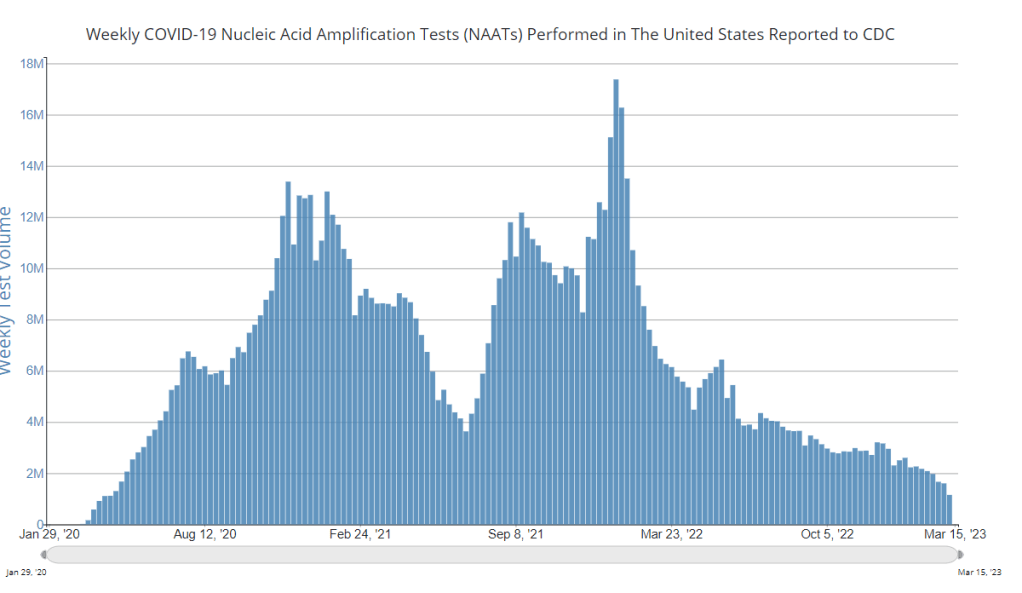
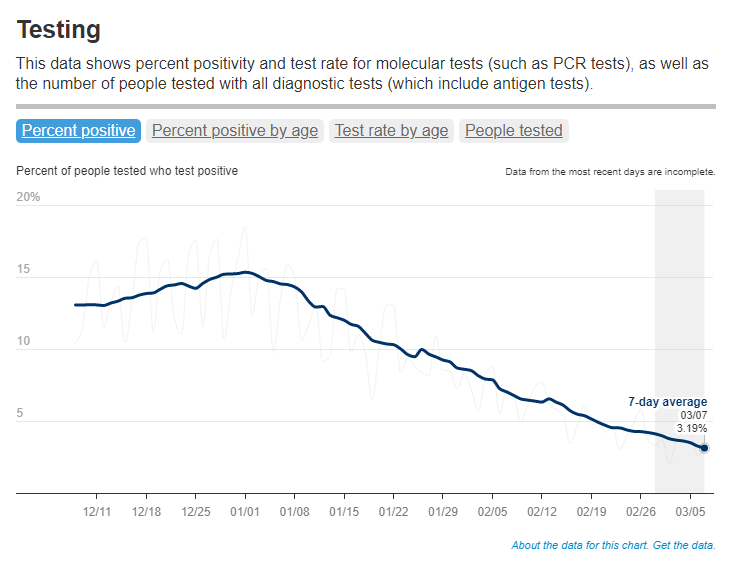
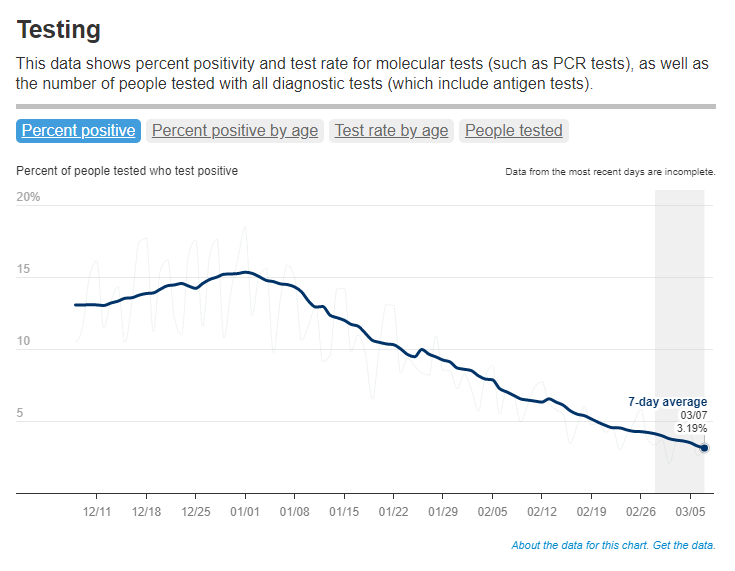
Nationwide, fewer people are getting lab-based COVID-19 tests now than at any time since the start of the pandemic. Chart via the CDC.
When the public health emergency ends this spring, COVID-19 testing is going to move further in two separate directions: rapid, at-home tests at the individual level, and wastewater testing at the community level.
That was my main takeaway from an online event last Tuesday, hosted by Arizona State University and the State and Territory Alliance for Testing. This event discussed the future of COVID-19 testing following the public health emergency, with speakers including regulatory experts, health officials from state agencies, and executives from diagnostic companies.
“The purpose of testing has shifted” from earlier in the pandemic, said Dr. Thomas Tsai, the White House’s COVID-19 testing coordinator, in opening remarks at the event. Public health agencies previously used tests to monitor COVID-19 in their communities and direct contact-tracing efforts; now, individual tests are mostly used for diagnosing people, and the resulting data are widely considered to be a major undercount of true cases.
While the speakers largely agreed about the continued value of rapid, at-home tests (for diagnosing people) and wastewater surveillance (for tracking COVID-19), they saw a lot of challenges ahead for both technologies. Here are some challenges that stuck out to me.
Challenges for rapid, at-home tests:
The public health emergency’s end won’t have an immediate impact on which COVID-19 tests are available, health policy researcher Christina Silcox from Duke University explained at the event. But, in the coming months, the FDA is likely to also end its emergency use authorization for COVID-19 diagnostics. As a result, companies that currently have tests authorized under this emergency will need to apply for full approval. Relatively few rapid tests are currently approved in this way, so the change could lead to fewer choices for people buying tests.
At the same time, it will become harder for many Americans to access rapid tests. After the federal emergency ends, private insurance companies will no longer be required to cover rapid tests. Some insurance providers might still do this (especially if large employers encourage it), said Amy Kelbik from McDermott+Consulting, but it will no longer be a universal option. At the same time, Medicare will stop covering rapid tests; Medicaid coverage will continue through fall 2024.
In light of these federal changes, state health officials at the ASU event talked about a need for continued funding to support rapid test distribution from state and local agencies. “Testing will continue to inform behavior, but will become drastically less available,” said Heather Drummond, testing and vaccine program leader at the Washington State Department of Health. Washington has led a free test distribution program, but it’s slated to end with the conclusion of the federal health emergency, Drummond said; she’d like to see services like this continue for the people who most need free tests.
Drummond and other health officials also discussed the challenges of educating people about how to interpret their test results, as COVID-19 guidance becomes less widely available. The vast majority of rapid, at-home test results are not reported to public health agencies—and, based on the event’s speakers, this isn’t a problem health agencies are particularly interested in devoting resources to solving right now. But as rapid tests become the default for diagnosing COVID-19, continued outreach will be needed on how to use them.
Also, as I’ve written before, some PCR testing infrastructure should still be maintained, for cases when someone needs a more definitive test result or wants documentation in case of long-term symptoms. PCR test access will likely get even worse after the federal health emergency ends, though, as insurance plans will also stop covering (or cover fewer costs for) these tests.
Challenges for wastewater surveillance:
Overall, wastewater surveillance is the best source for community-level COVID-19 data, speakers at the ASU event agreed. Official case numbers represent significant undercounts of true infections, and hospitalizations (while more reliable) are a delayed indicator. Wastewater data are unbiased, real-time, population-level—and the technology can be expanded to other common viruses and health threats, health officials pointed out at the event.
But wastewater surveillance is still very uneven across the U.S. It’s clear just from looking at the CDC’s map that some states have devoted resources to detailed wastewater testing infrastructure, with a testing site in every county—while others just have a handful of sites. Funding uncertainty likely plays a role here; speakers at the event expressed some confusion about the availability of CDC funds for long-term wastewater programs.
The CDC’s wastewater surveillance system has also faced challenges with standardizing data from different testing programs. And, at state and local agencies, health officials are still figuring out how to act on wastewater data. Agencies with more robust surveillance programs (such as Massachusetts, which had two officials speak at the ASU summit) may be able to provide success stories for other agencies that aren’t as far along.
Broader testing challenges:
For diagnostic company leaders who spoke at the event, one major topic was regulatory challenges. Andrew Kobylinski, CEO and co-founder of Primary.Health, said that the FDA’s test requirements prioritize highly accurate tests, even though less sensitive (but easier to use) tests might be more useful in a public health context.
Future COVID-19 tests—and tests for other common diseases—may need a new paradigm of regulatory requirements that focus more on public health use. At the same time, health agencies and diagnostic companies could do more to collect data on how well different test options are actually working. While it’s hard to track at-home tests on a large scale, more targeted studies could help show which tests work best in specific scenarios (such as testing after an exposure to COVID-19, or testing to leave isolation).
Company representatives also talked about financial challenges for developing new tests, particularly as interest in COVID-19 dies down and as recession worries grow this year. While a lot of biotech companies dove into COVID-19 over the last three years, they haven’t always received significant returns on their investments. For example, Lucira, the company behind the first flu-and-COVID-19 at-home test to receive authorization, recently filed for bankruptcy and blamed the long FDA authorization process.
Mara Aspinall, the ASU event’s moderator and a diagnostic expert herself, ended the event by asking speakers whether COVID-19 has led to lasting changes in this industry. The answer was a resounding, “yes!” But bringing lessons from COVID-19 to other diseases and health threats will require a lot of changes—to regulatory processes, funding sources, data collection practices, and more.
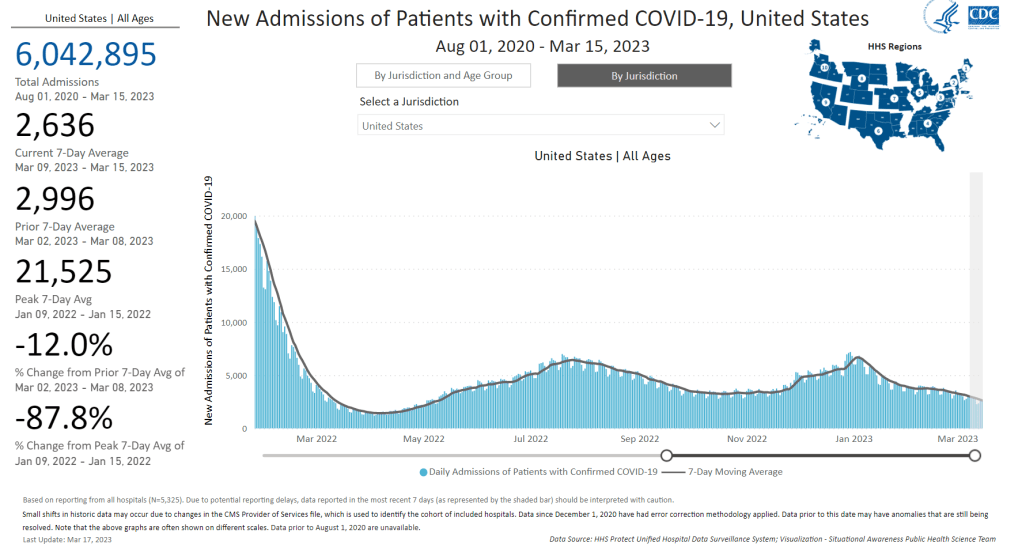
New hospital admissions have fallen significantly from their recent peak in January, but are still much higher than at this time last year. Chart from the CDC.
In the past week (March 9 through 15), the U.S. officially reported about 150,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 21,000 new cases each day
46 total new cases for every 100,000 Americans
20% fewer new cases than last week (March 2-8)
In the past week, the U.S. also reported about 19,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 2,800 new admissions each day
5.9 total admissions for every 100,000 Americans
10% fewer new admissions than last week
Additionally, the U.S. reported:
1,700 new COVID-19 deaths (240 per day)
90% of new cases are caused by Omicron XBB.1.5; 2% by XBB.1.5.1; 0.5% by CH.1.1 (as of March 18)
An average of 40,000 vaccinations per day
The trend continues: COVID-19 spread is still on the decline across the U.S., but it’s a slow decline. These updates are getting pretty repetitive to write, as we’ve been seeing this pattern since late January—which, honestly, I’m taking as a good sign.
Last week, I noted that the drop in official COVID-19 cases (reported to the CDC) was exaggerated slightly because of data delays; three states didn’t report cases in the week ending March 8. This week, the same thing happened for three different states: Texas, Arkansas, and Indiana. We’ll likely continue to see reporting issues like this, as state and local health departments put fewer resources into tracking COVID-19.
Even so, the official case data, hospital admissions, and wastewater surveillance all point to continued decreases in coronavirus transmission. National hospital admissions dropped by about 12% this week compared to the week prior. But there are still a lot of Americans getting severe COVID-19 symptoms, with more than 3,000 people newly hospitalized each week for the last month.
Wastewater surveillance data from Biobot suggest that coronavirus spread is getting lower, but it’s still at much higher levels nationally than we saw at this time in 2021 and 2022. Regionally, the Midwest now has slightly more virus circulating than other parts of the country, but all four major regions are seeing slow declines or plateaus.
In other good news: flu activity is still low nationally, according to the CDC’s flu surveillance. Experts had worried we might see a second flu surge, driven by a different strain of the influenza virus, after the initial surge died down in January. But so far, that hasn’t happened. Almost every state reported moderate or low levels of influenza-like activity in the week ending March 11.
XBB.1.5 continues to be the dominant coronavirus lineage in the U.S., causing an estimated 90% of cases nationwide in the week ending March 18. XBB.1.5.1, a descendant of XBB.1.5, is growing slowly (it caused an estimated 2% of cases nationwide this week) and doesn’t seem to be very competitive yet. The CDC also has yet to break out XBB.1.9 or XBB.1.16, other subvariants that mutated from XBB.
Yesterday, I spoke about wastewater surveillance at New York City School of Data, a civic conference that’s part of the city’s Open Data Week. While the conference wasn’t focused on health or science topics, the organizers required masks and checked attendees’ vaccinations. I also brought my CO2 monitor to the event, and found ventilation was generally good in the session rooms. This conference was a nice reminder that some organizations are still following the data and science on COVID-19 precautions.
American Oversight, a nonprofit watchdog organization that shares government information through public records requests, recently reached a settlement in a lawsuit with the CDC. The settlement’s terms will make it easier for anyone requesting CDC documents to get results.
Early in the pandemic, American Oversight filed a number of FOIA (Freedom of Information Act) requests to the CDC about the agency’s COVID-19 response. Some of those requests were rejected for being “overly broad,” which demonstrated “significant problems with the agency’s FOIA practices” and led to American Oversight filing a lawsuit in May 2020, the organization explains in a recent blog post.
The CDC and American Oversight have now reached a settlement about this records lawsuit—and its terms require the agency to instruct all CDC FOIA officers to be more considerate of “broad” requests. Rather than issuing blanket rejections, FOIA officers should look closely at request descriptions and consult with their supervisors “to ensure all angles of the request have been considered,” according to an email that CDC leadership has sent to staff, in consultation with American Oversight.
This settlement could have huge ramifications for other people requesting records from the CDC (including yours truly) as journalists and researchers continue to investigate how the U.S. handled COVID-19. Thank you to American Oversight for pushing on transparency!
COVID-19 polling data from Axios/Ipsos: During the workshop I led at NICAR last weekend, one attendee (who works at the market research company Ipsos) recommended that journalists and researchers interested in Long COVID data should check out the Axios/Ipsos polling project to track American attitudes on COVID-19. Recent iterations of the poll have included questions about Long COVID, and the polling results are broken out by demographics (age, race, houeshold income). The surveys ask many other COVID-19 questions as well, such as attitudes about masking. To access the data, you can download PDFs from the Ipsos site or spreadsheets from Roper.
CDC provides guidance for Long COVID deaths: The CDC National Center for Health Statistics has started to add information about Long COVID to its guidance for death certificates, following a report that the agency published in December about deaths from Long COVID. The guidance now explains that SARS-CoV-2 “can have lasting effects on nearly every organ and organ system of the body weeks, months, and potentially years after infection,” and can contribute to premature death months or years after a patient’s original infection. For context, see MuckRock’s report on Long COVID deaths from December.
Long COVID gastrointestinal symptoms: Ziyad Al-Aly and his team at the Veterans Affairs St. Louis Health Care System have a new paper in Nature about long-term gastrointestinal symptoms following COVID-19. Using the VA electronic health records database, the researchers compared 150,000 people who’d had COVID-19 to millions of controls. They found people with COVID-19 had elevated risks of many gastrointestinal disorders (including acid-related illness, intestinal disorders, pancreatitis, and more) in the year following their acute cases, compared to the controls. GI symptoms have long been an under-publicized aspect of COVID-19 and Long COVID.
Clinical trial for Long COVID shows promising results: And one more Long COVID study: researchers at the University of Minnesota examined the potential for three common medications to lower risk of Long COVID. This study was a blinded, randomized control trial—the gold standard of medical research. One of the drugs tested, metformin (which is a common medication for type 2 diabetes), led to a significantly lower risk of Long COVID compared to the placebo. The study hasn’t yet been peer-reviewed, but it shows promising results for metformin as a potential Long COVID treatment option.
Examining trust in public health agencies: Another new paper, published this week in Health Affairs, shares results from a survey of about 4,200 U.S. adults (a nationally representative sample) about trust in public health agencies. The survey suggested that trust in federal agencies is connected to perceptions of scientific expertise, while trust in state and local agencies is more tied to “perceptions of hard work, compassionate policy, and direct services.” Survey respondents who reported the least trust in public health cied concerns about political influence, private sector influence, inconsistency, and excessive restrictions.
Some parents lied about children’s COVID-19 status: One more notable survey study, published this week in JAMA Network Open: researchers at Middlesex Community College (in Connecticut) and University of Utah Health, among other collaborators, surveyed a group of 1,700 U.S. parents about COVID-19 protective measures for their children. The study found about 26% of respondents reported lying about or misrepresenting their child’s COVID-19 status in order to break quarantine rules. Common motivations for this behavior were wanting to “exercise personal freedom as a parent,” not being able to miss work or other responsibilities, and wanting kids to have normal experiences. The results suggest “a serious public health challenge” for continued COVID-19 outbreaks and other infectious diseases, the paper’s authors write.
Maternal mortality during the pandemic: MuckRock (where I work part-time) has published new analysis showing a significant increase in maternal deaths during the COVID-19 pandemic, based on CDC mortality data. The death rate for women ages 15 to 44 went from about 29 deaths per 100,000 births in 2019 to 46 deaths per 100,000 births in 2021. Death rates were significantly higher for Black women and in states with more restrictive policies on maternal healthcare. You can find the full analysis (including a selection of state-level data) here.
I have a new story out in National Geographic this week about a growing area of research connecting the gut microbiome—the diverse community of microorganisms that live in our digestive systems—with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), the chronic disease that often occurs after viral infection and has many commonalities with Long COVID. (Here’s a non-paywalled link to the story.)
Two recent papers, both funded by the National Institutes of Health, point to specific differences between the gut ecosystems of ME/CFS patients and those of healthy controls. The new studies built on previous research in this area, but utilized larger patient cohorts than typical ME/CFS studies. Their findings provide avenues for better diagnosing and treating ME/CFS patients, as well as people with Long COVID who meet the criteria for ME/CFS. (Some studies suggest about half of Long COVID patients fall into this category.)
Continued gut microbiome research could identify specific bacterial supplements that help alleviate ME/CFS symptoms, along with new drugs that target specific changes in these patients’ metabolisms and immune systems. But many people with ME/CFS and Long COVID aren’t waiting for the clinical trials; they’re experimenting with the supplement and diet changes that are already available.
One big project in this realm is Remission Biome, a study by two ME/CFS patients who were working scientists before their symptoms became disabling. Patient-researchers Tamara Romanuk and Tess Falor both have experienced “remission events,” in which their ME/CFS symptoms faded after taking bacterial supplements. When they met on Twitter, they started a project attempting to recreate those events—but it quickly grew into a much larger effort to understand how the microbiome interests with post-viral illness symptoms.
I talked to Romanuk and Falor for my National Geographic story. We discussed how to design a study in which the scientists are also the patients, how their project builds on big data in microbiome research, communicating with the patient community, future plans for Remission Biome, and more. Since most of the conversation didn’t make it into my story, I wanted to share it here.
This interview has been lightly edited and condensed for clarity.
Betsy Ladyzhets: I wanted to start by asking how you all came to do this project, specifically replicating remission events that you’d experienced in the past, and how that intersects with other research that’s been done in this area of ME/CFS and the microbiome.
Tamara Romanuk: I had always been planning on trying to replicate the event… It had been in my mind constantly to try to recreate the experience. I actually did, at one point, take another course of amoxicillin [an antibiotic] but I didn’t do anything else. I didn’t do the probiotics. I didn’t do the sort of the full suite that I was that we’re proposing here [in the Remission Biome protocol].
So, it’s something I would have come to on my own regardless. But when I met Tess and she told me that she had had a similar event, it seemed like, okay, this was something we were probably going to do in the future together. It was just a matter of when. I think we must have talked about it even within the first weeks of meeting each other.
Tess Falor: It was, 10 days [after we met]… I had an interesting experience, in that that I didn’t realize that it was the antibiotics that might have done this [alleviated symptoms]. So back when I had my event in 2009, I went gluten-free and started the antibiotics at the same time. And two days later, after I had my major remission, I accidentally ate gluten. And then I felt worse the next day. So for 13 years, I’ve been assuming that it was going gluten-free that made the difference. And I never consider that I could recreate it because I’ve been gluten for that whole time.
It wasn’t until I met Tamara last fall that I realized that, wow, this [remission event] actually could have been the antibiotics. So when that came up, then, Tamara had this idea to try to recreate it. If it was actually the antibiotics that did it, could we create this really extreme remission event?
BL: I see. In terms of identifying the antibiotics, the probiotics, and the other treatments that you’re using in this study, how did you arrive at this protocol that y’all are following?
TR: Yeah, great question. When we decided to recreate it, the plan started as, “let’s take the antibiotics, and let’s throw in some probiotics, and let’s see what happens.” But we’re scientists, so it morphed very, very quickly into something much, much bigger.
Where Tess and I went in our minds was directly to the theory and the models that would have given rise to a phenomenon like this. Instead of starting at a protocol, we went, “this is our pet theory [about why remission occurred], and if our pet theory is right, how do we work backwards and recreate the protocol?” One of the really interesting things about doing it from that angle was that most of the stuff that I had initially thought I would include I actually threw out very, very quickly. The probiotic that I thought we were almost for sure going to use has ended up being, “oh, that actually might have stopped my event from continuing rather than promoting it.”
And we’re working in an age where there’s some really new cutting-edge databases and information sources out there. I wouldn’t have actually been able to do this type of protocol development a few years ago, even. [For example], we knew that we wanted to manipulate tryptophan metabolites in the gut. And so we needed to find strains of bacteria that were involved in tryptophan metabolism. And then we also knew that we wanted really specific metabolites to be produced in the gut and get to the brain. We were able to go into a database and actually follow that chain, identify specific strains of bacteria that would do exactly what we wanted in terms of gut and brain metabolites, and then trace it back to probiotic manufacturers. That’s pretty phenomenal. And that wouldn’t have been possible two years ago.
BL: Yeah, that’s incredible that you could just follow it all the way through like that.
TF: Absolutely. I’ll also mention that we’ve gotten advice from experts, too. Three people who study the microbiome gave us specific advice, and it all kind of converged in the same ideas, the same strains. So that was cool, too.
BL: Actually, it’s interesting that you mentioned tryptophan, because that was one of the processes identified in the recent papers [the two studies that were the focus of my National Geographic story] as well. I think the main one they looked at was butyrate.
TF: Yeah, those are both things that we are thinking about as part of our hypotheses. When those papers came out, we were like, “wow, this is really cool timing.” We read the papers, and found [their findings] line up with what we’re thinking. And we’ve already been thinking about this for months.
TR: There’s a really neat tie-in here in terms of the tryptophan metabolism. Because initially, my theory had been surrounding Robert Phair’s idea of the “Metabolic Trap,” which is, of course dependent on tryptophan. But the [remission] event itself was also incredibly unique because it was a bit psychedelic. Colors were brighter, smells were smellier, the world was amazing, we felt overwhelming gratitude. I tell people that it was a little bit like a mix between doing MDMA and psilocybin mushrooms. But without the hallucination. It was just this overwhelming change in my mood.
So I was thinking about tryptophan, serotonin, the same receptors that might actually get activated during a psychedelic trip. It really seemed that this entire pathway—from tryptophan to serotonin, to some good and some bad molecules like kynurenine, which can be both pro- and anti-inflammatory, and then quinolinic acid, which is absolutely pro-inflammatory in the brain. When you start at tryptophan, you keep going along this pathway, and whatever path it ends up following, you get different neurotransmitter activity going on. [The remission] was a microbiome event, but it’s really a microbiome-mediated event that’s occurring in the brain.
BL: That makes sense, yeah. Because it’s the microbiome that impacts these metabolic processes that then impact what’s happening in the brain, right?
TR: Absolutely.
BL: In terms of tracking what happens when you do this protocol, what are you using to study the changes in your gut and the further progression that you were talking about?
TF: Tamara knows more details than I do, but I’ll just say we are measuring a ton of biomarkers. Everything from specific composition of the gut, to measures of the immune system, like cytokines, and measures of what’s going on in the brain.
TR: We probably have about a thousand metabolites that we’re gonna track. When you consider that we’re doing a lot of these pre[-trial], hopefully during as well as post, it really adds up. It’s actually one of the most exciting parts about the project, for Tess and I. We both have an explicitly systems thinking approach to science, and we love big data. This is something that actually really excites us, we’re going to be able to really dig in.
All of these tests really work in concert as well. The immunogenetics angles are really key for us. And Tess and I have some unique, similar genetic backgrounds, so that’s going to tie in. Then tracking neurotransmitters: actually tracking tryptophan, tracking serotonin, tracking kynurenic acid and quinolinic acid, as well as their ratios. And all of these metabolites.
BL: I see. Yeah, I feel like that will be really interesting to look at all the interactions between these different things. I know you mentioned that you’ve consulted with folks on the protocols, are there other things that you’re doing to maintain the safety of the experiment?
TR: Absolutely. So we’re working with one of my personal GPs [general practitioners], and she’s kind of acting as our GP safety liaison. She will be on hand if anything strange happens. But really what we’re doing in terms of safety is we’re testing ahead of time. We’re making sure we don’t have leaky gut, we’re making sure we don’t have a compromised blood-brain barrier, or making sure that we don’t have certain pathogenic bacteria in our system that could explode if they weren’t affected by the amoxicillin—and lead to a massive, very adverse reaction.
The main tests we’re doing there is from a company called Cyrex, they do these amazing immune tests… And then we’re doing tests like the GI effects from Genova, which will actually tell us if we have high levels of any pathogenic or potentially-pathogenic bacteria in our guts, before we actually start. If any of [certain concerning biomarkers] turn up as being really high for one of us, then we will take some time out, try to correct that specific defect and then proceed again.
BL: That makes sense.
TF: We do have a clinician who has a lot of experience with these specific tests, and specifically with the gut, who’s helping us. In addition to Tamara realizing it was a good idea to do all this pre-testing, she recommended it, too. So she can take a look at our results, and give us her perspective.
TR: One of the things we want to do there is, we want to actually figure out a very simplified testing protocol, which we can suggest to people to do for themselves before they do this [experimenting with supplements]. Because we want to actually bring this work to people who really need it, but we also want to make sure they’re safe. Hopefully, all of the testing that we do will help us arrive at a couple of biomarkers, which we can then tell people, “Look, if you test these one or two or three things, then you can do this without worrying so much about having side effects or adverse consequences.”
Right now, it would cost the regular person probably about $2,000 to test everything that we’re testing, in terms of making sure all these levels are safe. We want to figure out a way to decrease that cost, break that down into specific biomarkers. And then, hopefully, when we move into our Phase Two of Remission Biome—which is actually bringing this work to the patient population—we might even be able to give people these tests, or at least provide them with very significant discounts for these tests.
BL: Yeah, that’s something I wanted to ask you more about, too, is how you have been communicating with other people who want to try this sort of thing. I know from following y’all on Twitter and seeing some of the discussion around this project that folks are so interested. And generally, of course, there’s a big interest among people with Long COVID, ME, other similar conditions just trying to see what would work while there are no official FDA-approved treatments.
How have you found that experience? And, as you look towards Phase Two, what are some of the things you’re going to be thinking about, in bringing these results to other people?
TF: I’ve been talking to people on Twitter. And I would say, we’ve mostly been recommending, “wait until we do this first experiment, so that we can learn from it.” But for people who happen to be getting prescribed antibiotics [for an infection or something similar], then they have their doctor watching them. In that case, we can say, “you want to protect your gut, here are the probiotics that we’re doing, and you might possibly want to do a biome site test while working with your doctor.”
TR: We have had such an overwhelming response. I think hundreds of people must have contacted you [Tess] personally now with a story that they thought might be a revision event, like the one that we’re describing. And hundreds more have said that they’ve had some sort of a positive or negative reaction to antibiotics. And they’ve had ME/CFS, or Long COVID. Those stories are really the jumping-off point for us. We want to put together a very formal survey to actually figure out how people are responding to antibiotics in post-viral illness, in general. There are a lot of clues in people’s stories.
And the response of our community has been almost overwhelmingly positive, but there have been a few people who’ve had pretty severe baseline decreases after taking antibiotics. It’s always hard to know if the antibiotic itself was responsible for that decline or something else. But we really want to delve into that and figure out whether there’s a subset of people that seem to be having negative reactions.
BL: I also wanted to ask about communicating the results from this work. What are you thinking about in terms of both sharing with other people in the community, and also, are you looking towards like a preprint, or scientific publication?
TF: Yeah, we’ll be communicating in real-time with the community on Twitter, and getting input from all the scientists that we’ve talked to. That’s also something that we didn’t really mention yet is, we’ve talked to over 20 different researchers and gotten input from them. We have some that are interested in analyzing our results afterward. So, there’s community communication, but we are also planning to publish it, at least as a preprint.
TR: We’re going to be a great case study. And it’s going to be a great paper. It’s not going to end up in a formal journal, but we’ll definitely pop it into one of the preprint servers.
In addition to the case study, though, we really want to do a meta-analysis. A formal meta-analysis of all the studies that have ever looked at antibiotic use and post-viral illness. We think there are a lot of clues there. One of the things that’s really fascinating to us about this is that there are a number of similar situations that have happened in other conditions. One of the really key ones is PANS, or PANDAS, which often occurs in children when they get a staph infection—and then they get this crazy neurological event where their behavior changes and they develop OCD. Well, turns out, in an enormous number of those cases, if you give them antibiotics of the right type quickly enough—and a lot of the time, it’s amoxicillin plus minocycline, or doxycycline—you can actually completely put that child into remission.
And there’s other disease groupings that seem to have these remission events, in very similar ways. Even Alzheimer’s, many people who have a grandparent with Alzheimer’s will tell stories of moments of complete lucidity. This indicates that maybe brain damage isn’t the ultimate issue, maybe there’s something going on with the communication networks. And that’s really what we’re targeting here [in our research].
BL: That’s really interesting. I was actually just talking to another researcher for this story [Sonia Villapol at Houston Methodist Hospital], who mentioned that her lab, where she is studying Long COVID and the microbiome, has also done work on Alzheimer’s, and even traumatic brain injuries, where there’s some kind of microbiome interaction. I thought that was really interesting. It definitely seems like there’s so much more to be explored here.
TF: Yeah, one of the researchers that we talked to is also doing ME/CFS and Long COVID research, and then Parkinson’s—using probiotics for Parkinson’s. I think a lot of what we’re doing can apply to other conditions, too.
BL: Right. I also wanted to ask if y’all had any other comments about the two recent studies?
TR: Well, I was pretty excited to see butyrate as sort of the highlight molecule. Very early on, we decided that we were going to try to increase our butyrate levels… So we were really excited to see that both of those papers linked to butyrate-producing bacteria, which was really key for us. It’s not just that we want to increase butyrate during the experiment itself, but it’s also a great way to actually help heal leaky gut issues. So it’s a really great intervention.
BL: Yeah, that’s something that has come up a lot in the research I’ve done for this piece—the value of intervening early and trying to help people out before they’re going to have long-term symptoms, or at least in the earlier stages of illness. Which I know is one of the reasons why there’s so much interest in Long COVID, because you’re ideally diagnosing people earlier than what’s historically been the case for ME and some of these other related conditions.
TR: To me, the really exciting application of this is that antibiotics are a very safe intervention that have been used for dozens of years. If it turns out that there’s a chance that taking a quick course of amoxicillin and a tetracycline like minocycline or doxycycline, can take someone who might have developed much more severe Long COVID and then MECFS out of that track, well, that’s phenomenal. If there was actually something that you could go to your doctor and say, “hey, I’m having these Long COVID symptoms, what can we do right now?” And the answer is, “well, it’s pretty safe, why not just give you a week’s worth of antibiotics?” It’s a pretty exciting possibility that we could stop some of these more severe cases.
BL: Yeah, absolutely. I also wanted to ask, in terms of the institutional side of this, what do you think the NIH and other government agencies could be doing to better support this kind of work, and integrating ME/CFS and Long COVID research, as we try to understand the common mechanisms here?
TR: Well, they could actually be treating us. This is really the biggest roadblock: there are hundreds of thousands of people out there who are undiagnosed and untreated, and are trying to biohack their way out of serious post-viral illness. None of these people are seeing clinicians that know what they’re talking about. So, we need treatment centers—but not just the Long COVID treatment centers, where they just tell people to rest, but centers that actually do biochemical testing, figure out what’s actually going on in their bodies, and then doing targeted treatment.
Even if you can’t cure ME/CFS right now, it doesn’t mean that you can’t help people feel phenomenally better, and make sure that they don’t slide from moderate into severe. What you said before is so key, because most of us slide from moderate to severe when we get comorbidities. When we get MCAS on top of the Long COVID, for example. All of these comorbidities compound, and then they get people to a state where almost any intervention is aggravating to their systems, and they literally can’t tolerate light or sound or food. Treating someone at that stage is almost impossible, unfortunately, at this point. So early intervention is really key—but to get early intervention, you need clinicians that know what they’re doing interacting with patients.
BL: Which we don’t have nearly enough of.
TF: Yeah, that’s a major problem. Another angle that I’ll mention is more funding for research, specifically for ME/CFS. There are a lot of really great ME/CFS scientists who haven’t been able to get funding, but they’ve been trying to study this for decades. I keep hearing people saying that there’s these new researchers coming into Long COVID, who don’t really understand a lot about the history and what’s already been done. I think we need more funding for ME/CFS research, plus particularly funding for people who have been doing this for a long time.
TR: Absolutely. One of the things that Tess and I are really excited about is—I guess what we’re going to be calling Phase Three, but it’s starting now—is we’re putting together a hybrid DAO, plus a nonprofit, to actually provide funding for researchers in this area. It’s not just for researchers, it’s specifically for PhD patients.
We really want to tap into this community of sick scientists who’ve been sidelined by ME/CFS, by COVID, by other disabilities, and offer them the chance to actually get back into research in a way that they could do and would be supported. We’re really seeing a new model, a new way of being able to conduct research that is outside of academia, yet has checks and balances and support. Remission Biome has been, hands down, the best thing for my mental health that has happened in 10 years. If I could bring little bit of that to other people in my position—that’s what I would like.
TF: We’ve actually had a lot of people volunteer to help. And I’ve gotten the comment many times, people saying, “this feels so good to use my expertise again.” These are people that have been on disability for 10 years and haven’t been able to do any work or any research. And now they’re able to give their expertise towards our project, and help us gain momentum and move forward, and they’re just really happy about it. I think there’s so much untapped expertise out there.
BL: Yeah, that makes so much sense. And I hope I can keep following this project as y’all expand it.
In the past week (March 2 through 8), the U.S. officially reported about 170,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 24,000 new cases each day
52 total new cases for every 100,000 Americans
25% fewer new cases than last week (February 23-March 1)
In the past week, the U.S. also reported about 20,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 2,800 new admissions each day
6.1 total admissions for every 100,000 Americans
13% fewer new admissions than last week
Additionally, the U.S. reported:
1,900 new COVID-19 deaths (270 per day)
90% of new cases are caused by Omicron XBB.1.5; 2% by XBB.1.5.1; 1% by CH.1.1 (as of March 11)
An average of 50,000 vaccinations per day
Following the same pattern we’ve seen for the last few weeks, COVID-19 spread is still on the decline nationally. Official case counts, hospital admissions, and wastewater surveillance data all continue to point in this direction.
This week, the decline in CDC-reported cases was sharper than it’s been in a couple of months (with 25% fewer cases reported than the prior week). But this may be due to reporting issues, rather than an actual change in transmission patterns: the CDC’s case trends page explains that Florida, Washington State, and Utah all did not report cases in the week ending March 8.
Still, I’m heartened by the fact that hospital admissions—which are reported more reliably—dropped by 13% this week, compared to smaller week-over-week changes over the last month. Wastewater surveillance data from Biobot also continue to show steady declines, though we’re still not close to the national lows observed during this time in 2021 and 2022.
Biobot’s data suggest declining surveillance in all four major regions of the country, with coronavirus levels in the Northeast now dropping below the Midwest, South, and West coast. Some individual counties in the Midwest are still reporting increased viral concentrations in their wastewater; I specifically noted Sheridan County and Teton County, Wyoming in Biobot’s data.
Omicron XBB.1.5 has been the dominant variant in the U.S. since mid-January, and we have yet to see a new subvariant rise to meaningfully compete with it. CH.1.1, which has driven increased transmission in other parts of the world, has remained under 2% of new cases nationally, per the CDC’s estimates.
The CDC’s latest variant update also breaks out XBB.1.5.1, an offshoot of XBB.1.5, at about 2% of new cases nationally. I have yet to see much discussion of this offshoot or how it differs from XBB.1.5; I’ll cover it more in future issues as we learn more. In addition, variant experts are keeping an eye on XBB.1.9, XBB.1.16, and other subvariants that have further mutated from the XBB lineage.
In his latest Substack newsletter, long-time COVID-19 commentator Eric Topol suggests that the U.S. might be in a welcome “break from COVID-19 waves.” He points to XBB.1.5’s dominance and the fact that its rise “was not associated with a surge of COVID-19 hospitalizations or deaths in the United States or elsewhere in the world” despite the subvariant’s increased capacity to spread.
At the same time, Topol explains the problem with our current “high baseline” of continued COVID-19 spread, which leads to continued severe cases among vulnerable people and the ongoing risk of Long COVID. He also explores the potential for another Omicron-like event, which would potentially cause another major surge. His article is helpful for understanding our current COVID-19 moment.
In NYC, where I live, COVID-19 case rates and test positivity are lower than they’ve been since early 2022—while still much higher than we saw last spring post-Omicron BA.1, or in spring 2021 as vaccines were widely rolled out. And the numbers are likely going to get more unreliable soon, as the city begins to wind down public testing sites.
This Tuesday, March 7, will mark two years since the COVID Tracking Project stopped collecting data. For readers who might not know, I was a long-time volunteer for the Project; my early newsletters referenced it so frequently that I added a disclaimer to my “About” page clarifying that the COVID-19 Data Dispatch is a separate, personal endeavor.
I got to catch up with a few fellow COVID Tracking Project alums at the NICAR conference this past weekend, which led me to some reflection on the care and comradery that shaped CTP. The Project was a massive effort to provide U.S. COVID-19 data that would help people understand pandemic trends during a confusing, scary time. But it was also a place of collective learning, innovation, friendship, and so many Slack threads.
I have seen the Project as another form of mutual aid. I’ve given countless hours to CTP over the past year in the form of data entry shifts, analysis, writing, and custom emojis—but those hours have also been given back to me, in everything from Tableau tricks to playlist recommendations. My fellow volunteers, the vast majority of whom I’ve never met in person, are my neighbors. We live in the same spreadsheets and Slack channels; we see the world in the same way.
That final day of data collection feels like it was just yesterday, and also like more than two years have passed. Sometimes, I miss those earlier days of the pandemic, when covering COVID-19 felt like an “all hands on deck” top priority. The beat is lonelier these days, of course. (And I probably don’t have to tell you how few people were wearing masks at NICAR, even among those who used to report on COVID-19.)
Even so, CTP was a model for a newer, better, more collaborative form of data journalism. I hope the COVID-19 Data Dispatch can remain a vestige of those efforts, for as long as it’s necessary.
FDA authorizes joint COVID/flu rapid test, but there’s a catch: Late last week, the FDA issued emergency use authorization to the U.S.’s first at-home, rapid test capable of detecting both COVID-19 and the flu. This could be a really useful tool for people experiencing respiratory symptoms, since COVID-19 and flu can appear so similar. But you might not be seeing this test on pharmacy shelves anytime soon: Lucira Health, the test’s manufacturer, just declared bankruptcy. And the company actually blamed FDA authorization delays for contributing to its financial situation, as it had produced supplies anticipating a fall/winter sale of tests. Brittany Trang at STAT News reported on the situation; read her story for more details.
COVID-19 surveillance stressed out essential workers: For a new report, the nonprofit Data & Society interviewed 50 essential workers from meatpacking and food processing, warehousing, manufacturing, and grocery retail industries about their experiences with COVID-19 surveillance efforts, like temperature checks and proximity monitoring. Overall, workers found that these surveillance measures added time and stress to the job but did not actually provide information about COVID-19 spread in their workplaces. (Companies often cited privacy concerns as a reason not to share when someone got sick, according to the report.) The report shows how health data often doesn’t make it back to the people most impacted by its collection.
Vaccinations vs. Long COVID meta-analysis: A new paper published this week in the BMJ examines how COVID-19 vaccination impacts Long COVID risk. The researchers (at Bond University in Australia) performed a meta-analysis, compiling results from 16 prior studies. While the studies overall showed that vaccination can decrease risk of getting Long COVID after an infection (and may reduce symptoms for patients already sick with Long COVID), the studies were too different in their methodologies to actually allow for “any meaningful meta-analysis,” the authors noted. To better study this question, more rigorous clinical trials are needed, the researchers wrote.
Tracking Long COVID with insurance data: Another notable Long COVID paper, published this week in JAMA Health Forum: researchers at the insurance company Elevance Health compared health outcomes for about 13,000 people with post-COVID symptoms compared to 27,000 who did not have symptoms. The researchers found that, in the one year following acute COVID-19, Long COVID patients had higher risks for several health outcomes, including strokes, heart failure, asthma, and COPD; people in the post-COVID cohort were also more likely to die in that year-long period. I expect insurance databases like the one used in this paper may become more common Long COVID data sources. Also, see Eric Topol’s Substack for commentary.
FDA committee recommends RSV vaccine applications: Finally, a bit of good news on the “other respiratory viruses” front: the FDA’s vaccine advisory committee has recommended the agency move forward with two applications for RSV vaccines. Major pharmaceutical companies Pfizer and GlaxoSmithKline (GSK) have been working on RSV vaccine options; while early data appear promising, clinical trials on both vaccines have found potentially concerning safety signals. The trial populations have been relatively small, making these signals difficult to interpret right now but worthy of additional study. As usual, Katelyn Jetelina at Your Local Epidemiologist has provided a great summary of the FDA advisory committee meeting.
Cover slide from my workshop at NICAR this weekend.
On Friday, I led a workshop at NICAR about covering Long COVID. NICAR is a data journalism conference—the acronym stands for National Institute for Computer-Assisted Reporting, which is an old-school term for data journalism—so my session focused on data sources, along with suggestions for public records requests and for interviewing long-haulers.
My main goal for the workshop was to introduce Long COVID as a worthwhile coverage topic for journalists who aren’t already on the science or health beat. Plenty of science/health reporters (like myself) have written great articles about biomedical research, patient experiences, and other similar topics. But there are many other facets of Long COVID, ranging from its impact on work to the public agencies that should be held accountable for failing to address this crisis.
To that end, I spent part of the session talking about excellent Long COVID articles that don’t focus on science/health topics. I also gave attendees a prompt to brainstorm story ideas for their beats or coverage areas. This led to some interesting conversations about potential local stories on Long COVID clinics, Household Pulse Survey data, tracking disability applications, and more.
Also: as I’ve mentioned previously, I am currently leading a project at MuckRock (where I work part-time) to investigate U.S. government responses to Long COVID. For any journalists who may be interested in collaborating with MuckRock on Long COVID or other public health topics, you can reach out to us here.
Two weeks ago, I shared that I’d recently purchased a monitor to measure CO2 as a proxy for ventilation in my apartment and other spaces. That post led to responses from several readers who’ve also been using CO2 monitors—including Kate Nyhan, a research and education librarian at Yale University who specializes in public health.
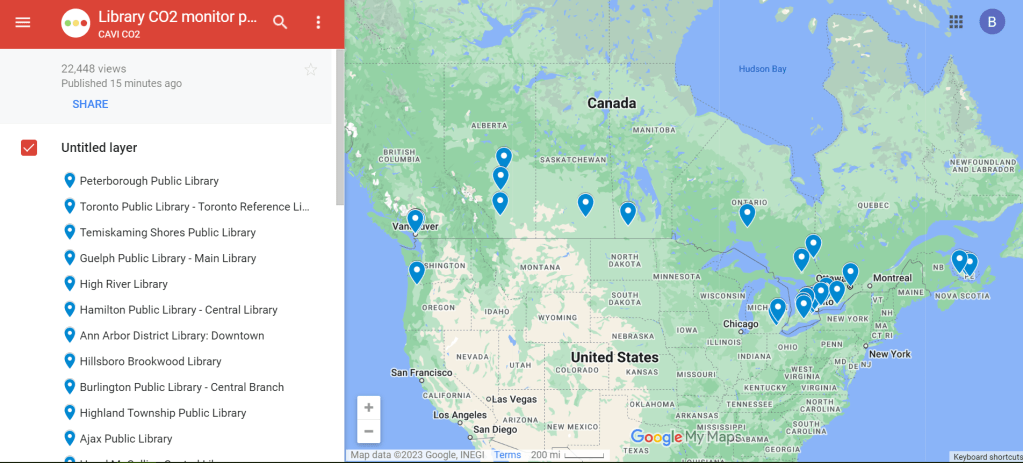
Nyhan explained that, in addition to using a CO2 monitor at her home and workplace, she co-founded a nonprofit that helps public libraries loan out monitors. This nonprofit, called Community Access to Ventilation Information (CAVI), has brought CO2 monitor access to libraries serving about one in five Canadians. In addition to the monitor-lending, CAVI develops educational materials to help library patrons use these tools and collaborates with other air quality initiatives.
I talked to Nyhan and Danielle Cane, CAVI’s managing director, to learn more about the organization and get their tips on using CO2 monitors. Here are the highlights from our conversation.
How CAVI started
Cheryl White, an engineer and air quality expert based in Toronto, Canada, got the idea for this organization in fall 2021. At that time, many people on the COVID-conscious side of Twitter started to express interest in air monitoring, Cane said.
“When we would post our readings from CO2 monitors on social media, a lot of people were saying, ‘This is really cool, I’d love to get involved,’” she recalled. “But it’s just so expensive to access these tools.” Higher-end monitors, like the Aranet device I purchased, can cost around $300.
White had the “bright idea” to partner with libraries as a way to make these monitors more accessible, Cane said. After Cane and Nyhan came onboard, the group reached out to Peterborough Public Library, a library system in a town northeast of Toronto. (Cane and White are both based in the area.)
“Peterborough Public Library was really game to introduce this program,” Cane said. CAVI also worked with the local public health department, which helped gain buy-in for lending out air monitors. The initial Peterborough pilot was launched in spring 2022 with 15 monitors, supported by funding from Canadian and American Aranet distributors.
The city of Toronto later joined the program, followed by other Canadian municipalities. Right now, about 22% of Canadians “have access to a co2 monitor through a public library,” Cane said. CAVI received additional funding in late 2022 to expand further. While the monitor-lending is focused on Canadian libraries, CAVI also produces free, open-source educational materials that can be used in other places.
Why do this in libraries?
Nyhan explained that libraries are well-poised to make air monitors more accessible. “Libraries want to empower community members with access to information,” she said. “In the context of indoor air quality, or COVID transmission risk mitigation, that might be information about airborne transmission, that might be about information about mitigations like air filters… It might be as tangible information as, what’s the number of CO2 parts per million in the space that I’m in right now?”
Lending out CO2 monitors also fits into the “Library of Things,” a concept in which libraries lend out non-traditional items—ranging from home repair tools to arts and crafts materials. As an expensive item that can provide valuable information to the community, CO2 monitors are a great addition to many libraries’ existing collections. In addition, some libraries already have people on staff with public health expertise or existing programming in this area, Nyhan said.
How the program works
The lending system tends to vary from one library to the next, but most places are loaning out CO2 monitors for one week at a time, Cane said: “Especially given the demand in certain areas, like big cities, we find that the one week schedule tends to work out best to both balance, giving people the opportunity to check a variety of settings… and allowing other people to also have that same opportunity.”
Some libraries have seen high demand, especially when the CO2 monitors first arrive at a new library. But as demand levels out over time, patrons might be able to “renew” their loans to keep the monitors for an additional week, Cane explained. Along with the physical monitors, libraries can point patrons to educational resources from CAVI that help interpret the findings.
Interpreting CO2 monitor data
As I’ve found in my own CO2 monitor adventures, there’s a lot these devices can tell you—but also a lot they can’t tell you. The biggest caveat, Cane explained, is that CO2 monitors are “a proxy for ventilation,” not a “proxy for infection risk.” In other words: a really high CO2 reading in a particular space doesn’t necessarily mean that infection is guaranteed, especially if other safety measures are in place. And “a really low reading doesn’t necessarily mean that you will not get infected,” Cane said.
Aranet monitors have a built-in interpretation feature, marking certain CO2 readings as green (good), yellow (less good), and red (bad). But CAVI has produced materials that go into more detail about explaining the ppm (parts per million) measurements. Cane shared one document, designed in partnership with Toronto Public Library, which goes into detail on what higher CO2 readings mean and how to act on them.
Taking action based on CO2 readings
Nyhan used the example of a small car to explain how people may take simple actions based on their CO2 monitors’ results. “Even if it’s just a single person, because [a car is] such a small and tightly enclosed environment, you can very quickly see the impact of breathing out, or opening the window, or changing the air to recirculate or not,” she said. Opening a window or telling the car not to recirculate brings in more outdoor air, causing CO2 levels to get lower.
This is a fairly simple lesson that a library patron might learn during the one week they have with a monitor, Nyhan said: “You learn that, and then you can give the CO2 monitor back to the library so someone else can use it.”
In a larger space, actions based on high CO2 readings might include adding external air filters, opening several windows, or hiring an HVAC engineer to evaluate the ventilation system, Cane said. Not everyone might have the capacity to hire an HVAC engineer, but many people can buy or make air filters; Corsi-Rosenthal boxes are one popular DIY model that can be constructed with commercially available box fans and filters. CAVI has recently partnered with a Canadian high-schooler who’s worked to build these boxes and share accessible instructions.
Nyhan also pointed out that CO2 monitors are “not just for people who control their own spaces” and can easily make ventilation changes. CO2 readings could also inform behavioral safety measures, she said, such as rapid testing before a social gathering in a poorly-ventilated apartment or avoiding certain poorly-ventilated parts of one’s workplace. In some cases, these readings could even be used to advocate for ventilation changes.
Next steps for CAVI
CAVI plans to continue expanding among public libraries in Canada. The organization also works with libraries elsewhere that may want to set up their own CO2 monitor lending programs, Nyhan said. Library staff and users are welcome to reach out to the CAVI team to learn more about the project: “We can share best practices, educational materials, assessment tools, grant proposals,” Nyhan said.
While CAVI, like other air quality citizen science efforts, is currently focused on mitigating COVID-19 risks, its work has implications for many other public health threats. “If we have a wider acceptance of how respiratory pathogens are transmitted, it could be useful to help mitigate other viruses, other bacteria,” Cane said. Improving ventilation can lower the chances of infection for many pathogens and reduce the health risks associated with indoor air pollutants.
Lending out air monitors fits into work that some public libraries are already doing on environmental health, Nyhan said. Libraries might have existing programs about wildfire smoke, radon, and similar air quality threats; COVID-19 and pathogens like it provide motivation for expanding these efforts. “Indoor air quality, and environmental health more generally, is a hot topic that’s only going to get more important,” Nyhan said.