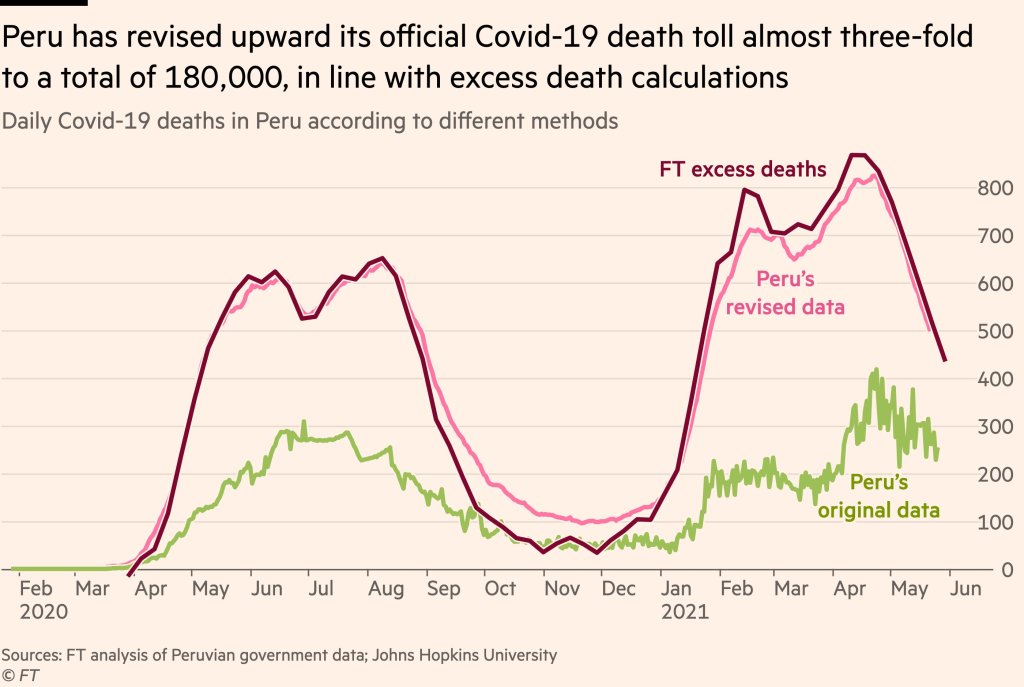
Peru’s revision led the country’s official death count to match its estimated excess deaths. Source: Financial Times..
Excess deaths are those deaths that occur above a region’s past baseline. Data scientists calculate the metric by determining the average deaths for a country or region over a period of several years—then comparing this past average to the deaths that occured in the current year.
The deaths occurring in the current year above that past average are the excess deaths. In New York City during the spring 2020 surge, for example, about four times more people were dying each week compared to the same time period in previous years.
During the pandemic, excess deaths have become a useful way for scientists to estimate the true toll of COVID-19. Especially during the earlier months of 2020, limited access to testing meant that many people who became infected with the coronavirus were not able to get the positive test required for their illness (or death) to actually be counted as a case. (In the U.S., this recording gap is currently causing issues for families who lost loved ones to COVID-19 early in the pandemic and are now seeking federal aid.)
Plus, the pandemic caused hospital systems to shut down and inspired widespread hesitancy for anyone seeking medical care for a non-COVID reason. The death of someone who had a heart attack and couldn’t get a hospital bed because of COVID-19, for example, is not a COVID-19 death but was undoubtedly caused by the pandemic.
Excess deaths, as a metric, allow researchers to see how the pandemic has impacted a country or region—above the official COVID-19 death counts. And a recent audit from Peru provides new evidence for this metric’s value.
The country essentially audited its COVID-19 deaths data to address undercounting. Government officials checked thousands of death certificates from 2020, and added any COVID-related deaths to past totals—which previously only included those Peruvians who had positive PCR tests.
After the audit was complete, Peru’s COVID-19 death toll rose by almost three times—to 180,000 deaths. The country now has the highest official death rate in the world: one in every 177 people.
When plotted over time, Peru’s revised death data match closely with its excess deaths, as calculated by the Financial Times data team. This audit—and its match with excess deaths—shows that excess deaths do, in fact, show the true toll of COVID-19 in a country.
It’s also notable as the first time a country has done such an audit on a wide scale. Some states (such as Washington) have added COVID-19 deaths to their official counts periodically, as they process death certificate backlogs, but none have done anything on Peru’s level.
Future death certificate audits and excess death analyses may help us understand the true toll COVID-19 has taken on the U.S. and the world.
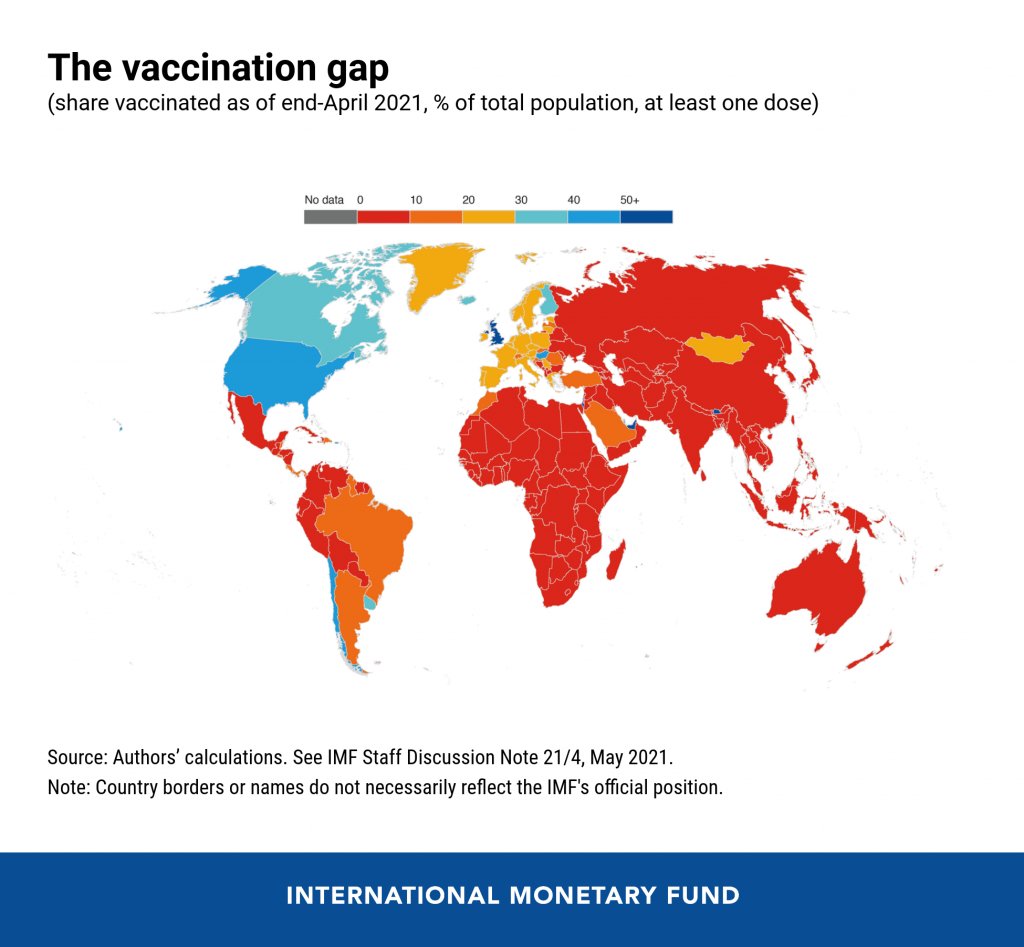
In the reader survey I sent out a few weeks ago, I asked, “What is one question you have about COVID-19 in the U.S. right now?” One reader responded with an inquiry into vaccine equity: “What will it look like when the U.S. is ‘open’ and vaccinated and many other parts of the world are not?”
That question feels especially relevant this week. On Thursday, the Biden administration made a big (and long-awaited) announcement: the federal government is sending 25 million vaccine doses from America’s stockpile to other countries. The administration has previously promised to send at least 80 million doses abroad by the end of June, but this week’s announcement included more details—such as countries that will receive these initial doses and other logistics.
Out of the 25 million, about 19 million doses are going to COVAX. COVAX, a global effort run by the World Health Organization and other international government bodies and philanthropic organizations, brings vaccines to low-income nations at no cost. The COVAX doses will go to India, other parts of Asia, Central and South America, and Africa, Bloomberg’s Josh Wingrove reports.
The remaining 6 million doses will be sent directly to countries, including Ukraine, Kosovo, Haiti, Georgia, Egypt, Jordan and Iraq. Some doses are going directly to India as well—while the worst of this nation’s surge may be over, it’s still facing high case counts, full hospitals, and a terrifying “black fungus” linked with the Delta variant (B.1.617).
At first glance, this might seem like a noble move on the Biden administration’s part. The U.S. is seeing low case numbers and widespread reopenings, so we can share some supplies to “help the pandemic around the globe,” as COVID-19 response coordinator Jeff Zients said at a briefing on Thursday.
But 25 million doses—or even the 80 million doses that the administration has promised by the end of this month—is a drop in the bucket compared to actual international needs. For example: COVAX needs 1.8 billiondoses to vaccinate about half the adult population in low-income countries. COVAX has specifically prioritized 92 low-income nations, representing a total population of 3.8 billion.
That 1.8 billion dose number is a highlight of a major report released last week by the Rockefeller Foundation, a global charitable foundation, discussing what it would take to vaccinate the world. I covered the report for Science News. According to this report, Gavi (the Vaccine Alliance), an international public-private body that runs COVAX, needs to raise $9.3 billion in order to pay for those 1.8 billion doses. Gavi has been working to raise this money from countries and independent donors at a global health summit this past week.
While $9.3 billion might seem like a massive price tag, the cost of failing to provide these vaccines would actually be far greater. The global economy may lose up to $9.2 trillion if richer nations fail to support equitable vaccine distribution, according to an estimate from the International Chamber of Commerce.
So far, the U.S. has administered about 300 million vaccine doses (as of yesterday), covering over half the total population. In a number of low-income countries, less than one percent of the population has received a dose. Tedros Adhanom Ghebreyesus, Director General of the WHO, said at a recent assembly that, if all doses administered globally had been sent out equitably, the doses would have covered “all health workers and older people.” Instead, high-income nations are largely protected while low-income nations are vulnerable to future surges and highly-transmissible variants.
Through this lens, the 25 million dose shipment announced this week is far from impressive. It’s a useful start, certainly, but it’s not going to end the pandemic anywhere. Even the 80 million doses promised by the end of June is a tiny number—about 4% of the doses COVAX is hoping to obtain. It’s also only 11% of the doses that vaccine makers have pledged to deliver to the U.S. by the end of July, according to Bloomberg.
That larger June shipment has also been held up because the Biden administration is planning to send AstraZeneca vaccines—which are under review from the FDA because they were produced at the Emergent factory that infamously wasted millions of Johnson & Johnson doses. The AstraZeneca vaccine is not authorized for use in the U.S., so of course it will make up the majority of the doses we send abroad this summer.
Speaking of unused doses: the Biden administration may also start sending unused doses from states to other countries, POLITICO reported this week. The administration wants to get thousands of Pfizer, Moderna, and J&J doses—on the verge of expiring—to countries that would actually use them. While this possible policy hasn’t yet been realized, it hammers home a clear message: the U.S. will donate “unwanted” vaccine doses only when we are absolutely certain that we don’t need them here.
Now, let’s return to our reader’s question. What happens when the U.S. is safely vaccinated, but other parts of the world aren’t?
From a health standpoint, the U.S. will probably be okay. The vaccines are very effective, even against variants—likely protecting the country from another major surge. We will need careful surveillance to guard against future variants that may evolve beyond the vaccines (see: last week’s issue), and it’s possible that overly zealous reopening this summer will lead to outbreaks next fall and winter. But seniors and other vulnerable people would be more protected than they have been in past surges, and booster shots (for the variants) will likely be on their way soon. In short, America’s wealth will protect us.
Around the world, however, outbreaks will continue. Every time a new person gets infected with the coronavirus, the virus has a new opportunity to mutate. And with every mutation, the virus learns to spread faster, to evade common treatments, even to evade vaccines. Thanks to globalization, as long as the virus is a threat anywhere, it continues to be a threat everywhere.
Plus, as low-income nations suffer from continued outbreaks, the global economy will continue to suffer. Out of that $9.2 trillion cost estimated by the International Chamber of Commerce, the majority will likely fall on wealthier nations (like the U.S.) that rely on other countries for products and labor.
“The pandemic itself has gone beyond a health crisis — it has now gone into an economic crisis,” Christy Feig, the Rockefeller Foundation’s director of communications and advocacy, told me when I spoke to her for Science News. “The only way to unchoke the economy is by getting the vaccines to as many countries as possible, so that we can stop the spread of the disease before more variants come.”
In the past week (May 29 through June 4), the U.S. reported about 100,000 new cases, according to the CDC. This amounts to:
An average of 14,000 new cases each day
31 total new cases for every 100,000 Americans
35% fewer new cases than last week (May 22-28)
Last week, America also saw:
18,000 new COVID-19 patients admitted to hospitals (5.5 for every 100,000 people)
2,300 new COVID-19 deaths (0.7 for every 100,000 people)
70% of new cases in the country now B.1.1.7-caused (as of May 8)
An average of 1 million vaccinations per day (per Bloomberg)
Cases continued to fall this week, with a seven-day average now under 20,000 new cases a day. This is basically the lowest number we’ve seen in the U.S. since spring 2020—though it’s important to note that the U.S. was doing minimal testing at that time, so the true case numbers in March 2020 were likely much higher than what was reported.
Also, last weekend’s holiday—like past holidays—likely resulted in fewer cases being reported early this week. Many testing sites and public health departments close for holidays, and it’s hard to imagine who might want to go get a nose swab on Memorial Day. Fewer than 10,000 new cases were reported last Monday and Tuesday, according to the CDC, followed by double that number each day for the rest of the week.
Despite such low overall case numbers, infection rates remain high for the unvaccinated. A recent Washington Post analysis adjusted COVID-19 infection rates by subtracting vaccinated residents from state populations. In Washington state, for example, the case rate among unvaccinated residents is “as high as it was in late January.”
Also, as policy researcher Julia Raifman pointed out on Twitter, fewer than half of the lowest income workers with kids are vaccinated—likely because of vaccine accessibility issues. Workers in this income bracket are also more likely to report that they had to miss work due to a COVID-19 infection, compared to higher-income Americans.
Nationwide, about half of the U.S. population has had at least one dose, including 63% of adults and 86% of seniors. The rate of vaccinations has slowed this past week (now only one million doses administered a day)—though this may in part be a holiday reporting lag as well. Biden’s administration continues throwing incentives at the problem in the hopes of meeting his July 4 goal.
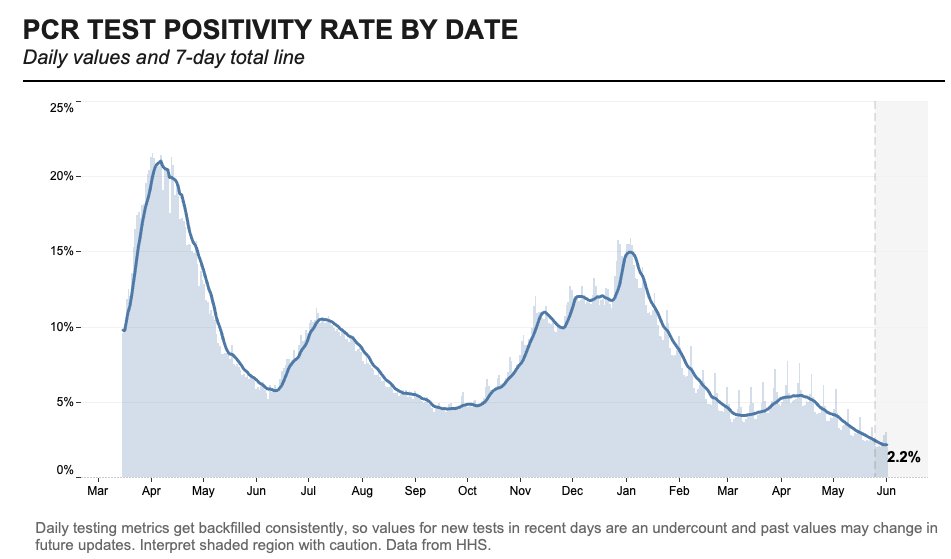
Testing numbers have also fallen in recent weeks, likely because vaccinated Americans have few reasons to need a test. Data watcher (and former COVID Tracking Project volunteer) Conor Kelly noted that we’re averaging under 1 million tests a day for the first time since fall 2020. At the same time, though, the national positivity rate for PCR tests is lower than ever—it hit 2.2% on June 1.
Despite the drop in tests, the positive rate is at an all-time low, reaching a 7-day total of 2.2% through 6/1 according to HHS data
Things are looking pretty good here in the U.S., though some experts say a summer or fall surge could still be possible if we relax restrictions too much. Other countries without vaccine access are not nearly so lucky.
I am not usually a dog person, but I have to make an exception for Babydog. Her owner, West Virginia Governor Jim Justice, has made her the mascot of his state’s vaccine lottery.
“If you won’t do it for your family, you have to get vaccinated for Babydog,” he said at a press conference. “She wants you vaccinated so badly.”
If I weren’t already vaccinated, I would do it for Babydog. Just look at that face!
Cases and deaths among healthcare workers: A new addition to the CDC COVID Data Tracker this week: a tab reporting cases and deaths in doctors, nurses, and other healthcare personnel. The CDC is reporting both totals and new cases/deaths by week, though the data here likely represent only a fraction of the true counts of healthcare workers infected during the pandemic. Notably, the total death toll is only about 1,600—less than half of the healthcare worker deaths reported by The Guardian and KHN’s “Lost on the Frontline” project.
Health Equity Tracker: When the COVID Tracking Project (including the COVID Racial Data Tracker) ceased data collection in March, it became much more difficult to compare COVID-19 case counts by race and ethnicity across states. A new project from the Morehouse School of Medicine fills that gap—and does much more. The Tracker incorporates data from the CDC, the Census, and other sources to provide comprehensive information on which communities have been hardest hit by the COVID-19 pandemic. Read more about it in this STAT article.
Coronavirus variant lineages: I came across this source a few days ago while researching variant lineages, prompted by a question on Twitter. Phylogenetic Assignment of Named Global Outbreak Lineages (or PANGO Lineages, for short) is a software tool developed by a lab in the U.K. that allows users to submit and analyze coronavirus sequences. The specific page I’ve linked here provides a comprehensive, searchable list of all the coronavirus variants that scientists have identified. Very useful if you need to search up an older or less-well-known variant.
Unemployment Insurance Data Explorer: This tool from progressive think tank The Century Foundation allows users to explore, visualize, and download data on unemployment insurance distributed during the pandemic. The tool includes data broken out by state and goes back in time to 1971—valuable for historical analysis.
Earlier this week, New York City mayor Bill de Blasio made a big announcement: all the city’s schoolchildren are going back to the classroom this fall. There will no longer be a remote option.
NYC was one of the first big cities to open with a hybrid model last fall, but it came with challenges—ranging from teachers protesting unsafe conditions, to in-person students doing “Zoom school” in the library, to closures dictated by confusing test positivity rates. The city’s choice to eliminate a remote option indicates a commitment to simple, unified policies for all students and teachers. It also suggests that many other districts may follow NYC’s lead—as the New York Times reported, a few districts already have.
Vaccine options for children ages 12 and older (now Pfizer, soon Moderna) make in-person education a safe bet for a lot of families. But younger students will likely have to wait much longer for their shots. As a result, regular testing will continue to be a key safety strategy, aided by American Rescue Plan funding dedicated specifically to school surveillance programs. Beyond identifying COVID-19 cases before they turn into outbreaks, testing can help parents and teachers feel safer about reopening plans.
But, as we have covered extensively here at the COVID-19 Data Dispatch, school testing data are incredibly hard to come by. New York continues to be the only state that reports any data on COVID-19 tests conducted in schools, and some states fail to even report COVID-19 school case counts.
Since Biden took office, more schools have returned to hybrid and in-person classes, but it remains unclear what percentage of school districts across the country are regularly screening students and teachers for Covid-19. An Education Department spokesperson said the department is “not tracking that level of detail.” A Centers for Disease Control and Prevention spokesperson said that “most states have offered or implemented testing programs in schools during the 2020-2021 school year,” adding that a survey conducted by the publication EdWeek in February found that just 16 percent of school district leaders said they were testing students.
Education and health groups — including the Association of State and Territorial Health Officials, the Rockefeller Foundation and American Federation of Teachers — also said they do not have comprehensive nationwide data on how many districts have testing programs in place.
This continued lack of data makes it difficult to evaluate how well school testing programs actually work. A lot of schools may be flying blind going into the fall 2021 semester, or they may choose not to set up regular testing at all.
I plan to do more reporting on this topic over the summer, including detailed investigations of individual school districts. If you have any burning questions, send them my way (betsy@coviddatadispatch.com).
On November 18, New York City mayor Bill de Blasio announced that the city’s schools would close until further notice. The NYC schools discrepancy is indicative of an American education system that is still not collecting adequate data on how COVID-19 is impacting classrooms—much less using these data in a consistent manner.
Earlier this month, the CDC made a pretty significant change in how it tracks breakthrough cases. Instead of reporting all cases, the agency is only investigating and collecting data on those cases that result in hospitalizations or deaths.
In case you need a refresher: “breakthrough cases” are those infections that occur after a patient is fully vaccinated (including both doses, if applicable, and the two-week waiting period after a final dose). These cases are rare—like, one in ten thousand rare. As I wrote back in April, it’s important to contextualize any reporting on these cases with their incredible rareness so that we hammer home just how effective the vaccines are.
But just because breakthrough cases are rare doesn’t mean we shouldn’t pay attention to them. In fact, it’s critical to pay attention to these cases in order to monitor precisely how well our vaccines are working—and how new variants may threaten the protections those vaccines provide.
Breakthroughs can offer a unique wellspring of data. Ferreting them out will help researchers confirm the effectiveness of COVID-19 vaccines, detect coronavirus variants that could evade our immune defenses, and estimate when we might need our next round of shots—if we do at all.
As I’ve discussed in past variant reporting, numerous studies have demonstrated that the vaccines currently in use in the U.S.—especially the Pfizer and Moderna vaccines—work well against all variants. That includes variants of concern, such as B.1.617 (from India), B.1.351 (from South Africa), and P.1 (from Brazil). But the vaccine efficacy rates for some of these variants are lower than that stellar 95% we saw in Pfizer and Moderna’s clinical trials. And some common therapeutic drugs don’t work well for patients infected with variants, too.
As a result, scientists are concerned that, while the vaccines are working well now, they might not work well forever. Whenever the coronavirus infects a new person, it has the opportunity to evolve. And that continued evolution must be monitored. The first coronavirus variant able to evade our vaccines may emerge in a foreign country with a raging outbreak—but it may also emerge here in the U.S. Closely monitoring all breakthrough cases will help us find that dangerous variant.
(Of note: A new, potentially-concerning variant was identified just last night in Vietnam; WHO scientist Maria Van Kerkhove described it as an offshoot of the variant from India, B.1.617, with “additional mutation(s).”)
With that in mind, let’s unpack the CDC’s reporting change. When the vaccine rollout started, the agency was investigating all breakthrough cases that came to its attention—including those in patients with only mild symptoms, or with no symptoms at all. According to an agency study released this past Tuesday, the CDC identified 10,262 such breakthrough cases from 46 U.S. states and territories between January 1 and April 30, 2021.
Keep in mind: By April 30, about 108 million Americans had been fully vaccinated. Dividing 10,262 by 108 million is where I got that “one in ten thousand” comparison I cited earlier. As I said: very rare.
Starting on May 1, however, the CDC changed its strategy. Now, it is only tracking breakthrough cases that result in severe illness for patients, leading to hospitalization and/or death. The CDC says that this choice is intended to focus on “the cases of highest clinical and public health significance” rather than tracking down asymptomatic cases.
In its May 25 report, CDC scientists said that 27% of the breakthrough cases identified before May 1 were asymptomatic. 10% of the infected individuals were hospitalized, though almost a third of those patients were hospitalized for a reason unrelated to COVID-19. Only 160 patients (less than 2% of the breakthrough cases) died.
We need to take these numbers with a grain of salt, though, because the CDC has likely undercounted the true number of asymptomatic cases. Both clinical trials and studies on vaccine effectiveness in the real world have suggested that those people who get infected with COVID-19 after completing a vaccination regime are more likely to have mild symptoms, or no symptoms at all.
Plus, the CDC is recommending that vaccinated Americans don’t need to get tested before traveling, if they have come into contact with someone known to have COVID-19, or for many of the other reasons that many of us got tested this past year. (The agency is still recommending that fully vaccinated people get tested if they’re experiencing COVID-19 symptoms, though.)
As I wrote at Slate Future Tense last month, such guidelines are likely to drive down the number of COVID-19 tests conducted across the U.S. And this trend seems to be happening, so far: PCR tests dropped from their winter surge levels this spring, and are now dropping again. (Antigen and other rapid tests may be getting used more, but we don’t have any comprehensive data on them.)
With that drop in testing—combined with the overall challenge of identifying asymptomatic COVID-19 cases outside of dedicated studies—it would be pretty damn hard for the CDC to track down all breakthrough cases. The agency’s focus on more serious cases instead may thus be considered a conservation of resources, directing research efforts and care to those Americans who get seriously ill after vaccination.
But “a conservation of resources” is also a nice way of saying, the CDC made a lazy choice here. The agency has poured money into genomic surveillance over the past few months, sequencing over 20,000 cases a week (compared to a few thousand cases a week before Biden took office). In recent weeks, the Biden administration has announced renewed funding for public health and similar commitments to prioritizing scientific research. If the CDC wants to find and sequence breakthrough cases in order to identify vaccine-busting variants, there should be nothing stopping the agency.
Or, as epidemiologist Dr. Ali Mokdad told the New York Times: “The C.D.C. is a surveillance agency. How can you do surveillance and pick one number and not look at the whole?”
Out of those 10,262 cases that the CDC reported this week, only 5% had sequence data available—but the majority of those sequined cases were variants of concern, including B.1.1.7 and P.1. At The Atlantic, Wu reported that epidemiologists in some parts of the country are seeing more breakthrough cases tied to concerning variants, while others are seeing breakthrough case sequences that match the overall infections in the community.
To me, this high level of unknowns and uncertainties mean that we need more breakthrough case reporting and sequencing, not less. And we need a national public health agency that commits to true surveillance, so that we aren’t flying blind when the coronavirus inevitably evolves beyond our current defenses.
I don’t understand why only 5% of COVID vaccination breakthrough infections are being sequenced. Wouldn’t sequencing breakthrough cases be highest yield for picking up emerging variants? https://t.co/ErgFpNQh5s
Following the end of the federal public health emergency in May, the CDC has lost its authority to collect vaccination data from all state and local health agencies that keep immunization records. As a result, the CDC is no longer providing comprehensive vaccination numbers on its COVID-19 dashboards. But we still have some information about this year’s vaccination campaign, thanks to continued CDC efforts as well as reporting by other health agencies and research organizations.
This week, the FDA authorized Novavax’s updated COVID-19 vaccine. Here’s why some people are excited to get Novavax’s vaccine this fall, as opposed to Pfizer’s or Moderna’s.
Last week, I asked you, COVID-19 Data Dispatch readers, to send me your stories of challenges you experienced when trying to get this fall’s COVID-19 vaccines. I received 35 responses from readers across the country, demonstrating issues with insurance coverage, pharmacy logistics, and more.
In the past week (May 22 through 28), the U.S. reported about 151,000 new cases, according to the CDC. This amounts to:
An average of 22,000 new cases each day
46 total new cases for every 100,000 Americans
22% fewer new cases than last week (May 15-21)
Last week, America also saw:
21,900 new COVID-19 patients admitted to hospitals (6.7 for every 100,000 people)
3,000 new COVID-19 deaths (0.9 for every 100,000 people)
70% of new cases in the country now B.1.1.7-caused (as of May 8)
An average of 1.4 million vaccinations per day (per Bloomberg)
Cases, deaths, and hospitalizations all continue to drop nationwide. The U.S. reported about 3,000 COVID-19 deaths last week, in total—at the peak of the winter surge, we saw more than 3,000 deaths a day.
This trend is echoed in most states. In the May 27 Community Profile Report, the HHS classifies almost every state as “orange” (between 50 and 100 new cases per 100,000 residents over the past week) or “yellow” (between 10 and 50 cases per 100,000). Wyoming is the only state in the “red” classification, at 101 cases per 100,000 over the past week—while California is in the green, with only 9 cases per 100,000.
In New York City, where I live, every single ZIP code currently has a test positivity rate at 3% or lower—for the first time since last summer. This is yet another piece of good news showing how well the vaccines work. Half of the total U.S. population has had at least one dose and more than half of the adult population is fully vaccinated, as of yesterday.
The vaccines also continue to do their part against variants. The CDC variant data—updated this week—indicate that B.1.1.7 is still growing, but it’s leveling off as new cases slow. This variant has gone from causing about 60% of cases in early April, to 67% in mid-April, to 70% in early May; a much slower decline than what we saw in February and March.
Of more concern: P.1, the variant first identified in Brazil, is causing 7% of U.S. cases as of May 8—and the CDC’s Nowcast estimate puts it at almost 10% of cases by May 22. B.1.617, the variant first identified in India, is also sharply increasing; its case share doubled from April 24 to May 8. Both of these variants are more transmissible (B.1.617 dangerously so) and may have lowered vaccine efficacy.
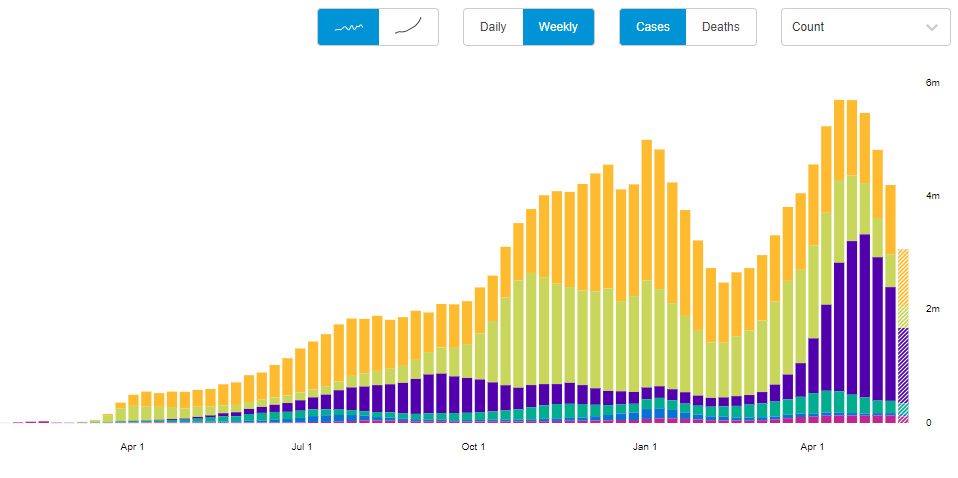
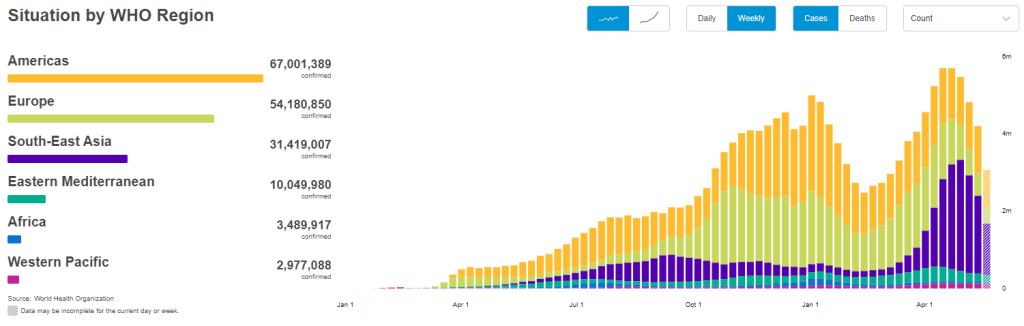
But the harm these variants can cause in the heavily-vaccinated U.S. pales in comparison to the risk they pose in other nations. As evidenced by the World Health Organization chart above, the share of cases in Southeast Asia and other lower-income nations is increasing even as cases in the U.S. and Europe drop. The U.S. should focus on providing aid to the nations where vaccinations are lagging so that we can help inoculate people before more, harder-to-contain variants evolve.
In other words, there’s a reason I’m not giving space to the lab leak theory in this publication. If you’d like to read more about the issue, I recommend this article by Amy Maxmen.
very fun and fresh how the "china deliberately released a bioweapon" narrative is "suddenly plausible" and "taking over global covid discourse" now when the US is hoarding vaccines and basically refusing to send supplies/money/etc to other nations :))))
— betsy ladyzhets 📊 (@betsyladyzhets) May 28, 2021
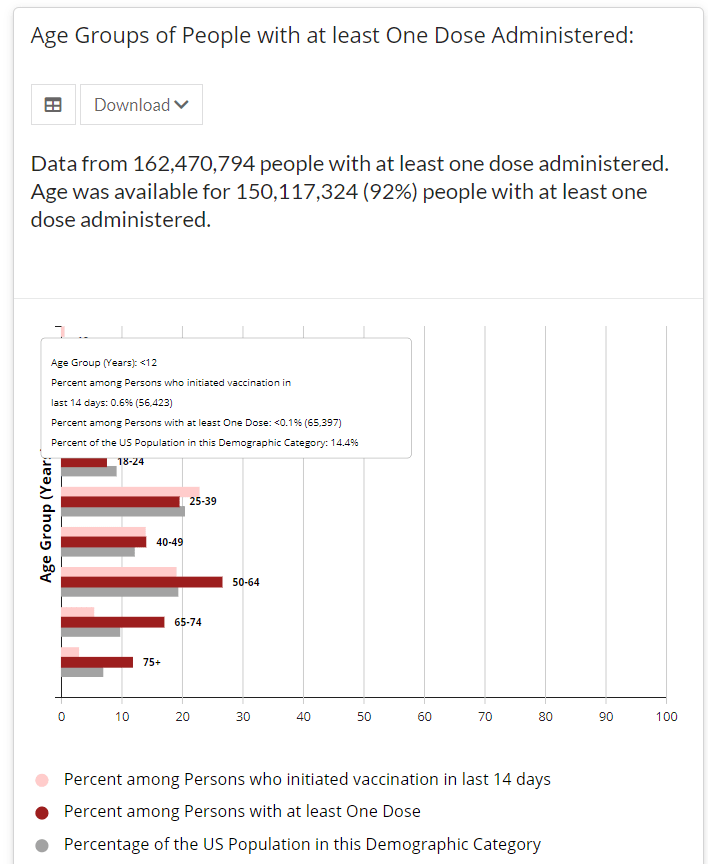
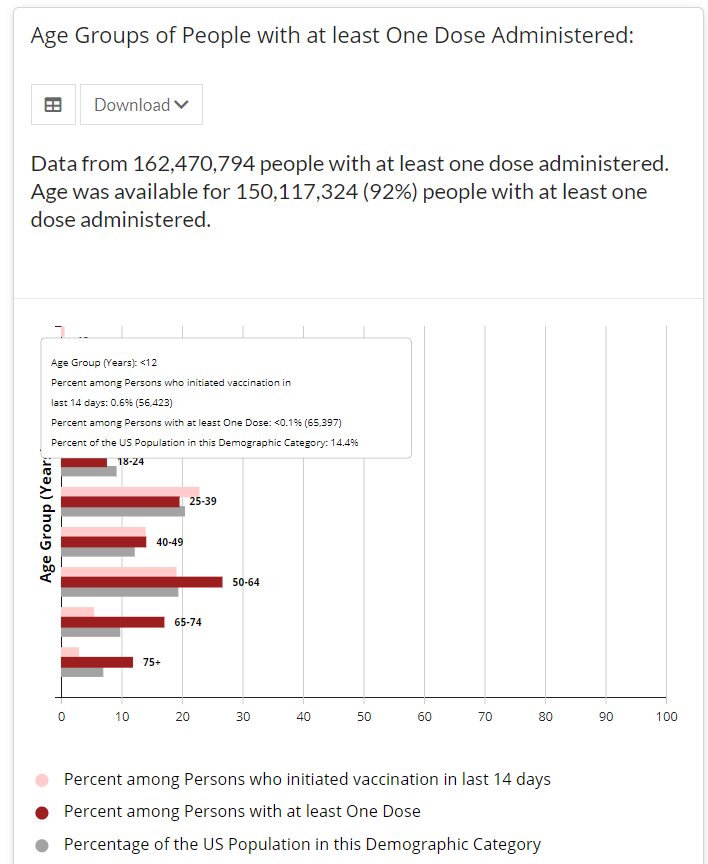
Screenshot of the CDC’s vaccine dashboard, showing about 65,000 first dose vaccinations for children under age 12.
When I sent out last week’s issue, the CDC’s Vaccination Demographics page was grouping newly eligible 12 to 15-year-olds in with 16 to 17-year-olds. Now, the agency’s age reporting has diversified a bit: you can find separate vaccination numbers for children ages 16 to 17, 12 to 15, and under 12.
Wait… under 12?
That’s right. The CDC reports that about 65,000 children under age 12 have received at least one vaccine dose as of May 22, even though this age group is not yet eligible for any of the vaccines on the market.
Where did this number come from? The CDC’s page doesn’t offer any explanations, but possibilities may include:
Pfizer and Moderna are currently running clinical trials for the under-12 population, and children in these trials may have been entered into vaccination records.
Errors in the data pipeline—maybe some kids in the 12 to 15 age group were logged as under 12 instead, or some birthdays were input incorrectly.
But the Pfizer and Moderna trials have enrolled only 12,000 under-12 participants total. That leaves over 50,000 vaccinations that we can’t explain—it’s a pretty big number to attribute to data errors.
GAO analysis of COVID-19 in nursing homes: The Government Accountability Office, an organization that does research and audits on behalf of Congress, has a new report out this week on the devastating COVID-19 outbreaks that took place in nursing homes. The GAO researched about 13,000 facilities, using CDC data from May 2020 to January 2021. 94% of the nursing homes in the study faced at least one COVID-19 outbreak, with the majority of outbreaks (85%) lasting five weeks or more.
Johns Hopkins Pandemic Data Initiative: The Johns Hopkins Coronavirus Resource Center is one of the most widely-cited sources of COVID-19 data, providing detailed and up-to-date information for both the U.S. and the world. But the resource center’s scientists “have struggled to work with COVID-19 data that is inconsistent, incomplete, and insufficient,” writes JHU data lead Beth Blauer in a blog post. A new section of the resource center will explore data inconsistencies and highlight possible solutions.
Excess deaths by U.S. county: Excess deaths, or those deaths that occur above a region’s past baseline, are a common metric for examining the true toll of COVID-19. In addition to reporting excess deaths by U.S. states and demographic categories, the CDC’s National Center for Health Statistics (NCHS) also reports this information by county. A group of researchers (Stokes et al.) recently analyzed these county-level data and found that U.S. COVID-19 deaths may be underestimated by about 20%; their findings were published this week in PLOS Medicine.
Vaccine consent laws by state: As the Pfizer vaccine is now available to children ages 12 to 15, a lot of teenagers out there may want to know if they can get vaccinated without parental permission. The site VaxTeen provides these kids with information on the consent laws in every state, as well as a guide for talking to your parents about vaccines and other resources. (H/T Robin Lloyd.)