An excellent article in the Financial Times, published this past Monday, illuminates one major challenge of estimating a vaccine campaign’s success: population data are not always reliable. Health reporter Oliver Barnes and data reporter John Burn-Murdoch explain that, in several countries and smaller regions, inaccurate counts of how many people live in the region have led to vaccination rate estimates that make the area’s vaccine campaign look more successful—or less successful—than it really is.
Why does this happen? It’s actually pretty challenging to get a precise count of how many people live somewhere. Think about the U.S. Census, for example: this program attempts to count every person living in the country, once every ten years. But it may miss people who don’t have a straightforward living situation (like college students, the incarcerated, and people living in shelters); it may have confusing messaging that discourages some people (like undocumented residents) from filling out the necessary form; and some people may simply choose not to give information to the government.
When the Census is inaccurate, the inaccuracies ripple out to different government analyses—including analyses of how many people have been vaccinated. Here’s a quote from the Financial Times article:
“The average person would be surprised that governments don’t know how many people are actually in the country,” said Stian Westlake, chief executive of the UK’s Royal Statistical Society. “But this great unknown can cause a whole host of data glitches, especially when responding to a health emergency.”
The Financial Times provides several examples of these data glitches leading to incorrect vaccination estimates.
In England: Overestimates of the unvaccinated population, based on data from the U.K.’s Health Security Agency, suggest that case rates are lower among unvaccinated Brits than they actually are.
In several EU countries: Underestimates of the senior population lead to vaccination rates inaccurately suggesting that over 100% of certain age groups in Ireland, Portugal, and other countries have received at least one dose of a vaccine.
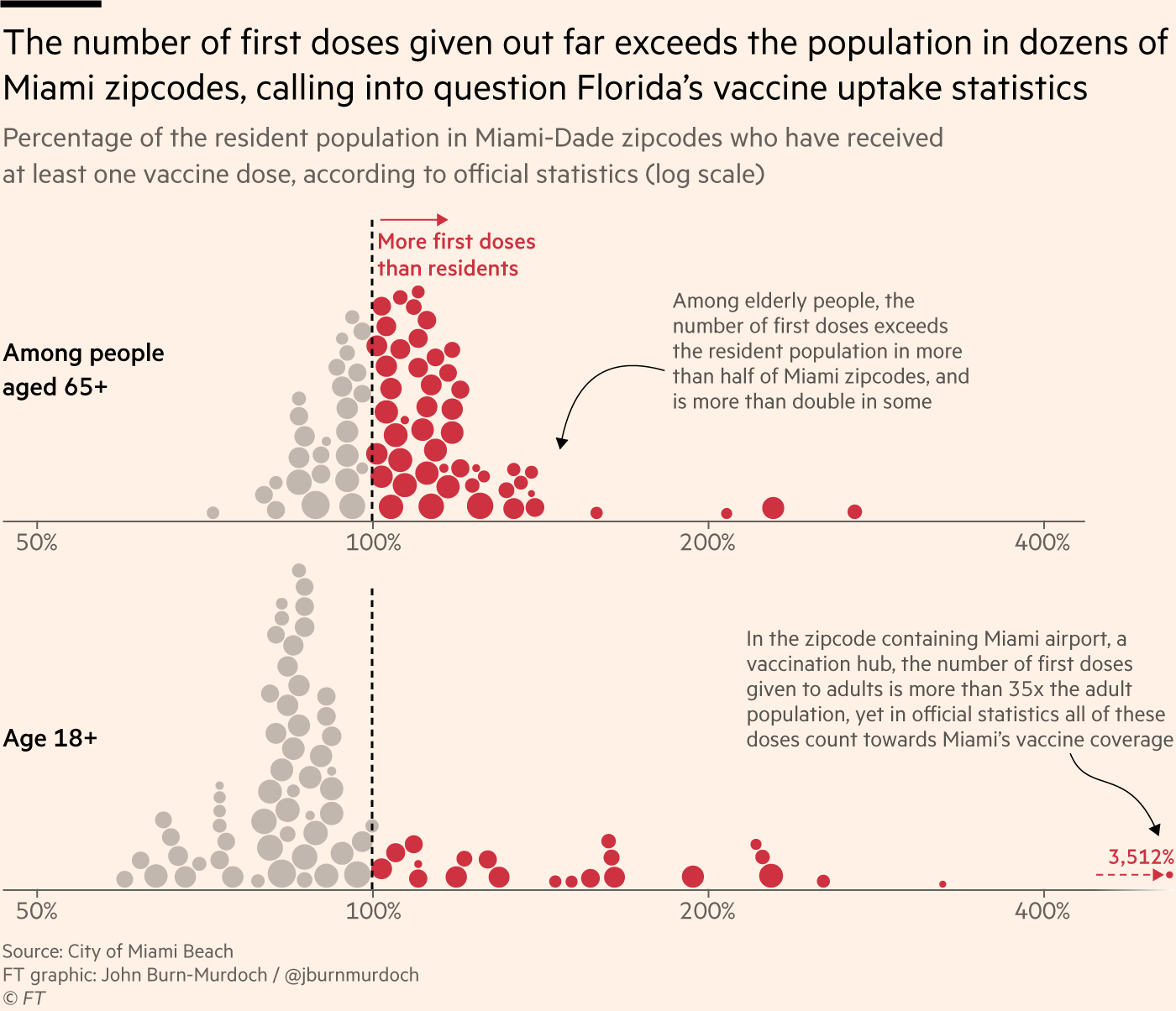
In Miami, Florida: A number of ZIP codes have senior vaccination rates that appear to be over 100% of seniors, due to retirees (who do not have permanent residence in Florida, and therefore aren’t counted in the state’s population) getting vaccinated in Miami during their winter vacations.
Incorrect vaccination rates can cause issues for public health agencies leading vaccine campaigns, the Financial Times reports. If you think you have vaccinated 100% of seniors in your county due to population underestimates, you likely aren’t looking out for the seniors who in fact remain unvaccinated—leaving those seniors still vulnerable to COVID-19.
At the same time, data glitches can provide fodder for anti-vax groups. “Worst of all, anti-vaxxers and Covid deniers feed on the daylight between reality and the incomplete data we currently have as evidence of a grand conspiracy or bureaucratic incompetence,” Jennifer Nuzzo, epidemiologist Jennifer Nuzzo told the Financial Times.
I recommend reading the Financial Times article in full. But you can also check out this Twitter thread from John Burn-Murdoch for more highlights:
NEW: people obsess over vaccine uptake stats, eagerly comparing one country to others to see which has jabbed the highest share of its population, but what if I told you many — perhaps most — of those stats are wrong?
Time for a thread on bad Covid data and how it can cost lives
This week, the World Health Organization (WHO) called for wealthy nations to stop giving out booster shots in a push towards global vaccine equity.
These nations should stall any booster shots until at least September, said WHO Director-General Tedros Adhanom Ghebreyesus at a press conference on Wednesday. Instead, excess vaccines should be donated to COVAX, the international vaccine distributor that aims to mitigate COVID-19 in low-income countries. When 10% of the population in every country has been vaccinated, then wealthy countries could resume administering boosters, Tedros said.
I understand the concern of all governments to protect their people from the Delta variant. But we cannot and we should not accept countries that have already used most of the global supply of vaccine using even more of it while the world’s most vulnerable people remain unprotected.
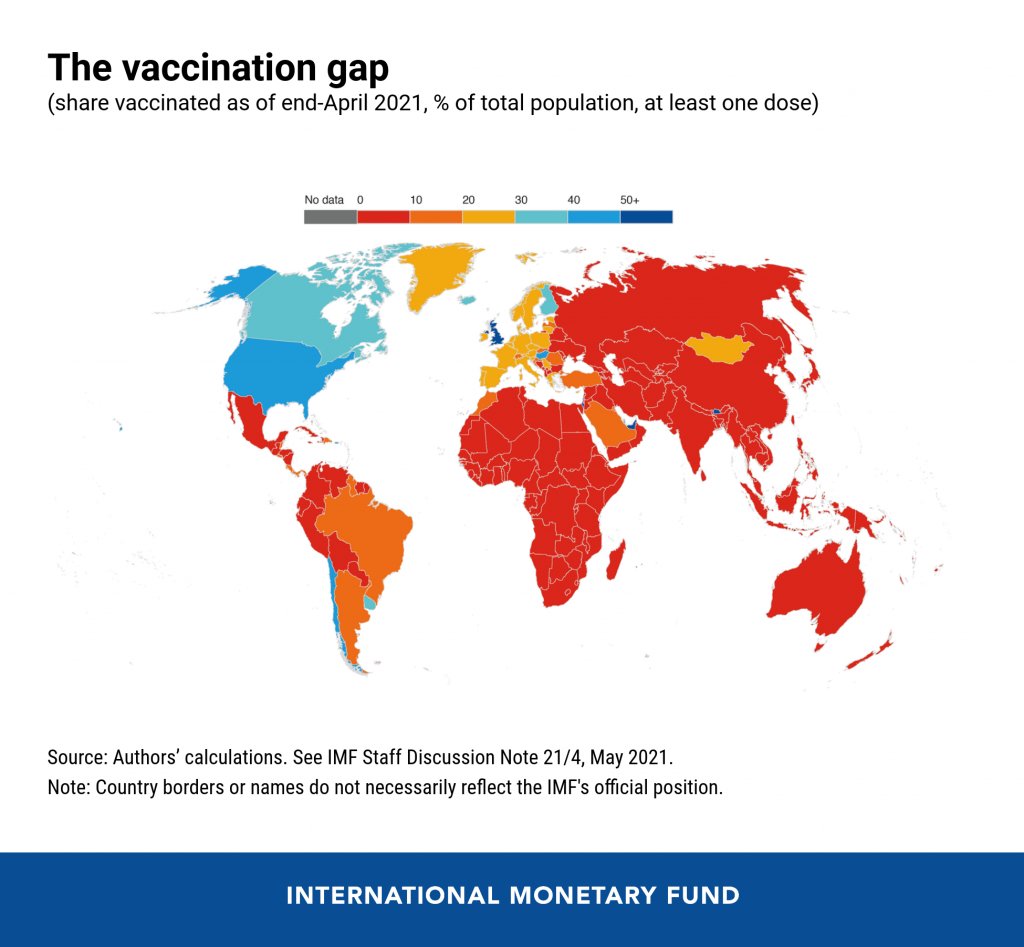
It may seem counterintuitive for a country to not provide its citizens with extra protection when it has the means to do so. But the global numbers are staggering. About 50% of the U.S. population has now been fully vaccinated, and we have doses to spare (some of which are going to waste). Meanwhile, in most African countries, 1% or less of the population is vaccinated. This is even though vaccine demand is actually far higher in low-income nations than in the U.S.
An internal analysis from the World Health Organization (WHO) estimates that if the 11 rich countries that are either rolling out boosters or considering it this year were to give the shots to everyone over 50 years old, they would use up roughly 440 million doses of the global supply. If all high-income and upper-middle-income nations were to do the same, the estimate doubles.
About 3.5 billion people in low- and lower-middle-income countries have yet to be vaccinated, Maxmen estimates. Give one dose to 10% of that number, and you use 350 million doses—less than the 440 million that rich nations would use up with boosters.
The longer that these low-income countries go without widespread vaccination, the more likely it is that new variants will emerge from their outbreaks. This is because, with every new COVID-19 case, the virus has a new opportunity to mutate. We’re already seeing Delta adapt to become even more transmissible and monitoring other potentially-concerning variants, like Lambda.
It’s unclear how much power the WHO has to enforce a booster shot moratorium, especially now that some countries (like Israel) have already gotten started on administering these extra shots. And it’s also worth noting that public health officials in the U.S. are shifting away from using “booster” to describe third shots for immunocompromised people or second shots who for those who received the one-and-done Johnson & Johnson vaccine; they say that these shots rather bring patients up to the same immunity levels as those who received two mRNA doses.
Following the end of the federal public health emergency in May, the CDC has lost its authority to collect vaccination data from all state and local health agencies that keep immunization records. As a result, the CDC is no longer providing comprehensive vaccination numbers on its COVID-19 dashboards. But we still have some information about this year’s vaccination campaign, thanks to continued CDC efforts as well as reporting by other health agencies and research organizations.
This week, the FDA authorized Novavax’s updated COVID-19 vaccine. Here’s why some people are excited to get Novavax’s vaccine this fall, as opposed to Pfizer’s or Moderna’s.
Last week, I asked you, COVID-19 Data Dispatch readers, to send me your stories of challenges you experienced when trying to get this fall’s COVID-19 vaccines. I received 35 responses from readers across the country, demonstrating issues with insurance coverage, pharmacy logistics, and more.
Recently, a lot of U.S. COVID-19 news has centered around booster shots—additional vaccine doses to boost patients’ immunity against the coronavirus. Questions abound: do we need these shots, when might we need them, how do they impact vaccination campaigns?
In other countries, booster shots are being deployed as a measure of extra protection for people with weaker immune systems as Delta spreads. In France, extra vaccine doses are available for organ transplant recipients, those on dialysis, and others. Israel is similarly offering third Pfizer doses to Israelis with medical conditions that cause immunodeficiency. And in Thailand, healthcare workers are getting booster shots of the AstraZeneca vaccine after two doses of Sinovac, which has demonstrated lower efficacy than other vaccines.
Even in the U.S., a small number of immunocompromised patients have received third doses—many of them in clinical trials analyzing how well boosters work. Medical experts tend not to question why boosters may be needed for immunocompromised patients, as their weakened immune systems also make the patients more vulnerable to severe cases of COVID-19.
The real questions come when we start to consider booster shots for everyone. Pfizer, which has developed a third dose for the general population, recently announced that the company applied for Emergency Use Authorization from the FDA. The company says its currently approved two-shot regimen will cause patients to lose some protection six months after they’ve been vaccinated—and become more vulnerable to Delta—with continued lower immunity over time.
Officials at the FDA and CDC, however, have said that boosters aren’t yet necessary. The agencies released a joint statement to that effect, and U.S. health officials say they want to see more data—especially from Israel, where Pfizer has been in heavy use. Pfizer’s data on waning efficacy aren’t yet public (released by press release, not scientific paper), which complicates the conversation. Still, some health officials say we will eventually need booster shots, just not right now, according to POLITICO.
While U.S. public health experts seek more data, our booster shot conversation appears selfish in other parts of the world. While over 3.6 billion doses have been administered globally across 180 countries, high-income countries are getting vaccinated 30 times faster than lower-income countries, according to Bloomberg. More than half of Americans have received at least one shot, compared to under 1% in many African countries.
Dr. Tedros Adhanom Ghebreyesus, Director-General of the WHO, slammed the U.S. and other wealthy nations at a press briefing last week for even considering booster shots. “The priority now must be to vaccinate those who have received no doses and protection,” he said. “Instead of Moderna and Pfizer prioritizing the supply of vaccines as boosters to countries whose populations have relatively high coverage, we need them to go all out to channel supply to COVAX, the Africa Vaccine Acquisition Task Team and low- and low-middle income countries, which have very low vaccine coverage.”
Following the end of the federal public health emergency in May, the CDC has lost its authority to collect vaccination data from all state and local health agencies that keep immunization records. As a result, the CDC is no longer providing comprehensive vaccination numbers on its COVID-19 dashboards. But we still have some information about this year’s vaccination campaign, thanks to continued CDC efforts as well as reporting by other health agencies and research organizations.
This week, the FDA authorized Novavax’s updated COVID-19 vaccine. Here’s why some people are excited to get Novavax’s vaccine this fall, as opposed to Pfizer’s or Moderna’s.
Last week, I asked you, COVID-19 Data Dispatch readers, to send me your stories of challenges you experienced when trying to get this fall’s COVID-19 vaccines. I received 35 responses from readers across the country, demonstrating issues with insurance coverage, pharmacy logistics, and more.
The Delta variant is now dominant in the U.S., but our high vaccination rates still put us in a much better position than the rest of the world—which is facing the super-contagious variant largely unprotected.
Let’s look at how the U.S.’s situation compares:
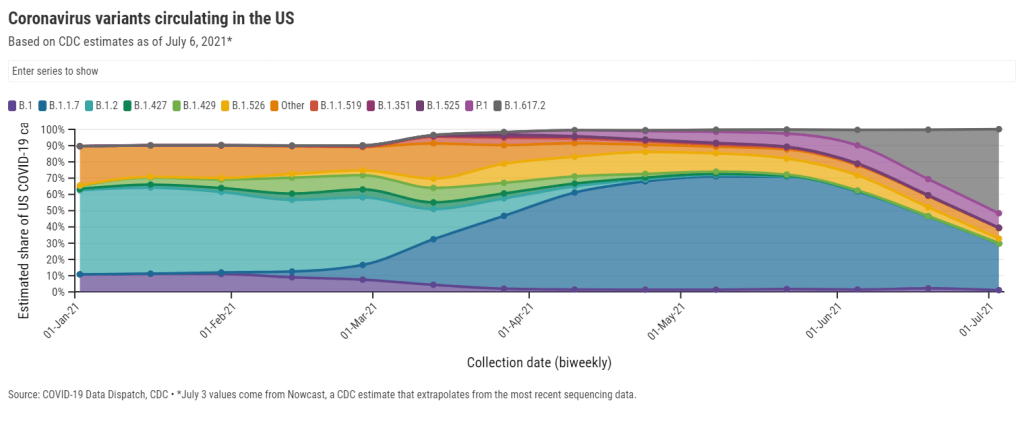
U.S.: Delta now causes 52% of new cases, according to the latest Nowcast estimate from the CDC. (This estimate is pegged to July 3, so we can assume the true number is higher now.) It has outcompeted other concerning variants here, including Alpha/B.1.1.7 (now at 29%), Gamma/P.1 (now at 9%), and the New York City and California variants (all well under 5%). And Delta has taken hold in unvaccinated parts of the country, especially the Midwest and Mountain West.
Israel and the U.K.: Both of these countries—lauded for their successful vaccination campaigns—are seeing Delta spikes. Research from Israel has shown that, while the mRNA vaccines are still very good at protecting against Delta-caused severe COVID-19, these vaccines are not as effective against Delta-caused infection. As a result, public health experts who previously said that 70% vaccination could confer herd immunity are now calling for higher goals.
The higher infectivity of Delta means the threshold for herd immunity will be higher. 70% may have been enough before, but likely isn’t high enough against Delta, as shown by case increases in places like the UK and Israel, which have high vaccination rates.
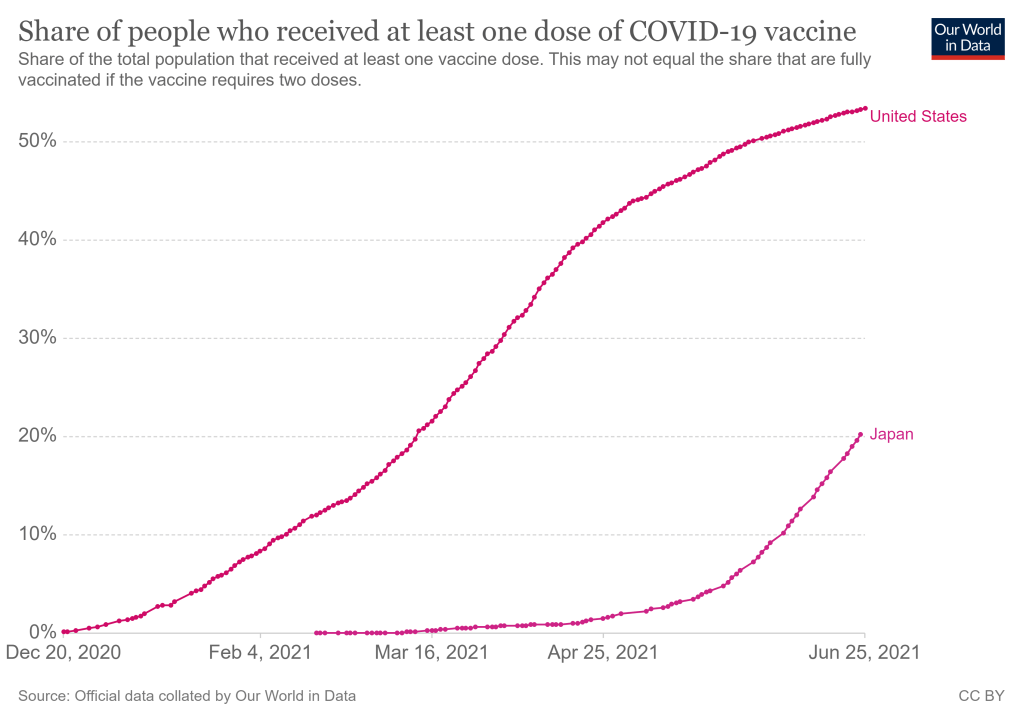
Japan: The Tokyo Olympics will no longer allow spectators after Japan declared a state of emergency. The country is seeing another spike in infections connected to the Delta variant, and just over a quarter of the population has received a dose of a COVID-19 vaccine. I argued in a recent CDD issue that, if spectators are allowed, the Olympics could turn into a superspreading event.
Australia: Several major cities are on lockdown in the face of a new, Delta-caused surge following a party where every single unvaccinated attendee was infected. Unlike other large countries that faced significant outbreaks, Australia has successfully used lockdowns to keep COVID-19 out: the country has under 1,000 deaths total. But the lockdown strategy has diminished incentives for Australians to get vaccinated; under 5% of the population has received a shot. Will lockdowns work against Delta, or does Australia need more shots now?
India: Delta was first identified in India, tied to a massive surge in the country earlier this spring. Now, India has also become the site of a Delta mutation, unofficially called “Delta Plus.” This new variant has an extra spike protein mutation; it may be even more transmissible and even better at invading people’s immune systems than the original Delta, though scientists are still investigating. India continues to see tens of thousands of new cases every day.
Africa: Across this continent, countries are seeing their highest case numbers yet; more than 20 countries are experiencing third waves. Most African countries have fewer genetic sequencing resources than the U.S. and other wealthier nations, but the data we do have are shocking: former CDC Director Dr. Tom Frieden reported that, in Uganda, Delta was detected in 97% of case samples. Meanwhile, vaccine delivery to these countries is behind schedule—Nature reports that many people in African countries and other low-income nations will not get their shots until 2023.
South America: This continent is also under-vaccinated, and is facing threats from Delta as well as Lambda, a variant detected in Peru last year. While Lambda is not as fast-spreading as other variants, it has become the dominant variant in Peru and has been identified in at least 29 other countries. Peru has the highest COVID-19 death rate in the world, and scientists are concerned that Lambda may be more fatal than other variants. Studies on this variant are currently underway.
In short: basically every region of the world right now is seeing COVID-19 spikes caused by Delta. More than 20 countries are experiencing exponential case growth, according to the WHO:
I’m struggling with how best to stress how fragile the global situation is, so I’ll be blunt:
Each week >2.6 million cases and >53,000 deaths are reported to @WHO
We’ve already seen more COVID-19 deaths worldwide so far in 2021 than in the entirety of 2020. Without more widespread vaccination, treatments, and testing, the numbers will only get worse.
Japan’s new COVID-19 cases and vaccinations, with U.S. vaccinations for comparison. Charts via Our World in Data.
Back in May, Sarah Braner wrote that Japan was seeing a COVID-19 spike in the lead-up to the Tokyo Olympics, which are scheduled to start in late July. The situation has remained worrying since then.
True, cases have dropped significantly since the May outbreak—the nation is now seeing around 1,500 cases a day, compared to a peak of 6,500 on May 14. But many Japanese residents are concerned that the Olympic games could push numbers back up.
Despite a recent push towards vaccinations, Japan’s numbers remain low: just over 20% of the population has received at least one dose, as of June 24. On social media, Japanese residents have reported issues with getting their shots due to a voucher system implemented earlier this spring. A resident must receive a vaccine voucher from the government in order to get their shot; without that bureaucratic step, they may be turned away from a vaccine clinic, even if doses are available.
Meanwhile, rules around the Olympics have focused on protecting the athletes themselves. Over 80% of the athletes have been vaccinated and Japan will prioritize getting shots to Olympics staffers, journalists, and volunteers, according to the New York Times. Athletes will also be tested regularly.
The Olympics are not allowing international spectators, but officials announced this week that Japanese crowds will be permitted—up to 50% of a venue’s capacity. While masks will be required and other guidelines will be in place, the rules for attendees are not nearly so strict as those for athletes.
It only takes one unvaccinated person to set off a superspreading event. And with variants like Delta and Gamma spreading rapidly around the world, such events are more likely and more dangerous. In order to truly make the Olympics safe, Japan should ensure the coronavirus is locked out of Olympic events—not just for athletes, but for workers and spectators as well.
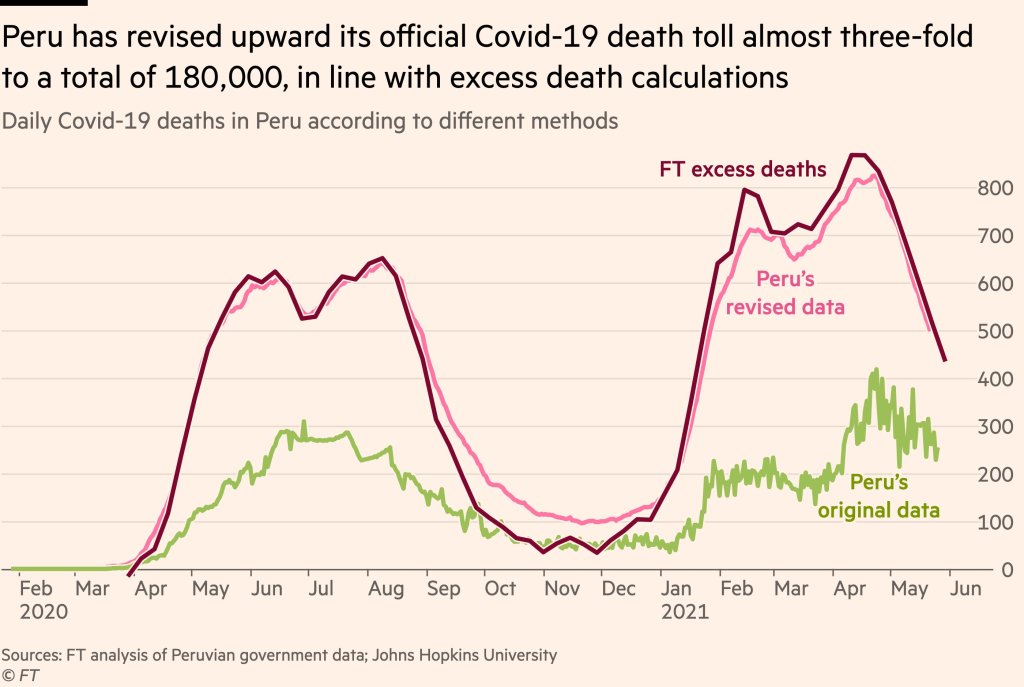
Peru’s revision led the country’s official death count to match its estimated excess deaths. Source: Financial Times..
Excess deaths are those deaths that occur above a region’s past baseline. Data scientists calculate the metric by determining the average deaths for a country or region over a period of several years—then comparing this past average to the deaths that occured in the current year.
The deaths occurring in the current year above that past average are the excess deaths. In New York City during the spring 2020 surge, for example, about four times more people were dying each week compared to the same time period in previous years.
During the pandemic, excess deaths have become a useful way for scientists to estimate the true toll of COVID-19. Especially during the earlier months of 2020, limited access to testing meant that many people who became infected with the coronavirus were not able to get the positive test required for their illness (or death) to actually be counted as a case. (In the U.S., this recording gap is currently causing issues for families who lost loved ones to COVID-19 early in the pandemic and are now seeking federal aid.)
Plus, the pandemic caused hospital systems to shut down and inspired widespread hesitancy for anyone seeking medical care for a non-COVID reason. The death of someone who had a heart attack and couldn’t get a hospital bed because of COVID-19, for example, is not a COVID-19 death but was undoubtedly caused by the pandemic.
Excess deaths, as a metric, allow researchers to see how the pandemic has impacted a country or region—above the official COVID-19 death counts. And a recent audit from Peru provides new evidence for this metric’s value.
The country essentially audited its COVID-19 deaths data to address undercounting. Government officials checked thousands of death certificates from 2020, and added any COVID-related deaths to past totals—which previously only included those Peruvians who had positive PCR tests.
After the audit was complete, Peru’s COVID-19 death toll rose by almost three times—to 180,000 deaths. The country now has the highest official death rate in the world: one in every 177 people.
When plotted over time, Peru’s revised death data match closely with its excess deaths, as calculated by the Financial Times data team. This audit—and its match with excess deaths—shows that excess deaths do, in fact, show the true toll of COVID-19 in a country.
It’s also notable as the first time a country has done such an audit on a wide scale. Some states (such as Washington) have added COVID-19 deaths to their official counts periodically, as they process death certificate backlogs, but none have done anything on Peru’s level.
Future death certificate audits and excess death analyses may help us understand the true toll COVID-19 has taken on the U.S. and the world.
In the reader survey I sent out a few weeks ago, I asked, “What is one question you have about COVID-19 in the U.S. right now?” One reader responded with an inquiry into vaccine equity: “What will it look like when the U.S. is ‘open’ and vaccinated and many other parts of the world are not?”
That question feels especially relevant this week. On Thursday, the Biden administration made a big (and long-awaited) announcement: the federal government is sending 25 million vaccine doses from America’s stockpile to other countries. The administration has previously promised to send at least 80 million doses abroad by the end of June, but this week’s announcement included more details—such as countries that will receive these initial doses and other logistics.
Out of the 25 million, about 19 million doses are going to COVAX. COVAX, a global effort run by the World Health Organization and other international government bodies and philanthropic organizations, brings vaccines to low-income nations at no cost. The COVAX doses will go to India, other parts of Asia, Central and South America, and Africa, Bloomberg’s Josh Wingrove reports.
The remaining 6 million doses will be sent directly to countries, including Ukraine, Kosovo, Haiti, Georgia, Egypt, Jordan and Iraq. Some doses are going directly to India as well—while the worst of this nation’s surge may be over, it’s still facing high case counts, full hospitals, and a terrifying “black fungus” linked with the Delta variant (B.1.617).
At first glance, this might seem like a noble move on the Biden administration’s part. The U.S. is seeing low case numbers and widespread reopenings, so we can share some supplies to “help the pandemic around the globe,” as COVID-19 response coordinator Jeff Zients said at a briefing on Thursday.
But 25 million doses—or even the 80 million doses that the administration has promised by the end of this month—is a drop in the bucket compared to actual international needs. For example: COVAX needs 1.8 billiondoses to vaccinate about half the adult population in low-income countries. COVAX has specifically prioritized 92 low-income nations, representing a total population of 3.8 billion.
That 1.8 billion dose number is a highlight of a major report released last week by the Rockefeller Foundation, a global charitable foundation, discussing what it would take to vaccinate the world. I covered the report for Science News. According to this report, Gavi (the Vaccine Alliance), an international public-private body that runs COVAX, needs to raise $9.3 billion in order to pay for those 1.8 billion doses. Gavi has been working to raise this money from countries and independent donors at a global health summit this past week.
While $9.3 billion might seem like a massive price tag, the cost of failing to provide these vaccines would actually be far greater. The global economy may lose up to $9.2 trillion if richer nations fail to support equitable vaccine distribution, according to an estimate from the International Chamber of Commerce.
So far, the U.S. has administered about 300 million vaccine doses (as of yesterday), covering over half the total population. In a number of low-income countries, less than one percent of the population has received a dose. Tedros Adhanom Ghebreyesus, Director General of the WHO, said at a recent assembly that, if all doses administered globally had been sent out equitably, the doses would have covered “all health workers and older people.” Instead, high-income nations are largely protected while low-income nations are vulnerable to future surges and highly-transmissible variants.
Through this lens, the 25 million dose shipment announced this week is far from impressive. It’s a useful start, certainly, but it’s not going to end the pandemic anywhere. Even the 80 million doses promised by the end of June is a tiny number—about 4% of the doses COVAX is hoping to obtain. It’s also only 11% of the doses that vaccine makers have pledged to deliver to the U.S. by the end of July, according to Bloomberg.
That larger June shipment has also been held up because the Biden administration is planning to send AstraZeneca vaccines—which are under review from the FDA because they were produced at the Emergent factory that infamously wasted millions of Johnson & Johnson doses. The AstraZeneca vaccine is not authorized for use in the U.S., so of course it will make up the majority of the doses we send abroad this summer.
Speaking of unused doses: the Biden administration may also start sending unused doses from states to other countries, POLITICO reported this week. The administration wants to get thousands of Pfizer, Moderna, and J&J doses—on the verge of expiring—to countries that would actually use them. While this possible policy hasn’t yet been realized, it hammers home a clear message: the U.S. will donate “unwanted” vaccine doses only when we are absolutely certain that we don’t need them here.
Now, let’s return to our reader’s question. What happens when the U.S. is safely vaccinated, but other parts of the world aren’t?
From a health standpoint, the U.S. will probably be okay. The vaccines are very effective, even against variants—likely protecting the country from another major surge. We will need careful surveillance to guard against future variants that may evolve beyond the vaccines (see: last week’s issue), and it’s possible that overly zealous reopening this summer will lead to outbreaks next fall and winter. But seniors and other vulnerable people would be more protected than they have been in past surges, and booster shots (for the variants) will likely be on their way soon. In short, America’s wealth will protect us.
Around the world, however, outbreaks will continue. Every time a new person gets infected with the coronavirus, the virus has a new opportunity to mutate. And with every mutation, the virus learns to spread faster, to evade common treatments, even to evade vaccines. Thanks to globalization, as long as the virus is a threat anywhere, it continues to be a threat everywhere.
Plus, as low-income nations suffer from continued outbreaks, the global economy will continue to suffer. Out of that $9.2 trillion cost estimated by the International Chamber of Commerce, the majority will likely fall on wealthier nations (like the U.S.) that rely on other countries for products and labor.
“The pandemic itself has gone beyond a health crisis — it has now gone into an economic crisis,” Christy Feig, the Rockefeller Foundation’s director of communications and advocacy, told me when I spoke to her for Science News. “The only way to unchoke the economy is by getting the vaccines to as many countries as possible, so that we can stop the spread of the disease before more variants come.”
As many Americans who lived through wildfire season, hurricane season, or the Texas winter storm know well: it’s hard to protect yourself in a pandemic when you’re dealing with another simultaneous disaster.
And it is especially hard to protect yourself when you live in a region that’s cut off from resources and medical expertise—as is the case for people in Gaza and other Palestinian territories.
In the past couple of weeks, violence in this region has shut down hospitals and prevented vaccine deliveries. Unvaccinated people have crowded into shelters in Gaza, while all testing and vaccination efforts have stalled.
Gaza has also lost critical medical leadership in the recent violence: two senior doctors at Al-Shifa Hospital, the largest hospital in the Gaza Strip, were killed in recent Israeli airstrikes. An early-morning attack on the al-Wehda district last Sunday killed Dr. Ayman Abu al-Ouf, head of internal medicine at the hospital, and Dr. Mooein Ahmad al-Aloul, a psychiatric neurologist, along with at least 30 others.
Al Jazeera reports that “medical personnel remain in short supply” throughout the Palestinian territories, leaving people to instead rely on international aid groups for medical care. And constant air raids have limited medical care even further. One Israeli attack blocked the main road leading to Al-Shifa hospital, for example, and a Doctors Without Borders clinic was hit last weekend.
“People are not daring to visit health facilities. We are fearing this will have a major negative impact,” Sacha Bootsma, an official from the World Health Organization, told the New York Times.
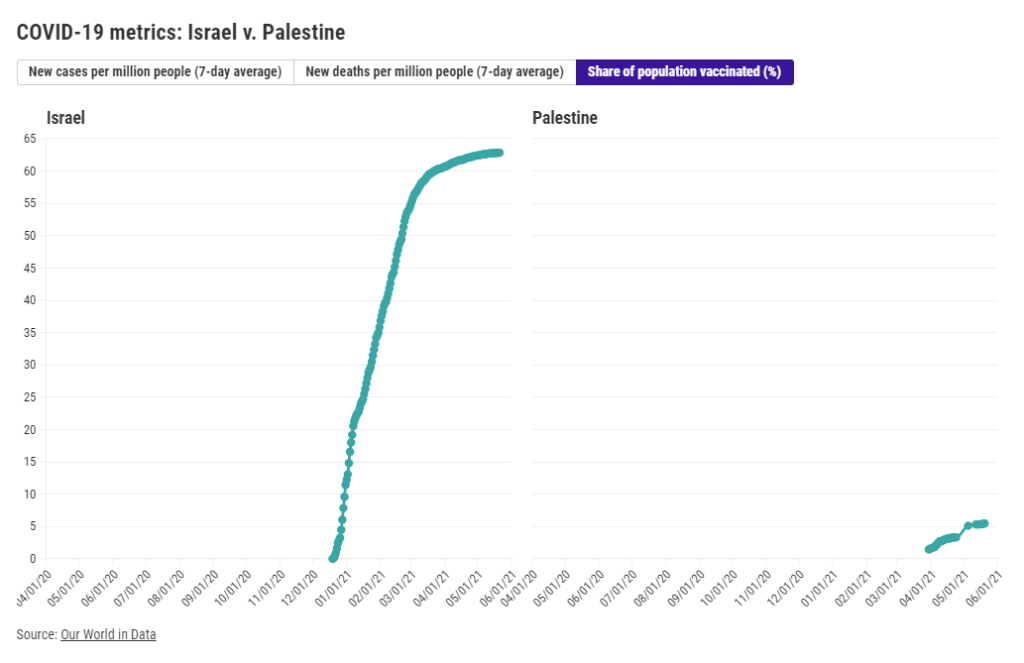
About 5% of Palestinians have been vaccinated as of May 20. Most of those doses have come from COVAX, the global vaccine alliance, and shipments have faced logistical challenges in getting to Gaza through an Israeli blockade. The United Nations released a statement in January calling on Israel to “ensure swift and equitable access to COVID-19 vaccines for the Palestinian people under occupation,” but Israeli leaders have denied this responsibility.
Israel, meanwhile, is largely protected against a COVID-19 surge. The country has been a global leader in vaccinations; by the end of February, over half of the population had received at least one dose. Now, almost two-thirds of the population are vaccinated.
Cases in Israel have remained at low levels throughout the violence in recent weeks thanks to the vaccines. The country has seen fewer than 20 new cases per million people a day since mid-April. Palestine, meanwhile, faced a surge during March and April, with the territories’ highest COVID-19 case numbers yet.
While reported case numbers in Palestine have dropped in recent weeks, this is more likely due to a lack of testing than an actual drop in infections. And the situation is not improving. Though Israeli and Palestinian forces have now formally reached a cease-fire, Israeli police have continued to attack Palestinians—including an attack against worshippers at al-Aqsa Mosque.
Continued violence and lack of medical care for Palestinians may mean that the pandemic continues here long after it ends for Israel. As is true of all COVID-19 outbreaks, continued transmission may breed coronavirus variants that threaten the rest of the world.
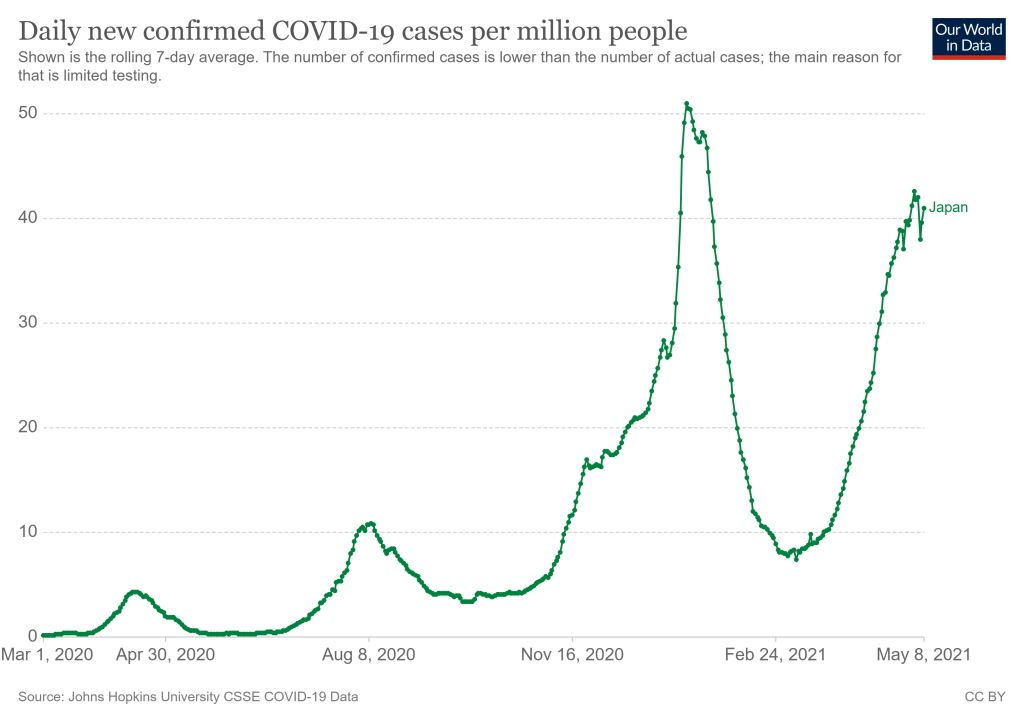
Japan’s new COVID-19 cases per million, as of May 8. Chart via Our World in Data.
They’re definitely not ready now. The Japanese government just announced it would extend an already-standing state of emergency through May 31 following a large spike in COVID-19 cases. After “Golden Week,” a sequence of Japanese Holidays lasting from late April to early May, Tokyo reported 907 new cases for the week. (New York City reported 985 cases just on May 7, for comparison.) A variant called N501Y has caused recent surges in cases, like in Osaka where hospitals struggled to treat the influx. N501Y is more infectious, and it has been correlated with more serious cases.
This surge comes as Japan struggles to roll out vaccinations. According to Our World in Data, as of May 6, 2.44% of the country’s population has received at least one dose of the vaccine. (In the United States, around 57% of the population has received at least one dose as of May 8.) So far, Japan has only approved the Pfizer-BioNTech vaccine for use, though it may approve the Moderna and AstraZeneca vaccines by May 20. Pfizer has also announced that the company will donate vaccines to athletes and staff, and the International Olympic Committee has said, “It is expected that a significant proportion of Games participants will have been vaccinated before arriving in Japan.”
An online campaign called Stop Tokyo Olympics has gained more than 200,000 signatures to an online petition, per Reuters. A Japanese poll in January showed that 80% of respondents said the games should be postponed or cancelled, and this trend has held true since.
Japan has been extremely successful in controlling the pandemic so far, but that has also led to a lack in urgency in vaccinating the population, and again, surges have happened. The Olympics are very difficult to do in an NBA-like bubble. The scale of the Olympics is much larger, and with case counts across the world as high as they are, it’s hard to imagine that someone won’t come down with COVID-19 during the games. As the New York Times points out, the chances of a COVID-19 free Olympics are slim—instead, the priority will be controlling cases as they come up.
Officials have repeatedly insisted that the games will go on as planned, and there is no sign that they will be cancelled or postponed. Will this current state of emergency crush the curve enough? We won’t know until July.
India’s COVID-19 curve resembles a vertical line right now. An already fragile health infrastructure is on its knees, the government has shown itself to be incapable. There are no hospital beds to be had, no medicines, no oxygen, no emergency care; even the dead have to endure 20-hour queues for last rites. A nine-day streak of 300,000-plus new cases daily has ended with fresh infections crossing the 400,000 mark on May 1. More than 3,000 COVID-related deaths have been recorded daily for three consecutive days. Still, the worst, experts say, is yet to come.
If one compares India’s cumulative figures with the U.S.’s, however, the numbers don’t seem to make sense. India’s 18.8 million confirmed cases, with 208,330 deaths, don’t seem anywhere near U.S. figures of 31.9 million and 568,836 respectively. India appears to record 1,360 cases and 15 deaths per 100,000 people, versus 9,684 cases and 172 deaths per 100,000 people in the U.S. Even accounting for the fact that India’s population (1.4 billion) is more than four times that of the U.S. (330 million), the scale of the devastation seen on the ground—patients three to a bed or being treated on the streets, people dying outside hospitals waiting for treatment, entire families being wiped out, and mass cremations taking place on pavements and car parks—appears disproportionate.
The reasons are complicated and intersecting. For one, the official figures are highly likely to be vastly underestimated in India. Moreover, the country’s health infrastructure has always been fragile. There are only 5.3 beds per 10,000 population (versus 28.7 for the U.S.), and given the sheer numbers of COVID-19 infections, it’s simply a case of just-not-enough. Other reasons for the low numbers in India could, quite simply, be a lack of testing—only 1.74 daily tests per 1,000 people—as well as a purposeful obfuscation of actual figures.
Experts say that COVID-19 deaths have been undercounted across the world for various reasons; testing methodologies and the recording of confirmed cases has not been uniform. “Every country reports those figures a little differently and, inevitably, misses undiagnosed infections and deaths,” Reuters’ COVID-19 Global Tracker states.
It’s like looking at an iceberg, says one of India’s top epidemiologists, Dr. Jayaprakash Muliyil, chairperson of the Scientific Advisory Committee of the National Institute of Epidemiology, in a phone conversation. “The number of cases the system picks up is a fraction [of the actual number of infections],” he says. “A large number of cases are subclinical [not severe enough to present definite or readily observable symptoms].” This fraction depends on several factors—it is lower in smaller states with better infrastructure, like Pudducherry, and higher in others with greater population density, like Bihar.
A recent study found a “severe under-ascertainment of COVID-19 cases” across U.S. states and countries worldwide. “In 25 out of the 50 countries, actual cumulative cases were estimated to be 5–20 times greater than the confirmed cases,” report authors Jungsik Noh and Gaudenz Danuser, adding that, “The estimation of the actual fraction of currently infected people is crucial for any definition of public health policies, which up to this point may have been misguided by the reliance on confirmed cases.”
Serological surveys (using antibody tests) indicate that the actual number of infected people could be 30 times higher in India than what official figures show. COVID-related deaths could be anything between 2 to 5 times and 10 to 15 times than what is being reported.
Modeling methods may be a headache, but pandemic curves always come down, and this one will too, says Dr. Muliyil. He is not a fan of lockdowns for a country like India—having said back in September that it had flattened the wrong curve, that of the economy. With newer mutations of the virus appearing to be more easily transmissible, he says that an infection rate of 70 to 75 percent might be required for herd immunity. Meanwhile, “natural protection to the virus is excellent.” He prescribes strategic vaccination—focusing on the 45-plus age group rather than younger people, and those who haven’t been infected— and “bring back the urge to mask up and avoid crowds.”
Payal Dhar is a freelance journalist from India who writes on science, technology and society.
Editor’s note: If you would like to contribute to help the situation in India, here are three recommendations from Payal:
India Covid Relief is a hub site that links to organizations helping on the ground, such as Hemkunt Foundation, Give India, Goonj, and Milaap.
@gresshaa on Twitter has compiled a list including Venmo accounts and other international options for direct donations.
The COVID-19 Data Dispatch was able to compensate Payal for this piece thanks to the support of the COVID-19 Data Dispatch’s members. We hope to be able to feature more guest writers in the future—if you’d like to support this work, please consider a contribution.










_C.jpg){kind=link}