
On July 14, the White House announced that hospitals across America would no longer report their COVID-19 patient numbers and supply needs to the Centers for Disease Control and Prevention (CDC). Instead, they would report numbers through a data portal set up in April by the Department of Health & Human Services (HHS). A July 10 guidance issued by HHS requests that hospitals send reports on how many overall patients they have, how many COVID-19 patients they have, the status of those patients, and their needs for crucial supplies such as PPE and remdesivir.
In some ways, this switch actually makes sense: HHS’ data portal, built by a contractor called TeleTracking, is designed specifically to support more efficient data collection during COVID-19. HHS was already collecting hospitalization data second-hand through state reports, some hospital-to-HHS reports, and the CDC’s old system, called the National Healthcare Safety Network; the new system is more streamlined at the federal level. HHS is also the primary federal entity collecting data on COVID-19 lab test results, through reports that go directly from laboratories to HHS (often bypassing local and state public health departments).
Simplifying data collection to one office—just HHS, rather than HHS and CDC—should theoretically make it easier for hospitals to report their needs and receive aid from the federal governmentquickly. But switching systems during the middle of a pandemic is dangerous. Switching systems during a COVID-19 surge in the Sun Belt when hospitals are being pushed to their full capacity is especially dangerous. Hospital databases, once set up to report to the CDC, must be reconfigured—or worse, exhausted healthcare workers must manually enter their numbers into the new system.
STAT News’ Nicholas Florko and Eric Boodman explore this issue in more detail, but here is one quote from John Auerbach, president and CEO of Trust for America’s Health, which summarizes the problem:
Hospitals are incredibly varied across the country in terms of their capacity to report data in a timely and accurate way. If you’re going to say every hospital, regardless of its size, its resources, its capacity, has to learn a new system quickly, it’s problematic.
It is inevitable that, for the first few weeks of this new system, any hospital capacity data reported by HHS will be rife with errors. And yet, public health leaders, researchers, and people simply living in Texas and Florida need to know how their hospitals are doing right now, so HHS has published the results of their new reporting system only a week after the ownership shift. The new website HHS built to publish these data, called the HHS Protect Public Data Hub, went live this past Monday, July 20. (Veteran users noted that this page copied the homework of the dataset’s former home on the CDC website—same color scheme and everything.)
As I send this newsletter, the HHS Protect dataset was most recently updated on Thursday, July 23 with data as of the previous day. Experts looking at these data, including my fellow volunteers at the COVID Tracking Project, quickly noticed that something seemed off:
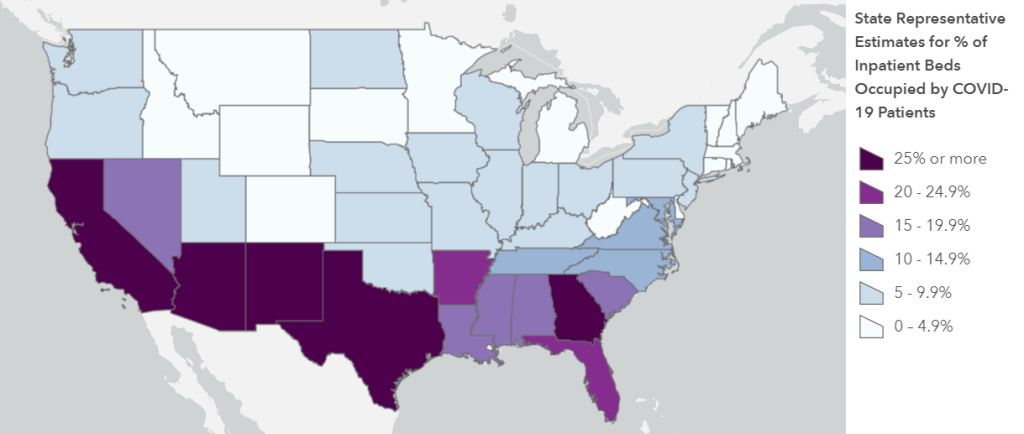
You read that right: according to HHS Protect, 118% of Rhode Island’s hospital beds are currently occupied. As are 123% of its intensive care beds. And that’s just an extreme example; when one compares the hospital capacity estimates in this HHS update to the most recent estimates from the CDC’s system (dated July 14), only 6 states do not show changes of at least 20%. New Mexico, for example, has supposedly seen its number of COVID-19 patients skyrocket 265% in eight days’ time.
Yes, the HHS system is collecting figures from about 1,500 more hospitals than the CDC system did. And yes, 21 states are currently listed as having “uncontrolled spread” by public health research groupCOVID Exit Strategy. But hospitalization figures typically rise slowly, with a slight delay from cases; for journalists like myself who have been looking at this data point for months, the jump reported by HHS is simply not reasonable.
It’s good news for journalists and public health leaders that hospital capacity data is once again publicly available from a standardized, federal source. But I have a lot of questions for HHS. What is the agency doing to support already-taxed hospitals that do not have the staff or resources to transfer their database systems? When hospitals inevitably submit their data with errors, what protocols are in place to catch these issues and ensure all data going out to the public portal is accurate? How will the new system support state public health departments, such as Missouri and South Carolina, that previously relied on the CDC for their hospitalization figures? Will HHS make other datasets available on the HHS Protect portal (such as lab data), and if so, when?
A fellow volunteer from the COVID Tracking Project and I are drafting a strongly worded email to HHS’s press team including these questions and many more; I hope to have some answers for you by next week. In the meantime, you can read Stacker’s story on hospital capacity by state, which does not cite the new HHS figures. Don’t ask me how many times I had to update the story’s methodology.

Leave a comment