Marc Johnson, a molecular virologist and wastewater surveillance expert at the University of Missouri, recently went viral on Twitter with a thread discussing his team’s investigation into a cryptic SARS-CoV-2 lineage in Ohio. I was glad to see the project get some attention, because I find Johnson’s research in this area fascinating and valuable for better understanding the links between coronavirus infection and chronic symptoms.
Ohio cryptic lineage update.
We’ve made no progress identifying the individual, but we have learned a few things. 1/ pic.twitter.com/IE2GB6CwPO
A “cryptic lineage” is a technical term for, basically, a strange viral mutation that researchers have identified in a specific location. Unlike common variants that spread through the population (Delta, Omicron, BA.5, XBB, etc.), these lineages typically are contained in one place, or even in one person. They’re usually identified by wastewater surveillance, since that technique picks up more people’s infections than testing at doctors’ offices.
Johnson has become a specialist in investigating these cryptic lineages over the last couple of years. His lab at the University of Missouri runs the state’s wastewater surveillance program, which includes genetic sequencing for sewage samples. And his team also collaborates on sequencing research for wastewater surveillance in other parts of the U.S. This Nature article from last year goes into more detail about how these investigations work.
In the last few months, Johnson and his colleagues have been investigating one cryptic lineage in Ohio. The scientists have traced the lineage to Columbus and a town called Washington Court House; they believe it represents one sick person, who lives in Columbus and goes to Washington Court House for work. This individual is shedding a massive amount of coronavirus, orders of magnitude higher than the average COVID-positive person. See more details in this story by The Columbus Dispatch.
Johnson and his colleagues would like to identify the person behind this lineage for two reasons. First, they can connect the person with doctors who can help treat their COVID-19 symptoms—it’s likely they’re having a pretty nasty gastrointestinal experience. Second, the scientists hope to better understand how viral particles that shed from a long-term infection might be related to chronic symptoms, as persistent virus in different organ systems is one of the leading hypotheses for why Long COVID occurs.
I’ve interviewed Johnson before for stories about wastewater surveillance and I think he does fascinating work, so I was glad to see his Twitter thread get some attention. If you can help identify the Ohio resident with lots of coronavirus in their gut, get in touch with him!
The CDC and its partners are sequencing far fewer coronavirus samples than they have at prior periods of the pandemic, making it harder to spot new variants of concern.
In the past week (April 30 through May 6), the U.S. reported about 9,500 new COVID-19 patients admitted to hospitals, according to the CDC. This amounts to:
An average of 1,400 new admissions each day
2.9 total admissions for every 100,000 Americans
7% fewer new admissions than last week (April 22-29)
Additionally, the U.S. reported:
A 14% lower concentration of SARS-CoV-2 in wastewater than last week (as of May 10, per Biobot’s dashboard)
64% of new cases are caused by Omicron XBB.1.5; 13% by XBB.1.9; 14% by XBB.1.16 (as of May 13)
An average of 70,000 vaccinations per day
COVID-19 spread continues to trend down in the U.S., though our data for tracking this disease is now worse than ever thanks to the end of the federal public health emergency. If newer Omicron variants cause a surge this summer, those increases will be hard to spot.
As a result of the PHE’s conclusion this week, the CDC is no longer collecting national case counts or testing data. Instead, the agency now recommends using hospitalization data to monitor how hard COVID-19 is hitting your community—even though this metric typically lags behind actual infection patterns—while variant data and wastewater surveillance may provide warnings about new surges.
My national updates will take a similar approach. This week, hospital admissions continue their national plateau, with a decrease of about 7% from the week ending April 29 to the week ending May 6. The CDC’s national map show that admissions are low across the country, with 99% of counties reporting fewer than 10 new admissions per 100,000 residents.
Wastewater surveillance also suggests that, while there’s still a lot of COVID-19 in the U.S., disease spread is still on a plateau or slight decline in most of the country. Biobot’s data show a minor national downturn in recent weeks; trends are similar across the four major regions, though the decline is a bit steeper on the West Coast.
The variant picture also hasn’t changed much: XBB.1.5 caused about two-thirds of new cases in the last two weeks, according to the CDC’s estimates. XBB.1.6 caused about 14% and XBB.1.9 caused 13%; these newer versions of Omicron are gaining ground, but fairly slowly. Regionally, XBB.1.6 is most prevalent in the Northeast and on the West Coast, while XBB.1.9 is most prevalent in the Midwest.
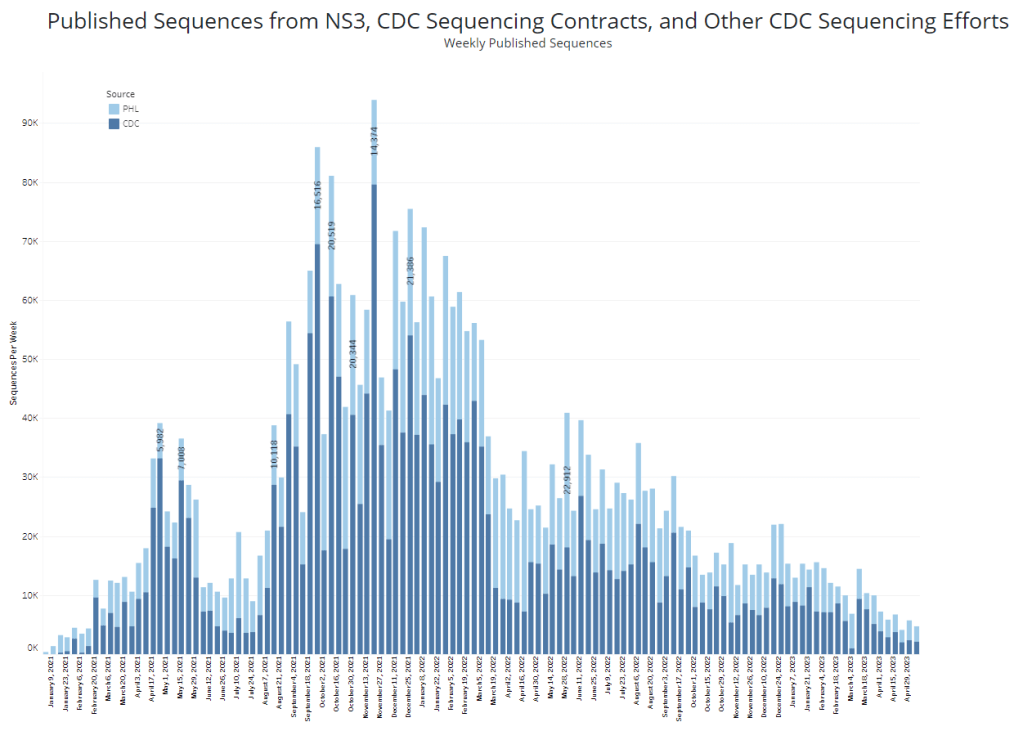
It’s worth noting, though, that the CDC has switched its variant reporting from weekly to every other week, as fewer patient specimens are going through sequencing for variant identification. The agency and its surveillance partners are sequencing around 5,000 samples every week, compared to over 80,000 a week at the height of the first Omicron surge.
Limited sequencing efforts will make it harder for the CDC to quickly identify (and respond to) new variants of concern. The same challenge is happening around the world, as PCR tests become less broadly available. Sequencing coronavirus samples from wastewater may help, but that’s only happening in a small subset of sewage testing sites right now.
One last bit of good news: vaccine administration numbers are up in the last couple of weeks, as seniors and other eligible high-risk people get their second bivalent boosters. About 70,000 people received vaccines each day this week, compared to around half that number a few weeks ago. If you’re eligible for a second booster, this is a good time to make an appointment!
While the CDC is not yet reporting BA.4 and BA.5 separately, the subvariants are included in B.1.1.529; this grouping is driving increased transmission in some Midwestern and Southern states. Chart via the CDC variant dashboard.
America’s current COVID-19 surge is being driven by BA.2 and its sublineage BA.2.12.1. But there are other versions of Omicron out there to which we need to pay attention—namely, BA.4 and BA.5. Here’s a brief FAQ on these two subvariants, including why scientists are concerned about them and where they’re spreading in the U.S.
What are BA.4 and BA.5?
Remember how, when South African scientists first sounded the alarm about Omicron in November, they identified three subvariants—BA.1, BA.2, and BA.3? BA.1 first spread rapidly around the world, followed by BA.2.
Then, in the winter, South African scientists again identified new Omicron subvariants, called BA.4 and BA.5. These two variations split from the original Omicron lineage, and tend to be discussed together because they have similar mutations. (Specifically, they have identical spike protein mutations; this article discusses the mutations in more detail).
It’s important to note that, while South African scientists characterized these subvariants, they likely didn’t originate in the country. South Africa has a better variant surveillance system than many other countries, particularly compared to its neighbors, allowing the country’s scientists to quickly identify variants of concern. BA.4 and BA.5 also caused a new surge in South Africa, allowing for study of the subvariants’ performance.
Why are scientists concerned about these subvariants?
Early studies of BA.4 and BA.5 indicate that not only are these subvariants more transmissible than other forms of Omicron, they’re also more capable of bypassing immunity from prior infection or vaccination.
While the differences between BA.4/BA.5 and BA.1/BA.2 are less dramatic than the differences between the Omicron family and Delta, scientists hypothesize that there is still enough distinction between these two Omicron sub-groups that people who already had Omicron BA.1 or BA.2/BA.2.12.1 could potentially get reinfected by BA.4 or BA.5.
My guess based on this: BA.4/BA.5 escape, while not as dramatic as Omicron escape from vaccine or Delta immunity, is enough to cause trouble and lead to an infection wave. But not likely to cause much more severe disease than the previous wave, especially in vaccinated.
What are BA.4 and BA.5 doing in South Africa and other countries?
BA.4 and BA.5 have been detected in over 30 countries, according to CNN. But scientists have again focused on South Africa, as this country has better surveillance than many others—particularly as PCR testing declines around the world.
In South Africa, the BA.4/BA.5 wave that started in April has peaked and is now on the decline. Hospital admissions and deaths were lower in this recent wave than in the Omicron BA.1 wave in November and Decenter, largely thanks to high levels of immunity in the country. Still, the continued Omicron infections suggest that reinfection is a real concern for these subvariants.
Brief trip back into Covid data today:
Promising news from South Africa, where the BA.4 / BA.5 variant wave has passed quietly, with high levels of immunity meaning this wave has had little impact on rates of severe illness or death pic.twitter.com/C5W6iZzDLK
South Africa never really had a BA.2 wave, so BA.4 and BA.5 mostly competed with other Omicron lineages in that country. But in the U.K., which did face BA.2, recent data suggest that BA.4 and BA.5 have a growth advantage over even BA.2.12.1. In other words, BA.4 and BA.5 could potentially outcompete BA.2.12.1 to become the most transmissible Omicron subvariants yet.
What are BA.4 and BA.5 doing in the U.S.?
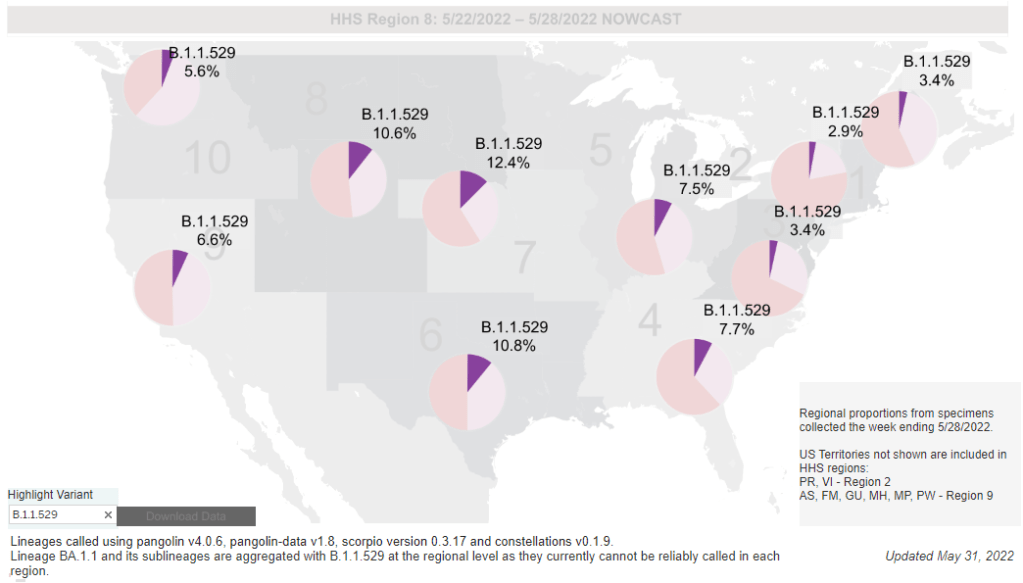
The subvariants are definitely here and spreading, but we have limited visibility into where and how much thanks to declined testing and surveillance. The CDC has yet to separate out BA.4 and BA.5 on its variant dashboard; according to White House COVID-19 Data Director Cyrus Shahpar, this is because the CDC has yet to identify these subvariants as causing 1% or more of new national cases in a given week.
Updated variant proportions just posted. BA.2.12.1 now estimated to be ~59% of specimens sequenced last week. BA.4 and BA.5 not yet meeting the 1%+ threshold to be listed separately https://t.co/YIeQkH8YmEpic.twitter.com/SsSyoVO5Gh
— Dr. Cyrus Shahpar Archived (@cyrusshahpar46) May 31, 2022
But the CDC does include BA.4 and BA.5 in its Omicron B.1.1.529 category, which has grown from causing 1% of new cases in the first week of May to causing 6% of new cases in the last week of the month. The number of cases sequenced in a week has dropped this spring compared to the first Omicron surge, leading me to wonder: are BA.4/BA.5 really causing fewer than 1% of new cases each, or do we just not have the data to detect them yet?
CDC data do show that the B.1.1.529 group (which includes BA.4/BA.5) is causing over 10% of new cases in the Plain States, Gulf Coast, and Mountain West—compared to under 5% in the Northeast, where BA.2.12.1 is more dominant. This data aligns with local reports of BA.4 and BA.5 spreading in wastewater in some Midwestern states that track variants in their sewage. For example, scientists at the Metropolitan Council in the Twin Cities recently said they expect BA.4 and BA.5 to “replace BA.2.12.1 as the dominant variants” in the next few weeks.
What could BA.4 and BA.5 mean for future COVID-19 trends in the U.S.?
As I noted above, data from the U.K. suggest that BA.4 and BA.5 could outcompete BA.2—and even BA.2.12.1—to become the dominant Omicron subvariants in the U.S. Early data from U.S. Omicron sequences are showing a similar pattern, reported variant expert Trevor Bedford in a recent Twitter thread.
“Focusing on the US, we see that BA.2.12.1 currently has a logistic growth rate of 0.05 per day, while BA.4 and BA.5 have logistic growth rates of 0.09 and 0.14 per day,” Bedford wrote. The country’s rising case counts can be mostly attributed to BA.2.12.1, he said, but BA.4 and BA.5 are clearly gaining ground. And, he noted, these two subvariants may be able to reinfect many people who already had BA.1 or BA.2.
Thus, we expect at least some portion of the BA.4 / BA.5 epidemics to be driven by increased vaccine breakthrough and increased reinfection relative to current BA.2 circulation. 12/12
In short: even more Omicron breakthrough infections and reinfections could be coming our way. Even if BA.2.12.1 transmission dips (as it seems to be doing in the Northeast), we could quickly see new outbreaks driven by BA.4 and BA.5—leading overall case numbers to plateau or rise again.
“For the summer, going into the winter, I expect these viruses to be out there at relatively high levels,” Dr. Alex Greninger from the University of Washington’s clinical virology lab told CNN. “Just the number of cases, the sheer disruptions of the workforce — It’s just a very high, high burden of disease.”
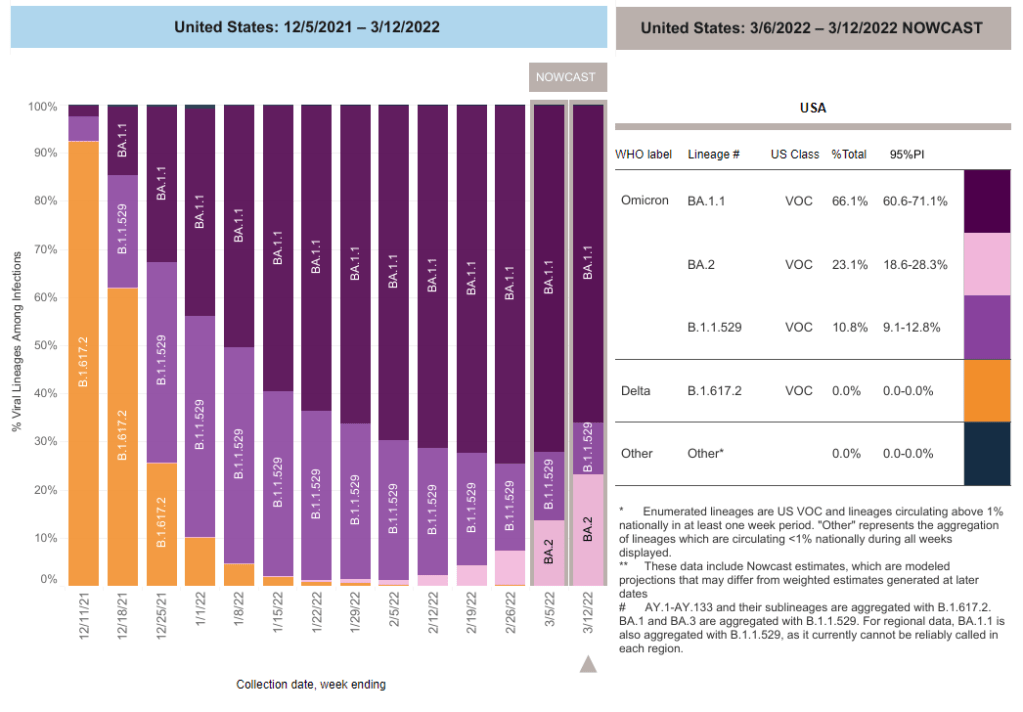
BA.2 caused about one in four U.S. COVID-19 cases in the week ending March 12, according to CDC estimates.
Two years into the pandemic, we now know some basic truisms about the coronavirus. For example: outdoor events are always safer than indoor events; older age is the most significant risk factor for severe symptoms; hospitalization trends typically follow case trends by a couple of weeks; and whenever Europe has a new surge, the U.S. is likely to also see a surge in the next month or so.
That last truism is particularly relevant right now, because Europe is experiencing a new surge. Cases are increasing in the U.K., Germany, the Netherlands, and many other countries. The new surge is likely due to European leaders’ decisions to end all COVID-19 safety measures in their countries, combined with the rise of Omicron sublineage BA.2.
As BA.2 prevalence increases here in the U.S.—and our leaders also end safety measures—we seem poised to follow in Europe’s footsteps once again. But a BA.2 surge is likely to look different from the intense Omicron surge that we experienced in December and January, in part because of leftover immunity from that Omicron surge.
Let’s go over what we know about BA.2, and what might happen in the next few weeks.
What is BA.2?
It’s important to note that this isn’t a new variant, at least not compared to the original Omicron strain. As I noted in a FAQ post about this strain back in January, South African scientists who originally characterized Omicron in November 2021 identified three sub-lineages: BA.1, BA.2, and BA.3.
BA.1 spread rapidly through the world, driving the surge that we experienced here in the U.S. in December through February. But BA.2, it turns out, is actually more transmissible than BA.1—allowing it to now outcompete that strain and contribute to case increases in countries that already faced major BA.1 surges.
How does BA.2 differ from BA.1, or original Omicron?
The main difference between these two strains is that BA.2 is more contagious: scientists estimate that BA.2 is about 30% more transmissible than other Omicron strains, if not more. (Note that this is a smaller difference than Omicron’s advantage over Delta and other earlier variants.)
In a recent report, the U.K. Health Security Agency estimated that someone infected with BA.2 would infect about 13.6% of their households and 5.3% of contacts outside of their households, compared to 10.7% of households and 4.2% outside contacts for other Omicron strains. The modest difference between these rates demonstrates why BA.2 is not outcompeting other Omicron strains as quickly as Omicron outcompeted Delta a couple of months ago.
Another notable feature of BA.2 is that, unlike BA.1, it can’t be identified with a PCR test. BA.1 has a mutation called S drop-out, which causes a special signal in PCR test results, allowing the variant to be flagged without sequencing; BA.2 doesn’t have this mutation. To be clear, a PCR test will still return a positive result for someone who is infected with BA.2—it’ll just take an additional sequencing step to identify that they have this particular strain.
Finally, one major challenge during the Omicron BA.1 surge has been that two of the three monoclonal antibody treatments used in the U.S. did not work well for people infected with Omicron. BA.2 may exacerbate this challenge, as some studies have suggested that the third treatment—called sotrovimab—continued working against BA.1, but may not hold up against BA.2. Luckily though, Eli Lilly (which developed one of the treatments that failed for BA.1) has produced an updated monoclonal antibody cocktail that does work for both Omicron strains.
How is BA.2 similar to BA.1, or original Omicron?
Two major pieces of good news here: 1) our existing COVID-19 vaccines work similarly well against BA.2 as they do against BA.1, and 2) prior infection with BA.1 seems to be protective against infection with BA.2.
Essentially, studies are showing that the two strains are close enough in their genetic profiles that antibodies from a BA.1 infection will provide some immunity against a BA.2 infection. And the same thing goes for vaccination, at least when it comes to protection against severe disease. A recent CDC study showed that, even during the Omicron surge, COVID-19 patients who had received three vaccine doses were far less likely to require mechanical ventilation or die from the disease than those who weren’t vaccinated.
There’s a flip side to this, though: for both BA.1 and BA.2, prior infection with a previous variant is not very protective against an Omicron infection. CDC seroprevalence data suggest that between 40% and 45% of Americans got infected with BA.1 during the winter surge; this means the remaining 55% to 60% of the population is susceptible to BA.2. Vaccines protect against severe disease and death from BA.2, but they don’t protect against BA.2 infection to the degree that they did against past variants.
This means that in terms of protection against infection, populations with high rates of vaccination or prior infection remain essentially naive to it. Though vaccines and prior infections still protect from severe disease and death (thanks to T-cell protection). 3/ pic.twitter.com/gmwlk2l7ZV
— Prof Francois Balloux (@BallouxFrancois) March 19, 2022
BA.2 and BA.1 are also similar in their severity. Both strains are less likely to cause severe disease than Delta; BA.1 had a 59% lower risk of hospital admission and 69% lower risk of death than Delta in the U.K., according to a new paper published this week in the Lancet.
It’s important to remember, however, that Delta was actually more severe than other variants that preceded it. As a result, “Omicron is about as mild/severe as early 2020 SARSCoV2,” wrote computational biologist Francois Balloux in his Twitter thread (referring to both BA.1 and BA.2).
What are the warning signs for a BA.2 surge in the U.S.?
First of all, many U.S. experts consider case increases in Europe to be an early indicator of increases in the U.S. As I said at the top of the post, Europe is seeing a surge right now, and many of the countries reporting case increases have estimated over 50% of their cases are caused by BA.2.
In the U.S., our BA.2 levels are lower: the CDC’s most recent estimates suggested that BA.2 was causing about 23% of new cases nationwide as of March 12. If BA.2 continues growing at the same rate we’ve seen in recent weeks, we have one or two more weeks before this variant hits 50% prevalence in the U.S.
“The tipping point seems to be right around 50%,” Keri Althoff, an epidemiologist at Johns Hopkins Bloomberg School of Public Health, told CNN. “That’s when we really start to see that variant flex its power in the population” as far as showing its severity.
At the same time, several Asian countries are also seeing major BA.2 surges at the moment. For example, Hong Kong was able to deal with early Omicron cases earlier in the winter, former COVID Tracking Project lead Erin Kissane pointed out in her Calm Covid newsletter; but now, the territory is facing a terrible BA.2 wave, driving what is now the world’s highest case fatality rate.
NEW: I’m not sure people appreciate quite how bad the Covid situation is in Hong Kong, nor what might be around the corner.
First, an astonishing chart.
After keeping Covid at bay for two years, Omicron has hit HK and New Zealand, but the outcomes could not be more different. pic.twitter.com/1Ol4HHs9kT
Here in the U.S., we’re also seeing warning signals in the form of rising coronavirus levels in wastewater. (Wastewater is considered an early indicator for surges, because coronavirus material often shows up in sewer systems before people begin to experience symptoms or get tested.) About one-third of sewershed collection sites in the CDC’s wastewater monitoring network are reporting increased virus prevalence in the two-week period ending March 15.
The CDC wastewater data must be interpreted cautiously, however, as this surveillance network is biased towards states like Missouri and Ohio, which have over 50 collection sites included in the national network. 12 states still do not have any collection sites in the network at all, while 23 states have fewer than 10. This recent Bloomberg article includes more context on interpreting wastewater data.
New York City is one place that’s reporting increased viral levels in wastewater, at the same time as the city health department reports that case numbers have plateaued—or may even be ticking up. An excellent time to loosen all mask and vaccination requirements, am I right?
What might a BA.2 surge in the U.S. look like?
Between the warning signals from Europe and the newly-lax safety measures throughout the U.S., it seems very likely that we will see a BA.2 surge in the coming weeks. The bigger question, though, is this surge’s severity: to what extent will it cause severe disease and death?
As I mentioned above, estimates suggest that about 40% to 45% of Americans have some Omicron antibodies from an infection earlier in the winter. At the same time, about 65% of the population is fully vaccinated and 45% of those fully vaccinated have received a booster shot, according to the CDC.
That’s a lot of people who are protected against severe COVID-19 symptoms, if they get infected with BA.2. But the U.S. has lower vaccination coverage than other countries, particularly when it comes to boosters. For example, in the U.K., 86% of eligible people are fully vaccinated and 67% are boosted, according to CNN. These lower vaccination rates contributed to the U.S.’s high mortality rate during the Omicron surge compared to other wealthy countries.
While the vaccines offer great protection, the U.S. appears to have given up on many other COVID-19 safety measures, like masks, social distancing, and limits on in-person gatherings. Without reinstating some of these measures, we would essentially be left without any tools to slow down the spread of BA.2; and even if some states and cities put safety measures in place, they’ll likely face more pushback now than they did in earlier surges.
To quote from Kissane’s newsletter:
In practical terms, with work and school happening in-person and without high-filtration (or any) masks or serious ventilation requirements in the US and most of Europe, governments in North America and Europe have made increased covid exposure essentially mandatory for most citizens.
I want to emphasize that for most vaccinated people, this increased risk probably won’t be a huge deal even if BA.2 causes a new case surge—they’ve either already racked up enough immunity to fight off BA.2 or they’ll be sick for a week.
One big caveat to this, though: we don’t have great data yet on how Omicron (or BA.2 specifically) might contribute to Long COVID rates; collecting data on this condition is very challenging and takes a lot of time. Studies suggest that vaccination reduces an individual’s risk of long-term symptoms if they get infected, but it does not eliminate this risk.
What can you do to prepare for this potential surge?
Here are a few things that I’m doing to prepare for a potential BA.2 surge in the coming weeks:
Promoting vaccination—particularly booster shots—to family members and friends.
Stocking up on good-quality masks (i.e. N95s and KN95s) and rapid tests. (Reminder, order a new round of free tests from covidtests.gov if you haven’t yet!)
Researching my options for COVID-19 treatments (antiviral pills and monoclonal antibodies) in the event that I get infected.
Getting tested frequently, particularly before attending indoor events (such as gathering with a few other friends, or going out to a movie theater.)
Watching wastewater and case trends in my area, and preparing to cut down on riskier behaviors if(/when) cases start rising.
I don’t know what BA.2 will mean for the US.
I do know this:
It hinges on vaccination/booster rates *now*.
So: 👆+
4th doses & Evusheld for immunocompromised ASAP, if not done.
Know where you’d get Paxlovid & Sotrovimab.
Order rapids now.
Get N95s or best possible now.
— Jeremy Faust MD MS (ER physician) (@jeremyfaust) March 16, 2022
As always, if you have any COVID-19 questions (about BA.2 or otherwise) that you’d like me to address, please reach out.
An offshoot strain of the Omicron variant has been making headlines this week as it spreads rapidly in some European and Asian countries. While the strain, called BA.2 by virologists, has not yet been identified in the U.S. in large numbers, it’s already spreading here, too: scientists have picked it up in wastewater samples in some parts of the country.
This strain clearly has a growth advantage over the original Omicron strain (also called BA.1), but it’s not cause for major concern at this point. Scientists are working to identify whether BA.2 has a higher capacity for breaking through immunity from past infection or vaccination; so far, early data suggest that it does not significantly differ from BA.1 on this front, though it may have a slight advantage.
Here’s a brief FAQ on what we know about the strain so far.
When and where did BA.2 emerge?
I’ve been careful not to call BA.2 a “new strain” or a “new variant” here because it’s not actually new—at least, it’s not any newer than Omicron BA.1. When South African scientists first sounded the alarm about Omicron in late November 2021, BA.2 was already present among the country’s cases of this variant.
In fact, a paper from South African scientists describing the Omicron wave in their country, published in Nature in early January, specifies that the earliest specimen of BA.2 was sampled on November 17; the earliest specimen of BA.1 was sampled on November 8. Around the same time, South African scientists also identified a third lineage, called BA.3—this one hasn’t yet become a cause for concern.
Why are scientists concerned about BA.2?
In the past couple of weeks, epidemiologists have identified that BA.2 is spreading faster in some countries than BA.1, the original Omicron strain. This means BA.2 has what scientists call a “transmission advantage” over BA.1: it is capable of getting from person to person fast enough that it may be able to outcompete BA.1.
For example, in Denmark, BA.2 became the dominant strain in mid-January, taking over from BA.1. The takeover has coincided with an additional increase in COVID-19 cases in the country after Denmark’s Omicron wave initially appeared to peak a couple of weeks ago—but it’s hard to determine whether this second increase is solely due to BA.2 or also connected to an announcement that Denmark will end its COVID-19 restrictions on February 1.
This past week, the World Health Organization (WHO) announced that investigations into BA.2, including its potential virulence and ability to escape prior immunity, “should be prioritized independently (and comparatively) to BA.1.” The WHO has yet to designate BA.2 as a separate variant of concern from BA.1, however; at the moment, both strains are still included under the Omicron label.
How does BA.2 compare to BA.1, the original Omicron strain?
As I’ve explained in previous posts about the variant, Omicron has the most antigenic drift of any coronavirus variant identified thus far—meaning that it’s the most genetically different from the initial Wuhan version of the virus. Omicron BA.1 has about 60 mutations compared to the Wuhan strain, but BA.2 has even more: about 85 mutations, according to a recent Your Epidemiologist post.
BA.2 is clearly more transmissible than BA.1, as we’ve seen from its rapid spread in countries including Denmark, the U.K., France, the Netherlands, India, and the Philippines. Scientists estimate that “BA.2 may be 30% to 35% more transmissible than BA.1,” STAT News reports.
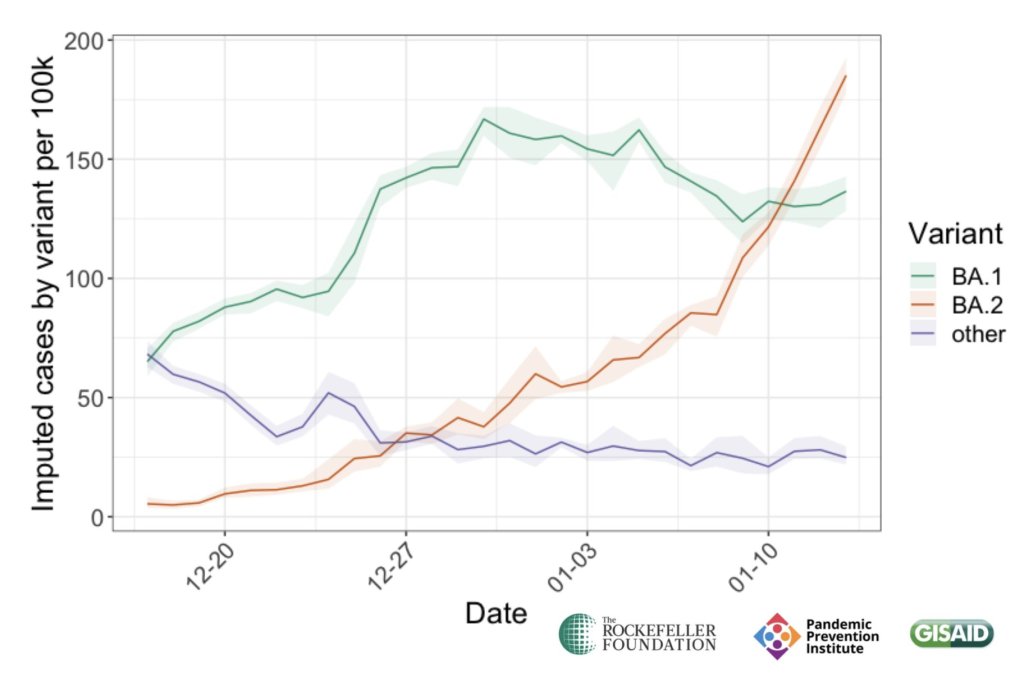
3/ In Denmark, BA.2 is spreading rapidly, despite BA.1 leveling off. This worrying trend is why scientists, including analysts at PPI like @ZacharySusswein & @KaitEJohnson9, are investigating. pic.twitter.com/ItsoO5jcJh
— Pandemic Prevention Initiative (@PPI_Insights) January 26, 2022
The question scientists hope to answer, then, is why BA.2 has this transmission advantage over BA.1. Do BA.2’s additional mutations lend it some adaptation in how it interacts with human cells, enabling faster spread? Or is BA.2 more capable of evading protection from past infection or vaccination compared to BA.1, leading it to cause more reinfections and breakthrough cases?
While we don’t know the answers to these questions yet, early data are indicating that there’s no major difference in disease severity between BA.1 and BA.2. In other words, BA.2 isn’t more likely to cause severe symptoms.
“There is no evidence that the BA.2 variant causes more disease, but it must be more contagious,” Danish Health Minister Magnus Heunicke said at a news conference last week, Reuters reported.
Why do some articles call BA.2 a “stealth variant?”
You might have seen some headlines referring to BA.2 as a “stealth variant” or a “stealth version of Omicron.” This is because of one major difference between BA.2 and BA.1: while BA.1 can be identified with a PCR test due to a key mutation that’s visible on PCR test results, BA.2 does not have this mutation.
As a result, BA.2 can be more time-consuming for COVID-19 testing labs to identify: labs need to sequence a sample’s genome to identify this strain rather than simply look out for an indicator on a PCR test. It’s unclear how much of a difference this will make in the U.S.’s ability to track BA.2, however, as many labs across the country are already performing routine full-genome sequencing of coronavirus samples.
How well do vaccines work against BA.2?
So far, it seems like there is no significant difference in vaccine protection between BA.1 and BA.2, at least when it comes to severe symptoms—which makes sense, scientists say, given how well vaccines have worked against every major variant to emerge thus far.
Early findings in this area come from the U.K., which designated BA.2 as a “Variant Under Investigation” (separate from BA.1) about a week and a half ago. This past Friday, the U.K.’s Health Security Agency released a report with information on BA.2, including how it compares to BA.1 or original Omicron.
Overall, U.K. epidemiologist Meaghan Kall wrote in a Twitter thread summarizing the report, early evidence suggests that “BA.2 is no more immune evasive than Omicron,” though confidence in this statement is low. The report found that, for Brits who had received booster shots, vaccine effectiveness against symptomatic COVID-19 disease was 70% for BA.2 and 63% for BA.1. The confidence intervals on these effectiveness estimates overlapped, indicating that vaccines perform similarly against BA.2 and BA.1.
• Transmissibility: 🟥 risk LOW confidence advantage due to being more infectious
• Immune evasion: 🟧 risk LOW confidence BA.2 is no more immune evasive than Omicron pic.twitter.com/kaEYFbIbP7
— Meaghan Kall has moved to Bluesky (@kallmemeg) January 28, 2022
When it comes to disease severity, Kall wrote, the U.K. doesn’t have enough data to compare BA.2 and BA.1; early data on this topic (suggesting BA.2 is not more severe) have come from Denmark and India.
How will BA.2 impact the U.S.’s COVID-19 trajectory?
BA.2 has already outcompeted BA.1 in some parts of Europe and Asia, and epidemiologists expect that countries like the U.K. and the U.S. could also follow this pattern—though it will likely be a longer, slower replacement process compared to the intense way Omicron pushed out Delta. A bigger unknown here is what effect this strain may have on case numbers, hospitalizations, and deaths.
17/ BUT wastewater testing from Marc Johnson's lab at @mumedicine shows that BA.2 is in the US, and spreading fast. This aligns with what we would expect given trends in other countries.
— Pandemic Prevention Initiative (@PPI_Insights) January 26, 2022
Countries and regions now passing the peaks of their Omicron BA.1 waves have extremely high levels of population immunity. As a result, people who are fully vaccinated with boosters and/or recently infected with Omicron BA.1 likely will have a lot of immune system protection against BA.2, though we don’t yet have good data on exactly how robust this protection is.
So, could BA.2 cause the current downturn in U.S. COVID-19 cases to reverse? It’s possible, explains Andrew Joseph in a recent STAT News article. However, thanks to our high immunity levels, a further spike in cases could be “broadly limited to infections” rather than causing major increases in hospitalizations and deaths. In the coming weeks, we’ll get a better sense of how well prior Omicron infections protect against BA.2 and other key information that will inform our understanding of how this strain may change the country’s COVID-19 trajectory.
Right now, COVID-19 experts are closely monitoring BA.2, but they’re not hugely concerned. As Dr. Jetelina put it in a recent Your Local Epidemiologist post, the bigger worry right now is that another variant could “pop out of nowhere” like Omicron did in November.
Major news items for this week include the potential peak of the U.S.’s Omicron surge and real-world data from the CDC on how well booster shots work against this variant.
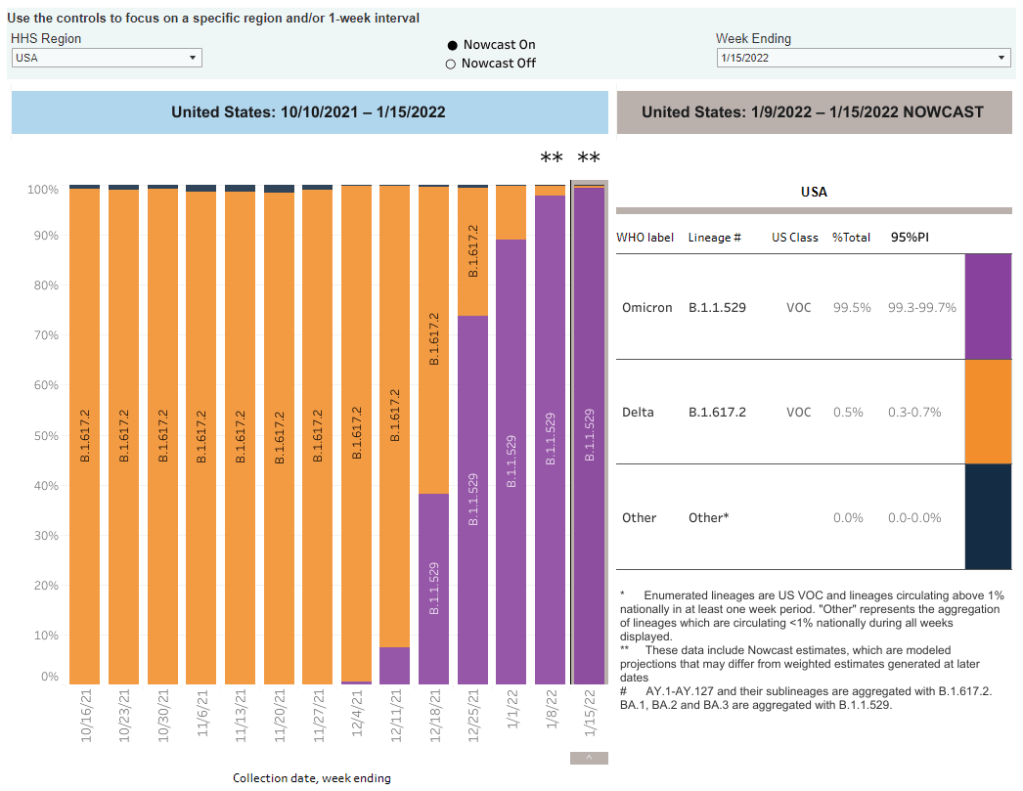
Omicron is now causing nearly 100% of new COVID-19 cases in the U.S. The latest CDC estimates of variant prevalence put Omicron at 99.5% of new cases in the U.S. as of January 15, with Delta causing the remaining 0.5% of cases. I have to say, it’s incredibly striking not only how quickly Omicron outcompeted Delta (it went from 1% of new cases to nearly 100% in just six weeks), but also how both of these highly contagious variants have dominated the country so thoroughly that they’re now the only two variants present here at all. For comparison, Alpha only got to 70% of cases at its peak. These trends show how drastically both Delta and Omicron changed the trajectory of the pandemic.
While the U.S. may be peaking, massive numbers of people are getting infected. As I noted in today’s National Numbers, America’s Omicron wave may have peaked this week, with the country’s massive case growth appearing to turn around. Computational biologist Trevor Bedford wrote a recent Twitter thread about this peak, pointing out that a huge share of the U.S. population was infected with Omicron in the past month: “between 18% and 23% of the country was infected by Omicron by Jan 17, with the large majority infected in a span of just ~4 weeks,” he hypothesized. By mid-February, Bedford says, this number could be “36%-46%.”
Case counts for the US appear to have peaked at a 7-day average of 806k on Jan 14. Omicron grew from approximately 35k daily cases on Dec 14 to ~800k daily cases in ~4 weeks. 1/9 pic.twitter.com/D1Y6R58SjN
The high infection numbers may give us “a bit of a break from the Covid roller coaster.” With so many people infected in such a short time, Omicron will have a huge impact on the “immunological landscape” of the U.S, Helen Branswell explains in a recent article for STAT News. Millions will have immunity from a recent infection, vaccination, or both; and Omicron’s unique biology may mean that people who caught this variant will be protected from other strains. As a result, the end of this wave may lead into “a bit of a break” from COVID-19, Branswell writes, with low case numbers for a few weeks or months. It’s hard to say whether this “break” will constitute the end of the pandemic, though—we don’t know how long post-Omicron immunity lasts.
Rapid at-home tests work well at detecting Omicron, though they’re far from perfect.As I’ve noted in past issues, there have been some questions recently about how well rapid antigen tests work at identifying Omicron infections. In a recent Your Local Epidemiologist post, Dr. Katelyn Jetelina walked through the data from several recent studies on this topic. The highlights: rapid tests likely won’t work well in the very beginning of an infection, so wait to test until five days after an exposure; if you test positive, trust the result; test repeatedly for higher accuracy; and, if you have the tests, wait for two negative results before coming out of isolation.
New CDC wastewater report shows how early Omicron was spreading in the U.S. The CDC published a report this week sharing findings from wastewater surveillance systems in a few states and localities. (Wastewater surveillance means the states are regularly testing samples from sewage to identify coronavirus levels coming from residents’, well, waste.) In New York City, Omicron was first detected in wastewater on November 21, the weekend before Thanksgiving. In California, Colorado, and Houston, Texas, the variant was detected in late November or early December.
An additional booster shot may not be enough to completely prevent Omicron infection, a small Israeli study suggests. Israel was one of the first countries to offer third vaccine doses to its residents, and now it’s also one of the first countries offering fourth doses. A new study presents the impact of these shots among about 270 healthcare workers. The additional doses produced more antibodies in the patients, but “this is probably not enough for the Omicron,” one of the study’s authors told Reuters—at least when it comes to completely preventing infection.
But: booster shots still reduce chances of infection significantly, compared to people who are unvaccinated. Another new CDC report published this week compares COVID-19 cases among vaccinated, boosted, and unvaccinated people in 25 U.S. jurisdictions. In late December, after Omicron started spreading widely, adults who were unvaccinated had a five times higher risk of COVID-19 infection compared to those who were fully vaccinated with a booster shot, the CDC found.
Booster shots also have a huge impact on risks of severe symptoms and hospitalization. One more CDC report released this week: scientists analyzed the impact of booster shots on emergency department visits and other hospitalization metrics in ten states. When both Delta and Omicron were the dominant variants in the U.S., the CDC researchers found, third doses had 94% efficacy rates in protecting people against COVID-related emergency department visits, and 82% efficacy rates in protecting against urgent care visits. Efficacy against hospitalization was also over 90%. In short: if you’re eligible for your booster, go get it!
Booster shots of Pfizer and Moderna vaccines could be critical for countries that used other brands.Last week, I shared a report that found 22 million mRNA vaccine doses are needed as booster shots in low-income countries, to protect the world against Omicron. This past week, a new study in Nature supported this report: a group of scientists in Hong Kong found that Pfizer doses are safe and highly effective booster shots for people who initially received the Chinese CoronaVac vaccine. The authors suggest that mRNA vaccines should be used as boosters in countries that originally distributed CoronaVac.
New research identifies a mutation that may contribute to Omicron’s super-contagiousness. A new study from the National Institutes of Health (NIH) found that a mutation present in the Alpha and Delta variants allows the coronavirus to more easily bind to human cells. When the coronavirus binds more easily, it can spread faster within the body; this rapid multiplication helps the virus quickly spread outside the body as well, increasing contagiousness. Though this study was done before the Omicron variant emerged, Omicron has this same mutation, explained lead author Dr. Lawrence Tabak in a post for the NIH Director’s Blog.
As the Omicron surge continues, we are still learning more about this variant. Here are the major updates from this week:
Omicron is now causing more than 90% of new cases in the U.S. In the latest update of the CDC’s variant proportions estimates, the agency found that Omicron caused 95% of new COVID-19 cases nationwide in the week ending January 1. The CDC also revised estimates for previous weeks, bringing us to 77% Omicron for the week ending December 25 and 38% Omicron for the week ending December 18. While these estimates continue to be based on weeks-old data, it the CDC now has enough sequencing information to make Omicron estimates with lower confidence intervals than it did a few weeks ago—suggesting that these numbers are closer to reality than the estimates we saw in December.
Omicron is causing the vast majority of cases in every state. Also included in the CDC’s variant proportions estimates: regional numbers. The latest figures estimate that, as of January 1, Omicron prevalence across the country ranges from 82% in the Northeast to 98% in New York/New Jersey and the Gulf states region (Texas, Louisiana, Arkansas, Oklahoma, and New Mexico). These numbers align with recent calculations from computational biologist Trevor Bedford based on sequences posed to the public repository GISAID. In short: Omicron is everywhere.
Evidence that Omicron is less likely to cause severe symptoms continues to mount. A combination of real-world hospitalization and lab data continue to suggest that Omicron is less likely to cause severe COVID-19 symptoms than past coronavirus variants. The hospitalization data: in Omicron hotspots, hospitalization numbers are not rising at the same rate as case numbers, nor are the numbers of patients who require intensive care or ventilators. “Despite steep rises in cases and patients, the number on ventilators has barely risen,” wrote Financial Times data journalist John Burn-Murdoch in a recent thread about U.K. data.
And the lab data: a growing number of studies show that Omicron is less capable of infecting patients’ lungs compared to past variants—meaning the worst respiratory symptoms are rarer. At the same time, people who catch Omicron after gaining immunity from vaccination and/or prior infection are protected against severe symptoms thanks to T cells and other aspects of immune system memory. Note that, however, we still don’t know about the risk of Long COVID following an Omicron case.
Still: U.S. Hospitals are now incredibly overwhelmed with Omicron and Delta cases. In the U.S. so far, the “decoupling” phenomenon (in which hospitalizations and ICU admissions don’t rise as fast as cases) has been less visible than in other countries hit by Omicron. Several states have already set hospitalization and/or ICU records during the Omicron surge. This is likely because many parts of the U.S. have lower vaccination rates than other countries like the U.K. At the same time, accounts from hospital workers show the toll that this surge is taking: “Thankfully the Covid patients aren’t as sick. BUT there’s SO many of them,” wrote NYC ER doctor Dr. Craig Spencer in a recent Twitter thread.
NEW chart for US Covid-watchers:
Key question with Omicron wave is whether severe disease — hospitalisations & ICU — decouples from cases.
In the UK it has, but there are signs the US decoupling is weaker, perhaps due in part to lower vax rates.
Omicron has more antigenic drift than any other variant.“Antigenic drift” is a virology term referring to the small mutations in virus genetic material that cause these viruses to change slowly over time. As I noted in early Omicron updates, this variant didn’t evolve out of Delta (as many experts were expecting) but rather showed up seemingly out of nowhere; it might have emerged from a part of the world with limited variant surveillance, an immunocompromised person, or even an animal host. We don’t know Omicron’s origin yet, but we now know that it is further apart, genetically speaking, from the original coronavirus than any other variant so far.
London’s Omicron surge may have peaked. According to U.K. data, both case numbers and hospital admission numbers have slowed in their increases, the Washington Post reports. “For the moment, we can probably say London appears to be over the worst,” U.K. hospital executive Chris Hopson said last week. Other U.K. health officials are more skeptical though, according to the Post: while case numbers are falling for teenagers and younger adults, London is still reporting increasing cases among seniors.
New York City also might be on the verge of peaking. Another tentative peak report: data from NYC’s health department suggest that case numbers might be starting to fall in the city. The citywide seven-day average for new cases fell from 3,261 per 100,000 people on January 2 to 2,754 per 100,000 on January 4, and NYC’s positivity rate is also trending down. Reduced COVID-19 testing over New Years and other reporting uncertainties are likely playing a role here, but still—NYC cases jumped right back up after Christmas, but haven’t yet jumped up after New Years. I am cautiously optimistic!
The last two days have seen quite strong week-over-week falls in NYC cases by specimen date pic.twitter.com/kb4aRkpp2R
New research maps out South Africa’s intense Omicron wave. This recent study caught my eye when it was published in Nature this week through accelerated approval. Nearly 100 scientists in South Africa, Botswana, the U.S., Switzerland, the U.K., and other countries collaborated to analyze Omicron’s genetic makeup and the variant’s rapid spread through South Africa, including its ability to cause breakthrough cases and reinfect people who’ve previously had COVID-19. The paper is just one example of the immense collaboration that has taken place over the past month as scientists work to quickly understand this variant. Thank you, scientists!
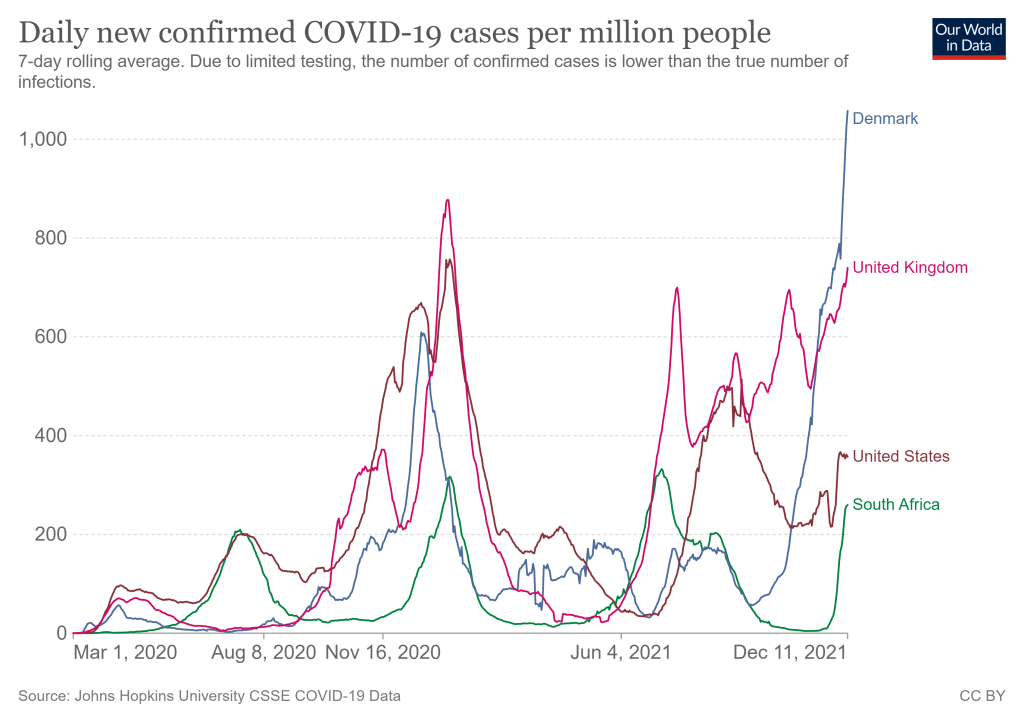
COVID-19 cases are rising rapidly in countries where Omicron is spreading, including South Africa, the U.K., and Denmark. Chart from Our World in Data, retrieved September 12.
We continue to learn more about this new variant as it spreads rapidly across the world, though much of the data are still preliminary. Here are a few major updates:
Omicron is still spreading very quickly in South Africa, as well as in the U.K. and Denmark—two other countries with great genetic surveillance. Preliminary estimatesbased on data from these countries suggest that the variant’s R-value is between 3 and 4, indicating that the average person infected with Omicron infects three or four others. As Sarah Zhang put it in The Atlantic: “Omicron is spreading in highly immune populations as quickly as the original virus did in populations with no immunity at all.”
Early vaccine studies show a drop in antibody levels against Omicron, but that doesn’t necessarily correspond to overall protection. This week, we saw the first results from early studies evaluating how well vaccines work against Omicron. Here’s a summary, drawing from Katherine Wu’s coverage of these studies in The Atlantic: vaccinated people confronted with Omicron appear to produce a lot fewer antibodies that can fight the virus, compared with older variants. Numbers range from a five-fold drop in antibodies to a 41-fold drop. But remember, antibodies are just one part of the immune system—specifically, they’re the part that’s easiest to measure. Vaccinated people also have memory immune cells that provide protection over a long time period, which isn’t captured in antibody studies. We’ll need more time and more data to actually evaluate how vaccines fare against Omicron in the real world, rather than in the lab.
The vaccines seem to protect against severe disease and death from Omicron. So far, the data suggest that our existing COVID-19 vaccines still work quite well at protecting people from severe symptoms—even when those severe symptoms are caused by an Omicron case. “When the shots’ protection ebbs, it tends to do so stepwise: first, against infection, then transmission and symptoms, and finally against severe disease,” Wu writes. For vaccinated people to lose protection against severe disease, the virus would have to change much more than Omicron has. At the same time, however, some experts are concerned that non-mRNA vaccines may not fare as well against Omicron as Moderna and Pfizer, conferring a disadvantage to the low- and middle-income countries that have had less access to the mRNA vaccines.
Booster shots increase protection against Omicron. While vaccinated people are less protected against infection with Omicron than previous variants, booster shots appear to help close that gap—even though currently-available booster shots are not designed specifically for Omicron. One U.K. study suggests that boosters can increase vaccine effectiveness against infection from 30% to 75%, for people who received the Pfizer vaccines. In other words: Omicron is a good reason to go get your booster shot, if you’re eligible and you live in a place where the shots are available.
Experts continue to be skeptical about Omicron being “more mild.” Reports out of South Africa continue to suggest that cases caused by Omicron are more mild than cases caused by Delta, with doctors saying that fewer patients are requiring hospitalization and those hospital stays are shorter than previous outbreaks. But many of the South Africans getting sick with Omicron may have some protection from vaccination or past infection; this means they’re more likely to have mild cases, as biostatistician Natalie Dean explains in an excellent Twitter thread. Plus, even if Omicron is more mild, it appears to be more transmissible—and a smaller share of severe cases out of a larger pool of cases overall can still lead to a pretty big number of people going to the hospital. In addition, we have zero data at this point on how Omicron may impact Long COVID cases, or how well vaccines protect against Long COVID from an Omicron infection.
Early U.K. data confirm Omicron’s high contagiousness and its capacity for evading protection from vaccines and prior cases. After the U.K.’s best-in-the-world genetic surveillance agency first identified Omicron in late November, I wrote that the country would likely provide invaluable data on this variant. Less than two weeks later, the U.K. Health Security Agency has released its first Omicron report. The country’s real-world data confirm that Omicron can spread quite fast: for example, “19% of Omicron cases resulted in household outbreaks vs 8.5% of Delta cases,” wrote epidemiologist Meaghan Kall in a summary of the report. The report also “paints a very consistent picture for Omicron being immune evading,” Kall said, though booster shots help a lot.
Anime NYC was a likely Omicron superspreader event. More and more reports have emerged of Omicron cases connected to Anime NYC, a convention held in Manhattan in mid-November. The CDC is currently investigating the convention: officials are working with the NYC health department to contact all 53,000 convention attendees for testing and contact tracing. “Data from this investigation will likely provide some of the earliest looks in this country on the transmissibility of the variant,” CDC Director Dr. Rochelle Walensky said at a press briefing on Tuesday.
The CDC formally named Omicron a Variant of Concern. On Friday, the CDC officially designated Omicron as a Variant of Concern and added it to the variant tracking page of the agency’s COVID-19 dashboard. As of December 4, Omicron is causing 0.0% of new COVID-19 cases in the U.S., the CDC estimates. The variant has yet to be added to the CDC’s state-by-state data. Given the continued geographic disparities of the U.S.’s genomic surveillance system, however, we may expect that the variant is already spreading in states where it has yet to be formally identified.
Omicron can likely compete with Delta, but we need more data to get a better sense of how well. “Omicron is picking up speed in Europe, which has often served as a preview of what was headed the U.S.’s way. It’s an early sign that the already bleak situation here may get worse,” writes Andrew Joseph in a recent STAT News story. U.K. data suggest that Omicron could cause a majority of cases there within two to four weeks, Joseph reports, and the U.S. may not be far behind. Still, more real-world data from countries and regions with clear Omicron outbreaks will give us a better idea of just how worried we need to be about a potential Omicron-fueled surge.
In summary:
There's been a lot of new data for Omicron in the last day, much still preliminary, but here's my summary of the good and bad pic.twitter.com/pL8uiD7hfV
This past Monday, President Biden gave a speech about the Omicron variant. He told America that Omicron is “cause for concern, not a cause for panic,” and thanked the South African scientists who alerted the world to this variant. (Though a travel ban is not a great way to thank those scientists!)
Towards the end of the speech, he said: “We’re throwing everything we can at this virus, tracking it from every angle.” Which I, personally, found laughable. As I’ve pointed out in a previous post about booster shots, the U.S.’s anti-COVID strategy basically revolves around vaccines, and has for most of 2021.
wild to hear Biden say "we are throwing everything we can at this virus" … like, sir, no we aren't. we are throwing ONE THING (vaccines) at this virus.
My Tweet about Biden’s vaccine-only strategy got more attention than I’m used to receiving on the platform, so I thought it was a worthwhile topic to expand upon in the COVID-19 Data Dispatch. Why aren’t vaccines enough to address Omicron—or our current surge, for that matter—and what else could the Biden administration be doing to slow the coronavirus’ spread?
Why aren’t vaccines enough?
Prior to Delta’s spread, there was some talk of reaching herd immunity: perhaps if 70% or 80% of Americans got fully vaccinated, it would be sufficient to tamp down on the coronavirus. But Delta’s increased capacity to spread quickly, combined with the vaccines’ decreased capacity to protect against infection and transmission, have shown that vaccines are not enough to eradicate the virus.
Here, then, is the current pandemic dilemma: Vaccines remain the best way for individuals to protect themselves, but societies cannot treat vaccines as their only defense. And for now, unvaccinated pockets are still large enough to sustain Delta surges, which can overwhelm hospitals, shut down schools, and create more chances for even worse variants to emerge. To prevent those outcomes, “we need to take advantage of every single tool we have at our disposal,” [Shweta Bansal of Georgetown University] said. These should include better ventilation to reduce the spread of the virus, rapid tests to catch early infections, and forms of social support such as paid sick leave, eviction moratoriums, and free isolation sites that allow infected people to stay away from others.
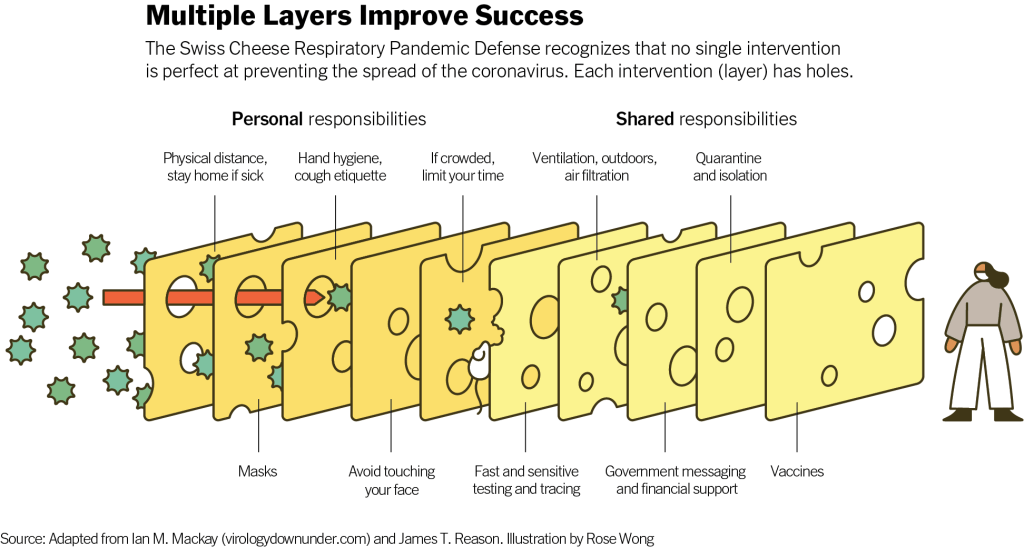
Remember that Swiss cheese model of pandemic interventions? Vaccines may be the best protection we have against the coronavirus, but they’re still just one layer of protection. All the other layers—masks, testing, ventilation, etc.—are still necessary, too. Especially when we’re dealing with a new variant that might not respond as well to our vaccines.
Re-upping this brilliant image from last year as a reminder on how mitigation measures work together to prevent the spread of coronavirus. pic.twitter.com/p7Z8u7fS2w
One strategy that we could employ against Omicron, as well as against the current Delta surge, is better masks. While cloth masks certainly make it less likely for the coronavirus to spread from one person to another, their efficacy varies greatly depending on the type of material, the number of layers, and the mask’s fit.
N95 masks do the best job at stopping the coronavirus from spreading, followed by KN95 masks. Surgical masks do a better job than cloth masks, but making sure these masks fit properly can be a challenge for some people (including yours truly, who has a very narrow face!). Layering a surgical mask and cloth mask may be a safer option to get both good fit and protection, though two layers of mask can be challenging to wear for long periods of time.
Some experts have recommended that the U.S. mail N95 or KN95 masks to all Americans, or at least require these masks in high-risk areas, such as on flights. Germany and other European countries established similar requirements last summer.
Given how transmissible Delta is—and the likelihood that Omicron is also highly transmissible—consider upgrading to an N95/KN95 mask or equivalent when indoors and around others, especially if you're elderly or immunocompromised.
In many countries—including the U.K., Germany, India, and others—rapid tests are freely available. Here in the U.S., on the other hand, the tests are quite expensive (often upwards of $10 for one test) and difficult to find, with pharmacies often limiting the number of packages that people can buy at once.
Biden has attempted to increase rapid testing access as part of his latest COVID-19 plan: in January, private insurance companies will be required to cover the cost of rapid tests. But this doesn’t solve the supply issue, and it doesn’t really make the tests more accessible, either. The measure would still require people to buy tests out of pocket, then fill out insurance reimbursement forms to maybe get their money back. Can you imagine anyone actually doing this?
In addition, as some experts have pointed out, the people most likely to need rapid tests—essential workers and others in high-risk environments—are also those less likely to have insurance. Biden is also distributing some rapid tests to community health centers, but that’s not enough to meet the need here.
This part of Biden’s omicron plan is also short-sighted.
Sure reimbursement by private health insurance of rapid test costs is a nice thing to have, but the people who MOST need rapid tests are the same people who DONT have private health care. What’s the plan for helping them? pic.twitter.com/tnlC8T0PDk
Ideally, the Biden administration would mail every American a pack of, like, 20 rapid tests, along with that pack of N95 or KN95 masks I mentioned above. Free of charge.
And at the same time, of course, we need more readily available PCR testing. Even in New York City, which has a better testing infrastructure than most other parts of the country, the lines at free testing sites are getting long again as cases go up. Any American who wants to get tested should be able to easily make an appointment within a day or two, and get their results within another day after that.
Increased testing is not only important for identifying Omicron cases (and cases of any other new variant); it’s also key for the Merck and Pfizer antiviral treatments due to be approved in the U.S. soon. Without efficient testing, patients won’t be able to start these treatments within days of their symptoms starting.
What we could do: improve genetic surveillance
The U.S. is doing a lot more coronavirus sequencing than we were in early 2021: we’ve gone from under 5,000 cases sequenced a week to over 80,000. The CDC worked with state and local health agencies, as well as research organizations and private companies, to increase sequencing capacity across the country.
Urban centers close to large academic centers tend to be well covered, while rural areas are less so. That means public health departments in large parts of the country are still flying blind, even as they are figuring out ways to prioritize Omicron-suspicious samples.
A lack of testing compounds this problem. If someone doesn’t confirm their COVID-19 case with a PCR test, their genetic information will never make it to a testing lab, much less a sequencing lab. While rapid tests are very useful for quickly finding out if you’re infected with the coronavirus, you need a PCR test for your information to actually be entered into the public health system.
In addition, even where the U.S. is sequencing a lot of samples, the process can take weeks. Vox’s Umair Irfan writes:
Still, it takes the US a median time of 28 days to sequence these genomes and upload the results to international databases. Contrast that with the United Kingdom, which sequences 112 genomes per 1,000 cases, taking a median of 10 days to deposit their results. A delay of only a few days in detection can give variants time to silently spread within communities and across borders.
Despite sequencing shortfalls in the U.S., we’re still doing much more surveillance than the majority of countries. Many nations in Africa, Asia, South America, and other parts of the world are sequencing fewer than 10 cases per 1,000, Irfan reports. As the U.S. should be doing more to get the world vaccinated, the U.S. should also do more to help other countries increase their sequencing capacity—monitoring for the variants that will inevitably follow Omicron.
What we could do: stricter domestic travel requirements
Starting on Monday, all international travelers coming into the U.S. by air will need to show a negative COVID-19 test, taken no more than one day before their flight. This includes all travelers regardless of nationality or vaccination status. At the same time, any non-U.S. citizens traveling into the country must provide proof of their vaccination against COVID-19.
But travelers flying domestically don’t face any such requirements. There are mask mandates on airplanes, true, but people can wear cloth masks, often pulled down below their noses, and airports tend to have limited enforcement of any mask rules.
Both experts and polls have supported requiring vaccination for domestic air travel, though the Biden administration seems very hesitant to put this requirement in place. Speaking for myself, I felt very unsafe the last time I flew domestically. A vaccine mandate for air travel would make me much more likely to fly again.
What we could do: more social support
In the U.S., a positive COVID-19 test usually means that you’re in isolation for 10 to 14 days, along with everyone else in your household. This can pull kids out of school, and pull income from families. As has been the case throughout the pandemic, support is needed for people who test positive, whether that’s a safe place to isolate for two weeks, grocery delivery, or rapid tests for the rest of the household.
This type of support could make people actually want to get tested when they have symptoms or an exposure risk, rather than avoiding the public health system entirely.
Within days of its first identification, the Omicron variant has been found on every continent except Antarctica. Chart via GISAID, retrieved December 5.
There is still a lot we don’t know about the Omicron variant, first identified in Botswana and South Africa in late November. For the most part, what I wrote last Sunday remains true: this variant is spreading quickly in South Africa and has a number of mutations—some of which may correspond to increased capacity for transmission or evading prior immunity—but we don’t yet have enough information to determine how it may shape the next phase of the pandemic.
Still, we’ve learned a few new things in the last week. Here’s a quick roundup:
More than 30 cases have been detected in the U.S., with the earliest detection in states with robust genetic surveillance. The first U.S. case was identified in California, in a San Francisco resident who had recently traveled to South Africa. As I pointed out on Twitter, California is one state that’s sequencing a lot of coronavirus genomes; combine that with San Francisco’s large international airport, and it may be unsurprising that the variant was first picked up there. The second U.S. case was identified in Minnesota; this state, too, has sequenced a lot of cases, with a lab at the University of Minnesota providing sequencing services for other Midwest states.
Omicron is spreading rapidly in South Africa. On Friday, South African scientists said that the variant may be spreading “more than twice as quickly as Delta,” according to the New York Times, though it may also be less contagious than Delta. This announcement aligns with modeling by computational biologist Trevor Bedford, who wrote on Saturday that Omicron appears to have a transmission advantage over Delta. “These are still very early estimates and all this will become more clear as we get comparable estimates from different geographies and with different methods,” Bedford wrote. “But ballpark current Rt of Omicron in South Africa of between 3 and 3.5 seems pretty reasonable.” Rt refers to how fast the virus is spreading; for context, Delta’s Rt when it first hit the U.S. was about 1.5.
Anime NYC may have been a superspreading event. The Minnesota resident who became the second Omicron case identified in the U.S. had attended Anime NYC, an anime convention held at the Javits Center between November 19 and 21. City and state officials urged other attendants of the convention to get tested; and a number of the Minnesota resident’s friends have tested positive, according to The Washington Post,though sequencing results are not yet available for these cases. Anime NYC attendees had to be vaccinated to attend, but could meet the requirement with just one dose received right before the convention. And photos from the convention show plenty of people disregarding the mask mandate. It’s too early to say, but I would not be surprised if Anime NYC turns out to be a superspreading event for Omicron.
A holiday party in Norway is another likely superspreading event. About 120 people attended a Christmas party in Oslo on November 26. As of this Friday, at least 13 attendees have been identified as Omicron cases, while a number of others have tested positive for COVID-19 (and are awaiting sequencing results). “Our working hypothesis is that at least half of the 120 participants were infected with the Omicron variant during the party,” Norwegian Institute of Public Health physician Preben Aavitsland told Reuters. “This makes this, for now, the largest Omicron outbreak outside South Africa.” Notably, this superspreading event occurred even though “all the attendees were fully vaccinated and had tested negative before the event,” Reuters reports.
Omicron appears to be more likely to reinfect people who’ve recovered from a previous COVID-19 case than past variants. On Thursday, South African scientists posted a preprint study suggesting that, when compared to the Delta and Beta variants, Omicron is more capable of reinfecting people who’ve previously had COVID-19. The finding comes from an analysis of over 35,000 reinfections among millions of positive COVID-19 tests. “Although there are a lot of uncertainties in the paper, it looks like an earlier infection only offers half as much protection against Omicron as it does against Delta,” writes Gretchen Vogel in Science, paraphrasing Emory University biostatistician Natalie Dean.
Omicron might cause less severe illness than other variants, but a lot more data are needed on this topic. On Saturday, the South African Medical Research Council posted a report that aligns with some other early reports about this variant: so far, patients infected with this variant seem to be getting less sick than those infected with previous coronavirus variants. Specifically: a lower share of Omicron patients in South Africa have required intensive care, oxygen support, or ventilators than physicians there have seen in previous COVID-19 waves. But this report, like other anecdotal reports, has been based on a small number of patients, and many of them have been younger—as older South Africans have been prioritized for vaccination. The number of severe Omicron cases may be low now, but may rise sharply in the coming weeks, Financial Times reporter John Burn-Murdoch pointed out in a Twitter thread responding to the report. Also, it’s way too soon to know how many of the so-called mild Omicron cases thus far may turn into Long COVID. So, a lot of experts are skeptical that Omicron is actually more mild—basically, we need more data.
BUT: now that I’ve injected a triple-dose of nuance, here’s your exponential case chart:
Even if far less than 25% of patients require ICU this time, a small share of a rapidly increasing number can still become a big number. And numbers are going up very, very fast. pic.twitter.com/HmWooHWoDw
I’ll end the post with this excellent thread from Muge Cevik, infectious disease expert at the University of St. Andrews, discussing the many uncertainties surrounding Omicron:
🦠 There’s a lot we don’t yet understand about Omicron, including its impact on immunity and what it means for vaccines. New data will be emerging over the next few wks, which could be misinterpreted w/o context. What we might expect & how to interpret the emerging data? 🧵(1/n)