After I shared my travel experience last week, a couple of readers reached out asking for more details on using a portable HEPA filter, essentially a small air filter that can be moved from one place to another.
Scientific research has shown that air filters can be valuable tools for reducing the risk of COVID-19, along with other respiratory viruses and pollution concerns, such as wildfire smoke. These filters essentially remove dangerous particles from the air, making indoor spaces safer.
These air filters can be costly (prices range from $50 to $1,000), but may prove to be a helpful long-term investment if used often. My partner and I used ours while traveling, as well as in our apartment when we have guests over and during periods of intense wildfire smoke pollution in New York City.
Here are a few tips and resources about using HEPA filters:
You might see filter options boasting their clean air delivery rate, or CADR. This is a measurement of an air purifier’s effectiveness, telling you how much filtered air the machine can provide in a given timespan (cubic meters per hour, cubic feet per minute, etc). For more details, see this blog post from Air Conditioner Lab.
Understanding your air filter’s CADR is important because it tells you the range in which your device works. For example, a smaller filter with a lower rating might clean the space immediately in front of you on a train, but would not clean the entire car. Smaller filters might also need to run for a longer time to clean an enclosed space (such as a hotel room).
If you’re traveling with an air filter, a portable battery can be helpful to extend the device’s runtime. My filter runs for a couple of hours on its own battery power, but will last for much longer if plugged into a portable battery.
Research and recommendations from air filter providers recommend placing your filter close to you and facing you, to get the clean air delivered as close to you as possible.
If you’re also using a CO2 monitor, it’s important to note that the monitor’s reading likely won’t change due to a HEPA filter. CO2 monitors measure clean outdoor air in a space, so they do not register when existing air is filtered. A monitor that measures particle pollution would be needed to see the difference your filter is making.
Know when to change your device’s air filter! Many devices have built-in indicators telling you to do this (i.e. a light that flicks on when the filter needs replacement), while others will come with instructions recommending a filter change after a given period of time.
Air filter use is not an exact science. While you can find answers to some questions in scientific literature, others might require crowdsourcing on social media or trial and error on your own to find what works best for you. Overall, though, remember that any use of an air filter will be better than taking no steps to clean your air.
I hope this is helpful. If you have more questions (or would like to share your own recommendations), please reach out!
Betsy and her partner’s portable HEPA filter, pictured on the train from Berlin to Brussels. Her partner (in an N95 mask) is visible in the background.
A few days ago, my partner and I returned home from a two-week vacation to several cities in Europe. It was our first time traveling internationally since before the COVID-19 pandemic, and the trip required a lot of time on planes, on public transportation, and in crowded spaces.
I’m sharing what we did to reduce our risk of COVID-19 (and other common pathogens!) during the trip, in the hope that this will be helpful for readers traveling this summer. While taking these sorts of precautions may be increasingly unpopular in many places, these measures still reduce the risk of illness for individual travelers and the people around them.
Here’s what we did:
Reduced potential exposure and tested before we traveled: It’s pretty typical for me to avoid crowds and indoor events prior to traveling. In this case, my partner and I did attend Pride marches in New York City the weekend before our trip, but we only attended outdoor events and wore masks in the crowds to reduce our risk. We also both got PCR tests the day before leaving (we’re lucky to live near one of the few public testing sites in the city that are still open).
Masked indoors, with high-quality masks: I consistently wore N95 masks on the trip, including my reusable respirator on planes. (I wrote more about my respirator in this post last summer.) My partner also wore an N95 or KN95 throughout the trip. We have different preferences for which masks fit us well, so we had a few masks of different brands packed to accommodate that.
Avoided indoor dining (as much as possible): All of our meals were outdoors. My partner is vegan, so any restaurant where we ate had to fit into a Venn diagram of “vegan options” plus “outdoor seating”; this might sound challenging to find, but with a bit of planning—and with thanks to the Happy Cow app—it was actually quite doable. We had to eat briefly on planes at a couple of points, but we minimized that time as much as possible (eg. masking in between bites) and did so only when plane air filtration systems were going.
Took advantage of smoking sections: European cities tend to have a more prominent smoking culture than the U.S., so many restaurants and bars have outdoor smoking sections. This can be a tricky situation for COVID-cautious travelers; yes, you’re outside, but you’re also breathing in a lot of second-hand smoke. Still, my partner and I found these sections to be a helpful option. We even had lunch in an outdoor smoking zone at the Keflavik Airport (in Iceland) during a layover on our way home to NYC.
Used a CO2 monitor to gauge ventilation in some spaces: I am a proud owner of an Aranet CO2 monitor, which I mostly use to track ventilation at my apartment and public spaces in NYC. I brought the monitor on the trip, and used it to identify which public buildings had better air quality. For example, train platforms at Berlin Hauptbahnhof (the city’s central train station) are open to outdoor air and have frequent airflow, as evidenced by a CO2 reading I took of 611 ppm—well within the Aranet monitor’s “green zone.” So, I felt comfortable taking off my mask there for a few minutes to drink coffee.
Used a HEPA filter on trains, hotel rooms: My partner and I have a personal, portable HEPA filter that runs on a battery and fits easily in my duffel bag. I brought it along on the trip and used it a few times, mostly on crowded trains and in hotel rooms that did not have great airflow. It also doubled as an extra fan in our Airbnb in Amsterdam (which was not air-conditioned).
Rapid-tested every two days: Over the two weeks of traveling, my partner and I took a rapid test every two days to check for any developing illness. We also requested testing from friends and family members with whom we spent time indoors, such as a friend whom we stayed with in Berlin.
Testing and symptom monitoring after getting home: Since arriving home in NYC on Wednesday evening, my partner and I have each gotten PCR tests. I also rapid-tested once, as an extra check before attending an event on Thursday. We’re planning to do another round of PCR testing next week and monitor for any symptoms; so far, we haven’t seen any signs of illness.
I acknowledge that these safety measures may sound like a lot of effort. Certainly, tools like rapid tests and a personal HEPA filter cost money, and may not be accessible to many people. And in an ideal world, everyone would be able to travel in a world where these tools are free and commonplace, rather than a reason for extra advanced planning.
There are also increasing social pressures to not take precautions, especially in some of the places that we visited. I had a few conversations with strangers who insisted I was strange for wearing an N95, that COVID-19 was “over”; I was even patted down and pulled into a security screening at the Amsterdam airport by guards who decided my respirator was suspicious.
I am the kind of person who doesn’t back down to this pressure, especially when I have the research and reporting to back up my convictions. But I don’t want to be an isolated person taking precautions in a sea of others who aren’t acting to protect public health.
Broader change is really needed; in the meantime, though, I hope my experience is informative for others. If you are also traveling this summer and you have other tips you’d like to share with the COVID-19 Data Dispatch community, please send them to me! You can email me or comment on this post.
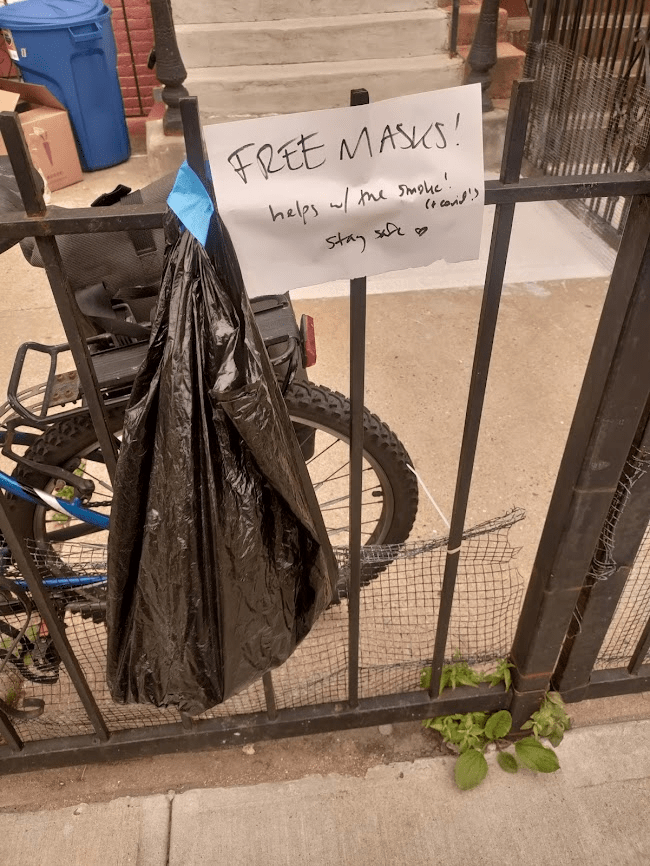
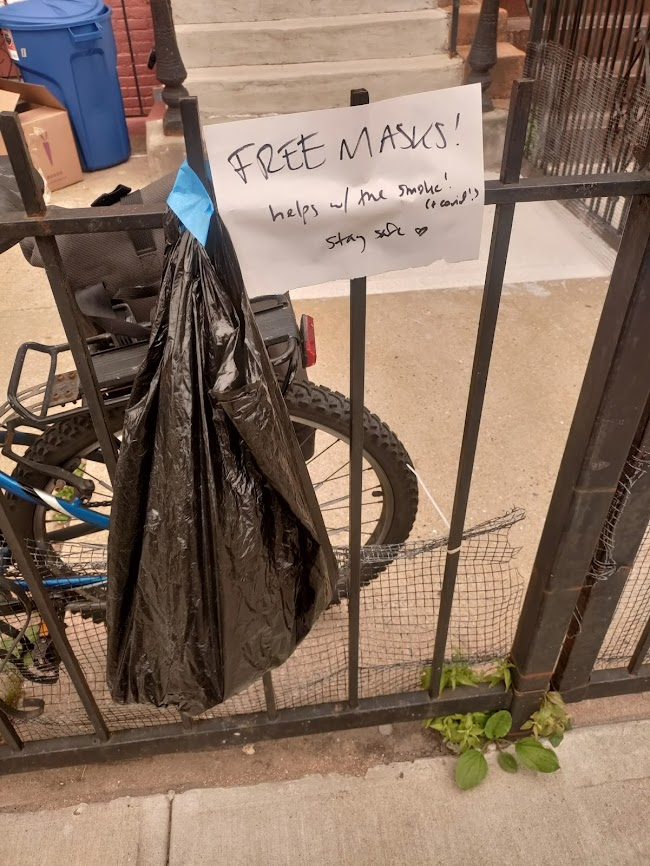
I left some free masks outside my apartment for my neighbors this week. That orange tint on the photo is from the poor air quality in NYC.
This week, much of the eastern U.S. was inundated with wildfire smoke that traveled south from Canada. While fires have been blazing across the country for several weeks, some recent particularly-intense wildfires in Quebec led to smoke so full of pollutants, it set poor air quality records in the U.S.
Americans living in California and other Western states have grown accustomed to wildfire smoke over the last few years; you might remember the orange skies over West Coast cities in fall 2020. But for people on the East Coast (myself included), this week’s smoke was a rude reminder that climate disasters have no borders or boundaries.
The smoke also reminded us how important clean air is for our health. The same public health measures that help reduce COVID-19 risk can also reduce the impacts of wildfire smoke. High-quality masks filter out both the pollution in smoke and coronavirus particles at the individual level; ventilation improvements do this at the collective level. And these health measures help with other respiratory viruses, other types of pollution, chronic conditions like asthma… the list goes on.
For COVID-cautious folks like me who still wear masks in public spaces, the smoke situation this week demonstrated that yes, many people are willing to put a mask on if they understand why it’s needed—and if the masks are widely available. In New York City this week, I saw more people wearing masks than I have since the height of the Omicron wave in winter 2021-2022. Public officials encouraged masking and even gave out masks in large numbers.
In addition to broader mask use, more people have become interested in cleaning the air in their homes and in public spaces. Air filter sales spiked on Amazon this week, CNN reported, as did Google searches for these items. My Twitter feed has been full of recommendations for air-cleaning devices and instructions for building DIY filters.
This is all great to see, but I hope it’s not just a one-week trend. If we invest in cleaner air now—both individually and collectively—we’ll be more prepared for the next round of wildfire smoke. (While the worst has likely passed for now, we’re likely to see more events like this in the future.) And we’ll be more protected against COVID-19 and other respiratory diseases.
With that in mind, here are some suggestions that apply to both COVID-19 and air pollution:
Stock up on high-quality masks, i.e. N95s and KN95s. This STAT article has some helpful information about which masks work well for COVID-19 protection as compared to air pollution. Notably, for COVID-19 protection, it’s more important to mask inside, while for air pollution protection, it’s more important to mask outside.
Buy or make air filters for your home. Air filters can dramatically improve air quality in an indoor space, and you don’t have to spend hundreds of dollars to get one. Corsi-Rosenthal boxes can be easily constructed with less than $100 of materials.
Monitor your local air quality. This can include buying a monitor to measure CO2 or pollutants, or following air quality data through public sources. I’ve personally started checking AirNow.gov, a site run by the U.S. government, and IQAir, a crowdsourced air quality tracking site. Checking local air quality data can inform your behavioral choices, similar to checking local COVID-19 statistics.
Get involved with mask distribution. This week has shown many people are willing to put on a mask, if they understand why it’s needed and can access one. You can help share information and resources, whether that’s getting involved with a mask distribution group in your area or simply donating individually to friends and neighbors. (For example, I left some free masks outside my apartment building this week.)
Advocate for clean air in public spaces. Public buildings can do a lot to improve their air, such as updating HVAC systems and adding air filters to high-traffic spaces. There are already many groups advocating for this, such as parents organizing for ventilation upgrades at their kids’ schools; I hope the recent wildfire smoke adds new motivation to those efforts.
Do you have other suggestions or resources that you’d like to share with other COVID-19 Data Dispatch readers? Email me, and I’ll send your suggestions in a future newsletter issue.
CDC updates ventilation guidance: On Friday, the CDC made its first-ever official air quality recommendation for all indoor spaces, in an update to its overall ventilation guidance. The agency now says all buildings should strive for five air changes per hour (ACH) at a minimum; in other words, clean air should circulate through the space every 12 minutes or more. This update is a victory for many clean air advocates who’ve pushed for better guidelines during the pandemic as a way to reduce the risk of COVID-19 and other respiratory pathogens. As expert and advocate Devabhaktuni Srikrishna said to me on Twitter: “This is exactly the clarity we were pushing CDC for for since last year… Now the question becomes, how does everyone do it in their home, school, and office? How much does it cost? Where do you get it?”
Millions Missing in Washington, D.C.: On Friday, myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and Long COVID patient advocates held a demonstration at the National Mall in Washington, D.C. to show U.S. leaders how chronic disease has pulled millions of Americans out of public life. The demonstration, organized by ME Action and Body Politic, included an installation of 300 cots with hand-made pillowcases created by patients across the country. Each cot is intended to represent people who can no longer work or do other day-to-day activities that were routine before they got sick with Long COVID or a similar chronic illness. You can learn more by watching ME Action’s press conference from the demonstration.
Post-PHE prices for COVID-19 testing: Researchers at the Kaiser Family Foundation put together a new report describing how much Americans will likely pay for PCR and at-home tests now that the federal government no longer supports blanket insurance coverage. At-home test prices range from $6 to $25 per test, depending on the brand and number of tests purchased at once, the KFF analysis found based on a variety of data sources. PCR tests and others performed in healthcare settings range from $25 to $150 per test, with medians around $50. Tests including COVID-19 and other pathogens are the priciest.
Sleep apnea and Long COVID risk: A new paper, published this week in the journal SLEEP, finds that people with sleep apnea have a higher risk of developing Long COVID compared to those who don’t have this condition. Researchers at New York University (and other institutions) compared Long COVID symptoms among adults and children with and without sleep apnea through multiple electronic health record databases, finding people with sleep apnea had up to a 75% higher risk of long-term COVID-19 symptoms. This study was supported by the National Institutes of Health’s RECOVER initiative. Like other papers to come out of RECOVER (including another recent study looking at comorbidities), it’s utilized health records rather than the actual cohort of patients recruited into the NIH’s research program.
Diagnosing COVID-19 through breath: Another notable recent paper, published in the Journal of Breath Research in April: researchers at the University of Colorado Boulder and the National Institute of Standards and Technology have found they can identify whether a patient has COVID-19 by testing their breath. The technique involves using sensitive lasers and artificial intelligence to differentiate between chemicals in a patient’s breath; it’s similar to a breathalyzer for alcohol testing, though more complicated. In addition to COVID-19, breath testing might help identify other diseases.
Two weeks ago, I shared that I’d recently purchased a monitor to measure CO2 as a proxy for ventilation in my apartment and other spaces. That post led to responses from several readers who’ve also been using CO2 monitors—including Kate Nyhan, a research and education librarian at Yale University who specializes in public health.
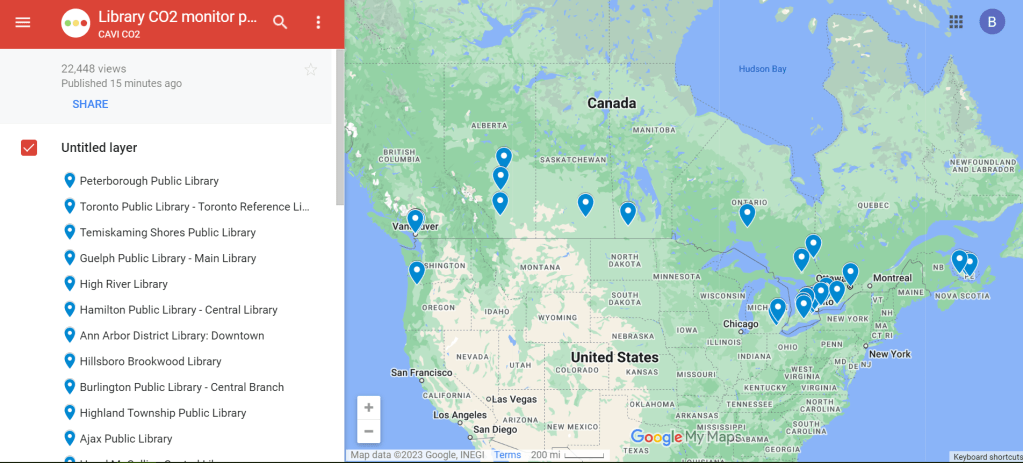
Nyhan explained that, in addition to using a CO2 monitor at her home and workplace, she co-founded a nonprofit that helps public libraries loan out monitors. This nonprofit, called Community Access to Ventilation Information (CAVI), has brought CO2 monitor access to libraries serving about one in five Canadians. In addition to the monitor-lending, CAVI develops educational materials to help library patrons use these tools and collaborates with other air quality initiatives.
I talked to Nyhan and Danielle Cane, CAVI’s managing director, to learn more about the organization and get their tips on using CO2 monitors. Here are the highlights from our conversation.
How CAVI started
Cheryl White, an engineer and air quality expert based in Toronto, Canada, got the idea for this organization in fall 2021. At that time, many people on the COVID-conscious side of Twitter started to express interest in air monitoring, Cane said.
“When we would post our readings from CO2 monitors on social media, a lot of people were saying, ‘This is really cool, I’d love to get involved,’” she recalled. “But it’s just so expensive to access these tools.” Higher-end monitors, like the Aranet device I purchased, can cost around $300.
White had the “bright idea” to partner with libraries as a way to make these monitors more accessible, Cane said. After Cane and Nyhan came onboard, the group reached out to Peterborough Public Library, a library system in a town northeast of Toronto. (Cane and White are both based in the area.)
“Peterborough Public Library was really game to introduce this program,” Cane said. CAVI also worked with the local public health department, which helped gain buy-in for lending out air monitors. The initial Peterborough pilot was launched in spring 2022 with 15 monitors, supported by funding from Canadian and American Aranet distributors.
The city of Toronto later joined the program, followed by other Canadian municipalities. Right now, about 22% of Canadians “have access to a co2 monitor through a public library,” Cane said. CAVI received additional funding in late 2022 to expand further. While the monitor-lending is focused on Canadian libraries, CAVI also produces free, open-source educational materials that can be used in other places.
Why do this in libraries?
Nyhan explained that libraries are well-poised to make air monitors more accessible. “Libraries want to empower community members with access to information,” she said. “In the context of indoor air quality, or COVID transmission risk mitigation, that might be information about airborne transmission, that might be about information about mitigations like air filters… It might be as tangible information as, what’s the number of CO2 parts per million in the space that I’m in right now?”
Lending out CO2 monitors also fits into the “Library of Things,” a concept in which libraries lend out non-traditional items—ranging from home repair tools to arts and crafts materials. As an expensive item that can provide valuable information to the community, CO2 monitors are a great addition to many libraries’ existing collections. In addition, some libraries already have people on staff with public health expertise or existing programming in this area, Nyhan said.
How the program works
The lending system tends to vary from one library to the next, but most places are loaning out CO2 monitors for one week at a time, Cane said: “Especially given the demand in certain areas, like big cities, we find that the one week schedule tends to work out best to both balance, giving people the opportunity to check a variety of settings… and allowing other people to also have that same opportunity.”
Some libraries have seen high demand, especially when the CO2 monitors first arrive at a new library. But as demand levels out over time, patrons might be able to “renew” their loans to keep the monitors for an additional week, Cane explained. Along with the physical monitors, libraries can point patrons to educational resources from CAVI that help interpret the findings.
Interpreting CO2 monitor data
As I’ve found in my own CO2 monitor adventures, there’s a lot these devices can tell you—but also a lot they can’t tell you. The biggest caveat, Cane explained, is that CO2 monitors are “a proxy for ventilation,” not a “proxy for infection risk.” In other words: a really high CO2 reading in a particular space doesn’t necessarily mean that infection is guaranteed, especially if other safety measures are in place. And “a really low reading doesn’t necessarily mean that you will not get infected,” Cane said.
Aranet monitors have a built-in interpretation feature, marking certain CO2 readings as green (good), yellow (less good), and red (bad). But CAVI has produced materials that go into more detail about explaining the ppm (parts per million) measurements. Cane shared one document, designed in partnership with Toronto Public Library, which goes into detail on what higher CO2 readings mean and how to act on them.
Taking action based on CO2 readings
Nyhan used the example of a small car to explain how people may take simple actions based on their CO2 monitors’ results. “Even if it’s just a single person, because [a car is] such a small and tightly enclosed environment, you can very quickly see the impact of breathing out, or opening the window, or changing the air to recirculate or not,” she said. Opening a window or telling the car not to recirculate brings in more outdoor air, causing CO2 levels to get lower.
This is a fairly simple lesson that a library patron might learn during the one week they have with a monitor, Nyhan said: “You learn that, and then you can give the CO2 monitor back to the library so someone else can use it.”
In a larger space, actions based on high CO2 readings might include adding external air filters, opening several windows, or hiring an HVAC engineer to evaluate the ventilation system, Cane said. Not everyone might have the capacity to hire an HVAC engineer, but many people can buy or make air filters; Corsi-Rosenthal boxes are one popular DIY model that can be constructed with commercially available box fans and filters. CAVI has recently partnered with a Canadian high-schooler who’s worked to build these boxes and share accessible instructions.
Nyhan also pointed out that CO2 monitors are “not just for people who control their own spaces” and can easily make ventilation changes. CO2 readings could also inform behavioral safety measures, she said, such as rapid testing before a social gathering in a poorly-ventilated apartment or avoiding certain poorly-ventilated parts of one’s workplace. In some cases, these readings could even be used to advocate for ventilation changes.
Next steps for CAVI
CAVI plans to continue expanding among public libraries in Canada. The organization also works with libraries elsewhere that may want to set up their own CO2 monitor lending programs, Nyhan said. Library staff and users are welcome to reach out to the CAVI team to learn more about the project: “We can share best practices, educational materials, assessment tools, grant proposals,” Nyhan said.
While CAVI, like other air quality citizen science efforts, is currently focused on mitigating COVID-19 risks, its work has implications for many other public health threats. “If we have a wider acceptance of how respiratory pathogens are transmitted, it could be useful to help mitigate other viruses, other bacteria,” Cane said. Improving ventilation can lower the chances of infection for many pathogens and reduce the health risks associated with indoor air pollutants.
Lending out air monitors fits into work that some public libraries are already doing on environmental health, Nyhan said. Libraries might have existing programs about wildfire smoke, radon, and similar air quality threats; COVID-19 and pathogens like it provide motivation for expanding these efforts. “Indoor air quality, and environmental health more generally, is a hot topic that’s only going to get more important,” Nyhan said.
Last week, I wrote about my experience with a CO2 monitor that I recently bought, and have been using to informally study the air quality in my New York City apartment. I asked readers to share their experiences with these monitors, and several of you did!
Here are some snippets from those responses; I hope it will be helpful for some readers to see how other folks are using air quality monitors.
Joyce R.:
I bought a much less expensive one (this one for $60), and I’ve been using it in my downtown office that I go to twice a week (it’s a WeWork facility and I’m in a small 2-person office there; my co-worker and I take turns using it so only one of us is in it at any given time). I of course am always masked in the building—unlike about 98% of the other tenants, sadly—except when I eat (alone in my office, or outdoors on the roof if the weather is good enough). I also have one of those personal HEPA air purifiers going all day. The monitor is showing that usually the range is 800-900, so I’m pretty happy with that.
Mark:
I have an Aranet4 and I’m amazed at the accuracy of it. I put it in my kid’s backpack and could track when he changed classes, went outside or got on the bus. It was REALLY interesting.
In a follow-up email, Mark added:
When I got his class schedule, the changes matched up to the exact 5 minute windows of changes. When I saw high numbers and asked my kid (who couldn’t see the numbers) what the class was like, he said ‘biggest class, 30 kids.’ Yep, the CO2 monitor picked it up. Really really impressive.
Kate:
Not only do I use a CO2 monitor to make risk decisions in my personal life—which shops and concert venues to avoid, are the university shuttles where I work safe (no), what setup of windows and fan make my car safer, what is the natural ventilation air exchange rate… But also, I used CO2 readings to persuade my boss to get facilities to fix a broken vent in my workplace… And EVEN BETTER, the non-profit I co-founded, ‘Community Access to Ventilation Information,’ has been helping libraries in Canada and the US lend patrons CO2 monitors and understand how to act on the readings.
I will be talking to Kate and her co-founder at Community Access to Ventilation Information this coming week, and plan to share a Q&A based on that conversation in next Sunday’s newsletter. If there are any specific questions you’d like me to ask them, please reach out!
A chart from the Aranet app shows CO2 concentrations in my apartment over the last week.
I recently bought a carbon dioxide monitor, and have been using it to collect data in my apartment and other places. In the week since I’ve been monitoring, I’ve noticed how personal data collection like this can be helpful in identifying ventilation issues, but comes with many caveats.
You might have seen photos of these devices on Twitter or in news articles; they’ve become an increasingly popular way to measure ventilation in public spaces, as a proxy for potential risks of COVID-19 spread. The basic theory is that CO2 builds up more in spaces where there’s not a lot of clean air circulation. So, when you see higher CO2 readings, that indicates less clean air coming in, which likely means COVID-19 and other viruses could be hanging around for longer, too. Higher CO2 is also correlated with other health risks, like headaches and diminished neurological function.
My CO2 monitor has mostly lived on the desk in my home office for the last week, with a couple of outings (to the park near my apartment, on the subway, etc.). I’ve been surprised by how much CO2 varies even in this one spot. A few observations:
The highest peaks of CO2 concentration usually correspond with cooking, since my kitchen has a gas stove. Even though my desk is across the apartment from the stove, the gas is still enough to send the meter above 1,500 ppm or higher.
CO2 concentration also tends to increase when there’s more conversation in the room, such as me doing Zoom interviews or talking to my partner, who shares the home office. (Talking puts more particles into the air than just breathing.)
CO2 concentration tends to drop when the room is empty and/or when the electric heater is turned off, leading to lowest levels overnight. (Our apartment has electric heating/cooling units instead of older-school radiators, and my desk sits right underneath the one in the office. Do these units expel CO2? I need to do more research here.)
Opening the office’s window usually corresponds with a decrease in CO2 concentration, though not as significant a decrease I’d expect given that the CO2 concentration outside is much lower—around 400 to 500 ppm. Perhaps opening the window further would lead to improvements, but it’s too cold in New York City to test that right now.
Of course, it’s hard to explain every single uptick and downturn in the CO2 monitor’s readings. I also have to acknowledge that a device I can buy for $250 on the internet is far from perfect; it has quirks and errors that will take me much longer than a week to fully understand. Still, I’m enjoying this small-self experiment into my environment.
Overall, the CO2 monitor has shown me and my partner that our apartment is not particularly well-ventilated. The CO2 concentrations in our office often range from 1,000 to 1,400 ppm, which indicates poor airflow. (Under 1,000 ppm is generally considered a safe level.) I’ve taken the meter on the subway a couple of times, and found that subway cars may even have lower CO2 than our office, if the car isn’t too crowded.
We were already thinking about buying an air filter for the apartment, and the CO2 results add some urgency to this task. Also, the next time we move, we’re going to look for places without gas stoves—often a challenging task when you’re renting in New York City, but there are some options.
Have you used a CO2 monitor, or tried to upgrade the ventilation in your home? I’d love to hear from you about it: comment below or reach out via email.
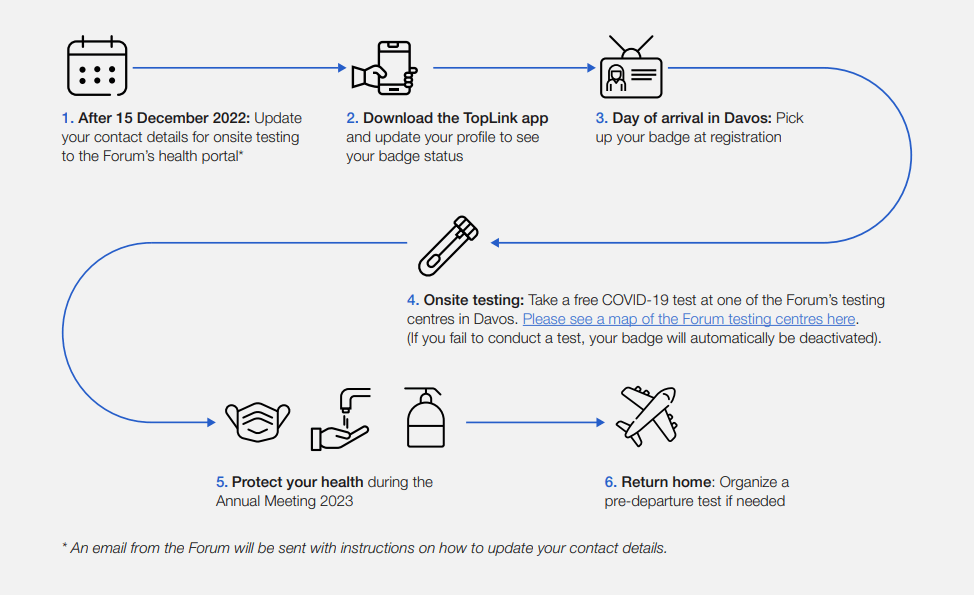
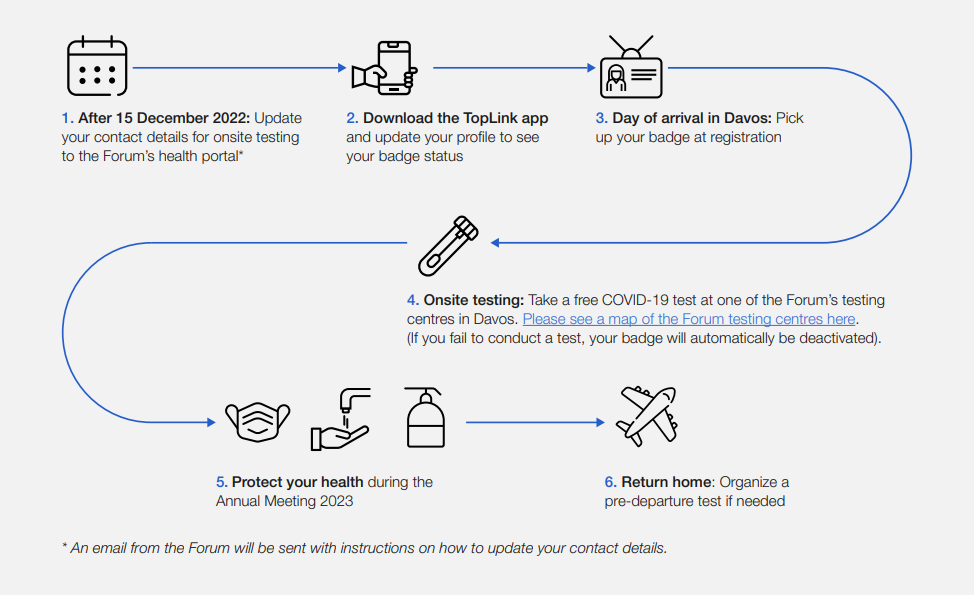
This week, thousands of top political and business leaders gathered in Davos, Switzerland for the World Economic Forum—one of the highest-profile mass events in the world. And the forum, colloquially called Davos after its location, had excellent COVID-19 safety protocols.
The protocols included: PCR tests required onsite (and event badges linked to negative results), masks recommended and available throughout the meeting venue, state-of-the-art ventilation systems, and far-UVC light. Only the best safety measures for the world’s elite, right? Even as many of those elites claim the pandemic is “over”?
News of the Davos COVID-19 protocols has led to media commentary and a Twitter hashtag, #DavosSafe, as public health experts point out that high-quality testing, ventilation, and other measures should not just be for billionaires.
Organizing tip for COVID activists: Highlighting (a) how elites are protecting themselves but not others (#DavosSafe) & (b) higher risk people are being harmed & locked out of society by status quo policies, are the most effective talking points for achieving policy change.
Rather than get angry about the inequities here, I’d like to use Davos as a reminder that many disease mitigation strategies don’t have to be expensive or restricted. Individuals can wear masks, build Corsi-Rosenthal boxes, test before gatherings, and take other relatively cheap measures to cut down on disease spread.
We deserve better. We deserve to be #DavosSafe as the hashtag going around on twitter puts it. Your children deserve to be treated with the care that world leaders are treating each other. Your family deserves to be protected from the disease which is still- unlike the flu- the third leading cause of death in the US. We don’t deserve to be shoved back into poorly ventilated workplaces while our politicians and press assure us that only crazy people would demand to breathe clean air.
This week, I’m sharing a short dispatch from the Society of Environmental Journalists (SEJ) conference in Houston, Texas. Unlike other journalism conferences I’ve attended, SEJ meetings don’t just sequester you in your hotel all day: the organizers plan field trips that are designed to give reporters on-the-ground information about environmental issues at the place they’re visiting.
I went on one of these trips, to the Houston Ship Channel and surrounding communities impacted by industrial pollution. For me, this experience was a lesson in the cascading health issues caused by environmental racism—including, of course, COVID-19—as well as the ways that data gaps can make it harder for hard-hit communities to get needed public health assistance.
The Houston Ship Channel, I learned this week, is a passage for ships going between Houston’s port and the Gulf of Mexico. According to the Port Houston website, it’s the largest container port in the Gulf Coast, handling about two-thirds of all shipping containers that travel through the region. (Shipping containers include all the consumer products that we order online.)
It is also the single largest U.S. port for petroleum exports. Every month, thousands of tons of oil and plastics (which are made from oil) pass through the Houston Ship Channel; much of this cargo is processed right on the banks of the channel, in massive refineries that define the landscape around Houston.
Houston is the largest U.S. port for petroleum exports. Refineries and chemical plants surround the ship channel. Photos by Betsy Ladyzhets.
With SEJ, I went on a boat tour through the Houston Ship Channel. We passed refineries and industrial plants from Valero, Chevron, Exxon-Mobil, and other major companies, getting a close look at just how much space these facilities take up and how they decimate the surrounding land.
After the boat, my group went to Manchester, a neighborhood close to the channel in southeast Houston. Community activists from the local environmental advocacy group TEJAS explained that this neighborhood’s population is overwhelmingly Latino; many residents are low-income workers with no college degrees who speak Spanish as their first language.
Manchester residents have faced intense pollution from industrial plants that border their homes, schools, and community spaces. We walked through a park that is surrounded on multiple sides by these plants; we could see smoke from chemicals burning, and smell the results of that burning in the air. Valero, which owns one of the nearby plants, had recently sponsored a playground in this park as a small gesture, barely acknowledging the harm it’s caused to this neighborhood.
Of course, my immediate question was: what are the COVID-19 statistics for this neighborhood? To me, it seemed obvious that Manchester residents living with this intense pollution would face higher rates of respiratory conditions, cancers, and other diseases that would make them more vulnerable to severe COVID-19 symptoms. (Poor quality air has been linked with more severe COVID-19 outcomes since the early days of the pandemic.)
Here’s the problem: nobody could actually answer my question. I spoke to Leticia Ablaza, government relations director at Air Alliance Houston and another speaker on the tour, who explained that the link between pollution and COVID-19 in Manchester and other similar Houston neighborhoods has yet to be studied. Anecdotally, she said, she knows community members with respiratory conditions who have faced heightened vulnerability to COVID-19. But there’s no formal data.
Manchester, a Houston neighborhood near the Ship Channel, is surrounded by industrial plants that pollute the community. Photos by Betsy Ladyzhets.
The reason for this lack of formal studies became clear to me later, when I attended a conference session on the links between COVID-19 and environmental health. Annie Xu, a Rice University student who has studied health disparities in Texas, said at this session that the state of Texas does not publish any COVID-19 data below the county level.
Xu’s research group did identify links between Texas counties’ racial demographics and their COVID-19 burden, published in Nature Scientific Reports in January. But when the group looked for links between air pollution and COVID-19, the analysis didn’t lead to significant results.
This finding is likely because pollution can vary widely within Texas counties, Xu said. For example, there’s a huge gap between air quality in Manchester and on Rice’s campus, both of which are included in Harris County. To truly find a connection between pollution and COVID-19, a research group like hers would require more granular data, such as at the ZIP code or census tract level.
But the Texas public health department only publishes COVID-19 data at the county level—with the exception of vaccinations, one metric that is available by ZIP code. The federal government doesn’t report COVID-19 data below the county level either.
Without this granular information, it’s difficult to demonstrate the impacts of petrochemical pollution on COVID-19 in neighborhoods like Manchester. The community isn’t able to get priority status for public health interventions like vaccines or testing—meaning that its vulnerabilities are unlikely to change.
As longtime readers know, I have spent a lot of time grappling with COVID-19’s demographic disparities. I was a leading volunteer for the COVID Tracking Project’s COVID Racial Data Tracker, and have sought to call attention to the terrible state of this type of COVID-19 data in the U.S. whenever I can. Still, it was a new experience to actually see a community left behind by the data gaps that I cover.
What kind of investment would be required to truly study how COVID-19 has impacted a place like Manchester, in Houston? And what other environment-related health conditions do we need to be investigating in these areas? I hope that future stories will enable me to answer these questions.
For now, if you have any questions, comments, or data source recommendations in this area, please reach out!















{kind=link}