
Anyone who regularly rides the New York City subway knows that the city’s mask requirement for public transportation has been unenforced and loosely followed—especially in the months following last winter’s Omicron surge.
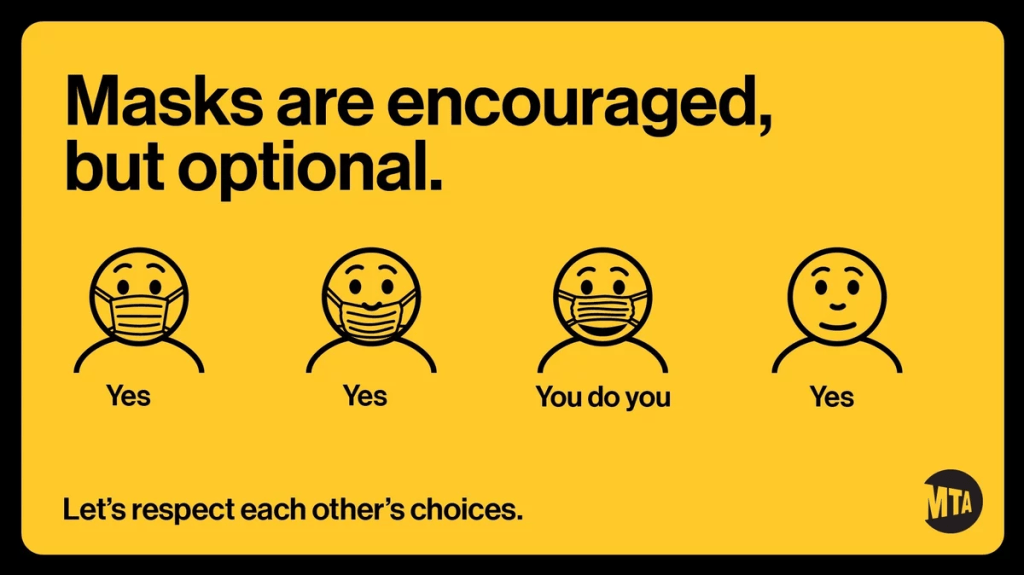
But last week, even the requirement itself was struck down. New York Governor Kathy Hochul (who oversees the Metropolitan Transportation Authority, as it’s a state-controlled agency) announced that masks are now optional on trains and buses. And she introduced the policy with a new version of the MTA’s masking graphic that felt like a slap in the face to higher-risk New Yorkers who now feel unsafe using the transit system.
NPR has a good article explaining why health experts have criticized the new graphic. Personally, I think it discourages people from thinking about how their COVID-19 safety choices impact a broader community—something that’s especially important in a dense, diverse city like NYC. Telling New Yorkers, “You do you,” when “doing you” could mean posing an immense risk to your neighbors, is a dangerous message.
The one silver lining here is, I’ve seen a few excellent posters parodying the MTA’s new mask graphic. Here’s one of my favorites: