It’s an unfortunate reality in the Long COVID media landscape that a lot of journalists and commentators write about this condition without really doing their research. I frequently see articles that misunderstand key aspects of Long COVID or dismiss patients’ experiences.
Two recent stories (one in the Washington Post and one in Slate) make these mistakes, in fairly high-profile outlets. I’m not going to link to the full pieces here to avoid giving them more attention, but I wanted to share a bit about what these stories get wrong, to help readers recognize similar issues in other pieces.
The Washington Post piece discusses results from a data analysis project that the news outlet did in collaboration with Epic, an electronic health records company that has access to anonymized data from millions of people. Researchers evaluated whether patients had sought medical care for common Long COVID symptoms following a positive COVID-19 test. According to this analysis, Long COVID symptoms have become less common during the Omicron era compared to earlier COVID-19 waves—which may sound like a promising conclusion, until you recognize the analysis’ flaws.
Epic and the Washington Post didn’t share the full data behind this analysis, which makes it difficult to fully evaluate. But the public methodology provides enough information to be critical. First of all, relying on electronic health records for Long COVID leaves out a lot of people. Many of the people most vulnerable to this condition have limited access to PCR tests and to the doctors who might help them diagnose new symptoms, and PCR tests in particular have only gotten harder to access since early 2022.
Second, this analysis focused on people who had new symptoms after COVID-19—and excluded people who had existing symptoms that might overlap with Long COVID before they got hit by COVID-19. This focus leaves out people with preexisting conditions (i.e. other chronic diseases), who tend to be at higher risk for Long COVID. Epidemiologist Deepti Gurdasani has a helpful Twitter thread explaining this issue in detail:
Please don't put out poorly thought out 'research' like this- These comparisons are heavily flawed and serve only to massively underestimate the impact of long COVID & serve abelist narratives. 🧵 pic.twitter.com/cYUAQJvDV2
Meanwhile, the Slate piece dismisses Long COVID, arguing that the condition is “neither as common nor as severe” as experts have warned it might become. Like the Washington Post piece, this article bases its conclusion on flawed research that focuses on biased health records, and other types of biased data. For example, the author argues that people aren’t getting social security disability benefits in large numbers; but Long COVID patients face many barriers to this program, as I’ve covered for KHN.
The Slate article fails to cite Long COVID patients or experts who have cared for those patients. It also fails to include extensive research showing that Long COVID can mean lasting damage to many organ systems. In fact, Slate issued a correction to the piece shortly after it was published, explaining that, yes, research has “identified biological changes” associated with Long COVID. (The author initially wrote that there were “no biomarkers” for Long COVID.)
I’ve signed onto a letter demanding that Slate retract this article, along with hundreds of other journalists, researchers, and clinicians with Long COVID expertise. You can read it and consider signing here.
These two articles fall into a similar trap: they cherry-pick evidence to suggest that Long COVID might not be as common as some experts and patient-advocates say it is. But they ignore substantial evidence showing how widespread and how damaging the condition actually is. And furthermore, even if Long COVID is getting “milder” or “rarer” with Omicron, so many people have been infected by it (and by prior variants) that there are still millions out there who need help. Arguing over prevalence distracts from the true story: people are suffering, and they need support.
It’s important to note that the majority of journalists covering Long COVID are doing so in good faith, simply trying to understand a complex and confusing condition. But it can be easy to make mistakes (like citing the wrong evidence, or failing to talk to a person with Long COVID). Plus, some bad actors have shown up in the media again and again; the author of the Slate article, for example, previously wrote a highly discredited story for New York Magazine.
For other journalists covering this topic, I’m always happy to help answer questions or point folks to resources. The tipsheet I compiled for NICAR might be a good place to start. And for editors assigning these stories: please make sure you’re giving assignments to a credible writer.
I have a new story out in National Geographic this week about a growing area of research connecting the gut microbiome—the diverse community of microorganisms that live in our digestive systems—with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), the chronic disease that often occurs after viral infection and has many commonalities with Long COVID. (Here’s a non-paywalled link to the story.)
Two recent papers, both funded by the National Institutes of Health, point to specific differences between the gut ecosystems of ME/CFS patients and those of healthy controls. The new studies built on previous research in this area, but utilized larger patient cohorts than typical ME/CFS studies. Their findings provide avenues for better diagnosing and treating ME/CFS patients, as well as people with Long COVID who meet the criteria for ME/CFS. (Some studies suggest about half of Long COVID patients fall into this category.)
Continued gut microbiome research could identify specific bacterial supplements that help alleviate ME/CFS symptoms, along with new drugs that target specific changes in these patients’ metabolisms and immune systems. But many people with ME/CFS and Long COVID aren’t waiting for the clinical trials; they’re experimenting with the supplement and diet changes that are already available.
One big project in this realm is Remission Biome, a study by two ME/CFS patients who were working scientists before their symptoms became disabling. Patient-researchers Tamara Romanuk and Tess Falor both have experienced “remission events,” in which their ME/CFS symptoms faded after taking bacterial supplements. When they met on Twitter, they started a project attempting to recreate those events—but it quickly grew into a much larger effort to understand how the microbiome interests with post-viral illness symptoms.
I talked to Romanuk and Falor for my National Geographic story. We discussed how to design a study in which the scientists are also the patients, how their project builds on big data in microbiome research, communicating with the patient community, future plans for Remission Biome, and more. Since most of the conversation didn’t make it into my story, I wanted to share it here.
This interview has been lightly edited and condensed for clarity.
Betsy Ladyzhets: I wanted to start by asking how you all came to do this project, specifically replicating remission events that you’d experienced in the past, and how that intersects with other research that’s been done in this area of ME/CFS and the microbiome.
Tamara Romanuk: I had always been planning on trying to replicate the event… It had been in my mind constantly to try to recreate the experience. I actually did, at one point, take another course of amoxicillin [an antibiotic] but I didn’t do anything else. I didn’t do the probiotics. I didn’t do the sort of the full suite that I was that we’re proposing here [in the Remission Biome protocol].
So, it’s something I would have come to on my own regardless. But when I met Tess and she told me that she had had a similar event, it seemed like, okay, this was something we were probably going to do in the future together. It was just a matter of when. I think we must have talked about it even within the first weeks of meeting each other.
Tess Falor: It was, 10 days [after we met]… I had an interesting experience, in that that I didn’t realize that it was the antibiotics that might have done this [alleviated symptoms]. So back when I had my event in 2009, I went gluten-free and started the antibiotics at the same time. And two days later, after I had my major remission, I accidentally ate gluten. And then I felt worse the next day. So for 13 years, I’ve been assuming that it was going gluten-free that made the difference. And I never consider that I could recreate it because I’ve been gluten for that whole time.
It wasn’t until I met Tamara last fall that I realized that, wow, this [remission event] actually could have been the antibiotics. So when that came up, then, Tamara had this idea to try to recreate it. If it was actually the antibiotics that did it, could we create this really extreme remission event?
BL: I see. In terms of identifying the antibiotics, the probiotics, and the other treatments that you’re using in this study, how did you arrive at this protocol that y’all are following?
TR: Yeah, great question. When we decided to recreate it, the plan started as, “let’s take the antibiotics, and let’s throw in some probiotics, and let’s see what happens.” But we’re scientists, so it morphed very, very quickly into something much, much bigger.
Where Tess and I went in our minds was directly to the theory and the models that would have given rise to a phenomenon like this. Instead of starting at a protocol, we went, “this is our pet theory [about why remission occurred], and if our pet theory is right, how do we work backwards and recreate the protocol?” One of the really interesting things about doing it from that angle was that most of the stuff that I had initially thought I would include I actually threw out very, very quickly. The probiotic that I thought we were almost for sure going to use has ended up being, “oh, that actually might have stopped my event from continuing rather than promoting it.”
And we’re working in an age where there’s some really new cutting-edge databases and information sources out there. I wouldn’t have actually been able to do this type of protocol development a few years ago, even. [For example], we knew that we wanted to manipulate tryptophan metabolites in the gut. And so we needed to find strains of bacteria that were involved in tryptophan metabolism. And then we also knew that we wanted really specific metabolites to be produced in the gut and get to the brain. We were able to go into a database and actually follow that chain, identify specific strains of bacteria that would do exactly what we wanted in terms of gut and brain metabolites, and then trace it back to probiotic manufacturers. That’s pretty phenomenal. And that wouldn’t have been possible two years ago.
BL: Yeah, that’s incredible that you could just follow it all the way through like that.
TF: Absolutely. I’ll also mention that we’ve gotten advice from experts, too. Three people who study the microbiome gave us specific advice, and it all kind of converged in the same ideas, the same strains. So that was cool, too.
BL: Actually, it’s interesting that you mentioned tryptophan, because that was one of the processes identified in the recent papers [the two studies that were the focus of my National Geographic story] as well. I think the main one they looked at was butyrate.
TF: Yeah, those are both things that we are thinking about as part of our hypotheses. When those papers came out, we were like, “wow, this is really cool timing.” We read the papers, and found [their findings] line up with what we’re thinking. And we’ve already been thinking about this for months.
TR: There’s a really neat tie-in here in terms of the tryptophan metabolism. Because initially, my theory had been surrounding Robert Phair’s idea of the “Metabolic Trap,” which is, of course dependent on tryptophan. But the [remission] event itself was also incredibly unique because it was a bit psychedelic. Colors were brighter, smells were smellier, the world was amazing, we felt overwhelming gratitude. I tell people that it was a little bit like a mix between doing MDMA and psilocybin mushrooms. But without the hallucination. It was just this overwhelming change in my mood.
So I was thinking about tryptophan, serotonin, the same receptors that might actually get activated during a psychedelic trip. It really seemed that this entire pathway—from tryptophan to serotonin, to some good and some bad molecules like kynurenine, which can be both pro- and anti-inflammatory, and then quinolinic acid, which is absolutely pro-inflammatory in the brain. When you start at tryptophan, you keep going along this pathway, and whatever path it ends up following, you get different neurotransmitter activity going on. [The remission] was a microbiome event, but it’s really a microbiome-mediated event that’s occurring in the brain.
BL: That makes sense, yeah. Because it’s the microbiome that impacts these metabolic processes that then impact what’s happening in the brain, right?
TR: Absolutely.
BL: In terms of tracking what happens when you do this protocol, what are you using to study the changes in your gut and the further progression that you were talking about?
TF: Tamara knows more details than I do, but I’ll just say we are measuring a ton of biomarkers. Everything from specific composition of the gut, to measures of the immune system, like cytokines, and measures of what’s going on in the brain.
TR: We probably have about a thousand metabolites that we’re gonna track. When you consider that we’re doing a lot of these pre[-trial], hopefully during as well as post, it really adds up. It’s actually one of the most exciting parts about the project, for Tess and I. We both have an explicitly systems thinking approach to science, and we love big data. This is something that actually really excites us, we’re going to be able to really dig in.
All of these tests really work in concert as well. The immunogenetics angles are really key for us. And Tess and I have some unique, similar genetic backgrounds, so that’s going to tie in. Then tracking neurotransmitters: actually tracking tryptophan, tracking serotonin, tracking kynurenic acid and quinolinic acid, as well as their ratios. And all of these metabolites.
BL: I see. Yeah, I feel like that will be really interesting to look at all the interactions between these different things. I know you mentioned that you’ve consulted with folks on the protocols, are there other things that you’re doing to maintain the safety of the experiment?
TR: Absolutely. So we’re working with one of my personal GPs [general practitioners], and she’s kind of acting as our GP safety liaison. She will be on hand if anything strange happens. But really what we’re doing in terms of safety is we’re testing ahead of time. We’re making sure we don’t have leaky gut, we’re making sure we don’t have a compromised blood-brain barrier, or making sure that we don’t have certain pathogenic bacteria in our system that could explode if they weren’t affected by the amoxicillin—and lead to a massive, very adverse reaction.
The main tests we’re doing there is from a company called Cyrex, they do these amazing immune tests… And then we’re doing tests like the GI effects from Genova, which will actually tell us if we have high levels of any pathogenic or potentially-pathogenic bacteria in our guts, before we actually start. If any of [certain concerning biomarkers] turn up as being really high for one of us, then we will take some time out, try to correct that specific defect and then proceed again.
BL: That makes sense.
TF: We do have a clinician who has a lot of experience with these specific tests, and specifically with the gut, who’s helping us. In addition to Tamara realizing it was a good idea to do all this pre-testing, she recommended it, too. So she can take a look at our results, and give us her perspective.
TR: One of the things we want to do there is, we want to actually figure out a very simplified testing protocol, which we can suggest to people to do for themselves before they do this [experimenting with supplements]. Because we want to actually bring this work to people who really need it, but we also want to make sure they’re safe. Hopefully, all of the testing that we do will help us arrive at a couple of biomarkers, which we can then tell people, “Look, if you test these one or two or three things, then you can do this without worrying so much about having side effects or adverse consequences.”
Right now, it would cost the regular person probably about $2,000 to test everything that we’re testing, in terms of making sure all these levels are safe. We want to figure out a way to decrease that cost, break that down into specific biomarkers. And then, hopefully, when we move into our Phase Two of Remission Biome—which is actually bringing this work to the patient population—we might even be able to give people these tests, or at least provide them with very significant discounts for these tests.
BL: Yeah, that’s something I wanted to ask you more about, too, is how you have been communicating with other people who want to try this sort of thing. I know from following y’all on Twitter and seeing some of the discussion around this project that folks are so interested. And generally, of course, there’s a big interest among people with Long COVID, ME, other similar conditions just trying to see what would work while there are no official FDA-approved treatments.
How have you found that experience? And, as you look towards Phase Two, what are some of the things you’re going to be thinking about, in bringing these results to other people?
TF: I’ve been talking to people on Twitter. And I would say, we’ve mostly been recommending, “wait until we do this first experiment, so that we can learn from it.” But for people who happen to be getting prescribed antibiotics [for an infection or something similar], then they have their doctor watching them. In that case, we can say, “you want to protect your gut, here are the probiotics that we’re doing, and you might possibly want to do a biome site test while working with your doctor.”
TR: We have had such an overwhelming response. I think hundreds of people must have contacted you [Tess] personally now with a story that they thought might be a revision event, like the one that we’re describing. And hundreds more have said that they’ve had some sort of a positive or negative reaction to antibiotics. And they’ve had ME/CFS, or Long COVID. Those stories are really the jumping-off point for us. We want to put together a very formal survey to actually figure out how people are responding to antibiotics in post-viral illness, in general. There are a lot of clues in people’s stories.
And the response of our community has been almost overwhelmingly positive, but there have been a few people who’ve had pretty severe baseline decreases after taking antibiotics. It’s always hard to know if the antibiotic itself was responsible for that decline or something else. But we really want to delve into that and figure out whether there’s a subset of people that seem to be having negative reactions.
BL: I also wanted to ask about communicating the results from this work. What are you thinking about in terms of both sharing with other people in the community, and also, are you looking towards like a preprint, or scientific publication?
TF: Yeah, we’ll be communicating in real-time with the community on Twitter, and getting input from all the scientists that we’ve talked to. That’s also something that we didn’t really mention yet is, we’ve talked to over 20 different researchers and gotten input from them. We have some that are interested in analyzing our results afterward. So, there’s community communication, but we are also planning to publish it, at least as a preprint.
TR: We’re going to be a great case study. And it’s going to be a great paper. It’s not going to end up in a formal journal, but we’ll definitely pop it into one of the preprint servers.
In addition to the case study, though, we really want to do a meta-analysis. A formal meta-analysis of all the studies that have ever looked at antibiotic use and post-viral illness. We think there are a lot of clues there. One of the things that’s really fascinating to us about this is that there are a number of similar situations that have happened in other conditions. One of the really key ones is PANS, or PANDAS, which often occurs in children when they get a staph infection—and then they get this crazy neurological event where their behavior changes and they develop OCD. Well, turns out, in an enormous number of those cases, if you give them antibiotics of the right type quickly enough—and a lot of the time, it’s amoxicillin plus minocycline, or doxycycline—you can actually completely put that child into remission.
And there’s other disease groupings that seem to have these remission events, in very similar ways. Even Alzheimer’s, many people who have a grandparent with Alzheimer’s will tell stories of moments of complete lucidity. This indicates that maybe brain damage isn’t the ultimate issue, maybe there’s something going on with the communication networks. And that’s really what we’re targeting here [in our research].
BL: That’s really interesting. I was actually just talking to another researcher for this story [Sonia Villapol at Houston Methodist Hospital], who mentioned that her lab, where she is studying Long COVID and the microbiome, has also done work on Alzheimer’s, and even traumatic brain injuries, where there’s some kind of microbiome interaction. I thought that was really interesting. It definitely seems like there’s so much more to be explored here.
TF: Yeah, one of the researchers that we talked to is also doing ME/CFS and Long COVID research, and then Parkinson’s—using probiotics for Parkinson’s. I think a lot of what we’re doing can apply to other conditions, too.
BL: Right. I also wanted to ask if y’all had any other comments about the two recent studies?
TR: Well, I was pretty excited to see butyrate as sort of the highlight molecule. Very early on, we decided that we were going to try to increase our butyrate levels… So we were really excited to see that both of those papers linked to butyrate-producing bacteria, which was really key for us. It’s not just that we want to increase butyrate during the experiment itself, but it’s also a great way to actually help heal leaky gut issues. So it’s a really great intervention.
BL: Yeah, that’s something that has come up a lot in the research I’ve done for this piece—the value of intervening early and trying to help people out before they’re going to have long-term symptoms, or at least in the earlier stages of illness. Which I know is one of the reasons why there’s so much interest in Long COVID, because you’re ideally diagnosing people earlier than what’s historically been the case for ME and some of these other related conditions.
TR: To me, the really exciting application of this is that antibiotics are a very safe intervention that have been used for dozens of years. If it turns out that there’s a chance that taking a quick course of amoxicillin and a tetracycline like minocycline or doxycycline, can take someone who might have developed much more severe Long COVID and then MECFS out of that track, well, that’s phenomenal. If there was actually something that you could go to your doctor and say, “hey, I’m having these Long COVID symptoms, what can we do right now?” And the answer is, “well, it’s pretty safe, why not just give you a week’s worth of antibiotics?” It’s a pretty exciting possibility that we could stop some of these more severe cases.
BL: Yeah, absolutely. I also wanted to ask, in terms of the institutional side of this, what do you think the NIH and other government agencies could be doing to better support this kind of work, and integrating ME/CFS and Long COVID research, as we try to understand the common mechanisms here?
TR: Well, they could actually be treating us. This is really the biggest roadblock: there are hundreds of thousands of people out there who are undiagnosed and untreated, and are trying to biohack their way out of serious post-viral illness. None of these people are seeing clinicians that know what they’re talking about. So, we need treatment centers—but not just the Long COVID treatment centers, where they just tell people to rest, but centers that actually do biochemical testing, figure out what’s actually going on in their bodies, and then doing targeted treatment.
Even if you can’t cure ME/CFS right now, it doesn’t mean that you can’t help people feel phenomenally better, and make sure that they don’t slide from moderate into severe. What you said before is so key, because most of us slide from moderate to severe when we get comorbidities. When we get MCAS on top of the Long COVID, for example. All of these comorbidities compound, and then they get people to a state where almost any intervention is aggravating to their systems, and they literally can’t tolerate light or sound or food. Treating someone at that stage is almost impossible, unfortunately, at this point. So early intervention is really key—but to get early intervention, you need clinicians that know what they’re doing interacting with patients.
BL: Which we don’t have nearly enough of.
TF: Yeah, that’s a major problem. Another angle that I’ll mention is more funding for research, specifically for ME/CFS. There are a lot of really great ME/CFS scientists who haven’t been able to get funding, but they’ve been trying to study this for decades. I keep hearing people saying that there’s these new researchers coming into Long COVID, who don’t really understand a lot about the history and what’s already been done. I think we need more funding for ME/CFS research, plus particularly funding for people who have been doing this for a long time.
TR: Absolutely. One of the things that Tess and I are really excited about is—I guess what we’re going to be calling Phase Three, but it’s starting now—is we’re putting together a hybrid DAO, plus a nonprofit, to actually provide funding for researchers in this area. It’s not just for researchers, it’s specifically for PhD patients.
We really want to tap into this community of sick scientists who’ve been sidelined by ME/CFS, by COVID, by other disabilities, and offer them the chance to actually get back into research in a way that they could do and would be supported. We’re really seeing a new model, a new way of being able to conduct research that is outside of academia, yet has checks and balances and support. Remission Biome has been, hands down, the best thing for my mental health that has happened in 10 years. If I could bring little bit of that to other people in my position—that’s what I would like.
TF: We’ve actually had a lot of people volunteer to help. And I’ve gotten the comment many times, people saying, “this feels so good to use my expertise again.” These are people that have been on disability for 10 years and haven’t been able to do any work or any research. And now they’re able to give their expertise towards our project, and help us gain momentum and move forward, and they’re just really happy about it. I think there’s so much untapped expertise out there.
BL: Yeah, that makes so much sense. And I hope I can keep following this project as y’all expand it.
Cover slide from my workshop at NICAR this weekend.
On Friday, I led a workshop at NICAR about covering Long COVID. NICAR is a data journalism conference—the acronym stands for National Institute for Computer-Assisted Reporting, which is an old-school term for data journalism—so my session focused on data sources, along with suggestions for public records requests and for interviewing long-haulers.
My main goal for the workshop was to introduce Long COVID as a worthwhile coverage topic for journalists who aren’t already on the science or health beat. Plenty of science/health reporters (like myself) have written great articles about biomedical research, patient experiences, and other similar topics. But there are many other facets of Long COVID, ranging from its impact on work to the public agencies that should be held accountable for failing to address this crisis.
To that end, I spent part of the session talking about excellent Long COVID articles that don’t focus on science/health topics. I also gave attendees a prompt to brainstorm story ideas for their beats or coverage areas. This led to some interesting conversations about potential local stories on Long COVID clinics, Household Pulse Survey data, tracking disability applications, and more.
Also: as I’ve mentioned previously, I am currently leading a project at MuckRock (where I work part-time) to investigate U.S. government responses to Long COVID. For any journalists who may be interested in collaborating with MuckRock on Long COVID or other public health topics, you can reach out to us here.
I got an interesting question from a reader last weekend, asking if excess deaths might be one way to identify the impact of Long COVID. It’s an interesting idea: could the numbers of deaths from medical causes above what researchers expect in a given timeframe indicate some premature deaths tied to Long COVID?
Based on my previous work with excess deaths (see MuckRock’s Uncounted project), I think this could be possible, though it’d likely be very hard to identify direct relationships between Long COVID and specific deaths. As far as I know, no researchers are working on this question; if you know of anyone who is, please reach out.
Still, the reader’s question got me thinking about how, exactly, we track the impacts of Long COVID. Doctors, researchers, and long-haulers themselves have learned a lot about the condition over the last three years. We still don’t have clear estimates of exactly how many people in the U.S. are dealing with this chronic disease, but we’ve come much closer to understanding its impacts than we were when patients first began advocating for themselves in 2020.
Tracking Long COVID is challenging because of uneven access to COVID-19 tests and to medical care, which means long-haulers with certain types of privilege are more likely to get an accurate diagnosis. A lack of knowledge about Long COVID, both among medical professionals and among the overall population of people who might get it, also contributes to this issue. (For more details, see this post from early December.)
Still, some strategies have emerged for identifying people with Long COVID and tracking how the condition is impacting them. Here are a few.
Following people who were hospitalized for COVID-19:
In this strategy, researchers identify people who had COVID-19 and track how the virus impacts them over time. It’s often easiest for researchers to track people who were hospitalized, since hospitals keep detailed medical records of their patients, though this tactic leaves out long-haulers who initially had mild cases.
Sometimes, researchers doing this type of follow-up study will directly survey COVID-19 patients, which can lead to more comprehensive data than using health records alone. One recent study in this category found that, among a group of 800 adults hospitalized for COVID-19, about half were still experiencing some financial issues and limitations in their ability to do day-to-day activities six months later. The study’s authors noted that financial issues were “reported more frequently” among patients who identified with demographic minorities.
Following COVID-positive patients through electronic health records:
Angela Vázquez, president of the Long COVID group Body Politic, summarized the two new studies succinctly on Twitter, writing: “Black and Hispanic Americans appear to experience more symptoms and health problems related to #LongCovid than white people, but are not as likely to be diagnosed with the condition.” Vázquez also pointed out that the studies may have missed neurological symptoms among Black and Hispanic patients, due to less access to care for these groups.
Black and Hispanic Americans appear to experience more symptoms and health problems related to #LongCovid than white people, but are not as likely to be diagnosed with the condition, according to new research funded by the National Institutes of Health.https://t.co/IUjyfdzqIZ
Electronic health records are far from perfect sources of Long COVID data, as they often present only sets of information that doctors are already compiling—and they are often biased towards the people who are able to access medical care for COVID-19 (or Long COVID) in the first place. As a result, some researchers track Long COVID through broader surveys, seeking to identify everyone who might have some long-term symptoms following a COVID-19 case, even if those people might not be calling their condition “Long COVID.”
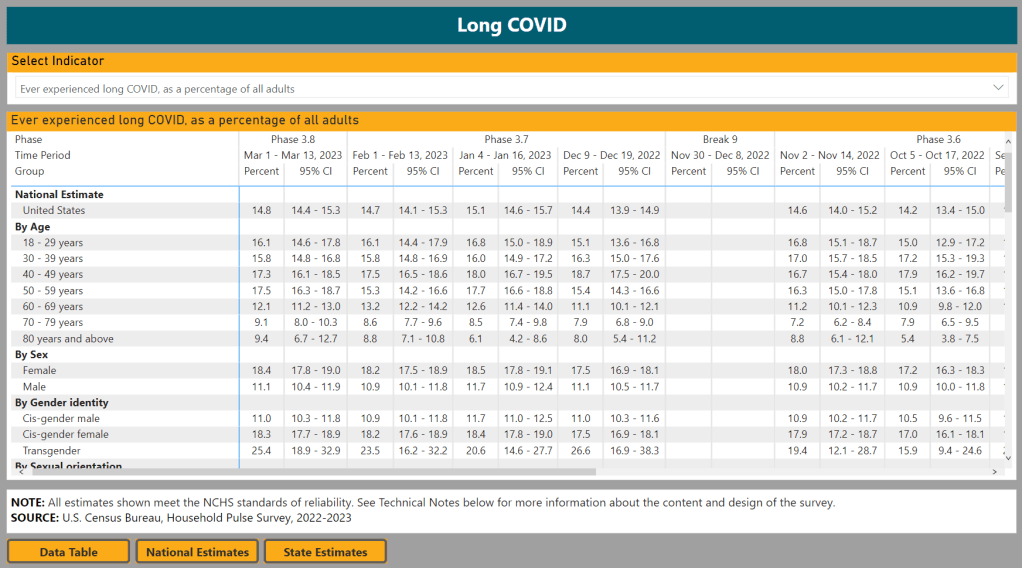
The Census and CDC’s Household Pulse Survey questions on Long COVID are one notable example of this strategy. Census researchers ask a random sample of Americans whether they’ve had “any symptoms lasting 3 months or longer” following a COVID-19 case, then follow up with questions about whether those symptoms are current and whether they impact the respondent’s ability to carry out day-to-day activities. The resulting data provide a broader view of Long COVID in the U.S., including people who may not have sought medical care for their symptoms.
Biological studies of specific organs impacted by COVID-19:
In order to better understand how a case of COVID-19 may lead to long-term, debilitating symptoms, some researchers focus on studying exactly what happens to different parts of the body after a coronavirus infection. This research sometimes focuses on testing for the continued presence of virus after a patient’s acute COVID-19 case is over or tracking changes to the immune system, as scientists test different theories into how Long COVID occurs.
One major area of research has been the brain. Freelance journalist Stephani Sutherland recently published a major feature in Scientific American exploring how Long COVID impacts the brain and nervous system, summarizing research into the biological causes of common symptoms like fatigue and brain fog. Physician E. Wesley Ely, who cares for Long COVID patients, wrote an essay on the same topic that appeared in STAT News this week; Ely discussed what he’s learned from autopsy studies examining the brains of people who had COVID-19.
Identifying trends in the labor market:
Finally, researchers often seek to track the impacts of Long COVID indirectly, by looking at statistics on people who have left the labor market during recent years. It’s no secret that a lot of people have left their jobs during the pandemic; Long COVID experts argue that the chronic disease may be one major driver of the labor shortage. One often-cited Brookings Institution analysis suggested two to four million people may be out of work due to Long COVID.
This strategy for studying Long COVID may be the most difficult, as it’s hard to actually tie job loss numbers to the condition without more specific data. Most research surveys or electronic health records databases don’t ask people about their work situations; the recent study cited above is a notable outlier. Similarly, most unemployment claims and short-term disability datasets don’t ask people if Long COVID is contributing to their need for assistance.
Still, I hope to see more studies in the future that examine Long COVID’s impact on work and other activities. Related: the U.S. Department of Labor recently published a report about the need for more assistance geared toward workers with Long COVID.
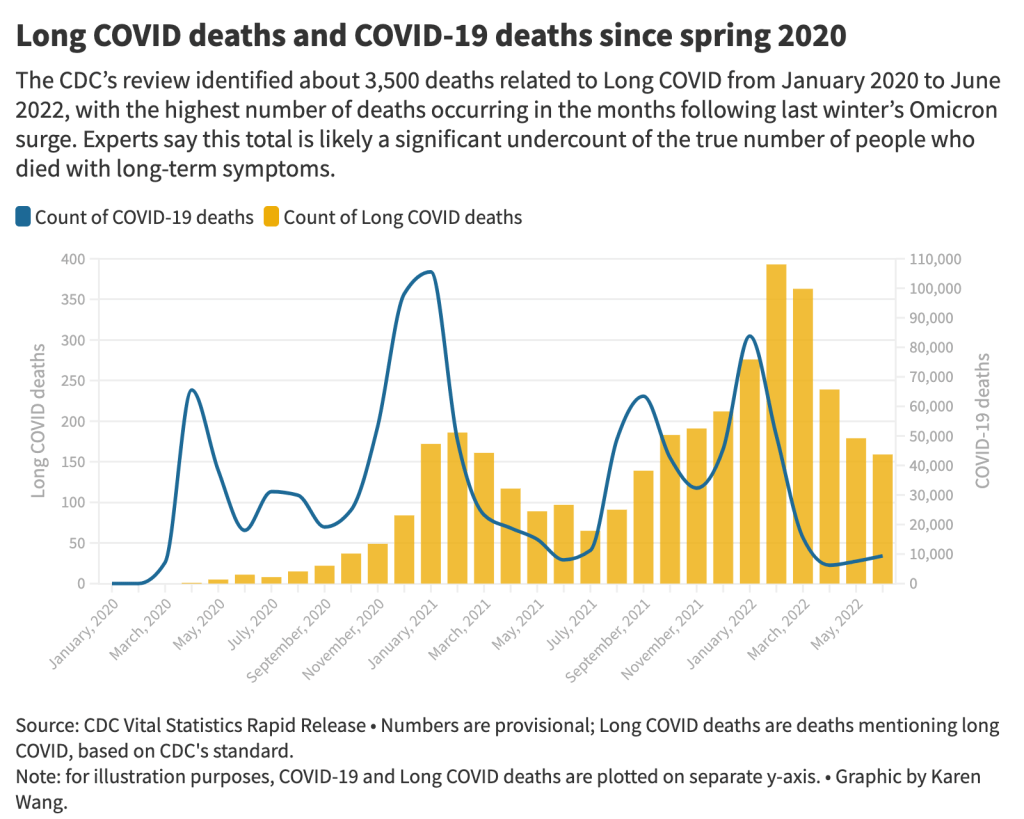
The 3,500 Long COVID-related deaths identified by the CDC’s review of death certificates are likely a significant undercount of mortality caused by this condition, experts say. Chart by Karen Wang; see the interactive version on MuckRock.
On Wednesday, the CDC’s National Center for Health Statistics (NHCS) released a major report on deaths from Long COVID. To identify a small (but significant) number of deaths, NCHS researchers searched through the text of death certificates for Long COVID-related terms. Their study demonstrates how bad our current health data systems are at capturing the results of chronic disease.
My colleagues and I at MuckRock did a similar analysis to the CDC’s, searching death certificate data that we received through public records requests and partnerships in Minnesota, New Mexico, and counties in California and Illinois. You can read our full story here and explore the death certificate data we analyzed on GitHub.
Here are the main findings from both analyses:
The CDC study is an important milestone in recognizing the reality of Long COVID: this is a serious, chronic disease that can lead to death for some patients. It’s not just an outcome of acute COVID-19.
From its national death certificate search, NCHS identified 3,544 deaths with Long COVID as a cause or contributing factor. This is almost certainly a major undercount, experts told me (and told other reporters who wrote about the study.)
This number is an undercount because we’re essentially seeing two poor-quality data systems intersect. Long COVID is undercounted in clinical settings because we lack standard diagnostic tools and widespread medical education about it—most doctors wouldn’t think to put it on a death certificate as a result. And the U.S.’s death investigation system is uneven and under-resourced, leading to inconsistencies in tracking even well-known medical conditions.
On top of these problems, when Long COVID is diagnosed, it tends to be among people who had severe cases of acute COVID-19 followed by difficulty recovering, experts told me. David Putrino and Ziyad Al-Aly, two leading Long COVID researchers, both pointed to the NCHS’s trend towards identifying Long COVID deaths among older adults (over age 75) as an example of this pattern in action, since this group is at higher risk for more severe acute symptoms.
The NCHS count of deaths thus misses Long COVID patients with symptoms similar to myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), which often arises after a milder initial case. It also misses people who have vascular impacts from a COVID-19 case, like a premature heart attack or stroke months after infection—something Al-Aly and his team have studied in depth. And, crucially, the NCHS count misses people who died from suicide, after suffering from severe mental health consequences of Long COVID.
While the NCHS count of Long COVID deaths is far too low to be accurate, the researchers did find more deaths as the pandemic went on—with the highest number in February 2022, following the first Omicron surge. This pattern could suggest increased recognition of Long COVID among the medical community.
The NCHS primarily identified Long COVID deaths among white people, even though acute COVID-19 has disproportionately impacted people of color in the U.S. Experts say this mismatch could reflect gaps in access to a diagnosis and care for Long COVID: if white people are more likely to be seen by a doctor who can accurately diagnose them, they will be overrepresented in Long COVID datasets. Putrino called this “a health disparity on top of a health disparity.”
MuckRock’s analysis of death certificate data in select states similarly found that most deaths labeled as Long COVID were among seniors and white people. The trends varied by state, though, reflecting differences in populations and in local death reporting systems. For example in New Mexico, which has a statewide medical examiner’s office (rather than a looser system of county coroners), three-fourths of the Long COVID deaths were among Hispanic or Indigenous Americans.
Our story also includes details about the RECOVER initiative’s autopsy study, which aims to use extensive postmortem testing on people who might have died from acute COVID-19 or Long COVID to identify biological patterns. Like the rest of RECOVER, this study is moving slowly and facing logistical challenges: about 85 patients have been enrolled so far, an investigator at New York University said.
Overall, the NCHS study suggests an urgent need for more medical education about Long COVID, especially as the CDC works to implement a new death code specific to this chronic condition. We also need broader outreach about the consequences of Long COVID. To quote from the story:
“Institutions like the CDC should do more to educate people about the long-term problems that could follow a COVID-19 case, said Hannah Davis, the patient researcher. “We need public warnings about risks of heart attack, stroke and other clotting conditions, especially in the first few months after COVID-19 infection,” she said, along with warnings about potential links to conditions like diabetes, Alzheimer’s and cancer.
And we need other methods of studying Long COVID outcomes that don’t rely on a deeply flawed death investigation system. These could include studies of excess mortality following COVID-19 cases, Long COVID patient registries that monitor people long-term, and collaborations with patient groups to track suicides.
For any reporters and editors who may be interested, MuckRock’s story is free for other outlets to republish.
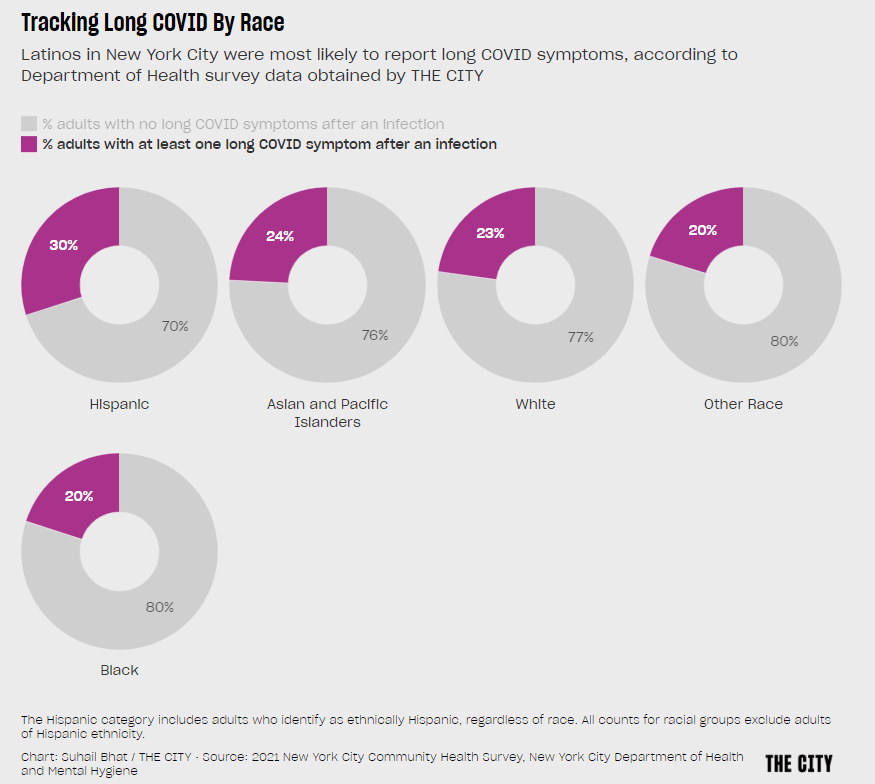
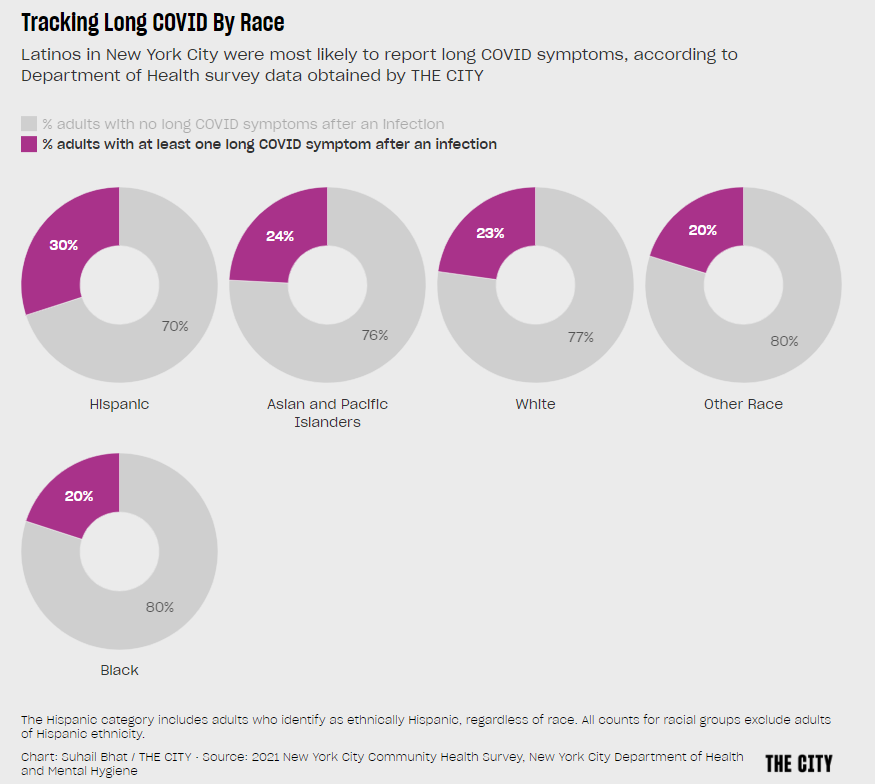
Hispanic or Latino New Yorkers were more likely to report Long COVID symptoms than other demographic groups, in a 2021 survey by the city health department. Chart via THE CITY.
I had two new articles about Long COVID published this week:
This story in Science News describes how researchers are working to fill gaps in Long COVID data, largely by collaborating with patients and across different areas of medicine.
This story in Gothamist/WNYC describes three public Long COVID clinics run by New York City Health + Hospitals, which offer a range of care to New Yorkers with the condition but fall short of all the specialties needed for comprehensive treatment.
The reporting process for both stories gave me a lot to think about, in considering potential improvements in recording who has Long COVID and how this chronic disease impacts people.
And we have a lot of room for improvement. There are plenty of reasons why Long COVID research and data collection are currently difficult, ranging from a lack of consistency in how the condition is diagnosed to historical underfunding for similar chronic diseases like myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and dysautonomia. For more details, see this post I wrote in May.
The U.S. scientific and medical systems also made specific mistakes early in the pandemic that contributed to our current data gaps, including the dearth of PCR testing—leading many current long-haulers to not have positive test results from their initial infections—and early refusals by many doctors to believe patients’ prolonged symptoms had resulted from the coronavirus. Most medical schools do not spend much time training new doctors to recognize complex, chronic diseases, leaving them unprepared to tackle Long COVID.
But these problems can be addressed—especially if doctors and researchers are willing to step outside their specific fields to collaborate with each other and with patients. Here are a few specific recommendations that I learned about in reporting my stories for Science News and Gothamist/WNYC.
Listen to and collaborate with patients.
“Patients know the right questions to ask to properly document their experience,” Lisa McCorkell, one of the founders of the Patient-Led Research Collaborative (PLRC), told me in an email interview for my story.
In fact, a survey study by PLRC in which patient-researchers asked other long-haulers to describe their symptoms is considered one of the most comprehensive accounts of this condition. Other researchers have used this list of symptoms in designing their own patient surveys.
Surveys are one important mechanism of compiling patient experiences, as they can capture information that does not make it into medical records. (Common Long COVID symptoms like post-exertional malaise often are not well-captured in these records.) But patients can also weigh in on other aspects of study methodologies, such as how to collect data in a way that won’t overly tax participants or how to compare groups of patients for accurate results.
Plus, hypotheses from patients can be valuable starting points for clinical trials, as Julia Moore Vogel from the Scripps Research Translational Institute explained to me. Vogel, who is a long-hauler herself, is working on a new study at Scripps that’s informed by her and other patients’ experiences with Garmin wearable devices. The projects funded by PLRC’s grant program offer further examples of research studies informed by patient priorities.
Connect health records from different sources.
One major challenge with studying Long COVID is that this complex condition can impact every organ system in the body. You can’t just analyze heart disease records from a cardiology practice, or lung function records from a pulmonary practice. Every patient could be seeing ten or more different specialists, and all of those doctors might inform different pieces of the overall disease puzzle.
As a result, devising systems that better compile and connect records from different sources is a priority for researchers studying Long COVID. Arjun Venkatesh, a patient-reported outcomes researcher, described this as “the clunkiest part” of his work: there are a lot of “hidden barriers” to connecting records, he said, ranging from privacy protections to technical mismatches. (For example, a patient requesting their records from a particular doctor might be asked to provide a fax number, something most people do not have in 2022.)
Still, new projects are in the works to make this type of data sharing easier. One example is Kindred, an app designed by Yale researchers that empowers patients to request their electronic health records and share them with scientists studying Long COVID. Patients also have more legal protections in making data requests now, thanks to a new federal rule that took effect this fall.
Use wearables and other new tracking technologies.
Smart watches, Fitbits, and other similar trackers are usually advertised for consumers interested in better tracking their individual health and fitness. But they can also provide valuable, long-term data to researchers studying health conditions like Long COVID.
The Scripps Research Translational Institute is one institution focused on wearable devices, through studies like Vogel’s and another program called the DETECT study, led by epidemiologist Jennifer Radin. In DETECT, researchers compile data from people across the country who have volunteered to share their wearable device data with Scripps. After one of the participants gets COVID-19, the scientists can compare their post-COVID health indicators to the patient’s pre-COVID baseline.
“We compare each person to themselves over time,” Radin told me when I talked to her for my Science News story. This method is different from traditional medical research, in which two similar groups of people are compared to each other on a population-wide basis.
Wearables research faces a lot of its own challenges, such as expanding access to more people (by making devices more affordable or even giving them to study participants for free) and creating analysis systems that can make sense of thousands of data points from each patient. But I personally find it fascinating and hope to continue covering this area. I was even inspired by my reporting to buy a smart watch, as a holiday present to myself.
Local surveys and outreach in partnership with community groups.
Anyone can get Long COVID—young or old, vaccinated or unvaccinated, with or without prior health conditions. But a lot of people still don’t know about this chronic condition, even when they might be experiencing long-term symptoms themselves.
As a result, a major priority for Long COVID researchers and patient-advocates is improving education and outreach about this condition. New York City has a program that could serve as an example here: NYC Health + Hospitals runs a hotline called AfterCare, which residents can call to learn about Long COVID and city resources, including the public clinics I wrote about.
While AfterCare has proactively called New Yorkers who previously tested positive for COVID-19, the program’s administrators are concerned that it’s likely not reaching everyone who could be served by the hotline. Local long-haulers who I talked to for my Gothamist/WNYC story want to see broader outreach—like subway ads, billboards, and commercials—telling people about Long COVID.
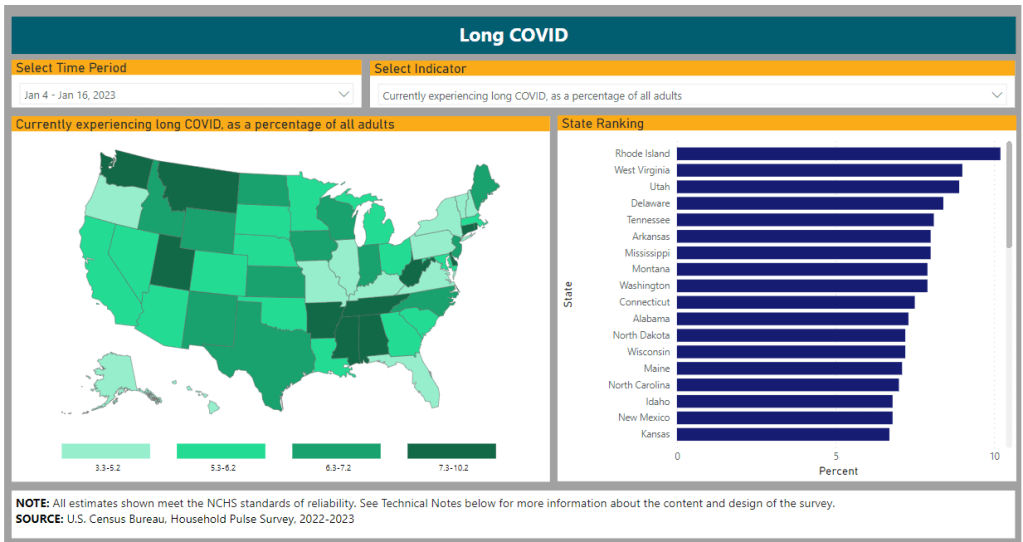
These same outreach programs could also help researchers collect more comprehensive data about Long COVID. Last week, THE CITY, another local NYC outlet, reported on some early results of a survey conducted by the city health department to find out which groups of New Yorkers are most vulnerable to the condition. Unsurprisingly, the survey found that Hispanic/Latino residents and those living in the Bronx were disproportionately impacted.
I hope to see more local health agencies follow in NYC’s lead to conduct surveys like this one, paired with outreach and education about Long COVID. This type of data could go a long way in showing political leaders where more resources are needed.
More data on the new, bivalent boosters: A new study, published this week in the CDC’s Morbidity and Mortality Weekly Report, has further evidence that the new, Omicron-specific booster shots provide additional protection against COVID-19 for people who previously received the original vaccines. Researchers used test results from pharmacies to compare symptomatic COVID-19 cases among people who had received the new boosters to those who had only received older vaccines. New booster recipients were less likely to get sick, they found, indicating protection against Omicron BA.4, BA.5, and their sublineages. In short: if you haven’t gotten one of the new boosters yet, now is a good time!
Patient-Led Research Collaborative announces grant winners: The Patient-Led Research Collaborative, an organization of Long COVID patient-researchers that has produced groundbreaking work about this condition, just announced the winners of its $5 million fund to support new biomedical research on Long COVID. The winning projects will pursue avenues of top priority to patients, such as understanding post-exertional malaise, testing for microclots, and a clinical trial for the drug naltrexone. Projects were themselves evaluated by a panel of patient experts and patients will be heavily involved in the resulting research. Congrats to the PLRC team on this announcement, and I look forward to following the results of these studies!
HHS publishes Health+ Long COVID report: Another piece of Long COVID news this week: the Department of Health and Human Services published a report summarizing interviews with people who have Long COVID. The report was one of several responses to the Biden administration’s call last spring for Long COVID research and support programs. It describes patients’ desires for meaningful research, better healthcare, financial support, and more. While this new report may not be adding much to the body of knowledge about Long COVID, it’s helpful to see this information coming from a major government source.
Football games associated with COVID-19 spread: And one more study that caught my attention this week: a new paper in JAMA Network Open describes a correlation between National Football League (NFL) games and COVID-19 spikes in the surrounding counties during the league’s 2020-2021 season. Counties hosting more popular games (with at least 20,000 fans present) were more likely to see increased COVID-19 spread afterwards. The paper shows how large events can contribute to widespread disease transmission, even among people who didn’t themselves attend the events.
The Long Haul and The Long COVID Survival Guide, pictured on Betsy’s desk. (Photo by Betsy Ladyzhets.)
Two new books about Long COVID were published this month, and I’d like to recommend both of them to any readers interested in learning more about the condition—especially to other journalists covering COVID-19.
First, The Long COVID Survival Guide (from the Experiment Publishing, released November 8) is a compilation of essays from people with Long COVID, for people with Long COVID, edited by journalist and Body Politic founder Fiona Lowenstein. The book covers everything from getting a medical diagnosis to finding community with advocates for other chronic illnesses.
The Survival Guide is structured like a manual, every chapter ending with specific “survival tips” for long-haulers to use in their own Long COVID journeys. But it’s also a very relevant read for people who don’t have Long COVID, as it provides context about the different challenges long-haulers might go through: medical gaslighting, cognitive challenges, women’s health issues, learning to ask for help, and more.
Personally, I got a lot of ideas for future journalism projects from this book. As someone covering scientific research and data, I found the chapters about getting a diagnosis (by Dona Kim Murphey, Rachel Robles, and David Putrino) and about navigating Long COVID research (by Lisa McCorkell) particularly valuable.
Second, The Long Haul (from Simon & Schuster, released November 15) is a nonfiction narrative about how people with Long COVID came together to better understand the condition and advocate for themselves. Author Ryan Prior is a journalist with experience at CNN and other national outlets, and has lived with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) since he was a teenager.
Prior brings his lived experience and his journalistic experience—which includes covering other chronic illnesses and patient advocacy movements—to covering Long COVID. The book provides valuable backstories on major Long COVID groups, like Body Politic, the Patient-Led Research Collaborative, and the COVID-19 Longhauler Advocacy Project. It also describes early research efforts seeking to better understand Long COVID, including the first stages of the National Institutes of Health’s RECOVER study.
I’m still reading The Long Haul (as of this writing, I’m a couple of chapters in), but am already finding it incredibly helpful to learn about how Long COVID advocates started pushing for research and recognition, with context from ME/CFS and other post-viral illness work.
The Long COVID Survival Guide and The Long Haul might not be the most upbeat reading choices for the holiday season, but they’re really vital for anyone engaging with Long COVID—whether you’re a journalist covering this topic or a friend to a long-hauler. To quote from Dr. Akiko Iwasaki’s afterword, in the Survival Guide:
Long COVID has changed the narrative. The world no longer has any excuse to make the same mistake over and over again, as we have done for previous pandemic and endemic infections. It’s finally time for us to listen.
Transparency note: I received advanced copies of both of these books to aid in my work as a journalist covering Long COVID, but am not getting any compensation to write this post—i.e., this isn’t sponsored content or anything. I genuinely want more people to learn about and read these books!
This week, I had a story published at Kaiser Health News (KHN) about barriers that people with Long COVID are facing as they apply for disability benefits, focusing on programs offered by the federal Social Security Administration. For me, working on this story highlighted the consequences of the U.S.’s poor data collection on Long COVID.
The article shares stories from a couple of individual patients who are unable to work due to their Long COVID symptoms, but can’t access the support they need. Here’s how the story starts, focusing on Brooklyn mom Josephine Cabrera Taveras:
When Josephine Cabrera Taveras was infected with covid-19 in spring 2020, she didn’t anticipate that the virus would knock her out of work for two years and put her family at risk for eviction.
Taveras, a mother of two in Brooklyn, New York, said her bout with long covid has meant dealing with debilitating symptoms, ranging from breathing difficulties to arthritis, that have prevented her from returning to her job as a nanny. Unable to work — and without access to Social Security Disability Insurance or other government help — Taveras and her family face a looming pile of bills.
“We are in the midst of possibly losing our apartment because we’re behind on rent,” said Taveras, 32. Her application for Social Security disability assistance, submitted last fall, was rejected, but she is appealing.
Like many others with long covid, Taveras has fallen through the cracks of a system that was time-consuming and difficult to navigate even before the covid pandemic. People are facing years-long wait times, insufficient legal support, and a lack of clear guidance on how to prove they are disabled — compounded by the challenges of a medical system that does not have a uniform process for diagnosing long covid, according to health experts and disability attorneys.
Estimates of how many people might be in situations similar to Taveras vary widely. I cite a couple of differing estimates in the story: one report from the Brookings Institution suggests between two and four million people may be out of work due to Long COVID, while another from the National Bureau of Economic Research suggests the number is closer to 500,000.
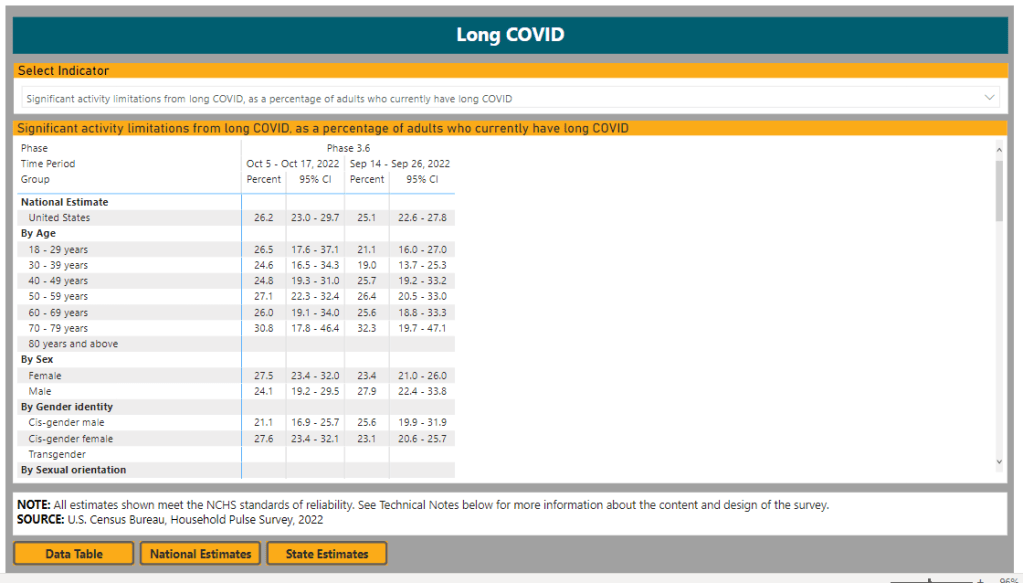
The CDC and Census’ Household Pulse Survey reports about 14% of all U.S. adults have experienced Long COVID symptoms, and about one in four adults who currently have Long COVID are experiencing “significant activity limitations” due to their symptoms. But the Social Security Administration itself said that it’s only identified 40,000 disability claims that “include indication of a COVID infection at some point,” in a comment for my story.
Why do these estimates vary so much? It goes back to the beginning of the pandemic, when PCR tests were not available to many people who likely had COVID-19 and early long-haulers were dismissed by their doctors. As we approach three years with COVID-19, there’s still no clear process for diagnosing Long COVID—much less a comprehensive system for identifying and tracking patients. (Many patients also might not yet identify as disabled, but will start looking for government support in the coming years, advocates pointed out to me.)
Right now, individual long-haulers lack standards or guidance for the medical paperwork they need to access programs like social security disability. And at a broader level, we lack clear estimates of how many people with Long COVID need these programs. The Household Pulse Survey has been a useful step towards such estimates in recent months, but more detailed data are needed to actually tackle the employment crisis that Long COVID presents.
Even so, we know enough to say that this is a crisis. For the story, I talked to Katie Bach, a senior fellow at the Brookings Institution and author of the report cited above. She told me that, while researchers disagree on the scale of Long COVID’s impact on employment, even the lowest estimates are reason for concern.
“Even if the bottom end of my range is overstated by 100%, we’re still losing $50 billion a year in wages,” she said. “I don’t think anyone who looks seriously at Long COVID would say this is not a significant problem for the U.S.”
This week, MuckRock (the public records and investigative nonprofit where I work part-time) launched a new project looking at the U.S. government’s response to the Long COVID crisis. I’m hoping that the project will build on previous work that I’ve done in this area, connecting the dots between different aspects of the crisis—with a focus on government accountability.
As a first step for the project, we’ve put together an AirTable form where Long COVID patients, advocates, caregivers, researchers, and others connected to this condition can share their experiences and story tips. If you’re part of the Long COVID community, please consider filling it out! The form is pretty short (just two required questions) and information you share won’t be used for publication without permission.
Long COVID patients and community members: I am working on a big project @MuckRock about the U.S. government's response to this crisis, and I'd like to hear from you! please consider sharing your experience in the form embedded here: https://t.co/LkQFpCRUna#LongCovid (1/4) pic.twitter.com/fa1iCF2UAe
MuckRock is also looking for other newsrooms that might want to collaborate on this project. If you’re a journalist who’s interested, please reach out to me at betsy@muckrock.com.
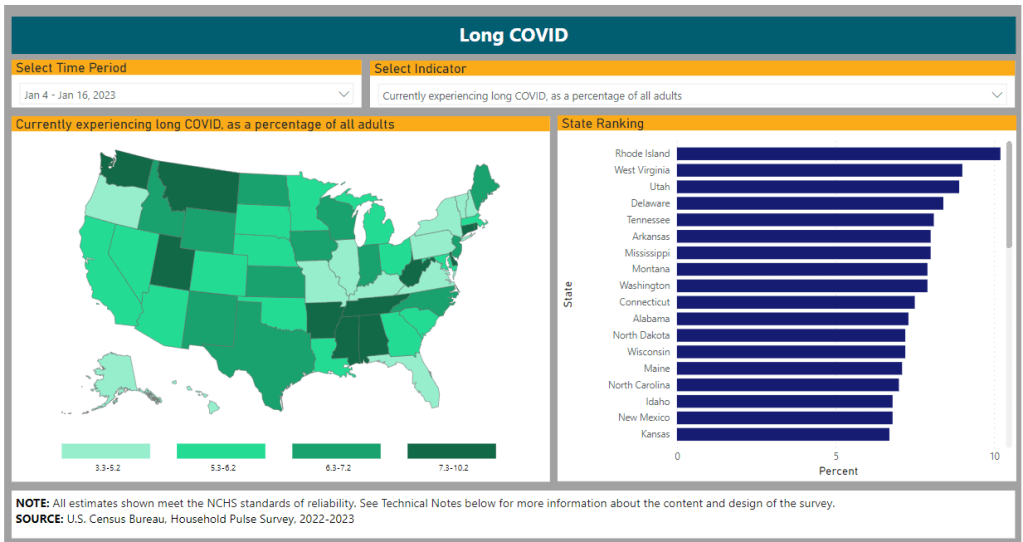
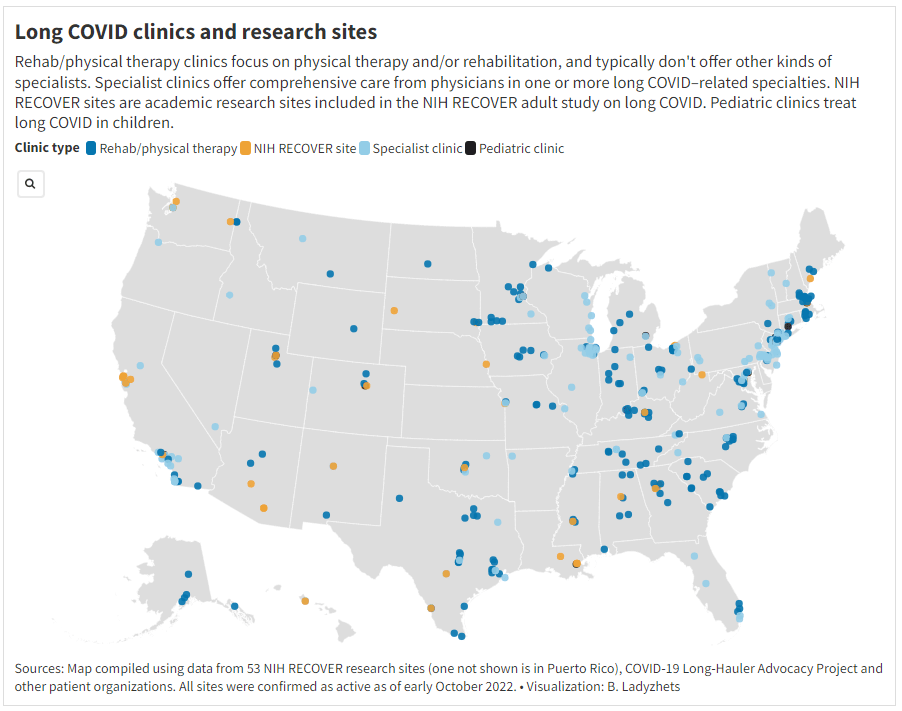
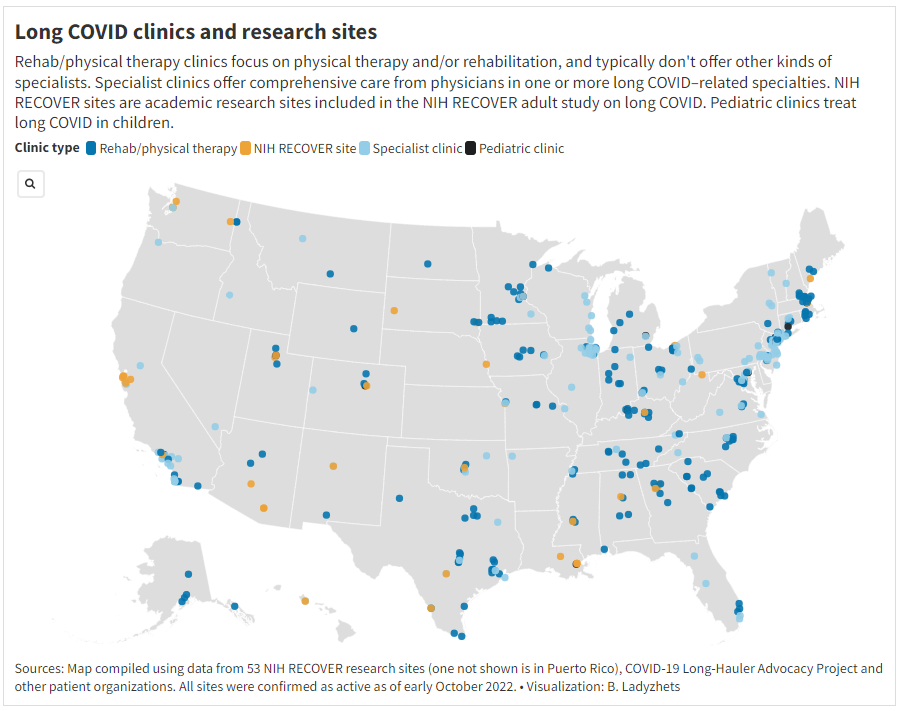
One topic that I’m hoping to dig into more is gaps in access to healthcare for Long COVID. A data project I did for Science News, published this week, shows that clinics dedicated to this condition are generally concentrated in big cities, particularly on the East coast. Yet many of the places with the highest Long COVID prevalence are rural areas in the South and Midwest, according to the Household Pulse survey.
This story shows just one small aspect of the barriers facing Long COVID patients trying to access the care they need. If you have more information to share about this issue, or anything else related to services needed for Long COVID, please consider filling out MuckRock’s callout form.