In the past week (January 24 through 31), the U.S. reported about 1.0 million new cases, according to the COVID Tracking Project. This amounts to:
An average of 148,000 new cases each day
317 total new cases for every 100,000 Americans
1 in 316 Americans getting diagnosed with COVID-19 in the past week
38% fewer new cases than we reported three weeks ago
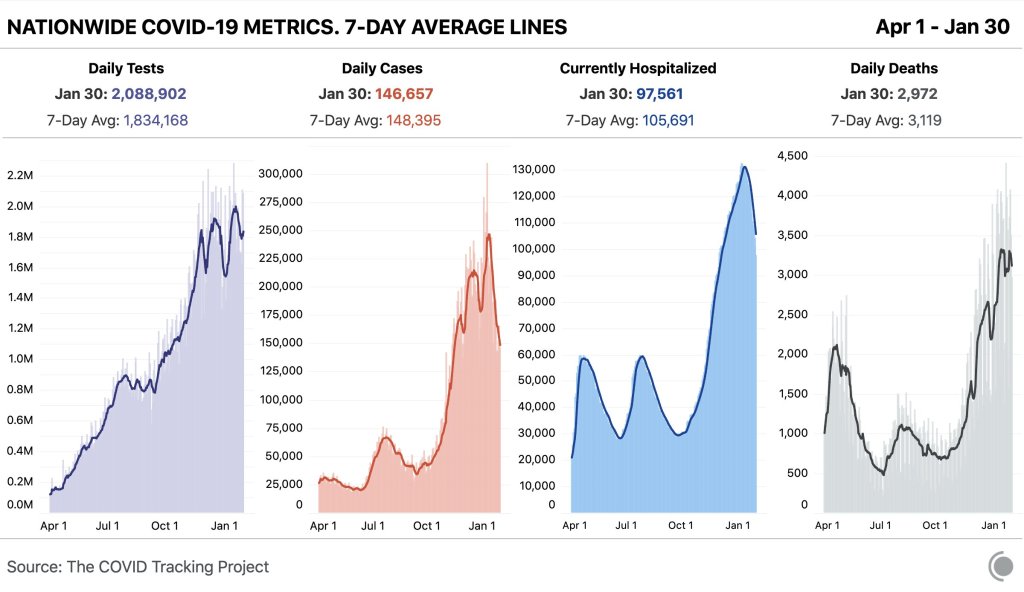
Nationwide COVID-19 metrics published in the COVID Tracking Project’s daily update on January 30. Current hospitalizations are under 100,000 for the first time in almost two months.
Last week, America also saw:
97,600 people now hospitalized with COVID-19 (30 for every 100,000 people)
21,800 new COVID-19 deaths (6.7 for every 100,000 people)
An average of 1.35 million vaccinations per day (according to Bloomberg)
The number of patients hospitalized with COVID-19 is under 100,000 for the first time since December 1. Still, this current number is about 60% higher than the peak number of patients hospitalized during either of the U.S.’s previous surges last spring and summer (60,000).
While new COVID-19 cases and hospitalizations continue to slow, continuing the trend from last week, new SARS-CoV-2 variants continue to give experts cause for concern. South Carolina’s public health department identified two cases of the B 1.351 variant first reported in South Africa; this variant is known to be more contagious and less susceptible to vaccines. Meanwhile, the B.1.1.7 variant (first reported in the U.K.) continues to spread—CDC officials are concerned that it could be the dominant strain here by the spring.
And New York—which has already reported 42 B.1.1.7 cases—is planning to open indoor dining in February. I’m no public health expert, but I plan to be ordering takeout for a long time yet.
While some of President Biden’s lieutenants in the pandemic control effort await Senate confirmation, many leaders have already taken charge. Mere hours after the inauguration, new CDC Director Rochelle Walensky extended the agency’s eviction moratorium until March 31. And Dr. Anthony Fauci is once again taking a prominent role in White House communications, appearing at press briefings and announcing America’s return to the World Health Organization.
We have two featured sources this week, both related to vaccination data:
US COVID-19 Vaccination Tracking: This is a new vaccination dashboard focused on demographics, developed by researchers at Georgetown University’s Bansal Lab. The dashboard compiles data on vaccination by race, ethnicity, sex, and gender from state reporting. Users can also hover over counties to see what share of the county’s population has been vaccinated, based on county or state data. Here’s a Twitter thread from lead researcher Shweta Bansal on the dashboard’s methodology and findings so far.
COVIDcast vaccination survey results: I’ve featured COVIDcast, a project by the Delphi Group at Carnegie Mellon University, before. The project’s dashboard interactive maps for a variety of COVID-19 indicators ranging from movement trends to antigen tests. But I’m featuring the source again this week because recently, the Delphi Group collected survey data on vaccine acceptance. You can download the data and compare vaccine hesitancy across counties; read more about the release in MIT Technology Review.
Earlier this week, I got a frantic email from my grandma. She wanted my help in finding a vaccination appointment. She’d talked to her primary care provider and looked at her state public health agency’s website, but wasn’t sure how to actually secure her own spot in line. She lives in California, which is still officially in Phase 1A (vaccinating healthcare workers and long-term care facility residents), but is allowing some providers to start vaccinating seniors and essential workers based on “available supply.”
My uncle did help my grandma get an appointment—one month from now and an hour’s drive away. Despite living in Berkeley, near several research universities, she’ll be heading to Palo Alto for her shots. I told her to keep a close eye on her county public health department’s website in case something becomes available there (which would be my advice to anyone else in this position), but I couldn’t guarantee that she’d be able to find an appointment any closer than the one she has now.
And she’s not alone: a lot of grandmas are having trouble getting vaccination appointments. In fact, recent survey data from the Kaiser Family Foundation suggests that the majority of American seniors “do not have enough information about when and where they will be able to get the vaccine.” Black, Hispanic, and low income adults also report not having enough information about vaccinations, according to KFF. The minority communities that continue to be heavily impacted by the pandemic are supposed to be first in line for vaccines, but barriers to information and technology—particularly to vaccine registration portals—are leaving them behind once again.
It would be easy to say the problem here is a lack of vaccine doses. But that’s not exactly it. The federal government is distributing millions of doses each week, and many of those doses are making it into arms: according to Bloomberg’s vaccine tracker, an average of 1.1 million shots were reported each day this past week. By sheer numbers, we are already on track to meet President Biden’s 100 million vaccinations in 100 days goal.
Our current problem is, in fact, a logistics one. It’s a build up of infrastructure failures, with all the weight falling on those underfunded local public health departments I mentioned in the previous section. Right now, these public health workers are trying to set up vaccination appointments, while also dealing with constantly-changing information from their state on how many doses they will get, while also stretching out a depleted budget, while also probably short on personnel because half of their staff quit or got COVID-19 in 2020, while also dealing with backlash from their communities, while also fielding endless calls from confused grandmas… and all of this while still testing, contact tracing, and communicating basic pandemic safety measures. Whew. I got tired just writing that sentence.
Some dimensions of this problem, such as the funding and lack of community trust, are years in the making. But there’s one piece the federal government may be able to solve soon, and it’s a data issue. The federal government is not giving states—and by extension, local public health agencies—enough lead time to coordinate their vaccine distribution. ProPublica reporters Caroline Chen, Isaac Arnsdorf and Ryan Gabrielson explained the situation in a detailed feature this week: unpredictable shipments at the national level mean that vaccine providers are unable to use up all of their shots in some weeks and cancelling appointments in others. The whole piece is worth reading, but I want to highlight the one quotation near the end:
Starting Wednesday, it will be up to the Biden administration to provide clear visibility for states, according to a member of the president-elect’s COVID-19 team, who asked not to be identified because he wasn’t authorized to speak on behalf of the new administration.
“The government can point at the manufacturer, but it’s like asking the [Defense Department], ‘How many planes do you have?’ and them saying, ‘I don’t know, ask Boeing,’” the person said.
Reporters at POLITICO similarly found that public health workers simply don’t trust the dose allocation system. While the Biden administration may want to ramp up vaccine production in order to vaccinate more Americans, this goal may be more easily achieved by ensuring vaccines are properly tracked. At every part of the vaccination pipeline, stakeholders should know how many doses they’re getting and when. Shipments should be predictable, and appointments should be easily managed, freeing up public health workers’ time to take on the important task of actually vaccinating people.
It also bears mentioning that Pfizer will now be shipping out fewer vaccine vials to account for the “surprise 6th dose” that providers are often able to get out of each vial—since Pfizer charges by the dose. It is unclear whether this reduction in dose availability will affect the rollout.
One piece of good news, on the vaccination data front: the CDC vaccination tracker stepped up its reporting to include weekend updates, as of yesterday. But the agency still isn’t reporting demographic data, comprehensive data on long-term care facilities, or even a time series of doses administered per day. Vaccination tracking has a long way to go.
Following the end of the federal public health emergency in May, the CDC has lost its authority to collect vaccination data from all state and local health agencies that keep immunization records. As a result, the CDC is no longer providing comprehensive vaccination numbers on its COVID-19 dashboards. But we still have some information about this year’s vaccination campaign, thanks to continued CDC efforts as well as reporting by other health agencies and research organizations.
This week, the FDA authorized Novavax’s updated COVID-19 vaccine. Here’s why some people are excited to get Novavax’s vaccine this fall, as opposed to Pfizer’s or Moderna’s.
Shortly after President Joe Biden’s inauguration, the official White House website got a makeover. It now hosts the president’s priorities and COVID-19 plan—including a promise to create a “Nationwide Pandemic Dashboard.”
Create the Nationwide Pandemic Dashboard that Americans can check in real-time to help them gauge whether local transmission is actively occurring in their zip codes. This information is critical to helping all individuals, but especially older Americans and others at high risk, understand what level of precaution to take.
We don’t have a clear timeline for this dashboard yet, of course, much less details on what it will include. But the foundation was laid this week: Biden released a detailed national COVID-19 plan and signed 30 executive orders—three of which are directly related to tracking the pandemic.
In the coming weeks, I’ll be closely watching to see how the Biden administration follows through on these plans. Will the new administration build on the strengths of existing federal and state data systems, or will it tear down old systems and sow unnecessary confusion?
What Biden is promising:
A Nationwide Pandemic Dashboard: We covered this one already. Biden’s national strategy document specifies that the federal government will track cases, testing, vaccinations, and hospital admissions—and will “make real-time information available.” The “real-time” promise here is worth highlighting, as real-time pandemic data do not actually exist; every metric from cases to vaccinations has its own lag based on reporting and data-sharing technologies. (COVID-19 deaths, in particular, may be reported weeks after they occur.) Still, the federal government is already tracking all of these metrics. The Biden team’s goal, then, is to consolidate them into an easily accessible dashboard that is widely used by everyone from county public health leaders to elementary school teachers.
Coordinated federal data collection: One of Biden’s executive orders, signed on January 21, requires several federal agencies to “designate a senior official” who will lead that agency’s COVID-19 data collection. The officials must both coordinate with each other and make data public. Meanwhile, the Department of Health and Human Services secretary will review the national public health data systems and figure out how to increase their efficiency and accuracy. (Xavier Becerra, Biden’s pick for HHS secretary, hasn’t been confirmed by the Senate yet; will this review need to wait until he officially starts the position?)
A focus on equity: Another Biden executive order promises to address the disproportionate impact that COVID-19 has had on people of color and other minority communities. The executive order specifically calls out a lack of standardized COVID-19 data on these communities, saying this data gap has “hampered efforts to ensure an equitable pandemic response.” Biden’s COVID-19 Health Equity Task Force will be required to address this data gap by coordinating with federal agencies—both expanding data collection for underserved populations right now and making recommendations to prevent this issue in future public health crises. This task is easier said than done, though; a recent STAT News article called using data to ensure vaccination equity one of the biggest challenges Biden faces as he takes office.
School data collection: Last week, I wrote that there was no mention of data-gathering in Biden’s K-12 COVID-19 plan. Well, maybe someone from his team reads the COVID-19 Data Dispatch, because his executive order on supporting school reopening requires data collection in two areas: data to inform safe reopening of K-12 schools, and data to understand the pandemic’s impact on students and educators. I would have liked to see a more specific promise to track COVID-19 cases, tests, and student enrollment in public schools, but this is a good start.
Data-based briefings: Jen Psaki, the new White House press secretary, said on Wednesday that the administration would hold regular briefings with health officials, “with data.” Ideally, such briefings should explain trends in COVID-19 data and put numbers into context for the Americans watching at home.
The promises are, well, promising. And I’m rooting for President Biden! Seriously! My job would be way easier if I could just give you all updates using one centralized dashboard each week. But I’ve spent enough time hacking through the weeds of this country’s highly confusing, irregular data systems to know that the new president can’t just flip a switch and make a nationwide pandemic dashboard magically appear on whitehouse.gov.
If anyone from the Biden administration is reading this, hello! Please put me on all your press lists! And here’s what this data reporter would, personally, like to see you focus on.
What I want to see:
Don’t break what we already have: Or, build on the existing federal data systems (and dashboards) rather than creating something entirely new. Last week, Alexis Madrigal published a feature in The Atlantic advocating for the new administration to keep COVID-19 hospitalization data under its current HHS control rather than transferring this responsibility back to the CDC. I’ve covered the HHS’s hospitalization data extensively in the CDD, but this feature really paints a cohesive picture of the dataset—from its turbulent, politically charged beginnings to its current, comprehensive, trustworthy format. The story is worth a read. And on a similar note, I’ve been glad to see federal data sources like the CDC’s dashboard and the Community Profile Reports, continue to update on their usual schedules. Biden’s team should seek to improve upon these systems and make them easier to access, not start from scratch.
More public metadata: When the federal government has put out large data releases in recent months, responsibility has largely fallen on journalists and other outside communicators to make those releases accessible. I’ve done some of that work in this publication and at the COVID Tracking Project. But it shouldn’t really be my job—the federal agencies that put out these datasets should be releasing FAQ documents, holding press calls, and generally making themselves available to help out researchers and communicators who want to use their data.
Count the rapid tests: Since August, I’ve called on the federal public health agencies to release national data on antigen tests and other types of rapid tests. A recent article in The Atlantic by Whet Moser makes clear that data for these tests are still widely unavailable. Moser writes that antigen test numbers are not reported at the federal level, and at the state level, such reporting is highly fractured and inconsistent; as a result, about three-quarters of the antigen tests that the federal government has distributed are unaccounted for in public data. The HHS should focus on tracking these tests as comprehensively as it has tracked PCR tests, and it should make the numbers publicly available.
Survey the genomes: Another massive challenge that the U.S. faces right now is keeping track of the SARS-CoV-2 variants that are circulating through the population, some of which may be more contagious or more life-threatening. As Sarah Braner reported two weeks ago, the majority of COVID-19 cases aren’t genomically sequenced, making it difficult for us to know how many of those cases are new strains as opposed to the regular coronavirus that we’ve all come to know and hate over the past year. Biden’s health and science leadership should make it a priority to step up the nation’s genetic sequencing game, and all of those data should be publicly shared.
Support the local public health agencies: Nationwide data coordination is obviously important, and is something that’s been desperately needed since last spring. But most of the COVID-19 data work—logging test results, standardizing those test results, sending them to a central location—is done by state and local public health officials. Local public health agencies, in particular, have been under-funded and threatened by partisan policies since before the pandemic started. To truly improve COVID-19 data collection, the Biden administration must provide support to these local agencies in the form of funding, personnel, technology, and truly anything else they need right now.
When Biden’s nationwide pandemic dashboard does drop, you’d better believe I’ll be giving it a comprehensive review. For now, if you want to see how well Biden’s doing at keeping his campaign trail promises, I recommend checking out Politifact’s Biden Promise Tracker.
In the past week (January 17 through 23), the U.S. reported about 1.2 million new cases, according to the COVID Tracking Project. This amounts to:
An average of 173,000 new cases each day
370 total new cases for every 100,000 Americans
1 in 270 Americans getting diagnosed with COVID-19 in the past week
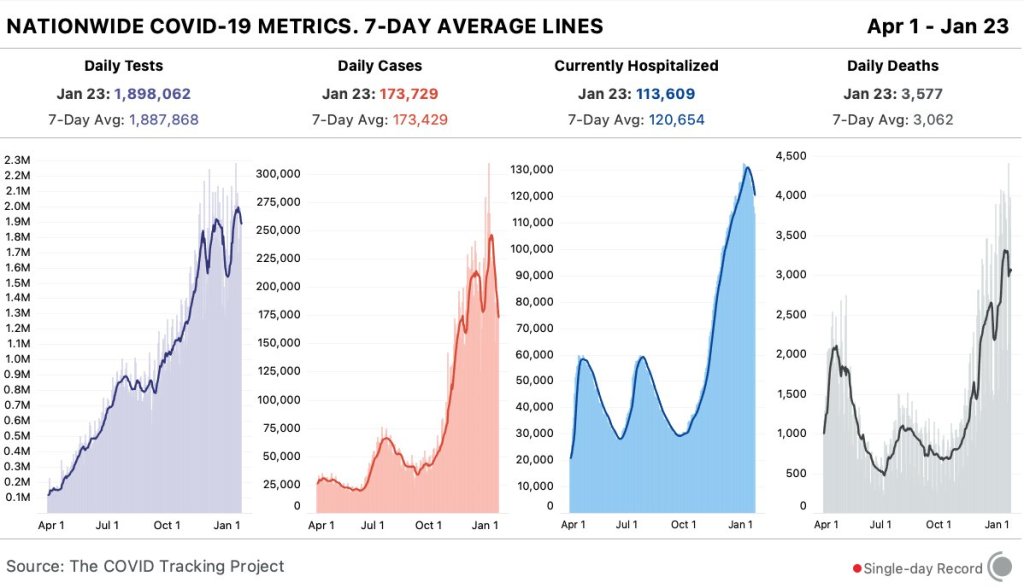
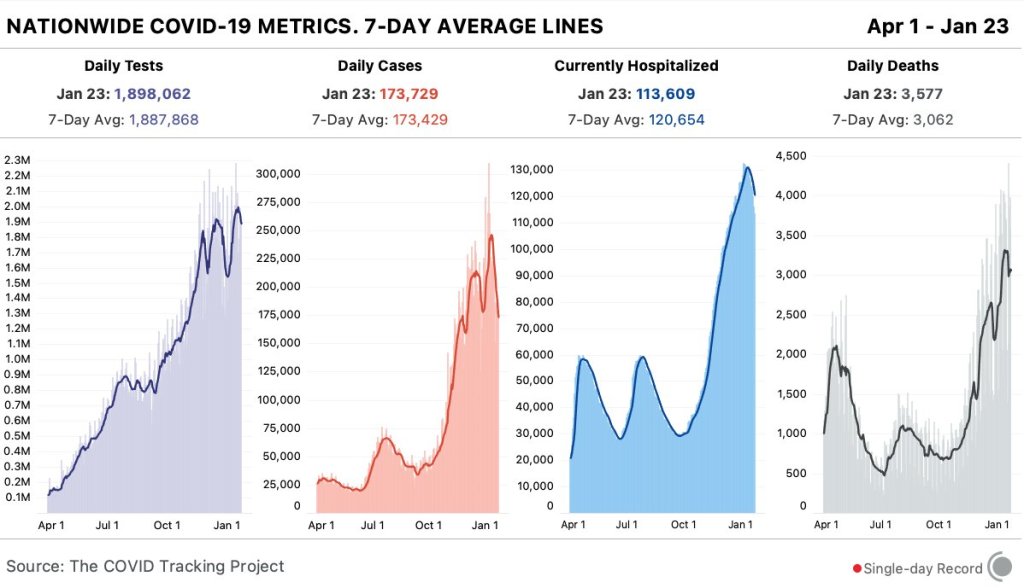
Nationwide COVID-19 metrics published in the COVID Tracking Project’s daily update on January 23. New daily cases and current hospitalizations are steadily dropping, but deaths are still over 3,000 each day.
Last week, America also saw:
113,600 people now hospitalized with COVID-19 (35 for every 100,000 people)
21,400 new COVID-19 deaths (6.5 for every 100,000 people)
Two major metrics, new cases and current hospitalizations, are down for the second week in a row. (See the numbers trending down on the COVID Tracking Project chart, above.) The number of new cases reported this week is the lowest it’s been since Thanksgiving. And, while well over 100,000 Americans are in the hospital with COVID-19, we are seeing about 17,000 fewer patients nationwide than we did two weeks ago.
A decline in COVID-19 cases sweeping the nation, backed by concurrent declines in COVID-19 hospitalizations. We may already be beyond the peak of this virus. https://t.co/vtUWyKSVTz
6-month consequences of COVID-19 in patients discharged from hospital (Huang et al., The Lancet): I don’t usually feature scientific papers here, but this new study is important. It’s the biggest paper so far on COVID-19 long haulers, those patients who struggle with the disease for months after their diagnosis (or after not getting a diagnosis at all). This study followed about 1,700 patients over 6 months.
Global.health COVID-19 dataset: Global.health describes itself as a “global data repository and visualization platform that enables open access to real-time epidemiological anonymized line list data.” Its COVID-19 dataset—which promises information on 5 million anonymized cases—is not yet published, but is definitely a source to look out for.
COVID-19 survey of Medicare beneficiaries: This week, the Centers for Medicare & Medicaid Services published results of a survey of Medicare beneficiaries, focused on their experiences with COVID-19. The data include American seniors’ perceptions of vaccines, perceptions of COVID-19 safety, care experiences, and more.
The COVID-19 Data Dispatch largely focuses on U.S. news. This country’s response to the pandemic has been so chaotic and confusing that it is a full-time job just to keep up with major developments. But sometimes, to truly understand COVID-19 in America, we need a global perspective. More specifically: seeing how other nations have succeeded in mounting a robust public health response—with actual support from the public—can show us how we have failed.
I got the opportunity to gain that perspective this week, by attending the (virtual) Futures Forum on Preparedness, hosted by tech nonprofit Schmidt Futures. At the forum, a diverse group of health, science, and policy leaders presented research on the global COVID-19 response and discussed how to better prepare for future public health crises.
One cornerstone of the forum was a comprehensive comparison of how 23 countries responded to COVID-19. Researchers at the Harvard Kennedy School, Cornell University, and other partners—including teams in each of the 23 countries—analyzed politics, policies, and social conditions in order to figure out what actually constitutes success in protecting a nation’s citizens from a public health threat.
The researchers classified countries into three major categories: control, consensus, and chaos. A nation in control exhibits public health authority—uncontested by political leaders or the general public—to actually contain the coronavirus (with border controls, contact tracing, etc.) without needing to disrupt daily life. A nation in consensus exhibits cooperation between the political system and the public health system, with citizens agreeing to some disruptions in their lives in order to more broadly keep people safe and keep the economy working. A nation in chaos fails to heed public health advice, fails to find agreement between political parties, and fails to preserve overall public safety at the expense of individual freedoms.
Speakers at the Forum provided examples for each category: Taiwan is a nation in control, Germany is a nation in consensus, and as for chaos… of course it’s the U.S. (Brazil, India, Italy, and the U.K. also fall into the chaos category.)
Now, some particularly nerdy readers might remember an index touted last winter, when we were just beginning to recognize the gravity of the threat posed by COVID-19. The 2019 Global Health Security Index bills itself as “the first comprehensive assessment of global health security capabilities in 195 countries.” It rates nations based on their ability to prevent public health threats, set up epidemiological surveillance, communicate risk, give citizens access to healthcare, and other similar metrics.
The U.S. is ranked number one. It seems laughable now, right? All the measures that were supposed to help us deal with these crises—our monitoring systems, our highly trained scientific workforce, our massive national GDP—have completely failed in the face of partisan fighting and a broad lack of trust in public health measures.
I remember hearing about this index at the American Association for the Advancement of Science last February, what seems like a million years ago. I pitched a story on the index to my colleagues at Stacker—we could rank countries on how prepared they are for this new coronavirus, I thought. My boss questioned the pitch, saying that the index was entirely prospective and couldn’t predict how countries would actually respond. Plus, the U.S. had already started to fuck up, via the complete lack of testing and the Trump administration downplaying how severe a threat COVID-19 might pose. We did not produce the story. (Sam, if you’re reading this: thank you.)
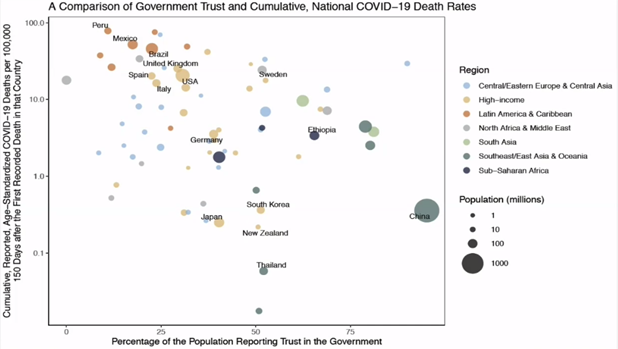
America was supposed to be great at this, but we failed. That’s not really news. I like the Comparative Covid Response report, though, because it highlights this failure in stark, neon lighting—and tells us exactly what we need to improve on, systematically, before the next crisis hits. At their Futures Forum on Preparedness talk, the researchers behind this report showed that a nation’s score on the Global Health Security index doesn’t correlate at all to the nation’s COVID-19 death rate. But then, they showed one property that does correlate: trust in the government.
Figure from presentation at the Futures Forum on Preparedness.
Countries where people actually trusted their governments to provide public health guidance, such as Thailand, New Zealand, and Germany, were able to institute those control or consensus measures I mentioned earlier and prevent widespread tragedy while keeping the basic functions of the country going. The U.S. needs to get to this point if we are to actually take advantage of all our money and resources in response to future public health crises.
One last note: I have to give credit to the Global Health Security index where credit is due. They did get one ranking right—the U.S. scored only 25 (of 100) points for healthcare access, ranking at 175 of 195 nations.
Every week, I come into your inbox and I say, the vaccine rollout is going badly. And you’re probably like, yeah, Betsy, I know, it’s on the news every single day.
You probably don’t need me to tell you about the announcement this past Tuesday, from Health and Human Services Secretary Alex Azar, telling states to stop saving their second doses and start prioritizing all adults over the age of 65… or the Washington Post scoop this past Friday, revealing that states couldn’t actually vaccinate more people because the federal vaccine reserve was already used up. (I salute all the policy reporters following this madness. Seriously.)
So instead, today, I’m focusing on a vaccination issue that hasn’t gotten as much press: who is actually getting vaccinated? On the national level, we largely can’t answer this question, thanks to a lack of demographic data.
While the CDC’s vaccination tracker has seen some upgrades recently (such as the inclusion of people receiving two doses and downloadable data), it does not report any information on the race, ethnicity, age, gender, or occupation of those Americans who have gotten shots. And the data aren’t much better at the state level, according to recent analysis from the COVID Tracking Project.
The COVID Tracking Project analysis discusses 17 states which report race and/or ethnicity data for vaccine recipients. Since the post was published, two more states—Missouri and West Virginia—have started reporting such data. Still, just reporting these data isn’t sufficient. Alice Goldfarb, Kara Schechtman, Charlotte Minsky, and other Project volunteers who compiled detailed annotations on the vaccine metrics reported by each state found that, even when states do report demographic data, each state uses vastly different categories, making it difficult to compare or combine this state-level information into a useful national dataset.
Using the limited data that are available, though, we can still see that the vaccination effort thus far is incredibly inequitable—despite government promises to prioritize vulnerable populations.
White Americans are getting vaccinated at much higher rates than Black Americans, according to a Kaiser Health News analysis of state data published yesterday. Reporters Hannah Recht and Lauren Weber discuss access issues and mistrust of the healthcare system—tied to systematic racism against Black Americans seeking healthcare—as reasons why Black Americans may be left behind.
But the disparities so far, at a stage of the vaccine rollout that has largely prioritized healthcare workers, means that both national and local public health agencies have a lot of work to do:
“My concern now is if we don’t vaccinate the population that’s highest-risk, we’re going to see even more disproportional deaths in Black and brown communities,” said Dr. Fola May, a UCLA physician and health equity researcher. “It breaks my heart.”
In New York—a state which finally released a vaccine dashboard today, but is not yet reporting demographic data—vaccination trends by hospital suggest a similar pattern. The hospitals with the highest shares of vaccinated workers are, by and large, private hospitals located in Manhattan. The hospitals with fewer vaccinated workers, on the other hand, include those located in Harlem, Brooklyn, and other working-class neighborhoods.
Data are also lacking for long-term care facilities. The CDC reports total vaccine doses administered in these facilities (which include nursing homes, assisted living facilities, and other care homes). But a national total is unhelpful in analyzing where states have been most successful at getting vaccines to this high-priority population. A COVID Tracking Project analysis, published on Thursday, found vaccine data for LTCs in only seven states. South Carolina is the only state releasing detailed data on individual facilities.
Meanwhile, CVS has published a state-by-state dataset of LTC vaccinations administered by this pharmacy chain. The COVID Tracking Project reports that Walgreens may release a similar dataset. It seems pretty wild that independent pharmacy chains are reporting more detailed vaccine data than the federal government itself—until you remember, well, how data reporting has gone this entire pandemic.
Vaccination data, right now, are about as messy as testing data were back in spring 2020. Every state is doing its own thing, and the federal government has yet to provide sufficiently detailed information for meaningful analysis. Readers: I urge you to push for better vaccine demographic data, both in your own region and nationally.
The COVID-19 Vaccine Communication Handbook is a new resource from communication initiative SciBeh aimed to help journalists, healthcare workers, and other communicators talk about COVID-19 vaccines and challenge misinformation.
Following the end of the federal public health emergency in May, the CDC has lost its authority to collect vaccination data from all state and local health agencies that keep immunization records. As a result, the CDC is no longer providing comprehensive vaccination numbers on its COVID-19 dashboards. But we still have some information about this year’s vaccination campaign, thanks to continued CDC efforts as well as reporting by other health agencies and research organizations.
This week, the FDA authorized Novavax’s updated COVID-19 vaccine. Here’s why some people are excited to get Novavax’s vaccine this fall, as opposed to Pfizer’s or Moderna’s.
!function(){“use strict”;window.addEventListener(“message”,(function(a){if(void 0!==a.data[“datawrapper-height”])for(var e in a.data[“datawrapper-height”]){var t=document.getElementById(“datawrapper-chart-“+e)||document.querySelector(“iframe[src*=’”+e+”‘]”);t&&(t.style.height=a.data[“datawrapper-height”][e]+”px”)}}))}();
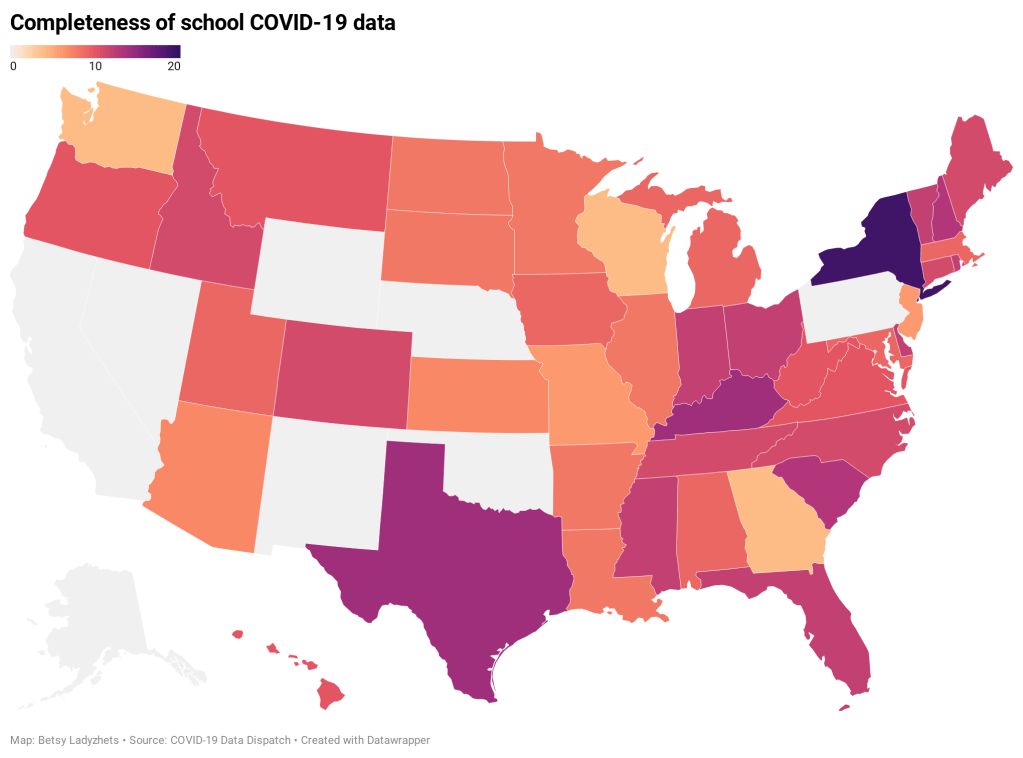
K-12 schools across the country are open for the spring semester, even as America faces serious outbreaks in almost every state and a more contagious strain—more contagious for both children and adults—begins to spread. At the national level, we are still overwhelmingly unable to track how the virus is spreading in these settings.
Perhaps the most newsworthy opening this week was in Chicago, where students returned to classrooms for the first time since last March. Chicago’s teachers union has waged an ongoing battle with Mayor Lori Lightfoot and district CEO Janice Jackson, whom teachers claim have not resolved ongoing safety issues in school buildings. The district is screening staff through optional rapid tests once a month; about 1,200 tests have been reported so far, including three positive results. Four Chicago students and 34 other staff members reported COVID-19 cases this week.
Meanwhile, President-elect Joe Biden announced a $175 billion plan aimed at getting students back to in-person learning. The plan includes $35 billion for higher education and $130 billion for public K-12 schools, with a focus on increasing testing, PPE for students and teachers, ventilation, and other safety measures for which educators have been calling since last spring.
Biden hopes to open “the majority of K-8 schools,” according to Education Week’s Evie Blad. A recent report by the CDC suggests that in-person learning for these younger students, when implemented safely, is not likely to seed an outbreak in the wider community. (College-aged students in the 18-24 range are more likely to cause such outbreaks.)
The report says: “CDC recommends that K–12 schools be the last settings to close after all other mitigation measures have been employed and the first to reopen when they can do so safely.”
But, as Blad points out, it will be difficult to track the impact that more school reopening would have on broader communities, as data on COVID-19 cases in schools are still limited and fractured. There is still no federal dataset on COVID-19 in American public schools. State datasets are fully unstandardized; and most states only report case counts, making it difficult to actually analyze how school outbreaks compare across schools.
As of our most recent K-12 state annotation update, only Delaware, New York, and Texas are providing enrollment numbers, and only New York is providing testing numbers. (Thank you to intern Sarah Braner for doing the update this week!)
In last week’s recommended reading section, I featured an op ed in Nature by school data leader Emily Oster calling on President-elect Biden to develop a unified, national system for tracking COVID-19 in schools. I wanted to highlight it again this week because I absolutely agree with Oster here. As important as her and others’ compilation efforts have been in filling the school data gap, no outside dashboard can replace the work of the federal government:
We need to be able to identify the virus spreading in schools and work out what went wrong. The data we do have suggest that outbreaks in schools are not common, but they do happen. We need a way to find them systematically.
And here’s one more school-related metric we should be tracking: teachers are starting to get vaccinated. According to a recent Kaiser Family Foundation analysis of state vaccination priority groups, 31 states have put K-12 and childcare personnel in their Phase 1 group. In Utah, teachers and childcare workers are even included in Phase 1A. California and New York, two of the biggest states, started vaccinating teachers this past week.
(If you want a heartwarming read this long weekend, I recommend this piece from THE CITY that profiles NYC teachers and other essential workers getting vaccinated in the middle of the night.)
But most states are barely reporting basic demographic data for their vaccinations, much less telling the public the occupations of those who have gotten shots. Without knowing how many teachers have been vaccinated, it will be difficult to factor these inoculations into reopening decisions—or determine how vaccination impacts future school outbreaks.