Utah hasn’t hit 70% adult vaccinations yet—but a recent data error led state officials to erroneously announce the benchmark had been hit. Spencer Cox, Utah’s governor, posted an apology on Twitter that drew attention for his commitment to transparency and accountability.
Welp. We screwed up. Because of a reporting error we have not yet hit 70% on our adult vaccinations. I promised to admit our mistakes and hold us accountable. I hope you will forgive us—and know we have made changes to ensure it won’t happen again. pic.twitter.com/NZK8A8gabt
“My fellow Utahns,” the statement opens, “We screwed up. And I sincerely apologize.” Cox goes on to explain the data error, affirm the state health agency’s commitment to accurate numbers, and emphasize the need for easily-accessible vaccinations.
The data error arose from the challenge of matching state and federal data. In Utah, like in every other state, a small number of vaccine doses are administered under the federal government’s purview via the federal-pharmacy chain partnership, the Department of Defense, Indian Health Services, and other agencies. When Utah officials added the federal doses to state numbers, they initially found that 70% of adults had received at least one shot—the true number is just over 67%, Cox said.
Also, while poking around Utah’s COVID-19 website to better understand the data error, I found that the state has some great vaccine promotions going. These include the option to request a free mobile vaccination clinic in your community and this truly incredible “Vaccine Mythbusters” video. With the help of these initiatives, Utah is sure to hit 70% soon.
The U.S. missed President Biden’s big vaccination goal: 70% of adults vaccinated with at least one dose by July 4. As of July 3, we are at 67% of adults with one dose, and 58% fully vaccinated.
I did a data-driven look at the vaccination goal this week in a story for the Daily Mail. The story focuses on which parts of the country have met the goal—and which areas fell short. Those under-vaccinated areas are highly vulnerable to the Delta variant (B.1.617.2), which is now spreading rapidly in many of those pockets. Reminder: the Delta variant is much more transmissible than even the Alpha variant (B.1.1.7), and its presence is doubling in the U.S. every two weeks.
There are over 1,000 counties in the U.S. with one-dose vaccination rates under 30%, CDC Director Dr. Walensky said at a press briefing last week. The U.S. has about 3,100 counties in total.
Is your county one of them? Check it out on this interactive map, reflecting data as of July 1:
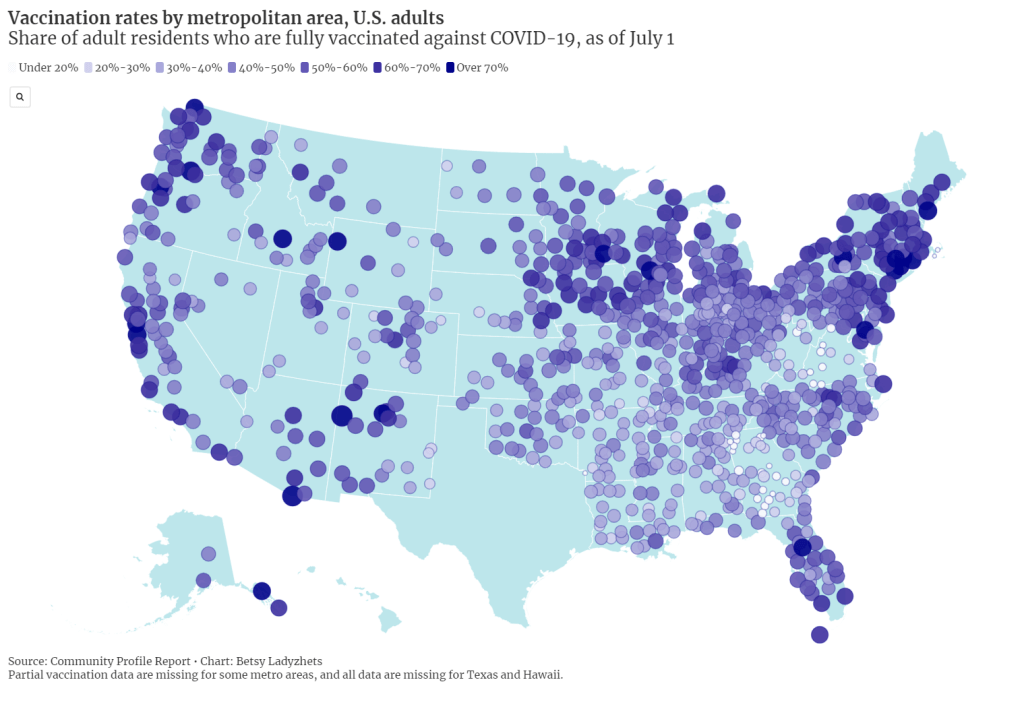
I also made a map showing vaccination rates by metropolitan area. You can clearly see clusters of high vaccination in the Northeast and on the West coast, while parts of the South and Midwest are under-vaccinated. Note that Texas is missing in both this dataset and the county-level data due to issues in the state’s reporting to the CDC.
For my Daily Mail story, I also asked two of the COVID-19 science communicators I most admire to explain the significance of that missed 70% goal. I talked to Dr. Uché Blackstock, physician and founder of the organization Advancing Health Equity, and Dr. Katelyn Jetelina, epidemiologist at the University of Texas and writer of the Your Local Epidemiologist newsletter.
Here are both of their takes on the missed goal:
So, we didn’t meet the 70% goal. It means that we fell short. It also means that we just don’t have enough people vaccinated, not even close, to reach herd immunity.
To me, as an epidemiologist, someone in the field and also someone within a community, it means that we have reached—or are about to reach—saturation [of the vaccine market]. We need to start becoming very innovative about how to address vaccine hesitancy, as well as how to address vaccine equity.
That’s really going to be the next phase of public health approaches. And then, how do we go about doing this… You know, we’re well beyond billboards now. We really need to mobilize a grassroots movement. We need to listen about concerns, we need to educate about these concerns.
And then, we need to make vaccines more accessible. Especially among pediatrics, where—pediatrician offices can’t store the vaccine. So we have to go to schools and really engage with families in a “nontraditional sense.”
Dr. Katelyn Jetelina
This 70%, especially for one dose, is sort of an arbitrary number, because we know that being fully vaccinated is what’s needed to fully protect you against variants. I think it was obviously wise and aspirational to have a goal. But at this point, because we’re basically seeing the number of people vaccinated decreasing weekly, and substantially since last April… I think we need to change our perspective.
We had the early adopters who came in droves to get vaccinated. We’re not going to see the same numbers anytime soon. And so, I think that this idea of having a goal, while it’s aspirational, I think that we have to put that aside and think more realistically about the challenges we’re dealing with.
And the challenges we’re dealing with are actually quite complicated… There are still access issues, although I do think the Biden administration is doing—at least trying to do a substantial job in knocking down those barriers. They’re providing transportation, childcare, increasing the access points for getting vaccinations, encouraging small businesses to offer their workers paid sick leave to get vaccinated and to recover from the vaccine.
But I think this other issue that we’re seeing among people who are not vaccinated, it varies depending on the population, the geographical area. We know rural populations are less likely [to get vaccinated]. And we know that, among the “wait and see” group, about half of those are people of color.
I hate to blame it on this so-called “vaccine hesitancy” because I don’t think it’s that simple. I do think, though, that there is a significant distrust of government, there is distrust of the healthcare system, and there is a lot of misinformation out there about the vaccines. All of these are essentially creating the perfect storm that is preventing us from getting to this aspirational [70%] number.
But here, we’re at this point where it’s a race against the variants, and I think that we just have to get as many people vaccinated as possible. I know that sounds incredibly vague, but that really is the goal.
Dr. Uché Blackstock
I made a third chart for today’s issue, visualizing vaccination rates by state from March through June. It really shows how vaccine enthusiasm has leveled off, just about everywhere in the country—but the plateaus started earlier in many of those states that have lower rates now.
I typically try to avoid anything approaching medical advice in the COVID-19 Data Dispatch, as I am a journalist with just an undergraduate biology degree and a couple of years of science reporting experience. But this week, it feels appropriate to wholeheartedly, unambiguously encourage vaccination.
I know the audience for a publication like this one skews towards people who probably have their shots already. Rather, I want to encourage you to find those people in your community who aren’t yet vaccinated, and help them take that step.
Recent research suggests that lotteries and other large-scale incentives do not significantly encourage vaccination; instead, we need small-scale incentives. One-on-one conversations with people, opportunities for concerns to be voiced and addressed, appointments that can be tailored to the individual’s needs. Anything that you can do to play a role in these initiatives, please get out there and do it.
Of course, if you (or your friends/family/community members/etc.!) have questions about vaccines, or anything else COVID-19 related, you know where to find me. Inquiries welcome at betsy@coviddatadispatch.com.
Following the end of the federal public health emergency in May, the CDC has lost its authority to collect vaccination data from all state and local health agencies that keep immunization records. As a result, the CDC is no longer providing comprehensive vaccination numbers on its COVID-19 dashboards. But we still have some information about this year’s vaccination campaign, thanks to continued CDC efforts as well as reporting by other health agencies and research organizations.
This week, the FDA authorized Novavax’s updated COVID-19 vaccine. Here’s why some people are excited to get Novavax’s vaccine this fall, as opposed to Pfizer’s or Moderna’s.
Last week, I asked you, COVID-19 Data Dispatch readers, to send me your stories of challenges you experienced when trying to get this fall’s COVID-19 vaccines. I received 35 responses from readers across the country, demonstrating issues with insurance coverage, pharmacy logistics, and more.
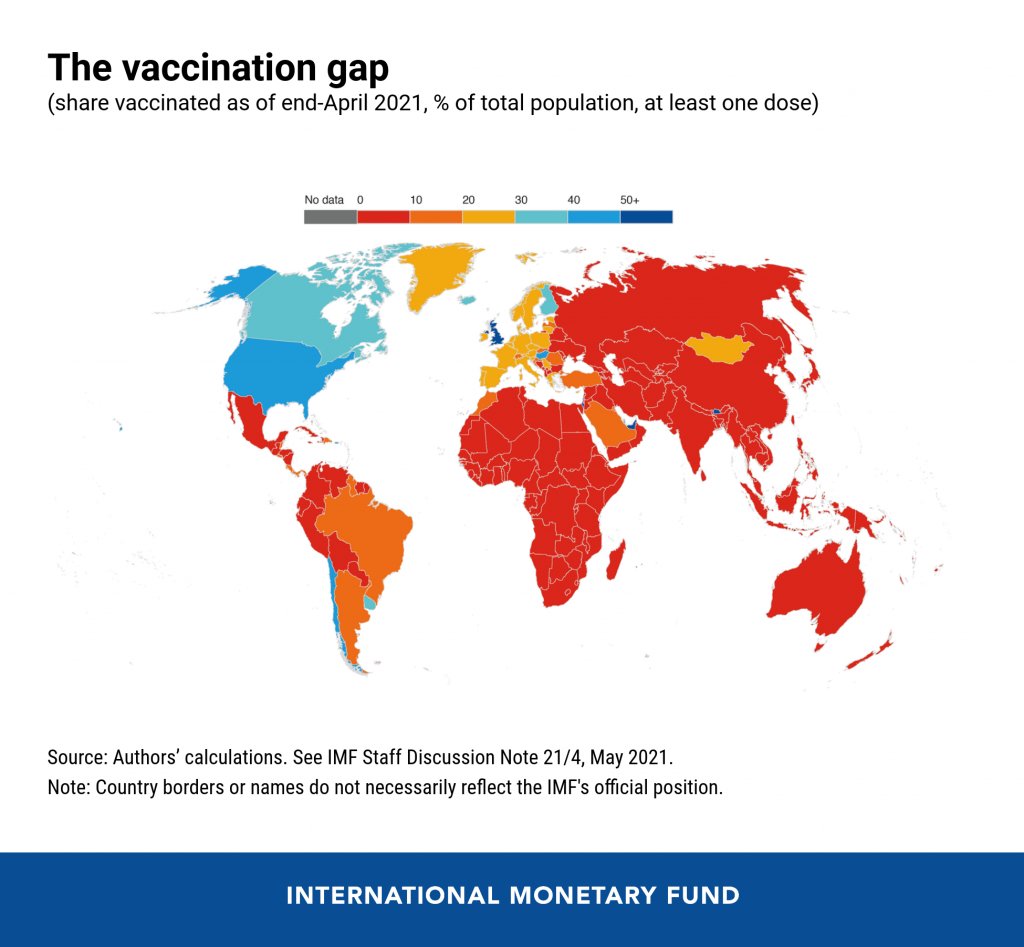
In the reader survey I sent out a few weeks ago, I asked, “What is one question you have about COVID-19 in the U.S. right now?” One reader responded with an inquiry into vaccine equity: “What will it look like when the U.S. is ‘open’ and vaccinated and many other parts of the world are not?”
That question feels especially relevant this week. On Thursday, the Biden administration made a big (and long-awaited) announcement: the federal government is sending 25 million vaccine doses from America’s stockpile to other countries. The administration has previously promised to send at least 80 million doses abroad by the end of June, but this week’s announcement included more details—such as countries that will receive these initial doses and other logistics.
Out of the 25 million, about 19 million doses are going to COVAX. COVAX, a global effort run by the World Health Organization and other international government bodies and philanthropic organizations, brings vaccines to low-income nations at no cost. The COVAX doses will go to India, other parts of Asia, Central and South America, and Africa, Bloomberg’s Josh Wingrove reports.
The remaining 6 million doses will be sent directly to countries, including Ukraine, Kosovo, Haiti, Georgia, Egypt, Jordan and Iraq. Some doses are going directly to India as well—while the worst of this nation’s surge may be over, it’s still facing high case counts, full hospitals, and a terrifying “black fungus” linked with the Delta variant (B.1.617).
At first glance, this might seem like a noble move on the Biden administration’s part. The U.S. is seeing low case numbers and widespread reopenings, so we can share some supplies to “help the pandemic around the globe,” as COVID-19 response coordinator Jeff Zients said at a briefing on Thursday.
But 25 million doses—or even the 80 million doses that the administration has promised by the end of this month—is a drop in the bucket compared to actual international needs. For example: COVAX needs 1.8 billiondoses to vaccinate about half the adult population in low-income countries. COVAX has specifically prioritized 92 low-income nations, representing a total population of 3.8 billion.
That 1.8 billion dose number is a highlight of a major report released last week by the Rockefeller Foundation, a global charitable foundation, discussing what it would take to vaccinate the world. I covered the report for Science News. According to this report, Gavi (the Vaccine Alliance), an international public-private body that runs COVAX, needs to raise $9.3 billion in order to pay for those 1.8 billion doses. Gavi has been working to raise this money from countries and independent donors at a global health summit this past week.
While $9.3 billion might seem like a massive price tag, the cost of failing to provide these vaccines would actually be far greater. The global economy may lose up to $9.2 trillion if richer nations fail to support equitable vaccine distribution, according to an estimate from the International Chamber of Commerce.
So far, the U.S. has administered about 300 million vaccine doses (as of yesterday), covering over half the total population. In a number of low-income countries, less than one percent of the population has received a dose. Tedros Adhanom Ghebreyesus, Director General of the WHO, said at a recent assembly that, if all doses administered globally had been sent out equitably, the doses would have covered “all health workers and older people.” Instead, high-income nations are largely protected while low-income nations are vulnerable to future surges and highly-transmissible variants.
Through this lens, the 25 million dose shipment announced this week is far from impressive. It’s a useful start, certainly, but it’s not going to end the pandemic anywhere. Even the 80 million doses promised by the end of June is a tiny number—about 4% of the doses COVAX is hoping to obtain. It’s also only 11% of the doses that vaccine makers have pledged to deliver to the U.S. by the end of July, according to Bloomberg.
That larger June shipment has also been held up because the Biden administration is planning to send AstraZeneca vaccines—which are under review from the FDA because they were produced at the Emergent factory that infamously wasted millions of Johnson & Johnson doses. The AstraZeneca vaccine is not authorized for use in the U.S., so of course it will make up the majority of the doses we send abroad this summer.
Speaking of unused doses: the Biden administration may also start sending unused doses from states to other countries, POLITICO reported this week. The administration wants to get thousands of Pfizer, Moderna, and J&J doses—on the verge of expiring—to countries that would actually use them. While this possible policy hasn’t yet been realized, it hammers home a clear message: the U.S. will donate “unwanted” vaccine doses only when we are absolutely certain that we don’t need them here.
Now, let’s return to our reader’s question. What happens when the U.S. is safely vaccinated, but other parts of the world aren’t?
From a health standpoint, the U.S. will probably be okay. The vaccines are very effective, even against variants—likely protecting the country from another major surge. We will need careful surveillance to guard against future variants that may evolve beyond the vaccines (see: last week’s issue), and it’s possible that overly zealous reopening this summer will lead to outbreaks next fall and winter. But seniors and other vulnerable people would be more protected than they have been in past surges, and booster shots (for the variants) will likely be on their way soon. In short, America’s wealth will protect us.
Around the world, however, outbreaks will continue. Every time a new person gets infected with the coronavirus, the virus has a new opportunity to mutate. And with every mutation, the virus learns to spread faster, to evade common treatments, even to evade vaccines. Thanks to globalization, as long as the virus is a threat anywhere, it continues to be a threat everywhere.
Plus, as low-income nations suffer from continued outbreaks, the global economy will continue to suffer. Out of that $9.2 trillion cost estimated by the International Chamber of Commerce, the majority will likely fall on wealthier nations (like the U.S.) that rely on other countries for products and labor.
“The pandemic itself has gone beyond a health crisis — it has now gone into an economic crisis,” Christy Feig, the Rockefeller Foundation’s director of communications and advocacy, told me when I spoke to her for Science News. “The only way to unchoke the economy is by getting the vaccines to as many countries as possible, so that we can stop the spread of the disease before more variants come.”
In the past week (May 29 through June 4), the U.S. reported about 100,000 new cases, according to the CDC. This amounts to:
An average of 14,000 new cases each day
31 total new cases for every 100,000 Americans
35% fewer new cases than last week (May 22-28)
Last week, America also saw:
18,000 new COVID-19 patients admitted to hospitals (5.5 for every 100,000 people)
2,300 new COVID-19 deaths (0.7 for every 100,000 people)
70% of new cases in the country now B.1.1.7-caused (as of May 8)
An average of 1 million vaccinations per day (per Bloomberg)
Cases continued to fall this week, with a seven-day average now under 20,000 new cases a day. This is basically the lowest number we’ve seen in the U.S. since spring 2020—though it’s important to note that the U.S. was doing minimal testing at that time, so the true case numbers in March 2020 were likely much higher than what was reported.
Also, last weekend’s holiday—like past holidays—likely resulted in fewer cases being reported early this week. Many testing sites and public health departments close for holidays, and it’s hard to imagine who might want to go get a nose swab on Memorial Day. Fewer than 10,000 new cases were reported last Monday and Tuesday, according to the CDC, followed by double that number each day for the rest of the week.
Despite such low overall case numbers, infection rates remain high for the unvaccinated. A recent Washington Post analysis adjusted COVID-19 infection rates by subtracting vaccinated residents from state populations. In Washington state, for example, the case rate among unvaccinated residents is “as high as it was in late January.”
Also, as policy researcher Julia Raifman pointed out on Twitter, fewer than half of the lowest income workers with kids are vaccinated—likely because of vaccine accessibility issues. Workers in this income bracket are also more likely to report that they had to miss work due to a COVID-19 infection, compared to higher-income Americans.
Nationwide, about half of the U.S. population has had at least one dose, including 63% of adults and 86% of seniors. The rate of vaccinations has slowed this past week (now only one million doses administered a day)—though this may in part be a holiday reporting lag as well. Biden’s administration continues throwing incentives at the problem in the hopes of meeting his July 4 goal.
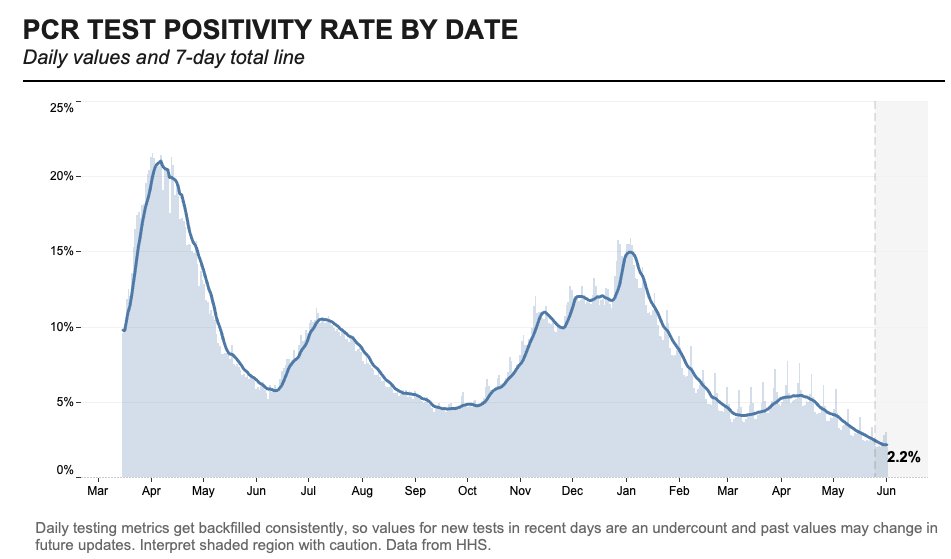
Testing numbers have also fallen in recent weeks, likely because vaccinated Americans have few reasons to need a test. Data watcher (and former COVID Tracking Project volunteer) Conor Kelly noted that we’re averaging under 1 million tests a day for the first time since fall 2020. At the same time, though, the national positivity rate for PCR tests is lower than ever—it hit 2.2% on June 1.
Despite the drop in tests, the positive rate is at an all-time low, reaching a 7-day total of 2.2% through 6/1 according to HHS data
Things are looking pretty good here in the U.S., though some experts say a summer or fall surge could still be possible if we relax restrictions too much. Other countries without vaccine access are not nearly so lucky.