GISAID, the global database of virus sequences, has faced a lot of criticism recently from the virologists and bioinformaticians who rely on it—potentially hindering responses to future virus outbreaks.
First, there was controversy around genetic information from environmental samples taken at the Huanan Seafood Wholesale Market in Wuhan, China, which Chinese researchers posted to GISAID. An outside group of scientists found the sequences and analyzed them, finding the samples supported the hypothesis that SARS-CoV-2 originated in animals and jumped to humans at the seafood market. And then, GISAID revoked those scientists’ access to the database. (The original Chinese research group eventually published their findings.)
Last week, another controversy came to light: GISAID is claiming that the first SARS-CoV-2 sequence to be publicly shared was posted on its platform, back in January 2020. Even though plenty of evidence suggests the first sequence was shared days earlier at virological.org, a virology forum. Reporting in Science Magazine and evidence shared on Twitter shows the true story of these early days of info-sharing, as well as how GISAID has tried to retroactively revise the narrative.
While these issues might seem inconsequential outside of a small circle of experts, the controversies could lead some of the world’s top virologists and epidemiologists to stop using a major source for outbreak information. It doesn’t really matter who posted a SARS-CoV-2 sequence first. But it does matter that experts have trusted places to share data and collaborate on vital research.
Without open data-sharing platforms like GISAID, the world may be less prepared for coming novel disease outbreaks. These recent controversies (and the broader debate over COVID-19’s origins) also speak to larger gaps in trust that could hinder future collaborations.
This week, I had a new article published in The Atlantic about how COVID-19 wastewater surveillance can be useful beyond entire sewersheds, the setting where this testing usually takes place. Sewershed testing is great for broad trends about large populations (like, an entire city or county), the story explains. But if you’re a public health official seeking truly actionable data to inform policies, it’s helpful to get more specific.
My story focuses on one wastewater testing setting that’s been in the news a lot lately: airplane bathrooms, from which researchers can identify new variants arriving with international travelers. But airplanes are far from the only place where specific wastewater surveillance can be valuable. Here are some of those other places, highlighting some information that I learned in reporting this story (but couldn’t fit in the final article).
K-12 schools
Early in the pandemic, colleges and universities became a hub for wastewater surveillance innovation. At campuses like Columbia University in NYC, researchers tested the sewage at individual dorms in order to determine exactly which students were getting sick—and take quick action, usually by requiring students at the infected dorm to get PCR-tested and quarantining the people who tested positive.
But the same technique can apply to schools with younger students. In late 2020, the University of California San Diego expanded its testing program to elementary schools, in an initiative called the Safer at School Early Alert System. The program started with 10 schools in the 2020-21 school year, then expanded to 26 in the 2021-22 year. Wastewater testing at specific sewershed points next to the schools led researchers to identify asymptomatic COVID-19 cases with high accuracy, program leader Rebecca Fielding-Miller told me.
The San Diego program isn’t alone: other public school systems have tried out building-level wastewater testing, usually in collaboration with nearby research groups. While the research projects tend to successfully show that wastewater surveillance can pick up infections, it’s challenging for school systems to get the funding to do these programs long-term. (Unlike universities, which are in total control of their funding, public schools need to rely on local governments).
As a consequence of these funding challenges, the San Diego program wasn’t renewed for the 2022-23 school year. “We really would have wanted to keep doing it, but funding ran out,” Fielding-Miller said.
Hospitals, other healthcare facilities
Much of the U.S.’s health strategy throughout the pandemic has focused on keeping hospitals from becoming overwhelmed—or at least helping hospitals weather COVID-19 surges. Wastewater surveillance can help accomplish this, by giving hospital administrators warnings about potential increased transmission; wastewater trends usually predict hospitalization trends by a week or more. And when wastewater surveillance is happening at hospitals themselves, these warnings can be really specific.
At NYC Health + Hospitals, the city’s public hospital system, administrators can get these warnings from wastewater testing at the system’s eleven hospitals. The surveillance program includes weekly tests for COVID-19, flu, and mpox (formerly called monkeypox), in collaboration with local researchers. The resulting data “gives us better situational awareness,” said Leopolda Silvera, a global health administrator at Health + Hospitals. If the health system notices a coming surge at one hospital, they can adjust resources accordingly—such as sending more staff to the emergency department.
The Health + Hospitals wastewater program has been running for about a year, Silvera said. At this point, it’s the only program she knows of that does building-level surveillance at hospitals. In the future, the hospital system might start testing for other pathogens and health threats like antimicrobial resistance.
Congregate facilities
Congregate facilities like nursing homes and senior living facilities can include a lot of vulnerable people who are at higher risk for severe COVID-19, all living in close quarters. As a result, this is another category of settings where it could be helpful to have building-level wastewater surveillance: facility administrators could learn quickly about upcoming surges and respond, by doing widespread PCR testing or instituting a temporary mask mandate.
The state of Maryland used to have a program doing exactly this, with a focus on correctional facilities throughout the state—particularly facilities housing the most vulnerable residents. The wastewater surveillance program ran through May 2022, at which point it “quietly ended,” according to local outlet the Maryland Daily Record. An initial $1 million in funding for wastewater testing in Maryland ran out; while the CDC National Wastewater Surveillance System picked up testing at wastewater treatment plants, no new entity was able to continue testing at the congregate living facilities.
According to the Daily Record, the building-level wastewater testing was incredibly helpful for informing COVID-19 measures at correctional facilities and helped keep cases down. I hope the Maryland program isn’t the last example we see of this testing in the U.S.
Large, communal workplaces
Early in the pandemic, some of the U.S.’s worst COVID-19 outbreaks happened at factories, particularly large food processing plants. People in these settings are often working in close quarters, easily able to infect each other—and when an outbreak happens, there are ramifications for both individual employees and the company’s business.
These large facilities could be another target for wastewater surveillance: if company administrators see a warning about rising COVID-19 from their buildings’ sewage, they could institute basic public health measures to curb the spread. Such is the strategy for some mine companies in rural Canada, which work with biotech company LuminUltra to test their wastewater. People often live and work at these sites, making them relatively closed settings for transmission.
At these locations, COVID-19 was previously “kind-of out of control, clinical testing was very reactive,” said Jordan Schmidt, director of product applications at LuminUltra. With wastewater testing, the mining companies can keep outbreaks “to a handful of people.” Fewer people get sick and there’s less interruption to business, he said.
Neighborhood-level testing
As public health agencies face lower budgets and overall lower awareness about COVID-19, some officials want to maximize their limited resources. If you only have the funding and staff for two mobile PCR testing sites this week, you’d want to make sure they go to a neighborhood where the testing would be most helpful, right?
The Boston Public Health Commission had this goal in mind when they launched a new neighborhood-level wastewater testing program, in collaboration with Biobot Analytics. The program includes testing twice a week at 11 sites across Boston, selected to provide good coverage of the city and also enable testing without too much disruption to traffic. While testing just started in January, the program is already helpful for identifying specific COVID-19 patterns, said Kathryn Hall, deputy commissioner for the health agency.
Boston’s program is focused on COVID-19 right now, but could expand to other diseases as needed, Hall said: “Now that we have the infrastructure in place, it allows us to be really be prepared and also to ask novel and interesting questions.”
Airplanes
Airplane surveillance fits into a slightly different category than the other settings I described here. When researchers test airplane wastewater, they aren’t seeking to get advanced warnings of new surges or inform public health policies. Instead, the goal is to track variants—with a focus on any new coronavirus mutations that might come into the U.S. from abroad. (Read the Atlantic story for more details on how this works!)
Other transportation hubs could be useful for tracking variants too, experts told me. This could mean large train stations, bus stations, shipping ports—any location that involves a lot of people moving from one place to another. After all, variants can evolve in the U.S. as easily as they can in other parts of the world.
Overall, the specific wastewater testing settings described here could be valuable pieces of expanding the U.S.’s overall surveillance network, along with the more-traditional sewershed testing. But all these testing sites need sustained funding to actually provide valuable data in the long run, something that could be in jeopardy as the federal public health emergency ends.
It’s the fourth year of the pandemic. I’ve written this statement in a few pitches and planning documents recently, and was struck by how it feels simultaneously unbelievable—wasn’t March 2020, like, yesterday?—and not believable enough—haven’t we been doing this pandemic thing for an eternity already?
As someone who’s been reporting on COVID-19 since the beginning, a new year is a good opportunity to parse out that feels-like-eternity. So this week, I reflected on the major trends and topics I hope to cover in 2023—both building on my work from prior years and taking it in new directions.
(Note: I actually planned to do this post last week, but then XBB.1.5 took higher priority. Hence its arrival two weeks into the new year.)
Expansions of wastewater, and other new forms of disease surveillance
As 2022 brought on the decline of large-scale PCR testing, wastewater surveillance has proven itself as a way to more accurately track COVID-19 at the population level—even as some health departments remain wary of its utility. We also saw the technology’s use for tracking monkeypox, polio, and other conditions: the WastewaterSCAN project, for example, now reports on six different diseases.
This year, I expect that wastewater researchers and public agencies will continue expanding their use of this surveillance technology. That will likely mean more diseases as well as more specific testing locations, in addition to entire sewersheds. For example, we’re already seeing wastewater testing on airplanes. I’m also interested in following other, newer methods for tracking diseases, such as air quality monitors and wearable devices.
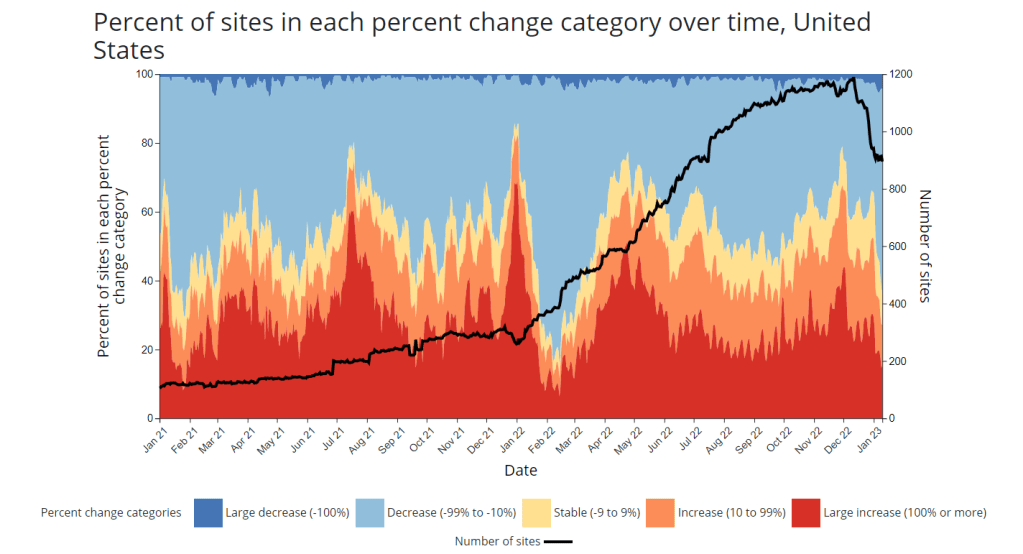
At the same time, these surveillance technologies will continue to face challenges around standardization and public buy-in. The CDC’s big contract with Biobot expires this month, and I’ve already noticed a decline in sites with recent data on the agency’s dashboard—will CDC officials and local agencies step in to fill gaps, or will wastewater testing become even more sporadic?
New variants, and how we track them
For scientists who track the coronavirus’ continued evolution, 2022 was the year of Omicron. We didn’t see all-new virus lineages sweeping the world; instead, Omicron just kept mutating, and mutating, and mutating. It seems likely that this pattern will continue in 2023, but experts need to continue watching the mutation landscape and preparing for anything truly concerning.
With declining PCR testing, public agencies and companies that track variants have fewer samples to sequence. (This led to challenges for the CDC team tracking XBB.1.5 over the holidays.) As a result, I believe 2023 will see increased creativity in how we keep an eye on these variants—whether that’s sequencing wastewater samples, taking samples directly from healthcare settings, increased focus on travel surveillance, or other methods.
Public health experts—and journalists like myself—also need to rethink how we communicate about variants. It’s no longer true that every new, somewhat-more-contagious variant warrants alarm bells: variants can take off in some countries or regions while having relatively little impact in others, thanks to differences in prior immunity, seasonality, behavior, etc. But new variants still contribute to continued reinfections, severe symptoms, Long COVID, and other impacts of COVID-19. Grid’s Jonathan Lambert recently wrote a helpful article exploring these communication challenges.
Long COVID and related chronic diseases
As regular readers likely know, Long COVID has been an increased topic of interest for me over the last two years. I’ve covered everything from disability benefits to mental health challenges, and am now leading a major project at MuckRock that will focus on government accountability for the Long COVID crisis.
Long COVID is the epidemic following the pandemic. Millions of Americans are disabled by this condition, whether they’ve been pushed out of work or are managing milder lingering symptoms. Some people are approaching their three-year anniversary of first getting sick, yet they’ve received a fraction of the government response that acute COVID-19 got. Major research projects are going in the wrong directions, while major media publications often publish articles with incorrect science.
For me, seeing poor Long COVID coverage elsewhere is great motivation to continue reporting on this topic myself, at MuckRock and other outlets. I’m also planning to spend more time reading about (and hopefully covering) other chronic diseases that are co-diagnosed with Long COVID, like ME/CFS and dysautonomia.
Ending the federal public health emergency.
Last year, we saw many state and local health agencies transition from treating COVID-19 as a health emergency to treating it as an endemic disease, like the many others that they respond to on a routine basis. This transition often accompanied changes in data reporting, such as shifts from daily to weekly COVID-19 updates.
This year, the federal government will likely do the same thing. POLITICO reported this week that the Biden administration is renewing the federal public health emergency in January, but will likely allow it to expire in the spring or summer. The Department of Health and Human Services has committed to telling state leaders about this expiration 60 days before it happens.
I previously wrote about what the end of the federal emergency could mean for COVID-19 data: changes will include less authority for the CDC, less funding for state and local health departments, and vaccines and treatments controlled by private markets rather than the federal government. I anticipate following up on this reporting when the emergency actually ends.
Transforming the U.S. public health system
Finally, I intend to follow how public health agencies learn from—or fail to learn from—the pandemic. COVID-19 exposed so many cracks in America’s public health system, from out-of-date electronic records systems to communication and trust issues. The pandemic should be a wakeup call for agencies to get their act together, before a new crisis hits.
But will that actually happen? Rachel Cohrs has a great piece in STAT this week about the challenges that systemic public health reform faces, including a lack of funding from Congress and disagreements among experts on what changes are necessary. Still, the window for change is open right now, and it may not be at this point in 2024.
XBB.1.5 caused about 28% of new cases in the week ending January 7 (confidence interval: 14% to 47%), according to the CDC’s estimates.
You’ve probably seen it in the news this week: XBB.1.5 is the latest Omicron subvariant to spread rapidly through the U.S.
It is, of course, more transmissible and more capable of evading immunity from past infections than other versions of Omicron that have gone before it, as this lineage continues mutating. Scientists are still learning about XBB.1.5; it emerged from the U.S. during the holiday season, which has posed surveillance challenges. But we know enough to say that this variant is bad news for an already overstretched healthcare system.
Here’s a brief FAQ post on XBB.1.5.
Where did XBB.1.5 come from?
XBB, the parent of this latest lineage, emerged in Asia in October 2022. It evolved from Omicron BA.2 via recombination, which basically means two different BA.2 subvariants fused—likely while the same person was infected with both—and formed this new strain. (See my variants post from October for more details on XBB.)
XBB started spreading and mutating in the U.S. a few weeks later, leading to XBB.1.5. This subvariant was first identified in New York State in mid-December, though it could have evolved elsewhere in the northeast (since New York has better variant surveillance than some other states). Eric Topol’s newsletter has more details about XBB evolution.
New variant to watch
XBB.1.5 really taking off in New York, where it appears to have evolved
BQ.1* in NY has been almost flat since dominance in Nov
What are XBB.1.5’s advantages compared to other variants?
It spreads faster, likely because it is more capable of evading immune system protections from past infection or vaccination than other Omicron subvariants. In the U.S., CDC data suggests that XBB.1.5 is starting to outcompete other lineages in the “Omicron variant soup” we currently have circulating.
BQ.1.1 and XBB (original) were already known to be the best-evolved subvariants in this area before XBB.1.5 came along, according to this December 2022 paper in Cell. XBB.1.5 has taken this immune escape further, as it evolved a mutation called F486P that’s tied to this property.
“It’s crazy infectious,” Paula Cannon, a virologist at the University of Southern California, told USA TODAY reporter Karen Weintraub. Cannon added that protections that have worked against other coronavirus strains for the last three years will likely be less effective against XBB.1.5 and other new variants.
What questions are scientists currently working to answer about XBB.1.5?
One major question that arises with any new subvariant is severity: will XBB.1.5 have a higher capacity to cause severe symptoms than other coronavirus lineages? (We now know, for example, that Delta was more severe compared to prior variants.)
The World Health Organization is currently working on a report about XBB.1.5’s severity, according to POLITICO. Scientists and public health officials will also study whether current COVID-19 treatments work against this subvariant. Antiviral treatments Paxlovid and Mulnopiravir likely won’t be impacted, but Omicron’s continued evolution has put a lot of restrictions on monoclonal antibodies.
Another important question will be how well our updated booster shots work against XBB.1.5. The shots used in the U.S. were primed for BA.4 and BA.5, while XBB is derived (albeit indirectly) from BA.2, so our shots are not the best match. Still, antibody neutralization studies have shown that the shots provide protection against XBB, meaning some impact on XBB.1.5 is likely. This is a great time to get your booster if you haven’t yet.
What impact is XBB.1.5 currently having in the U.S.?
The subvariant caused about 28% of new cases in the week ending January 7, according to CDC estimates. These estimates have a fairly wide confidence interval, though, meaning that XBB.1.5’s true prevalence could be between 14% and 47%; the CDC will improve these estimates in the coming weeks as it collects more XBB.1.5 samples.
But we know with more confidence that XBB.1.5 has already taken over in the Northeast. It’s causing the vast majority of cases in HHS Region 1 (New England) and Region 2 (New York and New Jersey). Other mid-Atlantic states are catching up.
Some experts have noted that New York and other Northeast states are currently reporting rising COVID-19 hospitalizations, which could be a sign that XBB.1.5 causes more severe disease. It’s currently unclear how much the increased hospitalizations may be attributed to XBB.1.5’s presence, though, as the entire country is seeing this trend already in the wake of the holidays.
Sam Scarpino, a disease surveillance expert at Northeastern University, has a helpful Twitter thread explaining this issue. “It’s clear that XBB.1.5 is correlated [to] an increase in hospitalizations in many highly vaccinated states,” he writes. “I suspect it will hit harder in states with lower bivalent booster rates.”
1/ For those concerned about #XBB15 and hospitalizations, I think the evidence is more mixed than many are admitting.
While it's true hospitalizations are up in states like MA where XBB.1.5 is common, they are up across the entire US, even in states w/ little-to-no #XBB15! pic.twitter.com/LVrYqjn44K
Why has XBB.1.5’s prevalence been harder to pin down than other subvariants?
Many of the news articles you might have read this week about XBB.1.5 cited that the subvariant’s prevalence more than doubled in about one week, according to CDC estimates. But then the CDC’s estimates were revised down this week, suggesting that XBB.1.5 actually caused 18% of new cases in the last week of December—not 41%.
Why did the estimate change so dramatically? Well, it actually didn’t: as the CDC itself pointed out in its Weekly Review newsletter this Friday, the 41% estimate had a big confidence interval (23% to 61%), so the revision down to 18% was not far outside the existing realm of possibility. The CDC revises its variant estimates constantly as new data come in; this might be a bigger shift than we’re used to seeing, but it’s still pretty unsurprising.
The CDC’s variant forecasting team is also facing a couple of challenges unique to XBB.1.5 right now. First, this is a homegrown, U.S.-derived variant, so they don’t have a wealth of international sequences to analyze in preparation for a U.S. surge. And second, XBB.1.5 arose during the holidays, when a lot of COVID-19 testing and sequencing organizations were taking time off. The CDC is currently working with very limited data, but it will continue to revise estimates—and make them more accurate—as more test results come in.
For more info on the CDC’s process here, I recommend this Twitter thread from epidemiologist Duncan MacCannell:
The variant surveillance dashboard on the CDC COVID Data Tracker was just updated to include projections up to 1/7/2022; this is a weekly update that posts like clockwork every Friday. https://t.co/rnE66MCoHSpic.twitter.com/WGtfHix8va
How will XBB.1.5 impact the next phase of the pandemic?
Scientists will be closely watching to see how quickly XBB.1.5 spreads in other parts of the U.S., as well as how it performs in other countries that recently had surges of other Omicron subvariants.
Overall, the data we have about this subvariant so far suggest that it’s not distinct enough from other versions of Omicron to drive a massive new surge on the level of Omicron BA.1 last winter. But it’s still arriving in the wake of holiday travel and gatherings—and in a country that has largely abandoned public health measures that stop the virus from spreading.
In New York, for example, XBB.1.5 might not be the main cause of rising hospitalizations. Yet it is undoubtedly making more people sick with COVID-19, at a time when this region also faces continued healthcare pressure from flu and RSV. And an impending nurses’ strike won’t help the situation either, to put it mildly.
I think this Twitter thread from T. Ryan Gregory, an evolutionary biology expert who tracks coronavirus variants, is helpful at putting XBB.1.5 into context. This latest lineage follows other versions of Omicron that have kept the U.S. and other countries at relatively high levels of COVID-19 transmission throughout the last year. While our current moment may not look as dire as January 2022, we are currently seeing COVID-19 go up from an already-unsustainable baseline.
“BA.1 was the highest peak,” he writes, referring to 2022 in Canada and the U.K., “but the area under the curve of the others was as bad or worse.”
That said, I don't think "not as bad as the first Omicron wave" should be the standard. As noted, Canada, the UK, etc. had their deadliest year in 2022 through multiple Omicron waves. BA.1 was the highest peak, but the area under the curve of the others was as bad or worse. pic.twitter.com/5JwU857oHo
Federal government opens up at-home test orders: The Biden administration has revived its program to mail out free COVID-19 at-home rapid tests, just in time for the holidays. Every household can now order four more tests. This feels pretty minimal (and late in the season) for a surge already overwhelming hospitals, but it’s better than nothing. Also, remember to report your results from these tests to the National Institutes of Health’s new portal!
COVID-19 vaccines saved millions of lives: A new report from the Commonwealth Fund estimates the hospitalizations and deaths saved by two years of COVID-19 vaccines, in honor of the two-year anniversary of those shots first becoming available. About 80% of Americans have received at least one vaccine dose, the authors write, “with the cumulative effect of preventing more than 18 million additional hospitalizations and more than 3 million additional deaths.” The modeling data underlying this analysis are available for download.
Congressional COVID-19 subcommittee issues final report: House Democrats on the Select Subcommittee on the Coronavirus Crisis recently released their final report, a 200-page document outlining how the U.S. should prepare for the next public health emergency. The report sums up information from three years of research and hearings, including some new findings from more recent investigations. It was released in time with the Subcommittee’s final hearing last Wednesday, which also focused on preparedness. Next year, the Republican-controlled House will have new COVID-19 priorities.
Helix and CDC build multi-disease surveillance program: This week, leading viral surveillance company Helix announced that its partnership with the CDC has expanded to include sequencing other respiratory viruses, beyond COVID-19. The company will work with major health systems in Minnesota and Washington to track viral variants for the coronavirus, flu, RSV, and other pathogens—and will build infrastructure connecting that sequencing data to electronic health records. That second piece is particularly intriguing, as variant data usually aren’t connected back to health records in the U.S.
State-level wastewater surveillance expansions: The University of Minnesota is working on a process to test wastewater for the coronavirus, flu, and RSV simultaneously, according to reporting by local outlet KARE11. A team of researchers at the university’s medical school currently test wastewater from 44 sewage treatment plants in Minnesota, and is working to broaden this work with grants from the CDC and state health department. Across the country, New Hampshire’s state health department has announced that it will start publishing results of its COVID-19 wastewater testing program online in the coming weeks. The New Hampshire program includes 14 plants across the state.
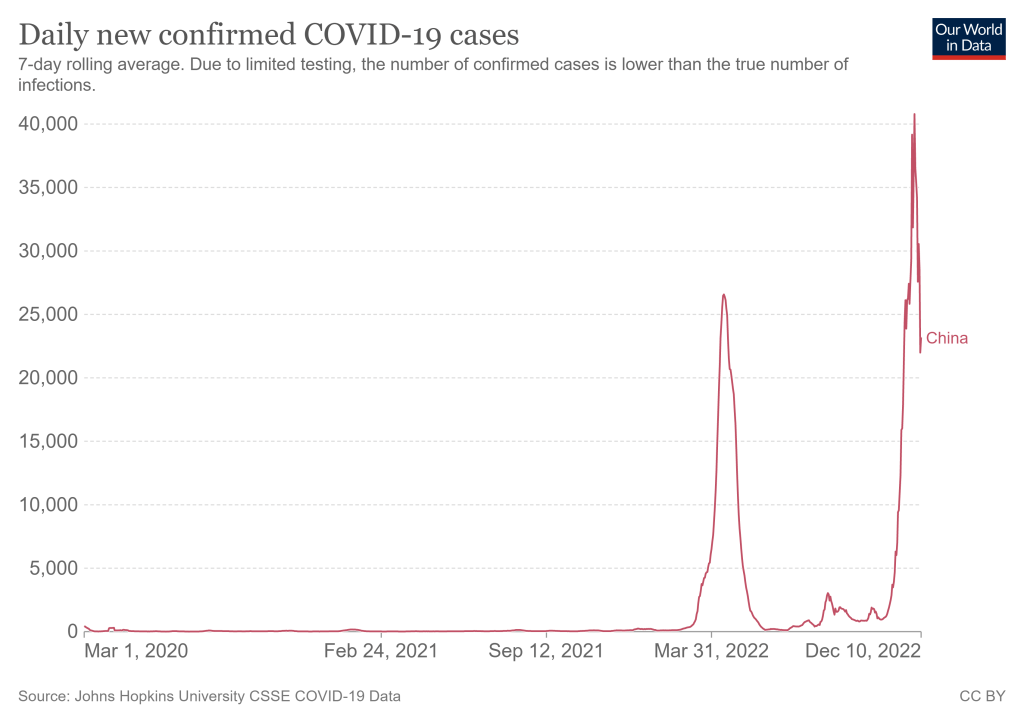
As China rolls back on COVID-19 safety measures, its rising case load is likely to shoot up further. Chart from Our World in Data.
China has rolled back some of its most rigorous COVID-19 safety policies, essentially moving away from its “zero COVID” strategy, following recent protests. I am no expert on China’s political or health policies here, but I did want to share some reflections on what this rollback could mean for global COVID-19 data, citing from Katherine Wu’s recent story in The Atlantic.
First of all, it’s important to note that we don’t have much information about coronavirus variants circulating in China. According to the global database GISAID, China has submitted a total of just 667 Omicron sequences—compared to nearly two million from the U.S. The country’s most recent sample was submitted on November 29, almost two weeks ago. Some reports, like this one in the Global Times, suggest that Omicron BF.7 is the dominant variant in Beijing, but the pattern could be different in other parts of the country.
Without more data, it’s hard to say for sure. And this is concerning because, if a new variant evolves in China as the virus spreads more widely there in the coming weeks, it could take more time for the rest of the world to learn about it than if a new variant emerged in other countries. Quick responses and international collaboration have been crucial in responses to new variants over the last two years; the global scientific community needs to be prepared to study and adapt to any new variant that might come out of China.
At the same time, China’s case data are going to become less reliable as the country reduces its clinical testing. Daily case numbers have already appeared to drop, per Our World in Data, but this could be a product of less testing for asymptomatic people (and/or data delays) rather than a surge actually turning around. I also noted that Our World in Data does not have any testing numbers for China more recent than April 2022.
China is already more limited at sharing COVID-19 data than other countries. But if case numbers become less reliable, it will get harder for international health experts to keep tabs on how bad China’s surge is getting. And it could get very bad: one modeling analysis, published in Nature in May, found that an unchecked Omicron wave in the country could lead to demand for intensive care units at 15.6 times the country’s current capacity—and 1.55 million deaths.
Based on its current healthcare system, China is not prepared for a massive national surge of severe COVID-19 cases. It’s probably even less prepared for the massive surge of Long COVID cases that could follow. This has implications for global health, economics, and more.
Even without a spike in severe disease, a wide-ranging outbreak is likely to put immense strain on China—which may weigh heavily on its economy and residents for years to come. After the SARS outbreak that began in 2002, rates of burnout and post-traumatic stress among health-care workers in affected countries swelled. Chinese citizens have not experienced an epidemic of this scale in recent memory, Chen told me. “A lot of people think it is over, that they can go back to their normal lives.” But once SARS-CoV-2 embeds itself in the country, it won’t be apt to leave. There will not be any going back to normal, not after this.
In the program—which is a collaboration between the agency’s Travelers Health Branch, biotech company Ginkgo Bioworks, and airport wellness company XpresSpa Group—travelers at four major airports can volunteer to be swabbed right after they get off the plane. The travelers’ test results are pooled by country of origin, meaning that analysts at Ginkgo combine their samples and PCR-test them together.
In addition to test positivity, Ginkgo also sequences the samples to identify variants spreading around the world. The program has included about 60,000 people between November 2021 and September 2022, according to the CDC. It’s now expanding to add more airports, with the CDC and Ginkgo working together to select international flights that should be targeted for testing.
Earlier this week, I talked to bioinformatics experts Andy Rothstein and Casandra Philipson, who work on the CDC travel surveillance program at Concentric (Ginkgo’s COVID-19 testing initiative), to learn more about how the program works. Swati Sureka from Ginkgo’s communications team also took part in the interview.
Here are a few key insights I learned from the conversation:
Travelers who volunteer to be tested don’t actually receive individual results back from Ginkgo, due to the company’s pool testing method. But they receive free at-home tests that can provide individual results.
Despite a relatively small sample size, the surveillance program tends to match global coronavirus variant trends from GISAID (a global repository of variant sequences).
The CDC uses data from this program as a complementary surveillance system, in coordination with the agency’s domestic variant surveillance, wastewater testing, and other systems.
Along with expansions to more airports, the Concentric scientists are working on testing wastewater from airplanes as another way to pull COVID-19 data from international travelers.
The experts named BQ.1 and BQ.1.1 as the most concerning variants they’re following right now, though the program has also picked up XBB.
This interview has been lightly edited and condensed for clarity.
Betsy Ladyzhets: I wanted to start by asking about the backstory behind the traveler-based genomic surveillance program. I’ve read a bit about it, but I’m curious to hear from you guys about how it got started and choices that have been made as you’ve expanded the program.
Andy Rothstein: Gingko has long recognized that biosecurity is an integral component to the growing bio-economy, even before COVID. But when spring 2020 came around, Ginko as an organization rapidly responded with a large commitment to the sequencing effort across the country… That really showed that there was an opportunity to grow a biosecurity business unit within Gingko, which became Concentric.
We built a K through 12 testing program, where we implemented this novel approach of pooled testing. We could have kindergarteners basically swabbing their noses in the classroom, everyone could put it one tube, it simplified the process, and we were able to get those results out quickly. But we really recognized that this is just one interface that can be a part of the biosecurity infrastructure.
We saw that travelers were this really important sentinel for bringing in new things like variants or tracking lineages. And we could combine the pooled testing approach with our sequencing capability at Ginkgo. Then, we got in contact with XpresSpa [now XpresCheck], which was pivoting their business model as well, because no one was going in the airports for manicures and massages. We approached them, as well as the CDC branch that deals with travel histories, quarantining, and things like that. We came to them to launch a pilot program in September 2021 as a proof of concept to say like, “Is this an interface that could provide valuable insights for public health and the CDC?”
We didn’t really know whether or not the pilot would work out. But we were one of the first to detect Omicron coming into the country in November [2021]. The program has now expanded, as of August 2022, into a two year program. And we’ve consistently been able to show that there’s real value in early warning, early detection through this novel interface.
Casandra Philipson: Gingko is an organism engineering company, we know that we’re going to be living with engineered organisms in the future. I think, because of that our founders have always had this prerogative to be able to have an early warning system or anomaly detection system for threats, whether or not they’re natural or manmade. And we have a lot of really smart people who had previous experience, in, like, Department of Defense surveillance exercises in the past. So I think there was an interest in early warning signals.
It’s also hard to be able to do surveillance in other countries, at least at that early, pandemic phase. And so this was a really easy way to have access to things that were coming in from other countries, that we otherwise wouldn’t have had access to.
BL: Yeah, that makes a lot of sense. I’m curious, building off of that, how is the CDC using the data that comes out of this program? Is it mostly about new variants? Or are there other things they’re kind of doing with it?
AR: CDC has a lot of complimentary surveillance systems ongoing, especially for SARS-CoV-2, that they’ve built up, whether it be clinical or whether it be wastewater. This is a novel interface for them to be detecting new things coming into the country. And so we really help source and, I guess, consolidate what is coming into the country and whether or not it’s a bad thing, or part of the existing evolution of SARS-CoV-2.
We work in tandem with them weekly, to not only optimize this program, but also give insights into the data that’s coming out. The [travel surveillance page of the] COVID Data Tracker has been a good culmination of all of this work that we’ve been doing. We can broadcast that publicly and show, almost side-by-side, here’s what’s happening in United States; here’s what’s happening, potentially coming into the United States.
BL: I did want to ask more about that new page on the COVID tracker, because I’m curious what you would want the average viewer to take from those charts. What should folks be getting out of both the test positivity rate and the variants?
AR: The first part is this test positivity rate. What we’ve seen is that, as testing declines in countries around the world, whether that’d be the appetite for testing or the funding for testing, we have a new sentinel to see what, potentially, the positivity looks like around the world. There’s been a number of times that we, in our program, have matched positivity rates in a country of origin [for a group of travelers]. Then as testing stopped [in that country], we still are picking up a positivity rate. For the public that is looking at this chart, it’s an opportunity to see into the window: What’s the global picture of what’s coming into this country?
Positivity is the first lens of data. The next is that we actually sequence, and we are understanding what is the breakdown or the frequencies of different variants coming into the country. You can see how what’s happening on [the CDC’s U.S. variant surveillance page] is lining up with the frequencies in our program. And because we’re finding new things, we end up sort-of being ahead of the curve in terms of what those frequencies might end up being in the United States.
BL: So you’re talking about comparing the CDC’s variant proportions estimates versus the travel estimates.
AR: Yeah, exactly. And the wastewater estimates… Not everybody is necessarily going and seeking testing when they’re sick with COVID, they might be doing an at-home test. So we’re using all of those [data systems] in a complementary sense to find, like, what’s a holistic picture of the SARS-CoV-2 coming in and outside of the United States?
BL: I also wanted to ask about, so like, if I’m a traveler coming into the U.S. at one of these airports where you have this program, how is it advertised? And what do people learn about it when they decide to volunteer to get tested?
AR: We have these pop-up testing booths, in collaboration with XpresCheck. They’re our on-the-ground infrastructure to basically be recruiting folks coming off of international flights. All the international flights go into one bottleneck where you’re going to leave the terminal, and you have an opportunity to see this booth that has some information about like, testing for public health, with the CDC logo—basically recruiting folks to come in. Folks that volunteer, they swab their noses and then we are pooling [tests] by those countries. We also have been giving them free, individual tests to take home.
We’re not collecting or giving back individual testing data to [the volunteers]. But we are showing that this is a part of the public health program. What we’ve found, through survey results, is that participation has really been increased by the fact that people feel like they’re being a part of this public health program and they want to help. We have great recruiters on the ground.
BL: So people don’t get their individual results, but you said they get an at-home test that they can use?
AR: Yeah. And then they can get their individual results [from that test]… They don’t get the pooled result.
BL: Are the data that you’re getting from this program linked to any other data? Because I know one big concern with variants is like, is a new variant going to be more severe? Is it going to be more likely for people to be hospitalized? So is there any capacity to link the tests that you’re doing with, say, hospitalization records?
AR: I think it’s a great idea, a great direction. Right now, we haven’t been linking those clinical data… We can try to look at the data within our program, and then contextualize it [using other sources] on what might be happening, in the United States or in origin countries.
But we’ve also been really excited about expanding our passive detection through wastewater. We’ve done an R&D project where we were looking at wastewater testing off of aircraft. So, that’s another complimentary data set off of the aircraft itself to help get a more holistic picture—not everyone is going to be using the bathroom [on the plane], but not everyone is going to be volunteering in this program.
BL: Testing the wastewater off the airplane seems like a great idea, I would not have thought of that.
AR: Yeah, we’re really excited about the opportunity to do something along those lines, since folks aren’t always going to volunteer to swab their nose.
We’re pooled testing by country, so we know that folks are coming from specific places. We can also—they can volunteer to give us any past travel history, so that we can try to link those data on our own. But there’s no systematic way to link [our results] to clinical data.
CP: Our sweet spot is microbes and viruses. So we actually don’t collect individual data that would allow us to associate an individual with their health record at all. I just wanted to emphasize that.
BL: That makes sense. I know that [linking datasets] is something that is very challenging to do, even with established health systems. I was just curious.
Swati Sureka: I can add one thing, just in terms of the knock-on benefits of the program. Say we do get early warning of an emerging variant that could potentially be of concern, that we don’t know on the global stage yet. We work directly with the CDC on getting them access to those [test] samples so that they can do direct viral characterization. Because, with emerging variants, it’s hard to get your hands on samples of it to be able to conduct research on how the virus behaves. I think that’s one of the side benefits, being able to actually pull those samples and share them directly with the CDC.
BL: Are there any variants that you’re all particularly watching right now? Like, I know, there’s been a lot of news about XBB, that’s spreading in East Asia. From your perspective, what are you seeing as concerning hotspots at the moment?
AR: Yeah. This is a big part of what our team does: as this data comes in, understanding what might be the trends happening globally. We have repeatedly shown that we can do early warning, [our data are] some of the first to identify a variant of concern. We can look and say, like, there’s certain mutations that we know, either from past variants or in predictive space, that [indicate this new variant is] going to be a problem for immune escape.
Variants that I think we’ve been really keeping an eye on and telling our CDC partners about are BQ.1 and BQ.1.1, which have been split out by CDC in the last couple of weeks. Our program was one of the first to identify and actually designate this BQ.1 variant. So we saw, early on, that it had characteristics because of its mutational profile [allowing it to] take hold. We continue to watch that.
The United States has been, pretty much, a few weeks to a month behind trends that we see in Western Europe. So I think it’s been pretty clear that BQ.1 is going to be something to watch for, as it sort of expands in its frequency… We also see XBB in our program, we’ve seen it as well. I think it’s going to be an interesting new chapter of SARS-CoV-2 evolution where we have potentially co-circulating variants of concern that have different dynamics in different parts of the world.
BL: Yeah, it’s very interesting… One other thing I wanted to ask you about is sample size. It seems like, from the data on the CDC dashboard, that you’re working with a small number of airports and a limited sample, compared to the number of international travelers coming into the U.S. So how do you think about analyzing that, and potentially expanding the sample?
AR: Definitely part of our plan is to ramp up the number of samples that we can get, as well as the number of airports that we might be operating out of.
But I think it’s just remarkable to talk about this program, when you see such a small sample size, and we’re still able to find new things and match GISAID, or global variant frequencies. It highlights, even with a small sample size, that the way that we’ve designed the program and the way our CDC counterparts think about where we’re going to be, what flights are we going to be choosing—that has been really, really successful so far. You always want more samples in science, but I think we’re working with what we have, and we’re excited to be expanding.
BL: That makes sense. So you’re able to say, “We want to send people to these flights, because this country has concerting variants right now,” that kind of thing?
AR: Yeah. Our CDC counterparts are tapped into both the CDC-wide conversations about variants and the global, WHO conversations about variants. So they’ll give us indications when there might be something to think about. And, again, this program is super nimble in its ability to pivot. When we think we want to focus on certain regions of the world, [we can recruit from specific flights].
It’s nice to be working in airports that have these direct flights and these long-haul flights. But thinking about how we prioritize is definitely—the CDC folks are thinking about this, and we sort-of help support them.
BL: The last main thing I wanted to ask about is, obviously in the U.S. and globally, we’re seeing so much less PCR testing now than we had at earlier points in the pandemic. How are you and—to any extent that you can talk about it—how are partners at the CDC thinking about making sure that we’re collecting a lot of samples from diverse settings, and looking in different places, looking at wastewater, and just continuing to keep track of what variants are circulating?
AR: I think back to, finding novel places to sample things. Like, the fact that we’ve invested and tried to build capability to do aircraft wastewater testing is just adding a complementary [data layer]. We’re going to have this layered interface or layered system where we might have some PCR tests, we might have wastewater, we might have sequencing, we might not have sequencing.
We’re figuring out, how do we just keep adding and keep building on this biosecurity infrastructure. I mean, the worst thing that could happen from this is we build all this and then no one uses it again, until something pops up. We’re really invested in finding new and novel ways to sample and to detect, and eventually sequence if we can get more robust data, like on variants.
BL: That makes sense. I wonder to what extent it can one day be useful for other viruses, too. I know we’re in a bad flu moment right now, or at least the beginnings of maybe a more intense flu season this year. And I know experts always talk about, like, “Can we read the tea leaves from the Southern hemisphere?” So that makes me think, “Okay, could we actually sample people who are coming in? And see if they have the flu, and not just COVID?” Or other things of that nature?
CP: This is something that keeps me up at night. Without being too forward-looking, absolutely, I would say, there are some commercial products out there right now—like from Illumina, which is a massive sequencing behemoth, they’ve just released some new sequencers on their end. They have this panel of, like, 66 viruses that you can detect in one panel. I think we’re gonna see more of that from many different types of partners who are looking at surveillance.
Moving beyond SARS-CoV-2, could samples be used for that? We’ve seen lots of publications that definitely prove that’s true. I think it’s right on cue, hopefully, with where we’re all headed.
BL: Yeah, I hope so. Well, those were all my main questions. Is there anything else you all think would be important for me to know about the program?
Swati Sureka: Stepping back, seeing how this [program] has played out over the past year, I’ve just been floored by, like, tens of thousands of people who have mobilized and participated and given samples in service of public health. For me, as a person who works in the communications space, I think we often hear a lot of these narratives of like, “People aren’t gonna do anything” or take any measures that they’re not forced to do.
People are inherently self-interested in all of these narratives that we hear. And it’s been really impressive to watch the participation that we’ve seen from travelers who want to help public health and want to help stop the spread, want to help pick up new variants. I don’t want to lose that thread of things.
BL: Totally. I can just envision, if you’re coming off a long flight, you just want to get through customs and get home. Taking a few extra minutes to get swabbed is not nothing.
AR: Yeah. And you could be doing that and say, “Oh, it doesn’t matter.” But we’re consistently seeing how helpful this data is, to inform all these complementary systems for building a biosecurity infrastructure. It’s really important data as we move forward.
BL: Yeah. When folks sign up, do you give them a link to the dashboard?
AR: Now we do. Now we can, right, it’s now live. It’s been really nice to have that public-facing thing, so that folks know where their efforts are going towards.
Genomic surveillance from international travelers: A new CDC dashboard page provides data from the agency’s program sequencing COVID-19 test samples from people arriving in the U.S. on international flights, aiming to identify and track new variants. This program—a partnership between the agency, Ginkgo Bioworks, and XpresSpa Group—started during the Delta wave in 2021 with flights from India, but has since expanded to include over 1,000 volunteers a week at four major airports. The CDC’s new page reports test positivity for travelers’ samples and variants detected through sequencing.
Implications of commercializing COVID-19 vaccines, treatments, tests: Researchers at the Kaiser Family Foundation analyzed how the federal government’s decreasing support for key COVID-19 products (vaccines, treatments, and tests) could impact Americans’ access. The government’s supply of these products has been depleted through 2022, and researchers anticipate the national Public Health Emergency will end in early 2023. As a result, Americans will soon likely need to rely on commercial products, leading to major challenges for low-income and uninsured people. (I wrote more about data implications of the PHE ending here.)
Disparities in flu hospitalizations and vaccinations: Much COVID-19 coverage, including in this publication, has focused on inequitable vaccine uptake. In early 2021, more white Americans were getting vaccinated than minority groups, potentially contributing to higher rates of severe disease in those groups through the second year of the pandemic. A new CDC study in the agency’s Morbidity and Mortality Weekly Report (MMWR) finds that a similar trend has occurred for flu over the last ten years: Black, Hispanic, and Native Americans had lower flu vaccine coverage than white Americans from 2009-10 through 2021-22 seasons, and the same groups had higher flu hospitalization rates. The study suggests equitable vaccination is a problem that goes beyond the pandemic.
Vaccine coverage among healthcare workers: Another CDC MMWR study that caught my attention this week provides results from a survey of healthcare workers, conducted in spring 2022. Among about 3,700 workers who responded to the survey, about four in five reported receiving a flu shot and two in three reported receiving a COVID-19 booster (during the 2021-22 flu season). Workers with vaccine mandates at their jobs had higher coverage than these averages, while long-term care workers had lower coverage. The results indicate more effort is needed to protect healthcare workers and their patients.
HospitalFinances.org is revamped, newly available: In 2018, the Association of Health Care Journalists (AHCJ) first launched HospitalFinances.org, a database of financial information on nonprofit hospitals pulling from 990 tax forms. The site has been offline for the past year due to a hosting issue, but is now back thanks to researchers at the University of Missouri (which hosts AHCJ). While this resource isn’t specifically COVID-related, it could be useful to reporters investigating hospitals in their areas.
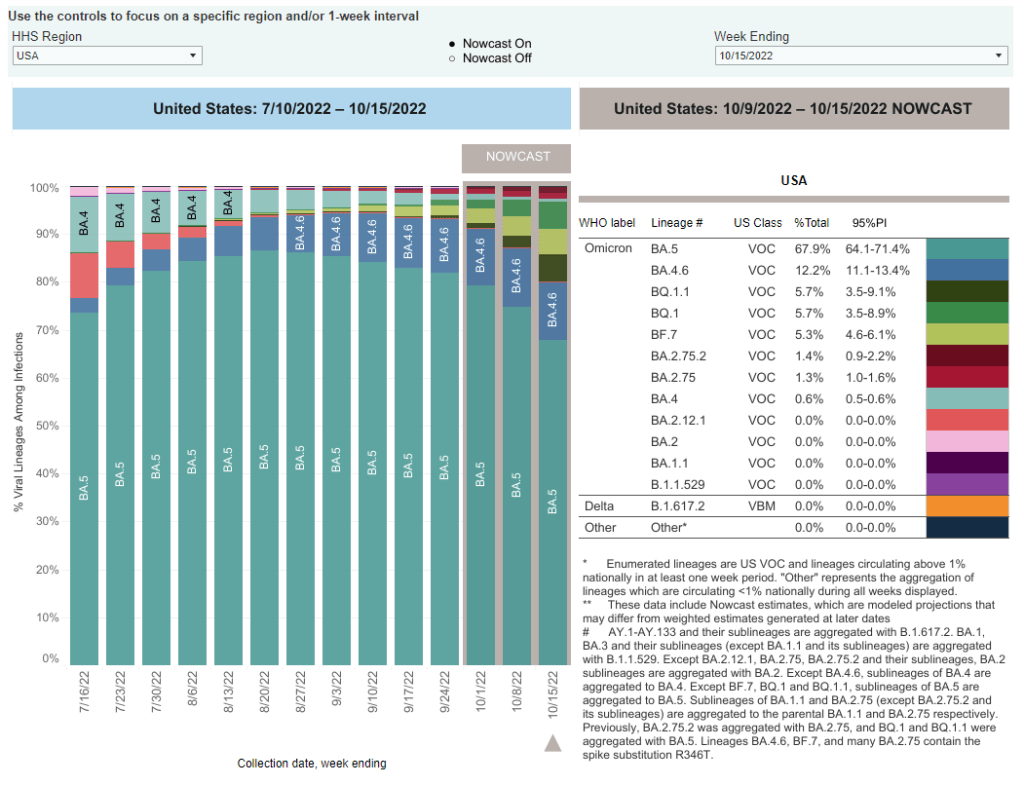
When the CDC updated its variant prevalence estimates this week, the agency added new versions of Omicron to the dashboard. In the U.S., COVID-19 cases are now driven by: BA.5, BA.4.6, BQ.1, BQ.1.1, BF.7, BA.2.75, and BA.2.75.2. And possibly more subvariants that we aren’t tracking yet.
As evolutionary biology expert T. Ryan Gregory pointed out on Twitter recently, Omicron’s evolution is “off the chart.”
Well, Omicron variant evolution is officially off the chart in terms of number of mutations. pic.twitter.com/8bVXX1n2jN
Or, to parody Smash Mouth: the Omicron variants start coming and they don’t stop coming and they don’t stop coming and they don’t stop coming…
Let’s go over the veritable alphabet soup of variants we’re dealing with right now, as well as one newer variant identified in east Asia that experts are closely watching.
BA.5, BA.4, BA.4.6
BA.5 is currently the dominant Omicron lineage in the U.S., causing about two-thirds of new COVID-19 cases in the week ending October 15. Along with BA.4, BA.5 split off from the original Omicron lineage and was first identified by South African scientists over the summer.
As these two subvariants spread around the world, it quickly became clear that they could spread faster than other versions of Omicron and reinfect people who’d previously gotten sick with those prior lineages. For more details, see this post from June. BA.5 later pulled out from BA.4 as the most competitive lineage.
BA.4.6 evolved out of BA.4. It appears to have a small advantage over BA.5, but can’t really compete with the newer subvariants we’re seeing now; according to the CDC’s estimates, it’s been causing around 10% to 12% of new cases nationwide for the last few weeks (without much growth).
BQ.1 and BQ.1.1
BQ.1 and its descendant BQ.1.1 are the two newest subvariants to show up in the CDC’s prevalence estimates, both causing about 5.7% of new cases nationwide in the last week. They actually evolved out of BA.5: BQ.1 is shorthand for a much longer, more unwieldy variant name that nobody wants to type out on Twitter.
In the U.S., BQ.1 and BQ.1.1 are starting to outcompete their parent lineage, BA.5. They’ve grown from causing less than 1% of new cases to over 10% of new cases in the last month. These subvariants are also now outcompeting other strains in the U.K. and other European countries.
As CBS News’s Alexander Tin explains, health experts are concerned that COVID-19 treatments like monoclonal antibodies might work less well against BQ.1 and BQ.1.1. We don’t have clear data on this yet, but pharmaceutical companies will test out the newer variants in the weeks to come. The Omicron bivalent boosters, at least, are expected to continue working against this lineage.
BF.7
BF.7 is another offshoot of BA.5 (again, this is shorthand for a longer name). I dedicated a post to it in late September, and the subvariant’s position hasn’t changed significantly since then: it seems to be a bit more transmissible than BA.5, but not so much that it is quickly outcompeting the parent lineage. BF.7 caused about 5% of new cases nationwide in the last week.
Similarly to BQ.1 and BQ.1.1, there are some concerns that COVID-19 treatments will be less effective against BF.7 than other versions of Omicron based on the subvariant’s spike protein mutations, but we do not have clinical data at this point.
BA.2.75 and BA.2.75.2
BA.2.75, as you might guess from the notation, evolved out of BA.2—the same original Omicron lineage that produced BA.2.12.1 and drove surges in places like New York City over the summer. It has also remained present at fairly low levels across the U.S. recently, causing just 1.3% of new cases in the last week, according to the CDC’s estimates.
But BA.2.75 now has its own offshoot, called BA.2.75.2, that appears to be a bit more competitive. The CDC recently started splitting BA.2.75.2 out of its parent lineage in its prevalence estimates, showing that it’s growing a bit faster (from 0.4% to 1.4% in the last month). Of course, this growth rate pales in comparison to what we’re seeing from the BA.5 sublineages described above.
XBB
XBB is the latest international subvariant of concern, identified this week in several east Asian countries. It has spread particularly quickly in Singapore, as described in this article by David Axe at the Daily Beast.
Like BA.2.75, XBB descended from Omicron BA.2—though it’s gone through more rounds of spike protein mutation; this is why experts are calling it XBB, rather than a long string attached to BA.2. Data so far indicate its growth advantage over BA.5 is similar to what we’re seeing from BQ.1.1. XBB has also raised concerns about treatment and vaccine efficacy, since the bivalent boosters were developed from BA.4 and BA.5.
The CDC and other health agencies have yet to identify XBB in the U.S.; experts are closely watching how this new subvariant might be able to compete with our current variations on BA.5.
BQ.1* and XBB have different geographic foci BQ.1* is mostly in Africa, Europe and North America XBB in South (East) Asia 3 countries with similar levels worth watching for comparison and potential co-circulation are: – Japan – Australia – South Koreahttps://t.co/YHzvfLgGOh 1/ pic.twitter.com/BiHKquBGxV
Overall, both in the U.S. and around the world, we’re seeing a lot of competition between these subvariants. All of them have small growth advantages over BA.5—which is currently dominant in the U.S.—but none are so different that they’re completely pulling ahead.
As I wrote last weekend, many experts are anticipating a surge this fall and winter, driven by both new subvariants and less-cautious beavior. We likely won’t see a huge spike at the level of last winter’s massive Omicron surge, but this season will still have plenty of infections (and reinfections).
We will need more data on how all these newer variants respond to vaccines and treatments, especially the antiviral Paxlovid. But it’s at least promising that many of the circulating variants right now evolved from BA.5, against which our bivalent boosters were specifically designed. It’s a great time to get that booster!
CDC adds data on new booster shots: The latest addition to the CDC’s COVID Data Tracker is the Omicron-specific, bivalent booster shots, authorized a couple of weeks ago. So far, the CDC has only provided a total count of Omicron booster recipients (4.4 million, as of September 21) and incorporated these boosters into total counts of Americans who’ve received “first” and “second boosters. A note at the top of the dashboard explains the CDC is working to provide more granular data about the new boosters as separated out from past boosters.
Evidence Commons (ASU): Researchers at Arizona State University’s College of Health Solutions have compiled this detailed dashboard of scientific publications related to COVID-19 tests, supported with funding from the Rockefeller Foundation. The dashboard incorporates information from over 3,000 papers, sorted by the type of test under study, methodology, analysis location, and more. It’s a helpful tool to sort through diagnostic details that are often buried in technical documents.
Helix announces new CDC partnership: Speaking of testing, the viral sequencing and population genomics company Helix announced this week that it has an “extended agreement” with the CDC to sequence coronavirus samples for the agency’s analysis. While Helix has been working with the CDC on variant tracking for some time, the new partnership extends this important effort: Helix (and research partners) will sequence over 3,000 coronavirus samples per week for the next year, “with the option to double the number of samples during surge moments,” according to the company’s press release.
Pathogen Genomics Centers of Excellence: The CDC has also directed new surveillance funding to five state health departments that will test out new genomics technologies and respond to infectious disease outbreaks. These five departments—Georgia, Massachusetts, Minnesota, Virginia, and Washington—are receiving $90 million over the next five years; the funding came out of $1.7 billion allocated for genomic surveillance in the American Rescue Plan. I’m glad to see this sustained funding going beyond COVID-19, though I wish more than five states were getting the money!
Long-term nervous system damage from COVID-19: Ziyad Al-Aly and his team at the Veterans Affairs St. Louis Healthcare System have published a new paper on long-term impacts from a COVID-19 infection. The study used a large dataset of electronic health records from a national VA database, including 154,000 people with COVID-19 and over five million controls. COVID-19 patients had an elevated risk of strokes, cognition and memory problems, seizures, mental health disorders, encephalitis, and more. While the VA population isn’t the best representation for the U.S. population as a whole (it skews older and male), the study still provides evidence for long-term neurological complications from COVID-19.
Long COVID estimates in Europe: And one more piece of Long COVID news for this week: the World Health Organization’s European division has produced new estimates on Long COVID for the continent. Between 10% and 20% of COVID-19 cases in Europe have led to mid- or long-term symptoms, the WHO found, impacting up to 17 million people. The study also found women are more likely to develop Long COVID.