This week, MuckRock (the public records and investigative nonprofit where I work part-time) launched a new project looking at the U.S. government’s response to the Long COVID crisis. I’m hoping that the project will build on previous work that I’ve done in this area, connecting the dots between different aspects of the crisis—with a focus on government accountability.
As a first step for the project, we’ve put together an AirTable form where Long COVID patients, advocates, caregivers, researchers, and others connected to this condition can share their experiences and story tips. If you’re part of the Long COVID community, please consider filling it out! The form is pretty short (just two required questions) and information you share won’t be used for publication without permission.
Long COVID patients and community members: I am working on a big project @MuckRock about the U.S. government's response to this crisis, and I'd like to hear from you! please consider sharing your experience in the form embedded here: https://t.co/LkQFpCRUna#LongCovid (1/4) pic.twitter.com/fa1iCF2UAe
MuckRock is also looking for other newsrooms that might want to collaborate on this project. If you’re a journalist who’s interested, please reach out to me at betsy@muckrock.com.
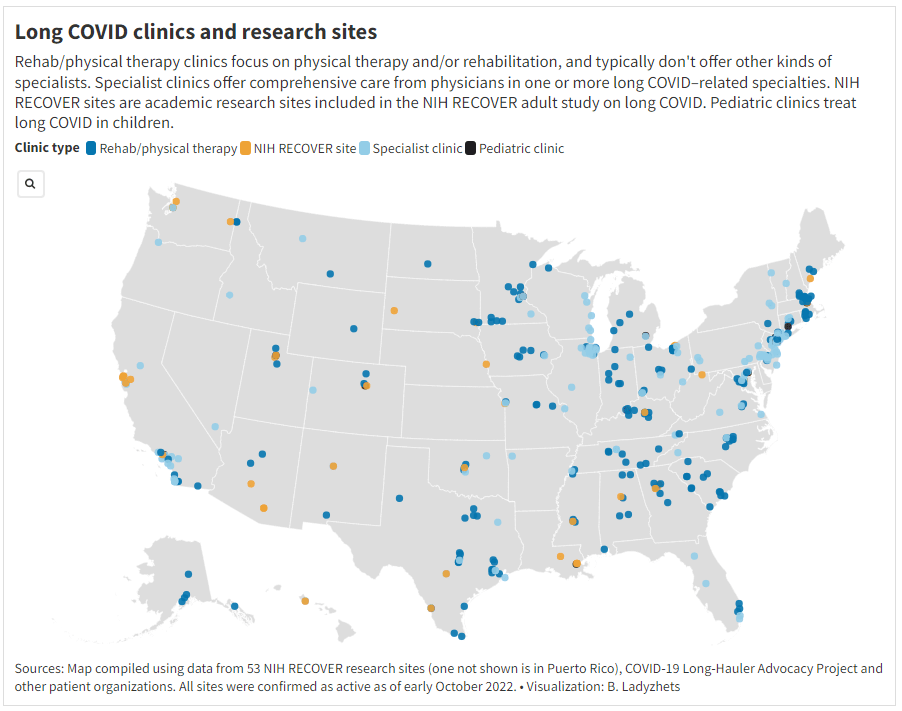
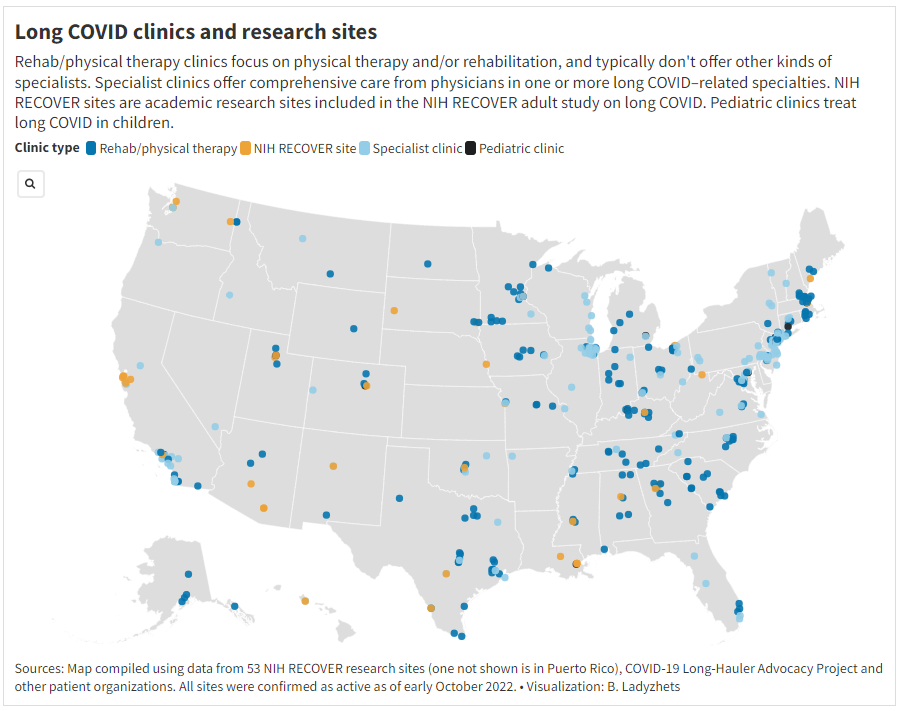
One topic that I’m hoping to dig into more is gaps in access to healthcare for Long COVID. A data project I did for Science News, published this week, shows that clinics dedicated to this condition are generally concentrated in big cities, particularly on the East coast. Yet many of the places with the highest Long COVID prevalence are rural areas in the South and Midwest, according to the Household Pulse survey.
This story shows just one small aspect of the barriers facing Long COVID patients trying to access the care they need. If you have more information to share about this issue, or anything else related to services needed for Long COVID, please consider filling out MuckRock’s callout form.
More detailed bivalent booster data: As of this week, the CDC is reporting some demographic data for the bivalent, Omicron-specific booster shots. The new data suggest that these boosters have had higher uptake among seniors, with about 11 million people over age 65 receiving a shot (compared to just 60,000 in the 5 to 11 age group). White and Asian Americans have higher booster rates than Black, Hispanic, and Native Americans, suggesting that the new doses are following a similar equity pattern to what we’ve seen with prior vaccines.
COVID-19 mortality by occupation: A new report by the CDC’s National Vital Statistics System provides a rare area of data we don’t usually get in the U.S.: occupational data. CDC researchers used mortality data from 46 states and New York City to examine risk of death by occupation. People working in protective services, accommodation and food services, and other essential jobs that couldn’t be done remotely had the highest death rates—confirming what many public health experts have suspected throughout the pandemic.
Life expectancy changes during the pandemic: A new study published in Nature, by researchers at the University of Oxford and other European institutions, estimated how life expectancy changed in 29 countries since the start of the pandemic. After a universal life expectancy decline in 2020, the researchers found, some western European countries “bounced back” in 2021 while the U.S. and eastern European countries did not. The results show the impacts of lower vaccination uptake in the U.S., particularly among younger adults.
Disparities in Paxlovid prescriptions: Another CDC study that caught my attention this week was this analysis in Morbidity and Mortality Weekly Report (MMWR), describing racial and ethnic disparities in prescriptions of Paxlovid—the antiviral COVID-19 treatment which reduces risk of severe symptoms. Between April and July 2022, the researchers found, the share of COVID-19 patients over age 20 who received a Paxlovid prescription was 36% lower among Black patients than among White patients, and 30% lower among Hispanic patients. More work is needed to make Paxlovid availability more equitable.
New estimates of Long COVID prevalence: One more notable paper published this week: researchers at Massachusetts General Hospital, Harvard, and collaborators conducted an online survey of about 16,000 U.S. adults who tested positive for COVID-19 in the last two months. Of those survey respondents, 15% reported current symptoms of Long COVID. The survey found that older adults and women were more likely to report Long COVID, while those who were fully vaccinated prior to infection had a somewhat lower risk of long-term symptoms. All of these findings are in line with results from other studies, but it’s helpful to see continued validation of these known trends.
New paper outlines the CDC’s COVID-19 data failures: A new study by researchers at Johns Hopkins and Stanford, published this week in PLOS One, outlines missing and poor-quality epidemiological data that hindered the U.S.’s response to COVID-19. The researchers reviewed hundreds of reports by the CDC and other health agencies, finding that public data couldn’t answer key questions ranging from how long immune system protection lasts after an infection to which occupations and settings face the highest COVID-19 risk. (H/t Amy Maxmen.)
White House pushes for improvements to indoor air quality: This week, the White House hosted a summit event on indoor air quality while launching new resources to help building owners improve their air. The summit featured talks by government officials and leading experts, discussing why indoor air quality is important—especially in public facilities like schools—and providing recommendations. (For more details, see this Twitter thread by Jon Levy.) Biden officials are calling on building owners to participate in the “Clean Air in Buildings Challenge,” which includes bringing in more clean outdoor air and enhancing filtration. While these are important steps for health improvements, some experts would like to see the federal government go further by mandating clean air.
Voters do actually support safety measures, poll shows: New polling data from the left-wing think tank Data for Progress suggests that, contrary to popular narratives, a majority of Americans understand that COVID-19 still poses risks and support safety measures. For example, 74% of likely voters support the federal government requiring schools and workplaces to improve indoor air quality, and 70% of likely voters understand that certain groups (disabled people, seniors, etc.) remain at high risk from COVID-19.
New study demonstrates long-term risks of infection: Another notable new paper from this week: researchers in Scotland used health records and surveys to follow about 33,000 people who tested positive for COVID-19, compared to 63,000 who did not. The patients were all surveyed at six, 12, and 18 months post-infection; between the six- and 18-month surveys, about 6% of the cohort had not recovered while 42% reported only partial recovery. As one of the biggest studies to date that doesn’t rely solely on health records, this paper shows how Long COVID can be devastating long-term for patients.
Further research backs up testing out of isolation: And one more study I wanted to highlight this week: researchers at the University of California San Francisco examined how long people remained contagious after a coronavirus infection. The study included over 60,000 people who were tested at community sites in San Francisco. Five days after symptoms started, the researchers found, about 80% of patients infected during the Omicron BA.1 period were still positive on rapid tests—suggesting that, as other studies have found in the past, five days is an inadequate isolation period. Rapid testing out of isolation is the way to go.
Household Pulse Survey updates, expands Long COVID data: This week, the CDC and Census released an update of their Household Pulse Survey results on how Long COVID is impacting Americans. In addition to more recent data on Long COVID prevalence, the update includes new information on how adults with the condition find it limiting their day-to-day activities. The data shows that, out of all adults currently experiencing Long COVID symptoms, over 80% have some activity limitations and 25% have “significant” activity limitations. (For more context on this dataset, see my post from June.)
NIH shares update on RECOVER study: Speaking of Long COVID, the National Institutes of Health’s Directors Blog shared a post this week with updates on its flagship RECOVER study to learn more about the condition. Major updates include: RECOVER’s current recruitment goal is 17,000 adults and 18,000 children; the NIH recently awarded more than 40 grants to research projects examining the condition’s underlying biology; and RECOVER is utilizing electronic health records to track patients over time. While this is all valuable progress, patient advocates have expressed concerns about limited involvement by post-viral chronic illness experts in RECOVER so far.
Paxlovid is going under-utilized, study finds: A new report from the health records company Epic Research provides evidence that Paxlovid reduces severe COVID-19 outcomes: patients over age 50 who received the antiviral drug were about three times less likely to be hospitalized, compared with those who didn’t. The study also found, however, that eligible Americans aren’t taking advantage of this treatment. Out of about 570,000 people who “could have received Paxlovid” between March and August 2022, only 146,000 (about one in four) actually got prescriptions. Paxlovid needs to be better advertised and easier to access.
New COVID-19 pill added to Medicines Patent Pool: And a new COVID-19 treatment option is becoming available internationally. Shionogi, a Japanese pharmaceutical company, recently signed an agreement with the Medicines Patent Pool, an international public health organization that facilitates increased drug access in low- and middle-income countries. The agreement allows other drug companies to make Shoinogi’s antiviral COVID-19 pill, called ensitrelvir fumaric acid, which has seen some promising results in clinical trials so far. Paxlovid and Molnupiravir (Merck’s antiviral pill) are already licensed by the pool.
Patient access to electronic health records expands: This past Thursday, new federal rules took effect requiring healthcare companies to “give patients unfettered access to their full health records in digital format,” as STAT News reporter Casey Ross put it. This is a major milestone for the democratization of health data, as patient records have historically been locked in a labyrinth of private databases—though more public education is needed to help people actually take advantage of the new rules. Personally, I hope this is a first step towards more record-sharing between health institutions, which could be a key step for more comprehensive analysis in the future.
CDC adds data on new booster shots: The latest addition to the CDC’s COVID Data Tracker is the Omicron-specific, bivalent booster shots, authorized a couple of weeks ago. So far, the CDC has only provided a total count of Omicron booster recipients (4.4 million, as of September 21) and incorporated these boosters into total counts of Americans who’ve received “first” and “second boosters. A note at the top of the dashboard explains the CDC is working to provide more granular data about the new boosters as separated out from past boosters.
Evidence Commons (ASU): Researchers at Arizona State University’s College of Health Solutions have compiled this detailed dashboard of scientific publications related to COVID-19 tests, supported with funding from the Rockefeller Foundation. The dashboard incorporates information from over 3,000 papers, sorted by the type of test under study, methodology, analysis location, and more. It’s a helpful tool to sort through diagnostic details that are often buried in technical documents.
Helix announces new CDC partnership: Speaking of testing, the viral sequencing and population genomics company Helix announced this week that it has an “extended agreement” with the CDC to sequence coronavirus samples for the agency’s analysis. While Helix has been working with the CDC on variant tracking for some time, the new partnership extends this important effort: Helix (and research partners) will sequence over 3,000 coronavirus samples per week for the next year, “with the option to double the number of samples during surge moments,” according to the company’s press release.
Pathogen Genomics Centers of Excellence: The CDC has also directed new surveillance funding to five state health departments that will test out new genomics technologies and respond to infectious disease outbreaks. These five departments—Georgia, Massachusetts, Minnesota, Virginia, and Washington—are receiving $90 million over the next five years; the funding came out of $1.7 billion allocated for genomic surveillance in the American Rescue Plan. I’m glad to see this sustained funding going beyond COVID-19, though I wish more than five states were getting the money!
Long-term nervous system damage from COVID-19: Ziyad Al-Aly and his team at the Veterans Affairs St. Louis Healthcare System have published a new paper on long-term impacts from a COVID-19 infection. The study used a large dataset of electronic health records from a national VA database, including 154,000 people with COVID-19 and over five million controls. COVID-19 patients had an elevated risk of strokes, cognition and memory problems, seizures, mental health disorders, encephalitis, and more. While the VA population isn’t the best representation for the U.S. population as a whole (it skews older and male), the study still provides evidence for long-term neurological complications from COVID-19.
Long COVID estimates in Europe: And one more piece of Long COVID news for this week: the World Health Organization’s European division has produced new estimates on Long COVID for the continent. Between 10% and 20% of COVID-19 cases in Europe have led to mid- or long-term symptoms, the WHO found, impacting up to 17 million people. The study also found women are more likely to develop Long COVID.
Long COVID and ME/CFS patients protest in front of the White House, telling Biden that the pandemic is not over and demanding action on their conditions. Image courtesy of ME Action.
“The pandemic is over,” Biden said, while walking through the Detroit Auto Show with 60 Minutes correspondent Scott Pelley. “We still have a problem with COVID. We’re still doing a lot of work on it. But the pandemic is over. If you notice, nobody’s wearing masks, everybody seems to be in pretty good shape.”
Most of the debate and dissection of this interview has focused on Biden’s statement that the “pandemic is over.” Is it, actually? (Epidemiologists say no.) Does he have the authority to declare it over? (No, that’s a job for the WHO.) Was his statement just reflecting what most Americans are already thinking? (Depends on who you call “most Americans.”)
See, I think the key part of Biden’s quote here actually comes at the end: “everybody seems to be in pretty good shape.” Seems to be is doing a lot of work here. In the interview, Biden is strolling through the auto show, through groups of unmasked people looking at car exhibits.
He is not actually talking to these bystanders, asking them whether they’ve lost loved ones to COVID-19, lost work during the pandemic, or faced any lingering symptoms after catching the virus themselves. Biden also isn’t considering the people who were excluded from this auto show: the Americans who were left disabled with Long COVID, and those still taking safety precautions due to other health conditions.
Images of the auto show, like those of packed indoor restaurants or maskless stadiums, seem to suggest that, yeah, Americans no longer care about COVID-19. But there are plenty of other images that don’t make it into high-profile media settings like Biden’s interview.
Today, I invite you to consider a few of the images that Biden isn’t seeing. Here are 12 statistics showing how the COVID-19 pandemic continues to have a massive impact on Americans:
At least 400 Americans are dying with COVID-19 every day, about 47,000 deaths total between June and September 2022. Daily death data tend to be underestimates, because it can take weeks to process death certificates (and numbers are often retroactively edited up). But we can still see that hundreds of people are dying each day. As Sarah Zhang points out in The Atlantic, this is several times the threshold experts set in early 2021 for calling the pandemic at an end.
About 25,000 people are currently hospitalized with COVID-19 cases. Yes, many of the people included in this statistic probably entered the hospital for another reason, then tested positive as part of routine screening. But incidental coronavirus infections still put pressure on the hospitals caring for these patients, and can intersect with a wide variety of other health conditions, potentially causing long-term issues for patients.
About 7.6% of adults are currently experiencing some form of Long COVID, as of early August. This estimate, which I pulled from the Census and CDC’s Household Pulse Survey, rises for certain demographics: almost 10% of women, 11% of transgender adults, 11% of adults with less than a high school diploma, and 15% of adults with a disability are currently experiencing Long COVID.
Hundreds of Long COVID and ME/CFS patients protested at the White House and online on Monday. Biden’s statement coincidentally landed the night before a planned protest, in which patient-advocates called for the president to declare a national emergency around Long COVID and ME/CFS. The protest was covered in the New York Times,MedPage Today, the BMJ, and other outlets.
Long COVID and ME patients are at the White House calling for action on these conditions! Chants I've heard on the livestream include: "No treatment, no peace, we won’t ever cease," "Too sick to chant, funding now." #MillionsMissingpic.twitter.com/phJiTzgwzm
19 patients, patient-advocates, and experts testified at a New York City Council hearing about Long COVID and gender on Thursday. Long COVID patients and those with related conditions (like ME/CFS and HIV) talked about dismissals from doctors and inability to return to their pre-COVID lives. They called for more comprehensive medical care and other forms of financial and social support for patients. I covered the hearing for Gothamist/WNYC.
About 2.5 million adults were recently out of work due to a COVID-19 case, either because they were sick themselves or were caring for a sick person. Another 1.6 million adults were out of work due to concern about getting or spreading COVID-19. These statistics come from the most recent iteration of the Household Pulse Survey, conducted from July 27 to August 8, 2022.
About 2.2 million adults were recently laid off or furloughed due to the COVID-19 pandemic. Another one million had their employers go out of business due to the pandemic, and 900,000 had their employers close temporarily due to COVID-19. These data are from the same Household Pulse Survey.
Over 50 million adults experienced symptoms of anxiety for at least half the days in the last two weeks, at the time of the most recent Household Pulse Survey. Almost 40 million adults experienced symptoms of depression for at least half the days in the same two-week period.
Over 80% of Americans still support the federal government providing free COVID-19 vaccines, treatments, and tests to anyone who needs them, according to an Axios-Ipsos poll conducted in early September. A past iteration of that poll, from March 2022, found that 74% of Americans reported they were “likely to wear a mask outside the home if COVID-19 cases surge again in their area.”
About 3% of Americans, or around 12 million people, are immunocompromised and still have reason to take intense COVID-19 precautions. Immunocompromised people have been eligible for extra vaccine doses, but are still more vulnerable to both severe COVID-19 symptoms and Long COVID.
2.5 billion people worldwide still haven’t been vaccinated, according to estimates from Our World in Data. Bloomberg’s vaccine tracker estimates that, at the current pace of first doses administered, it will take another 10 months for just 75% of the global population to have received at least one COVID-19 shot. As long as COVID-19 continues to spread anywhere in the world, new variants can be a threat everywhere.
Flyer for the Long COVID and ME/CFS-led protest, happening tomorrow at the White House. Image via ME Action.
Tomorrow afternoon, patient-advocates living with Long COVID and other chronic diseases will be at the White House demanding that the federal government act urgently to address these conditions. ME Action, an advocacy group focused on myalgic encephalomyelitis or chronic fatigue syndrome (ME/CFS), is the leading organization behind the protest.
The protest’s demands include nationwide education on ME/CFS and Long COVID, education specifically for doctors in diagnosing these conditions, funding for research and potential treatments, and economic support for patients.
While the main event will take place in Washington, D.C., organizers are also encouraging people from other parts of the country to participate online. You can learn more about the event here. (I personally plan to watch and cover the protest remotely.)
Patient advocacy around Long COVID and related conditions like ME/CFS has grown mostly remotely over the last two years, so it’s a major milestone for patient groups to converge on the White House in an event like this one. For any journalists interested in covering the protest, feel free to email or DM me for background info, connections to organizers, etc!
A reminder that this protest is happening Monday in DC!! We need as many people involved as possible – please join if you’re able. Masks will be required for the event.
COVID-19’s impact on the workforce: Economists at the National Bureau of Economic Research released a new working paper this week, showing that COVID-19 has “persistently” reduced the U.S.’s labor supply. Using data from the Census’ Current Population Survey, the researchers found that workers who had to take off at least a week from work due to COVID-19 were seven percentage points less likely to still be in the labor force a year later, compared to those who didn’t miss a week. Overall, Long COVID pushed about 500,000 people out of the workforce, the paper estimates. Notably, this estimate is much lower than the analysis from the Brookings Institution published last month; the gap between these two reports suggests a need for more robust data collection on Long COVID and work.
Long COVID prevalence from a population survey: Last week, I shared a new preprint from Denis Nash and his team at the City University of New York, reporting on the results of a national survey used to determine true COVID-19 prevalence during the BA.5 surge. This week, Nash et al. shared another preprint from that same survey, focused on Long COVID. Based on the nationally-representative survey (sample size: about 3,000), the researchers estimate about 7.3% of U.S. adults are currently experiencing Long COVID symptoms—matching estimates from the Household Pulse Survey. One-quarter of those Long COVID patients surveyed reported that their day-to-day life activities were significantly impacted.
Our pre-print on "The epidemiology of long COVID in US adults two years after the start of the US SARS-CoV-2 pandemic". 7.3% of the US adult population (~18.5 million) reported having long COVID by July. What does the epidemiology look like? https://t.co/lbBIDWNe2l [thread]
Lancet COVID-19 Commission shares lessons from the pandemic: The Lancet COVID-19 Commission is an interdisciplinary group of scientists convened by the journal to study the COVID-19 crisis and make recommendations for the future. In the group’s final report, released this week, the scientists focus on “failures of international cooperation” that have contributed to unnecessary illness and deaths. Those failures include delays in acknowledging that the coronavirus spreads through the air, not enough funding for low- and middle-income countries, “the lack of timely, accurate, and systematic data,” and more.
COVID-19 archive of Dr. Fauci’s emails: The COVID-19 Archive is a project aiming to compile digital documents tracing the early phases of the pandemic. Its prototype iteration allows users to search and sort through the early-COVID inbox of Dr. Anthony Fauci, via email records contributed by investigative reporter Jason Leopold. (MuckRock, where I work part-time, is a collaborator on the project, but I’m not personally involved with it.)
U.S. has active circulation of vaccine-derived polio: This week, the CDC and World Health Organization formally announced that the polioviruses spreading in New York state constitute active circulation of vaccine-derived polio. Most other countries that meet this WHO classification are developing nations in Africa, as well as Israel, the U.K., and Ukraine. For more on what exactly “vaccine-derived polio” means and how the disease made a comeback in the U.S., I recommend reading Maryn McKenna in WIRED.
Neurological symptoms associated with monkeypox: Here’s one study in the CDC’s Morbidity and Mortality Weekly Report that caught my eye this week: the agency has identified two cases in which monkeypox patients faced inflammation in their brains (called encephalomyelitis), leading to neurological symptoms. Both patients were hospitalized and required weeks of rehab, including use of walkers. The CDC says these symptoms are rare but worth monitoring, and is encouraging local health agencies to report any further cases.
White House plans for annual boosters: This week, Biden administration officials announced a plan for one COVID-19 shot each year, on a similar timeline to the flu shots distributed every fall. In this plan, this fall’s Omicron-specific boosters are the first iteration of annual boosters. Some scientists are skeptical about the plan, given that (as I discussed last week) we have very little data on how well the new boosters work. It could be preemptive to say just one shot each year will be enough, and the federal government should also be investing in next-generation vaccines that might better prevent infection and transmission.
Urgency of Equity Toolkit: The People’s CDC, a health advocacy organization aiming to fill gaps in COVID-19 guidance left by the official CDC, has published a toolkit focused on school safety for the fall. The presentation walks readers through why public health measures are still needed in K-12 schools and potential layers of protection, such as improved ventilation, surveillance testing, and improving pediatric vaccination rates.
Parents and caregivers lost to COVID-19: Speaking of protecting children, a new study published in JAMA Pediatrics this week estimates how many children have lost parents or caregivers during the pandemic. The researchers (an international group including experts at the World Health Organization, World Health Organization, and others) produced their estimates based on global excess mortality data—going beyond deaths officially reported as COVID-19. In total, the study estimates about 10.5 million lost parents or caregivers and 7.5 million became orphans worldwide.
True virus prevalence during the BA.5 surge: I’ve previously cited the work of Denis Nash and his team at the City University of New York; they utilized a population survey to estimate how many New Yorkers actually got COVID-19 during the city’s spring surge. This week, the team shared a new study that uses the same approach for the whole country. While their sample size was fairly small (about 3,000 people) and the study has yet to be peer-reviewed, its findings are striking: about 17% of U.S. adults surveyed were infected by the coronavirus during a two-week period from late June to early July, around the peak of the BA.5 surge.
New independent effort to study Long COVID: This week, a group of researchers, clinicians, and patients announced the Long Covid Research Initiative, a new collaborative effort to study the condition and identify potential treatments. The group has raised $15 million in private funding and aims to move more quickly than public or academic efforts that have been bogged down in bureaucracy (among other challenges). I’m excited to see what this new group finds.
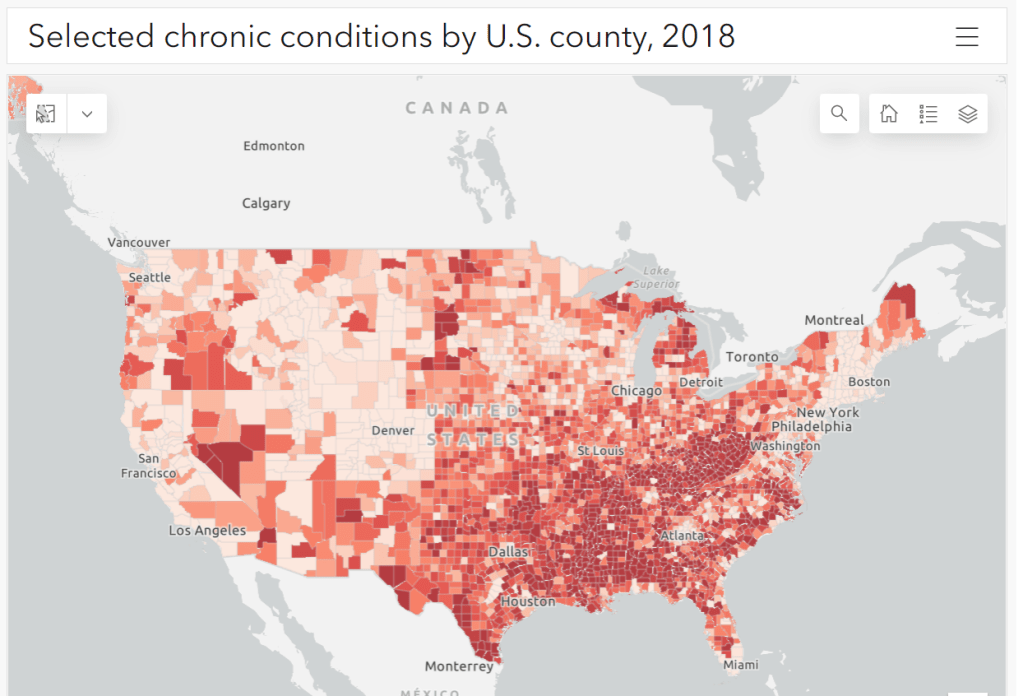
Parts of the South and Midwest have higher rates of chronic conditions (colored darker red on the map) that confer higher risk for severe COVID-19. Chart via the CDC.
The U.S. has started a new booster shot campaign, this time using vaccines designed to specifically target super-contagious subvariants Omicron BA.4 and BA.5. (For more details on the shots themselves, see last week’s post.)
Unlike previous vaccination campaigns, these boosters are available to all adults across the country who have been previously inoculated. There was no prioritization for seniors, healthcare workers, or other higher-risk adults. The official guidance from the federal government is actually pretty straightforward, for once: everyone should get the new booster. And get a flu shot soon, too, possibly even at the same time as your COVID-19 shot.
But all previously-vaccinated Americans are not facing similar levels of COVID-19 risk. Many of the same qualifications that might have warranted you an earlier dose in spring 2021 should now lead you to prioritize your Omicron booster, even if you might have been infected recently. At the same time, people who fall in these groups (or who share their households) have a good reason to continue using other safety measures after their boosters.
Here are the major qualifications for higher risk, with data to back them up:
Seniors, especially those over age 70: More than 90% of Americans over age 65 have received at least their primary vaccine series, according to the CDC, while over 70% have received at least one booster. Yet older Americans continue to have the highest rates of hospitalizations and deaths. For example, those older than 70 have consistently been hospitalized at several times the rate of younger adults (when adjusted for population). The same pattern is true for deaths among adults over age 75. Seniors who receive the new booster shots will face a lower risk of severe COVID-19 this fall and winter.
Black, Indigenous, and other Americans of color, especially seniors: Despite dedicated vaccination campaigns and other health equity efforts, Americans of color have continued to be hit harder by the pandemic than white Americans. Higher rates of chronic conditions in minority populations combined with other socioeconomic factors (POC are more likely to work essential jobs, to lack healthcare, etc.) have led to disproportionately high hospitalization and death rates. And the U.S.’s booster shot campaigns so far have been inequitable, as shown in a recent study by demography experts. Reaching these populations should be a priority for the new Omicron boosters.
Immunocompromised people: National estimates consider about 3% of Americans to be moderately or severely immunocompromised, meaning that their immune systems have limited capacity to respond to infections without medical assistance. This group includes cancer patients, organ transplant recipients, people with autoimmune diseases, and more. (This Yale Medicine article provides more information.) Immunocompromised people might have already had multiple booster shots but are still eligible to receive an Omicron booster as soon as possible, the CDC recommends.
People with Long COVID and related conditions: While there isn’t as much established data in this area, I have seen a lot of anecdotal reports from Long COVID patients who work hard to avoid new coronavirus infections—concerned about reinfection’s possibility to worsen their symptoms. On the flip side, vaccination might lead to improvement in Long COVID patients, as the shot boosts a patient’s immune system in responding to lingering reservoirs of virus. The Atlantic covered this possibility when Long COVID patients were first eligible for vaccination in early 2021, and other studies since then have backed it up. More research is needed, but at the very least, Long COVID patients receiving a new booster will have lower risk of a new severe case.
People with other preexisting health conditions: The CDC has an extensive list of medical conditions that can confer additional risk for severe COVID-19, with plenty of links to other CDC pages and medical sites where you can learn more about relevant evidence. I won’t go through them all here (that’s a topic for another week’s issue), but I do recommend checking out the CDC’s information and linked sources if you have a condition on the list. You can also explore this map of chronic condition rates by county.