This past week, the Centers for Disease Control and Prevention (CDC) released a long-awaited guidance on school reopening.
While the CDC isn’t able to actually regulate what schools do, many state and local leaders look to the agency for advice on how to best follow the available scientific evidence. And, if you’ve been following the reopening debate, you know that there are a lot of differing opinions on how to best follow the available scientific evidence. Pro-opening advocates hoped to see the CDC strongly insist that schools go in-person, perhaps with limited cleaning and allowing less than six feet of distancing. Pro-closure advocates hoped to see the agency insist that teachers needed to be vaccinated before they could go back to their classrooms.
Rather than strictly advocating for either closed or open classrooms, however, the guidance takes a moderate route. It emphasizes three strategies already familiar to school leaders: layering different COVID-19 protection methods (masks, distancing, ventilation, and so on); looking at COVID-19 cases in the surrounding community to determine whether it’s safe for you to open; and having multiple opening “phases” available depending on community safety. Frequent testing and vaccinations of school staff are included as “additional” options, which the CDC suggests schools should employ if they have the resources.
New York Times reporter Apoorva Mandavilli, who has covered the epidemiological questions around reopening, wrote a Twitter thread that further explains why this is a moderate route:
My big question of this guidance, though, was: what does this mean for data? As we’ve written in the CDD before, the Biden administration has the opportunity to correct a longstanding failure of its predecessor. Under Biden, national public health leadership could require that all public schools report their case counts, testing numbers, and enrollment numbers to the federal government—and publish these figures in a systematic way. But the new CDC guidance largely retains the status quo for school COVID-19 data.
“Every COVID-19 testing site is required to report to the appropriate state or local health officials all diagnostic and screening tests performed,” the guidance says. This requirement has been in place since last spring. Similarly, the CDC says that school administrators should notify parents, teachers, and staff when cases are reported—again, such internal reporting systems are already in place.
But there’s no mention of making these data public. The CDC is not promising a national school data dashboard, or even requiring state and local public health departments to put their data up on a portal with the rest of their COVID-19 figures.
You’d think that state and local agencies wouldn’t need such a push, over a year into the pandemic. But, as we’ve reported in the CDD before, the vast majority of states currently fail to publish K-12 COVID-19 data in a way that makes it possible to actually track transmission rates in schools.
While 34 states and D.C. regularly report counts of COVID-19 cases that have occurred in schools, 16 states report incomplete data—or no data at all. And for the states that do report case counts, most don’t report enrollment numbers, making it difficult to discern whether the virus is impacting a single family or running rampant in a school. (Four cases in a school with 4,000 kids in classrooms, for example, is vastly different from four cases in a school with 100 kids in classrooms.)
New York continues to be the model state for K-12 data, as it’s one of only four to report enrollment numbers and the only state to report school-specific testing numbers. As the CDC seems to consider systematic school testing “optional,” it seems likely that this will continue.
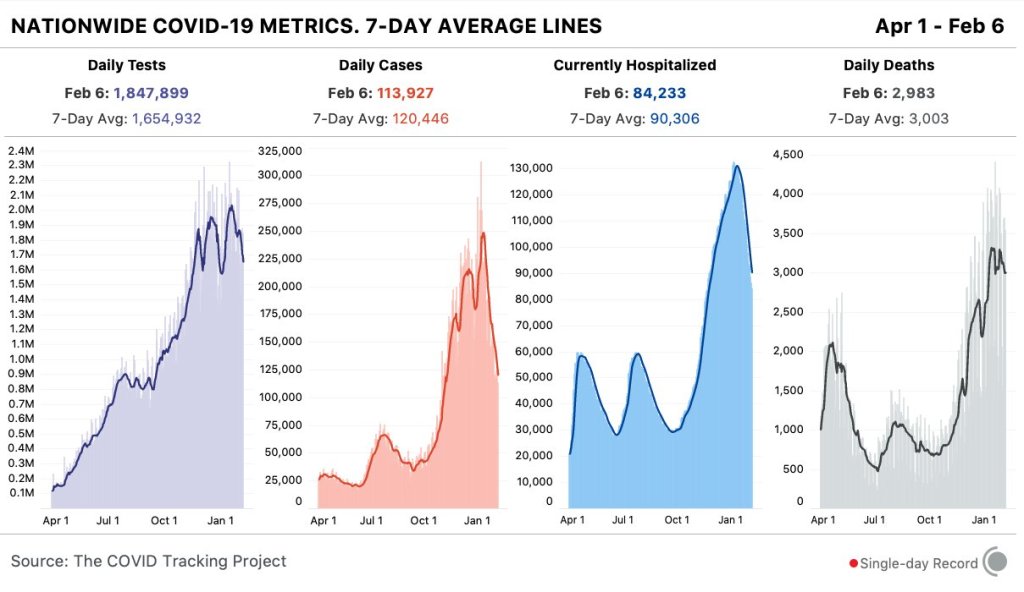
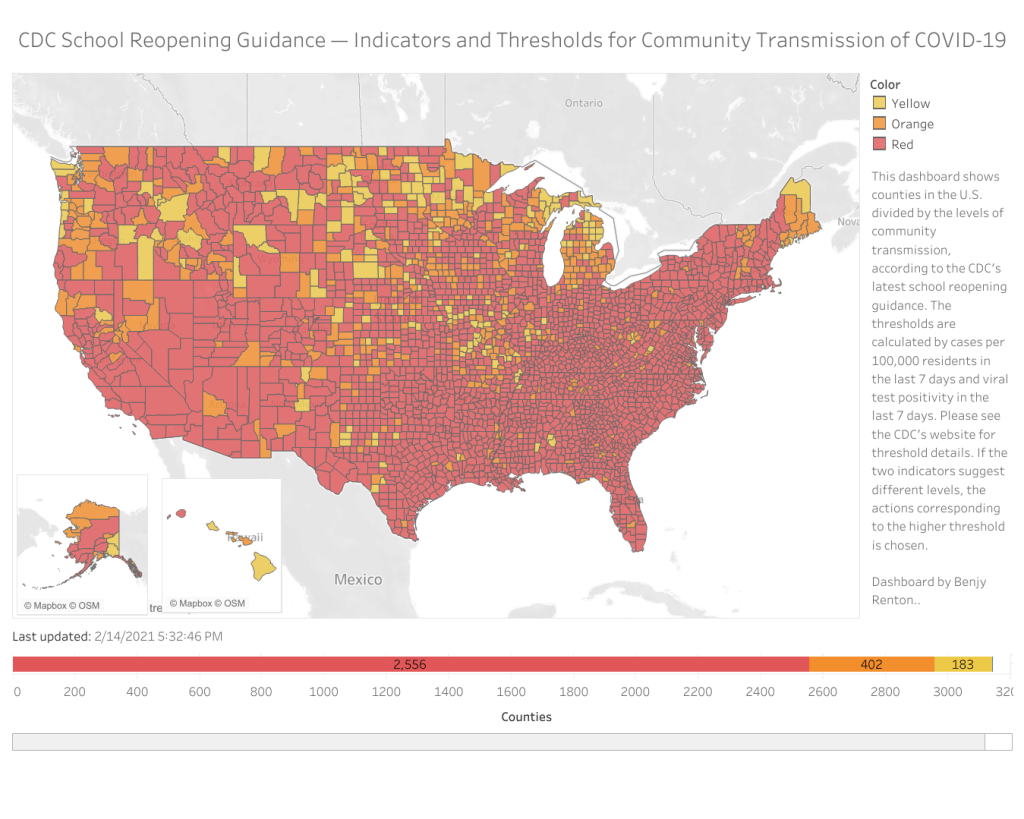
We can see that most counties in the U.S. have high enough community transmission rates—or, COVID-19 cases in the general public—that the CDC’s new guidance would categorize them as being in the “red zone,” a.k.a. too dangerous for schools to be open. But without case numbers for schools themselves, reported in a standard way, it’s hard to know whether the CDC’s assessment is accurate.
School data continues to be a massive gap in America’s pandemic tracking. Readers, I urge you to see what data are available for your state, county, and district—and push your local officials to be more transparent.
Dashboard by Benjy Renton.
Related posts
- COVID-19 school data remain sporadicOn November 18, New York City mayor Bill de Blasio announced that the city’s schools would close until further notice. The NYC schools discrepancy is indicative of an American education system that is still not collecting adequate data on how COVID-19 is impacting classrooms—much less using these data in a consistent manner.