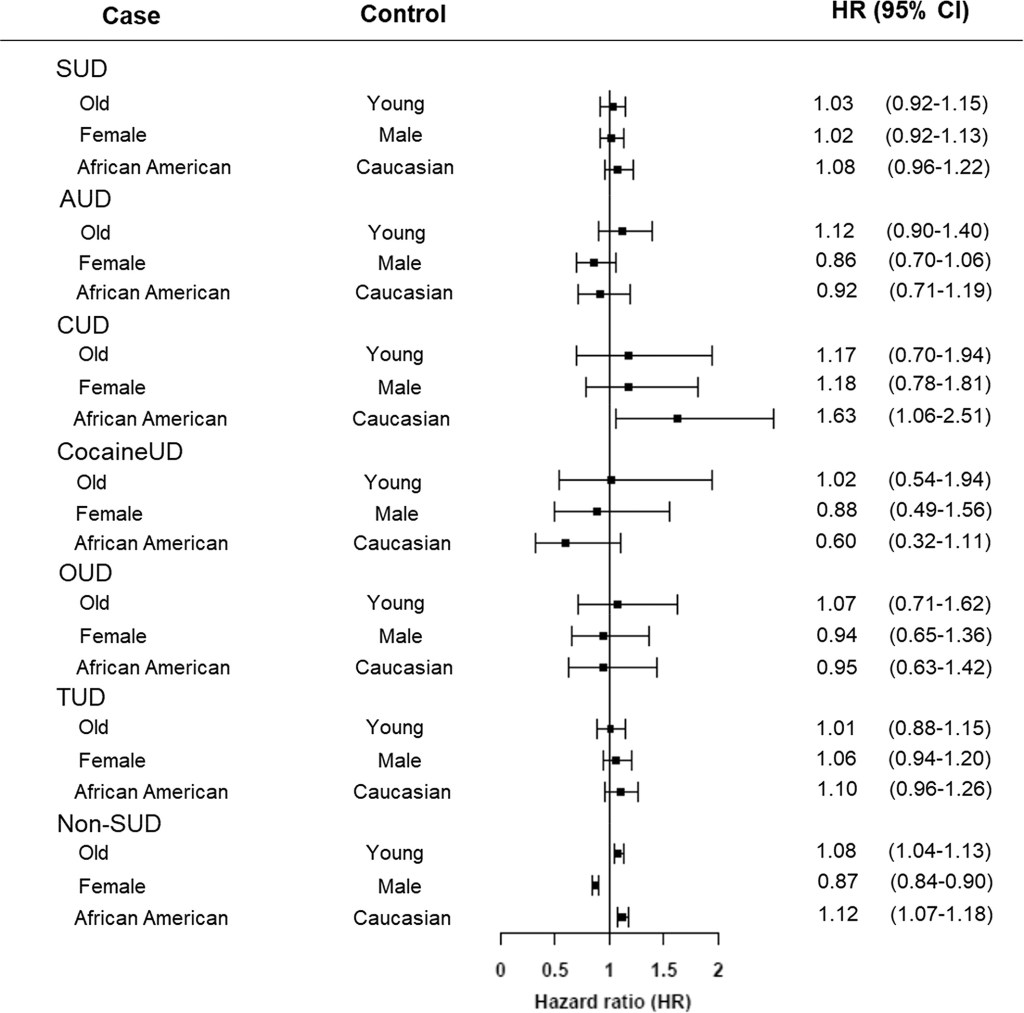
Adults with substance use disorders have an increased risk of breakthrough cases, according to a new study published this week in the journal World Psychiatry. Though the chances of a COVID-19 case after vaccination were very low in this group, these patients’ odds of a breakthrough case were about twice as high as the odds for adults without substance use disorders, researchers from the National Institutes of Health (NIH) found.
This study is the first I’ve seen to delineate breakthrough case risk in a specific, vulnerable population—besides studies demonstrating higher risk for older adults. As I wrote two weeks ago, a lack of specific data on breakthrough cases has contributed to confusion and debate surrounding who should be eligible for a booster shot in the U.S.
So, how did these NIH researchers determine the risk for people with substance abuse? They used anonymous, electronic health records from 63 healthcare organizations across the U.S., compiled in the TriNetX Analytics platform. The study included health records from about 30,000 patients with substance use disorders, compared with 550,000 patients without these disorders. From this large pool of anonymous data, the researchers were able to determine breakthrough case risk among different patient demographics, different substance use disorders, and more.
I got a chance to talk to Dr. Nora Volkow, director of the NIH’s National Institute on Drug Abuse and one of the study’s lead authors, about this methodology, as I covered the paper for DailyMail.com. I asked her if she expected to see similar studies examining breakthrough case risk for other health risks and occupations.
“Absolutely,” Dr. Volkow said. She told me she’s already seen other papers comparing the risk of a breakthrough with Delta compared to other variants, and that more research looking at specific patient groups may be ongoing. Still, using electronic health records has its drawbacks.
“We are basically basing [the analysis] on the electronic health records,” she said. “But it could be useful to complement this with studies that actually are genotyping, getting information about, what was the virus that is responsible?” In other words: health records from hospitals and clinics typically are not matched with genetic sequencing information, making it difficult to link specific variants with breakthrough case risk.
As for why patients struggling with substance abuse have a higher risk of breakthrough COVID-19: Dr. Volkow said this is largely due to socioeconomic factors, such as lack of access to healthcare, low income, and homelessness. Drugs and alcohol are also capable of weakening patients’ immune systems, though; marijuana in particular can hinder immune system regulation.
Last week, one of the reader questions I answered addressed Long COVID, the condition in which people have COVID-related symptoms for weeks or months after their initial coronavirus infection. One reader had asked about monitoring for Long COVID patients (also called long-haulers); I later received another question about the risks of Long COVID after vaccination.
These questions made me realize that I’ve devoted very little space to Long COVID in the COVID-19 Data Dispatch—even though I consider it one of the biggest COVID-19 data gaps in the U.S. Though it’s now been well over a year since the first Long COVID patients were infected, there is still so much we don’t know about the condition.
For example, we don’t know a very rudimentary number: how many people in the U.S. are struggling with Long COVID. We also don’t have a clear, detailed picture of Long COVID symptoms, or how these symptoms arise from a coronavirus infection, or how they impact the daily lives of Long COVID patients.
Why does this massive data gap exist? Long COVID studies are challenged by the lack of standardized patient data in the U.S., making it difficult to identify symptom patterns across large groups of people. We face a similar problem in tracking breakthrough cases, demographic information, and other COVID-19 trends.
Plus, thanks to limited COVID-19 testing in the U.S. throughout the pandemic (and restrictions on who could get tested, back in spring 2020), a lot of Long COVID patients never had a positive test result—making it difficult for them to get a formal diagnosis. And many of the Long COVID studies that have been conducted focus on patients who had a positive COVID-19 test or were hospitalized for the disease, thus narrowing much of our clinical data to a small subset of the actual Long COVID population.
As I noted last week, the National Institutes of Health (NIH) has set up a major research initiative to study Long COVID. This initiative, called RECOVER, is poised to become our best source for Long COVID data in the future. But it’s in early stages right now, beginning to distribute funding to different research groups and recruit Long COVID patients for study. It could be years before we get results.
All of that said, there are still a few things we know about Long COVID based on research thus far. Here’s a roundup of twelve key statistics.
Between 10% and 30% of coronavirus infections lead to Long COVID. This statistic comes from the NIH’s RECOVER Initiative website; it summarizes findings from past studies. Consider: 30% of the 44.2 million Americans with a documented COVID-19 case amounts to 13.3 million people with Long COVID. Even 10% of those 44.2 million would amount to 4.4 million people.
Some studies suggest that as many as one-third of COVID-19 patients may have persistent or returning symptoms. A recent study of electronic health records in the U.S. and U.K., run by scientists at the University of Oxford, suggests that the true share of COVID-19 patients who contract Long COVID is on the higher end of that 10%-30% estimate that the NIH provides. This new study found that 36% of COVID-19 patients (among a sample size of 270,000) had symptoms three and six months after their diagnosis.
Long COVID may manifest with over 100 different potential symptoms. There is a Long COVID paper that I personally come back to, whenever I want to see a clear picture of the many ways that this condition can impact patients. The paper, published in The Lancet in July, reports results from a survey of over 3,000 Long COVID patients conducted by the Patient-Led Research Collaborative. According to this survey, Long COVID patients may suffer from about 100 possible symptoms, including systemic, reproductive, cardiovascular, musculoskeletal, immunologic/autoimmune, head/eyes/ears/nose/throat, pulmonary, gastrointestinal, and dermatologic symptoms.
Long COVID symptoms may change over time. The Patient-Led Research Collaborative survey found that some patients may have changing symptoms, or relapses brought on by different activities. One very common Long COVID symptom is Post-Exertional Malaise, a condition in which patients experience a relapse after physical or mental exertion, even if that exertion is relatively minor.
Some Long COVID patients have been sick for over 18 months. The Patient-Led Research Collaborative survey covers symptoms over a course of seven months, but some Long COVID patients have been suffering for far longer. Some patients who initially contracted the coronavirus in spring 2020, during the first wave in the U.S., have now been sick for 18 months or more.
Many Long COVID patients are unable to work. According to the Patient-Led Research Collaborative survey, almost half of the Long COVID patients who responded (45%) “required a reduced work schedule, compared to pre-illness.” Another 22% were not working at the time of the survey because of Long COVID. Other studies have backed up the findings from this survey. At this point in the pandemic, some Long COVID patients are struggling to receive accommodations from their employers, even though the condition is recognized as a disability at the federal level.
Long COVID can occur at all age ranges, but is documented most in younger and middle-age adults. Among respondents to the Patient-Led Research Collaborative survey, about 24% were in their thirties, 31% in their forties, and 25% in their fifties—though patients ranged in ages from 18 to over 80. This survey and others have also found that Long COVID seems to be more common for women; this pattern aligns with other post-infectious conditions, like chronic fatigue syndrome and chronic Lyme disease.
Long COVID may lead to long-term neurological issues. This past summer at the Alzheimer’s Association International Conference, a few researchers presented findings on Long COVID and Alzheimer’s. Brain scans of COVID-19 patients, along with observations of patients’ prolonged symptoms, suggest that adults who suffer from Long COVID may have an increased risk of Alzheimer’s later in life. Severe COVID-19 patients in their sixties and seventies are already starting to see symptoms matching early-onset Alzheimer’s, one researcher told NPR.
Autoimmune response may be one cause for Long COVID symptoms. While scientists are still working to determine exactly how a coronavirus infection may lead to numerous symptoms, research thus far suggests that overreaction of the immune system could be a major player. Some clinicians who work with Long COVID patients have developed treatments based on dysautonomia, medical conditions caused by immune and autonomic nervous system issues.
About 5,200 children in the U.S. have been diagnosed with MIS-C, and 46 have died. MIS-C stands for Multisystem Inflammatory Syndrome in Children. The condition follows a COVID-19 infection in rare cases, leading to inflammation of different parts of the body. While this condition is not directly comparable to Long COVID, scientists think it may have similar causes. The condition has disproportionately impacted children of color in the U.S.: out of 5,200 cases, 61% are Black or Hispanic/Latino.
The risk of Long COVID is dramatically lower after a breakthrough infection, even if you contract the coronavirus. A recent study published in The Lancet found that vaccinated patients who later had a breakthrough COVID-19 case were about half as likely to report symptoms after four weeks, compared to unvaccinated patients who had a non-breakthrough COVID-19 case. Plus, vaccinated people are already far less likely to contract the coronavirus in the first place, because vaccination reduces risk of infection. Commenting on the study, NIH Director Dr. Francis Collins called it “encouraging news,” though he cautioned that more research is needed on this topic.
Vaccination may help alleviate COVID-19 symptoms for Long COVID patients. In addition to reducing one’s risk of developing Long COVID, vaccination can alleviate symptoms for Long COVID patients. A recent preprint, posted online at the end of September, found that Long COVID patients who got vaccinated were about twice as likely to completely recover, compared to unvaccinated patients. “Overall, this study adds to growing evidence that vaccines can improve symptoms and lessen the disease impact in Long COVID,” wrote Long COVID researcher Dr. Akiko Iwasaki, sharing the study on Twitter.
To me, these Long COVID statistics—along with everything we still don’t know about the condition—provide a strong argument for vaccination. Long COVID can impact people who were young and healthy before they were infected, completely messing up their lives for months or even years. It surprises me that public health and political leaders don’t discuss this condition more when they tell people to get vaccinated.
As for continued research: the NIH’s RECOVER Initiative has received over $1 billion in funding from Congress, and it’s just getting started on setting up studies. If you’re interested in learning more about the research—or signing up to participate in a RECOVER study—you can sign up for email alerts on the NIH website.
I couldn’t decide which of these news items to focus on for a short post this week, so I wrote blurbs for all five. This title and format are inspired by Rob Meyer’s Weekly Planet newsletter.
HHS added vaccinations to its facility-level hospitalization dataset: Last week, I discussed the HHS’s addition of COVID-19 patient admissions by age to its state-level hospitalization dataset. This week, the HHS followed that up with new fields in its facility-level dataset, reflecting vaccinations among hospital staff and patients. You can find the dataset here and read more about the new fields in the FAQ here (starting on page 14). It’s crucial to note that these are optional fields, meaning hospitals can submit their other COVID-19 numbers without any vaccination reporting. Only about 3,200 of the total 5,000 facilities in the HHS dataset have opted in—so don’t sum these numbers to draw conclusions about your state or county. Still, this is the most detailed occupational data I’ve seen for the U.S. thus far.
A new IHME analysis suggests the global COVID-19 death toll may be double reported counts: 3.3 million people have died from COVID-19 worldwide as of May 8, according to the World Health Organization. But a new modeling study from the University of Washington’s Institute for Health Metrics and Evaluation (IHME) suggests that the actual death number is 6.9 million. Under-testing and overburdened healthcare systems may contribute to reporting systems missing COVID-19 deaths, though the reasons—and the undercount’s magnitude—are different in each country. In the U.S., IHME estimates about 900,000 deaths, while the CDC counts 562,000. Read STAT’s Helen Branswell for more context on this study.
The NYT published a dangerous misrepresentation of vaccine hesitancy (then quietly corrected it): A New York Times story on herd immunity garnered a lot of attention (and Twitter debate) earlier this week. One specific aspect of the story stuck out to some COVID-19 data experts, though: a U.S. map entitled, “Uneven Willingness to Get Vaccinated Could Affect Herd Immunity.” The map, based on HHS estimates, claims to display vaccine confidence at the county level. But the estimates are really more reflective of state averages, and moreover, the NYT originally double-counted the people who are strongly opposed to vaccines, leading to a map that made the U.S. look much more hesitant than it actually is. Biologist Carl Bergstrom has a thread detailing the issue, including original and corrected versions of the map.
We still need better demographic data: A poignant article in The Atlantic from Ibram Kendi calls attention to gaps in COVID-19 data collection that continue to loom large, more than a year into the pandemic. The story primarily discusses race and ethnicity data, citing the COVID Racial Data Tracker (which I worked on), but Kendi also highlights other underreported populations. For example: “The only available COVID-19 data on undocumented immigrants come from Immigration and Customs Enforcement detention centers.”
NIH college student trial is having a hard time recruiting: If you, like me, have been curious about how that big NIH trial to study vaccine effectiveness in college students has progressed since it was announced last March, I recommend this story from U.S. News reporter Chelsea Cirruzzo. The study aimed to recruit 12,000 students at a select number of colleges, but because the vaccine rollout has progressed faster than expected, researchers are having a hard time finding not-yet-vaccinated students to enroll. (1,000 are enrolled so far.) Now, students at all higher ed institutions can join.
Last spring, the National Institutes of Health (NIH) set up a special website compiling guidance on how to treat COVID-19 patients, intended as a resource for physicians and researchers. We featured this source in an issue a couple of months ago, but I wanted to revisit it today because the site’s one-year anniversary is coming up this week!
According to Dr. Fauci, who gave the site a shout-out at the White House COVID-19 press briefing this past Friday, the website has seen 3.8 million American users and 2.6 international users since its launch on April 21, 2020. There have also been 23 updates to the guidelines themselves.
It’s pretty universally acknowledged in the science/health world that the U.S. federal public health agencies abdicated a lot of responsibility in 2020. But the NIH was one part of the infrastructure that kept chugging along, both through its support of vaccine development and its leadership in the global medical community. This website is a small part of those efforts.
Happy birthday, COVID-19 Treatment Guidelines! I hope your usage rate goes down through the rest of 2021.
On Friday, Collins posted a video of a “COVIDized” “Here Comes The Sun” to his NIH Director’s blog, in which he thanked “NIH-ers” and promised a way out of the “long, dark, COVID winter.” It’s best if you see for yourself:
The song was great of course but I loved the cat (her name is Zoe!) cameo the most.
Indeed, while numbers are looking a little worrying now, it’s pretty certain that we’re riding out the tail end, at least in the U.S.