This past Monday, President Biden gave a speech about the Omicron variant. He told America that Omicron is “cause for concern, not a cause for panic,” and thanked the South African scientists who alerted the world to this variant. (Though a travel ban is not a great way to thank those scientists!)
Towards the end of the speech, he said: “We’re throwing everything we can at this virus, tracking it from every angle.” Which I, personally, found laughable. As I’ve pointed out in a previous post about booster shots, the U.S.’s anti-COVID strategy basically revolves around vaccines, and has for most of 2021.
wild to hear Biden say "we are throwing everything we can at this virus" … like, sir, no we aren't. we are throwing ONE THING (vaccines) at this virus.
My Tweet about Biden’s vaccine-only strategy got more attention than I’m used to receiving on the platform, so I thought it was a worthwhile topic to expand upon in the COVID-19 Data Dispatch. Why aren’t vaccines enough to address Omicron—or our current surge, for that matter—and what else could the Biden administration be doing to slow the coronavirus’ spread?
Why aren’t vaccines enough?
Prior to Delta’s spread, there was some talk of reaching herd immunity: perhaps if 70% or 80% of Americans got fully vaccinated, it would be sufficient to tamp down on the coronavirus. But Delta’s increased capacity to spread quickly, combined with the vaccines’ decreased capacity to protect against infection and transmission, have shown that vaccines are not enough to eradicate the virus.
Here, then, is the current pandemic dilemma: Vaccines remain the best way for individuals to protect themselves, but societies cannot treat vaccines as their only defense. And for now, unvaccinated pockets are still large enough to sustain Delta surges, which can overwhelm hospitals, shut down schools, and create more chances for even worse variants to emerge. To prevent those outcomes, “we need to take advantage of every single tool we have at our disposal,” [Shweta Bansal of Georgetown University] said. These should include better ventilation to reduce the spread of the virus, rapid tests to catch early infections, and forms of social support such as paid sick leave, eviction moratoriums, and free isolation sites that allow infected people to stay away from others.
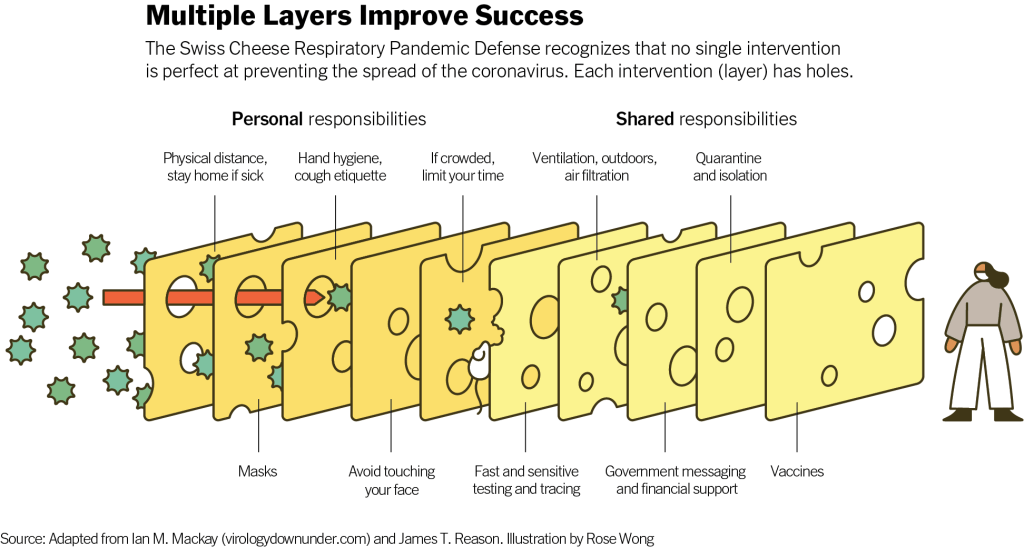
Remember that Swiss cheese model of pandemic interventions? Vaccines may be the best protection we have against the coronavirus, but they’re still just one layer of protection. All the other layers—masks, testing, ventilation, etc.—are still necessary, too. Especially when we’re dealing with a new variant that might not respond as well to our vaccines.
Re-upping this brilliant image from last year as a reminder on how mitigation measures work together to prevent the spread of coronavirus. pic.twitter.com/p7Z8u7fS2w
One strategy that we could employ against Omicron, as well as against the current Delta surge, is better masks. While cloth masks certainly make it less likely for the coronavirus to spread from one person to another, their efficacy varies greatly depending on the type of material, the number of layers, and the mask’s fit.
N95 masks do the best job at stopping the coronavirus from spreading, followed by KN95 masks. Surgical masks do a better job than cloth masks, but making sure these masks fit properly can be a challenge for some people (including yours truly, who has a very narrow face!). Layering a surgical mask and cloth mask may be a safer option to get both good fit and protection, though two layers of mask can be challenging to wear for long periods of time.
Some experts have recommended that the U.S. mail N95 or KN95 masks to all Americans, or at least require these masks in high-risk areas, such as on flights. Germany and other European countries established similar requirements last summer.
Given how transmissible Delta is—and the likelihood that Omicron is also highly transmissible—consider upgrading to an N95/KN95 mask or equivalent when indoors and around others, especially if you're elderly or immunocompromised.
In many countries—including the U.K., Germany, India, and others—rapid tests are freely available. Here in the U.S., on the other hand, the tests are quite expensive (often upwards of $10 for one test) and difficult to find, with pharmacies often limiting the number of packages that people can buy at once.
Biden has attempted to increase rapid testing access as part of his latest COVID-19 plan: in January, private insurance companies will be required to cover the cost of rapid tests. But this doesn’t solve the supply issue, and it doesn’t really make the tests more accessible, either. The measure would still require people to buy tests out of pocket, then fill out insurance reimbursement forms to maybe get their money back. Can you imagine anyone actually doing this?
In addition, as some experts have pointed out, the people most likely to need rapid tests—essential workers and others in high-risk environments—are also those less likely to have insurance. Biden is also distributing some rapid tests to community health centers, but that’s not enough to meet the need here.
This part of Biden’s omicron plan is also short-sighted.
Sure reimbursement by private health insurance of rapid test costs is a nice thing to have, but the people who MOST need rapid tests are the same people who DONT have private health care. What’s the plan for helping them? pic.twitter.com/tnlC8T0PDk
Ideally, the Biden administration would mail every American a pack of, like, 20 rapid tests, along with that pack of N95 or KN95 masks I mentioned above. Free of charge.
And at the same time, of course, we need more readily available PCR testing. Even in New York City, which has a better testing infrastructure than most other parts of the country, the lines at free testing sites are getting long again as cases go up. Any American who wants to get tested should be able to easily make an appointment within a day or two, and get their results within another day after that.
Increased testing is not only important for identifying Omicron cases (and cases of any other new variant); it’s also key for the Merck and Pfizer antiviral treatments due to be approved in the U.S. soon. Without efficient testing, patients won’t be able to start these treatments within days of their symptoms starting.
What we could do: improve genetic surveillance
The U.S. is doing a lot more coronavirus sequencing than we were in early 2021: we’ve gone from under 5,000 cases sequenced a week to over 80,000. The CDC worked with state and local health agencies, as well as research organizations and private companies, to increase sequencing capacity across the country.
Urban centers close to large academic centers tend to be well covered, while rural areas are less so. That means public health departments in large parts of the country are still flying blind, even as they are figuring out ways to prioritize Omicron-suspicious samples.
A lack of testing compounds this problem. If someone doesn’t confirm their COVID-19 case with a PCR test, their genetic information will never make it to a testing lab, much less a sequencing lab. While rapid tests are very useful for quickly finding out if you’re infected with the coronavirus, you need a PCR test for your information to actually be entered into the public health system.
In addition, even where the U.S. is sequencing a lot of samples, the process can take weeks. Vox’s Umair Irfan writes:
Still, it takes the US a median time of 28 days to sequence these genomes and upload the results to international databases. Contrast that with the United Kingdom, which sequences 112 genomes per 1,000 cases, taking a median of 10 days to deposit their results. A delay of only a few days in detection can give variants time to silently spread within communities and across borders.
Despite sequencing shortfalls in the U.S., we’re still doing much more surveillance than the majority of countries. Many nations in Africa, Asia, South America, and other parts of the world are sequencing fewer than 10 cases per 1,000, Irfan reports. As the U.S. should be doing more to get the world vaccinated, the U.S. should also do more to help other countries increase their sequencing capacity—monitoring for the variants that will inevitably follow Omicron.
What we could do: stricter domestic travel requirements
Starting on Monday, all international travelers coming into the U.S. by air will need to show a negative COVID-19 test, taken no more than one day before their flight. This includes all travelers regardless of nationality or vaccination status. At the same time, any non-U.S. citizens traveling into the country must provide proof of their vaccination against COVID-19.
But travelers flying domestically don’t face any such requirements. There are mask mandates on airplanes, true, but people can wear cloth masks, often pulled down below their noses, and airports tend to have limited enforcement of any mask rules.
Both experts and polls have supported requiring vaccination for domestic air travel, though the Biden administration seems very hesitant to put this requirement in place. Speaking for myself, I felt very unsafe the last time I flew domestically. A vaccine mandate for air travel would make me much more likely to fly again.
What we could do: more social support
In the U.S., a positive COVID-19 test usually means that you’re in isolation for 10 to 14 days, along with everyone else in your household. This can pull kids out of school, and pull income from families. As has been the case throughout the pandemic, support is needed for people who test positive, whether that’s a safe place to isolate for two weeks, grocery delivery, or rapid tests for the rest of the household.
This type of support could make people actually want to get tested when they have symptoms or an exposure risk, rather than avoiding the public health system entirely.
School Learning Modalities (HHS): Is that… could it be… comprehensive K-12 school COVID-19 data from the federal government?! Indeed: after over a year of calling out the government’s lack of data on this crucial topic, I was delighted to see the Department of Health and Human Services add a new dashboard to its COVID-19 data hub this week. The dashboard, produced in a collaboration between the CDC and the Department of Education, provides weekly updates on the learning status of school districts: in-person, hybrid, or remote. As of November 6, the dashboard included data for about 89% of students in 62% of districts. Next up, can we get some school case data?
When To Test (NIH): Earlier this year, the National Institutes of Health (NIH) supported production of an online tool aimed at helping schools, businesses, and other organizations develop routine COVID-19 testing programs. The tool, called When To Test, was updated this week with a new calculator aimed at individuals. Input some COVID-19 information (such as your location, vaccination status, and daily contacts), and the tool will help you determine whether to get tested. It could be useful for planning holiday gatherings!
COVID-19 Diagnostics Commons (ASU): Here’s another testing source, from Arizona State University. ASU researchers built a database of over 2,500 COVID-19 testing technologies that are available or going through the regulatory approval process around the world. You can search through the tests by regulatory status, diagnostic target, accuracy levels, and more.
Directory of federal government prime contractors: All businesses that contract with the federal government have until January 4, 2022 to ensure that all of their employees are vaccinated against COVID-19. This directory, from the U.S. Small Business Association, provides a comprehensive list of those contractors. You can see business names, what they do for the government, and more. (h/t Al Tompkins’ Covering COVID-19 newsletter.)
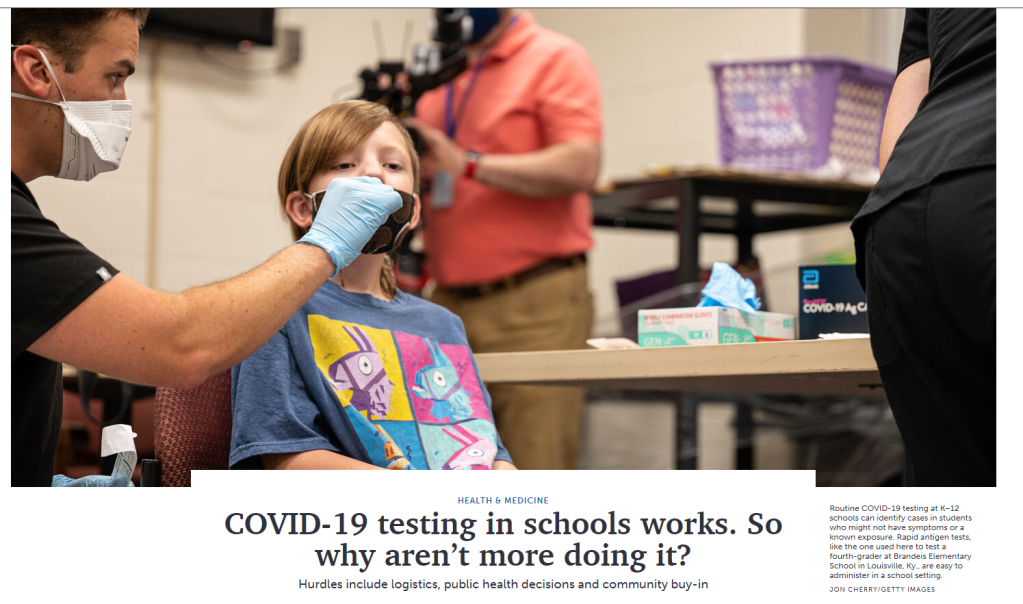
At this point in the pandemic, we know that routine COVID-19 testing can be a key tactic for reducing transmission in communal settings. If you identify cases as soon as they occur through asymptomatic testing, you can quickly isolate those cases and quarantine their contacts—preventing the cases from turning into outbreaks. This strategy works everywhere from kindergarten classrooms to the NBA.
Despite the clear evidence that testing works, high case numbers in children in recent months, and millions of dollars in federal funding, many K-12 schools across the U.S. still aren’t doing any COVID-19 testing. Why not? I explain the hurdles in a story for Science News.
I found five major challenges:
Without clear guidance from public health officials, school leaders may struggle to make crucial decisions about testing logistics (such as which tests to use, how often to test, and who will do the testing).
One logistical decision can be particularly tough: what happens when a student or staff member tests positive?
Obtaining COVID-19 tests themselves can be a struggle in this era of endless supply chain shortages, if schools are not getting tests directly from state health agencies.
Schools must gain consent from their students’ families for COVID-19 testing, which can be logistically complicated and require a lot of communication.
Testing, like all COVID-19 safety measures, has become polarized—and can come with both political and personal baggage for families.
You can read the full story for more details. But here, I wanted to share some notes from a section that was cut out of the article: one focusing on data. As longtime COVID-19 Data Dispatch readers know, I love to call out the lack of data on COVID-19 cases, tests, and other metrics in school settings.
Through reporting this article, I also learned that simply reporting testing numbers can be a major barrier for schools. In most cases, schools are required to submit all their test results to their state or local health departments; this type of health data reporting is not something that schools are cut out to do.
“Reporting test results to the appropriate public health authorities was something that school administrators, frankly, were not used to doing, and didn’t really know how to do,” Divya Vohra, an epidemiologist at the research organization Mathematica who studies testing programs, told me. Such reporting might require schools to set up an electronic records system like those used by hospitals, or it might require school nurses to manually enter data for every student.
Ideally, a school district would partner with “a vendor that comes in, reports the data for you to the state, and then also feeds that data into a dashboard” which school administrators can use in making decisions, said Leah Perkinson, testing program coordinator at the Rockefeller Foundation. But this type of partnership may be hard to come by, especially if schools are attempting to set up testing without support from their state health or education agencies.
As I’ve pointed out in the past, there is no national dataset of COVID-19 tests conducted in K-12 schools. New York is the only state reporting these data, along with some large districts such as Los Angeles Unified. Due to a lack of interest in K-12 testing prior to this fall, Perkinson says, “it wasn’t apparent that we need to build a centralized data reporting repository.” Now, many schools that might consider setting up a testing program are flying blind, without clear success stories to follow.
In addition, when the schools with testing programs in place do not actively monitor their own test results, they may miss out on valuable information, Alyssa Bilinski, a biostatistician at Brown’s School of Public Health, told me. Many districts rely on community COVID-19 metrics, such as the case rate in a county.
But “schools can vary a lot from the overall average, because kids can be really different from adults,” Bilinski said. “It’s a much more precise indicator if we have data for a particular school community.” (For more reading on this topic, I recommend Bilinski’s recent opinion piece in STAT News!)
Two Abbott BinaxNOW antigen tests used by Betsy and her sister during their trip, demonstrating single-line negative results.
As I mentioned in last week’s newsletter, I went on vacation during the last week of August. I traveled to California to visit my younger sister, who was living there over the summer for an internship. We spent a couple of days in the Bay Area, then drove to Southern California, hit a few different destinations, and finally flew out of Los Angeles International Airport (LAX).
Both my sister and I are fully vaccinated, of course, but we still took a number of precautions to make our trip as safe as possible in light of the current COVID-19 surge. I wanted to share what we did in case it’s useful for others thinking about travel right now.
Key precautions included:
Limited exposure and tests before traveling: For ten days before my flight out to California, I avoided all unmasked indoor activities, including small gatherings with fully vaccinated friends. Closer to my flight, I also avoided other activities outside my home (grocery shopping, taking the subway, and the like). I got a PCR test at a NYC Health site two days before my flight, and didn’t leave my apartment between that test and heading out to the airport.
Rapid testing every two days during the trip: I carried three packs’ worth of Abbott BinaxNOW rapid antigen tests in my suitcase, and bought a couple more packs in California. Starting two days after I arrived, my sister and I tested ourselves every other day. While antigen tests like these are more likely to give you a false negative than PCR tests, testing frequently increases your chances of catching a case—and catching it early in your disease progression, when you’re most likely to infect others. The tests were easy to incorporate into our routines, especially once we got used to the swabbing process.
Sticking to outdoor activities: Our trip included a lot of outside time: hiking in a redwood forest, hitting up Southern California beaches, camping for a night at Joshua Tree National Park, and lots of outdoor dining. The riskiest two activities of the week, we agreed, were an afternoon at Monterey Bay Aquarium and a day at Universal Studios in LA. But both of those establishments did a great job of reminding all patrons (including the vaccinated) to keep their masks on inside—following current mask regulations in the Bay Area and LA County.
Double-masking indoors: On both my flights and whenever I needed to be inside for a longer period of time, I wore two masks: a surgical mask and a fitted, multi-layer cloth mask. Studies suggest that cloth masks on their own are not the best option for protecting against Delta, but layering a cloth and surgical mask can increase protection. I especially like to layer masks because surgical masks typically don’t fit well on my face; when I add a cloth mask on top, the fit becomes much more snug.
Precautions when visiting relatives: My sister and I visited a few relatives over the course of our trip. For these visits, we basically followed the precautions that health experts recommended last Thanksgiving: eat outside whenever possible, mask up in common areas inside, open windows for extra ventilation, etc. We also organized the trip so that no visits occurred after Universal Studios, which we had deemed the riskiest activity of the week.
Extra testing after traveling: Flying out of LAX proved to be incredibly stressful, as neither the airport nor our airline put in effort to enforce mask guidance. My sister and I even gave extra masks to two fellow travelers at the check-in desk, because the airline apparently did not have any extras available. Because of this extra COVID-19 exposure risk, I did some extra testing upon my return to the East coast: daily rapid tests for two days in a row, followed by a PCR test.
hi @JetBlue! your mask availability and enforcement is apparently so bad that my sister and I had to literally GIVE TWO OF OUR OWN EXTRA MASKS to fellow travelers at the (very crowded) LAX check-in desk. this is extremely irresponsible in the face of the current covid surge.
Personally, this will probably be my last major trip for a while. Conferences that I’d planned to attend in the fall have been moved to all-virtual formats, and I’m lucky to live close enough to my parents that I don’t need a flight to see them for the holidays. If I were to travel again, though, I’d likely follow these same precautions—with adjustments based on COVID-19 infection rates at my destination. Also, I would probably avoid LAX.
Earlier this week, New York City mayor Bill de Blasio made a big announcement: all the city’s schoolchildren are going back to the classroom this fall. There will no longer be a remote option.
NYC was one of the first big cities to open with a hybrid model last fall, but it came with challenges—ranging from teachers protesting unsafe conditions, to in-person students doing “Zoom school” in the library, to closures dictated by confusing test positivity rates. The city’s choice to eliminate a remote option indicates a commitment to simple, unified policies for all students and teachers. It also suggests that many other districts may follow NYC’s lead—as the New York Times reported, a few districts already have.
Vaccine options for children ages 12 and older (now Pfizer, soon Moderna) make in-person education a safe bet for a lot of families. But younger students will likely have to wait much longer for their shots. As a result, regular testing will continue to be a key safety strategy, aided by American Rescue Plan funding dedicated specifically to school surveillance programs. Beyond identifying COVID-19 cases before they turn into outbreaks, testing can help parents and teachers feel safer about reopening plans.
But, as we have covered extensively here at the COVID-19 Data Dispatch, school testing data are incredibly hard to come by. New York continues to be the only state that reports any data on COVID-19 tests conducted in schools, and some states fail to even report COVID-19 school case counts.
Since Biden took office, more schools have returned to hybrid and in-person classes, but it remains unclear what percentage of school districts across the country are regularly screening students and teachers for Covid-19. An Education Department spokesperson said the department is “not tracking that level of detail.” A Centers for Disease Control and Prevention spokesperson said that “most states have offered or implemented testing programs in schools during the 2020-2021 school year,” adding that a survey conducted by the publication EdWeek in February found that just 16 percent of school district leaders said they were testing students.
Education and health groups — including the Association of State and Territorial Health Officials, the Rockefeller Foundation and American Federation of Teachers — also said they do not have comprehensive nationwide data on how many districts have testing programs in place.
This continued lack of data makes it difficult to evaluate how well school testing programs actually work. A lot of schools may be flying blind going into the fall 2021 semester, or they may choose not to set up regular testing at all.
I plan to do more reporting on this topic over the summer, including detailed investigations of individual school districts. If you have any burning questions, send them my way (betsy@coviddatadispatch.com).
On November 18, New York City mayor Bill de Blasio announced that the city’s schools would close until further notice. The NYC schools discrepancy is indicative of an American education system that is still not collecting adequate data on how COVID-19 is impacting classrooms—much less using these data in a consistent manner.
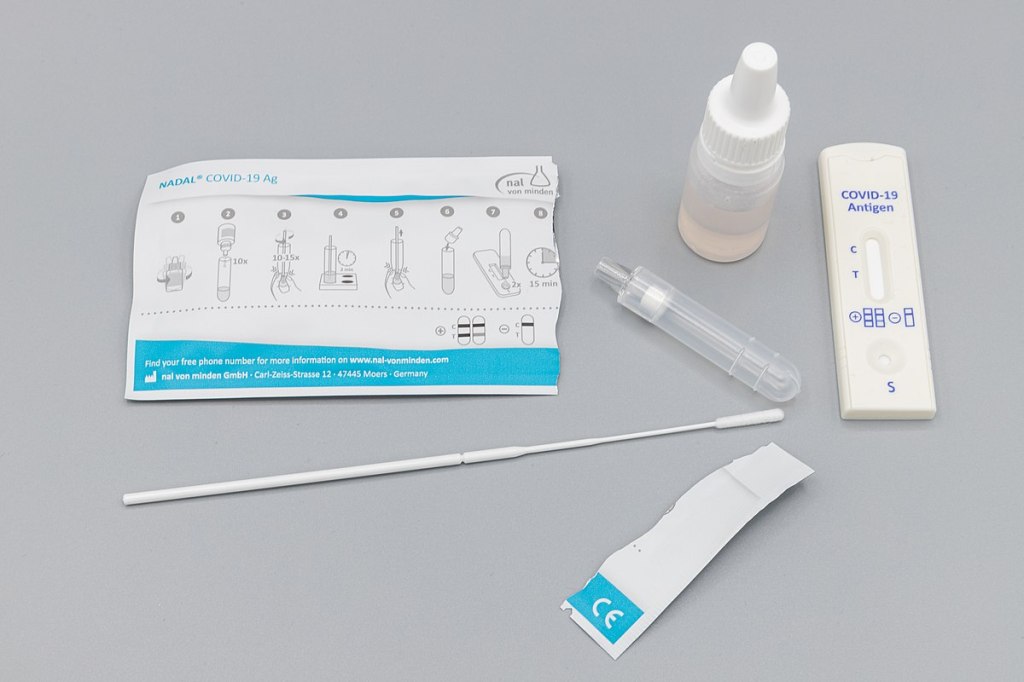
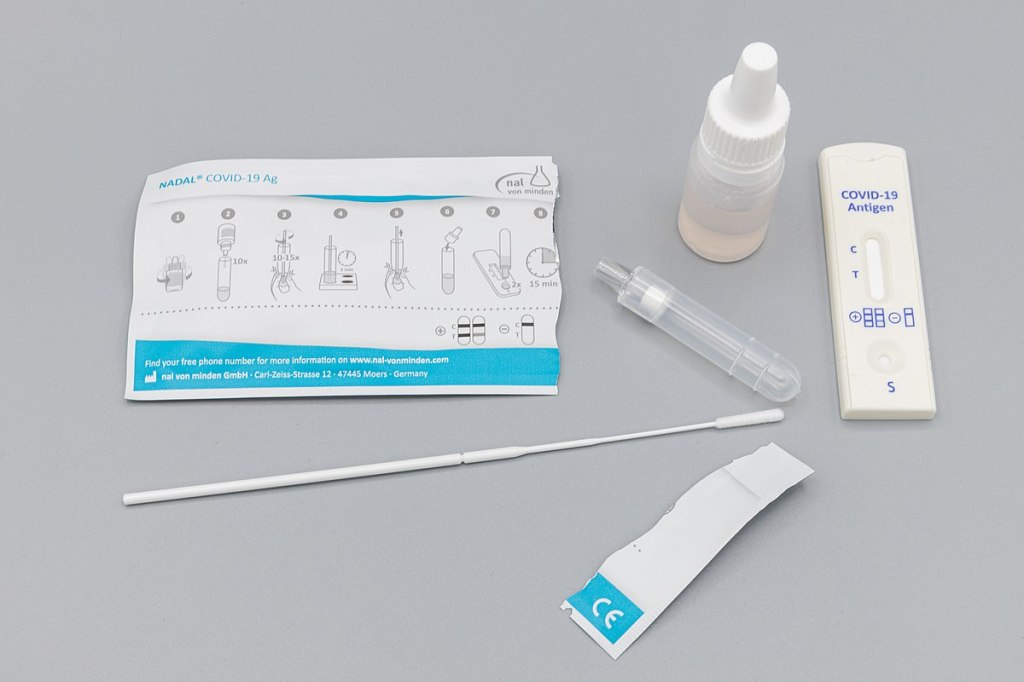
Antigen test kit image via Dronepicr // Wikimedia Commons.
This week, I had a story on COVID-19 testing published in Slate’s Future Tense vertical. The piece explores how testing will change in the next few months as more Americans become vaccinated and rapid tests become more widely available, with a practical focus: how should you interpret the test numbers on your local COVID-19 dashboard?
Overall, I found, we will need to keep getting tested even post-vaccination. But the purpose of testing may shift, for many of us in the U.S., from diagnostic testing—a test to figure out if you are currently sick with COVID-19—to more screening and surveillance testing—tests to identify case trends and stomp out outbreaks in a broader community. This shift may be aided by the rise of rapid, at-home tests, which are becoming much more widely available thanks to investment from the federal government. Just this week, USA Today reported that at-home tests will soon be sold at national pharmacies CVS, Walgreens, and Walmart.
In the CDD today, I’m excited to share one of the interviews I conducted for the piece, with Dan Larremore, a statistician at the University of Colorado and long-time advocate for the potential of rapid tests. We talked on April 2, just days after two major developments in the testing space: the FDA gave Emergency Use Authorization to several rapid tests for over-the-counter use, and the CDC and NIH announced a massive study to investigate how well these tests work for population-level screening. (One more piece of context: when we talked, case numbers were rising at a more concerning rate than they are now.)
Larremore and I talked about his reaction to the rapid test news, how to interpret testing numbers, other new test types that may come on the market, and more.
The interview below has been lightly edited and condensed for clarity.
Betsy Ladyzhets: First question is, since a lot of this piece is meant to be about the numbers of testing, what would you consider the most useful metric or metrics right now to how successful testing is, whether that’s test positivity or other things?
Dan Larremore: I think about testing for three different reasons. One reason is information about the trajectory of the pandemic, which is things like test positivity rates, number of new cases. We test to kind-of get our bearings in the movement of the pandemic. The second reason that we test is more at the individual level, but it’s still that [same] information. And that is, I would test because I want to know, am I sick? Might I give the disease to somebody else? Or, can my current symptoms be explained by being infected? So the first two are informational.
The third reason that we might test is specifically just to break transmission chains, which is more like testing as an answer, not as a question. And so, for at-home testing, for serial testing, for the regular kind of testing that we have to do to be on campus here [at the University of Colorado]… To me, that’s much more about an intervention to slow down transmission than it is about gaining information.
So, that’s a roundabout way of answering your question. But I think, in terms of what numbers to look at, it really matters what the intention of the testing is. So if people continue to take the pandemic seriously, and continue to, like, get tested regularly, or get tested when they feel sick, then those sort of daily case numbers will remain useful and interesting. And therefore the test positivity rate information will continue to tell us something about the trajectory of the pandemic. Does that answer your question?
BL: Yeah, I think that does answer my question. Because I think that was one of the big kind of questions I had going into this story is like, is test positivity still useful if maybe, as people get vaccinated, they stopped thinking they need to get tested or as other dynamics change. But yeah, I had another person who I’ve interviewed for this story also had kind of a hierarchy description [of testing], so that definitely is a useful thing to think about.
DL: Knowing why people come in to get tested just gives you so much more interpretability of like, what the numbers mean. Here on campus, if I want to be here on campus, I need to get tested weekly. I’ve been vaccinated, one dose, dose number two soon. But nevertheless, I still need to spit in the tube every week, and they test it. So, the test positivity rates here on campus are minuscule. Because with high compliance, everybody gets tested, so the denominator in that positivity rate is huge. At a drive up site, or at a doctor’s office, where people are coming in because they feel sick, the test positivity rates are going to be a lot higher.
And I think, as people get more and more vaccinated—regardless of the case counts—as the pandemic feels like it’s winding down, I think people may be less likely to get tested. And so you can imagine test positivity rate being driven by, not just what the virus is doing, but a lot of the human behavior as well… I guess, the way that you can put it is, that you can see changes in the test positivity that are driven entirely by human behavior with respect to getting tested at all. And not so much about changes in the virus.
BL: That makes sense. And I think it’s also about access, right? Are people able to go and get tested if they feel sick? Or if you’re thinking about schools and workplaces, is their employer having everyone get tested once a week? Is that something we’re going to see more of now that we have—like, literally earlier this week, the FDA gave EUA to a bunch of antigen tests, right?
DL: Yeah, for at-home use.
BL: Right. Do you think we’re gonna finally see that massive use of rapid tests that experts have wanted to see since, like, the summer?
DL: A lot of people, myself included, have been excited about the possibility of at-home repeated antigen testing, as a way to really take community transmission levels and push them down. Because we know that asymptomatic transmission occurs, we know that getting people results rapidly is absolutely critical. Because four-day-old information is totally useless if you have infected people in those four days.
I don’t know how useful those test kits are going to be right away, like, right now, given that we just now have an EUA for that kind of at home use that we’ve been hoping for for a long time. But at the same time, cases are shooting up due to these new variants around the U.S. and more importantly, around the world. So, I think these tools are still going to be useful, especially this fall, as we get a lot more kids in school. And we start bringing people together, temperatures starting to cool off, more people are indoors. I think that having the rapid test as a screening tool will still be valuable, particularly if we see limited uptake of the vaccine.
BL: That makes sense… Another question around rapid tests is, that I know in the U.S., it’s really hard to get comprehensive data on them. I volunteered at the COVID Tracking Project, and I wrote [a blog post] about the problem of antigen test data. So I was curious as to how we will know how well the tests are working. And if there are any specific studies that you’re watching or data sources that you recommend, in terms of, like, knowing if people are actually using these at home tests.
DL: I am excited about… On the 30th, there was a press release about the NIH and CDC rolling out at-home testing to two cities.
BL: I saw that, yeah!
DL: The work that Michael Mina and I did last year was showing that, at the individual level, the trade off between test sensitivity and turnaround time, should really tell us that turnaround time is critical. Like, theoretically, at the individual person level, the rapid test idea is really, really good. What we’ve not yet seen—outside of Slovakia—is the ability to flood the zone with tests, as Fauci put it, and just catch as many positives as possible and drive the epi curve downward, just because of the rapid tests.
My feeling is that, really, the proof is in the pudding. If people can, at a community level, use a boatload of rapid tests regularly for a few weeks, and we can watch the new cases spike as we find those positives and then crash as we break all the transmission chains. That’s the key thing. That’s the key thing that I’m looking out for in these new trials.
The Slovakia folks showed some of the limitations of this [strategy]. There’s a paper in Science where they wrote up their results. And basically what they found was the rapid testing worked really well, but the problem was on the isolation side. [Not everyone who tests positive can truly and effectively isolate.] In the short term, while they still had the supplies, these three waves of everybody in the country getting tested, worked like they were supposed to work, worked like the theory said. However, once you stop testing, you take your foot off the brakes, things re-accelerate. The second thing is that a lot of folks in particularly rural areas were like, okay, well, I’m positive, but I live with my family. How am I going to isolate? So unlike on a college campus here, where when somebody tests positive, we have a separate dorm set up for them for two weeks—in real life, that isolation stuff is going to be harder.
BL: So it’s kind-of like, you need to pair it with the social services aspect, or some other way to help people out. I know, in New York, there’s a hotel room program, where if you test positive, you can contact the City Department of Health, and they’ll like, put you up in a hotel for two weeks. I don’t know how much it gets used, but it definitely seems like something that should be around in more places.
DL: I mean, even if it’s just supporting people, by telling them like, this is gonna be awkward, but wear your mask at home, and don’t hang out with your family. Go watch TV in the basement, or, you know, otherwise keep distance from people. Whatever these interventions are, they can help. And we know that what we call the secondary attack rate is actually not that high. So, even among people who live in the same household, even among spouses, if one person is sick, that doesn’t mean that the other person definitely gets it. It’s only [around 20%] chance that they do. We looked at pairs of roommates here on campus, and studied [transmission between] them. And even among roommates, the secondary attack rate is not that high [20-28%].
BL: Well, that brings me to another question I wanted to ask you, which is how public health communication around testing either is changing or should be changing in order to express like, okay, maybe you’ve been vaccinated, but you still need to get tested, or what needs to be communicated about these at home tests, or any other messages that you think are important to be conveying.
DL: One thing that’s important is that we know that we need to keep our eye on the variants. And evidence is emerging… that there are some breakthrough variants, they are less well handled by the vaccine, even though the vaccine works really well… So, testing is going to remain important, even as, more broadly, the vaccine protects people from the most severe disease.
We’re seeing a really interesting split right now, right? Where like, cases are going up, and we expect hospitalizations to then go up, and then mortality to go up. But I wonder if we’re gonna see that in the U.S. this time. Like, week on week, mortality continues to go down. And the question is, are we gonna get it again?
BL: Is it gonna go up again?
DL: Or did we vaccinate enough of the high-risk people that the mortality stays flat even while cases go up?
BL: I definitely think there’s going to be kind-of a demographic aspect of it. Like,I’ve seen charts where people do, with the HHS hospitalization data, they publish it by age. So, you can see that hospitalizations are going way up in people ages, like, 18 to 30, but not so much in seniors. Although, kind-of tangentially, one data gap that I get annoyed by is that there’s very little demographic data for testing. Like, if you look at race data, for example, there are maybe five states that publish testing data by race and ethnicity. And there’s not a lot of it by age. So it’s kind-of hard to track patterns there.
DL: I mean, I don’t know what the right messaging is around testing, other than, [if you feel like you’re sick], if you have the symptoms, you’ve got to go get tested. It doesn’t matter if you’re vaccinated or not. If you feel sick, you should go get tested. If you are going to be around somebody who you know is really vulnerable, if testing is available, go get tested.
I still think it’s a valuable intervention, especially in places where vaccine uptake is low or vaccine availability is low. But I think the question is, like, really, how long is—what’s the expiration date on recommendations about testing? If 70% of the US is vaccinated by July, let’s say, does it still make sense to recommend a huge amount of testing? And I don’t know the answer to that. What I would like to see is people equipped for this fall, if there are spikes in cases, or if there are variants that are circulating even among vaccinated people, it would be amazing if, like, a local public health authority could tell everybody, this Sunday, I want everybody to use your rapid at-home test. Report your results anonymously to this number. And, if you test positive, take it seriously, take precautions. Measures like that could preserve privacy, while still collecting that key surveillance data and crashing the epidemic curve.
BL: Right, that would be really cool to see. Are there any other types of COVID tests or surveillance methods that you think might become more useful and more prevalent in the next few months or heading into the fall?
DL: Yeah, there are two kinds. So, one key point about at-home tests is that privacy-preserving aspect. Like, I trust local public health here. But I tend to vote left of center and generally trust the government. I live in Colorado, and not everybody feels that way. There’s definitely a strong libertarian independent streak. And I feel like one of the key advantages of at-home tests is that they appeal to that kind of person. They empower a person and their family to make health decisions, and they give you the information. But they don’t necessarily get recorded by something like COVID Tracking Project or HHS.
BL: Yeah.
DL: There’s less visibility for authorities, but for some folks who want information that they can act on to protect themselves and others, then that’s going to be fine. And so, as much as I would like to know exactly what is happening with the pandemic, if the trade-off for lower cases is that we don’t know about a lot of cases among folks who would rather not report their data, I think that’s a fair trade-off.
BL: Yeah, that makes sense.
DL: But it’s sort of like uncomfortable for me, who likes the data to say that. You know what I mean?
BL: It reminds me of the conversation around exposure notification apps. I talked to someone who works on those apps recently, and she kind-of said the same thing, that she would rather have everyone using the app than really good data from a tiny subset of the population that’s okay with their privacy being violated.
DL: A big thing to me is that, we know that the pandemic has been political. And I don’t see any reason why we can’t have solutions that work for the person who votes left of center, the person who votes in the middle, and the person who votes right of center.
But the other kind of tests that I’m excited about, only because they’re extremely cheap and really easy, are anosmia screens. We know that loss of sense of smell is highly specific to COVID. If you don’t have a stuffy nose, and you [suddenly] can’t smell things, you probably have COVID. So, there are companies that produce, like, a little card with a scratch-and-sniff quiz. You don’t know what’s behind the panel, but you scratch, pull up a smartphone app, and then say what you think the smell is from a multiple choice test.
One of the cool things is that anosmia only occurs in around 40% of people [with COVID] if you ask them to self-report. But if you give them one of these objective quizzes, the prevalence of anosmia as a symptom goes up to [around 75 or 80%], depending on which study you look at. The important thing is that those cards cost 25 cents apiece, and multiple people can use the same card. It’s literally a scratch-and-sniff with an online quiz.
BL: That’s incredible. Do you know if there are tests like that that are up for EUA?
DL: Yeah. Roy Parker, Michael Mina, and I collaborated with a great team to write this paper last year on typical COVID testing [PCR, LAMP, and antigen testing], test sensitivity and frequency and turnaround time. Then, Roy and I teamed up with Derek Toomre at Yale School of Medicine, and took the same idea and said, well, what if we use frequent, repeated anosmia screening tests?
One of the things that I like about those is that they’re cheap. But another thing that I like about them is that nobody thinks that [a smell test is] the same thing as a proper COVID test. You can’t get them confused. [This is important because one of the questions with rapid tests is how people may interpret a negative test—they might be infected, but the virus is at a low level. So if they get a negative rapid test and then go to the gym, the test could actually have an unintended effect. But if an anosmia test tells you that you still have your sense of smell… People understand that just because you still have your sense of smell doesn’t mean that you’re COVID-free. There’s lower risk of unintended consequences.]
Anyway, I think the messaging around those [anosmia] tests is easy. They’re easy to use, you can do them at home. And they can print them for, like, a quarter apiece. So the modeling suggests that they could be pretty effective and really cheap. You could literally mail somebody a stack of 10 of these things to everybody in the U.S.
BL: And do it once a week!
DL: Yeah, do it once a week. So, that’s another kind of test that I would like to see out there. The company that Derek started, that makes those [tests], just won one of the XPRIZEs for COVID testing. So, I think that’s cool. It’s a more creative kind of test, and it’s inexpensive.
BL: Sweet. So, that was all the questions that I had. Is there anything you think is important on this topic that I should know for this article?
DL: I just think it’s really important to keep a global perspective… As with vaccines, we know there are inequities within the U.S. But there are definitely global inequities. And while we might feel like we’re on a glide path to herd immunity through vaccination here in the States, things look very different in the rest of the world. And so, the use of these tests may become more important this fall, we may get more variants globally, even as the U.S. cases go down. I think it’s an ongoing story, even if hospitalizations and deaths continue to drop here in the States.
BL: And those tests you’re talking about that are cheaper and easier to use are useful in many places, not just here.
DL: Yeah, that’s the hope… I feel generally optimistic about [the state of the pandemic], but like, hesitant.
BL: I feel you. It’s definitely weird to see everyone getting very excited about the summer when I’m kind-of sitting here in my COVID reporting bubble, like, ahhh, not there yet.
DL: Well, one of the hardest parts, I think, for public health officials is going to be, if cases are going up, but mortality and hospitalizations are flat or going down. If COVID is only making people sick, but it’s not hospitalizing and killing them. Then, like, do we just reopen everything? Do we open up the schools? That’s tough when we’ve been acclimated to keep our foot on the brakes as much as possible.
In a press conference on Wednesday, NYC mayor Bill de Blasio confirmed that the recently identified NYC variant (since christened B-1526) is outpacing the original strain in spreading speed, and his senior advisor for Public Health, Dr. Jay Varma, said that these two variants combined account for 51% of all cases in the city. This is coming from a preliminary analysis, and so far, they have not found that B-1526 is more deadly or that it may evade vaccine efficacy. However, it’s still worrying.
It’s probably contributing to the relatively slower pace of decline in cases in NY versus the rest of the country:
Change in avg. daily covid cases over past 14 days:
* United States: -19%
* NY State (outside of NYC): -5%
* New York City: +1%
Something different is happening in NYC. Likely variants are a big factor. We need folks to remain cautious for just a little longer.
And this comes when NYC is increasing indoor dining capacity to 50%, and when NY is going to scrap its rule on people from out of state having to quarantine on April 1. De Blasio has told New Yorkers to stay the course, but the people in charge (Andrew Cuomo) don’t seem to want to follow that advice.
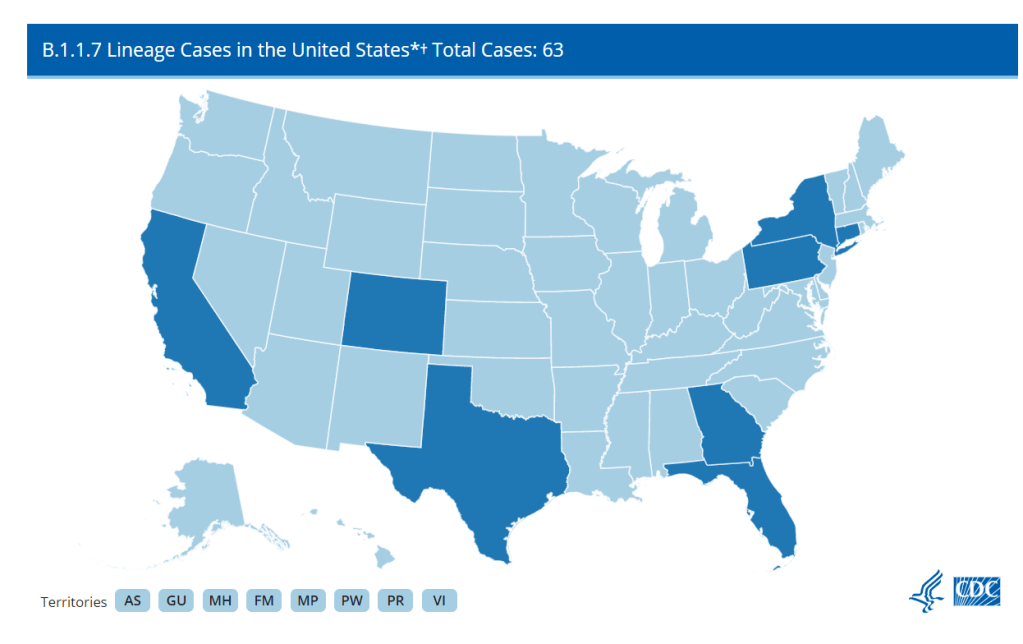
The CDC has identified 63 cases of the B.1.1.7 variant as of Jan. 8, but this is likely a significant undercount thanks to the nation’s lack of systematic sequencing.
A new, more transmissible strain of COVID-19 (known as B.1.1.7) has caused quite a stir these past few weeks. It surfaced in the United Kingdom and has been detected in eight states: California, Colorado, Connecticut, Florida, Georgia, New York, Texas, and Pennsylvania. The fact that a mutant strain happened isn’t a surprise, as RNA viruses mutate quite often. But as vaccines roll out, the spread of a new strain is yet another reminder that we’re nowhere near out of the woods yet.
It’s entirely possible to differentiate between strains of SARS-CoV-2 through genetic testing. To detect the B.1.1.7 variant, COVID-19 positive samples can be sequenced to search for a telltale deletion in the virus’s RNA. And in theory, we could track the spread of this variant with good testing data. A truly robust tracking effort should include a centralized surveillance program to sequence the RNA of the SARS-CoV-2 virus in all positive cases—or at least a good sample—to detect any mutant strains and track their impact. However, this is an area where the US has consistently faltered: as of December 23rd, only 51,212 out of 18 million positive cases had been sequenced.
As with most of the government’s response, handling this seems to be mostly up to the states. According to releases from Colorado, Pennsylvania, Connecticut, and Texas, it looks like these states are making sequencing efforts. Georgia said, “The variant was discovered during analysis of a specimen sent by a pharmacy in Georgia to a commercial lab”, which I can only assume means they have been conducting some kind of sequencing effort. I couldn’t find references to the extent of sequencing efforts in the announcements from California, Florida, or New York.
From these releases, it’s obvious that there is no unified cross-state effort. Pennsylvania stated that they had been sending “10-35 random samples biweekly to the CDC since November to study sequencing,” but that’s not going to be nearly enough to track this more transmissible variant. Are there any plans to ramp up sequencing? And that’s just from Pennsylvania because they deigned to tell us—are all states going to ramp up sequencing? It’s just not clear.
And after all that, starting to test for the variant now still won’t tell us just how widespread it is. The first case in New York was in someone with no evident travel history. Indeed, this is true for most people who have been infected, and, per Dr. Angela Rasmussen in Buzzfeed News, this suggests that the variant is already circulating in the community. To know how widespread the variant is, we would need to retroactively test samples that had already tested positive. Colorado’s press release mentioned that they would be doing some retroactive testing, but what about the other seven states?
Plus, that’s just states with already confirmed cases—there absolutely will be more confirmed cases in other states, because if it is already present in the community, there probably already are cases in other states. To know just where this variant is, every positive test in the US stretching back months into the past would have to be retroactively re-tested for the variant—an unlikely occurrence.
Even if there were a coordinated effort to retroactively sequence all positive tests, some cases of the variant could still slip through the cracks, because most states still aren’t doing enough PCR testing as it is. As of January 8th, according to Ashish Jha’s team at the Brown University School of Public Health, 86% of states aren’t meeting their testing targets. (Meeting testing targets indicates that enough testing is happening to “identify most people reporting symptoms and at least two of their close contacts.” State targets on this dashboard were last configured on October 1, so keep that in mind.) Only two states where the variant has surfaced, Connecticut and New York, are meeting their targets—and cases are surging in bothstates right now. Longtime readers are going to be very familiar with this problem, but if any new people are reading, this means that in most states we don’t even know how widespread our “garden variety” COVID-19 is. So how are we supposed to know where the UK variant is if we can’t even keep track of the virus that’s been here for almost a year?
Beyond testing, even reporting on confirmed cases of the variant is spotty at best. The CDC is reporting how many detected cases of COVID-19 have been caused by the variant, but no state with a confirmed case caused by B.1.1.7 is displaying that data on their dashboard. (I checked the 8 states’ dashboards and left a comment on California’s because the ask box was right there.) Why is this not on their dashboards? I couldn’t tell you, but it seems like important information that should be reported.
All of these unanswered questions show, yet again, that we desperately need a unified effort from the federal government to track and combat this virus. It should not be this hard to find how we’re tracking the spread of this variant, it should not be this hard to tell which methods work for even identifying the variant, and it should at least be possible to find this data on state health dashboards. It might look like we’re close to the finish line as vaccines continue to be distributed, but we’re tripping over the exact same problems we did at the beginning.
For months, public health advocates have called on the federal government to release in-depth data reports that are compiled internally by the White House Coronavirus Task Force.
The reports include counts of COVID-19 cases, deaths, and tests, as well as test positivity calculations. In addition to state-level data, the reports feature county-level data and even data for individual metropolitan areas, color-coded according to risk levels for each region. The reports have also drawn on these data to provide specific recommendations for each state. They have been a key piece of the federal government’s support for governors and other state leaders—but they haven’t been shared with the public.
Liz Essley Whyte and her colleagues at the Center for Public Integrity have obtained copies of many of these reports and made them publicly available. But the scattered PDFs—often posted for only a few states at a time—provided only small snapshots from the vast trove of data HHS was using behind the scenes.
This past Friday, the Department of Health and Human Services (HHS) began releasing all national COVID-19 reports and the data behind them. Now officially called “COVID-19 Community Profile Reports,” the reports are expected to be released as PDFs and spreadsheets every day.
I asked Liz Essley Whyte why this release—one that she’s spent months pushing for—is so important. Here’s what she said:
This release has local data that is so important for helping people make daily decisions about what’s safe. It also gives us the same picture of the pandemic that our federal government does, allowing us to weigh its response. It’s data that was assembled with taxpayer dollars and that affects everyone’s lives, so it was past time for it to be made public. I’m very glad it’s out there now. I think if it’s pursuing full transparency the White House should also make public the policy recommendations it gives to states weekly in the governors’ reports, alongside this helpful data.
Here’s my own tour, a.k.a. why I’m excited about this new dataset:
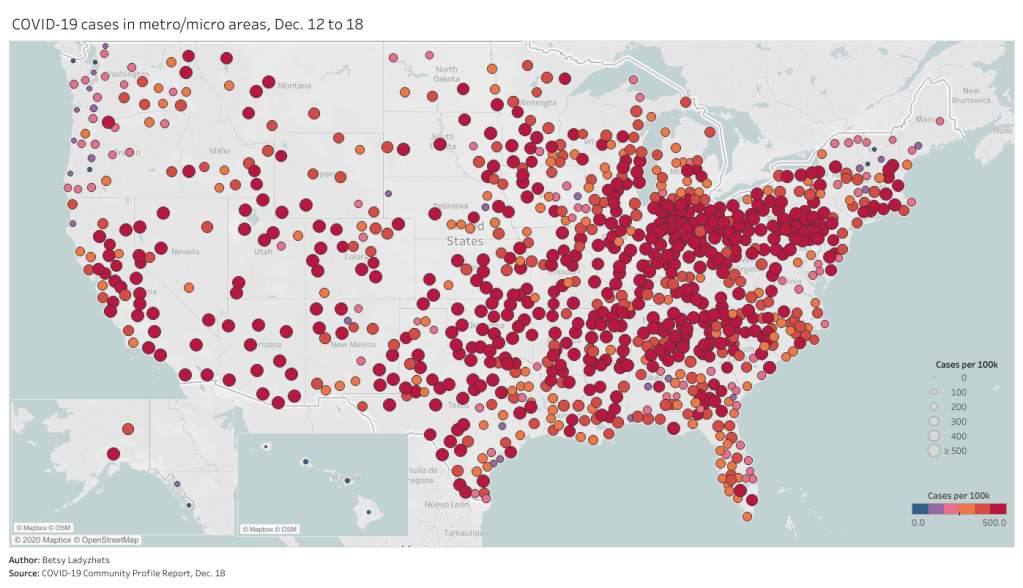
Data on metropolitan areas: Other sources were compiling state- and county-level data prior to Friday, but standardized data on how COVID-19 is impacting America’s cities were basically impossible to find. This new dataset includes information on over 900 metropolitan and micropolitan areas, making it much easier to compare outbreaks in urban centers.
Standardized data: One of the biggest challenges for COVID-19 data users has been a lack of consistency. Some states report every day of the week, some skip weekends. Some states report their tests using one unit, some report using another. Some states include antigen tests in their numbers, some don’t. And so on. But the HHS can smooth out these inconsistencies internally, as national testing laboratories and state public health departments are all required to report in the same way. What I’m saying is, this new report allows us to do something we haven’t been able to reliably do since the start of the pandemic: compare testing numbers across states.
Major metrics in one place: Before Friday, if I wanted case and death numbers by county, I’d go to the New York Times, while if I wanted testing numbers by county, I’d go to the Center for Medicare & Medicaid Services. The scattered nature of pandemic reporting has led researchers and journalists to cobble together stories from multiple disparate sources; now, we can get three major metrics in one easy place. (This data reporter loves to only have one Excel spreadsheet open at a time.)
Contextual data built in: Not only does this new dataset include several important metrics in one place, it also contextualizes those metrics with key demographic information. For each state, county, and metro area in the dataset, numbers such as the share of this region living without insurance and the share of the region over age 65 are included right next to that region’s COVID-19 metrics. Two indices that indicate the region’s demographic vulnerability to the virus are also included: the CDC’s Social Vulnerability Index and the Surgo Foundation’s COVID-19 Community Vulnerability Index. I covered both in my November 29 issue.
Rankings for policymakers: In addition to raw counts of cases, deaths, and tests, the Community Profile Reports include calculated values that make it easy for local leaders to see how their communities compare. The reports rank states according to their cases per 100,000 population, positivity rate (for PCR tests), hospital admissions, and other metrics. They highlight key cities that demand attention and aid, such as Phoenix, Arizona and Nashville, Tennessee. They even forecast death totals based on current case counts—a morbid metric, but a useful one nonetheless.
More transparency: Like the facility-level hospitalization dataset released last week, the Community Profile Reports signify that the HHS is finally stepping up to provide the American public with the information that informs key public health decisions. The absence of national data during this pandemic was never meant to be filled permanently by journalists or volunteer data-gatherers—the federal government is built for this work. Journalists are, instead, built to watch this work closely and hold it accountable.
HHS believes in the power of open data and transparency. By publicly posting the reports that our own response teams use and by having others outside of the federal response use the information, the data will only get better.
As of Saturday night, the dataset has already been downloaded nearly 6,000 times. That’s nearly 6,000 people who can use these data and make them better—and the number will only grow.
HHS funds new COVID-19 tests: On October 31, HHS and the Department of Defense announced a $12.7 million contract with InBios International, a Seattle-based diagnostic testing company. The contract aims to help InBios increase its production capacity for two COVID-19 tests: a rapid antigen test called the SCoV-2 Ag Detect Kit and an antibody test called the SCoV-2 Detect IgM/IgG Food & Drug Administration (FDA).
HHS distributes antigen tests to HBCUs: At the end of September, the Trump administration announced that Historically Black Colleges and Universities (HBCUs) would be one category of priority sites for the distribution of Abbott BinaxNOW antigen tests, of which the administration has purchased 150 million. This promise is now coming to fruition; HHS announced on October 31 that 389,000 BinaxNow tests have been distributed to 83 HBCUs in 24 states, at no cost to the schools. How these schools will use the tests and report their testing data, however, remains to be seen.
FDA reminds antigen test providers to use them properly: The FDA issued a letter to clinical laboratory staff and health care providers on November 3, reminding them that antigen tests may incur false positives when the instructions for these tests’ use are not correctly followed. FDA recommendations include using antigen tests for symptomatic individuals, handling tests correctly, and using PCR tests to confirm results in low incidence counties. As I’ve discussed in this newsletter before, incorrect use of antigen tests may lead to misleading results that waste clinical resources or instill false confidence in people who receive false negatives.
HHS needs better testing oversight and data: Two new articles in STAT News this past week have discussed COVID-19 test regulation and reporting. An investigation by Kathleen McLaughlin finds that laboratory developed tests, diagnostic tools developed by and for specific facilities, fall in a “regulatory gray area” which makes it easy for innacuracies to slip past the FDA and HHS. Meanwhile, an op-ed by OB-GYN Joia Crear-Perry points out the public health danger in allowing demographic data on testing to be lost when rapid tests are not incoporated into reporting pipelines.