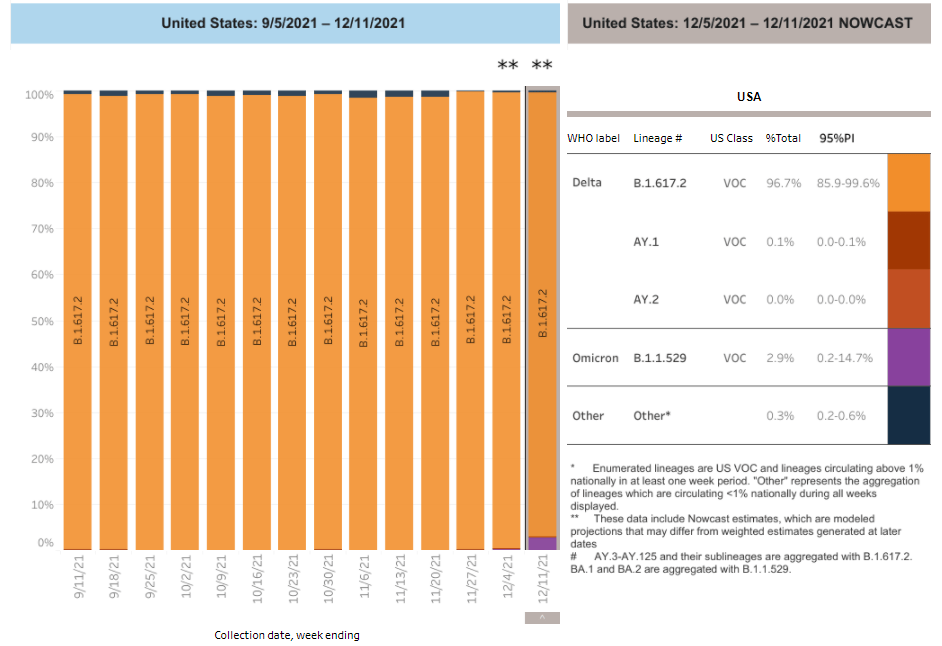
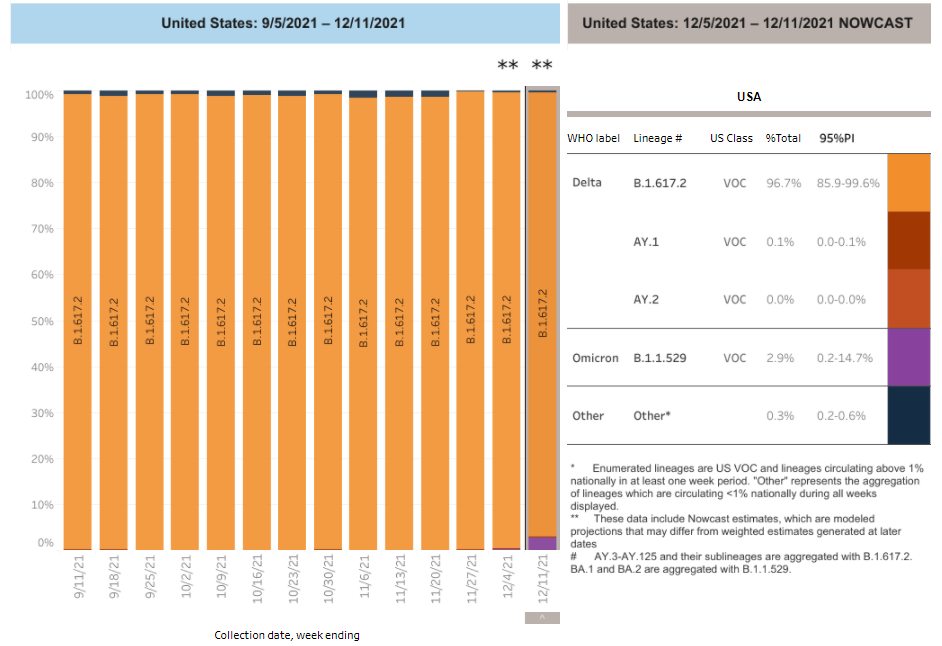
Due to reporting delays, the CDC’s variant data fails to convey Omicron’s rapid spread through the country. Chart retrieved on December 19.
On Tuesday, the CDC updated the Variant Proportions tab of its COVID-19 data dashboard. This update included some alarming information: Omicron had jumped from causing about 0.4% of cases in the week ending December 4, to 2.9% of cases in the week ending December 11. In the New York and New Jersey area, it was causing 13% of cases.
At this rate of increase, we can anticipate that, as of yesterday (December 18), Omicron is already causing roughly 21% of cases in the U.S.—and more than 90% of cases in New York and New Jersey. But because of the CDC’s delayed updates, the majority of people who go look at the CDC’s dashboard anytime before its next update, this coming Tuesday, would likely presume that Omicron is still causing a tiny minority of cases.
I’ve written before about the delays in collecting and reporting coronavirus sequencing data. It can take weeks for a COVID-19 test sample to go from a patient’s nose to a nationwide sequencing database, which leads to inevitable lags in the U.S.’s genomic surveillance. This is understandable. But in a crisis moment, when Omicron is here and spreading rapidly, the agency should clearly label the lags and update its projections to provide a more accurate view of the variant’s growth.
What’s more, the CDC’s data update on Tuesday was not communicated widely; Director Dr. Rochelle Walensky gave a TODAY Show interview, and that was about it.
being asked questions about this all day. I’m puzzled why such important health information that should be mobilizing hospital surge plans across the country would be done through a @TODAYshow interview? Maybe I’m missing something? https://t.co/jklCLdjTx8
We keep learning about this dangerous variant as it spreads through the U.S. and the world. A few major updates from this week:
Omicron is spreading rapidly in the U.S. Last Tuesday, the CDC announced that Omicron had gone from causing 0.4% of new COVID-19 cases nationwide in the week ending December 4, to 2.9% of cases in the week ending December 11. That’s a seven-fold increase over the course of a week; the variant appears to be doubling every two to three days, based on data from the U.K. We can assume that it will be the dominant variant in the U.S. by the end of December, if not sooner.
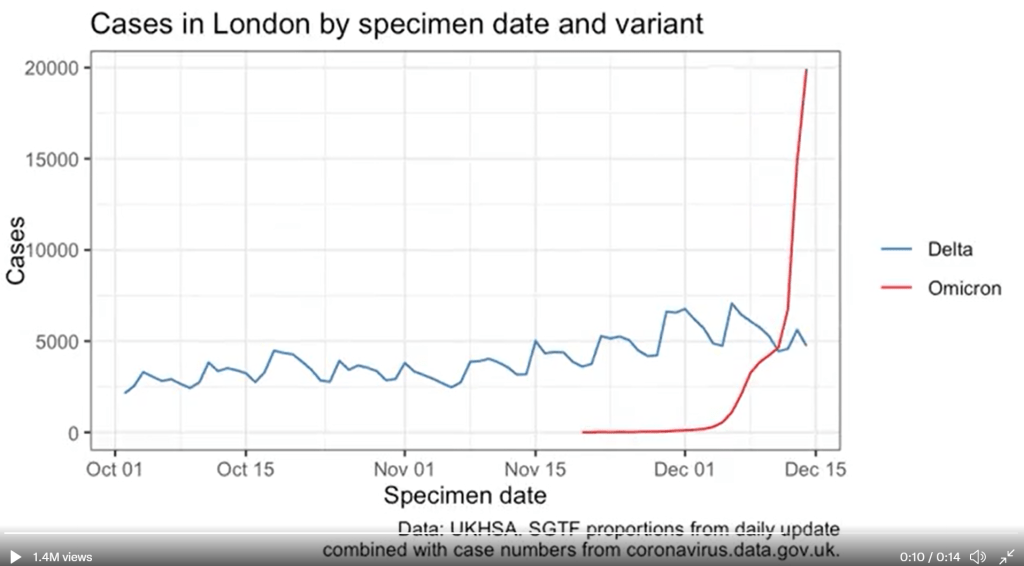
U.K. data provides information on just how fast Omicron can spread. The U.K.’s comprehensive genomic surveillance system, combined with its unified national public health system, allows British researchers to analyze their country’s Omicron cases in high detail. According to the latest briefing from the U.K. Health Security Agency (summarized by Meaghan Kall): risk of reinfection with Omicron is three to four times higher than with Delta; risk of household transmission with Omicron is two to three times higher than with Delta; and the variant is doubling every two days—or even every 1.5 days, in some parts of the U.K.
New research from Hong Kong provides insight into why Omicron spreads so fast. Preliminary data from a Hong Kong University research team suggests that, within 24 hours of an Omicron infection, the virus “multiplied about 70 times faster inside respiratory-tract tissue than the Delta variant,” reports Megan Molteni at STAT News. More virus in the respiratory tract means more virus getting out into the air, Molteni explains. At the same time, the variant seems to be worse at multiplying within lung tissue, which may contribute to milder disease. While the Hong Kong study has yet to be peer reviewed, this finding aligns with reports of superspreading events among fully vaccinated people.
Skepticism about “Omicron being mild” continues despite more reports. Early this week, the largest health insurance company in South Africa posted results of a study examining the country’s Omicron wave. The study found that risk of hospitalization was 29% lower for Omicron patients than it had been during the country’s spring 2020 COVID-19 surge. While this finding follows other reports out of South Africa, experts are still skeptical: in part because it can take weeks for a coronavirus infection to progress to hospitalization, and in part because South Africa’s population has a lot of prior immunity from past surges and vaccinations. Also, a “milder” variant that’s more transmissible can still lead to significantly more hospitalizations.
We’re getting more evidence that vaccination protects against severe disease from Omicron. Basically: two shots are good, three shots are better. “Though these data are preliminary, they suggest that getting a booster will help protect people already vaccinated from breakthrough or possible severe infections with Omicron during the winter months,” writes NIH Director Dr. Francis Collins in a recent blog post summarizing both laboratory and real-world studies. If you’re eligible for a booster and haven’t yet gotten it, now is a great time.
But: We don’t know how well vaccines protect against Long COVID from an Omicron infection. As many experts continue to say that Omicron cases are mild for those who are vaccinated, the Long COVID experts and advocates I follow have pointed out that a mild breakthrough case can still lead to this prolonged condition. “Omicron is a huge individual threat,” wrote Long COVID researcher Hannah Davis on Twitter recently. “A 15-30% chance of being disabled for at least a year, but likely for the rest of your life, is a bigger threat than most of us ever faced ever before the pandemic.”
Omicron *is* a huge individual threat. A 15-30% chance of being disabled for at least a year, but likely for the rest of your life, is a bigger threat than most of us ever faced *ever* before the pandemic. #LongCovidhttps://t.co/bDpM9GTlBy
New York City is an Omicron hotspot in the U.S. As I noted in today’s National Numbers post, this variant has clearly hit NYC, as seen in record case numbers and felt in long lines for testing throughout the city. According to CDC estimates, Omicron was causing about 13% of new cases reported in New York and New Jersey in the week ending December 11. One week later, knowing how fast Omicron has outcompeted Delta in the U.K. and elsewhere, we can assume that it’s now causing the majority of cases in this region.
Other U.S. states and regions may be behind in their Omicron sequencing, so assume it’s spreading in your area even if it hasn’t been officially identified yet. As I’ve written before, genomic surveillance in the U.S. is geographically very spotty. NYC is a clear hotspot, but it’s also a city with a lot of sequencing infrastructure. In other parts of the country, Omicron may not have been formally identified yet—but that doesn’t mean it isn’t spreading. Take Orlando, Florida as an example: wastewater sampling in the surrounding county found that Omicron was completely dominating the community this week, according to AP, even though “practically no cases of clinical infection” have been reported.
Good news: South Africa’s case numbers are now trending down. As of yesterday, COVID-19 case numbers in Gauteng, the center of South Africa’s COVID-19 outbreak, as well as in other parts of the country, seem to be turning around. Computational biologist Trevor Bedford offered some potential explanations in an interview with New York Magazine: limited testing capacity and milder disease may lead to underreporting of COVID-19 cases in South Africa; less of the population may be susceptible due to prior immunity; and the variant may spread so fast that it can quickly burn through social networks and other avenues of transmission. We’ll need to see whether South Africa’s decline holds, and whether we see similar patterns in other Omicron hotspots.
The U.S. is not prepared for an Omicron surge. If you haven’t yet, take some time today to read Ed Yong’s latest feature in The Atlantic, which discusses how the U.S. has failed to learn from past COVID-19 outbreaks and prepare for the Omicron surge that has already arrived. “Rather than trying to beat the coronavirus one booster at a time, the country needs to do what it has always needed to do—build systems and enact policies that protect the health of entire communities, especially the most vulnerable ones,” Yong writes.
Omicron has altered the trajectory of the pandemic. Another piece to take time for today is this article in Science by Kai Kupferschmidt, discussing the “really, really tough winter” that scientists now see coming. Kupferschmidt explains that, even if many Omicron cases are mild, the variant is still spreading fast enough that it could land a lot of people in the hospital. In addition, the variant “may bring other, unpleasant evolutionary surprises” if future coronavirus variants evolve out of Omicron, Kupferschmidt writes.
This is one of the most confusing times of the pandemic, w/ a firehose of new Omicron data (lots of fab work on #medtwitter putting it into context). In this (long) 🧵, I'll offer my take on how the new information is changing my thinking & behavior.(1/25)
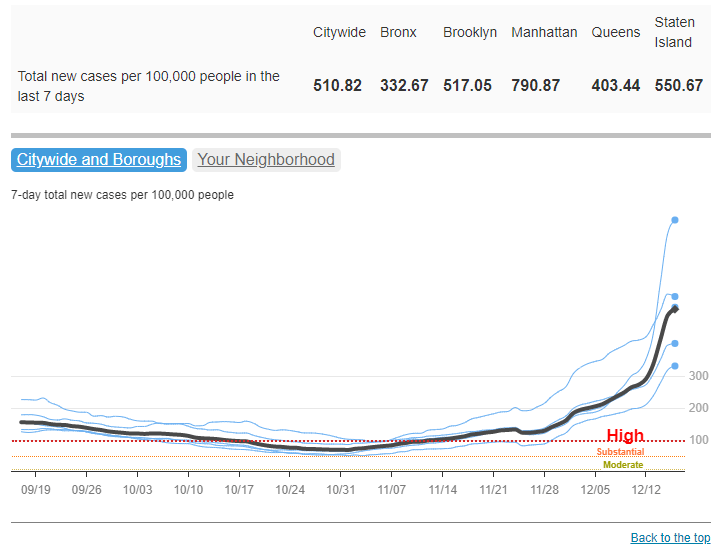
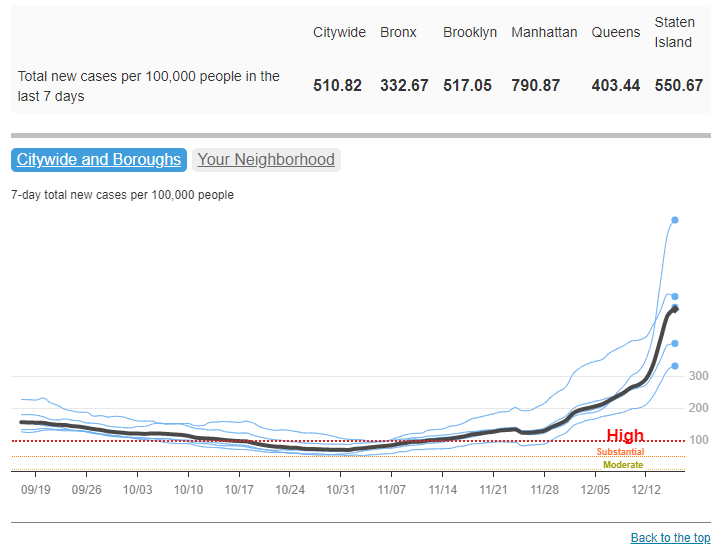
COVID-19 cases have increased sharply in New York City in the past week, to over 500 new cases for every 100,000 people city-wide. Chart via NYC Health, retrieved December 19.
In the past week (December 11 through 17), the U.S. reported about 860,000 new cases, according to the CDC. This amounts to:
An average of 122,000 new cases each day
261 total new cases for every 100,000 Americans
2%more new cases than last week (December 4-10)
Last week, America also saw:
55,000 new COVID-19 patients admitted to hospitals (17 for every 100,000 people)
8,300 new COVID-19 deaths (2.5 for every 100,000 people)
2.9% of new cases are Omicron-caused (as of December 11)
An average of 1.6 million vaccinations per day (including booster shots; per Bloomberg)
The Omicron surge has arrived in the U.S. While national COVID-19 cases are not significantly up from last week to this week, last week’s bump in the numbers from delayed Thanksgiving reporting has been replaced with a true increase, thanks to the combined pressures of both Delta and Omicron.
Hospitalizations are also increasing, with about 60,000 Americans hospitalized with COVID-19 nationwide as of December 15—a 9% increase from the previous week. The number of Americans dying from COVID-19 each day is increasing as well, now at about 1,200 deaths a day.
To be fair, the case rates reported in NYC this week are probably lower than the true case rates during spring 2020, as testing wasn’t widely available during the city’s first COVID-19 surge. But on a personal level, this city’s current Omicron surge is undeniable: testing lines stretch around the block, and everyone from my old college friends to my local City Council representative is reporting a breakthrough case. I personally have yet to catch “the Media Variant,” but I’m rapid testing frequently and avoiding indoor activities as I prepare to visit my parents for Christmas.
the more I hear about friends/acquaintances/nyc media people/etc getting breakthrough covid cases, the more I'm assuming that, like, every other one of these cases is omicron pic.twitter.com/mSonuhdrHm
Omicron was causing 13% of new COVID-19 cases in New York and New Jersey in the week ending December 11. By today, it’s likely causing the majority of new cases. But the NYC region isn’t the only part of the country seeing rapid case increases: Hawaii, Florida, Connecticut, Maine, and D.C. have all reported more than a 30% increase in cases from the previous week to this one, according to the latest Community Profile Report. Rhode Island, New Hampshire, Maine, and other Northern states have the highest cases per capita.
Vaccines, particularly booster shots, can protect against this dangerous variant (more on that later in this issue). While 61% of Americans are fully vaccinated, according to the CDC, less than 30% have received booster doses. This includes about 53% of Americans over 65, even though seniors were one of the first groups become eligible for boosters—and are among those most in need of this additional protection.
Boost every adult, especially high risk
Use lots of rapid tests
Encourage masks in high-risk public indoor spaces
Use test and stay to keep kids, workers safe in school/work
And be prepared for a complicated and disruptive January
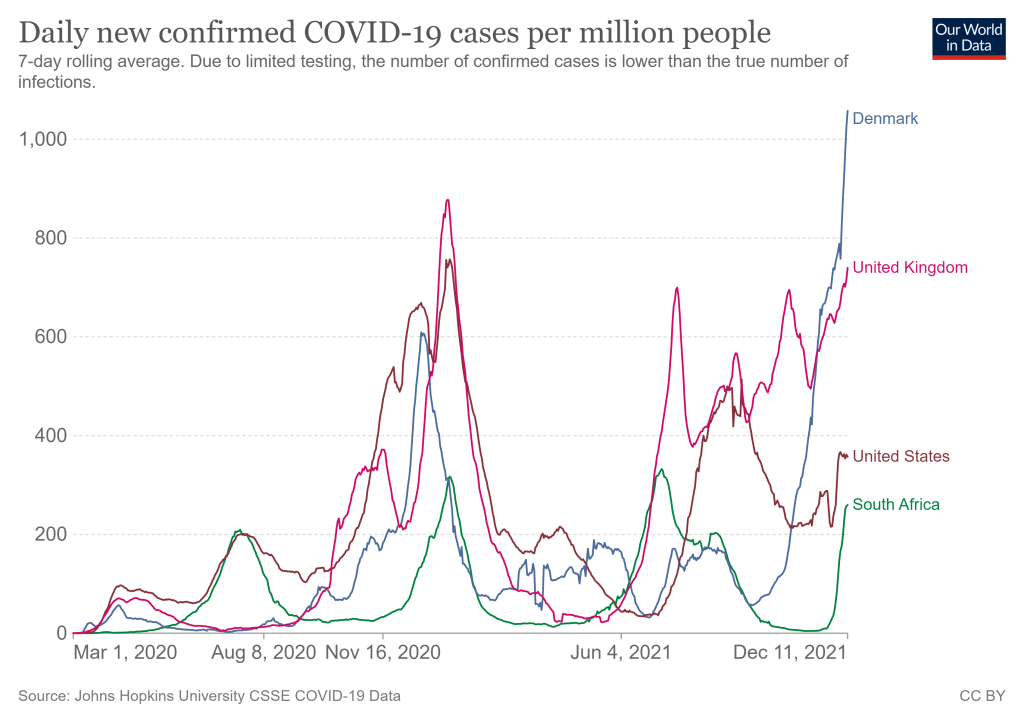
COVID-19 cases are rising rapidly in countries where Omicron is spreading, including South Africa, the U.K., and Denmark. Chart from Our World in Data, retrieved September 12.
We continue to learn more about this new variant as it spreads rapidly across the world, though much of the data are still preliminary. Here are a few major updates:
Omicron is still spreading very quickly in South Africa, as well as in the U.K. and Denmark—two other countries with great genetic surveillance. Preliminary estimatesbased on data from these countries suggest that the variant’s R-value is between 3 and 4, indicating that the average person infected with Omicron infects three or four others. As Sarah Zhang put it in The Atlantic: “Omicron is spreading in highly immune populations as quickly as the original virus did in populations with no immunity at all.”
Early vaccine studies show a drop in antibody levels against Omicron, but that doesn’t necessarily correspond to overall protection. This week, we saw the first results from early studies evaluating how well vaccines work against Omicron. Here’s a summary, drawing from Katherine Wu’s coverage of these studies in The Atlantic: vaccinated people confronted with Omicron appear to produce a lot fewer antibodies that can fight the virus, compared with older variants. Numbers range from a five-fold drop in antibodies to a 41-fold drop. But remember, antibodies are just one part of the immune system—specifically, they’re the part that’s easiest to measure. Vaccinated people also have memory immune cells that provide protection over a long time period, which isn’t captured in antibody studies. We’ll need more time and more data to actually evaluate how vaccines fare against Omicron in the real world, rather than in the lab.
The vaccines seem to protect against severe disease and death from Omicron. So far, the data suggest that our existing COVID-19 vaccines still work quite well at protecting people from severe symptoms—even when those severe symptoms are caused by an Omicron case. “When the shots’ protection ebbs, it tends to do so stepwise: first, against infection, then transmission and symptoms, and finally against severe disease,” Wu writes. For vaccinated people to lose protection against severe disease, the virus would have to change much more than Omicron has. At the same time, however, some experts are concerned that non-mRNA vaccines may not fare as well against Omicron as Moderna and Pfizer, conferring a disadvantage to the low- and middle-income countries that have had less access to the mRNA vaccines.
Booster shots increase protection against Omicron. While vaccinated people are less protected against infection with Omicron than previous variants, booster shots appear to help close that gap—even though currently-available booster shots are not designed specifically for Omicron. One U.K. study suggests that boosters can increase vaccine effectiveness against infection from 30% to 75%, for people who received the Pfizer vaccines. In other words: Omicron is a good reason to go get your booster shot, if you’re eligible and you live in a place where the shots are available.
Experts continue to be skeptical about Omicron being “more mild.” Reports out of South Africa continue to suggest that cases caused by Omicron are more mild than cases caused by Delta, with doctors saying that fewer patients are requiring hospitalization and those hospital stays are shorter than previous outbreaks. But many of the South Africans getting sick with Omicron may have some protection from vaccination or past infection; this means they’re more likely to have mild cases, as biostatistician Natalie Dean explains in an excellent Twitter thread. Plus, even if Omicron is more mild, it appears to be more transmissible—and a smaller share of severe cases out of a larger pool of cases overall can still lead to a pretty big number of people going to the hospital. In addition, we have zero data at this point on how Omicron may impact Long COVID cases, or how well vaccines protect against Long COVID from an Omicron infection.
Early U.K. data confirm Omicron’s high contagiousness and its capacity for evading protection from vaccines and prior cases. After the U.K.’s best-in-the-world genetic surveillance agency first identified Omicron in late November, I wrote that the country would likely provide invaluable data on this variant. Less than two weeks later, the U.K. Health Security Agency has released its first Omicron report. The country’s real-world data confirm that Omicron can spread quite fast: for example, “19% of Omicron cases resulted in household outbreaks vs 8.5% of Delta cases,” wrote epidemiologist Meaghan Kall in a summary of the report. The report also “paints a very consistent picture for Omicron being immune evading,” Kall said, though booster shots help a lot.
Anime NYC was a likely Omicron superspreader event. More and more reports have emerged of Omicron cases connected to Anime NYC, a convention held in Manhattan in mid-November. The CDC is currently investigating the convention: officials are working with the NYC health department to contact all 53,000 convention attendees for testing and contact tracing. “Data from this investigation will likely provide some of the earliest looks in this country on the transmissibility of the variant,” CDC Director Dr. Rochelle Walensky said at a press briefing on Tuesday.
The CDC formally named Omicron a Variant of Concern. On Friday, the CDC officially designated Omicron as a Variant of Concern and added it to the variant tracking page of the agency’s COVID-19 dashboard. As of December 4, Omicron is causing 0.0% of new COVID-19 cases in the U.S., the CDC estimates. The variant has yet to be added to the CDC’s state-by-state data. Given the continued geographic disparities of the U.S.’s genomic surveillance system, however, we may expect that the variant is already spreading in states where it has yet to be formally identified.
Omicron can likely compete with Delta, but we need more data to get a better sense of how well. “Omicron is picking up speed in Europe, which has often served as a preview of what was headed the U.S.’s way. It’s an early sign that the already bleak situation here may get worse,” writes Andrew Joseph in a recent STAT News story. U.K. data suggest that Omicron could cause a majority of cases there within two to four weeks, Joseph reports, and the U.S. may not be far behind. Still, more real-world data from countries and regions with clear Omicron outbreaks will give us a better idea of just how worried we need to be about a potential Omicron-fueled surge.
In summary:
There's been a lot of new data for Omicron in the last day, much still preliminary, but here's my summary of the good and bad pic.twitter.com/pL8uiD7hfV
As the world waits for more information on Omicron, I’d like to give a shout-out to the scientists collecting data on this novel variant and sharing it with the public. As of today, over 500 Omicron sequences have been posted to the genome sharing site GISAID.
If you’d like to keep up with the new sequences, there are three sources I recommend:
GISAID, an international organization working to quickly share data on coronavirus and flu virus strains.
Nextstrain, an open-source pathogen tracking platform supported by the Fred Hutchinson Cancer Research Center and other institutions.
CoVariants, a platform visualizing coronavirus variant data, run by Dr. Emma Hodcroft at the University of Bern with support from other scientists.
This past Monday, President Biden gave a speech about the Omicron variant. He told America that Omicron is “cause for concern, not a cause for panic,” and thanked the South African scientists who alerted the world to this variant. (Though a travel ban is not a great way to thank those scientists!)
Towards the end of the speech, he said: “We’re throwing everything we can at this virus, tracking it from every angle.” Which I, personally, found laughable. As I’ve pointed out in a previous post about booster shots, the U.S.’s anti-COVID strategy basically revolves around vaccines, and has for most of 2021.
wild to hear Biden say "we are throwing everything we can at this virus" … like, sir, no we aren't. we are throwing ONE THING (vaccines) at this virus.
My Tweet about Biden’s vaccine-only strategy got more attention than I’m used to receiving on the platform, so I thought it was a worthwhile topic to expand upon in the COVID-19 Data Dispatch. Why aren’t vaccines enough to address Omicron—or our current surge, for that matter—and what else could the Biden administration be doing to slow the coronavirus’ spread?
Why aren’t vaccines enough?
Prior to Delta’s spread, there was some talk of reaching herd immunity: perhaps if 70% or 80% of Americans got fully vaccinated, it would be sufficient to tamp down on the coronavirus. But Delta’s increased capacity to spread quickly, combined with the vaccines’ decreased capacity to protect against infection and transmission, have shown that vaccines are not enough to eradicate the virus.
Here, then, is the current pandemic dilemma: Vaccines remain the best way for individuals to protect themselves, but societies cannot treat vaccines as their only defense. And for now, unvaccinated pockets are still large enough to sustain Delta surges, which can overwhelm hospitals, shut down schools, and create more chances for even worse variants to emerge. To prevent those outcomes, “we need to take advantage of every single tool we have at our disposal,” [Shweta Bansal of Georgetown University] said. These should include better ventilation to reduce the spread of the virus, rapid tests to catch early infections, and forms of social support such as paid sick leave, eviction moratoriums, and free isolation sites that allow infected people to stay away from others.
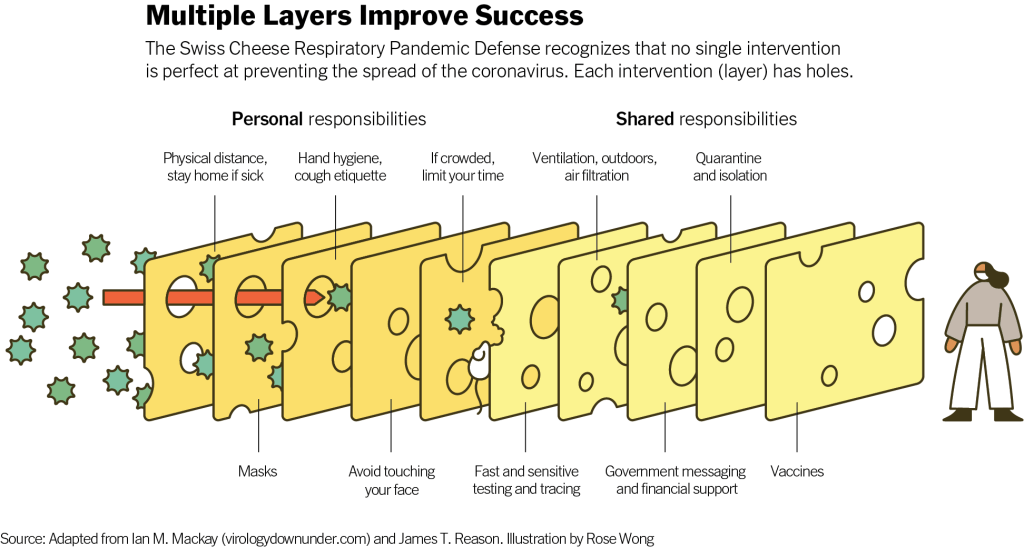
Remember that Swiss cheese model of pandemic interventions? Vaccines may be the best protection we have against the coronavirus, but they’re still just one layer of protection. All the other layers—masks, testing, ventilation, etc.—are still necessary, too. Especially when we’re dealing with a new variant that might not respond as well to our vaccines.
Re-upping this brilliant image from last year as a reminder on how mitigation measures work together to prevent the spread of coronavirus. pic.twitter.com/p7Z8u7fS2w
One strategy that we could employ against Omicron, as well as against the current Delta surge, is better masks. While cloth masks certainly make it less likely for the coronavirus to spread from one person to another, their efficacy varies greatly depending on the type of material, the number of layers, and the mask’s fit.
N95 masks do the best job at stopping the coronavirus from spreading, followed by KN95 masks. Surgical masks do a better job than cloth masks, but making sure these masks fit properly can be a challenge for some people (including yours truly, who has a very narrow face!). Layering a surgical mask and cloth mask may be a safer option to get both good fit and protection, though two layers of mask can be challenging to wear for long periods of time.
Some experts have recommended that the U.S. mail N95 or KN95 masks to all Americans, or at least require these masks in high-risk areas, such as on flights. Germany and other European countries established similar requirements last summer.
Given how transmissible Delta is—and the likelihood that Omicron is also highly transmissible—consider upgrading to an N95/KN95 mask or equivalent when indoors and around others, especially if you're elderly or immunocompromised.
In many countries—including the U.K., Germany, India, and others—rapid tests are freely available. Here in the U.S., on the other hand, the tests are quite expensive (often upwards of $10 for one test) and difficult to find, with pharmacies often limiting the number of packages that people can buy at once.
Biden has attempted to increase rapid testing access as part of his latest COVID-19 plan: in January, private insurance companies will be required to cover the cost of rapid tests. But this doesn’t solve the supply issue, and it doesn’t really make the tests more accessible, either. The measure would still require people to buy tests out of pocket, then fill out insurance reimbursement forms to maybe get their money back. Can you imagine anyone actually doing this?
In addition, as some experts have pointed out, the people most likely to need rapid tests—essential workers and others in high-risk environments—are also those less likely to have insurance. Biden is also distributing some rapid tests to community health centers, but that’s not enough to meet the need here.
This part of Biden’s omicron plan is also short-sighted.
Sure reimbursement by private health insurance of rapid test costs is a nice thing to have, but the people who MOST need rapid tests are the same people who DONT have private health care. What’s the plan for helping them? pic.twitter.com/tnlC8T0PDk
Ideally, the Biden administration would mail every American a pack of, like, 20 rapid tests, along with that pack of N95 or KN95 masks I mentioned above. Free of charge.
And at the same time, of course, we need more readily available PCR testing. Even in New York City, which has a better testing infrastructure than most other parts of the country, the lines at free testing sites are getting long again as cases go up. Any American who wants to get tested should be able to easily make an appointment within a day or two, and get their results within another day after that.
Increased testing is not only important for identifying Omicron cases (and cases of any other new variant); it’s also key for the Merck and Pfizer antiviral treatments due to be approved in the U.S. soon. Without efficient testing, patients won’t be able to start these treatments within days of their symptoms starting.
What we could do: improve genetic surveillance
The U.S. is doing a lot more coronavirus sequencing than we were in early 2021: we’ve gone from under 5,000 cases sequenced a week to over 80,000. The CDC worked with state and local health agencies, as well as research organizations and private companies, to increase sequencing capacity across the country.
Urban centers close to large academic centers tend to be well covered, while rural areas are less so. That means public health departments in large parts of the country are still flying blind, even as they are figuring out ways to prioritize Omicron-suspicious samples.
A lack of testing compounds this problem. If someone doesn’t confirm their COVID-19 case with a PCR test, their genetic information will never make it to a testing lab, much less a sequencing lab. While rapid tests are very useful for quickly finding out if you’re infected with the coronavirus, you need a PCR test for your information to actually be entered into the public health system.
In addition, even where the U.S. is sequencing a lot of samples, the process can take weeks. Vox’s Umair Irfan writes:
Still, it takes the US a median time of 28 days to sequence these genomes and upload the results to international databases. Contrast that with the United Kingdom, which sequences 112 genomes per 1,000 cases, taking a median of 10 days to deposit their results. A delay of only a few days in detection can give variants time to silently spread within communities and across borders.
Despite sequencing shortfalls in the U.S., we’re still doing much more surveillance than the majority of countries. Many nations in Africa, Asia, South America, and other parts of the world are sequencing fewer than 10 cases per 1,000, Irfan reports. As the U.S. should be doing more to get the world vaccinated, the U.S. should also do more to help other countries increase their sequencing capacity—monitoring for the variants that will inevitably follow Omicron.
What we could do: stricter domestic travel requirements
Starting on Monday, all international travelers coming into the U.S. by air will need to show a negative COVID-19 test, taken no more than one day before their flight. This includes all travelers regardless of nationality or vaccination status. At the same time, any non-U.S. citizens traveling into the country must provide proof of their vaccination against COVID-19.
But travelers flying domestically don’t face any such requirements. There are mask mandates on airplanes, true, but people can wear cloth masks, often pulled down below their noses, and airports tend to have limited enforcement of any mask rules.
Both experts and polls have supported requiring vaccination for domestic air travel, though the Biden administration seems very hesitant to put this requirement in place. Speaking for myself, I felt very unsafe the last time I flew domestically. A vaccine mandate for air travel would make me much more likely to fly again.
What we could do: more social support
In the U.S., a positive COVID-19 test usually means that you’re in isolation for 10 to 14 days, along with everyone else in your household. This can pull kids out of school, and pull income from families. As has been the case throughout the pandemic, support is needed for people who test positive, whether that’s a safe place to isolate for two weeks, grocery delivery, or rapid tests for the rest of the household.
This type of support could make people actually want to get tested when they have symptoms or an exposure risk, rather than avoiding the public health system entirely.
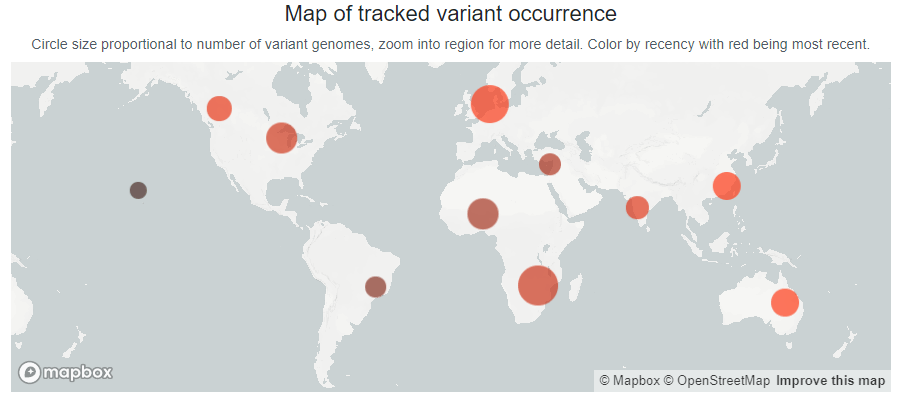
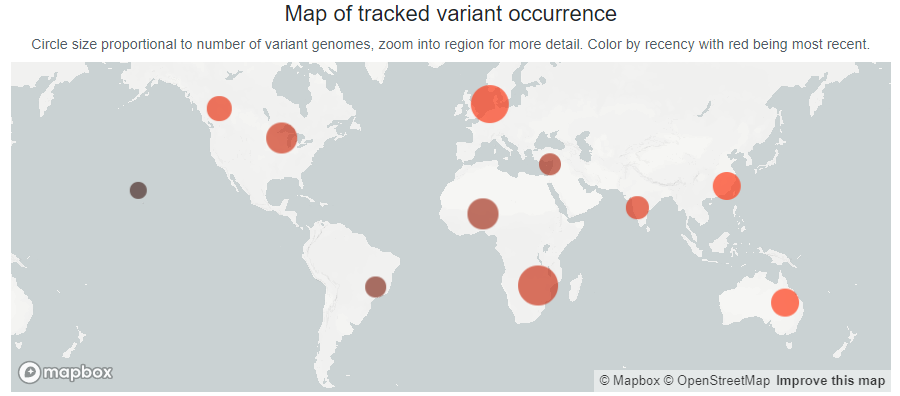
Within days of its first identification, the Omicron variant has been found on every continent except Antarctica. Chart via GISAID, retrieved December 5.
There is still a lot we don’t know about the Omicron variant, first identified in Botswana and South Africa in late November. For the most part, what I wrote last Sunday remains true: this variant is spreading quickly in South Africa and has a number of mutations—some of which may correspond to increased capacity for transmission or evading prior immunity—but we don’t yet have enough information to determine how it may shape the next phase of the pandemic.
Still, we’ve learned a few new things in the last week. Here’s a quick roundup:
More than 30 cases have been detected in the U.S., with the earliest detection in states with robust genetic surveillance. The first U.S. case was identified in California, in a San Francisco resident who had recently traveled to South Africa. As I pointed out on Twitter, California is one state that’s sequencing a lot of coronavirus genomes; combine that with San Francisco’s large international airport, and it may be unsurprising that the variant was first picked up there. The second U.S. case was identified in Minnesota; this state, too, has sequenced a lot of cases, with a lab at the University of Minnesota providing sequencing services for other Midwest states.
Omicron is spreading rapidly in South Africa. On Friday, South African scientists said that the variant may be spreading “more than twice as quickly as Delta,” according to the New York Times, though it may also be less contagious than Delta. This announcement aligns with modeling by computational biologist Trevor Bedford, who wrote on Saturday that Omicron appears to have a transmission advantage over Delta. “These are still very early estimates and all this will become more clear as we get comparable estimates from different geographies and with different methods,” Bedford wrote. “But ballpark current Rt of Omicron in South Africa of between 3 and 3.5 seems pretty reasonable.” Rt refers to how fast the virus is spreading; for context, Delta’s Rt when it first hit the U.S. was about 1.5.
Anime NYC may have been a superspreading event. The Minnesota resident who became the second Omicron case identified in the U.S. had attended Anime NYC, an anime convention held at the Javits Center between November 19 and 21. City and state officials urged other attendants of the convention to get tested; and a number of the Minnesota resident’s friends have tested positive, according to The Washington Post,though sequencing results are not yet available for these cases. Anime NYC attendees had to be vaccinated to attend, but could meet the requirement with just one dose received right before the convention. And photos from the convention show plenty of people disregarding the mask mandate. It’s too early to say, but I would not be surprised if Anime NYC turns out to be a superspreading event for Omicron.
A holiday party in Norway is another likely superspreading event. About 120 people attended a Christmas party in Oslo on November 26. As of this Friday, at least 13 attendees have been identified as Omicron cases, while a number of others have tested positive for COVID-19 (and are awaiting sequencing results). “Our working hypothesis is that at least half of the 120 participants were infected with the Omicron variant during the party,” Norwegian Institute of Public Health physician Preben Aavitsland told Reuters. “This makes this, for now, the largest Omicron outbreak outside South Africa.” Notably, this superspreading event occurred even though “all the attendees were fully vaccinated and had tested negative before the event,” Reuters reports.
Omicron appears to be more likely to reinfect people who’ve recovered from a previous COVID-19 case than past variants. On Thursday, South African scientists posted a preprint study suggesting that, when compared to the Delta and Beta variants, Omicron is more capable of reinfecting people who’ve previously had COVID-19. The finding comes from an analysis of over 35,000 reinfections among millions of positive COVID-19 tests. “Although there are a lot of uncertainties in the paper, it looks like an earlier infection only offers half as much protection against Omicron as it does against Delta,” writes Gretchen Vogel in Science, paraphrasing Emory University biostatistician Natalie Dean.
Omicron might cause less severe illness than other variants, but a lot more data are needed on this topic. On Saturday, the South African Medical Research Council posted a report that aligns with some other early reports about this variant: so far, patients infected with this variant seem to be getting less sick than those infected with previous coronavirus variants. Specifically: a lower share of Omicron patients in South Africa have required intensive care, oxygen support, or ventilators than physicians there have seen in previous COVID-19 waves. But this report, like other anecdotal reports, has been based on a small number of patients, and many of them have been younger—as older South Africans have been prioritized for vaccination. The number of severe Omicron cases may be low now, but may rise sharply in the coming weeks, Financial Times reporter John Burn-Murdoch pointed out in a Twitter thread responding to the report. Also, it’s way too soon to know how many of the so-called mild Omicron cases thus far may turn into Long COVID. So, a lot of experts are skeptical that Omicron is actually more mild—basically, we need more data.
BUT: now that I’ve injected a triple-dose of nuance, here’s your exponential case chart:
Even if far less than 25% of patients require ICU this time, a small share of a rapidly increasing number can still become a big number. And numbers are going up very, very fast. pic.twitter.com/HmWooHWoDw
I’ll end the post with this excellent thread from Muge Cevik, infectious disease expert at the University of St. Andrews, discussing the many uncertainties surrounding Omicron:
🦠 There’s a lot we don’t yet understand about Omicron, including its impact on immunity and what it means for vaccines. New data will be emerging over the next few wks, which could be misinterpreted w/o context. What we might expect & how to interpret the emerging data? 🧵(1/n)
On Thanksgiving, my Twitter feed was dominated not by food photos, but by news of a novel coronavirus variant identified in South Africa earlier this week. While the variant—now called Omicron, or B.1.1.529—likely didn’t originate in South Africa, data from the country’s comprehensive surveillance system provided enough evidence to suggest that this variant could be more contagious than Delta, as well as potentially more able to evade human immune systems.
Note that the words suggest and could be are doing a lot of work here. There’s plenty we don’t know yet about this variant, and scientists are already working hard to understand it.
But the early evidence is substantial enough that the World Health Organization (WHO) designated Omicron as a Variant of Concern on Friday. And, that same day, the Biden administration announced new travel restrictions on South Africa and several neighboring countries. (More on that later.)
In today’s issue, I’ll explain what we know about the Omicron variant so far, as well as the many questions that scientists around the world are already investigating. Along the way, I’ll link to plenty of articles and Twitter threads where you can learn more. As always, if you have more questions: comment below, email me, (betsy@coviddatadispatch.com), or hit me up on Twitter.
Where did the Omicron variant come from?
This is one major unknown at the moment. South Africa was the first country to detect Omicron this past Monday, according to STAT News. But the variant likely didn’t originate in South Africa; rather, this country was more likely to pick up its worrying signal because it has a comprehensive variant surveillance system.
Per The Conversation, this system includes: “a central repository of public sector laboratory results at the National Health Laboratory Service, good linkages to private laboratories, the Provincial Health Data Centre of the Western Cape Province, and state-of-the-art modeling expertise.”
1) My gut feeling from hearing of Omicron cases in Botswana, ex-Malawi, ex-Egypt (2 now it seems) and in South Africa is, that the variant was flying under the radar in undersequenced countries for some time until Botswana and South Africa detected it and sounded the alarm.
Researchers from South Africa and the other countries that have detected Omicron this week are already sharing genetic sequences on public platforms, driving much of the scientific discussion about this variant. So far, one interesting aspect of this variant is that, even though Delta has dominated the coronavirus landscape globally for months, Omicron did not evolve out of Delta.
Instead, it may have evolved over the course of a long infection in a single, immunocompromised individual. It also may have flown under the radar in a country or region with poor genomic surveillance—which, as computational biologist Trevor Bedford pointed out on Twitter, is “certainly not South Africa”—and then was detected once it landed in that country.
This extremely long branch (>1 year) indicates an extended period of circulation in a geography with poor genomic surveillance (certainly not South Africa) or continual evolution in a chronically infected individual before spilling back into the population. 4/16 pic.twitter.com/8mEI46VFMn
Omicron seems to be spreading very quickly in South Africa—potentially faster than the Delta variant. Based on publicly available sequence data, Bedford estimated that it’s doubling exponentially every 4.8 days.
An important caveat here, however, is that South Africa had incredibly low case numbers before Omicron was detected—its lowest case numbers since spring 2020, in fact. So, we cannot currently say that Omicron is “outcompeting” Delta, since there wasn’t much Delta present for Omicron to compete with. The current rise in cases may be caused by Omicron, or it may be the product of a few superspreading events that happen to include Omicron; we need more data to say for sure.
Still, as Financial Times data reporter John Burn-Murdoch pointed out: “There’s a clear upward trend. This may be a blip, but this is how waves start.”
2) This is coinciding with a wider rise in cases in South Africa.
Again, currently we’re talking about small numbers (both of B.1.1.529 and of cases in SA overall), but there’s a clear upward trend. This may be a blip, but this is how waves start. pic.twitter.com/sn9IIKtzUm
Another major cause for concern is that Omicron has over 30 mutations on its spike protein, an important piece of the coronavirus that our immune systems learn to recognize through vaccination. Some of these mutations may correlate to increased transmission—meaning, they help the virus spread more quickly—while other mutations may correlate to evading the immune system.
Notably, a lot of the mutations on Omicron are mutations that we simply haven’t seen yet in other variants. On this diagram from genomics expert Jeffrey Barrett, the purple, yellow, and blue mutations are all those we haven’t seen on previous variants of concern, while the red mutations (there are nine) have been seen in previous variants of concern and are known to be bad.
Took a look at the spike mutations in B.1.1.529 this evening, and colour coded them (details below)…there is…not much green.🧵 pic.twitter.com/yNHM55oTTH
Some of these new mutations could be terrible news, or they could be harmless. We need more study to figure that out. This recent article in Science provides more information on why scientists are worried about Omicron’s mutations, as well as what they’re doing to investigate.
How many Omicron cases have been detected so far?
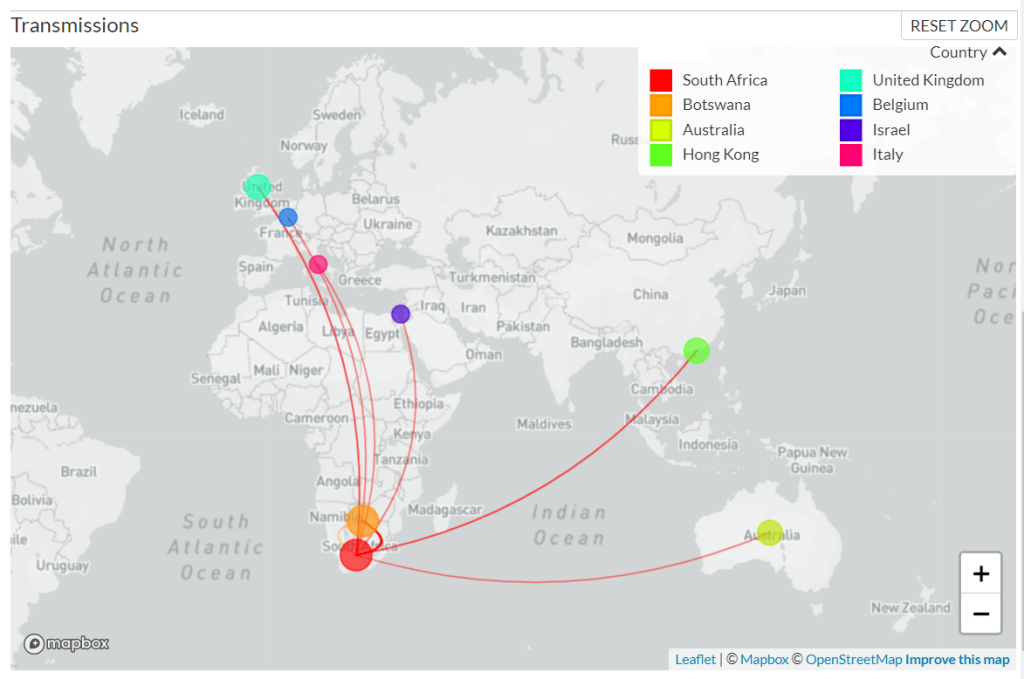
As of Sunday morning, genetic sequences from 127 confirmed Omicron cases have been shared to GISAID, the international genome sharing platform. The majority of these cases (99) were identified in South Africa, while 19 were identified in nearby Botswana, two in Hong Kong, two in Australia, two in the U.K., one in Israel, one in Belgium, and one in Italy.
According to BNO News, over 1,000 probable cases of the variant have already been identified in these countries. Cases have also been identified in the Netherlands, Germany, Denmark, the Czech Republic, and Austria. Many of the cases in the Netherlands are connected to a single flight from South Africa; the travelers on this flight were all tested upon their arrival, and 61 tested positive—though authorities are still working to determine how many of those cases are Omicron.
The U.K. Health Security Agency announced on Saturday that it had confirmed two Omicron cases in the country. Both of these cases, like those in Israel and Belgium, have been linked to travel—though the Belgium case had no travel history in South Africa. “This means that the virus is already circulating in communities,” Dr. Katelyn Jetelina writes in a Your Local Epidemiologist post about Omicron.
After South African scientists sounded the alarm about Omicron, cases were detected in Botswana, Australia, Hong Kong, Israel, the U.K., and other countries. Chart via GISAID, screenshot taken about 11:30 AM NYC time on November 28.
Luckily, Omicron is easy to identify because one of its spike protein mutations enables detection on a PCR test—no genomic sequencing necessary. Alpha, the variant that originated in the U.K. last winter, has a similar quality.
How does Omicron compare to Delta?
This is another major unknown right now. As I mentioned earlier, Omicron is spreading quickly in South Africa, at a rate faster than Delta spread when it arrived in the country a few months ago. But South Africa was seeing a very low COVID-19 case rate before Omicron arrived, making it difficult to evaluate whether this new variant is directly outcompeting Delta—or whether something else is going on.
(Note that a couple of the tweets below refer to this variant as “Nu,” as they were posted prior to the WHO designating it Omicron.)
A short list of what NO ONE knows about the Nu (B.1.1.529) variant:
– We DON'T KNOW if it spreads faster than delta – We DON'T KNOW where it originated – We DON'T KNOW if it bypasses immunity/causes more severe disease
We also don’t know if Omicron could potentially evade the human immune system, whether that means bypassing immunity from a past coronavirus infection or from vaccination. However, vaccine experts say that a variant that would entirely evade vaccines is pretty improbable.
Every single coronavirus variant of concern that we’ve encountered so far has responded to the vaccines in some capacity. And the variants that have posed more of a danger to vaccine-induced immunity (Beta, Gamma) have not become dominant on a global scale, since they’ve been less transmissible than Delta. Our vaccines are very good—not only do they drive production of anti-COVID antibodies, they also push the immune system to remember the coronavirus for a long time.
But remember that our immune system has more than just neutralising antibodies in store, so none of this tells us just how much this variant is going to escape immunity and if it will mostly affect protection from infection or also severe disease.
It’s also worth noting here that, so far, Omicron does not appear to be more likely to cause severe COVID-19 symptoms. Angelique Coetzee, chairwoman of the South African Medical Association, announced on Saturday that cases of the variant have been mild overall. Hospitals in South Africa are not (yet) facing a major burden from Omicron patients.
What can scientists do to better understand Omicron?
One thing I cannot overstate here is that scientists are learning about Omicron in real time, just as the rest of us are. Look at all the “We don’t know yet.”s in this thread from NYU epidemiologist Céline Gounder:
1/ FAQs I'm getting re: Omicron variant:
Q: Is Omicron more infectious than Delta? A: We don't know yet. Possibly. Or it could be "hitching a ride" with lax behavior or super spreading. pic.twitter.com/SWtUB8BjeQ
Gounder wrote that we may have answers to some pressing questions within two weeks, while others may take months of investigation. To examine the vaccines’ ability to protect against Omicron, scientists are doing antibody studies: essentially testing antibodies that were produced from past vaccination or infection to see how well they can fight off the variant.
At the same time, scientists are closely watching to see how fast the variant spreads in South Africa and in other countries. The variant’s performance in the U.K., where it was first identified on Saturday, may be a particularly useful source of information. This country is currently facing a Delta-induced COVID-19 wave (so we can see how well Omicron competes); and the U.K. has the world’s best genomic surveillance system, enabling epidemiologists to track the variant in detail.
How does Omicron impact vaccine effectiveness?
We don’t know this yet, as scientists are just starting to evaluate how well human antibodies from vaccination and past infection size up against the new variant. The scientists doing these antibody studies include those working at Pfizer, Moderna, and other major vaccine manufacturers. Pfizer’s partner BioNTech has said it expects to share lab data within two weeks, according to CNBC reporter Meg Tirrell:
What vaccine makers are saying about B.1.1.529:
-Moderna notes it's shown it can get into clinic (human trials) within 60 days; question is regulatory process from there. Manufacturing new doses could take a few months.
If BioNTech finds that Omicron is able to escape immunity from a Pfizer vaccination, the company will be able to update that vaccine within weeks. Moderna is similarly able to adjust its vaccine quickly, if lab studies show that an Omicron-specific vaccine is necessary.
Even if we need an updated vaccine for this variant, though, people who are already vaccinated are not going back to zero protection. As microbiologist Florian Krammer put it in a Twitter thread: “And even if a variant vaccine becomes necessary, we would not start from scratch… since it is likely that one ‘variant-booster’ would do the job. Our B-cells can be retrained to recognize both, the old version and the variant, and it doesn’t take much to do that.”
What can the U.S. do about Omicron?
On Friday, the Biden administration announced travel restrictions from South Africa and neighboring countries. The restrictions take effect on Monday, but virus and public health experts alike are already criticizing the move—suggesting that banning travel from Africa is unlikely to significantly slow Omicron’s spread, as the variant is very likely already spreading in the U.S. and plenty of other countries.
At the same time, travel restrictions stigmatize South Africa instead of thanking the country’s scientists for alerting the world to this variant. Such stigma may make other countries less likely to share similar variant news in the future, ultimately hurting the world’s ability to fight the pandemic.
What IS clear is that knee-jerk reactions like banning flights may be politically palatable, but will do little to slow the spread of this variant.
In the coming days more countries will identify cases. And there’s a good chance it’s already spreading here and in other places. https://t.co/YSbrSe0EdO
So what should the U.S. actually be doing? First of all, we need to step up our testing and genomic surveillance. As I mentioned above, Omicron can be identified from a PCR test; an uptick in PCR testing, especially as people return home from Thanksgiving travel, could help identify potential cases that are already here.
We also need to increase genomic surveillance, which could help identify Omicron as well as other variants that may emerge from Delta. In a post about the Delta AY.4.2 variant last month, I wrote that the U.S. is really not prepared to face surges driven by coronavirus mutation:
We’re doing more genomic sequencing than we were at the start of 2021, which helps with identifying potentially concerning variants, but sequencing still tends to be clustered in particular areas with high research budgets (NYC, Seattle, etc.). And even when our sequencing system picks up signals of a new variant, we do not have a clear playbook—or easily utilized resources—to act on the warning.
I’ll raise you one: BY THE TIME YOU DETECT ONE VARIANT ANOTHER IS ALREADY CIRCULATING UNDER THE RADAR SOMEWHERE SO WITH A MIX OF SURVEILLANCE LAGS, LOW VACCINE UPTAKE, INEQUITABLE VACCINE ACCESS WE ARE WILL BE CHASING VARIANTS ENDLESSLY.
We also need to get more people vaccinated, in the U.S. and—more importantly—in the low-income nations where the majority of people remain unprotected. In South Africa, under one-quarter of the population is fully vaccinated, according to Our World in Data.
What can I do to protect myself, my family, and my community?
Also: Wear a mask in indoor spaces, ideally a good quality mask (N95, KN95, or double up on surgical and cloth masks). Avoid crowds if you’re able to do so. Monitor yourself for COVID-19 symptoms, including those that are less common. Utilize tests, including PCR and rapid tests—especially if you’re traveling, or if you work in a crowded in-person setting.
I’ve seen some questions on social media about whether people should consider canceling holiday plans, or other travel plans, because of Omicron. This is a very personal choice, I think, and I’m no medical expert, but I will offer a few thoughts.
As I said in the title of this post, we don’t yet know enough about this variant for it to be worth seriously panicking over. All of the evidence—based on every single other variant of concern that has emerged—suggests that the vaccines will continue to work well against this variant, at least protecting against severe disease. And all of the other precautions that work well against other variants will work against this one, too.
So, if you are vaccinated and capable of taking all the other standard COVID-19 precautions, Omicron is most likely not a huge risk to your personal safety right now. But keep an eye on the case numbers in your community, and on what we learn about this variant in the weeks to come.
If you’re worried about your risk from omicron, get vaccinated if you aren’t already. Continue to layer other precautions. And more than anything, follow the science and advocate for collaborative global health. Travel bans won’t do shit. Vaccines and global health equity WILL.
What does Omicron mean for the pandemic’s trajectory?
This variant could potentially lead to an adjustment in our vaccines, as well as to new surges in the U.S. and other parts of the world. It’s too early to say how likely either scenario may be; we’ll learn a lot more in the next couple of weeks.
But one thing we can say right now, for sure, is that this variant provides a tangible argument for global vaccine equity. If the country where Omicron originated had a vaccination rate as high as that of the U.S. and other high-income nations, it may not have gained enough purchase to spread—into South Africa, and on the global path that it’s now taking.
💉 7.8 billion COVID vaccine doses have been administered
👥 53% of world population with at least 1 dose
🌍 Total doses per 100 people High-income countries: 147 Upper-middle income: 146 Lower-middle income: 68 Low income: 7
If we had ensured that everyone had equal access to vaccination and really pushed the agenda on getting global vaccination to a high level, then maybe we could have possibly delayed the emergence of new variants, such as the ones that we’re witnessing.
I will end the post with this tweet from Amy Maxmen, global health reporter at Nature. The Omicron variant was a choice.
“Instead of solving the problem by vaccinating the world & cutting off new variants, rich countries seem prepared to fork over more money for boosters, & live in a state of endless fear,” Achal Prabhala told me back in JULY. https://t.co/Z1trCXN9Dp