The Delta variant (also known as B.1.617.2) was first identified in India earlier this spring. It’s now known to spread more easily than any other variant found so far and evade immunity from a prior COVID-19 infection. Scientists are also investigating the variant’s potential to more easily cause severe disease—as well as links to a “black fungus” that has become a secondary epidemic in India.
Harvard epidemiologist William Hanage called the variant “really, really anxiety-inducing,” STAT’s Andrew Joseph reports. (If you’d like to read more on the biology of this variant, Joseph’s article provides a useful overview.)
The Delta variant was first identified in the U.S. in April. It’s making up a small fraction of new cases at the moment, but is spreading rapidly: from an estimated 1.3% of cases on May 8, to 2.5% of cases on May 22, to 6.1% of cases on June 5. The June 5 estimate comes from CDC’s Nowcast predictions, which extrapolate from the most recent available sequencing data (typically reported with a lag of two weeks or more.)
The share of cases caused by this variant appears to be doubling every two weeks, which means that Delta could become the dominant variant here this summer. Some data suggest that domination could happen within a month—a dashboard run by the testing company Helix puts Delta at 10% of new cases as of May 31, suggesting an even faster transmission rate for the variant.
Helix scientist Alexandre Bolze wrote on Twitter that Delta could become dominant “next week or next 2 weeks” based on these trends.
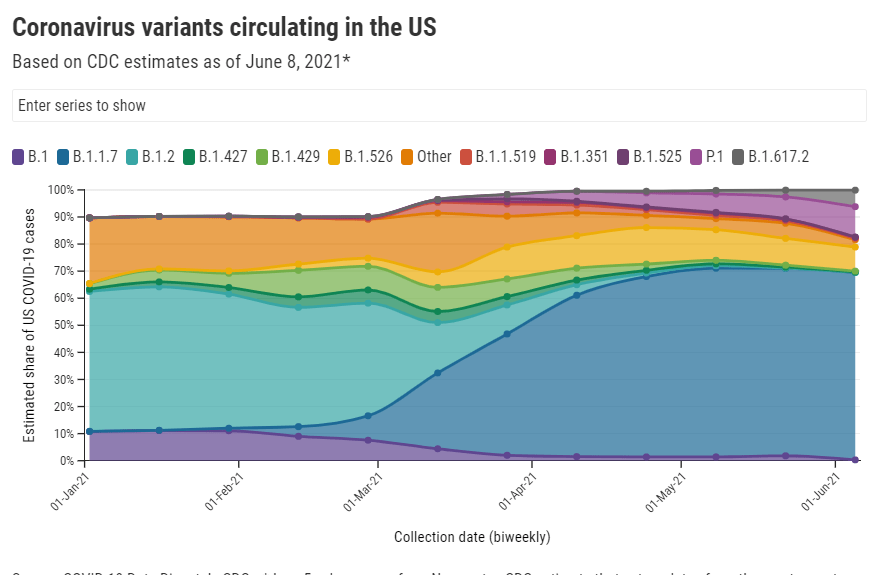
Other variant trends also support Delta’s dominance. This variant, along with Gamma (or P.1, the variant first identified in Brazil), appears to be outcompeting other variants of concern in the U.S. Alpha (or B.1.1.7) has now plateaued at around 70% of U.S. cases, according to CDC data. The variants found in California and New York, both of which made up more than 10% of new cases earlier in the spring, are now declining.
While the CDC is not yet publishing data on Delta’s prevalence in individual states, we can assume that state-by-state variant trends—especially in those states where Delta cases were first identified—are reflecting the variant’s rise on a national level.
Many experts are now looking at Delta’s spread in the U.K. as a portent for its spread here. The variant has become dominant in the U.K., thoroughly outcompeting Alpha, and is driving a new surge—even though over half of the British population has received at least one vaccine dose. In fact, the U.K. has delayed its full reopening plans by a month due to this case resurgence.
The COVID-19 vaccines currently in use in both the U.K. and the U.S. do work well against Delta, especially the Pfizer and Moderna vaccines—and especially after a full two-dose regimen is complete. But anyone not yet vaccinated is highly vulnerable to this variant. In the U.K., the current case surge is driven by young adults and teenagers who aren’t yet eligible for vaccination.
As physician and public health expert Vin Gupta put it: “Being unvaccinated on June 9, 2021 is much more risky to your own wellbeing than being unvaccinated on June 9, 2020.” And the longer one waits, the riskier this condition becomes.
The Delta variant should serve both as an additional reason for those in wealthy nations who aren’t yet vaccinated to get their shots—and a reason for wealthy nations to share doses with the rest of the world.
B.1.1.7. B.1.351. P1. B.1.671.2. It’s exhausting trying to keep up with emerging SARS-CoV-2 variants with names as inscrutable as these.
But thankfully, we finally have a straightforward naming system: on May 31, the WHO announced a system using letters of the Greek alphabet. B.1.1.7 (first identified in the U.K. is now Alpha, B.1.351 (first identified in South Africa) is now Beta, and so on. You can find the complete list (so far) here. While there are an innumerable amount of SARS-CoV-2 variants, so far the WHO naming system only applies to “variants of concern” and “variants of interest.”
While there have been non-place-related names for these variants for a while, colloquially they have been called things like “the U.K. variant” and “the South African variant” because most people won’t just toss “B.1.1.7” around in conversation. (I tried, and no one knew what I was talking about.) However, this is problematic for a few reasons. First, we don’t know for sure that B.1.1.7. originated in the United Kingdom — that’s just where they found it first. And for other countries, naming a coronavirus variant after them associates a dangerous stigma with that country (like how nicknaming the coronavirus “the China virus” earlier in the pandemic contributed to a rise in anti-Asian hate). According to WHO coronavirus lead Maria Van Kerkhove in an interview with STAT News, a country will be more likely to report a variant if the name of the variant will not be associated with the country name.
The WHO naming system is nice for now, but it’s not clear if it’ll catch on and become the norm or if it’ll just be yet another naming system in a crowded patchwork. It’s also unclear what will happen if we run out of Greek letters, but we certainly hope it doesn’t come to that. (Making this yet another reason to vaccinate the world.)
Earlier this month, the CDC made a pretty significant change in how it tracks breakthrough cases. Instead of reporting all cases, the agency is only investigating and collecting data on those cases that result in hospitalizations or deaths.
In case you need a refresher: “breakthrough cases” are those infections that occur after a patient is fully vaccinated (including both doses, if applicable, and the two-week waiting period after a final dose). These cases are rare—like, one in ten thousand rare. As I wrote back in April, it’s important to contextualize any reporting on these cases with their incredible rareness so that we hammer home just how effective the vaccines are.
But just because breakthrough cases are rare doesn’t mean we shouldn’t pay attention to them. In fact, it’s critical to pay attention to these cases in order to monitor precisely how well our vaccines are working—and how new variants may threaten the protections those vaccines provide.
Breakthroughs can offer a unique wellspring of data. Ferreting them out will help researchers confirm the effectiveness of COVID-19 vaccines, detect coronavirus variants that could evade our immune defenses, and estimate when we might need our next round of shots—if we do at all.
As I’ve discussed in past variant reporting, numerous studies have demonstrated that the vaccines currently in use in the U.S.—especially the Pfizer and Moderna vaccines—work well against all variants. That includes variants of concern, such as B.1.617 (from India), B.1.351 (from South Africa), and P.1 (from Brazil). But the vaccine efficacy rates for some of these variants are lower than that stellar 95% we saw in Pfizer and Moderna’s clinical trials. And some common therapeutic drugs don’t work well for patients infected with variants, too.
As a result, scientists are concerned that, while the vaccines are working well now, they might not work well forever. Whenever the coronavirus infects a new person, it has the opportunity to evolve. And that continued evolution must be monitored. The first coronavirus variant able to evade our vaccines may emerge in a foreign country with a raging outbreak—but it may also emerge here in the U.S. Closely monitoring all breakthrough cases will help us find that dangerous variant.
(Of note: A new, potentially-concerning variant was identified just last night in Vietnam; WHO scientist Maria Van Kerkhove described it as an offshoot of the variant from India, B.1.617, with “additional mutation(s).”)
With that in mind, let’s unpack the CDC’s reporting change. When the vaccine rollout started, the agency was investigating all breakthrough cases that came to its attention—including those in patients with only mild symptoms, or with no symptoms at all. According to an agency study released this past Tuesday, the CDC identified 10,262 such breakthrough cases from 46 U.S. states and territories between January 1 and April 30, 2021.
Keep in mind: By April 30, about 108 million Americans had been fully vaccinated. Dividing 10,262 by 108 million is where I got that “one in ten thousand” comparison I cited earlier. As I said: very rare.
Starting on May 1, however, the CDC changed its strategy. Now, it is only tracking breakthrough cases that result in severe illness for patients, leading to hospitalization and/or death. The CDC says that this choice is intended to focus on “the cases of highest clinical and public health significance” rather than tracking down asymptomatic cases.
In its May 25 report, CDC scientists said that 27% of the breakthrough cases identified before May 1 were asymptomatic. 10% of the infected individuals were hospitalized, though almost a third of those patients were hospitalized for a reason unrelated to COVID-19. Only 160 patients (less than 2% of the breakthrough cases) died.
We need to take these numbers with a grain of salt, though, because the CDC has likely undercounted the true number of asymptomatic cases. Both clinical trials and studies on vaccine effectiveness in the real world have suggested that those people who get infected with COVID-19 after completing a vaccination regime are more likely to have mild symptoms, or no symptoms at all.
Plus, the CDC is recommending that vaccinated Americans don’t need to get tested before traveling, if they have come into contact with someone known to have COVID-19, or for many of the other reasons that many of us got tested this past year. (The agency is still recommending that fully vaccinated people get tested if they’re experiencing COVID-19 symptoms, though.)
As I wrote at Slate Future Tense last month, such guidelines are likely to drive down the number of COVID-19 tests conducted across the U.S. And this trend seems to be happening, so far: PCR tests dropped from their winter surge levels this spring, and are now dropping again. (Antigen and other rapid tests may be getting used more, but we don’t have any comprehensive data on them.)
With that drop in testing—combined with the overall challenge of identifying asymptomatic COVID-19 cases outside of dedicated studies—it would be pretty damn hard for the CDC to track down all breakthrough cases. The agency’s focus on more serious cases instead may thus be considered a conservation of resources, directing research efforts and care to those Americans who get seriously ill after vaccination.
But “a conservation of resources” is also a nice way of saying, the CDC made a lazy choice here. The agency has poured money into genomic surveillance over the past few months, sequencing over 20,000 cases a week (compared to a few thousand cases a week before Biden took office). In recent weeks, the Biden administration has announced renewed funding for public health and similar commitments to prioritizing scientific research. If the CDC wants to find and sequence breakthrough cases in order to identify vaccine-busting variants, there should be nothing stopping the agency.
Or, as epidemiologist Dr. Ali Mokdad told the New York Times: “The C.D.C. is a surveillance agency. How can you do surveillance and pick one number and not look at the whole?”
Out of those 10,262 cases that the CDC reported this week, only 5% had sequence data available—but the majority of those sequined cases were variants of concern, including B.1.1.7 and P.1. At The Atlantic, Wu reported that epidemiologists in some parts of the country are seeing more breakthrough cases tied to concerning variants, while others are seeing breakthrough case sequences that match the overall infections in the community.
To me, this high level of unknowns and uncertainties mean that we need more breakthrough case reporting and sequencing, not less. And we need a national public health agency that commits to true surveillance, so that we aren’t flying blind when the coronavirus inevitably evolves beyond our current defenses.
I don’t understand why only 5% of COVID vaccination breakthrough infections are being sequenced. Wouldn’t sequencing breakthrough cases be highest yield for picking up emerging variants? https://t.co/ErgFpNQh5s
Following the end of the federal public health emergency in May, the CDC has lost its authority to collect vaccination data from all state and local health agencies that keep immunization records. As a result, the CDC is no longer providing comprehensive vaccination numbers on its COVID-19 dashboards. But we still have some information about this year’s vaccination campaign, thanks to continued CDC efforts as well as reporting by other health agencies and research organizations.
This week, the FDA authorized Novavax’s updated COVID-19 vaccine. Here’s why some people are excited to get Novavax’s vaccine this fall, as opposed to Pfizer’s or Moderna’s.
Last week, I asked you, COVID-19 Data Dispatch readers, to send me your stories of challenges you experienced when trying to get this fall’s COVID-19 vaccines. I received 35 responses from readers across the country, demonstrating issues with insurance coverage, pharmacy logistics, and more.
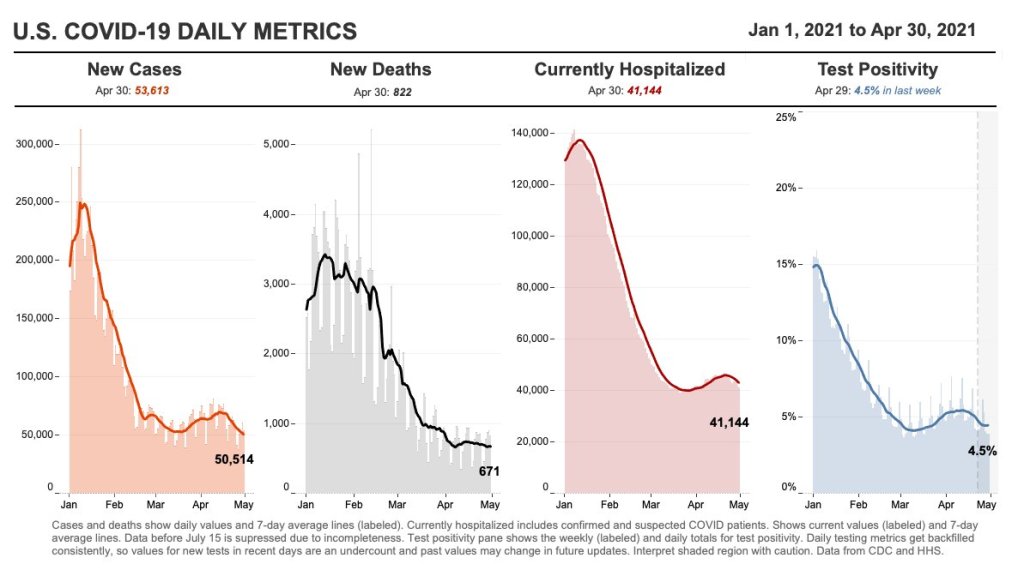
In the past week (May 22 through 28), the U.S. reported about 151,000 new cases, according to the CDC. This amounts to:
An average of 22,000 new cases each day
46 total new cases for every 100,000 Americans
22% fewer new cases than last week (May 15-21)
Last week, America also saw:
21,900 new COVID-19 patients admitted to hospitals (6.7 for every 100,000 people)
3,000 new COVID-19 deaths (0.9 for every 100,000 people)
70% of new cases in the country now B.1.1.7-caused (as of May 8)
An average of 1.4 million vaccinations per day (per Bloomberg)
Cases, deaths, and hospitalizations all continue to drop nationwide. The U.S. reported about 3,000 COVID-19 deaths last week, in total—at the peak of the winter surge, we saw more than 3,000 deaths a day.
This trend is echoed in most states. In the May 27 Community Profile Report, the HHS classifies almost every state as “orange” (between 50 and 100 new cases per 100,000 residents over the past week) or “yellow” (between 10 and 50 cases per 100,000). Wyoming is the only state in the “red” classification, at 101 cases per 100,000 over the past week—while California is in the green, with only 9 cases per 100,000.
In New York City, where I live, every single ZIP code currently has a test positivity rate at 3% or lower—for the first time since last summer. This is yet another piece of good news showing how well the vaccines work. Half of the total U.S. population has had at least one dose and more than half of the adult population is fully vaccinated, as of yesterday.
The vaccines also continue to do their part against variants. The CDC variant data—updated this week—indicate that B.1.1.7 is still growing, but it’s leveling off as new cases slow. This variant has gone from causing about 60% of cases in early April, to 67% in mid-April, to 70% in early May; a much slower decline than what we saw in February and March.
Of more concern: P.1, the variant first identified in Brazil, is causing 7% of U.S. cases as of May 8—and the CDC’s Nowcast estimate puts it at almost 10% of cases by May 22. B.1.617, the variant first identified in India, is also sharply increasing; its case share doubled from April 24 to May 8. Both of these variants are more transmissible (B.1.617 dangerously so) and may have lowered vaccine efficacy.
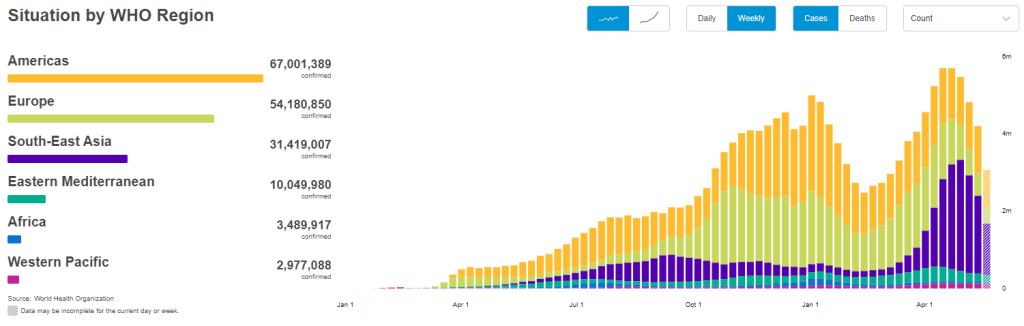
But the harm these variants can cause in the heavily-vaccinated U.S. pales in comparison to the risk they pose in other nations. As evidenced by the World Health Organization chart above, the share of cases in Southeast Asia and other lower-income nations is increasing even as cases in the U.S. and Europe drop. The U.S. should focus on providing aid to the nations where vaccinations are lagging so that we can help inoculate people before more, harder-to-contain variants evolve.
In other words, there’s a reason I’m not giving space to the lab leak theory in this publication. If you’d like to read more about the issue, I recommend this article by Amy Maxmen.
very fun and fresh how the "china deliberately released a bioweapon" narrative is "suddenly plausible" and "taking over global covid discourse" now when the US is hoarding vaccines and basically refusing to send supplies/money/etc to other nations :))))
— betsy ladyzhets 📊 (@betsyladyzhets) May 28, 2021
Two more important CDC data updates for this week:
Vaccine demographics, for the past 14 days and over time: This week, the CDC added a new category to its Vaccine Demographics page. Previously, the page allowed users to compare overall first dose and fully vaccinated rates for different race/ethnicity, age, and sex groups; now, you can also make those comparisons specifically for vaccinations in the last two weeks. For a time series view, check out the Vaccine Demographic Trends page, which shows vaccination rates over time—now available for race/ethnicity, sex, and age. The race/ethnicity view clearly shows that White and Asian Americans are getting vaccinated at higher rates than other groups.
Variant tracker “Nowcast”: Loyal CDD readers will already know that I love to drag the CDC for reporting their variant data with an enormous lag; often the most recent figures on the agency’s Variant Proportions page are a month old. Well, maybe somebody on their team is reading, because this week, the CDC added a new option to its variant dashboard that addresses this issue. Selecting “Nowcast On” (below the variant color bars) allows you to view prevalence estimates for the current week, in addition to the agency’s most recent week of data collection. A note below the dashboard explains that the “Nowcast” figures are based on modeling estimates that extrapolate from known proportions. For example, B.1.1.7 is known to cause 66% of U.S. cases as of April 24, but the “Nowcast” estimate puts it at 72% of cases as of May 8. This is actually pretty useful, thanks CDC!
It takes three to four weeks for data on a variant COVID-19 case to be made public. I have been quietly stressing out about this fact for about a month, since I learned it from Will Lee, VP of science at the genomics company Helix.
I talked to Lee for a recent Science News piece on the drivers and demographic patterns of the U.S.’s April rise in COVID-19 cases. During our conversation, he shared many details of Helix’s coronavirus sequencing process; most of this information was too technical for me to include in my Science News story, but in the COVID-19 Data Dispatch, I can get as technical as I want.
Here’s an excerpt from our interview, following my question: What is the turnaround time for sequencing? How does it compare to getting a PCR test result?
It is much, much slower. The median time from collection to [PCR] results, it’s varied quite a bit over time, but I think right now, for many labs, it’s less than 48 hours. And so what we do is, after the test result is done—we’re only picking from positive tests, obviously, for sequencing—so we would select the sample, probably somewhere on the order of two to three days after the sample is collected, after the test result is reported. From then, I’d say there’s probably seven to ten days before the sequencing result is available…
What happens is, we do the [PCR] test result, we send it out for sequencing. The turnaround time for sequencing—I’d say in a good case, it’s in the seven to eight day timeframe, sometimes it’s longer than that. There’s an additional holdback on the data before we make it publicly available, because the CDC wants to make sure that public health agencies have time to act on the information first, if it turns out [the case is] someone in their jurisdiction who’s identified to have a variant of concern. That’s potentially another week, depending on how fast they [the local public health agency] act.
And then there’s additionally a lag for when you submit to somewhere like GISAID, and however long it takes them to do their review process and publish it. You add it all together, and you end up with something like 3-4 weeks [from test sample collection to sequence publication].
So, let’s recap. Here’s what it takes to sequence and report a coronavirus variant case:
PCR test: 1-2 days
The testing company selects the positive test sample for sequencing: 1-2 days
Genomic sequencing takes place: 7-10 days
Local public health department gets notified, uses the sequencing results for contact tracing: Up to one week
Sequence is submitted to a public repository: Possibly another 1-2 weeks
When you add all this up, it’s no surprise that the most recent variant data on the CDC’s COVID Data Tracker are as of April 10, almost four weeks ago. I’m focusing on this process today because I believe the data lag is worth emphasizing. When you see a news report about B.1.1.7 or another variant, remember that the data took several weeks to get from test sample to newspaper.
In other words, when the CDC tells us that B.1.1.7 now makes up about 60% of new cases in the U.S., remember that this number is a snapshot from a month ago. The true number as of today, May 9, is likely far higher.
My interview with Will Lee inspired me to look at lag times for other common variant data sources. Let’s compare:
CDC’s Variant Proportions page,data from the national genomic surveillance program: Lag of 2-4 weeks, depending on how far away one is from an update when checking the page. (The CDC updates this page every two weeks.)
Helix’s Surveillance Dashboard, data from the company’s testing sites: Lag of 3-4 weeks. As of May 8, Helix is reporting B.1.1.7 sequence data as of April 15 and SGTF data as of late April. (SGTF, or S gene target failure, is a coronavirus mutation which usually indicates that a case is B.1.1.7-caused.)
Nextstrain dashboard, data from GISAID: Lag of 1-2 weeks. When I looked at Nextstrain’s coronavirus page yesterday, the most recent available sample sequences were collected on May 1 and the global variant frequencies chart ended at April 27.
CoVariants dashboard, data from Nextstrain/GISAID: Lag of 2-4 weeks, depending on the country. As of May 8, CoVariants reports data from the week of April 19 for some countries with more robust sequencing programs (U.S., U.K., etc.) and data from the week of April 5 for others.
Nextstrain and CoVariants, both of which are powered by the public sequence repository GISAID, have more recent data than the CDC—likely because academic labs can submit sequences to GISAID without waiting on public health departments. Helix has a lag similar to the CDC’s because its partnerships require the company to submit sequences to public health departments before releasing the information publicly. Some state public health departments report variant data of their own, but this is often done in press releases rather than regular dashboard updates.
Now, bearing in mind that the variant data are all weeks old, what are the most recent variant numbers for the U.S.? And why should we be worried about these variants?
Here’s a status check on the major variants I’m watching:
B.1.1.7 (first identified in the U.K.): Causing about 60% of cases nationwide as of April 10. Among the states where the CDC reports variant data, it’s most prevalent in Tennessee (74%), Michigan (71%), Minnesota (68%), Georgia (65%), and Florida (63%). This variant is concerning because it spreads a lot more easily than older coronavirus variants; estimates range from 40% to 70% more transmissible.
B.1.526 (first identified in New York City): Causing about 12% of cases nationwide as of April 10. This variant is also likely more transmissible, but a recent CDC report suggests that it does not lead to more severe disease or increased risk for vaccine breakthrough cases. B.1.526 has yet to be classified nationally as a variant of concern, so the CDC isn’t publishing state-by-state data for it. (But if you live in NYC, check out this Gothamist article for ZIP code-level prevalence data.)
B.1.427/B.1.429 (first identified in California): Causing about 6% of cases nationwide as of April 10. I suspect the pair may be getting outcompeted by B.1.1.7, as it was representing closer to 10% of cases in a previous CDC reporting period—it’s more transmissible than the wildtype coronavirus, but not as transmissible as B.1.1.7 . This variant pair is most prevalent in California (38%), Arizona (28%), and Colorado (24%).
P.1 (first identified in Brazil): Causing about 4% of cases nationwide as of April 10. This variant has been tied to surges in Brazil and other South American countries; it’s more transmissible, associated with a higher death rate, and can reinfect patients who already recovered from COVID-19. While it currently represents a fairly small share of U.S. cases, computational biologist Trevor Bedford recently pointed out that P.1. “has been undergoing more rapid logistic growth in frequency” compared to other variants.
B.1.351 (first identified in South Africa): Causing about 1% of cases nationwide as of April 10. Soon after it was identified last December, the COVID-19 vaccines were shown to be less effective against this variant. But “less effective,” for the mRNA vaccines, is still pretty damn effective, as this recent study from Qatar demonstrates.
B.1.617 (first identified in India): Not yet represented in CDC data, but it’s been identified in several U.S. states over the course of April and May. This variant is strongly tied to India’s recent surge. While you may see it called a “double variant” because it has mutations at two key coding sequences, B.1.617 doesn’t actually have double the transmission bump or double the severity of older coronavirus variants, as explained here by epidemiologist Katelyn Jetelina.
It’s also worth emphasizing that genomic sequencing is still not conducted evenly across the country. The CDC releases state-by-state variant prevalence data for states which have submitted more than 300 coronavirus sequences in a four-week period. As of April 10, only half of the states have met this benchmark; many states in the Midwest and South still aren’t represented in the CDC’s data.
I am considering adding a variant data annotations page to the CDD website, in order to more consistently keep track of all the different info sources on these lineages. Would you use this page? What information would you like to see there? Shoot me an email (betsy@coviddatadispatch.com) or leave a comment here on the website to let me know.
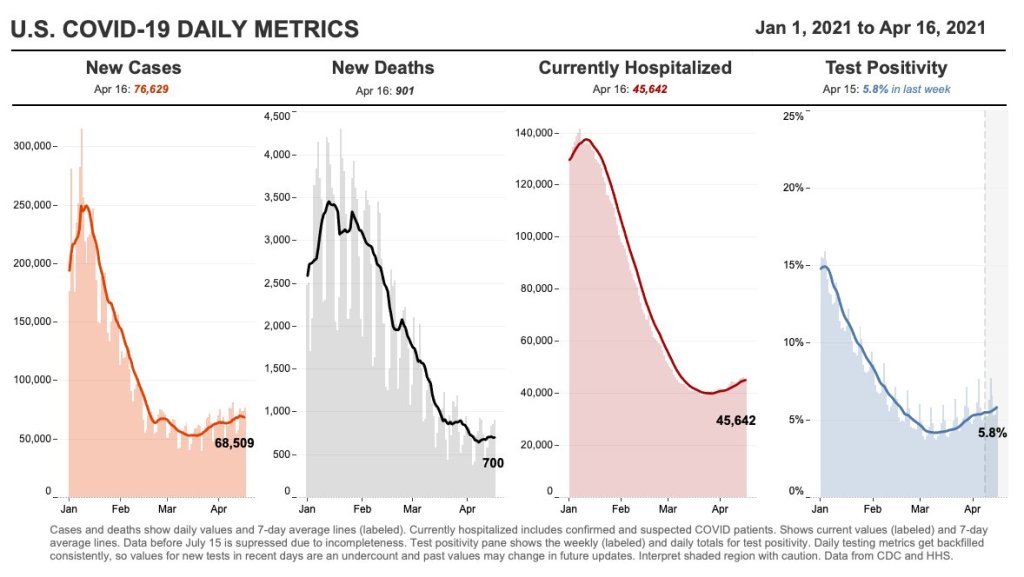
35,400 new COVID-19 patients admitted to hospitals (11 for every 100,000 people)
4,400 new COVID-19 deaths (1.3 for every 100,000 people)
59.2% of new cases in the country now B.1.1.7-caused (as of April 10)
An average of 2.55 million vaccinations per day (per Bloomberg)
New cases are down for the second week in a row—good news after the 70,000-plus peak of mid-April. Still, 50,000-plus cases in a day is no good place to plateau, new hospital admissions remain over 5,000 a day, and vaccinations are slowing: the U.S. is now averaging about 2.6 million shots a day, down from 3.4 million a couple of weeks ago.
As we discussed last week, the U.S. vaccination campaign has entered a phase in which supply is higher than demand. Even with Johnson & Johnson now back on the market, many of the people who were desperate to get their shots have already secured those doses, leaving public health experts and local leaders to figure out how to both lower access barriers and alleviate concerns in less vaccine-confident communities.
There is one good piece of vaccine news this week, though: several states are closing their vaccine equity gaps, according to Bloomberg’s tracker. White vaccination rates are slowing more drastically than rates in minority populations, allowing those communities to catch up. “Since early February, Alabama, Louisiana, Maryland, Mississippi and North Carolina have narrowed their Black vaccination gaps most,” Bloomberg’s team reports.
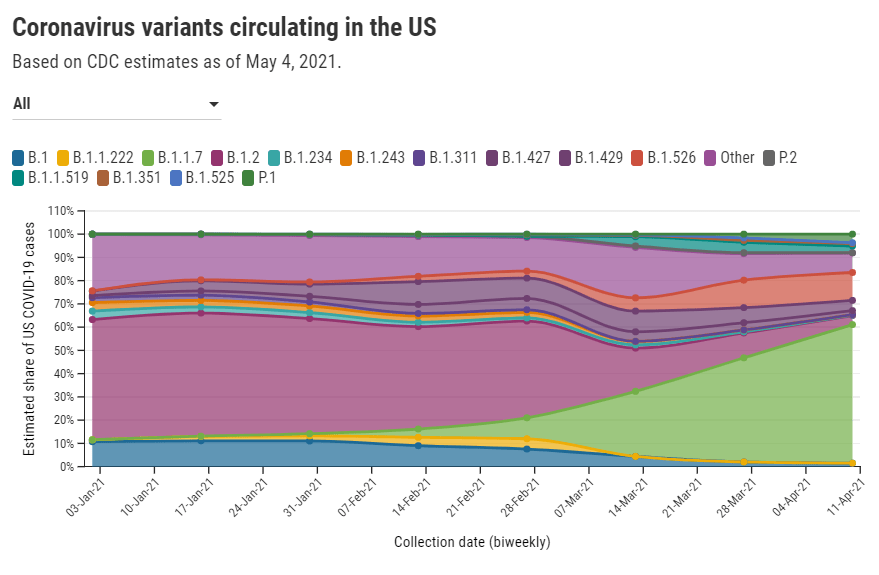
Meanwhile, the coronavirus variants just keep spreading. The CDC updated its variant proportions data this week, reporting that B.1.1.7 is now causing a clear majority of COVID-19 cases in the country (59%). Michigan, Minnesota, and Tennessee have B.1.1.7 proportions closer to 70%. B.1.1.7 also appears to be outcompeting the California variants (B.1.427/B.1.429) in parts of the West where those variants had previously dominated. Still, as we keep emphasizing, these data are several weeks old; this week’s CDC update includes figures as of April 10, and the true B.1.1.7 numbers are likely higher.
Stay safe out there, readers, and help your communities get vaccinated.
This week, The Hill posted an article with a rather misleading headline: “CDC finds less than 1 percent of fully vaccinated people got COVID-19.” If you actually click into the piece, you’ll find that the precise number is less than 0.008%. Less than 0.0005% have been hospitalized and less than 0.0001% have died.
This headline reflects a common issue with vaccine reporting that I’ve seen in the past few weeks. A lot of journalists, especially those who aren’t familiar with the science/health beat, may be inclined to publish news of breakthrough cases as surprising or monumental. In fact, these cases—referring to a COVID-19 infection that occurs after someone has been fully vaccinated—are entirely normal, yet incredibly rare.
No vaccine is perfect. Even the Pfizer and Moderna vaccines, which both demonstrated 95% efficacy in their late-stage clinical trials and over 90% effectiveness in the real world, are not perfect. Scientists still expect a few COVID-19 infections to slip through the immune system defenses built up by these vaccines and cause illness in a small number of patients.
And it really is a small number: 129 million Americans have received at least one dose of a COVID-19 vaccine as of yesterday, per the CDC, and 82 million have been fully vaccinated. The agency has only documented 5,800 breakthrough cases. Less than 0.008% of those people who have been fully vaccinated. That’s the equivalent of one-quarter of a seat in Queens’ Citi Field baseball stadium (which seats about 42,000).
So, if you’re a journalist reporting on this issue—whether it’s nationally or in your community—it’s important to stress that denominator. 82 million fully vaccinated, 5,800 breakthrough cases. Emphasizing the difference in magnitude between these numbers can show readers that, while they should still maintain some caution after getting vaccinated, the vaccines are overwhelmingly safe and effective.
Small as the breakthrough case numbers are, though, it is important that we still talk about them. A new article by ProPublica’s Caroline Chen discusses how a failure to collect data on breakthrough cases is making it harder for COVID-19 researchers to understand what causes them. Specifically: we should be sequencing the genomes of the coronavirus strains that caused these cases, and by and large, we aren’t.
Chen describes how many state health departments aren’t getting breakthrough case samples to sequence, whether that’s due to testing labs failing to store the test samples or cases being identified through rapid tests, which do not have established pipelines. Plus, in some cases, we aren’t even recording whether the patients went to the hospital or died—key data points in the U.S.’s continued vaccine monitoring.
I definitely recommend you read the full piece, but here’s a section that will give you the big idea:
In many instances, patients’ samples are not sequenced to find out if a variant might have been involved; some labs are throwing out test samples before an analysis can be done; hospitals and clinics aren’t always collecting new samples to analyze them. That means that for so many people, nobody will ever know if a variant was involved, leaving public health officials without data to be able to examine the extent to which variants are contributing to breakthrough cases.
“It’s alarming that we can’t sequence more of the virus than we’re able to now — that’s something we need to resolve,” said Brian Castrucci, chief executive officer at the de Beaumont Foundation, a health philanthropy. “The more we know, the better we can react. We want to know the information so that we can make the right policy and health decisions.”
While the CDC has an info page on breakthrough cases, no data on these cases are available on the agency’s COVID-19 dashboard. Reporters need to walk a delicate line on this issue: pursue the data, but report it in a careful, conscientious way that appropriately puts the tiny breakthrough case numbers in context.
Following the end of the federal public health emergency in May, the CDC has lost its authority to collect vaccination data from all state and local health agencies that keep immunization records. As a result, the CDC is no longer providing comprehensive vaccination numbers on its COVID-19 dashboards. But we still have some information about this year’s vaccination campaign, thanks to continued CDC efforts as well as reporting by other health agencies and research organizations.
This week, the FDA authorized Novavax’s updated COVID-19 vaccine. Here’s why some people are excited to get Novavax’s vaccine this fall, as opposed to Pfizer’s or Moderna’s.
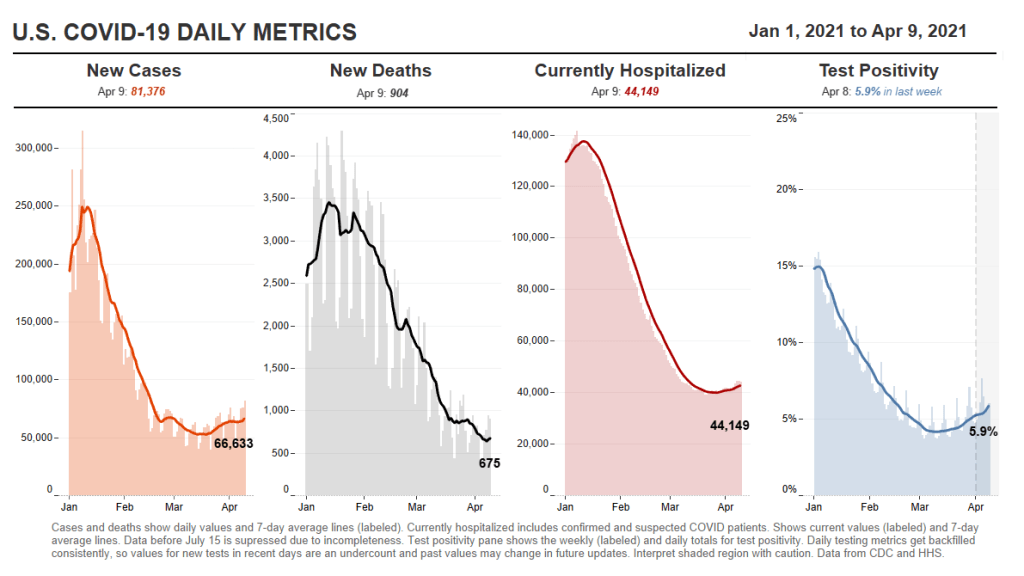
38,500 new COVID-19 patients admitted to hospitals (11.7 for every 100,000 people)
5,000 new COVID-19 deaths (1.5 for every 100,000 people)
44.1% of new cases in the country now B.1.1.7-caused (as of March 27)
An average of 3.2 million vaccinations per day (per Bloomberg)
I am really worried about Michigan. The state comprises a full 11% of new U.S. cases in the past week—and Michigan only makes up 3% of the national population. On any COVID-19 chart right now, Michigan sticks out like a sore thumb. Over 500 new cases per 100,000 people in a week, 4,200 new COVID-19 patients in a week, 15% positivity rate… none of the signs are good.
B.1.1.7 seems to have truly taken hold in Michigan. Combine that with a resistance to safety restrictions, and the state may serve as a warning of what other parts of the country may experience soon if we don’t keep up the pace on vaccinations. For more reporting on the state, I recommend Jonathan Cohn’s recent story in HuffPost.
B.1.1.7 has taken hold elsewhere, too. The variant is now causing at least 44% of the new cases in the country, as of the CDC’s most recent data (March 27). As that figure is now over two weeks old, the true prevalence is most likely much higher. Meanwhile, the NYC variant (B.1.526) and California variants (B.1.427/B.1.427) are each accounting for 10% of cases nationally, troubling figures on their own.
On the optimistic front, though, the daily average for vaccinations is now up at 3.2 million. The last few states that haven’t yet opened up eligibility to their entire adult populations will do so tomorrow, meeting President Biden’s deadline. We’ve also reached 200 million doses administered, ahead of Biden’s (revised) goal for his first 100 days in office.
Will these vaccinations be enough to break the tide of variant cases? I hope so. The vaccines at least appear to be protecting our most vulnerable neighbors so far, though; the death rate has remained below 1,000 per day despite several weeks of rising cases and hospitalizations.
37,400 new COVID-19 patients admitted to hospitals (11.4 for every 100,000 people)
5,000 new COVID-19 deaths (1.5 for every 100,000 people)
An average of 3.1 million vaccinations per day (per Bloomberg)
This is the fourth week in a row of case increases in the U.S. While this week’s jump is lower (we went from 57,000 new daily cases two weeks ago, to 63,000 last week, to 64,000 this week), the level where we’ve landed is still reason for concern. Our case numbers now are comparable to last July, when the summer surge was threatening hospital systems in the South and West.
Five states now account for almost half of our new cases, Dr. Katelyn Jetelina notes in her newsletter Your Local Epidemiologist. Those states are Michigan, New York, New Jersey, Florida, and Pennsylvania. “These states also happen to have some of the highest B.1.1.7 levels reported by the CDC,” Jetelina writes. “Is this a coincidence? Probably not.”
CDC data on coronavirus variants are reported with a significant time lag, as I discussed in detail last week. Still, the most recent update of the agency’s Variant Proportions page (now reflecting data as of March 13) tells us that B.1.1.7 accounts for at least 39% of cases in Michigan, 35% of cases in Tennessee, and 35% of cases in Florida. B.1.1.7 accounts for at least 20% of cases in five other states; it is now the most common variant in the country, CDC Director Dr. Rochelle Walensky said in a press briefing last week.
Vaccinations are of course continuing—more than one in three Americans has now had a shot, and one in five is fully vaccinated—but we can’t get complacent. This week’s seven-day average is barely above last week’s (both about 3 million), and as more states open up their eligibility to all adults, we’re seeing access issues and vaccine hesitancy prevent all shots from getting used.
Also, as Dr. Eric Topol pointed out on Twitter, the federal government is refusing to send surplus vaccine supply to Michigan despite pleas from Michigan leaders and public health experts to support this hotspot state in its time of crisis.