The COVID-19 Data Dispatch does not endorse the new MTA mask guidance.
Anyone who regularly rides the New York City subway knows that the city’s mask requirement for public transportation has been unenforced and loosely followed—especially in the months following last winter’s Omicron surge.
But last week, even the requirement itself was struck down. New York Governor Kathy Hochul (who oversees the Metropolitan Transportation Authority, as it’s a state-controlled agency) announced that masks are now optional on trains and buses. And she introduced the policy with a new version of the MTA’s masking graphic that felt like a slap in the face to higher-risk New Yorkers who now feel unsafe using the transit system.
NPR has a good article explaining why health experts have criticized the new graphic. Personally, I think it discourages people from thinking about how their COVID-19 safety choices impact a broader community—something that’s especially important in a dense, diverse city like NYC. Telling New Yorkers, “You do you,” when “doing you” could mean posing an immense risk to your neighbors, is a dangerous message.
The one silver lining here is, I’ve seen a few excellent posters parodying the MTA’s new mask graphic. Here’s one of my favorites:
White House plans for annual boosters: This week, Biden administration officials announced a plan for one COVID-19 shot each year, on a similar timeline to the flu shots distributed every fall. In this plan, this fall’s Omicron-specific boosters are the first iteration of annual boosters. Some scientists are skeptical about the plan, given that (as I discussed last week) we have very little data on how well the new boosters work. It could be preemptive to say just one shot each year will be enough, and the federal government should also be investing in next-generation vaccines that might better prevent infection and transmission.
Urgency of Equity Toolkit: The People’s CDC, a health advocacy organization aiming to fill gaps in COVID-19 guidance left by the official CDC, has published a toolkit focused on school safety for the fall. The presentation walks readers through why public health measures are still needed in K-12 schools and potential layers of protection, such as improved ventilation, surveillance testing, and improving pediatric vaccination rates.
Parents and caregivers lost to COVID-19: Speaking of protecting children, a new study published in JAMA Pediatrics this week estimates how many children have lost parents or caregivers during the pandemic. The researchers (an international group including experts at the World Health Organization, World Health Organization, and others) produced their estimates based on global excess mortality data—going beyond deaths officially reported as COVID-19. In total, the study estimates about 10.5 million lost parents or caregivers and 7.5 million became orphans worldwide.
True virus prevalence during the BA.5 surge: I’ve previously cited the work of Denis Nash and his team at the City University of New York; they utilized a population survey to estimate how many New Yorkers actually got COVID-19 during the city’s spring surge. This week, the team shared a new study that uses the same approach for the whole country. While their sample size was fairly small (about 3,000 people) and the study has yet to be peer-reviewed, its findings are striking: about 17% of U.S. adults surveyed were infected by the coronavirus during a two-week period from late June to early July, around the peak of the BA.5 surge.
New independent effort to study Long COVID: This week, a group of researchers, clinicians, and patients announced the Long Covid Research Initiative, a new collaborative effort to study the condition and identify potential treatments. The group has raised $15 million in private funding and aims to move more quickly than public or academic efforts that have been bogged down in bureaucracy (among other challenges). I’m excited to see what this new group finds.
BA.2.75, a newer subvariant that evolved from BA.2, has been driving increased coronavirus transmission in some other countries recently. You might also see it referred to as “Centaurus” on social media. This lineage has yet to be identified in large numbers in the U.S., but I was inspired by a recent reader question to share what we’ve learned about it since my previous post in July.
Scientists are concerned about BA.2.75 because it has several new mutations that are distinct from BA.2, most of those in the spike protein (where the virus binds to human cells). And some preliminary research, including recent studies in the Lancet Infectious Diseases and in the New England Journal of Medicine, have found that BA.2.75 is less susceptible to neutralizing antibodies from prior infections or treatments than past variants.
This could mean people who previously caught BA.2 or other versions of Omicron could be susceptible to BA.2.75, reports Hannah Flynn in Medical News Today. Of course, more research and data are needed on the new variant. But BA.2.75 has been driving new surges in India, Nepal, and other countries—another signal that it’s worth watching.
As I noted in today’s National Numbers post, the CDC is not yet reporting BA.2.75 prevalence estimates separately from other versions of BA.2. But it has reported an increase in BA.2 overall in recent weeks, from 0.6% of new cases in the week ending August 27 to 1% in the week ending September 10. This is probably BA.2.75, given that older versions of BA.2 haven’t been competitive in the U.S. for a few months.
Helix, a COVID-19 testing company that works with the CDC and other agencies on variant surveillance, is tracking BA.2.75 separately from BA.2 on its dashboard. According to Helix’s data, original BA.2 has stayed at very low prevalence in recent weeks while BA.2.75 has risen to 1% of cases sequenced.
It’s currently unclear—as it was in July—to what extent BA.2.75 might be able to compete with BA.5 or BA.4.6, which are the main subvariants of concern spreading across the U.S. right now. But if BA.2.75 does become dominant, it will be helpful that the newly-authorized booster shots include genetic material from the original, Wuhan variant, not just BA.4 and BA.5.
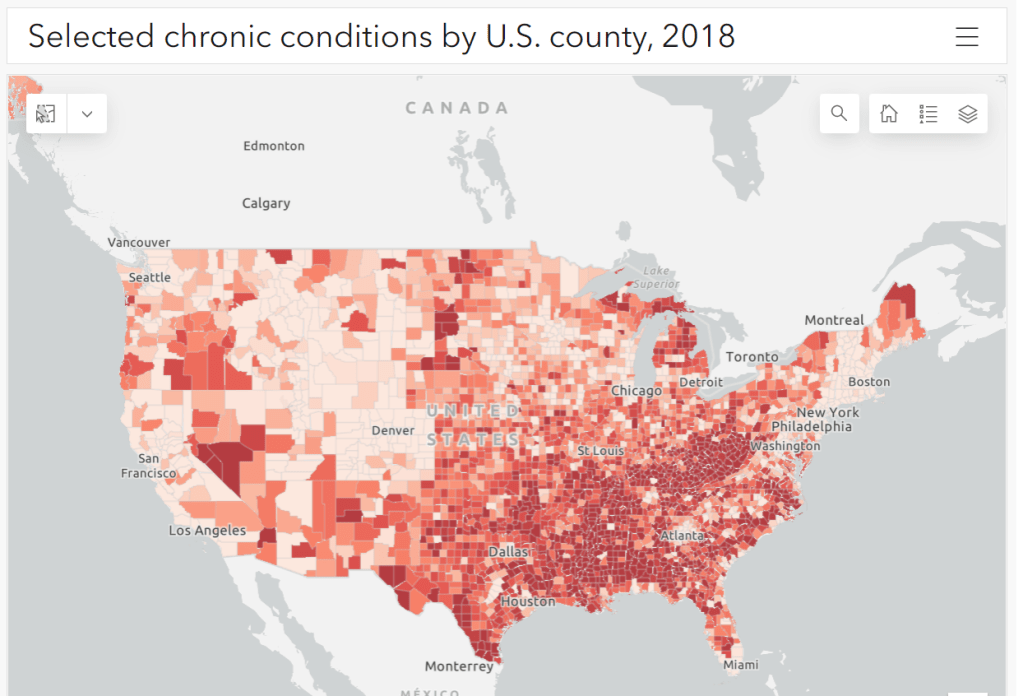
Parts of the South and Midwest have higher rates of chronic conditions (colored darker red on the map) that confer higher risk for severe COVID-19. Chart via the CDC.
The U.S. has started a new booster shot campaign, this time using vaccines designed to specifically target super-contagious subvariants Omicron BA.4 and BA.5. (For more details on the shots themselves, see last week’s post.)
Unlike previous vaccination campaigns, these boosters are available to all adults across the country who have been previously inoculated. There was no prioritization for seniors, healthcare workers, or other higher-risk adults. The official guidance from the federal government is actually pretty straightforward, for once: everyone should get the new booster. And get a flu shot soon, too, possibly even at the same time as your COVID-19 shot.
But all previously-vaccinated Americans are not facing similar levels of COVID-19 risk. Many of the same qualifications that might have warranted you an earlier dose in spring 2021 should now lead you to prioritize your Omicron booster, even if you might have been infected recently. At the same time, people who fall in these groups (or who share their households) have a good reason to continue using other safety measures after their boosters.
Here are the major qualifications for higher risk, with data to back them up:
Seniors, especially those over age 70: More than 90% of Americans over age 65 have received at least their primary vaccine series, according to the CDC, while over 70% have received at least one booster. Yet older Americans continue to have the highest rates of hospitalizations and deaths. For example, those older than 70 have consistently been hospitalized at several times the rate of younger adults (when adjusted for population). The same pattern is true for deaths among adults over age 75. Seniors who receive the new booster shots will face a lower risk of severe COVID-19 this fall and winter.
Black, Indigenous, and other Americans of color, especially seniors: Despite dedicated vaccination campaigns and other health equity efforts, Americans of color have continued to be hit harder by the pandemic than white Americans. Higher rates of chronic conditions in minority populations combined with other socioeconomic factors (POC are more likely to work essential jobs, to lack healthcare, etc.) have led to disproportionately high hospitalization and death rates. And the U.S.’s booster shot campaigns so far have been inequitable, as shown in a recent study by demography experts. Reaching these populations should be a priority for the new Omicron boosters.
Immunocompromised people: National estimates consider about 3% of Americans to be moderately or severely immunocompromised, meaning that their immune systems have limited capacity to respond to infections without medical assistance. This group includes cancer patients, organ transplant recipients, people with autoimmune diseases, and more. (This Yale Medicine article provides more information.) Immunocompromised people might have already had multiple booster shots but are still eligible to receive an Omicron booster as soon as possible, the CDC recommends.
People with Long COVID and related conditions: While there isn’t as much established data in this area, I have seen a lot of anecdotal reports from Long COVID patients who work hard to avoid new coronavirus infections—concerned about reinfection’s possibility to worsen their symptoms. On the flip side, vaccination might lead to improvement in Long COVID patients, as the shot boosts a patient’s immune system in responding to lingering reservoirs of virus. The Atlantic covered this possibility when Long COVID patients were first eligible for vaccination in early 2021, and other studies since then have backed it up. More research is needed, but at the very least, Long COVID patients receiving a new booster will have lower risk of a new severe case.
People with other preexisting health conditions: The CDC has an extensive list of medical conditions that can confer additional risk for severe COVID-19, with plenty of links to other CDC pages and medical sites where you can learn more about relevant evidence. I won’t go through them all here (that’s a topic for another week’s issue), but I do recommend checking out the CDC’s information and linked sources if you have a condition on the list. You can also explore this map of chronic condition rates by county.
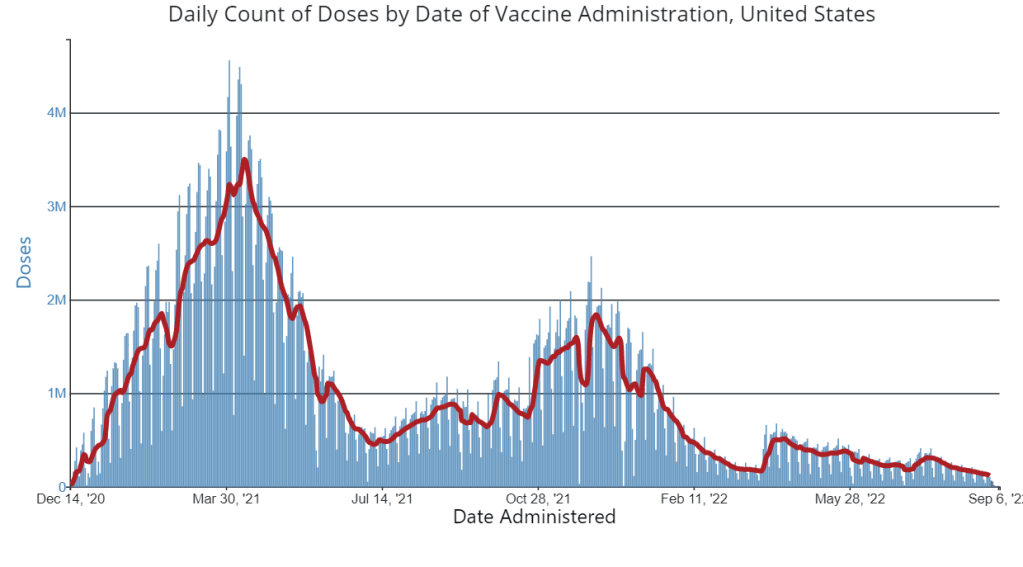
A week after new COVID-19 boosters were authorized, the U.S. has yet to see a significant jump in vaccine doses administered. Chart via the CDC.
In the past week (September 3 through 9), the U.S. reported about 500,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 70,000 new cases each day
150 total new cases for every 100,000 Americans
19% fewer new cases than last week (August 27-September 2)
In the past week, the U.S. also reported about 32,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 4,600 new admissions each day
9.9 total admissions for every 100,000 Americans
11% fewer new admissions than last week
Additionally, the U.S. reported:
2,200 new COVID-19 deaths (0.7 for every 100,000 people)
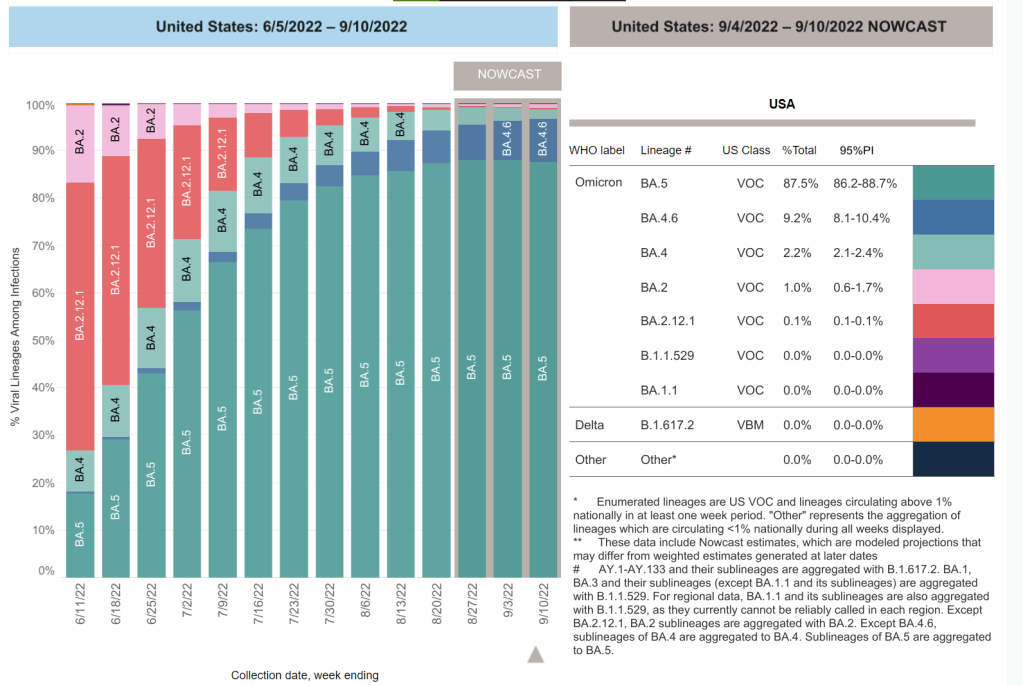
88% of new cases are caused by Omicron BA.5; 9% by BA.4.6 (as of September 10)
An average of 25,000 vaccinations per day (per Bloomberg)
It might appear that the U.S. reported a significant drop in COVID-19 cases last week, as the CDC’s numbers dropped to about 70,000 new cases a day last week from 87,000 new cases a day in the prior week. But in fact, the decline was likely exaggerated by Labor Day weekend, as testing labs and the public health workers who crunch data took time off.
Wastewater data from the last two weeks tell a different story. In Biobot’s most recent update, the company reported a slight increase in coronavirus concentration in wastewater at the national level. Regionally, the virus grew in the Northeast, Midwest, and South.
There has been a slight increase in our #COVID19#wastewater data from last week—a departure from the previous 5 weeks of decline. The national average went up 3% & 3/4 regions experienced small rises (1-6%). Levels in the Midwest fell 1%. Explore more at https://t.co/GBL4twvGGTpic.twitter.com/6SCwvbOMpf
While hospital admissions and other healthcare system metrics continue to show a decline, wastewater data is often an advanced indicator for new coronavirus surges. In this case, it could mean the often-predicted fall wave is beginning in some parts of the country. Remember: wastewater surveillance can catch transmission upticks early because it doesn’t rely on individuals getting PCR tests or seeking out healthcare—factors that can cause lags and undercounting in case and hospitalization data.
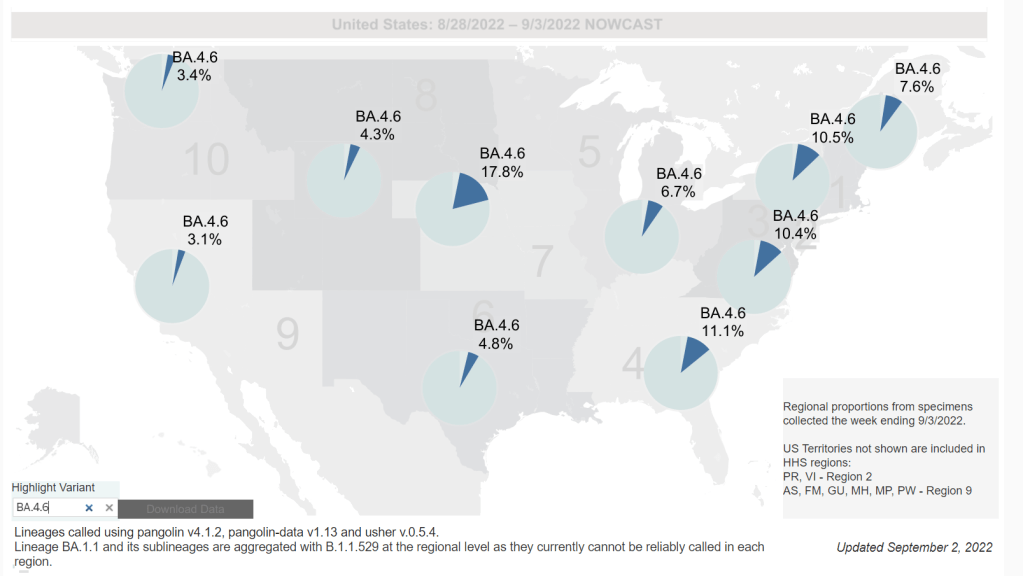
Potential factors contributing to increased COVID-19 outbreaks might include holiday gatherings and travel, the start of the school year, and new Omicron subvariants taking over. BA.4.6, the lineage from BA.4 that may be even more transmissible, went from causing about 8% of new cases in the week ending September 3 to 9% in the week ending September 10, according to CDC estimates; meanwhile, BA.5’s prevalence dropped by about 1%.
This might seem like a small shift, but it is an indicator of BA.4.6’s capacity to eventually outcompete BA.5—and reinfect people who previously caught a different version of Omicron. BA.4.6 is causing a higher share of cases in the Midwest, specifically in Iowa, Kansas, Missouri, and Nebraska, so those are states to particularly watch for increased COVID-19 spread.
At the same time, the CDC reports that 1% of cases nationwide were caused by BA.2 lineages (not BA.2.12.1) last week. This is likely the work of BA.2.75, another subvariant of concern that the CDC isn’t yet tracking separately. (More on that later in the issue.)
The federal government’s main action to mitigate this probably-coming surge is a new booster campaign, with the Omicron BA.4/BA.5 shots authorized last week. But vaccination numbers have been low so far, with far fewer than 100,000 doses administered each day last week.
A lot of COVID-19 data sources have become decidedly less reliable since the beginning of 2022, through a combination of official case counts becoming poorer reflections of prevalence (thanks to less PCR testing) and fewer resources devoted to data tracking at public health departments from local agencies up to the CDC.
But one federal source has remained fairly consistent: the Household Pulse Survey. This project, run by the Census in collaboration with a variety of other government agencies, started in spring 2020 as a way to track how the pandemic was impacting Americans’ daily lives. Every two weeks, government researchers randomly survey U.S. adults with questions ranging from their employment status to mental health. As of this summer, the Household Pulse Survey also includes data on Long COVID prevalence.
For every question asked by the Household Pulse Survey, you can find results over time, by state, and for a variety of other demographics: race, ethnicity, age, gender, sexuality, etc. I appreciate that this source has continued measuring the pandemic’s impact, and I think journalists (myself included!) could be referencing it a lot more.
Omicron BA.4.6, a newer version of BA.4, is currently more prevalent in the Midwest than other regions of the country. Chart via the CDC, retrieved September 4.
Slow rise of BA.4.6 is worth watching: As I mentioned in today’s National Numbers post, a newer subvariant labeled BA.4.6 is gaining ground over other versions of Omicron in the U.S. BA.4.6 evolved from BA.4, and has an additional mutation in the virus’ spike protein that enables it to bypass protection from prior infections. It’s unclear whether BA.4.6 will be able to fully outcompete BA.5, which is currently causing the vast majority of U.S. COVID-19 cases—these two strains are similar enough that the competition may go slowly. So far, the subvariant has been more prevalent in the Midwest than other regions of the country, according to CDC data. Also worth watching: BA.2.75, a subvariant that is dominating some European countries but hasn’t shown up significantly in the U.S. yet.
Up to 4 million people may be out of work due to Long COVID: Last week, policy research organization the Brookings Institute published a new report discussing the massive impacts Long COVID is having on America’s labor force. The report utilizes recent data from the Household Pulse Survey (released in June) estimating Long COVID prevalence, in conjunction with research on how many long-haulers might be out of work due to their condition. The results: between two and four million Americans potentially lost their jobs (or are working significantly less) due to Long COVID, costing at least $170 billion a year in lost wages. Even the low ends of these estimates are staggering.
U.S. life expectancy declined again in 2021: Americans born in 2021 may expect to live for 76 years on average, according to the CDC’s National Vital Statistics System. This is the lowest life expectancy has been since 1996. CDC researchers attribute the sharp decline in the last two years to the pandemic and drug overdose deaths. Disparities in life expectancy have also increased: Native Americans born in 2021 may expect to live only 65 years on average and Black Americans may expect to live 71 years, compared to 76 years for white Americans.
Biobot expands wastewater surveillance for opioid tracking: In the last couple of months, we’ve seen wastewater used to track monkeypox and polio, in addition to COVID-19—suggesting the technology’s capacity for broader public health surveillance. This week, leading wastewater company Biobot announced a new initiative to track opioid use and other high-risk substance use through a similar platform to its current COVID-19 efforts. Tracking the opioid crisis was actually the original focus for Biobot’s founders pre-pandemic, so it’s notable to see the company expanding in this direction now.
This week, the FDA and CDC authorized new booster shots from both Pfizer and Moderna that are tweaked to specifically target Omicron BA.4 and BA.5. The vaccines will start becoming available at pharmacies and doctors’ offices across the country in the coming days.
Much of the media coverage of these new boosters has focused on the fact that they’re the first COVID-19 vaccines derived from a newer variant, as opposed to the original Wuhan strain. BA.5 and BA.4.6, a sublineage of BA.4, are causing almost all COVID-19 cases in the country right now; some experts hope that a booster campaign targeted to these versions of the coronavirus will lead to actual decreases in transmission, not just severe disease.
While this is an important milestone, I’d like to focus on a couple of reasons these shots are notable from a data perspective. First, the Omicron boosters are the first COVID-19 vaccines authorized in the U.S. without data from human trials. During vaccine development, companies typically start with lab studies, then test the vaccine in animal models, then in humans. Because the BA.4/BA.5 shots were designed so recently, Pfizer and Moderna haven’t had time to test them in humans yet.
From a safety and efficacy perspective, this lack of data isn’t a huge concern because the new vaccines are very close to BA.1 versions that have been tested in humans. As Katelyn Jetelina explained in a Your Local Epidemiologist post about the new vaccines:
Literally the difference of a few amino acids—like a few letter edits on a Word document. We aren’t changing the number of words in the paper (like dosage of RNA), or the content of the paper, or the platform (like Word to Excel). Because of the minimal change, we are confident that BA.1 bivalent safety data will accurately reflect BA.5 safety.
Another important piece of context here is that flu vaccines—which are updated each year to reflect currently circulating versions of the virus—are typically not tested in humans before they’re rolled out in annual flu campaigns. So, the new COVID-19 shots are following an existing process; future vaccine adjustments for new variants going forward will likely happen in a similar way.
Second, the Omicron boosters are the first COVID-19 vaccines authorized in the U.S. before they’ve been tested in other countries. For previous booster campaigns, effectiveness data from countries with better-organized health systems that started using new rounds of shots before we did (such as the U.K. and Israel) have been key for U.S. regulators making authorization decisions.
But the BA.4/BA.5 boosters haven’t been rolled out anywhere else yet. Several other countries (the E.U., the U.K., Canada, Switzerland, Australia) have authorized Omicron BA.1 boosters—those that have gone through more clinical testing. The U.S. is the first to try the BA.4/BA.5 option. It will be interesting to see whether there are significant differences in how these countries’ fall booster campaigns mitigate potential surges.
And third, these boosters are likely to be the last COVID-19 vaccines authorized while they’re still covered by federal funding.Recent announcements from officials like Ashish Jha have suggested that, in 2023, the government will stop buying vaccine supplies in large quantities to distribute for free. Instead, COVID-19 vaccines will start to be privately-purchased, health insurance-mediated products like other vaccines.
While some local governments and large health institutions will likely still organize free vaccine distributions for future rounds of shots, the lack of federal supplies will be a major shift. It will make COVID-19 vaccination harder to access, especially among people without health insurance—likely leading to even lower uptake. We need to make this last free booster campaign count.
Going forward, here are a few questions I’ll be tracking as these boosters get rolled out:
How will public health agencies track the effectiveness of these new vaccines? We’ll want to see how the BA.4/BA.5 shots compare to prior boosters at preventing infections, hospitalizations, and deaths. Data on breakthrough cases is already pretty limited in the U.S., so we may have to rely on specific local health departments and health systems that have better infrastructure for this.
What additional boosters might be needed in the future? As we examine how well these Omicron-specific boosters work, we will need to keep track of the potential need for more shots. Will immunocompromised people or older adults need second rounds of Omicron shots, for example?
What new variants will come on the scene? Also impacting the potential need for further vaccine shots: the arrival of new variants, either continued Omicron mutations or something else entirely. Wastewater surveillance may be particularly helpful for variant tracking as PCR testing continues to be less available.
How will the privatization of vaccines impact tracking? If COVID-19 vaccines are no longer purchased and distributed by the federal government after 2022, will this impact the CDC’s ability to track vaccinations? We’re already seeing more vaccine distribution at private pharmacies and doctors’ offices as opposed to publicly-run clinics; I wonder how this trend may continue.
For more information on the new boosters, check out:
This is my first COVID-19 Data Dispatch issue after my August hiatus! Here are a few updates on how that went and changes I’m thinking about for the publication going forward.
First off, I owe a big thank you to everyone who reached out with well wishes on this break. After two years without missing a single week of publication, I was (perhaps irrationally) nervous that some readers would be upset that I was taking off for a bit. But that didn’t happen! I appreciate everyone’s understanding and patience.
Besides a few hours at my part-time job (MuckRock’s Documenting COVID-19 project) and one day of poll working for New York City’s August primary, I didn’t work at all between August 4 and August 29. Here are a few fun things I did instead:
Spent a lot of time outside (mostly at various beaches and NYC parks);
Biked in every NYC borough (longest trip: to Van Cortlandt Park and Woodlawn Cemetery in the Bronx);
Read three books (highly recommend “An Immense World” by Ed Yong!);
Drafted most of a long fanfiction project;
Watched a lot of Star Trek: The Original Series.
If you’re curious about the logistics of taking a longer vacation as a freelancer, you can check out this Twitter thread I wrote last week:
today was my first day back at work after a break of over three weeks — my longest vacation in a while! I wanted to share a bit about why & how I did this. freelance transparency thread incoming: 🧵(1/12) pic.twitter.com/BAIDkim4GU
The break was really all that I had hoped it would be: a refreshing step away from constant COVID-19 coverage that allowed me to reflect on why I do this job. With the COVID-19 Data Dispatch and my other work, I aim to give readers the information they need to make individual health decisions, while also thinking about how they fit into broader communities. While my work has evolved a lot over the last two years, that basic tenet hasn’t changed.
At the same time, though, my hiatus made me think more about how I can balance the newsletter and blog with other activities that are important for maintaining my mental health: getting off my computer, spending time outside, non-journalism writing, investing in new skills, and so on. I’m probably not unlike other independent creators when I say there are weeks when writing this newsletter/blog feels more like a chore than a useful service; I want to keep it feeling like the latter.
With that in mind, here are a few shifts I’m thinking about for the coming months:
The “National numbers” and “Sources and updates” sections will stay consistent. In considering this project’s format, I knew that these two sections are particularly valuable for readers (and they tend to be fairly straightforward for me to write). So, don’t expect any big changes here.
Shorter posts. As any editor who’s worked with me could tell you, I am a writer who constantly goes over my assigned word count. And when I have no set word count, as is the case for these issues… They often get quite long, even though I know that shorter summaries tend to be more helpful for readers. In the future, I’m aiming to keep posts shorter, and only write a longer explainer or commentary when it seems actually necessary.
More reader engagement. We continue to be in a confusing phase of the pandemic, with less reliable data or reliable guidance. I want to prioritize answering your questions. To that end, I’ve made an anonymous Google form for submitting COVID-19 queries. It’ll be linked in every issue going forward and on the website’s homepage. While you can still reply to emails too, I hope this will be an easier way to send me ideas for topics I should cover.
Potential events and multimedia: As older readers may remember, in spring 2021, the COVID-19 Data Dispatch ran a series of virtual data workshops— which I really enjoyed putting together! I’m thinking about more possible virtual events for the future, as well as ideas for new content formats (maybe a podcast miniseries? should I do explainers on TikTok?). I’d love to hear from you, readers, if there’s anything in particular you want to see here.
Expanding beyond COVID-19: Between the continued monkeypox outbreak, the resurgence of polio in New York, and plenty of climate disasters this summer, it’s clear that COVID-19 is far from our only public health concern right now. While my projects in the immediate future are still mostly COVID-focused, you might see some other public health and data information creep into newsletters/blogs going forward. (For example, this week’s “Sources and updates” section includes a couple of non-COVID items.)
Occasional breaks. While I have no intention of making like the CDC and pausing my newsletter for any federal holiday, you can expect that the COVID-19 Data Dispatch will not run every single weekend going forward. Like, I’ll take Christmas off. Reasonable stuff.
None of these are particularly major changes, but in the spirit of transparency, I wanted to share what I’m thinking about with all of you. As always, comments or questions are very welcome: just shoot me an email or fill out the new anonymous question form.
In the past week (August 27 through September 2), the U.S. reported about 590,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 80,000 new cases each day
179 total new cases for every 100,000 Americans
8% fewer new cases than last week (August 20-26)
In the past week, the U.S. also reported about 36,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 5,100 new admissions each day
10.8 total admissions for every 100,000 Americans
4% fewer new admissions than last week
Additionally, the U.S. reported:
2,800 new COVID-19 deaths (0.9 for every 100,000 people)
89% of new cases are caused by Omicron BA.5; 8% by BA.4.6 (as of September 3)
An average of 70,000 vaccinations per day (per Bloomberg)
Over the past month, COVID-19 trends in the U.S. have been fairly consistent: disease spread has declined slowly around the country. Official case counts dropped from about 120,000 a day in the first week of August, to about 80,000 a day last week.
New hospital admissions, a more reliable metric these days, have also declined. A month ago, U.S. hospitals were admitting over 6,000 new COVID-19 patients a day; last week, that number was about 5,000. Wastewater data from Biobot and from the CDC suggest that this trend has been broadly consistent across different regions.
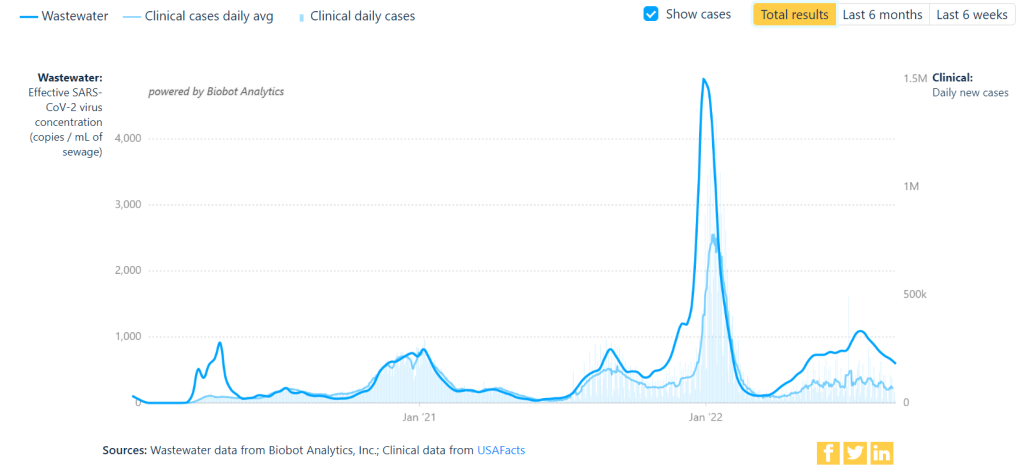
But coronavirus transmission is not currently at low levels by any means. For example, look at Biobot’s national chart showing virus concentration in wastewater compared to officially-reported case numbers. From case numbers alone, you might think that COVID-19 is much less prevalent now than it was in late August or early September last year. But the wastewater data reveal that transmission now is actually pretty close to early-Delta surge levels. (It is, in fact, PCR testing that has declined.)
Similarly, the CDC’s Community Transmission Levels (also known as the older metrics, based on cases and test positivity) show that about 90% of U.S. counties are currently facing high transmission and should require masks indoors. Even the current—and much more lenient—Community Levels suggest that more than half of the country is in a high- or medium-COVID-risk zone.
The summer surge has waned so slowly thanks to the U.S.’s complete abandonment of measures to mitigate COVID-19’s spread, combined with the rise of newer Omicron subvariants. BA.5 continues to dominate here, causing almost 90% of new cases in the week ending September 3, though it’s facing competition from BA.4.6: a version of BA.4 that appears to have a slight advantage.
Most experts agree that we will probably face another surge this fall and winter, as more people gather inside and travel for the holidays. The question is how severe that wave will be, which may be determined via a contest between updated vaccines (more on that later in the issue) and the coronavirus’ continued capacity for mutation.
One potential sign of such a wave: wastewater surveillance in South Africa has picked up an increase in coronavirus concentration, Bloomberg reported yesterday. Also: your usual reminder to be wary of data trends in the days following the holiday weekend.