After I shared my travel experience last week, a couple of readers reached out asking for more details on using a portable HEPA filter, essentially a small air filter that can be moved from one place to another.
Scientific research has shown that air filters can be valuable tools for reducing the risk of COVID-19, along with other respiratory viruses and pollution concerns, such as wildfire smoke. These filters essentially remove dangerous particles from the air, making indoor spaces safer.
These air filters can be costly (prices range from $50 to $1,000), but may prove to be a helpful long-term investment if used often. My partner and I used ours while traveling, as well as in our apartment when we have guests over and during periods of intense wildfire smoke pollution in New York City.
Here are a few tips and resources about using HEPA filters:
You might see filter options boasting their clean air delivery rate, or CADR. This is a measurement of an air purifier’s effectiveness, telling you how much filtered air the machine can provide in a given timespan (cubic meters per hour, cubic feet per minute, etc). For more details, see this blog post from Air Conditioner Lab.
Understanding your air filter’s CADR is important because it tells you the range in which your device works. For example, a smaller filter with a lower rating might clean the space immediately in front of you on a train, but would not clean the entire car. Smaller filters might also need to run for a longer time to clean an enclosed space (such as a hotel room).
If you’re traveling with an air filter, a portable battery can be helpful to extend the device’s runtime. My filter runs for a couple of hours on its own battery power, but will last for much longer if plugged into a portable battery.
Research and recommendations from air filter providers recommend placing your filter close to you and facing you, to get the clean air delivered as close to you as possible.
If you’re also using a CO2 monitor, it’s important to note that the monitor’s reading likely won’t change due to a HEPA filter. CO2 monitors measure clean outdoor air in a space, so they do not register when existing air is filtered. A monitor that measures particle pollution would be needed to see the difference your filter is making.
Know when to change your device’s air filter! Many devices have built-in indicators telling you to do this (i.e. a light that flicks on when the filter needs replacement), while others will come with instructions recommending a filter change after a given period of time.
Air filter use is not an exact science. While you can find answers to some questions in scientific literature, others might require crowdsourcing on social media or trial and error on your own to find what works best for you. Overall, though, remember that any use of an air filter will be better than taking no steps to clean your air.
I hope this is helpful. If you have more questions (or would like to share your own recommendations), please reach out!
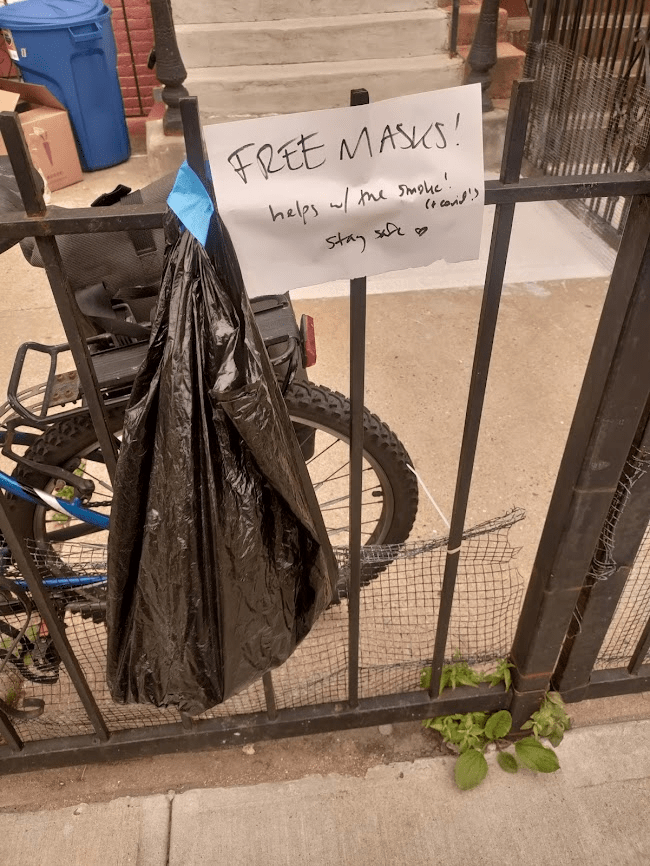
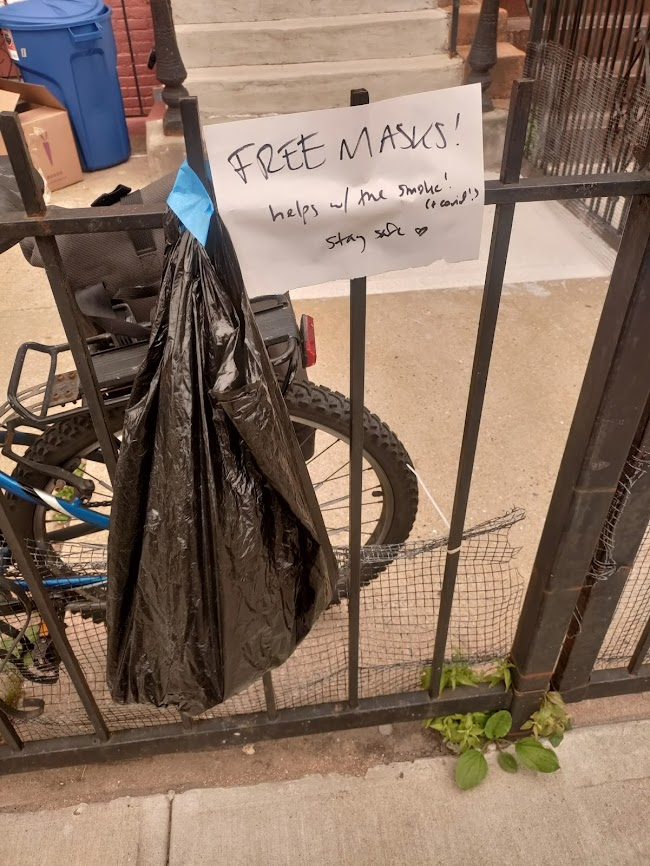
I left some free masks outside my apartment for my neighbors this week. That orange tint on the photo is from the poor air quality in NYC.
This week, much of the eastern U.S. was inundated with wildfire smoke that traveled south from Canada. While fires have been blazing across the country for several weeks, some recent particularly-intense wildfires in Quebec led to smoke so full of pollutants, it set poor air quality records in the U.S.
Americans living in California and other Western states have grown accustomed to wildfire smoke over the last few years; you might remember the orange skies over West Coast cities in fall 2020. But for people on the East Coast (myself included), this week’s smoke was a rude reminder that climate disasters have no borders or boundaries.
The smoke also reminded us how important clean air is for our health. The same public health measures that help reduce COVID-19 risk can also reduce the impacts of wildfire smoke. High-quality masks filter out both the pollution in smoke and coronavirus particles at the individual level; ventilation improvements do this at the collective level. And these health measures help with other respiratory viruses, other types of pollution, chronic conditions like asthma… the list goes on.
For COVID-cautious folks like me who still wear masks in public spaces, the smoke situation this week demonstrated that yes, many people are willing to put a mask on if they understand why it’s needed—and if the masks are widely available. In New York City this week, I saw more people wearing masks than I have since the height of the Omicron wave in winter 2021-2022. Public officials encouraged masking and even gave out masks in large numbers.
In addition to broader mask use, more people have become interested in cleaning the air in their homes and in public spaces. Air filter sales spiked on Amazon this week, CNN reported, as did Google searches for these items. My Twitter feed has been full of recommendations for air-cleaning devices and instructions for building DIY filters.
This is all great to see, but I hope it’s not just a one-week trend. If we invest in cleaner air now—both individually and collectively—we’ll be more prepared for the next round of wildfire smoke. (While the worst has likely passed for now, we’re likely to see more events like this in the future.) And we’ll be more protected against COVID-19 and other respiratory diseases.
With that in mind, here are some suggestions that apply to both COVID-19 and air pollution:
Stock up on high-quality masks, i.e. N95s and KN95s. This STAT article has some helpful information about which masks work well for COVID-19 protection as compared to air pollution. Notably, for COVID-19 protection, it’s more important to mask inside, while for air pollution protection, it’s more important to mask outside.
Buy or make air filters for your home. Air filters can dramatically improve air quality in an indoor space, and you don’t have to spend hundreds of dollars to get one. Corsi-Rosenthal boxes can be easily constructed with less than $100 of materials.
Monitor your local air quality. This can include buying a monitor to measure CO2 or pollutants, or following air quality data through public sources. I’ve personally started checking AirNow.gov, a site run by the U.S. government, and IQAir, a crowdsourced air quality tracking site. Checking local air quality data can inform your behavioral choices, similar to checking local COVID-19 statistics.
Get involved with mask distribution. This week has shown many people are willing to put on a mask, if they understand why it’s needed and can access one. You can help share information and resources, whether that’s getting involved with a mask distribution group in your area or simply donating individually to friends and neighbors. (For example, I left some free masks outside my apartment building this week.)
Advocate for clean air in public spaces. Public buildings can do a lot to improve their air, such as updating HVAC systems and adding air filters to high-traffic spaces. There are already many groups advocating for this, such as parents organizing for ventilation upgrades at their kids’ schools; I hope the recent wildfire smoke adds new motivation to those efforts.
Do you have other suggestions or resources that you’d like to share with other COVID-19 Data Dispatch readers? Email me, and I’ll send your suggestions in a future newsletter issue.
CDC updates ventilation guidance: On Friday, the CDC made its first-ever official air quality recommendation for all indoor spaces, in an update to its overall ventilation guidance. The agency now says all buildings should strive for five air changes per hour (ACH) at a minimum; in other words, clean air should circulate through the space every 12 minutes or more. This update is a victory for many clean air advocates who’ve pushed for better guidelines during the pandemic as a way to reduce the risk of COVID-19 and other respiratory pathogens. As expert and advocate Devabhaktuni Srikrishna said to me on Twitter: “This is exactly the clarity we were pushing CDC for for since last year… Now the question becomes, how does everyone do it in their home, school, and office? How much does it cost? Where do you get it?”
Millions Missing in Washington, D.C.: On Friday, myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and Long COVID patient advocates held a demonstration at the National Mall in Washington, D.C. to show U.S. leaders how chronic disease has pulled millions of Americans out of public life. The demonstration, organized by ME Action and Body Politic, included an installation of 300 cots with hand-made pillowcases created by patients across the country. Each cot is intended to represent people who can no longer work or do other day-to-day activities that were routine before they got sick with Long COVID or a similar chronic illness. You can learn more by watching ME Action’s press conference from the demonstration.
Post-PHE prices for COVID-19 testing: Researchers at the Kaiser Family Foundation put together a new report describing how much Americans will likely pay for PCR and at-home tests now that the federal government no longer supports blanket insurance coverage. At-home test prices range from $6 to $25 per test, depending on the brand and number of tests purchased at once, the KFF analysis found based on a variety of data sources. PCR tests and others performed in healthcare settings range from $25 to $150 per test, with medians around $50. Tests including COVID-19 and other pathogens are the priciest.
Sleep apnea and Long COVID risk: A new paper, published this week in the journal SLEEP, finds that people with sleep apnea have a higher risk of developing Long COVID compared to those who don’t have this condition. Researchers at New York University (and other institutions) compared Long COVID symptoms among adults and children with and without sleep apnea through multiple electronic health record databases, finding people with sleep apnea had up to a 75% higher risk of long-term COVID-19 symptoms. This study was supported by the National Institutes of Health’s RECOVER initiative. Like other papers to come out of RECOVER (including another recent study looking at comorbidities), it’s utilized health records rather than the actual cohort of patients recruited into the NIH’s research program.
Diagnosing COVID-19 through breath: Another notable recent paper, published in the Journal of Breath Research in April: researchers at the University of Colorado Boulder and the National Institute of Standards and Technology have found they can identify whether a patient has COVID-19 by testing their breath. The technique involves using sensitive lasers and artificial intelligence to differentiate between chemicals in a patient’s breath; it’s similar to a breathalyzer for alcohol testing, though more complicated. In addition to COVID-19, breath testing might help identify other diseases.
Long COVID care access challenges: A new paper, published this week in JAMA Network Open, shares the results of a survey by the Urban Institute think tank. The researchers surveyed about 9,500 adults, including 800 with self-reported Long COVID, about their experiences accessing medical care. The long-haulers were more likely to report difficulties with accessing and paying for care, compared to adults who don’t have the condition. To address this issue, the healthcare system needs to develop clinical guidelines for Long COVID, train workers about it, address insurance barriers, and more, the researchers said.
PolyBio announces Long COVID research agenda: Speaking of Long COVID: the PolyBio Research Foundation, a nonprofit devoted to Long COVID, ME/CFS, and other chronic conditions, has announced several research projects that it’s supporting. The projects will evaluate potential biological mechanisms underlying Long COVID symptoms, such as virus persisting in different parts of the body, changes in T cell activity, microclots, and more. PolyBio has a great reputation for pushing ahead post-viral disease research, and I’m looking forward to seeing the results of these studies.
Bivalent boosters hold up against XBB variants: Another new study that caught my attention this week: researchers at the University of North Carolina and North Carolina state health department reported on how well the bivalent, Omicron-specific boosters worked, based on the agency’s surveillance data. The study examined data from September 2022 through February 2023, a period when the BQ and XBB subvariants were dominating coronavirus spread. North Carolina residents who received the bivalent boosters were significantly less likely to experience severe COVID-19 symptoms, the researchers found, but their protection started to wane within a month after receiving the shots.
Resources on indoor air quality in schools: Journalist’s Resource recently updated this list of research and resources for journalists interested in covering indoor air quality in K-12 schools. The update follows a CDC report showing that many public schools across the U.S. have failed to upgrade their ventilation, despite federal funding to do so (which I covered last week). School air quality is a topic that deserves more reporting, especially from local journalists who can dig into how their school districts are doing.
Arizona county starts monitoring for a fungus in wastewater: I’m always on the lookout for new uses of wastewater surveillance, and one promising application could be tracking Candida auris, a fungal pathogen that’s resistant to common drugs and spreads quickly in healthcare settings. The Arizona state health department and a lab at the University of Arizona recently launched a pilot program to track this fungus through Yuma County’s wastewater. Arizona and neighboring southwest states have been a hotbed for C. auris; if this pilot is successful, other states could start similar efforts.
Second Omicron boosters for high-risk adults: The FDA and CDC are planning to authorize a second round of bivalent, Omicron-specific vaccines for high-risk adults, the Washington Post reported this week. This decision will apply to Americans over age 65 and those who have compromised immune systems, with these groups becoming eligible four months after their initial bivalent boosters. It’s unclear exactly when the decision will become official; the FDA and CDC will make authorizations sometime “in the next few weeks,” according to WaPo.
HHS announces (underwhelming) Long COVID progress: This week marks one year since Biden issued a presidential memo kicking off a “whole-of-government response” to Long COVID. The Department of Health and Human Services (HHS) commemorated the occasion with a fact sheet sharing the federal government’s progress so far. Unfortunately, that progress has been fairly minor, mostly consisting of reports and guidance that largely summarize existing government programs or build on existing systems (such as Veterans Affairs hospitals). Many of the Long COVID programs that Biden previously proposed have not received funding from Congress; meanwhile, the National Institutes of Health’s RECOVER initiative, the one program that has been funded, has faced a lot of criticism.
RECOVER PIs recommend action on treatment: Speaking of RECOVER: this week, a group of scientists leading research hubs within the national study called for federal funding that would support treatment. The principal investigators (PIs) of these hubs have developed expertise in Long COVID through recruiting and studying patients, leading them to identify gaps in available medical care for long-haulers. To respond, the PIs recommend that Congress allocate $37.5 million to support Long COVID medical care at the RECOVER research sites. Their proposed budget includes patient outreach, telehealth support, educating healthcare workers on Long COVID, and more.
Ventilation improvements in K-12 schools: The CDC released a new study this week in its Morbidity and Mortality Weekly Report, sharing results of a survey (conducted last fall) including about 8,400 school districts representing 62% of public school students in the U.S. Research company MCH Strategic Data asked the districts about how they’d improved ventilation in their school buildings, along with other COVID-19 safety measures. About half of the districts reported “maintaining continuous airflow in classrooms,” one-third reported HVAC improvements, 28% reported using HEPA filters, and 8% reported using UV disinfectants. The results indicate that many districts have a long way to go in upgrading their indoor air quality.
Flu vs. COVID-19 mortality risk: Ziyad Al-Aly and his colleagues at the VA healthcare system in St. Louis have published another paper analyzing COVID-19 through the VA’s electronic health records. This study, published in JAMA Network, describes the mortality risk of COVID-19 compared to seasonal flu for patients hospitalized during the 2022-2023 winter season. The researchers evaluated about 9,000 COVID-19 patients and 2,400 flu patients, finding that risk of death for COVID-19 patients in the 30 days following hospitalization was about 1.6 times as high as the risk of death for flu patients. Despite great advances in vaccines and treatments, COVID-19 remains more dangerous than other seasonal viruses, the study suggests.
Biobot launches mpox dashboard: This week, leading wastewater surveillance company Biobot Analytics launched a new dashboard displaying its mpox (formerly monkeypox) monitoring. Biobot tests for mpox at hundreds of sewage sites across the U.S., largely through its partnership with the CDC, and will continue this monitoring through at least summer 2023. The new dashboard shows mpox detections nationally over time and monitoring sites by state; it also includes some information on how mpox surveillance differs from COVID-19 surveillance.
Two weeks ago, I shared that I’d recently purchased a monitor to measure CO2 as a proxy for ventilation in my apartment and other spaces. That post led to responses from several readers who’ve also been using CO2 monitors—including Kate Nyhan, a research and education librarian at Yale University who specializes in public health.
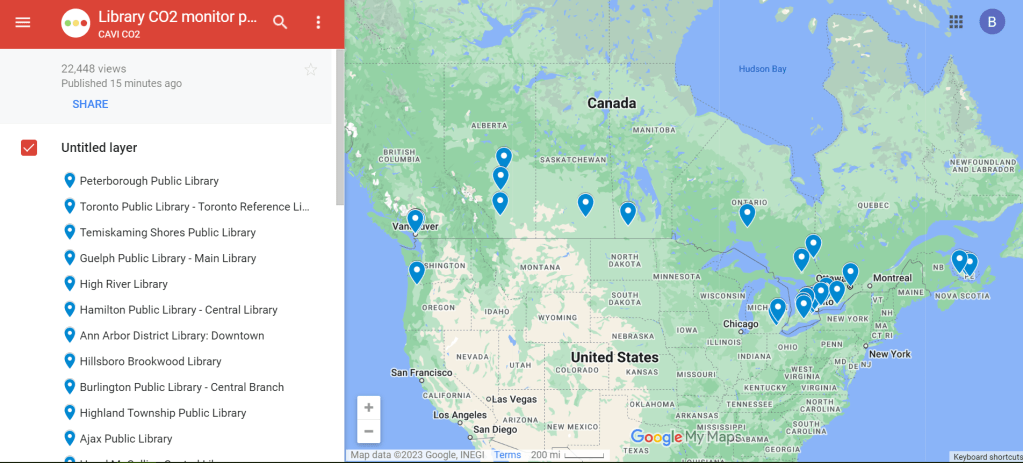
Nyhan explained that, in addition to using a CO2 monitor at her home and workplace, she co-founded a nonprofit that helps public libraries loan out monitors. This nonprofit, called Community Access to Ventilation Information (CAVI), has brought CO2 monitor access to libraries serving about one in five Canadians. In addition to the monitor-lending, CAVI develops educational materials to help library patrons use these tools and collaborates with other air quality initiatives.
I talked to Nyhan and Danielle Cane, CAVI’s managing director, to learn more about the organization and get their tips on using CO2 monitors. Here are the highlights from our conversation.
How CAVI started
Cheryl White, an engineer and air quality expert based in Toronto, Canada, got the idea for this organization in fall 2021. At that time, many people on the COVID-conscious side of Twitter started to express interest in air monitoring, Cane said.
“When we would post our readings from CO2 monitors on social media, a lot of people were saying, ‘This is really cool, I’d love to get involved,’” she recalled. “But it’s just so expensive to access these tools.” Higher-end monitors, like the Aranet device I purchased, can cost around $300.
White had the “bright idea” to partner with libraries as a way to make these monitors more accessible, Cane said. After Cane and Nyhan came onboard, the group reached out to Peterborough Public Library, a library system in a town northeast of Toronto. (Cane and White are both based in the area.)
“Peterborough Public Library was really game to introduce this program,” Cane said. CAVI also worked with the local public health department, which helped gain buy-in for lending out air monitors. The initial Peterborough pilot was launched in spring 2022 with 15 monitors, supported by funding from Canadian and American Aranet distributors.
The city of Toronto later joined the program, followed by other Canadian municipalities. Right now, about 22% of Canadians “have access to a co2 monitor through a public library,” Cane said. CAVI received additional funding in late 2022 to expand further. While the monitor-lending is focused on Canadian libraries, CAVI also produces free, open-source educational materials that can be used in other places.
Why do this in libraries?
Nyhan explained that libraries are well-poised to make air monitors more accessible. “Libraries want to empower community members with access to information,” she said. “In the context of indoor air quality, or COVID transmission risk mitigation, that might be information about airborne transmission, that might be about information about mitigations like air filters… It might be as tangible information as, what’s the number of CO2 parts per million in the space that I’m in right now?”
Lending out CO2 monitors also fits into the “Library of Things,” a concept in which libraries lend out non-traditional items—ranging from home repair tools to arts and crafts materials. As an expensive item that can provide valuable information to the community, CO2 monitors are a great addition to many libraries’ existing collections. In addition, some libraries already have people on staff with public health expertise or existing programming in this area, Nyhan said.
How the program works
The lending system tends to vary from one library to the next, but most places are loaning out CO2 monitors for one week at a time, Cane said: “Especially given the demand in certain areas, like big cities, we find that the one week schedule tends to work out best to both balance, giving people the opportunity to check a variety of settings… and allowing other people to also have that same opportunity.”
Some libraries have seen high demand, especially when the CO2 monitors first arrive at a new library. But as demand levels out over time, patrons might be able to “renew” their loans to keep the monitors for an additional week, Cane explained. Along with the physical monitors, libraries can point patrons to educational resources from CAVI that help interpret the findings.
Interpreting CO2 monitor data
As I’ve found in my own CO2 monitor adventures, there’s a lot these devices can tell you—but also a lot they can’t tell you. The biggest caveat, Cane explained, is that CO2 monitors are “a proxy for ventilation,” not a “proxy for infection risk.” In other words: a really high CO2 reading in a particular space doesn’t necessarily mean that infection is guaranteed, especially if other safety measures are in place. And “a really low reading doesn’t necessarily mean that you will not get infected,” Cane said.
Aranet monitors have a built-in interpretation feature, marking certain CO2 readings as green (good), yellow (less good), and red (bad). But CAVI has produced materials that go into more detail about explaining the ppm (parts per million) measurements. Cane shared one document, designed in partnership with Toronto Public Library, which goes into detail on what higher CO2 readings mean and how to act on them.
Taking action based on CO2 readings
Nyhan used the example of a small car to explain how people may take simple actions based on their CO2 monitors’ results. “Even if it’s just a single person, because [a car is] such a small and tightly enclosed environment, you can very quickly see the impact of breathing out, or opening the window, or changing the air to recirculate or not,” she said. Opening a window or telling the car not to recirculate brings in more outdoor air, causing CO2 levels to get lower.
This is a fairly simple lesson that a library patron might learn during the one week they have with a monitor, Nyhan said: “You learn that, and then you can give the CO2 monitor back to the library so someone else can use it.”
In a larger space, actions based on high CO2 readings might include adding external air filters, opening several windows, or hiring an HVAC engineer to evaluate the ventilation system, Cane said. Not everyone might have the capacity to hire an HVAC engineer, but many people can buy or make air filters; Corsi-Rosenthal boxes are one popular DIY model that can be constructed with commercially available box fans and filters. CAVI has recently partnered with a Canadian high-schooler who’s worked to build these boxes and share accessible instructions.
Nyhan also pointed out that CO2 monitors are “not just for people who control their own spaces” and can easily make ventilation changes. CO2 readings could also inform behavioral safety measures, she said, such as rapid testing before a social gathering in a poorly-ventilated apartment or avoiding certain poorly-ventilated parts of one’s workplace. In some cases, these readings could even be used to advocate for ventilation changes.
Next steps for CAVI
CAVI plans to continue expanding among public libraries in Canada. The organization also works with libraries elsewhere that may want to set up their own CO2 monitor lending programs, Nyhan said. Library staff and users are welcome to reach out to the CAVI team to learn more about the project: “We can share best practices, educational materials, assessment tools, grant proposals,” Nyhan said.
While CAVI, like other air quality citizen science efforts, is currently focused on mitigating COVID-19 risks, its work has implications for many other public health threats. “If we have a wider acceptance of how respiratory pathogens are transmitted, it could be useful to help mitigate other viruses, other bacteria,” Cane said. Improving ventilation can lower the chances of infection for many pathogens and reduce the health risks associated with indoor air pollutants.
Lending out air monitors fits into work that some public libraries are already doing on environmental health, Nyhan said. Libraries might have existing programs about wildfire smoke, radon, and similar air quality threats; COVID-19 and pathogens like it provide motivation for expanding these efforts. “Indoor air quality, and environmental health more generally, is a hot topic that’s only going to get more important,” Nyhan said.
Last week, I wrote about my experience with a CO2 monitor that I recently bought, and have been using to informally study the air quality in my New York City apartment. I asked readers to share their experiences with these monitors, and several of you did!
Here are some snippets from those responses; I hope it will be helpful for some readers to see how other folks are using air quality monitors.
Joyce R.:
I bought a much less expensive one (this one for $60), and I’ve been using it in my downtown office that I go to twice a week (it’s a WeWork facility and I’m in a small 2-person office there; my co-worker and I take turns using it so only one of us is in it at any given time). I of course am always masked in the building—unlike about 98% of the other tenants, sadly—except when I eat (alone in my office, or outdoors on the roof if the weather is good enough). I also have one of those personal HEPA air purifiers going all day. The monitor is showing that usually the range is 800-900, so I’m pretty happy with that.
Mark:
I have an Aranet4 and I’m amazed at the accuracy of it. I put it in my kid’s backpack and could track when he changed classes, went outside or got on the bus. It was REALLY interesting.
In a follow-up email, Mark added:
When I got his class schedule, the changes matched up to the exact 5 minute windows of changes. When I saw high numbers and asked my kid (who couldn’t see the numbers) what the class was like, he said ‘biggest class, 30 kids.’ Yep, the CO2 monitor picked it up. Really really impressive.
Kate:
Not only do I use a CO2 monitor to make risk decisions in my personal life—which shops and concert venues to avoid, are the university shuttles where I work safe (no), what setup of windows and fan make my car safer, what is the natural ventilation air exchange rate… But also, I used CO2 readings to persuade my boss to get facilities to fix a broken vent in my workplace… And EVEN BETTER, the non-profit I co-founded, ‘Community Access to Ventilation Information,’ has been helping libraries in Canada and the US lend patrons CO2 monitors and understand how to act on the readings.
I will be talking to Kate and her co-founder at Community Access to Ventilation Information this coming week, and plan to share a Q&A based on that conversation in next Sunday’s newsletter. If there are any specific questions you’d like me to ask them, please reach out!
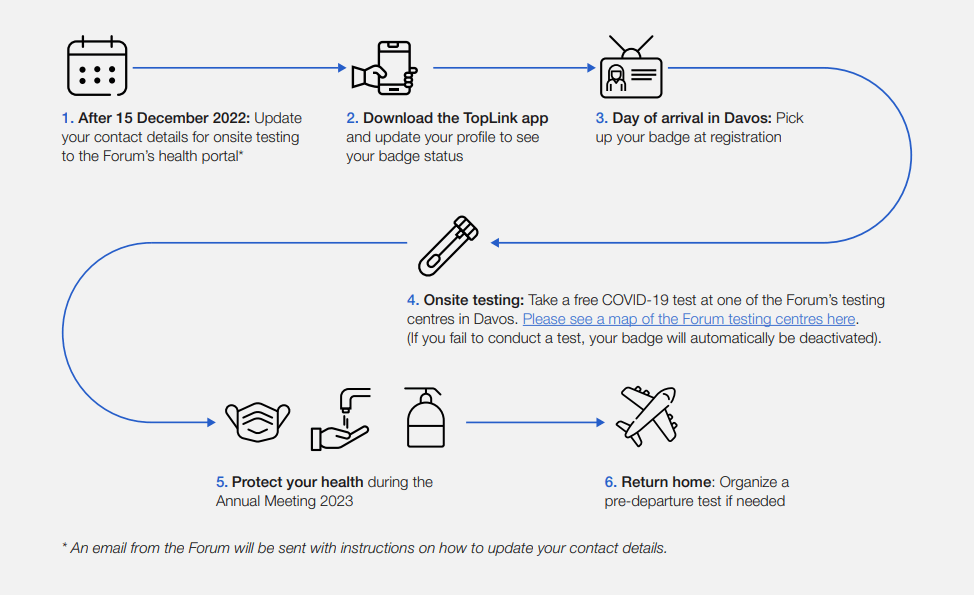
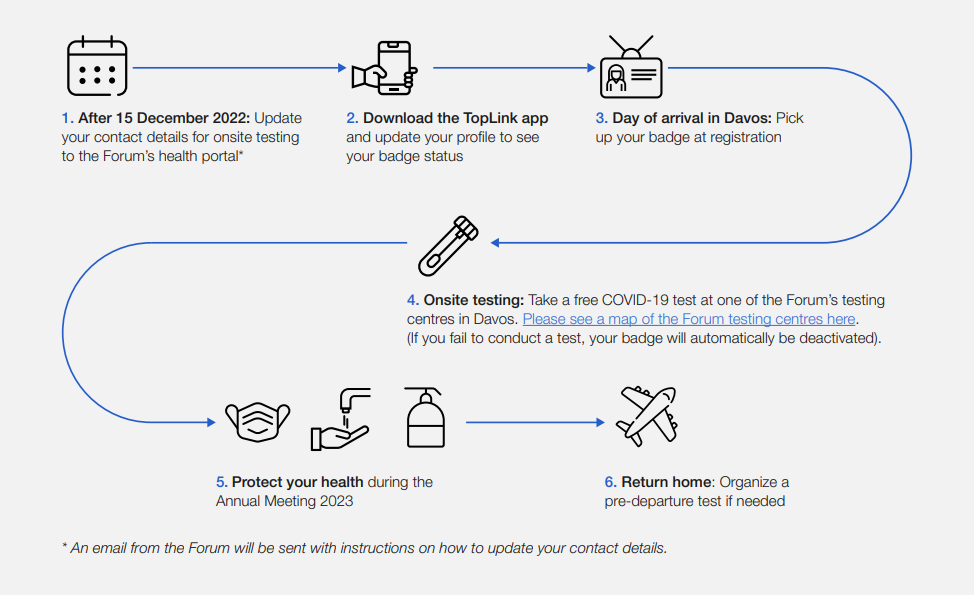
This week, thousands of top political and business leaders gathered in Davos, Switzerland for the World Economic Forum—one of the highest-profile mass events in the world. And the forum, colloquially called Davos after its location, had excellent COVID-19 safety protocols.
The protocols included: PCR tests required onsite (and event badges linked to negative results), masks recommended and available throughout the meeting venue, state-of-the-art ventilation systems, and far-UVC light. Only the best safety measures for the world’s elite, right? Even as many of those elites claim the pandemic is “over”?
News of the Davos COVID-19 protocols has led to media commentary and a Twitter hashtag, #DavosSafe, as public health experts point out that high-quality testing, ventilation, and other measures should not just be for billionaires.
Organizing tip for COVID activists: Highlighting (a) how elites are protecting themselves but not others (#DavosSafe) & (b) higher risk people are being harmed & locked out of society by status quo policies, are the most effective talking points for achieving policy change.
Rather than get angry about the inequities here, I’d like to use Davos as a reminder that many disease mitigation strategies don’t have to be expensive or restricted. Individuals can wear masks, build Corsi-Rosenthal boxes, test before gatherings, and take other relatively cheap measures to cut down on disease spread.
We deserve better. We deserve to be #DavosSafe as the hashtag going around on twitter puts it. Your children deserve to be treated with the care that world leaders are treating each other. Your family deserves to be protected from the disease which is still- unlike the flu- the third leading cause of death in the US. We don’t deserve to be shoved back into poorly ventilated workplaces while our politicians and press assure us that only crazy people would demand to breathe clean air.
New paper outlines the CDC’s COVID-19 data failures: A new study by researchers at Johns Hopkins and Stanford, published this week in PLOS One, outlines missing and poor-quality epidemiological data that hindered the U.S.’s response to COVID-19. The researchers reviewed hundreds of reports by the CDC and other health agencies, finding that public data couldn’t answer key questions ranging from how long immune system protection lasts after an infection to which occupations and settings face the highest COVID-19 risk. (H/t Amy Maxmen.)
White House pushes for improvements to indoor air quality: This week, the White House hosted a summit event on indoor air quality while launching new resources to help building owners improve their air. The summit featured talks by government officials and leading experts, discussing why indoor air quality is important—especially in public facilities like schools—and providing recommendations. (For more details, see this Twitter thread by Jon Levy.) Biden officials are calling on building owners to participate in the “Clean Air in Buildings Challenge,” which includes bringing in more clean outdoor air and enhancing filtration. While these are important steps for health improvements, some experts would like to see the federal government go further by mandating clean air.
Voters do actually support safety measures, poll shows: New polling data from the left-wing think tank Data for Progress suggests that, contrary to popular narratives, a majority of Americans understand that COVID-19 still poses risks and support safety measures. For example, 74% of likely voters support the federal government requiring schools and workplaces to improve indoor air quality, and 70% of likely voters understand that certain groups (disabled people, seniors, etc.) remain at high risk from COVID-19.
New study demonstrates long-term risks of infection: Another notable new paper from this week: researchers in Scotland used health records and surveys to follow about 33,000 people who tested positive for COVID-19, compared to 63,000 who did not. The patients were all surveyed at six, 12, and 18 months post-infection; between the six- and 18-month surveys, about 6% of the cohort had not recovered while 42% reported only partial recovery. As one of the biggest studies to date that doesn’t rely solely on health records, this paper shows how Long COVID can be devastating long-term for patients.
Further research backs up testing out of isolation: And one more study I wanted to highlight this week: researchers at the University of California San Francisco examined how long people remained contagious after a coronavirus infection. The study included over 60,000 people who were tested at community sites in San Francisco. Five days after symptoms started, the researchers found, about 80% of patients infected during the Omicron BA.1 period were still positive on rapid tests—suggesting that, as other studies have found in the past, five days is an inadequate isolation period. Rapid testing out of isolation is the way to go.
The author in a 3M respirator (with P100 filters), on the plane to Denver, Colorado.
This weekend, I traveled to Denver, Colorado for the final trip in an early-career fellowship which has covered some travel and trainings for me this past year.
Of course, going anywhere on a plane right now, during an intense COVID-19 surge, is not something I’d normally choose to do. This is basically my one plane trip of the summer; all my other travel has been by train and/or car. (And the fellowship event itself had some safety measures in place, eg. required masks and rapid tests.)
But I know a lot of people are traveling by plane right now—I know, because I saw so many of them at JFK Airport. So, I wanted to share a few things I did on this trip to reduce my risk.
First: I bought a respirator. These devices, considered to be a step above N95s/KN95s, are intended for use in occupational settings, such as for workers in chemical plants or firefighters going into smoke. You can read more about them on this CDC NIOSH (National Institute for Occupational Safety and Health) page.
I think of mine like a reusable N95 mask, with great longevity and an excellent seal to my face. I ordered one from 3M, which has several NIOSH-approved options. I also learned more about different respirators at Patient Knowhow, a site with reviews of a few major N95-equivalent options. (I recently talked to the site’s founder, Devabhaktuni Srikrishna, for an upcoming article on ventilation.)
plane trip with respirator was a success! TSA asked me to take it off when I went through security (so I put on a disposable mask for a few minutes), but otherwise I had no issues. pic.twitter.com/SDUA4slIQY
It’s important to note that, if you get one of these respirators, you may need to order air filters separately. I got P100 filters, which are the highest grade. Another add-on may be an exhalation valve filter, which cleans the air you exhale out of your respirator (basically, further ensuring that you aren’t getting other people sick as you wear it).
Now, one challenge with these respirators is that they may freak people out a little. I feel like a bug-eyed sci-fi villain with mine on; though I’m well-accustomed to NYC’s blase attitude towards weird behavior, so I don’t mind if I freak people out. For others, this could be a greater concern.
Respirators also aren’t common mask options yet, though they seem to be growing more popular—my Twitter selfie of me in my respirator on the plane got over 200 likes. But they aren’t yet well-known in transit settings. While I personally didn’t have issues (other than a bit of confusion at JFK’s security screening), I know that others have been told to take these off on flights. It’s good to have a backup N95/KN95 in case that happens.
Second: I follow guidance from ventilation experts. If you’d like to read about how plane ventilation works, masking options, and other small ways to improve travel safety, you can find a lot of this advice on Twitter. “Ventilation Twitter,” as I recently described it to a journalist friend, is generally very welcoming and willing to triage questions.
One key piece of advice: while I kept my respirator on throughout my flights (seriously, the briefest breaks possible for water and food), I made especially sure to stay masked while planes were at the gate or landing. These are the points in a flight when the plane’s ventilation system isn’t switched on, making masking more important.
Saahil Desai provides a helpful explanation of these priority periods for masking in a recent Atlantic article. Though I’d like to note, some experts have suggested that the article downplays the importance of masking as much as you can throughout a flight and using other safety strategies as well.
More helpful threads on this subject…
Top 10 tips everyone should know about wearing #N95 & #elastomeric masks.
Third: I avoid indoor dining as much as possible. This is, of course, one of the highest-risk settings for catching the coronavirus, because you have to take your mask off to eat or drink—while others nearby are also unmasking to eat or drink.
Sometimes, one can be put into tricky situations when there are truly no outdoor dining options (such as on a long airplane trip). But even in that scenario, there are ways to reduce risk. For example, when I needed to eat breakfast at JFK Airport, I found a corner of an unused gate where I could be relatively far from other people, rather than sitting in a crowded food court area.
I also appreciated that the other fellows in my group followed my recommendation for an outdoor dinner on Thursday evening, before our official activities started!
And finally: lots of testing. Remember, rapid tests can indicate whether you’re actively spreading the coronavirus, but PCR tests are still the gold standard for accuracy. I try to get PCR tests before and after travel or large gatherings, to be certain of my status. (Though I acknowledge that I live in NYC, where public testing is still available, albeit in decline.)
This trip went from Thursday to Saturday, with the riskiest event being an indoor dinner on Friday evening. My tests included: PCR test on Wednesday (same-day results); rapid test on Thursday morning; rapid test on Friday morning; rapid test on Friday evening (right before the dinner); rapid test on Saturday morning; and a planned PCR test for next Wednesday or Thursday. Rapid tests and symptom monitoring were also required for the rest of my group.
Is all of this inconvenient? Sure, somewhat. But I consider it worthwhile to have a safe trip and protect the people around me. If you have other safety tips or questions on this topic to share, please reach out and let me know.






{kind=link}