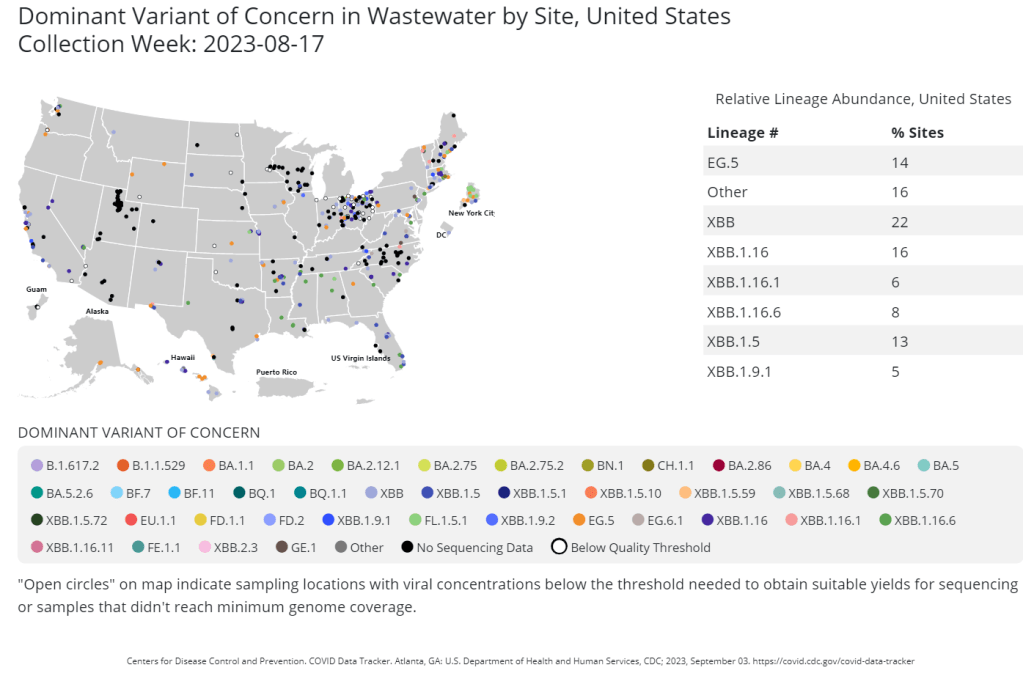
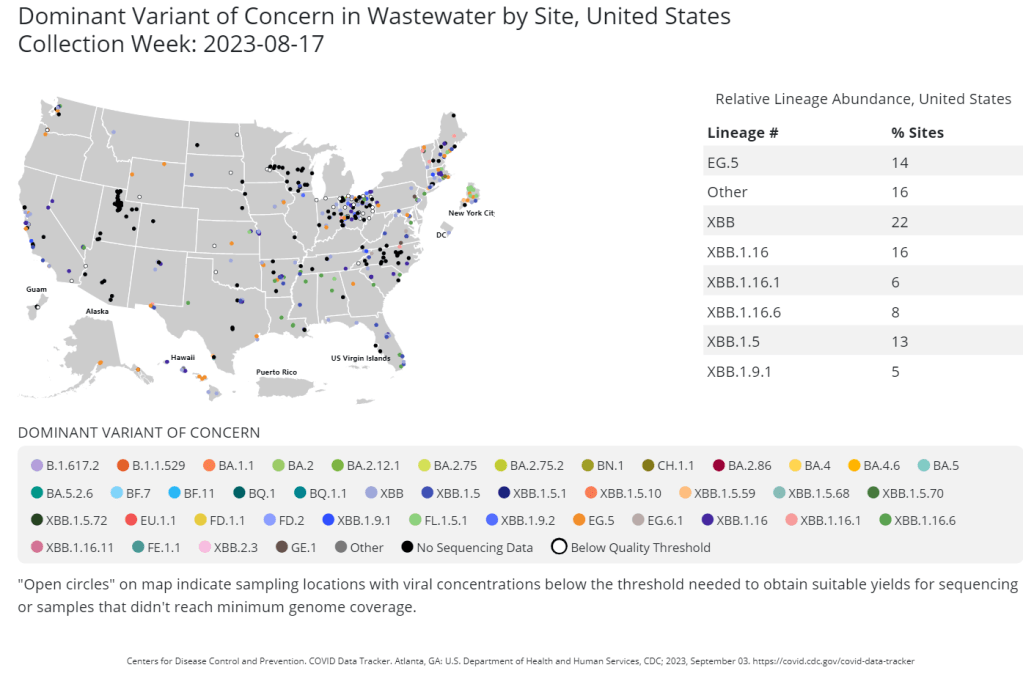
The CDC publishes data from about 400 wastewater testing sites that are sequencing their samples. Chart shows data from the week of August 17.
This week, the health department in New York City, where I live, announced that they’d identified new variant BA.2.86 in the city’s wastewater. (For more details about BA.2.86, see last week’s Q&A post.)
I covered the news for local outlet Gothamist/WNYC, and the story got me thinking about how important wastewater surveillance has become for tracking variants. With less clinical testing, sewage is now a crucial source for understanding how the coronavirus is mutating and what impacts those mutations have. But there are continued barriers to obtaining and interpreting wastewater data.
Quoting from the story:
The declaration of the end of the public health emergency in May made COVID-19 tests less available in health care settings, and sewage monitoring has since emerged as an important way to identify new variants.
“As the wastewater testing has gotten better, the patient surveillance has decreased,” [said Marc Johnson, a virologist at the University of Missouri]. Several variants have been found in sewage before cases were confirmed, he said.
Wastewater surveillance has some distinct advantages, when it comes to variant monitoring:
It covers thousands of people—the entire population of a sewershed—with one sample. In big cities like NYC, one sample can include data from more than one million residents.
Through sewage samples, scientists can look for multiple variants at once, rather than compiling data over many PCR test results. They can also track population-level trends over time.
Unlike traditional case data, wastewater data don’t rely on how many people are getting tested or where. This lack of testing bias is important, as people typically use rapid tests—which are not reported to health systems—over PCR these days (rapid tests are easier to access, PCR sites have closed following the end of the federal public health emergency, etc.).
But there are also some problems, as the NYC detection this week demonstrated:
Public health officials are still getting used to using and sharing wastewater data, as this is a relatively novel source with novel pipelines for transmitting data. While the CDC and other organizations are working to compile these data in a standardized way, it’s still a work in progress.
Discrepancies and delays can sometimes occur as a result. For example, in New York, the governor’s office put out a press release on Tuesday morning claiming that BA.2.86 hadn’t been detected in the state yet—then, just hours later, the city health department announced they’d found it. State health officials weren’t aware of the detection before the city made its public announcement, I learned for my news story.
Health officials are also still learning how to interpret and act on wastewater data. The NYC health department failed to answer my questions about in which sewershed or from which sampling date they found BA.2.86; it’s unclear if they’re using the detection to take any specific actions, besides simply warning the public that this variant is present.
As wastewater surveillance captures such broad samples, it’s difficult to tie new variant detections to clinical data, such as whether an infected person went to the hospital due to their symptoms. Officials can’t contact trace from these detections, making it hard to answer questions like whether BA.2.86 causes more severe symptoms.
In the past week (May 28 through June 3), the U.S. reported about 7,200 new COVID-19 patients admitted to hospitals, according to the CDC. This amounts to:
An average of 1,000 new admissions each day
2.2 total admissions for every 100,000 Americans
6% fewer new admissions than last week (May 21-27)
Additionally, the U.S. reported:
4.2% of tests in the CDC’s surveillance network came back positive (an 8% decrease from last week)
40% of new cases are caused by Omicron XBB.1.5; 26% by XBB.1.16; 21% by XBB.1.9 (as of June 10)
(Biobot update delayed)
Nationally, the COVID-19 situation in the U.S. is similar to where we’ve been for the last few weeks. Major metrics (such as we have them) show an overall plateau in disease spread. Wastewater trends in a few places suggest a summer surge might be coming, but it’s hard to say for sure.
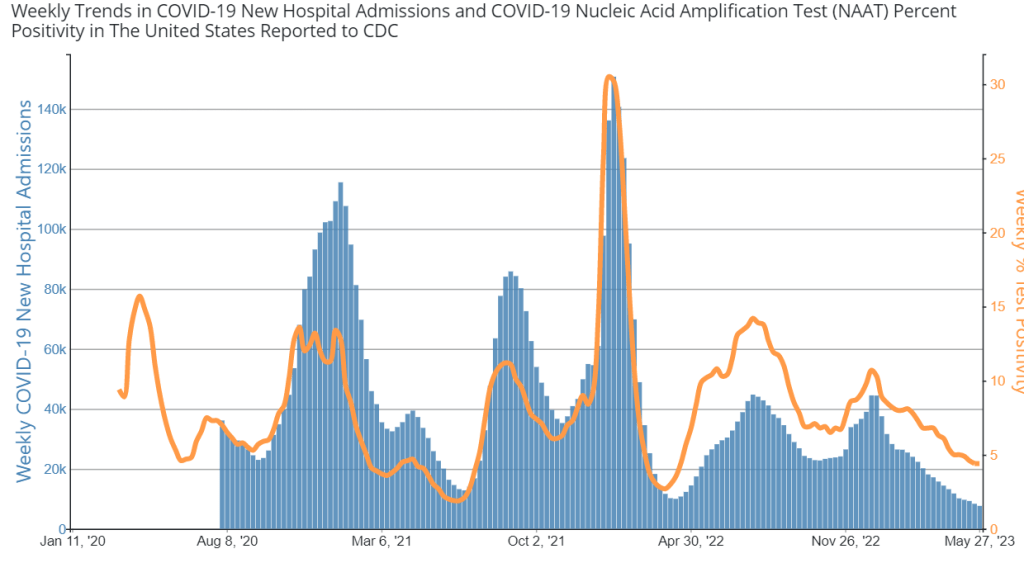
Hospital admissions and test positivity (from the specific network of labs reporting to the CDC) are trending slightly down at the national level. But there are still about 1,000 people being hospitalized with COVID-19 every day.
Biobot Analytics, my usual go-to source for wastewater surveillance data, did not update their dashboard this week due to a tech issue. The company’s most recent data, as of May 29, show plateaus in all four major regions.
The CDC’s National Wastewater Surveillance System (NWSS) shows a similar picture. Among about 1,100 sewage testing sites that recently reported to the CDC, 60% reported decreases in coronavirus levels in the last two weeks while 40% reported increases.
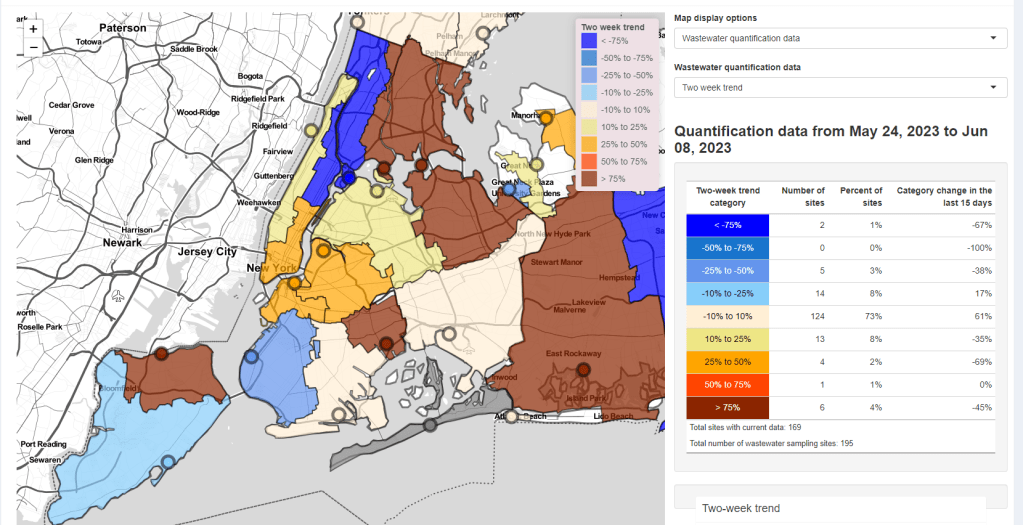
New York City is one of the places seeing wastewater increases, as I noted last week. Patterns differ somewhat across the city’s fourteen sewersheds, with some reporting more than 1000% increases in wastewater levels in recent weeks while others are still in plateaus.
Both the New York/New Jersey and New England regions are reporting slight upticks in their test positivity, according to the CDC’s surveillance network. This (along with the trends in NYC’s sewage) could be a precursor of more COVID-19 spread this summer, but it’s currently hard to say for sure.
The CDC updated its variant estimates (now reported every other week) this past Friday. XBB.1.5 is still the most common lineage, causing an estimated 40% of cases, the CDC reports. XBB.1.16 and XBB.1.9 continue to outcompete it, causing about 26% and 21% of cases respectively.
These newer lineages have yet to contribute to a significant shift in transmission, from what I can tell. We have yet to see if past immunity in the U.S. can hold off against the ever-evolving Omicron variants this summer.
Both hospital admissions and test positivity for COVID-19 have ticked down in recent weeks. Chart via the CDC.
In the past week (May 21 through 27), the U.S. reported about 7,600 new COVID-19 patients admitted to hospitals, according to the CDC. This amounts to:
An average of 1,100 new admissions each day
2.3 total admissions for every 100,000 Americans
8% fewer new admissions than last week (May 14-20)
Additionally, the U.S. reported:
4.4% of tests in the CDC’s surveillance network came back positive (a 0% change from last week)
A 17% lower concentration of SARS-CoV-2 in wastewater than last week (as of May 31, per Biobot’s dashboard)
54% of new cases are caused by Omicron XBB.1.5; 19% by XBB.1.16; 18% by XBB.1.9 (as of May 27)
The COVID-19 plateau of the last few weeks continues at the national level, though experts are concerned that a summer surge could occur in parts of the country. Wastewater surveillance and testing data are indicating potential increases in the New York City region.
Hospital admissions for COVID-19 remain at the levels we’ve seen throughout the spring, with about 1,100 people admitted nationwide each day last week. These numbers are similar to the hospitalizations reported at previous low points for COVID-19, in spring 2022 and 2021.
Testing data from the CDC’s National Respiratory and Enteric Virus Surveillance System (NREVSS) also suggest a plateau: national test positivity didn’t change from last week to this week. While this CDC system includes a small fraction of the PCR labs that reported COVID-19 tests before the federal emergency ended, it’s still a helpful indicator for testing trends.
Wastewater surveillance data from Biobot shows a similar picture, with coronavirus levels in sewage remaining consistent at the national level for the last two months. All four major regions of the country are trending down, according to Biobot’s analysis.
But national data can hide more concerning trends at the local level. Wastewater data from New York City’s fourteen water treatment plants suggest potential increases in COVID-19 spread in the city and outlying suburbs over the last couple of weeks. The city’s wastewater data are reported with a delay (as of today, the most recent update was May 21), so I find it worrying that an increase may have predated the Memorial Day holiday. Test positivity data for the New York/New Jersey region suggest an uptick as well.
NYC has been a bellwether for the rest of the U.S. at many points during the pandemic, and it’s possible that the city could see a surge before other regions again this summer. Health experts are also closely watching the South, where people gather indoors more in the summer.
About 96% of Americans over age 16 have some COVID-19 protection from vaccination, past infections, or both, according to a recent CDC study. This protection will help many people avoid severe COVID-19 symptoms this summer even if they get infected. But Long COVID continues to be a risk—potentially even escalating with more infections.
Political leaders in New York State recently ended a policy requiring masks in healthcare settings. This is obviously a big issue for high-risk New Yorkers, many of whom have spoken out on social media about wanting to attend important doctors’ appointments without risking COVID-19.
In response to the change, local advocacy organization Mandate Masks NY has compiled a list of hospitals and healthcare centers in New York that are still maintaining mask requirements independently of the state policy. You can find the list here; and the organization has compiled several other lists of businesses requiring masks, available on their website.
As a former COVID Tracking Project volunteer, I’m always glad to see volunteer efforts producing important databases that wouldn’t otherwise be available. Also: it looks like the Mandate Masks NY Twitter account was suspended this weekend—if you know anything about that, please reach out!
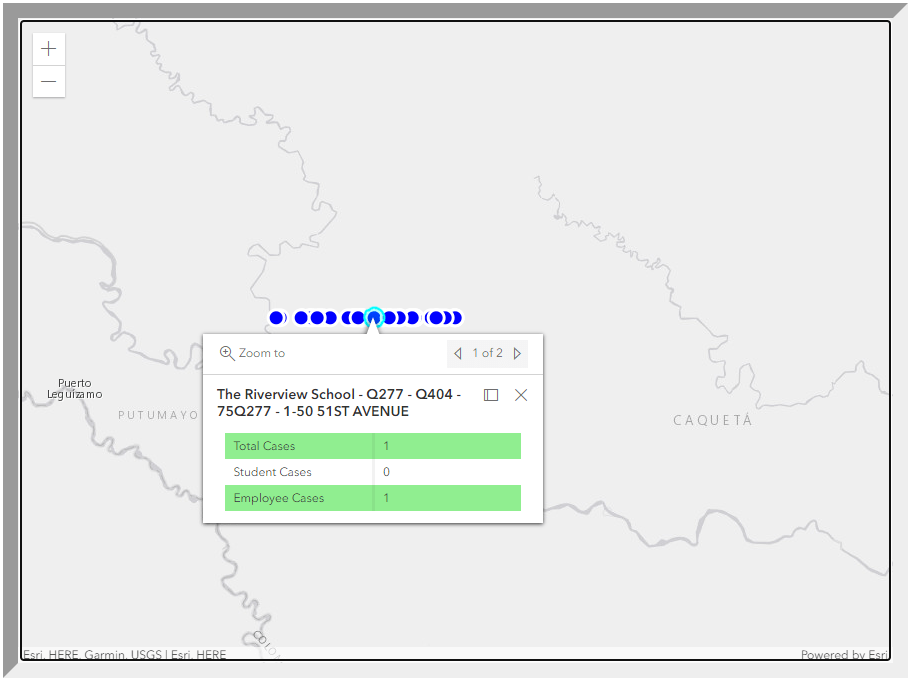
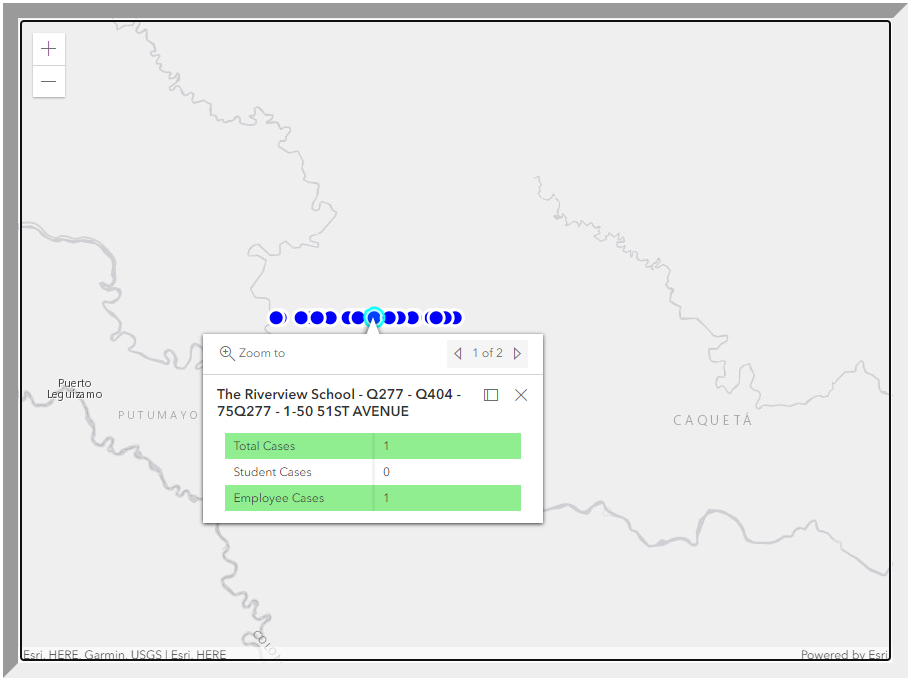
The error appears to be a problem with the dashboard’s geographical tagging, putting these schools in another continent instead of their correct NYC neighborhoods. But it’s a pretty big issue for parents and school staff who might be checking the map, looking for COVID-19 cases at their schools.
If these users didn’t know to zoom out and then scroll down a fair amount—which they probably wouldn’t, unless they got very creative or followed the right people on Twitter—they would think there were no cases. Which is far from the truth.
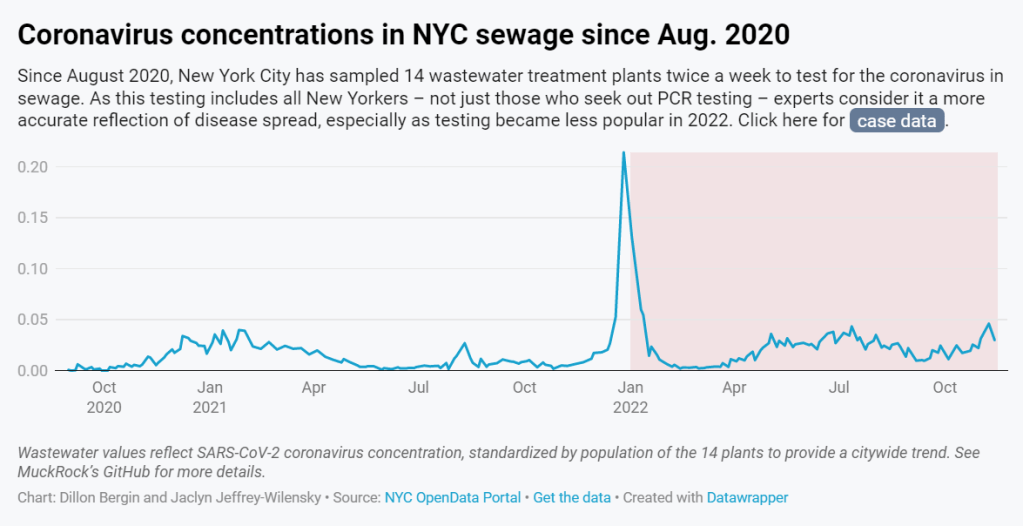
In 2022, wastewater data in NYC have more accurately reflected COVID-19 spread in the city than case data. See the full story (on MuckRock or Gothamist) for the interactive chart; links are below.
My second big story this week is a detailed report about New York City’s wastewater surveillance program, highlighting its lack of transparency. You can read the story on Gothamist and/or on MuckRock. I’m particularly excited to share this one with NYC-based readers, as it uncovers a public program that’s been running under our feet for nearly three years.
Longtime readers might remember that, back in April, I noticed that NYC wastewater data had disappeared from the CDC’s national dashboard. And the city’s data stayed unavailable even when other locations (which were similarly interrupted by the CDC’s switch between wastewater contractors) resumed reporting to the dashboard.
That observation piqued my curiosity about how, exactly, NYC agencies are testing our wastewater—and what they’re doing with the data. So, I started investigating, with the support of MuckRock and Gothamist/WNYC. My project eventually revealed the answers to my questions: while NYC has set up an impressive, novel program to test all 14 city wastewater treatment plants for COVID-19, the health department doesn’t appear to be taking advantage of these results.
In a joint statement, NYC’s health and environmental protection agencies said that they still see wastewater surveillance as a “developing field” and are skeptical about its utility for public health. Even though NYC’s program has been running since early 2020 and cost over $1 million. And even though other wastewater programs across the U.S. and internationally have demonstrated the potential of this type of data.
Here are the story’s main findings, as drafted for MuckRock’s version of the article:
New York City’s Department of Environmental Protection created a brand-new program to test city wastewater for COVID-19 in 2020, working with limited lab equipment and personnel to sample from 14 sewage treatment plants across the city. In doing so, the city brushed off assistance offered from “multitudes of academics” and private sector researchers, and set up its program in-house. It has cost more than $1 million over the past three years.
But the city didn’t publicly post any wastewater data until January 2022, almost two years after testing started. Unlike other large cities, such as Boston, New York City lacks a public dashboard for wastewater data. The city’s data available on dashboards run by the Centers for Disease Control and Prevention and New York State are often delayed by a week or more, making it less useful for New Yorkers seeking advanced warning about potential new surges.
In other parts of the U.S. — and at Columbia University in uptown Manhattan — wastewater surveillance is used for public health strategies, such as encouraging people to get PCR tests or sending extra resources to hospitals before a surge. However, New York City’s health and environmental agencies say they still consider wastewater research a “developing field” and aren’t using it for policy decisions.
In response to our questions, city health and environment agency officials argued that wastewater results “do not generally provide a complete picture” of how COVID-19 is spreading and said, unlike in other parts of the country, trends in city wastewater data tend to align with case counts rather than predicting them. But wastewater has shown a higher level of COVID-19 spread than PCR testing, as the latter became less available in 2022, according to Gothamist and MuckRock analyses. This pattern suggests that the sewage numbers may more accurately reflect actual disease patterns.
A bill introduced to the New York City Council in August would make the wastewater surveillance program permanent, expand it to other public health threats as needed, and require the health department to report data on a public dashboard.
For readers outside NYC, I think this story provides an informative case study of the hurdles that wastewater surveillance for COVID-19 (and other diseases) will need to clear.
First, you have the resource challenges. If the NYC Department of Environmental Protection, which oversees the largest municipal water network in the country, had a hard time getting equipment and personnel for testing—imagine the challenges facing small, rural public health departments.
Next, after testing is set up, you have to interpret the data. NYC’s health department seems to be somewhat stuck on this step, with no public dashboard and its insistence that city residents should look at clinical case data—which we know are a significant undercount of true infections—rather than wastewater data. To be fair, wastewater data are new terrain for public health experts, with a lot of analytical issues. (See my MuckRock/FiveThirtyEight story from the spring for more details on this.)
And finally, you have to communicate the data. How do you share wastewater results with the public in a way that is clear, real-time, local—and acknowledging necessary caveats? This is a tough challenge that health agencies across the U.S. are just starting to tackle, in tandem with the private companies that work on wastewater analysis.
As I said in the radio story accompanying my piece, I hope that, someday, we can get wastewater surveillance updates as easily and regularly as we get weather updates. That future feels a long way off right now, but I intend to keep reporting on the journey in 2023.
If you live somewhere with a thriving (or faltering) wastewater surveillance program, reach out and tell me about it!
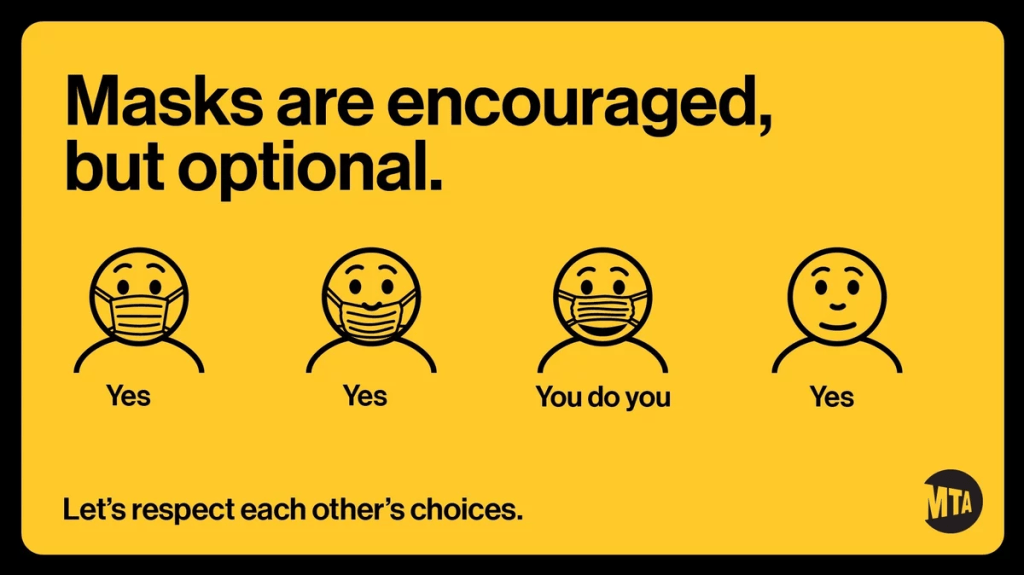
The COVID-19 Data Dispatch does not endorse the new MTA mask guidance.
Anyone who regularly rides the New York City subway knows that the city’s mask requirement for public transportation has been unenforced and loosely followed—especially in the months following last winter’s Omicron surge.
But last week, even the requirement itself was struck down. New York Governor Kathy Hochul (who oversees the Metropolitan Transportation Authority, as it’s a state-controlled agency) announced that masks are now optional on trains and buses. And she introduced the policy with a new version of the MTA’s masking graphic that felt like a slap in the face to higher-risk New Yorkers who now feel unsafe using the transit system.
NPR has a good article explaining why health experts have criticized the new graphic. Personally, I think it discourages people from thinking about how their COVID-19 safety choices impact a broader community—something that’s especially important in a dense, diverse city like NYC. Telling New Yorkers, “You do you,” when “doing you” could mean posing an immense risk to your neighbors, is a dangerous message.
The one silver lining here is, I’ve seen a few excellent posters parodying the MTA’s new mask graphic. Here’s one of my favorites:
This is not a direct COVID-19 callout, but I wanted to acknowledge that many of the public health failures we saw early in the COVID-19 crisis are now being repeated with monkeypox—which the WHO just declared a global health emergency.
One major issue is a shortage of tests, leading public health experts to suggest that the true number of cases is much higher than what’s been reported. Also, while vaccines are available for monkeypox, the rollout has been inaccessible and inequitable, with very limited appointments in hotspots like NYC. ACT UP actually held a protest in the city last week to criticize local and federal officials for these issues.
According to BuzzFeed News coverage of the ACT UP protest, their demands included: “an ‘emergency safety net fund’ for those testing positive, increased access to vaccines, language-inclusive educational resources, and adequate staffing for both vaccination sites and quarantine locations.” All of which sounds familiar!
New CDC report on drug overdose deaths during the pandemic: Drug overdose deaths increased by 30% from 2019 to 2020, according to a new CDC report compiling data from 25 states and D.C. But this increase was higher for Black and Native Americans: deaths among these groups increased by 44% and 39%, respectively. The full report includes more details on how overdose deaths disproportionately occurred in Black and Native populations, as well as the need for more easily accessible treatments for substance abuse.
CDC survey of public health workers: Another CDC report that caught my attention this week presented results from a national survey of state and local public health workers in 2021. Almost three in four of the workers surveyed were involved with COVID-19 response last year. The survey provides further evidence of burnout among public health workers: 40% of those surveyed reported that they intend to leave their jobs within the next five years.
COVID-19 testing options: COVID-19 Testing Commons is a research group at Arizona State University’s College of Health Solutions that has compiled comprehensive information about COVID-19 tests available worldwide. You can search the database for tests by company, platform, type of specimen collected, regulatory status, and more. The group also recently compiled a report summarizing these testing options in the pandemic to date.
Congressional hearing on Long COVID: This week, Congress’s Select Subcommittee on the Coronavirus Crisis held a hearing specifically about Long COVID. Congressmembers heard from Long COVID patient advocates and researchers about the impacts of this condition and the urgent need for more research and support. I highly recommend reading or listening to the testimony of Hannah Davis, cofounder of the Patient-Led Research Collaborative, for a powerful summary of these impacts and needs. (If you’re watching the video: her testimony starts at about 28:50.)
CDC recommends Novavax vaccine: The CDC has officially authorized Novavax’s COVID-19 vaccine, following the FDA authorization that I mentioned in last week’s issue. Novavax’s vaccine is protein-based, which is an older type of vaccine but has been less common for COVID-19; some experts are hopeful that people who have hesitated with the mRNA vaccines may be more likely to get Novavax. Dr. Katelyn Jetelina has a helpful summary of this vaccine’s potential impact at Your Local Epidemiologist.
NYC prevalence preprint updated: I’ve linked a couple of times to this study from a group at the City University of New York, with the striking finding that an estimated one in five New Yorkers got COVID-19 during a two-week period in the BA.2/BA.2.12.1 surge. The researchers recently revised and updated their study, based on some feedback from the scientific community. Their primary conclusions are unchanged, lead author Denis Nash wrote in a Twitter thread, but the updated study includes some context about population immunity and NYC surveillance.
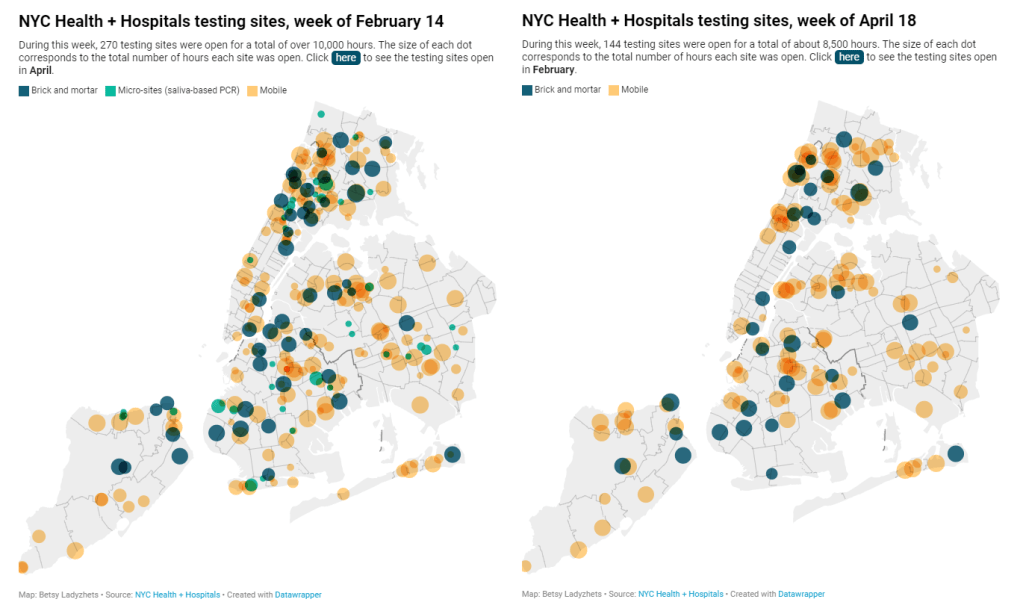
New York City has been closing PCR testing sites, even as the city faced a major Omicron resurgence this spring. This was the main finding from a story I wrote for Gothamist and WNYC (New York Public Radio), based on my analysis of public information on city-run testing sites.
While this was a local story, I think the trends I found—and the pushback that the piece received from city health officials—are pretty indicative of the national state of COVID-19 testing right now. Since the federal government ran out of funding to cover testing for Americans without health insurance in late March, private testing companies have started requiring insurance information and, in many cases, raising their prices.
At the same time, state and local health departments have closed their public PCR testing sites and directed people to use at-home rapid tests instead. New York City still has more accessible testing than most of the country, but my story showed how even here, getting tested is becoming more difficult—and less popular.
NYC has faced a major COVID-19 surge this spring — yet the city closed public testing sites and made it harder to get PCR results.
— betsy ladyzhets 📊 (@betsyladyzhets) July 5, 2022
Here are a few key statistics from the piece:
The number of public PCR testing sites run by NYC Health + Hospitals was cut in half between mid-February and mid-April.
The total hours that public testing sites were open decreased from over 10,000 during a week in February, to 8,500 during a week in April, to 7,500 in the last week of June.
Manhattan testing hours remained relatively constant (about 1,500 in each of the weeks I analyzed), while hours were cut in other boroughs.
The numbers of New Yorkers getting tested on a daily basis were similar in June 2021 and June 2022—even though reported case rates were about ten times higher this year.
New York City’s test positivity rate recently shot above 10%, and is now over 15%. It was closer to 1% at this time last year.
The NYC health department had some issues with my story. In fact, city health commissioner Dr. Ashwin Vasan posted a Twitter thread stating that it was “missing key information” and that the city actually has “more testing resources than ever.” But the “testing resources” he cites here are mostly at-home tests; PCR testing in NYC is both less accessible and less popular. A follow-up story that I coauthored with Nsikan Akpan, my editor at Gothamist/WNYC, further explains the situation in the city.
The decline in PCR testing is making it harder to understand where and how fast the coronavirus is spreading, both in the city and around the U.S. To explain the implications of this trend, here’s a short FAQ on how to think about testing during our current surge.
Why is PCR testing still important for individuals?
One of the city officials’ main responses to my story was that NYC has made it easy for people to get free at-home rapid tests, in place of PCR testing. The city has distributed more than 35 million at-home tests at hundreds of libraries and other community sites.
At-home tests certainly have advantages: they’re more convenient, with results back in 15 minutes. Turnaround times for PCR tests are generally pretty fast right now thanks to limited demand (usually under 48 hours, if not under 24 hours, in NYC), but that’s still a long wait compared to a rapid test. Rapid, at-home tests also provide a better indicator of contagiousness.
Still, PCR tests have continued utility because they remain the gold standard of accuracy: they’re able to identify a COVID-19 case with much smaller amounts of coronavirus present in someone’s respiratory tract than a rapid test. As a result, if you were recently exposed or are showing some mild symptoms—but testing negative on rapid tests—a PCR test could be valuable to provide a more reliable COVID-19 status.
PCR tests can also be helpful for documenting a COVID-19 case. While many doctors will take a rapid test positive as a clear indicator of an infection, some settings may require a PCR test—in which results are verified by the lab that processes the test. This can be particularly true for Long COVID clinics, health advocate JD Davids told me. So, if you tested positive on a rapid test but are concerned about Long COVID symptoms, a PCR test may be a helpful verification step.
Why is PCR testing still important for communities?
Rapid, at-home test results generally do not travel further than your trashcan, or maybe your phone camera. They don’t get reported to testing companies, or local public health departments, or the CDC—unlike PCR tests, which have established data pipelines for such reporting. Some jurisdictions do have options for residents to self-report rapid test results, but this self-reporting is generally a small fraction of the total tests conducted.
As a result, public health experts generally rely upon PCR testing data to understand patterns in COVID-19 spread. When less PCR testing takes place, these patterns become more difficult to interpret. For example, in the U.S. as a whole, around 100,000 new cases a day have been reported for the last several weeks; but we know that the true trend would likely be a lot more variable if we had data from rapid tests.
Also, as Brown University epidemiologist Dr. Jennifer Nuzzo pointed out when my editor Nsikan interviewed her for our follow-up story, PCR tests are necessary for tracking variants. A selection of PCR test samples get genetically sequenced; this doesn’t happen for rapid tests.
“It’s really important for us to stay ahead of what variants are circulating in our communities,” Nuzzo said, citing what society has already learned about different variants to date. “Some are more transmissible. Some have been more severe. We need to stay ahead of the virus, so that we can know when and how and if to change our strategy about how to control it.”
What’s the value of abundant local testing sites?
If PCR testing is less popular in this current phase of the pandemic, you might ask, why not just have a few central testing hubs in a place like NYC, and maintain testing capacity in a more efficient way? This seems to be the city’s response, to some extent: officials explained that some brick-and-mortar testing sites (mostly at NYC hospitals) are staying open, while the city’s fleet of mobile testing vans can move around as needed.
But for a lot of people, traveling outside their neighborhood to get a test or tracking down the right mobile van can be a major barrier to getting tested. This is especially true for essential workers and low-income New Yorkers—who are the people most in need of testing. Maintaining public testing throughout the city is a health equity issue.
And even if the testing capacity is technically maintained, location is important. Consider a region like South Brooklyn: Four brick-and-mortar testing sites scheduled to close in mid-July are all located in this area: 4002 Fort Hamilton, Bay Ridge, Bensonhurst and Midwood Pre-K.
It’s unclear whether mobile sites will move to South Brooklyn in response. Shrier said each closing site has “dedicated at-home test distribution sites” within one mile. But residents of Bay Ridge, Bensonhurst and other nearby neighborhoods may need to travel further to get a PCR test — or face high costs at private sites.
What data sources could replace information from PCR tests?
Dr. Denis Nash, an epidemiologist at the City University of New York whom I interviewed for the first NYC story, talked about two types of data that may be collected by a health agency tracking disease spread.
“There’s active surveillance and passive surveillance,” he said. “In active surveillance, the health department staff are actively going out and trying to ascertain how many cases there might be. They’re going to hospitals and to homes, looking for cases. And when you do that, you’re more likely to exhaustively find a high proportion of cases.” One example of active surveillance: a survey conducted by Nash and his team at CUNY in April and May, which indicated about 20% of New Yorkers may have had COVID-19 within a two-week period.
Meanwhile, passive surveillance “relies on healthcare providers and laboratories to voluntarily report their tests and cases to the health department,” Nash said. NYC and other health departments which receive much of their COVID-19 data—PCR test results, hospital admissions, etc.—from healthcare providers are exemplifying this passive approach.
As COVID-19 becomes less of a public concern and testing is less popular, health agencies should step up their active surveillance, Nash said. Wastewater can be another source of data that’s more active than PCR test results, since it reflects COVID-19 spread across a large population. (Unfortunately, in NYC, wastewater data is pretty inaccessible; that’s a topic for another time.)
What’s the best way to use at-home rapid tests?
Rapid test use can fall into three different categories. First, if you are trying to determine whether you’re actively contagious right before a gathering or seeing a high-risk person: take one test, as close in time to the event as possible. (For example, if I’m going to a large march in NYC, I plan to test myself a few minutes before heading to the subway.)
Second, if you had a recent COVID-19 exposure (or attended a high-risk event), test multiple times in succession—ideally at least twice in 48 hours. This testing process should start a couple of days after the exposure, because rapid tests aren’t accurate enough to pick up the infection right away. You could also use a single PCR test to serve the same purpose as multiple rapid tests.
And third, if you are isolating after a positive COVID-19 test, rapid tests can help identify when you’re no longer contagious and able to return to society. As I wrote in an earlier post, the CDC’s five-day isolation guidance is not actually backed up by data; testing out of isolation is much safer.
As always, if you have questions about testing or any other COVID-19 topic, my inbox is open.