies and claims, making sense of new findings and their implications, and more. Members can also participate in various types of learning opportunities and activities, including one-on-one peer mentoring, guided Slack discussions, reading groups, webinars centered on core challenges of covering science, and informal virtual gatherings.
With support from the Burroughs Wellcome Fund, we are now accepting applications for new members. The program will run at least through September, 2023, and we hope to establish the program as a sustainable, continuously running community.
I know a lot of COVID-19 Data Dispatch readers are local or general-assignment journalists; if you fit into this category, please consider applying to join the Slack server! It’s a great opportunity to learn more about science reporting in an informal setting, with a relatively low time commitment. Also, I’m now one of the mentors in the server, if that’s a draw for anyone.
Transparency note: This is not a paid advertisement or anything in that capacity, though I have written for The Open Notebook in the past (including a collaborative project between TON and the CDD). I’m just sharing this because I think it’s a valuable opportunity and would love for readers to take advantage of it.
Last week, in response to my call for donations to the COVID-19 Data Dispatch, I received some very generous support from readers. Thank you to everyone who donated—you are truly helping me keep this a free, accessible publication for anyone following COVID-19 news.
Following up on last week’s post, I wanted to share some suggestions for other COVID-related organizations that are taking donations this holiday season. If you have the resources and are looking for places to donate, please consider these nonprofits!
Body Politic, which runs one of the foremost Long COVID online support groups, is seeking donations to transition from a grassroots, all-volunteer organization to a format that’s more sustainable in the long-term. Their funding goal is $500,000.
The COVID-19 Longhauler Advocacy Project seeks donations to support its work advancing Long COVID research and supporting patients. Like Body Politic, this organization was founded by volunteers themselves dealing with Long COVID.
Marked by COVID is a nonprofit advocacy organization, also volunteer-run, seeking recognition of the Americans who lost their lives to COVID-19 and improved public health policies in the U.S.
Peste Magazine is a new online magazine focused on health journalism, advocacy, and the arts. The publication’s work so far has focused on COVID-19 but also includes other health justice topics; donations help to support payments for writers.
ME Action is a leading advocacy organization for people with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), a chronic condition that shares many symptoms with (and is often co-diagnosed with) Long COVID. Since the pandemic started, it’s also been involved with Long COVID advocacy.
Solve ME/CFS is another advocacy organization for ME/CFS and now Long COVID, focused particularly on funding and supporting research on these conditions.
Dysautonomia International is a leading advocacy group for dysautonomia, an umbrella term for conditions involving a malfunctioning autonomic nervous system. Similar to ME/CFS, dysautonomia is often a co-diagnosis for Long COVID.
Your local mutual aid group: Early in the pandemic, hundreds of mutual aid groups started across the country to help share food and other supplies with people in need. Some of them are still doing this important work! Websites like Mutual Aid Hub and this NYC directory can help you find a group in your area.
Disclaimer: This is not sponsored content, these recommendations come from my own research and reporting on COVID-19. If you’d like to recommend another organization, let me know and I’ll include it in a future issue.
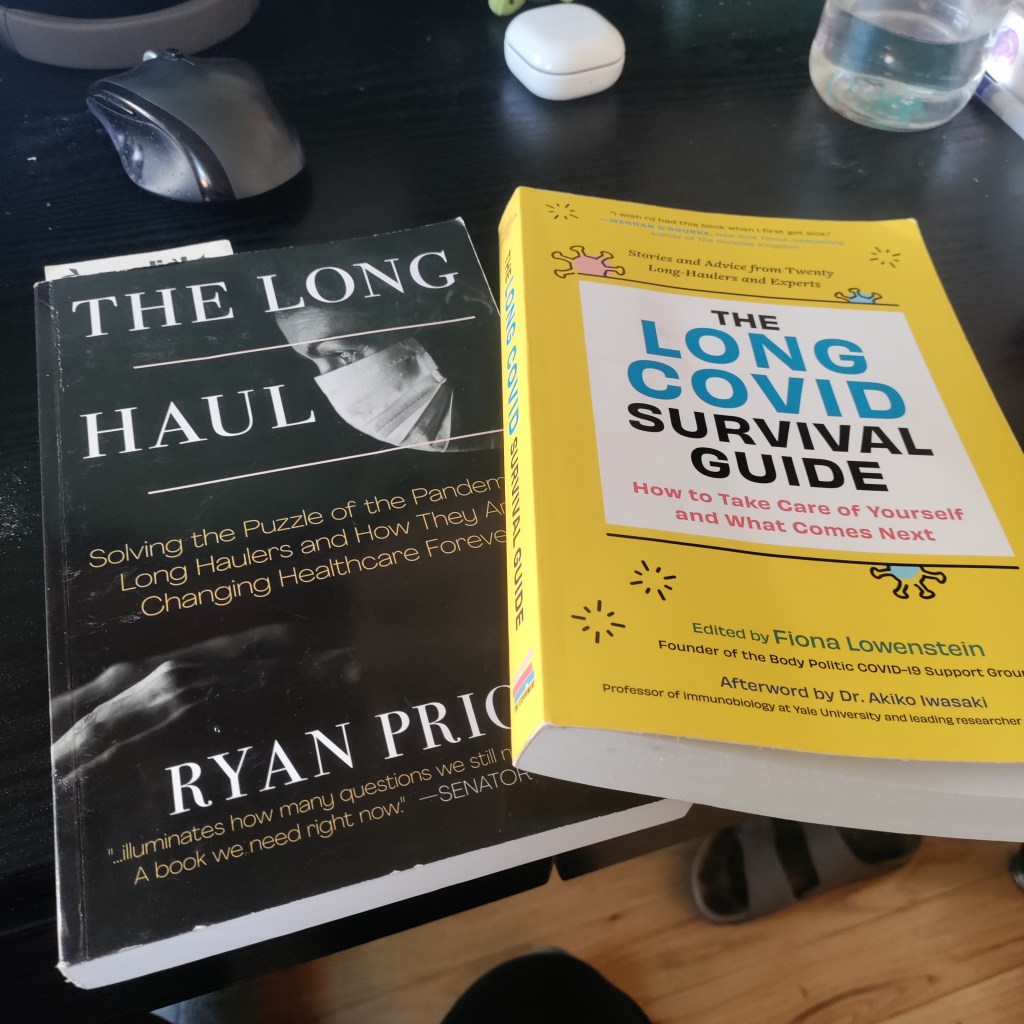
The Long Haul and The Long COVID Survival Guide, pictured on Betsy’s desk. (Photo by Betsy Ladyzhets.)
Two new books about Long COVID were published this month, and I’d like to recommend both of them to any readers interested in learning more about the condition—especially to other journalists covering COVID-19.
First, The Long COVID Survival Guide (from the Experiment Publishing, released November 8) is a compilation of essays from people with Long COVID, for people with Long COVID, edited by journalist and Body Politic founder Fiona Lowenstein. The book covers everything from getting a medical diagnosis to finding community with advocates for other chronic illnesses.
The Survival Guide is structured like a manual, every chapter ending with specific “survival tips” for long-haulers to use in their own Long COVID journeys. But it’s also a very relevant read for people who don’t have Long COVID, as it provides context about the different challenges long-haulers might go through: medical gaslighting, cognitive challenges, women’s health issues, learning to ask for help, and more.
Personally, I got a lot of ideas for future journalism projects from this book. As someone covering scientific research and data, I found the chapters about getting a diagnosis (by Dona Kim Murphey, Rachel Robles, and David Putrino) and about navigating Long COVID research (by Lisa McCorkell) particularly valuable.
Second, The Long Haul (from Simon & Schuster, released November 15) is a nonfiction narrative about how people with Long COVID came together to better understand the condition and advocate for themselves. Author Ryan Prior is a journalist with experience at CNN and other national outlets, and has lived with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) since he was a teenager.
Prior brings his lived experience and his journalistic experience—which includes covering other chronic illnesses and patient advocacy movements—to covering Long COVID. The book provides valuable backstories on major Long COVID groups, like Body Politic, the Patient-Led Research Collaborative, and the COVID-19 Longhauler Advocacy Project. It also describes early research efforts seeking to better understand Long COVID, including the first stages of the National Institutes of Health’s RECOVER study.
I’m still reading The Long Haul (as of this writing, I’m a couple of chapters in), but am already finding it incredibly helpful to learn about how Long COVID advocates started pushing for research and recognition, with context from ME/CFS and other post-viral illness work.
The Long COVID Survival Guide and The Long Haul might not be the most upbeat reading choices for the holiday season, but they’re really vital for anyone engaging with Long COVID—whether you’re a journalist covering this topic or a friend to a long-hauler. To quote from Dr. Akiko Iwasaki’s afterword, in the Survival Guide:
Long COVID has changed the narrative. The world no longer has any excuse to make the same mistake over and over again, as we have done for previous pandemic and endemic infections. It’s finally time for us to listen.
Transparency note: I received advanced copies of both of these books to aid in my work as a journalist covering Long COVID, but am not getting any compensation to write this post—i.e., this isn’t sponsored content or anything. I genuinely want more people to learn about and read these books!
Masked Science Writers attendees watch a conference session. Photo by Betsy Ladyzhets.
A couple of weeks ago, I wrote that the Science Writers conference—which I attended in-person—had great COVID-19 safety policies, better than other events I’ve gone to this year.
The meeting of about 450 science journalists and communicators included required masks indoors, outdoor space for meals, and a vaccine requirement, among other safety measures. As I write this, about three weeks after the conference, there have been no reports of COVID-19 outbreaks (though the organizers were not requiring attendees to share all test results).
I’ve previously reported on COVID-19 safety at large events, so I wanted to learn more about how the Science Writers organizers planned the conference and communicated policies to attendees. To find out, I talked to Tinsley Davis, executive director of the National Association of Science Writers.
Davis shared behind-the-scenes insight into planning the 2022 Science Writers conference and tips for other event organizers. Her insight might be helpful whether you’re organizing a large journalism meeting or a small family gathering at Thanksgiving.
Rather than transcribing the entire interview, I wrote a paraphrased summary (with quotes from Davis throughout). Let me know what you think about this format in comparison to past Q&As!
Paying attention to COVID-19 news, planning in advance
Representatives from both organizations meet regularly on a steering committee to plan the annual meeting, Davis explained. In early 2021, that group paid attention to the vaccine rollout and started thinking about safety for a potential in-person meeting in the fall.
“We are very fortunate to have, amongst our volunteer leadership, science journalists and science communicators, and people who are generally paying very close attention to not only what’s happening in the news, but what’s happening in the research community,” Davis said. “And they’re paying to attention to it both out of professional interests, but also out of personal interest… So we can leverage that in our discussions, and we don’t need to separately bring people up to speed.”
These discussions led to initial plans for a hybrid meeting in October 2021, which would have both in-person and virtual components. The in-person conference planned to include a vaccine requirement and other safety measures. But in August, when the Delta variant surged across the country, NASW and CASW decided to shift the meeting to only virtual.
Still, the 2021 plans and discussions proved to be helpful when the steering committee began to plan the next year’s meeting. “When we started the conversation in earnest in early 2022, we looked back to those policies that we had developed for 2021 and used those as a base to start thinking,” Davis said.
Collaborating with the venue
Science Writers 2022 took place in Memphis, Tennessee, with most events at the Renesant Convention Center. But unlike other conferences I’ve attended this year, most sessions with food were not held inside the convention center: the center had space available outside for people to eat and drink in a much lower-risk environment.
I asked Davis about how she and the other organizers planned for outdoor dining. Staff at the convention center were very receptive to safety requests, she said: “We were met with such support and creativity.” This included closing down a street outside the conference center for one outdoor lunch event, and taking advantage of another outdoor area that was closed to traffic.
It’s worth noting here, the weather really worked in favor of outdoor dining and socializing. For most of the weekend, temperatures were pleasant (in the 60s and 70s) and there was no rain. “It was a beautiful fall weekend,” Davis said.
In addition to the outdoor plans, venue staff shared what they’d learned about COVID-19 safety from hosting other large conferences in spring and summer 2022, Davis told me. That included plans for how to arrange chairs in conference rooms for social distancing, and using security guards (required for crowd control) to help “gently remind” conference attendees to keep their masks on. Staff were also “readily able to talk about MERV ratings,” a measure of ventilation in the building, Davis added.
Conferences like Science Writers typically aren’t able to extend their COVID-19 safety measures beyond attendees—in other words, the organizers can’t require convention center staff to mask up. But staff at the Resenant Convention Center “were very thoughtful about masking up” in conference spaces, Davis noted. (I observed and appreciated this as well.)
Balancing safety and cost
One of the best measures to reduce COVID-19 spread at a large event is rapid testing at the door, a safety policy backed up by scientific studies. But this type of mass testing can get pretty expensive for a conference of about 450 people, the size of Science Writers this year.
“Cost is part of any decision,” Davis said. “And anytime you put the word ‘conference’ in front of something, it gets way more expensive. Like even a cup of yogurt gets more expensive when you have the words ‘conference catering’ in front of it.”
Operating with a limited budget, the Science Writers organizing committee chose to prioritize an independent vaccine verification system, so that staff didn’t need to check all attendees’ vaccine cards upon arrival. They used the CrowdPass system and required everyone attending in-person to submit their vaccination information before traveling to Memphis.
CrowdPass does offer on-site testing, Davis said. It would have been a great layer of safety, “but that was just an order of magnitude more expensive, and not something we could afford.” The conference also didn’t require attendees to report positive COVID-19 tests, though people were encouraged to stay home if they felt sick before the conference.
Communication and control
In the U.S.’s current COVID-19 environment, with rapidly-spreading variants and limited safety measures in most places, having an entirely COVID-free event is not really possible, Davis said. “What we did want to do is try and mitigate as much as possible in the spaces that we could control,” she explained.
“Spaces of control” included vaccine verification before the event, required masks in the conference center, and prohibiting eating or drinking during sessions so that attendees stayed masked in those settings. Outside of the official event—in spaces like hotel elevators or nearby bars—the conference organizers had less control.
But the safety policies for official events made it easier for attendees of varying COVID-19 risk comfort levels to participate. Making the conference broadly accessible was a priority for organizers, Davis said, as was providing safety information well in advance.
“We tried to be very thorough, very clear, communicate early, and to really manage expectations,” she said. “We wanted someone to know, when they registered, exactly the kinds of precautions that we would be taking as a conference, and what would be expected of them as an attendee, and to really underlie it with the ‘why.’”
Organizers aimed to clearly convey why this conference was taking COVID-19 safety so seriously: to help keep the community safe so that a wide group of people could participate. “We are so lucky as a community to be able to even ponder getting back together in person after two and a half horrible years, that we really owe it to each other, to be as thoughtful as possible,” Davis said.
Overall, the communication strategy seemed effective: throughout the conference, Davis had to remind “exactly one person” to put a mask on, she said. It probably helped that many people attending the meeting had reported on COVID-19, or at least had closely followed pandemic news in their communities.
“It was very heartening to see the level of, not just compliance with the COVID policies, but really the embracing of and the appreciation for them,” Davis said. Regardless of personal risk, everyone followed the conference policies.
COVID-19 safety as a statement of values
When I posted about the Science Writers conference’s COVID-19 safety policies on Twitter, one commenter pointed out that this meeting had “more precautions than some medical conferences.”
Incredible to see how Science Writers conference is taking more #COVID precautions than some medical conferences! https://t.co/skvFBRThi1
I asked Davis for her thoughts on this comment, as well as how the safety measures on display at the conference showed NASW and CASW’s organizational values. “Not being a medical professional myself, but being someone who organizes conferences, I’m really proud of the values that we were able to bring forward and really proud of our community for complying with them, if not embracing them,” she said. She acknowledged, however, that as a relatively small conference, Science Writers might have been able to prioritize safety in a way that would’ve been more challenging for a bigger event.
Our conversation ended with a few other tips for organizers of large events:
Make COVID-19 safety “a continuing part of the conversation,” not just a “box that you need to tick off.” Organizers should keep an eye on the evolving COVID-19 landscape and be prepared to adjust their policies if needed.
Think about accessibility tradeoffs, such as when and for whom masks should be required. For example, Science Writers allowed speakers to take off their masks while at a distance from audience members so that people could read their lips and see facial signals if needed.
Take note of any tricky situations that come up and plan for the next year, so that safety measures and communications can continuously improve over time.
Put your COVID-19 policies online! Davis and other organizers found it helpful to look at public safety policies from other organizations. “Someone will find the experiences you’ve had helpful in craft crafting their own event, even if it’s much, much smaller than yours,” she said.
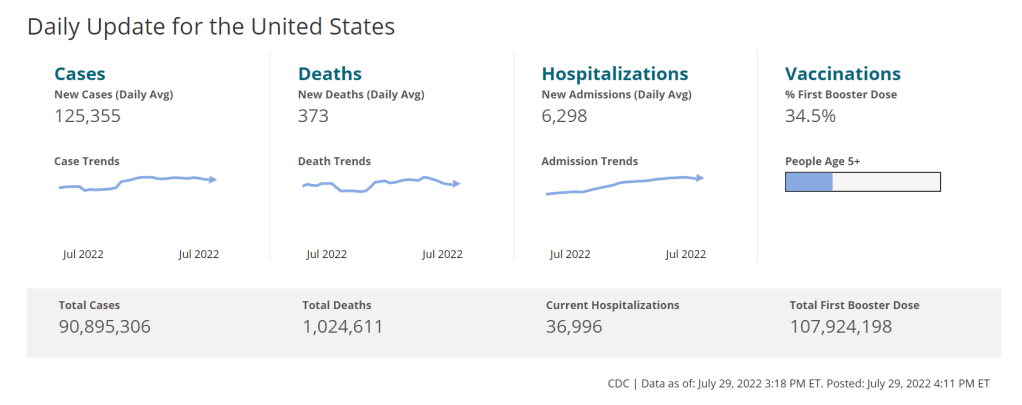
As of this week, the CDC has switched to reporting COVID-19 cases and deaths on a weekly basis.
As of this Thursday, the CDC is updating COVID-19 case and death data every week instead of every day. Here are some thoughts on interpreting COVID-19 data in the wake of this change, citing an article I recently wrote for The Atlantic.
To me, the CDC’s shift to weekly updates feels like the end of an era for tracking COVID-19. While I understand the change, considering both our less-complete case information and other data analysis needs for the agency, I can’t help but wish we had a national public health agency with enough resources to continue providing us with frequent, reliable information on this ongoing pandemic. After all, shouldn’t that be the CDC’s job?
The CDC has clearly deprioritized two major metrics (cases and deaths) that used to be the first places people looked to see the pandemic’s impact on their communities. Instead, the agency now points us to hospitalization metrics, variant surveillance, and wastewater—all metrics that are certainly useful, but may be harder for the average user to interpret.
And even the case data we do have are quite unreliable at this point, as PCR tests become less and less accessible compared to rapid tests. Case numbers may be underreported by twenty times or more; it’s difficult to even get a good estimate of how far off the numbers are. Public communications like the CDC’s “Weekly Review” report fail to acknowledge this problem, and the agency does not appear to be making any effort to determine the true infection rates right now.
Through its current data communication choices, the CDC seems to be saying, “If you still care about keeping track of COVID-19, you’re on your own.” Even though we are likely heading for a fall surge and many people need to keep track of this disease in order to keep their communities safe.
In absence of useful information from our public health leaders, it falls on us to survey the best available data sources and help others interpret them. My article in The Atlantic takes on this question, focusing on wastewater surveillance and population surveys as particularly useful sources we should consider right now.
Interpreting wastewater data
Wastewater data, unlike case data, don’t require people to actively go out and get tested: if their public sewer system is getting sampled for COVID-19, they will automatically be included in the data. You can look for wastewater surveillance in your area on Biobot’s dashboard, the CDC’s dashboard, or other state and local dashboards, depending on where you live. (I have a list of state dashboards here.)
But interpreting wastewater data can be pretty different from interpreting case data. Here are a couple of key tips for approaching this source, based on my interview with Biobot president and cofounder Newsha Ghaeli:
Look at “directionality” and “magnitude.” “Directionality” means whether viral levels are going up or down, and “magnitude” means how they compare with earlier points in the pandemic. To quote from the story: “A 10 percent uptick when levels are low is less concerning than a 10 percent uptick when the virus is already spreading widely.”
If you do not have public wastewater data for your county, data from a neighboring county still provides useful info. When we talked, Ghaeli gave the example of a New York City resident looking at data from New Jersey or Connecticut counties neighboring the city: as people from these areas commute into NYC, a surge in one place could quickly drive a surge in the other.
Wastewater data are not a perfect proxy for infections. Scientists are still learning about how to best use this newer surveillance tool. Unlike clinical metrics (like cases), wastewater data can differ based on local environmental factors, and it often takes a long time for researchers to build useful interpretations of their communities. (See my past FiveThirtyEight story for more detail on this.)
These data can’t tell you who is getting sick. To comprehensively answer demographic questions, we need to actively survey people in our communities and ask them about their experiences with COVID-19. (See the story for more about how this works.)
Other interpretation tips
Beyond looking at wastewater data, here are a couple of tips I received from experts for readers seeking to watch their local COVID-19 numbers this fall:
“Look as local as you can,” said Pandemic Prevention Initiative expert Sam Scarpino. In other words, if you can find data for your individual county or even ZIP code, go there.
Consider local events and behavior, Scarpino said. Quoting from the story: “If a popular community event or holiday happened recently, low case numbers might need to be taken with a grain of salt.”
I also wanted to give a quick shout-out here to the People’s CDC, a volunteer science communication and advocacy organization. If you’re looking for more thoughtful analysis of national COVID-19 data, their weekly “weather reports” are a really helpful and accessible source. The organization also provides resources to help people push for more COVID-19 safety measures in their communities.
“People do want layers of protection, they do want to keep themselves in each other safe from COVID,” said Mary Jirmanus Saba, a geographer and volunteer with the People’s CDC whom I interviewed (with a couple of other volunteers) for my story. The weather reports and other similar initiatives help the organization’s followers “see that we really are there for each other,” she said.
On July 26, 2020, I sent out the first COVID-19 Data Dispatch newsletter. In the two years since that day, I have sent newsletters (and published blog posts) every Sunday, with no breaks. I’ve posted from vacations, over holidays, and on days when I was exhausted or approaching burnout.
While this schedule has felt punishing at times, I’m proud of it. The coronavirus doesn’t care about holiday schedules, after all, and I enjoy maintaining regular updates for the readers relying on this publication as a key source of COVID-19 news. (Also, not many writers can say they’re more consistent than the CDC.)
But even I have to admit that two years without breaks is a long time. When I’m scrambling to send out an issue every Sunday, it’s difficult to reflect on key questions, like, “Is my current posting format meeting readers’ needs?” and, “What does helpful COVID-19 coverage look like right now?” I wouldn’t call myself burned out, but at a few points in the last few months, I have felt like I’m operating on autopilot: writing around 3,000 words every weekend because it’s my routine, without evaluating how I might improve that routine.
This is a rather longwinded way of announcing that I’m about to take a break from the COVID-19 Data Dispatch. August 2022 will be a brief hiatus: over the next four weeks, I won’t write any newsletters or blog posts. I’m also taking this month off of freelancing and working fewer hours at my part-time job, making it basically the longest vacation I’ve had since graduating college.
I plan to use this time to reflect on this project’s future, including potential format and content changes that might make it easier for me to maintain long-term. I’m also going to reflect on some potential CDD side projects—more resources, events, even a podcast idea?—that I haven’t had the bandwidth to pursue while producing weekly issues.
Readers: if you have any feedback for me, please reach out! I would love to hear from you about the topics and formats you’d find helpful at this point in the pandemic.
I also wanted to share some tips for keeping track of COVID-19 data while this publication is on a break, as I’m very aware that we are still in an active surge across the country. (This post is also responding to a reader question that I received from a fellow data reporter last week, after I announced this upcoming break in the newsletter.)
Look at multiple data sources or metrics.
COVID-19 case data, once our best window into the virus’ spread, are becoming much less reliable thanks to a decline in PCR testing. Other singular metrics have their own flaws: hospitalization numbers often lump together patients admitted for severe COVID-19 symptoms with those who tested positive while admitted for other reasons; wastewater data are unevenly reported across the country and can be hard to interpret; death data lag significantly behind transmission trends, and so on.
As a result, it’s important to check a few different metrics rather than relying on just one. For example, you might notice that my “National numbers” posts these days typically cite cases, hospital admissions, and wastewater together to identify national trends.
Similarly, if I were trying to identify what’s going on in New York City, where I live, I would likely look at: case and test positivity data from the city health department, cases in public schools (which include positive at-home test results) compiled by the department of education, and wastewater data from Biobot, focusing on the northeast region and counties in the greater NYC area.
Case rates are still useful, if we acknowledge that they are undercounts.
Hospitalization rates are useful, particularly new hospital admissions.
The CDC’s old transmission level guidance is still actually pretty helpful for guiding health policies, especially for vulnerable populations.
Look at wastewater surveillance, if it’s available in your area.
The COVID Cast dashboard, from Carnegie Mellon University’s Delphi Group, is another helpful source.
Look at multi-week trends.
Just as you don’t want to rely on a single metric, you shouldn’t look at only one week of data. (Looking at just one or two days at a time is an even worse idea.) This has always been a good rule for interpreting COVID-19 numbers, but it’s even more true now, as many public health departments have fewer resources devoted to tracking COVID-19—and may take more time to compile data for a given day or week.
For example, the New York City health department’s daily updates to its COVID-19 dashboard frequently include changes to case numbers for prior days, in addition to new data for the past day. Experts call this “backdating”: in a data update on a Friday, new cases might be dated back to other days earlier in the week, changing broader trends.
Keep in mind data reporting schedules.
You especially need to be wary of backdating when there’s a holiday or some other interruption in reporting. For this reason, it’s important to keep track of reporting schedules: know when a health department is and is not updating their data, and interpret the data accordingly.
The biggest example of this is that most state and local health departments—and the CDC itself—are no longer updating COVID-19 data on weekends. In most places, every Saturday and Sunday is now essentially a mini-holiday, with numbers from those days incorporated into backdated updates on Mondays. (And then edited in further backdated updates on later weekdays.)
When I volunteered at the COVID Tracking Project, we regularly observed lower COVID-19 numbers on weekends, followed by increases towards the middle of the week when states “caught up” on cases that they didn’t report over the weekend. You can read more about this trend here; I suspect it has only become more pronounced as more places take weekends off.
Acknowledge uncertainty in the data.
This is the most important recommendation I can give you. Every COVID-19 number you see comes with a margin of error. Sometimes, we can approximate that margin of error: for example, we can estimate how far official COVID-19 death statistics might be off by looking at excess deaths. Sometimes, we really can’t: estimates of how far official case numbers might be off range from a factor of three to a factor of thirty.
As a result, it’s often helpful to look at trends in the data, rather than trying to approximate exactly how many people in your town or county have COVID-19 right now. Is transmission trending up or down? Are you at high risk of encountering the coronavirus if you go to a large gathering? These questions can still be answered, but the answers will never be as precise as we’d like.
Follow leaders from your local healthcare system.
To augment official data sources, I often find it helpful to see what people in healthcare settings are saying about COVID-19 trends. Experts like Dr. Craig Spencer (who works in an ER in NYC) and Dr. Bob Wachter (who leads the University of California San Francisco’s department of medicine) frequently share updates about what they’re seeing in their practices. This kind of anecdotal evidence can help back up trends in case or hospitalization data.
In a similar vein, you can look to essential workers in your community, like teachers and food service workers, as early indicators for transmission trends. If NYC teachers and parents are talking about more cases in their schools, for example, I know COVID-19 spread is increasing—because schools are often sources for transmission in the broader community.
Keep your goals in mind.
As you monitor COVID-19 numbers, it’s important to remember why this information is valuable. What are you using the numbers for? Are you making choices about when to put a mask on, or when to rapid test before a gathering? Are there high-risk people in your family or your broader social network whom you’re trying to protect? Or, if you’re a journalist, what questions are you trying to help your readers answer?
Keeping track of COVID-19 data and news can feel like a large burden, especially when it seems like so many people have entirely forgotten about the pandemic. I always find it helpful to remember why I do this: to stay informed about this ongoing health crisis, and to keep others in my community safe.
The author in a 3M respirator (with P100 filters), on the plane to Denver, Colorado.
This weekend, I traveled to Denver, Colorado for the final trip in an early-career fellowship which has covered some travel and trainings for me this past year.
Of course, going anywhere on a plane right now, during an intense COVID-19 surge, is not something I’d normally choose to do. This is basically my one plane trip of the summer; all my other travel has been by train and/or car. (And the fellowship event itself had some safety measures in place, eg. required masks and rapid tests.)
But I know a lot of people are traveling by plane right now—I know, because I saw so many of them at JFK Airport. So, I wanted to share a few things I did on this trip to reduce my risk.
First: I bought a respirator. These devices, considered to be a step above N95s/KN95s, are intended for use in occupational settings, such as for workers in chemical plants or firefighters going into smoke. You can read more about them on this CDC NIOSH (National Institute for Occupational Safety and Health) page.
I think of mine like a reusable N95 mask, with great longevity and an excellent seal to my face. I ordered one from 3M, which has several NIOSH-approved options. I also learned more about different respirators at Patient Knowhow, a site with reviews of a few major N95-equivalent options. (I recently talked to the site’s founder, Devabhaktuni Srikrishna, for an upcoming article on ventilation.)
plane trip with respirator was a success! TSA asked me to take it off when I went through security (so I put on a disposable mask for a few minutes), but otherwise I had no issues. pic.twitter.com/SDUA4slIQY
It’s important to note that, if you get one of these respirators, you may need to order air filters separately. I got P100 filters, which are the highest grade. Another add-on may be an exhalation valve filter, which cleans the air you exhale out of your respirator (basically, further ensuring that you aren’t getting other people sick as you wear it).
Now, one challenge with these respirators is that they may freak people out a little. I feel like a bug-eyed sci-fi villain with mine on; though I’m well-accustomed to NYC’s blase attitude towards weird behavior, so I don’t mind if I freak people out. For others, this could be a greater concern.
Respirators also aren’t common mask options yet, though they seem to be growing more popular—my Twitter selfie of me in my respirator on the plane got over 200 likes. But they aren’t yet well-known in transit settings. While I personally didn’t have issues (other than a bit of confusion at JFK’s security screening), I know that others have been told to take these off on flights. It’s good to have a backup N95/KN95 in case that happens.
Second: I follow guidance from ventilation experts. If you’d like to read about how plane ventilation works, masking options, and other small ways to improve travel safety, you can find a lot of this advice on Twitter. “Ventilation Twitter,” as I recently described it to a journalist friend, is generally very welcoming and willing to triage questions.
One key piece of advice: while I kept my respirator on throughout my flights (seriously, the briefest breaks possible for water and food), I made especially sure to stay masked while planes were at the gate or landing. These are the points in a flight when the plane’s ventilation system isn’t switched on, making masking more important.
Saahil Desai provides a helpful explanation of these priority periods for masking in a recent Atlantic article. Though I’d like to note, some experts have suggested that the article downplays the importance of masking as much as you can throughout a flight and using other safety strategies as well.
More helpful threads on this subject…
Top 10 tips everyone should know about wearing #N95 & #elastomeric masks.
Third: I avoid indoor dining as much as possible. This is, of course, one of the highest-risk settings for catching the coronavirus, because you have to take your mask off to eat or drink—while others nearby are also unmasking to eat or drink.
Sometimes, one can be put into tricky situations when there are truly no outdoor dining options (such as on a long airplane trip). But even in that scenario, there are ways to reduce risk. For example, when I needed to eat breakfast at JFK Airport, I found a corner of an unused gate where I could be relatively far from other people, rather than sitting in a crowded food court area.
I also appreciated that the other fellows in my group followed my recommendation for an outdoor dinner on Thursday evening, before our official activities started!
And finally: lots of testing. Remember, rapid tests can indicate whether you’re actively spreading the coronavirus, but PCR tests are still the gold standard for accuracy. I try to get PCR tests before and after travel or large gatherings, to be certain of my status. (Though I acknowledge that I live in NYC, where public testing is still available, albeit in decline.)
This trip went from Thursday to Saturday, with the riskiest event being an indoor dinner on Friday evening. My tests included: PCR test on Wednesday (same-day results); rapid test on Thursday morning; rapid test on Friday morning; rapid test on Friday evening (right before the dinner); rapid test on Saturday morning; and a planned PCR test for next Wednesday or Thursday. Rapid tests and symptom monitoring were also required for the rest of my group.
Is all of this inconvenient? Sure, somewhat. But I consider it worthwhile to have a safe trip and protect the people around me. If you have other safety tips or questions on this topic to share, please reach out and let me know.
In the last few weeks, I’ve been thinking a lot about how to remain hopeful.
COVID-19 continues to spread—in fact, the U.S. is likely in the second-largest surge of the entire pandemic right now—but we aren’t counting the majority of cases, much less taking collective health actions to prevent them. Leaders across the political spectrum have largely shrugged off any potential for new safety measures, instead focusing on business interests.
It takes a lot of effort not to simply give up, in this environment. Sometimes, at a gathering or on the New York City subway, I feel a lot of peer pressure to just take off my mask and ignore the risks. But I think about people I’ve talked to in my reporting: Long COVID advocates, people with weakened immune systems, exhausted experts, school officials working to keep their students safe, and so many others. In solidarity with them, I keep the mask on.
I thought about solidarity this week, when I read Ed Yong’s latest COVID-19 feature in The Atlantic. The story is headlined, “America is Sliding into the Long Pandemic Defeat.” But I like the subtitle better: “In the face of government inaction, the country’s best chance at keeping the crisis from spiraling relies on everyone to keep caring.”
In this piece, Yong takes readers through a history of public health’s connections to other social movements, and introduces us to people across the U.S. who are making those connections now. He talks about community health work: “It creates a bedrock of trust and solidarity, without which public health cannot operate.” And he talks about the potential for new policies and health infrastructure that could save lives, even in our current COVID-ambivalent climate.
Obviously, you should read the full story. I personally found it motivating to continue my own COVID-19 work. But, in reflection, I also wanted to share a few ideas for how to find hope and solidarity in this difficult period. This is a little outside my usual data wheelhouse, but it’s informed by my two years of reporting on (and living through) this pandemic.
Here are eight suggestions.
Talk to people. To friends, family members, people you meet at the grocery store, and so on. Ask them, “Did you know, we’re in a surge right now?” “Have you received your booster shot?” “Do you know where to get free rapid tests in our community, and when to use them?” The simplest questions can spark valuable conversation, in my experience.
Educate specifically about Long COVID. Show people the recent statistics from the Household Pulse Survey, now the best estimates we have for how many Americans are currently dealing with this condition. Talk about potential symptoms and how the condition may impact someone’s life. There is still not enough awareness in the U.S. about how COVID-19 can cause more than short-term symptoms; individual conversations can help with this.
Ask for the extra safety measures. If your friend is hosting a party, for example, can you ask them to instruct the guests to rapid test beforehand? If you’re attending a large meeting, can you ask the organizers about recommending masks? Even if not everybody follows the guidance, people might think about safety in a way that they hadn’t before. And vulnerable people in the room will be grateful that they didn’t need to do all the asking themselves.
Make connections around health. How can you build trust in public health in your community? Who are the leaders who could help advocate for measures like free testing, or would continue to encourage vaccinations when we likely need a new round of booster shots in the fall? Think about who you know, and how they can help.
Advocate for federal measures. This means funding for more vaccines, tests, and treatments, of course. But it also means federal air quality standards for buildings. Protections for essential workers. Disability rights, which could include (as Yong’s story notes) requiring masks when a disabled person may be present. Call your representatives, and ask them what they’re doing in these areas.
Learn about public health history. There are actually a lot of precedents that we can draw on for COVID-19 advocacy, Yong explains in his story. These range from the Black Panthers serving breakfast at schools to ACT UP pushing for a new paradigm in clinical trials. Reading history like this can provide ideas for current actions.
Reframe language around safety measures. Nobody likes a “mandate” or a “requirement.” Americans hate following rules. For this reason, I often see health experts instead using words like “safety measures,” and explaining why they work. Connecting to the language of a particular community can also help; for example, in activist spaces, I remind people that “we keep us safe” also applies to COVID-19 protections.
Think about the long game. What can you do to maintain energy, avoid burnout, and share your resources with others? This is another lesson from history, I think: even if I feel discouraged about a lack of change in the short-term, I remember that true paradigm shifts take a long time. Hope is a long-term practice.
I wrote about a change in hospitalization data, which had just shifted from the purview of the CDC to a different team at the Department of Health and Human Services (HHS). This felt like a niche topic at the time, but I wanted to provide a clear explanation of the change after seeing some misleading articles and social media posts suggesting that the CDC was losing control of all COVID-19 data.
At the time, my goals were simple: explain where COVID-19 data come from and how to interpret the numbers; provide tips and resources for other reporters on this complicated beat; and help people in my broader social network understand pandemic trends. The COVID-19 Data Dispatch’s aims haven’t changed too much, even as I’ve expanded it to its own website, worked with guest writers, coordinated events, and more.
As I look back on 100 issues, I wanted to share a few lessons for other reporters still on the COVID-19 beat (and, more broadly, anyone working on public health communications). I’m also sharing a couple of notes from readers about how the publication has helped them.
Lessons I’ve learned:
Lay readers can handle complicated topics! You don’t need to overly simplify things, just use clear language and examples that are easy to follow. This is honestly my entire ethos as a science writer so I found it hard to pick an example post, but one may be my piece on why U.S. Long COVID research is so difficult, which built on reporting for a Grid feature.
FAQs are good formats for breaking down complex topics or new information. I like to use FAQ formats and lots of subheaders whenever I’m writing about a new variant (or subvariant) of concern, like this post on BA.4 and BA.5, or when walking through the implications of a federal guidance change, like this post discussing testing and isolation with the Omicron variant.
Consistency is key. One thing I frequently hear from readers is that they appreciate the regularity of COVID-19 Data Dispatch issues; if they tune out of other pandemic news, they can still expect me to deliver some important updates once a week. This is definitely a built-in advantage of the newsletter format, but I try to take the consistency further by having regular sections (such as “National numbers”) with statistics reported in a similar way each week.
Emphasizing the same issues over and over can feel repetitive to the writer, but it’s helpful for readers. Whenever I remind readers about holiday data reporting lags, for example, I have to remind myself that most people are not constantly thinking about COVID-19 trends the way that I am—and might not be consistently reading my newsletters, either. It’s another aspect of being consistent.
Provide trends and context, not just isolated numbers. This is another key aspect of my “National numbers” updates: I always explain how a given week’s case or hospitalization numbers compare to previous weeks. Another important piece of context, I think, is where numbers come from: for example, reminding readers that case numbers mainly include PCR test results, not at-home antigen test results.
Acknowledge uncertainty! This is crucial in any kind of data reporting, especially when reporting from data systems that are as flawed and incomplete as the U.S.’s COVID-19 data systems. For example, last month’s post about interpreting limited data during our undercounted surge explains the limitations of several common sources, as well as what the sources can still tell us.
Provide readers with tools to see local data. This is a central reason why so many publications built COVID-19 dashboards in 2020, and why some outlets continue to maintain them now. People love to look up their states or counties! I often don’t have the bandwidth for hyperlocal visualizations myself, but point to these resources in “Featured sources” updates whenever possible.
Use readers’ questions to drive reporting. Some of my favorite COVID-19 Data Dispatch posts have been inspired by reader questions, from the “Your Thanksgiving could be a superspreader” post in fall 2020 to my explanation of why the CDC’s isolation guidance is not based on scientific evidence earlier this spring. If you write to me with a question, you’re probably not the only person with that question—at least, if my metrics on these posts are anything to go by.
Testimonials from readers:
Josh Zarrabi (software engineer at the Health Equity Tracker): “You’re, like, the only COVID news I get anymore. Every Sunday morning with my coffee.”
Chris Persaud (data reporter, Palm Beach Post): “Thanks to your newsletter, I’ve found useful data for my news reports.”
Jeremy Caplan (director of Teaching & Learning at Newmark J School): “COVID-19 Data Dispatch is consistently informative. I limit my COVID news diet, so it’s helpful to have this singularly focused resource for keeping up with the data.”
Congrats to the COVID-19 Data Dispatch on its upcoming 100th post. @c19datadispatch by @BetsyLadyzhets is consistently informative. I limit my COVID news diet, so it's helpful to have this singularly focused resource for keeping up with the data. Sign up: https://t.co/mEu1Af6f6W
My Grandma: “In our Berkeley family (C, P and me) we have relied on you and your newsletter for helping us through these difficult times. The research, guidance and advice in your Data Dispatch, is invaluable.”
Thank you to all of my readers for your support over the last 100 weeks. I hope the COVID-19 Data Dispatch can continue to provide you with the news and resources you need to navigate the (continuing!) pandemic.
This weekend, I spoke on a panel at the Association of Health Care Journalists (AHCJ) annual conference, held in person in Austin, Texas. (Yes, the irony of my first air travel post-end of the mask mandate being a trip to a health journalism conference is not lost on me.)
My session focused on COVID-19 data, particularly the data gaps left by the federal government—which, longtime readers know, is a topic I’ve reported on extensively. We provided attendees with a tipsheet, sharing some source suggestions and tips for reporting on this topic.
Derek Kravitz, my editor and project lead of the Documenting COVID-19 project, moderated the session; Nsikan Akman, health and science editor at Gothamist/WNYC, was another panelist. Dr. Katelyn Jetelina, author of the incredible Your Local Epidemiologist newsletter, was scheduled to be a panelist as well, but unfortunately couldn’t make it to the conference last minute. (Her contributions are still reflected in our slides and tipsheet, though.)
During the session, we discussed a range of COVID-19 data topics, including:
The lack of standardization for COVID-19 data collection and reporting in the U.S., exacerbated by our decentralized healthcare and public health systems;
Discrepancies between New York State and New York City data, as an example of this lack of standardization (a specialty for Nsikan);
Challenges around (and some recommendations for) communicating COVID-19 data to audiences;
One of the most challenging aspects of reporting on the pandemic has been accessing reliable, accurate data about COVID-19 and its impact on Americans. The need for trustworthy, real-time data has caused a few journalism and nonprofit groups to create repositories to pull together data from varying sources.
A Thursday session at Health Journalism 2022 in Austin, “The quest for COVID-19 data: Where “official sources” fell short and journalism stepped in,” focused on these efforts and provided journalists with a wealth of resources for up-to-date data related to the pandemic.
Most high-income countries have national health care systems, so data collection and collation is far more straightforward than in the federalized U.S. health care system, where a mix of private and public payers are governed by national and differing state laws. Without a national registry or centralized healthcare system, it’s been harder to track statistics on COVID cases, hospitalizations, deaths, vaccinations, and other relevant numbers.
The tipsheet from this session includes links and blurbs to a few of the panel’s favorite COVID-19 data sources, including:
CDC mortality data, cleaned and sorted by Documenting COVID-19
HHS Community Profile Reports
MCH Strategic Data’s COVID-19 in schools dashboard
COVIDPoops19 dashboard
Historical wastewater data from CDC NWSS
Long COVID Source List
Health Equity Tracker
Open Government Data
And the tipsheet also includes a few tips for communicating COVID-19 data, supplemented with stories that provide useful examples. Here are the tips:
Explain where data come from and how they’re collected – using as little jargon as possible.
Be clear about uncertainties and caveats; what can’t the data tell you?
Share how data points, trends or study results can be translated into actionable information for readers.
Use questions from readers to guide reporting.
Look for differences in how state and municipalities track their COVID-19 data.
Look for ways that data collection methods (or the lack of clear methods) may hide health inequities.
Use visuals/multimedia to communicate the pandemic’s immense tolls.
Provide larger context about the reasons why COVID-19 data in the U.S. are often fractured and difficult to interpret.