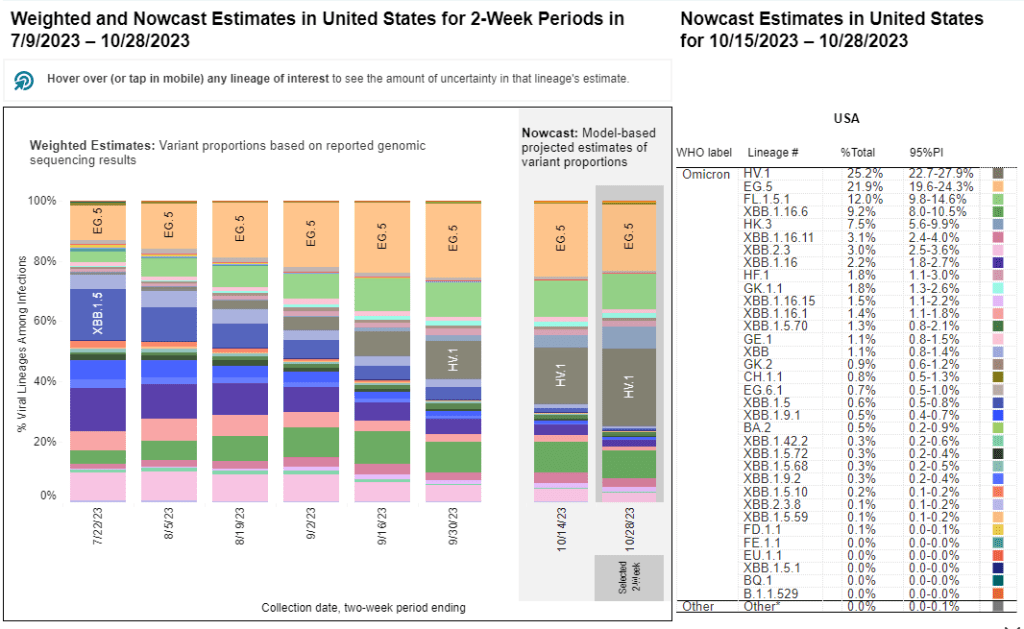
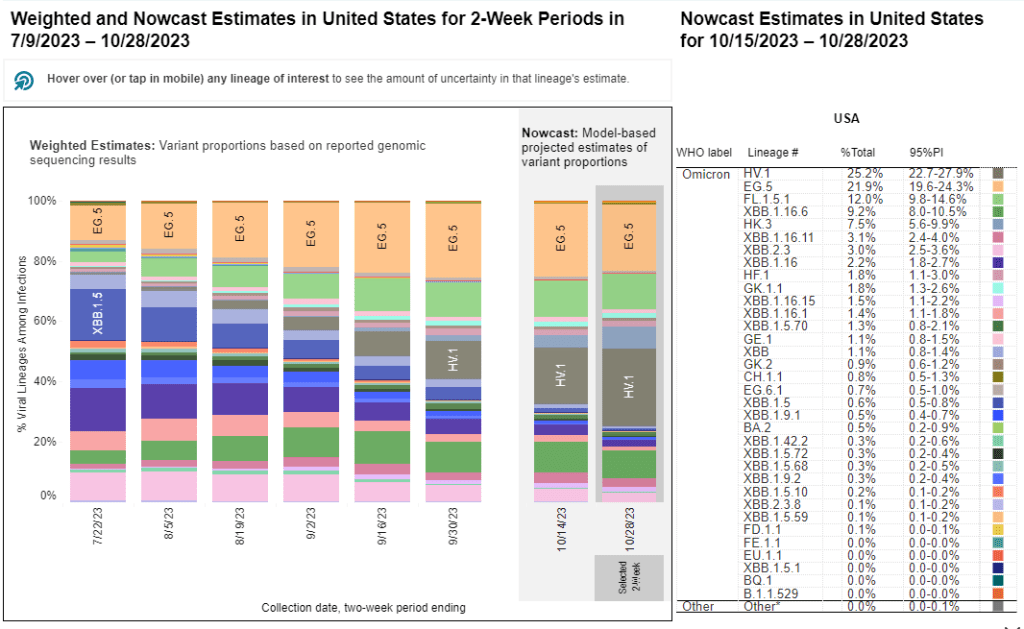
HV.1, a relative of the XBB.1.5 variant family, is the most prevalent variant in the U.S. right now, according to CDC estimates.
As winter approaches, pretty much every public health expert I follow is anticipating a COVID-19 surge. Experts anticipate that indoor gatherings and travel for the holiday season—with fewer COVID-19 precautions than we had earlier in the pandemic—will lead to more disease spread, just as these behaviors have historically contributed to more spread of flu and other common pathogens this time of year.
While it seems a surge is likely, the size and severity of that surge may depend in part on SARS-CoV-2 variants. Variants can evolve to more efficiently reinfect people who got COVID-19 recently or to evade our vaccines. These explosive variants can add fuel to the fire when people are already spending a lot of time indoors together with relatively few precautions, as we saw with the original Omicron in winter 2021-22.
As a result, experts are closely watching a few current variants that might lead to faster COVID-19 spread this winter. Here’s a review of what’s circulating right now, what to watch for in the coming weeks, and how our public health system is tracking the variants.
XBB.1.5 and relatives
Omicron XBB emerged in late 2022 when two different versions of BA.2, one of the first Omicron lineages, merged together in an evolutionary process called recombination. While the original XBB didn’t really take off globally, it started to mutate as it spread in the U.S., leading to XBB.1.5 in early 2023. See my FAQ post from January for more details.
XBB.1.5 has remained a dominant lineage in the U.S. and globally for much of this year. Scientists tracking variants have mostly identified new variants that descend from XBB.1.5, though you might not guess it from the naming schemes which often shorten names for convenience (for example, XBB.1.9.2.5 became EG.5). As a result, the FDA advised vaccine manufacturers to base their COVID-19 shots for this year on XBB.1.5.
EG.5 and FL.5.1
EG.5 and FL.5.1 are two of those XBB.1.5 relatives, descended from the XBB recombinant variant with enough evolutionary steps that virologists gave them these shorthand titles. These two variants are notable because they share a specific mutation, dubbed “FLip,” which helped the variants reinfect people more easily after prior infection or vaccination.
The CDC’s variant surveillance estimates suggest that EG.5 and FL.5.1 have been prominent—but not really dominant—variants in the U.S. this fall. In the CDC’s most recent update, the agency estimates that these variants caused 22% and 12% of cases respectively during the two weeks ending October 28. They don’t appear different enough from other XBB.1.5 relatives to really break through and cause a surge.
HV.1, descendant of EG.5
HV.1 evolved from EG.5, making it another XBB.1.5 relative. It’s the most common variant in the U.S. right now, with the CDC’s latest update estimating that it caused about one in four COVID-19 cases during the last two weeks. Like the other variants discussed above, HV.1 has a slight evolutionary advantage over its relatives; but it’s not significantly different enough to cause a huge surge right now.
There's a new COVID-19 variant predominant, @CDCgov is now estimating
HV.1, a descendant of EG.5 that's not too distantly related to those other XBB descendants
BA.2.86 got some attention when it emerged in August. This variant, unlike the others that have circulated in 2023, is not related to XBB.1.5. Instead, it takes us back in the coronavirus’ evolution, as it evolved directly from BA.2—a version of Omicron that spread widely back in early 2022. Scientists expressed concern about some worrying mutations in BA.2.86 and wondered if our vaccines, matched to XBB.1.5, might not work well against it.
Two months later, BA.2.86 hasn’t spread widely around the world as scientists worried that it might. It doesn’t appear to have a huge advantage over the XBB.1.5 descendants. While CDC surveillance has identified BA.2.86 across the U.S., it’s caused less than 1% of cases, according to the agency’s estimates.
JN.1, descendant of BA.2.86
But BA.2.86 could still indirectly cause some problems: this variant, like all the others, has been mutating. In the last couple of weeks, scientists have started to closely watch one BA.2.86 descendant called JN.1. JN.1 has picked up mutations that make it better at evading immunity from past infections or vaccinations, leading, of course, to faster spread.
JN.1 has shown up in many countries now, besides France and the UK, including the US, Iceland, Portugal, Belgium, Israel, Spain, Netherlands, Canada Germany, and Singapore. Other derivatives of BA.2.86 such as JN.2 and JN.3 are also being identified in multiple countries.
We won’t know for a few weeks as to whether JN.1 will be linked with a significant rise in COVID or how well our immune response from prior vaccinations, infection(s) and the XBB.1.5 new booster will keep us protected.
So, while BA.2.86 itself may be more benign than expected, JN.1 and its relatives are worth watching. Sequence data shared in the global repository GISAID suggest that this variant is spreading quickly globally, and may be contributing to increased spread in France in particular.
JN.1 growth is real.
New big data dump from France and other countries.
I think this solidifies things, this is quite fast. The trend in the last 4 weeks is so tight that it's messing with the confidence intervals!
As I described in my post about BA.2.86, the U.S. has a few ways of tracking variants. The CDC recently highlighted four key surveillance systems in a report about monitoring BA.2.86, published in the agency’s Morbidity and Mortality Weekly Report:
The national SARS-CoV-2 genomic surveillance program, in which the CDC and commercial partners anonymously select and sequence samples from people who had positive COVID-19 PCR tests;
The Traveler-based Genomic Surveillance program, in which international travelers returning to U.S. airports can voluntarily get PCR-tested in groups;
The National Wastewater Surveillance System, in which some public health labs sequence sewage samples that are part of the CDC’s wastewater surveillance program (with about 400 sewersheds participating in sequencing);
Digital public health surveillance, using coronavirus sequences that are shared on public, open-source platforms like GISAID.
CDC scientists use all four of these systems to keep track of variants circulating in the U.S. Sequencing wastewater samples is particularly important these days with fewer PCR tests available, I argued in a post last month.
Variants don’t happen in isolation
Sometimes, news reports about coronavirus variants cover the virus’ evolution as though it happens in isolation. Like the virus is just mutating in a vacuum, and would do so forever regardless of our human behavior.
But this isn’t accurate. The coronavirus mutates because we keep spreading it, with each infection creating an opportunity for new mutations to arise. If our public institutions really took measures to stop COVID-19 from spreading, it would also be much harder for the virus to keep evolving and evading us.
As variant expert J.P. Weiland pointed out on Twitter: “Timing is so important for impact. If it [JN.1] becomes dominant before the holidays, the wave will be quite a lot bigger than dominance in Jan.”
So, in case you need another motivator to keep up the COVID-19 precautions this holiday season: consider it doing your part to reduce viral evolution.
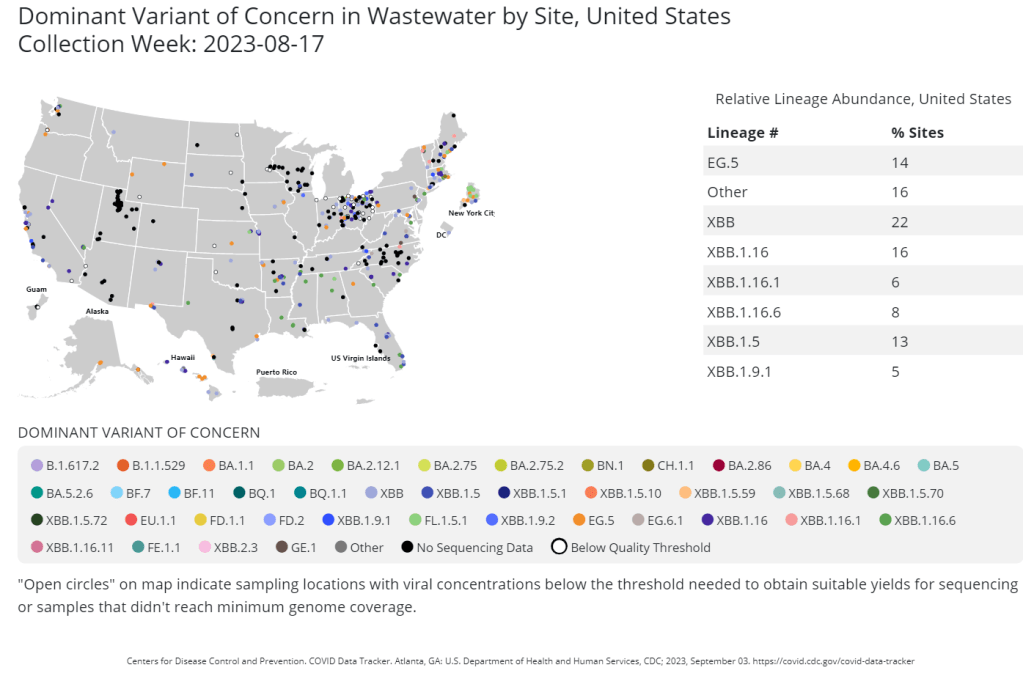
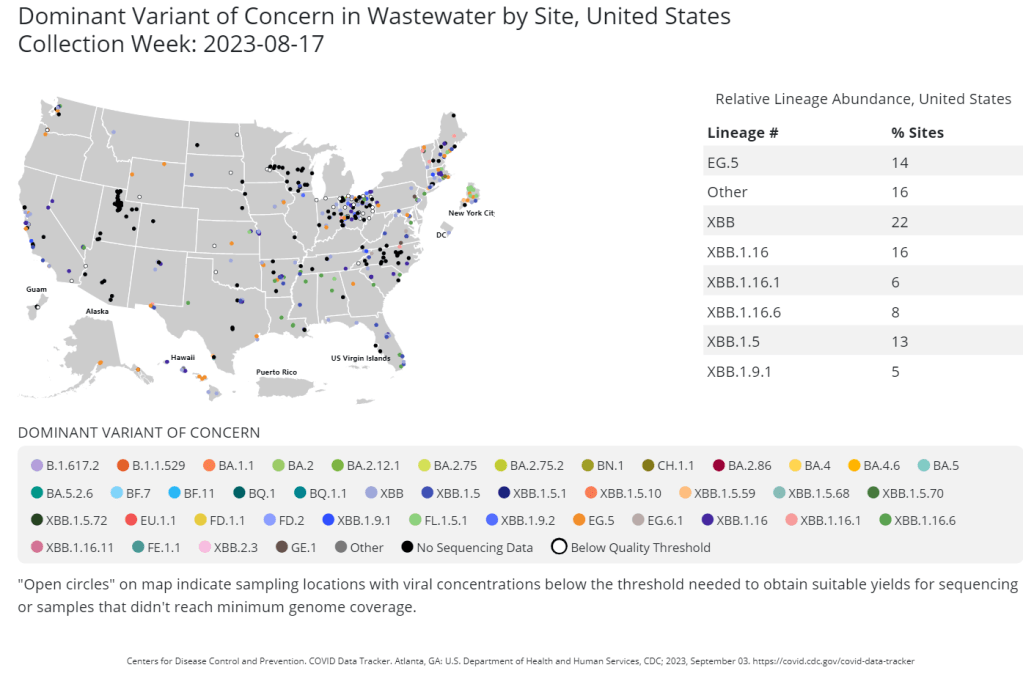
The CDC publishes data from about 400 wastewater testing sites that are sequencing their samples. Chart shows data from the week of August 17.
This week, the health department in New York City, where I live, announced that they’d identified new variant BA.2.86 in the city’s wastewater. (For more details about BA.2.86, see last week’s Q&A post.)
I covered the news for local outlet Gothamist/WNYC, and the story got me thinking about how important wastewater surveillance has become for tracking variants. With less clinical testing, sewage is now a crucial source for understanding how the coronavirus is mutating and what impacts those mutations have. But there are continued barriers to obtaining and interpreting wastewater data.
Quoting from the story:
The declaration of the end of the public health emergency in May made COVID-19 tests less available in health care settings, and sewage monitoring has since emerged as an important way to identify new variants.
“As the wastewater testing has gotten better, the patient surveillance has decreased,” [said Marc Johnson, a virologist at the University of Missouri]. Several variants have been found in sewage before cases were confirmed, he said.
Wastewater surveillance has some distinct advantages, when it comes to variant monitoring:
It covers thousands of people—the entire population of a sewershed—with one sample. In big cities like NYC, one sample can include data from more than one million residents.
Through sewage samples, scientists can look for multiple variants at once, rather than compiling data over many PCR test results. They can also track population-level trends over time.
Unlike traditional case data, wastewater data don’t rely on how many people are getting tested or where. This lack of testing bias is important, as people typically use rapid tests—which are not reported to health systems—over PCR these days (rapid tests are easier to access, PCR sites have closed following the end of the federal public health emergency, etc.).
But there are also some problems, as the NYC detection this week demonstrated:
Public health officials are still getting used to using and sharing wastewater data, as this is a relatively novel source with novel pipelines for transmitting data. While the CDC and other organizations are working to compile these data in a standardized way, it’s still a work in progress.
Discrepancies and delays can sometimes occur as a result. For example, in New York, the governor’s office put out a press release on Tuesday morning claiming that BA.2.86 hadn’t been detected in the state yet—then, just hours later, the city health department announced they’d found it. State health officials weren’t aware of the detection before the city made its public announcement, I learned for my news story.
Health officials are also still learning how to interpret and act on wastewater data. The NYC health department failed to answer my questions about in which sewershed or from which sampling date they found BA.2.86; it’s unclear if they’re using the detection to take any specific actions, besides simply warning the public that this variant is present.
As wastewater surveillance captures such broad samples, it’s difficult to tie new variant detections to clinical data, such as whether an infected person went to the hospital due to their symptoms. Officials can’t contact trace from these detections, making it hard to answer questions like whether BA.2.86 causes more severe symptoms.
The CDC’s Traveler Surveillance program, which offers free PCR tests to international travelers entering the U.S., was one of the first surveillance programs to pick up BA.2.86, pictured in dark red on the right-most bar of this chart.
Last week, I introduced you to BA.2.86, a new Omicron variant that’s garnered attention among COVID-19 experts due to its significant mutations. We’ve learned a lot about BA.2.86 since last Sunday, though there are many unanswered questions to be answered as more research is conducted.
Here’s my summary of what we know so far—and what scientists are still working to understand. Overall, this variant has some concerning properties, but more data are needed before we know what kind of impact it will have on disease transmission and severity.
Where did BA.2.86 come from?
BA.2.86 was first identified in Israel earlier this month. Scientists then picked it up in Denmark, the U.S., U.K., and several other countries across multiple continents (and in people without recent travel history), suggesting that it has been spreading under the radar for a while.
However, as I’ve noted with past variants, the country where BA.2.86 was first identified is not necessarily the country where it developed. Many countries around the world are doing fairly limited COVID-19 testing and sequencing these days, so nations like Israel and the U.S. (which have more robust surveillance, relatively speaking) are likely to catch new variants.
Why are scientists concerned about BA.2.86?
BA.2.86 worries experts because it has a number of mutations: about 30 in its spike protein, compared to BA.2, its closest relative. The spike protein is the part of the coronavirus that binds to and enters human cells, so mutations tend to accumulate here, enabling the virus to cause new infections in people who have already been infected or vaccinated.
BA.2, you might remember, was a dominant variant in early 2022, so it’s unexpected to see a descendant of this lineage pop up now. Scientists hypothesize that BA.2.86 might have evolved in a single person with a persistent infection; the virus could have multiplied and mutated over the course of several months or a year in someone originally infected with BA.2. This evolution also could have occurred in an animal population, then transferred back to humans.
Scientists have similar hypotheses about the original Omicron variant, which was also very different from circulating strains when it emerged. In fact, BA.2.86 is about as different from XBB.1.5 (a recently dominant variant globally) as Omicron BA.1 was from Delta.
Where has BA.2.86 been identified so far?
Surveillance efforts in many countries have now found BA.2.86, ranging from Thailand to South Africa. This variant is evidently already spreading globally; unlike Omicron’s initial emergence, however, we don’t have a singular country to watch for signals of how BA.2.86 may impact transmission trends.
In the U.S., researchers have found BA.2.86 in three different states:
One case in Michigan, from a person tested in early August
One traveler returning to a D.C.-area airport from Japan, their infection caught through the CDC’s travel surveillance program
Wastewater from a sewershed in Elyria, Ohio
As surveillance is currently fairly uneven across the U.S., we can likely assume that BA.2.86 is present in other states already. Continued testing in the next few weeks will provide a clearer picture of the situation.
How does BA.2.86 impact transmission and disease severity?
This is one question that we can’t answer yet, though scientists are concerned about its potential. In a risk assessment report published this past Wednesday, the CDC said that mutations present in BA.2.86 suggest that this variant may have greater capacity to “escape from existing immunity from vaccines and previous infections” when compared to recent variants.
However, this is just a hypothesis based on genomic sequences. The CDC report cautions that it’s too soon to know how transmissible BA.2.86 is or any impact it may have on symptom severity. To answer this question, scientists will need to identify more cases caused by this variant, then track their severity and spread.
Will our new booster shots work against BA.2.86?
The FDA and CDC are planning to distribute booster shots this fall, based on the XBB.1.5 variant that dominated COVID-19 spread in the U.S. this spring and earlier in the summer. As Eric Topol points out in a recent Substack post, this booster choice made sense a couple of months ago, but it’s unlikely to work well against BA.2.86 if that variant takes off.
More research is needed on this topic, of course, but the existing genomic data is concerning. Having an XBB.1.5 booster this fall, if we see a BA.2.86-driven surge, would be like having a booster based on Delta, when Omicron is spreading: better than no booster, but unlikely to provide full protection.
“The strategy of picking a spike variant for the mRNA booster at one point in time and making that at scale, going through regulatory approval, and then for it to be given 3 or more months later is far from optimal,” Topol writes. “We desperately need to pursue a variant-proof vaccine and there are over 50 candidate templates from broad neutralizing antibodies that academic labs have published over the last couple of years.”
Will current COVID-19 tests and treatments work for BA.2.86?
According to the CDC’s risk assessment, current tests should still detect BA.2.86 and treatments should work against it, based on early studies of the variant’s genomic sequences. More research (from health agencies and companies) will provide further data on any changes to test or treatment effectiveness.
Mara Aspinall points out in her testing-focused Substack that rapid tests, in particular, tend to be unaffected by variants because they test for the N protein, a different part of the coronavirus from the spike protein (which is the main area of viral evolution). However, if you’re taking a rapid test, it’s always a good idea to follow best practices for higher accuracy—testing multiple times, swabbing your throat, etc.—and get a PCR if available.
How are scientists tracking the coronavirus’ continued evolution?
BA.2.86 has arrived in an era of far less COVID-19 surveillance, compared to what we had available a year or two ago. Most people rely on rapid tests (if they test at all), which are rarely reported to the public health system and can’t be used for genomic surveillance. As a result, it might take longer to identify BA.2.86 cases even as this variant spreads more widely.
However, there are still some surveillance systems tracking the virus—and all are now attuned to BA.2.86. A couple worth highlighting in the U.S.:
Wastewater surveillance increasingly includes testing for variants. The CDC has a dashboard showing variant testing results from sewage; this is happening in about 400 sewersheds now and will likely increase in the future.
The CDC also supports a travel surveillance program at major international airports, in partnership with Concentric by Ginkgo and XpressCheck. This program caught one of the first BA.2.86 cases in the U.S. (the traveler from Japan mentioned above).
Several major testing companies and projects continue virus surveillance, via both limited PCR samples and wastewater. These include Helix, Biobot, and WastewaterSCAN.
What will BA.2.86 mean for COVID-19 spread this fall and winter?
While BA.2.86 is similar to Omicron BA.1 in its level of mutations, it’s not yet driving significant disease spread at the same level that we saw from Omicron when that variant first emerged in late 2021. All warnings at this point are tentative, based on very limited data.
It could “fizzle,” or fail to outcompete currently-circulating variants and spread widely despite its concerning array of mutations.
It could “displace” the current variants and contribute to increased transmission, but not cause a huge wave on the same level as Omicron BA.1 in late 2021.
It could cause a major wave, comparable to the initial Omicron spread.
Based on analysis from Johnson and other experts I follow, the second scenario seems most likely. But if the U.S. and other countries had meaningful public health protections in place, we could actually contribute to those odds, rather than leaving things up to evolutionary chance. Remember: variants don’t just evolve in a vacuum. We create them, by letting the virus spread.
Last week, several variant experts that I follow on Twitter (which I refuse to call by its new name, thanks) started posting about a new SARS-CoV-2 variant, first detected in Israel. They initially called it Omicron BA.X while waiting for more details to emerge about the sequence; it’s now been named BA.2.86.
Scientists and health officials are concerned about BA.2.86 because it has many mutations on its spike protein, showing significant deviation from other versions of Omicron. This variant evolved from an earlier Omicron strain (BA.2) rather than XBB, which is the primary lineage spreading across the world right now—and is the primary focus of booster development for this fall.
Here are two relevant threads with more info (the first for a more general audience, the second going into more details about mutations):
Quick summary of the "BA.X" variant that trackers are watching closely. Bear in mind, there are only a few sequences of it so far and it may not be able to compete with currently dominant variants and may not take off. But it's interesting and *potentially* concerning.
Virologists hypothesize that BA.2.86 may have evolved in someone with a chronic infection—essentially gaining more and more mutations as the same person stayed sick for many months. Similar hypotheses apply to Delta and Omicron, though it’s hard to get definitive answers without actually finding those patients.
Another reason for concern: as of today, BA.2.86 has been detected on three different continents. In addition to Israel, scientists have found it in Denmark and the U.S. Since most countries are not doing rigorous genomic surveillance these days, the cases found so far suggest that this variant is actually far more widespread; it just went undetected until now.
I’m keeping today’s post about BA.2.86 short due to the limited information we have so far. But I’d like to dive into it more next week. So, send me your questions about this variant or about genomic surveillance more broadly, and I will answer them in next Sunday’s newsletter.
New York Times COVID-19 tracker is back: After shutting down ahead of the ending federal public health emergency, the New York Times COVID-19 tracker has now resumed updates. Since the tracker is based on CDC data, case numbers and other major metrics are no longer available; but readers can find hospital admissions, deaths, and vaccinations nationally and by state, along with some local data based on hospital service areas. The NYT website doesn’t give much information about why they resumed updates—if anyone reading this can share what happened, please let me know! (And thank you to reader Robin Lloyd who flagged the renewed updates.)
CDC Director calls for more data authority: CDC Director Rochelle Walensky appeared in front of Congress this week, speaking to Republican lawmakers for a hearing about her time leading the agency before she steps down at the end of June. One notable trend from the hearing, according to reporting by Rachel Cohrs at STAT News: Walensky acknowledged that the CDC wasn’t able to collect some key COVID-19 data points, such as vaccination rates for COVID-19 patients in hospitals. Walensky called for Congress to give the CDC more authority in collecting data from state and local health departments.
CDC expanding its wastewater testing targets: Another CDC update for this week: the agency’s National Wastewater Surveillance System is expanding the pathogens that it will look for in sewage, Genome Web reports. NWSS plans to test for several respiratory viruses (COVID-19, flu, RSV), foodborne infections such as E. coli and norovirus, antimicrobial resistance genes, mpox, and other pathogens that may warrant concern. CDC scientists are working with the company GT Molecular to develop and test new assays. Other wastewater research groups are similarly developing tests to expand the health data that we get from sewage, I’ve learned in reporting for an upcoming story (which will be out later this summer).
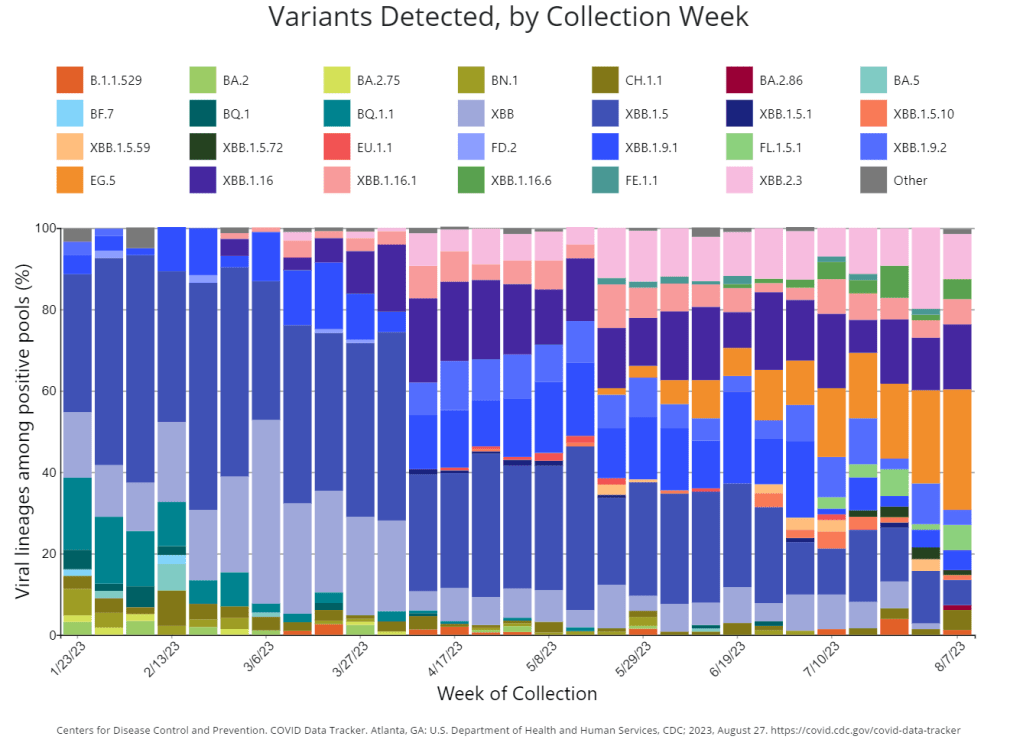
Genomic surveillance to keep tabs on Omicron’s evolution: CDC researchers invovled with tracking coronavirus variants shared some updates in a study published this week by the agency’s Morbidity and Mortality Weekly Report. As fewer people are getting PCR tests across the U.S., the CDC has access to fewer samples for sequencing than it did at prior points in the pandemic. As a result, scientists have had to update their analytical procedures for using available data to estimate how much different variants are spreading. According to the CDC, Omicron has dominated the U.S. since early 2022, with earlier BA lineages giving way to XBB.
Fungal infections increased during the pandemic: In recent years, hospital patients have become increasingly at risk of infection with fungi, which can spread widely in healthcare settings. A new paper from the CDC adds evidence to this trend: fungal infections in hospitals have increased steadily from 2019 through 2021, the researchers found. The researchers also found that patients hospitalized with COVID-19 and a fungal infection had high mortality rates, with almost half of these patients dying in 2020-2021. COVID-19 can disrupt patients’ immune systems and make them more vulnerable to fungi, the researchers suggested. This is a major threat that’s likely to continue in coming years.
Marc Johnson, a molecular virologist and wastewater surveillance expert at the University of Missouri, recently went viral on Twitter with a thread discussing his team’s investigation into a cryptic SARS-CoV-2 lineage in Ohio. I was glad to see the project get some attention, because I find Johnson’s research in this area fascinating and valuable for better understanding the links between coronavirus infection and chronic symptoms.
Ohio cryptic lineage update.
We’ve made no progress identifying the individual, but we have learned a few things. 1/ pic.twitter.com/IE2GB6CwPO
A “cryptic lineage” is a technical term for, basically, a strange viral mutation that researchers have identified in a specific location. Unlike common variants that spread through the population (Delta, Omicron, BA.5, XBB, etc.), these lineages typically are contained in one place, or even in one person. They’re usually identified by wastewater surveillance, since that technique picks up more people’s infections than testing at doctors’ offices.
Johnson has become a specialist in investigating these cryptic lineages over the last couple of years. His lab at the University of Missouri runs the state’s wastewater surveillance program, which includes genetic sequencing for sewage samples. And his team also collaborates on sequencing research for wastewater surveillance in other parts of the U.S. This Nature article from last year goes into more detail about how these investigations work.
In the last few months, Johnson and his colleagues have been investigating one cryptic lineage in Ohio. The scientists have traced the lineage to Columbus and a town called Washington Court House; they believe it represents one sick person, who lives in Columbus and goes to Washington Court House for work. This individual is shedding a massive amount of coronavirus, orders of magnitude higher than the average COVID-positive person. See more details in this story by The Columbus Dispatch.
Johnson and his colleagues would like to identify the person behind this lineage for two reasons. First, they can connect the person with doctors who can help treat their COVID-19 symptoms—it’s likely they’re having a pretty nasty gastrointestinal experience. Second, the scientists hope to better understand how viral particles that shed from a long-term infection might be related to chronic symptoms, as persistent virus in different organ systems is one of the leading hypotheses for why Long COVID occurs.
I’ve interviewed Johnson before for stories about wastewater surveillance and I think he does fascinating work, so I was glad to see his Twitter thread get some attention. If you can help identify the Ohio resident with lots of coronavirus in their gut, get in touch with him!
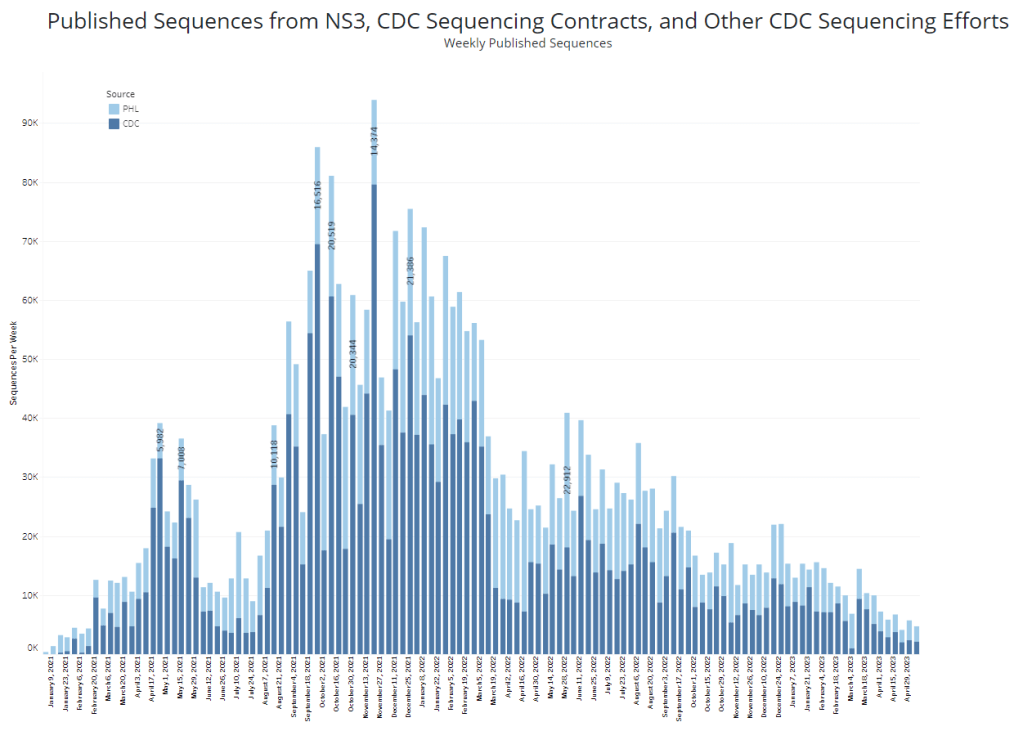
The CDC and its partners are sequencing far fewer coronavirus samples than they have at prior periods of the pandemic, making it harder to spot new variants of concern.
In the past week (April 30 through May 6), the U.S. reported about 9,500 new COVID-19 patients admitted to hospitals, according to the CDC. This amounts to:
An average of 1,400 new admissions each day
2.9 total admissions for every 100,000 Americans
7% fewer new admissions than last week (April 22-29)
Additionally, the U.S. reported:
A 14% lower concentration of SARS-CoV-2 in wastewater than last week (as of May 10, per Biobot’s dashboard)
64% of new cases are caused by Omicron XBB.1.5; 13% by XBB.1.9; 14% by XBB.1.16 (as of May 13)
An average of 70,000 vaccinations per day
COVID-19 spread continues to trend down in the U.S., though our data for tracking this disease is now worse than ever thanks to the end of the federal public health emergency. If newer Omicron variants cause a surge this summer, those increases will be hard to spot.
As a result of the PHE’s conclusion this week, the CDC is no longer collecting national case counts or testing data. Instead, the agency now recommends using hospitalization data to monitor how hard COVID-19 is hitting your community—even though this metric typically lags behind actual infection patterns—while variant data and wastewater surveillance may provide warnings about new surges.
My national updates will take a similar approach. This week, hospital admissions continue their national plateau, with a decrease of about 7% from the week ending April 29 to the week ending May 6. The CDC’s national map show that admissions are low across the country, with 99% of counties reporting fewer than 10 new admissions per 100,000 residents.
Wastewater surveillance also suggests that, while there’s still a lot of COVID-19 in the U.S., disease spread is still on a plateau or slight decline in most of the country. Biobot’s data show a minor national downturn in recent weeks; trends are similar across the four major regions, though the decline is a bit steeper on the West Coast.
The variant picture also hasn’t changed much: XBB.1.5 caused about two-thirds of new cases in the last two weeks, according to the CDC’s estimates. XBB.1.6 caused about 14% and XBB.1.9 caused 13%; these newer versions of Omicron are gaining ground, but fairly slowly. Regionally, XBB.1.6 is most prevalent in the Northeast and on the West Coast, while XBB.1.9 is most prevalent in the Midwest.
It’s worth noting, though, that the CDC has switched its variant reporting from weekly to every other week, as fewer patient specimens are going through sequencing for variant identification. The agency and its surveillance partners are sequencing around 5,000 samples every week, compared to over 80,000 a week at the height of the first Omicron surge.
Limited sequencing efforts will make it harder for the CDC to quickly identify (and respond to) new variants of concern. The same challenge is happening around the world, as PCR tests become less broadly available. Sequencing coronavirus samples from wastewater may help, but that’s only happening in a small subset of sewage testing sites right now.
One last bit of good news: vaccine administration numbers are up in the last couple of weeks, as seniors and other eligible high-risk people get their second bivalent boosters. About 70,000 people received vaccines each day this week, compared to around half that number a few weeks ago. If you’re eligible for a second booster, this is a good time to make an appointment!
GISAID, the global database of virus sequences, has faced a lot of criticism recently from the virologists and bioinformaticians who rely on it—potentially hindering responses to future virus outbreaks.
First, there was controversy around genetic information from environmental samples taken at the Huanan Seafood Wholesale Market in Wuhan, China, which Chinese researchers posted to GISAID. An outside group of scientists found the sequences and analyzed them, finding the samples supported the hypothesis that SARS-CoV-2 originated in animals and jumped to humans at the seafood market. And then, GISAID revoked those scientists’ access to the database. (The original Chinese research group eventually published their findings.)
Last week, another controversy came to light: GISAID is claiming that the first SARS-CoV-2 sequence to be publicly shared was posted on its platform, back in January 2020. Even though plenty of evidence suggests the first sequence was shared days earlier at virological.org, a virology forum. Reporting in Science Magazine and evidence shared on Twitter shows the true story of these early days of info-sharing, as well as how GISAID has tried to retroactively revise the narrative.
While these issues might seem inconsequential outside of a small circle of experts, the controversies could lead some of the world’s top virologists and epidemiologists to stop using a major source for outbreak information. It doesn’t really matter who posted a SARS-CoV-2 sequence first. But it does matter that experts have trusted places to share data and collaborate on vital research.
Without open data-sharing platforms like GISAID, the world may be less prepared for coming novel disease outbreaks. These recent controversies (and the broader debate over COVID-19’s origins) also speak to larger gaps in trust that could hinder future collaborations.
XBB.1.5 caused about 28% of new cases in the week ending January 7 (confidence interval: 14% to 47%), according to the CDC’s estimates.
You’ve probably seen it in the news this week: XBB.1.5 is the latest Omicron subvariant to spread rapidly through the U.S.
It is, of course, more transmissible and more capable of evading immunity from past infections than other versions of Omicron that have gone before it, as this lineage continues mutating. Scientists are still learning about XBB.1.5; it emerged from the U.S. during the holiday season, which has posed surveillance challenges. But we know enough to say that this variant is bad news for an already overstretched healthcare system.
Here’s a brief FAQ post on XBB.1.5.
Where did XBB.1.5 come from?
XBB, the parent of this latest lineage, emerged in Asia in October 2022. It evolved from Omicron BA.2 via recombination, which basically means two different BA.2 subvariants fused—likely while the same person was infected with both—and formed this new strain. (See my variants post from October for more details on XBB.)
XBB started spreading and mutating in the U.S. a few weeks later, leading to XBB.1.5. This subvariant was first identified in New York State in mid-December, though it could have evolved elsewhere in the northeast (since New York has better variant surveillance than some other states). Eric Topol’s newsletter has more details about XBB evolution.
New variant to watch
XBB.1.5 really taking off in New York, where it appears to have evolved
BQ.1* in NY has been almost flat since dominance in Nov
What are XBB.1.5’s advantages compared to other variants?
It spreads faster, likely because it is more capable of evading immune system protections from past infection or vaccination than other Omicron subvariants. In the U.S., CDC data suggests that XBB.1.5 is starting to outcompete other lineages in the “Omicron variant soup” we currently have circulating.
BQ.1.1 and XBB (original) were already known to be the best-evolved subvariants in this area before XBB.1.5 came along, according to this December 2022 paper in Cell. XBB.1.5 has taken this immune escape further, as it evolved a mutation called F486P that’s tied to this property.
“It’s crazy infectious,” Paula Cannon, a virologist at the University of Southern California, told USA TODAY reporter Karen Weintraub. Cannon added that protections that have worked against other coronavirus strains for the last three years will likely be less effective against XBB.1.5 and other new variants.
What questions are scientists currently working to answer about XBB.1.5?
One major question that arises with any new subvariant is severity: will XBB.1.5 have a higher capacity to cause severe symptoms than other coronavirus lineages? (We now know, for example, that Delta was more severe compared to prior variants.)
The World Health Organization is currently working on a report about XBB.1.5’s severity, according to POLITICO. Scientists and public health officials will also study whether current COVID-19 treatments work against this subvariant. Antiviral treatments Paxlovid and Mulnopiravir likely won’t be impacted, but Omicron’s continued evolution has put a lot of restrictions on monoclonal antibodies.
Another important question will be how well our updated booster shots work against XBB.1.5. The shots used in the U.S. were primed for BA.4 and BA.5, while XBB is derived (albeit indirectly) from BA.2, so our shots are not the best match. Still, antibody neutralization studies have shown that the shots provide protection against XBB, meaning some impact on XBB.1.5 is likely. This is a great time to get your booster if you haven’t yet.
What impact is XBB.1.5 currently having in the U.S.?
The subvariant caused about 28% of new cases in the week ending January 7, according to CDC estimates. These estimates have a fairly wide confidence interval, though, meaning that XBB.1.5’s true prevalence could be between 14% and 47%; the CDC will improve these estimates in the coming weeks as it collects more XBB.1.5 samples.
But we know with more confidence that XBB.1.5 has already taken over in the Northeast. It’s causing the vast majority of cases in HHS Region 1 (New England) and Region 2 (New York and New Jersey). Other mid-Atlantic states are catching up.
Some experts have noted that New York and other Northeast states are currently reporting rising COVID-19 hospitalizations, which could be a sign that XBB.1.5 causes more severe disease. It’s currently unclear how much the increased hospitalizations may be attributed to XBB.1.5’s presence, though, as the entire country is seeing this trend already in the wake of the holidays.
Sam Scarpino, a disease surveillance expert at Northeastern University, has a helpful Twitter thread explaining this issue. “It’s clear that XBB.1.5 is correlated [to] an increase in hospitalizations in many highly vaccinated states,” he writes. “I suspect it will hit harder in states with lower bivalent booster rates.”
1/ For those concerned about #XBB15 and hospitalizations, I think the evidence is more mixed than many are admitting.
While it's true hospitalizations are up in states like MA where XBB.1.5 is common, they are up across the entire US, even in states w/ little-to-no #XBB15! pic.twitter.com/LVrYqjn44K
Why has XBB.1.5’s prevalence been harder to pin down than other subvariants?
Many of the news articles you might have read this week about XBB.1.5 cited that the subvariant’s prevalence more than doubled in about one week, according to CDC estimates. But then the CDC’s estimates were revised down this week, suggesting that XBB.1.5 actually caused 18% of new cases in the last week of December—not 41%.
Why did the estimate change so dramatically? Well, it actually didn’t: as the CDC itself pointed out in its Weekly Review newsletter this Friday, the 41% estimate had a big confidence interval (23% to 61%), so the revision down to 18% was not far outside the existing realm of possibility. The CDC revises its variant estimates constantly as new data come in; this might be a bigger shift than we’re used to seeing, but it’s still pretty unsurprising.
The CDC’s variant forecasting team is also facing a couple of challenges unique to XBB.1.5 right now. First, this is a homegrown, U.S.-derived variant, so they don’t have a wealth of international sequences to analyze in preparation for a U.S. surge. And second, XBB.1.5 arose during the holidays, when a lot of COVID-19 testing and sequencing organizations were taking time off. The CDC is currently working with very limited data, but it will continue to revise estimates—and make them more accurate—as more test results come in.
For more info on the CDC’s process here, I recommend this Twitter thread from epidemiologist Duncan MacCannell:
The variant surveillance dashboard on the CDC COVID Data Tracker was just updated to include projections up to 1/7/2022; this is a weekly update that posts like clockwork every Friday. https://t.co/rnE66MCoHSpic.twitter.com/WGtfHix8va
How will XBB.1.5 impact the next phase of the pandemic?
Scientists will be closely watching to see how quickly XBB.1.5 spreads in other parts of the U.S., as well as how it performs in other countries that recently had surges of other Omicron subvariants.
Overall, the data we have about this subvariant so far suggest that it’s not distinct enough from other versions of Omicron to drive a massive new surge on the level of Omicron BA.1 last winter. But it’s still arriving in the wake of holiday travel and gatherings—and in a country that has largely abandoned public health measures that stop the virus from spreading.
In New York, for example, XBB.1.5 might not be the main cause of rising hospitalizations. Yet it is undoubtedly making more people sick with COVID-19, at a time when this region also faces continued healthcare pressure from flu and RSV. And an impending nurses’ strike won’t help the situation either, to put it mildly.
I think this Twitter thread from T. Ryan Gregory, an evolutionary biology expert who tracks coronavirus variants, is helpful at putting XBB.1.5 into context. This latest lineage follows other versions of Omicron that have kept the U.S. and other countries at relatively high levels of COVID-19 transmission throughout the last year. While our current moment may not look as dire as January 2022, we are currently seeing COVID-19 go up from an already-unsustainable baseline.
“BA.1 was the highest peak,” he writes, referring to 2022 in Canada and the U.K., “but the area under the curve of the others was as bad or worse.”
That said, I don't think "not as bad as the first Omicron wave" should be the standard. As noted, Canada, the UK, etc. had their deadliest year in 2022 through multiple Omicron waves. BA.1 was the highest peak, but the area under the curve of the others was as bad or worse. pic.twitter.com/5JwU857oHo
In the program—which is a collaboration between the agency’s Travelers Health Branch, biotech company Ginkgo Bioworks, and airport wellness company XpresSpa Group—travelers at four major airports can volunteer to be swabbed right after they get off the plane. The travelers’ test results are pooled by country of origin, meaning that analysts at Ginkgo combine their samples and PCR-test them together.
In addition to test positivity, Ginkgo also sequences the samples to identify variants spreading around the world. The program has included about 60,000 people between November 2021 and September 2022, according to the CDC. It’s now expanding to add more airports, with the CDC and Ginkgo working together to select international flights that should be targeted for testing.
Earlier this week, I talked to bioinformatics experts Andy Rothstein and Casandra Philipson, who work on the CDC travel surveillance program at Concentric (Ginkgo’s COVID-19 testing initiative), to learn more about how the program works. Swati Sureka from Ginkgo’s communications team also took part in the interview.
Here are a few key insights I learned from the conversation:
Travelers who volunteer to be tested don’t actually receive individual results back from Ginkgo, due to the company’s pool testing method. But they receive free at-home tests that can provide individual results.
Despite a relatively small sample size, the surveillance program tends to match global coronavirus variant trends from GISAID (a global repository of variant sequences).
The CDC uses data from this program as a complementary surveillance system, in coordination with the agency’s domestic variant surveillance, wastewater testing, and other systems.
Along with expansions to more airports, the Concentric scientists are working on testing wastewater from airplanes as another way to pull COVID-19 data from international travelers.
The experts named BQ.1 and BQ.1.1 as the most concerning variants they’re following right now, though the program has also picked up XBB.
This interview has been lightly edited and condensed for clarity.
Betsy Ladyzhets: I wanted to start by asking about the backstory behind the traveler-based genomic surveillance program. I’ve read a bit about it, but I’m curious to hear from you guys about how it got started and choices that have been made as you’ve expanded the program.
Andy Rothstein: Gingko has long recognized that biosecurity is an integral component to the growing bio-economy, even before COVID. But when spring 2020 came around, Ginko as an organization rapidly responded with a large commitment to the sequencing effort across the country… That really showed that there was an opportunity to grow a biosecurity business unit within Gingko, which became Concentric.
We built a K through 12 testing program, where we implemented this novel approach of pooled testing. We could have kindergarteners basically swabbing their noses in the classroom, everyone could put it one tube, it simplified the process, and we were able to get those results out quickly. But we really recognized that this is just one interface that can be a part of the biosecurity infrastructure.
We saw that travelers were this really important sentinel for bringing in new things like variants or tracking lineages. And we could combine the pooled testing approach with our sequencing capability at Ginkgo. Then, we got in contact with XpresSpa [now XpresCheck], which was pivoting their business model as well, because no one was going in the airports for manicures and massages. We approached them, as well as the CDC branch that deals with travel histories, quarantining, and things like that. We came to them to launch a pilot program in September 2021 as a proof of concept to say like, “Is this an interface that could provide valuable insights for public health and the CDC?”
We didn’t really know whether or not the pilot would work out. But we were one of the first to detect Omicron coming into the country in November [2021]. The program has now expanded, as of August 2022, into a two year program. And we’ve consistently been able to show that there’s real value in early warning, early detection through this novel interface.
Casandra Philipson: Gingko is an organism engineering company, we know that we’re going to be living with engineered organisms in the future. I think, because of that our founders have always had this prerogative to be able to have an early warning system or anomaly detection system for threats, whether or not they’re natural or manmade. And we have a lot of really smart people who had previous experience, in, like, Department of Defense surveillance exercises in the past. So I think there was an interest in early warning signals.
It’s also hard to be able to do surveillance in other countries, at least at that early, pandemic phase. And so this was a really easy way to have access to things that were coming in from other countries, that we otherwise wouldn’t have had access to.
BL: Yeah, that makes a lot of sense. I’m curious, building off of that, how is the CDC using the data that comes out of this program? Is it mostly about new variants? Or are there other things they’re kind of doing with it?
AR: CDC has a lot of complimentary surveillance systems ongoing, especially for SARS-CoV-2, that they’ve built up, whether it be clinical or whether it be wastewater. This is a novel interface for them to be detecting new things coming into the country. And so we really help source and, I guess, consolidate what is coming into the country and whether or not it’s a bad thing, or part of the existing evolution of SARS-CoV-2.
We work in tandem with them weekly, to not only optimize this program, but also give insights into the data that’s coming out. The [travel surveillance page of the] COVID Data Tracker has been a good culmination of all of this work that we’ve been doing. We can broadcast that publicly and show, almost side-by-side, here’s what’s happening in United States; here’s what’s happening, potentially coming into the United States.
BL: I did want to ask more about that new page on the COVID tracker, because I’m curious what you would want the average viewer to take from those charts. What should folks be getting out of both the test positivity rate and the variants?
AR: The first part is this test positivity rate. What we’ve seen is that, as testing declines in countries around the world, whether that’d be the appetite for testing or the funding for testing, we have a new sentinel to see what, potentially, the positivity looks like around the world. There’s been a number of times that we, in our program, have matched positivity rates in a country of origin [for a group of travelers]. Then as testing stopped [in that country], we still are picking up a positivity rate. For the public that is looking at this chart, it’s an opportunity to see into the window: What’s the global picture of what’s coming into this country?
Positivity is the first lens of data. The next is that we actually sequence, and we are understanding what is the breakdown or the frequencies of different variants coming into the country. You can see how what’s happening on [the CDC’s U.S. variant surveillance page] is lining up with the frequencies in our program. And because we’re finding new things, we end up sort-of being ahead of the curve in terms of what those frequencies might end up being in the United States.
BL: So you’re talking about comparing the CDC’s variant proportions estimates versus the travel estimates.
AR: Yeah, exactly. And the wastewater estimates… Not everybody is necessarily going and seeking testing when they’re sick with COVID, they might be doing an at-home test. So we’re using all of those [data systems] in a complementary sense to find, like, what’s a holistic picture of the SARS-CoV-2 coming in and outside of the United States?
BL: I also wanted to ask about, so like, if I’m a traveler coming into the U.S. at one of these airports where you have this program, how is it advertised? And what do people learn about it when they decide to volunteer to get tested?
AR: We have these pop-up testing booths, in collaboration with XpresCheck. They’re our on-the-ground infrastructure to basically be recruiting folks coming off of international flights. All the international flights go into one bottleneck where you’re going to leave the terminal, and you have an opportunity to see this booth that has some information about like, testing for public health, with the CDC logo—basically recruiting folks to come in. Folks that volunteer, they swab their noses and then we are pooling [tests] by those countries. We also have been giving them free, individual tests to take home.
We’re not collecting or giving back individual testing data to [the volunteers]. But we are showing that this is a part of the public health program. What we’ve found, through survey results, is that participation has really been increased by the fact that people feel like they’re being a part of this public health program and they want to help. We have great recruiters on the ground.
BL: So people don’t get their individual results, but you said they get an at-home test that they can use?
AR: Yeah. And then they can get their individual results [from that test]… They don’t get the pooled result.
BL: Are the data that you’re getting from this program linked to any other data? Because I know one big concern with variants is like, is a new variant going to be more severe? Is it going to be more likely for people to be hospitalized? So is there any capacity to link the tests that you’re doing with, say, hospitalization records?
AR: I think it’s a great idea, a great direction. Right now, we haven’t been linking those clinical data… We can try to look at the data within our program, and then contextualize it [using other sources] on what might be happening, in the United States or in origin countries.
But we’ve also been really excited about expanding our passive detection through wastewater. We’ve done an R&D project where we were looking at wastewater testing off of aircraft. So, that’s another complimentary data set off of the aircraft itself to help get a more holistic picture—not everyone is going to be using the bathroom [on the plane], but not everyone is going to be volunteering in this program.
BL: Testing the wastewater off the airplane seems like a great idea, I would not have thought of that.
AR: Yeah, we’re really excited about the opportunity to do something along those lines, since folks aren’t always going to volunteer to swab their nose.
We’re pooled testing by country, so we know that folks are coming from specific places. We can also—they can volunteer to give us any past travel history, so that we can try to link those data on our own. But there’s no systematic way to link [our results] to clinical data.
CP: Our sweet spot is microbes and viruses. So we actually don’t collect individual data that would allow us to associate an individual with their health record at all. I just wanted to emphasize that.
BL: That makes sense. I know that [linking datasets] is something that is very challenging to do, even with established health systems. I was just curious.
Swati Sureka: I can add one thing, just in terms of the knock-on benefits of the program. Say we do get early warning of an emerging variant that could potentially be of concern, that we don’t know on the global stage yet. We work directly with the CDC on getting them access to those [test] samples so that they can do direct viral characterization. Because, with emerging variants, it’s hard to get your hands on samples of it to be able to conduct research on how the virus behaves. I think that’s one of the side benefits, being able to actually pull those samples and share them directly with the CDC.
BL: Are there any variants that you’re all particularly watching right now? Like, I know, there’s been a lot of news about XBB, that’s spreading in East Asia. From your perspective, what are you seeing as concerning hotspots at the moment?
AR: Yeah. This is a big part of what our team does: as this data comes in, understanding what might be the trends happening globally. We have repeatedly shown that we can do early warning, [our data are] some of the first to identify a variant of concern. We can look and say, like, there’s certain mutations that we know, either from past variants or in predictive space, that [indicate this new variant is] going to be a problem for immune escape.
Variants that I think we’ve been really keeping an eye on and telling our CDC partners about are BQ.1 and BQ.1.1, which have been split out by CDC in the last couple of weeks. Our program was one of the first to identify and actually designate this BQ.1 variant. So we saw, early on, that it had characteristics because of its mutational profile [allowing it to] take hold. We continue to watch that.
The United States has been, pretty much, a few weeks to a month behind trends that we see in Western Europe. So I think it’s been pretty clear that BQ.1 is going to be something to watch for, as it sort of expands in its frequency… We also see XBB in our program, we’ve seen it as well. I think it’s going to be an interesting new chapter of SARS-CoV-2 evolution where we have potentially co-circulating variants of concern that have different dynamics in different parts of the world.
BL: Yeah, it’s very interesting… One other thing I wanted to ask you about is sample size. It seems like, from the data on the CDC dashboard, that you’re working with a small number of airports and a limited sample, compared to the number of international travelers coming into the U.S. So how do you think about analyzing that, and potentially expanding the sample?
AR: Definitely part of our plan is to ramp up the number of samples that we can get, as well as the number of airports that we might be operating out of.
But I think it’s just remarkable to talk about this program, when you see such a small sample size, and we’re still able to find new things and match GISAID, or global variant frequencies. It highlights, even with a small sample size, that the way that we’ve designed the program and the way our CDC counterparts think about where we’re going to be, what flights are we going to be choosing—that has been really, really successful so far. You always want more samples in science, but I think we’re working with what we have, and we’re excited to be expanding.
BL: That makes sense. So you’re able to say, “We want to send people to these flights, because this country has concerting variants right now,” that kind of thing?
AR: Yeah. Our CDC counterparts are tapped into both the CDC-wide conversations about variants and the global, WHO conversations about variants. So they’ll give us indications when there might be something to think about. And, again, this program is super nimble in its ability to pivot. When we think we want to focus on certain regions of the world, [we can recruit from specific flights].
It’s nice to be working in airports that have these direct flights and these long-haul flights. But thinking about how we prioritize is definitely—the CDC folks are thinking about this, and we sort-of help support them.
BL: The last main thing I wanted to ask about is, obviously in the U.S. and globally, we’re seeing so much less PCR testing now than we had at earlier points in the pandemic. How are you and—to any extent that you can talk about it—how are partners at the CDC thinking about making sure that we’re collecting a lot of samples from diverse settings, and looking in different places, looking at wastewater, and just continuing to keep track of what variants are circulating?
AR: I think back to, finding novel places to sample things. Like, the fact that we’ve invested and tried to build capability to do aircraft wastewater testing is just adding a complementary [data layer]. We’re going to have this layered interface or layered system where we might have some PCR tests, we might have wastewater, we might have sequencing, we might not have sequencing.
We’re figuring out, how do we just keep adding and keep building on this biosecurity infrastructure. I mean, the worst thing that could happen from this is we build all this and then no one uses it again, until something pops up. We’re really invested in finding new and novel ways to sample and to detect, and eventually sequence if we can get more robust data, like on variants.
BL: That makes sense. I wonder to what extent it can one day be useful for other viruses, too. I know we’re in a bad flu moment right now, or at least the beginnings of maybe a more intense flu season this year. And I know experts always talk about, like, “Can we read the tea leaves from the Southern hemisphere?” So that makes me think, “Okay, could we actually sample people who are coming in? And see if they have the flu, and not just COVID?” Or other things of that nature?
CP: This is something that keeps me up at night. Without being too forward-looking, absolutely, I would say, there are some commercial products out there right now—like from Illumina, which is a massive sequencing behemoth, they’ve just released some new sequencers on their end. They have this panel of, like, 66 viruses that you can detect in one panel. I think we’re gonna see more of that from many different types of partners who are looking at surveillance.
Moving beyond SARS-CoV-2, could samples be used for that? We’ve seen lots of publications that definitely prove that’s true. I think it’s right on cue, hopefully, with where we’re all headed.
BL: Yeah, I hope so. Well, those were all my main questions. Is there anything else you all think would be important for me to know about the program?
Swati Sureka: Stepping back, seeing how this [program] has played out over the past year, I’ve just been floored by, like, tens of thousands of people who have mobilized and participated and given samples in service of public health. For me, as a person who works in the communications space, I think we often hear a lot of these narratives of like, “People aren’t gonna do anything” or take any measures that they’re not forced to do.
People are inherently self-interested in all of these narratives that we hear. And it’s been really impressive to watch the participation that we’ve seen from travelers who want to help public health and want to help stop the spread, want to help pick up new variants. I don’t want to lose that thread of things.
BL: Totally. I can just envision, if you’re coming off a long flight, you just want to get through customs and get home. Taking a few extra minutes to get swabbed is not nothing.
AR: Yeah. And you could be doing that and say, “Oh, it doesn’t matter.” But we’re consistently seeing how helpful this data is, to inform all these complementary systems for building a biosecurity infrastructure. It’s really important data as we move forward.
BL: Yeah. When folks sign up, do you give them a link to the dashboard?
AR: Now we do. Now we can, right, it’s now live. It’s been really nice to have that public-facing thing, so that folks know where their efforts are going towards.