This past Thursday, the FDA’s advisory committee on vaccines and similar biological products met to discuss COVID-19 boosters for this fall. They voted in favor of updating the vaccines based on Omicron XBB, a variant lineage that has dominated both in the U.S. and globally this year.
The fall boosters will be monovalent, meaning they’ll only include the XBB strain—unlike our most recent boosters, which were bivalent (including BA.4/BA.5 and the original, Wuhan strain). The FDA has recommended this switch because research suggests monovalent vaccines may be more effective, and because the original coronavirus strain is no longer circulating; we’re mostly seeing XBB right now.
The FDA has not yet decided which exact variant will be used for this fall’s boosters. While experts generally agree that it should be an XBB lineage, the FDA will make a final call on this closer to the fall respiratory virus season. XBB.1.5, XBB.1.9, and XBB.1.16 are all major contenders right now.
This fall’s vaccination campaign is likely to prioritize at-risk populations, including seniors and those with medical conditions that damage their immune systems, similar to the bivalent booster shot rollouts. Ongoing vaccine effectiveness research suggests that these groups benefit most from the protection of an additional booster shot, though people not in these groups obviously benefit as well.
The CDC will make final decisions about which groups will most need the fall boosters, as well as whether some groups may be eligible for more than one of the shots. Children may also become eligible for new boosters; that’ll be up to the CDC as well.
In choosing XBB for the fall boosters, the FDA is standardizing with recommendations from the World Health Organization and European Union, which have also suggested that XBB be the target for the next boosters. Last year, the WHO recommended BA.1, while the U.S. used BA.4/BA.5. Standardizing will be helpful for ongoing data collection, since…
Data problems persist: I’ve written a lot about the U.S.’s disadvantages in tracking vaccine effectiveness, particularly compared to other countries with more standardized health systems. This problem has persisted through all rounds of boosters, including the shots planned for this fall; in fact, it’s even harder now for U.S. agencies to monitor how well the vacines work, as the federal public health emergency’s end led to fewer data collection authorities for the CDC. (Safety monitoring systems will continue, though.)
It’s also worth noting that the boosters this fall will be the first major COVID-19 vaccine rollout following the end of the federal public health emergency. While the Biden administration has devoted some funding for getting vaccines to uninsured Americans, most people will now be getting vaccinated through their health insurance.
This is certain to make the process more complicated and more challenging for many. I’ve already seen stories of people who are eligible for a second bivalent booster having a hard time getting that shot. (See this recent Death Panel episode, for example.) The federal government is doing very little to improve this situation in time for the fall boosters to arrive—and no matter how well XBB vaccines work in theory, they’ll do little in practice if nobody can actually get them.
New Long COVID papers from the Patient-Led Research Collaborative: Speaking of new Long COVID research: the Patient-Led Research Collaborative, a group of long-haulers who do and support research on their condition, has recently published two new papers. The first, published in Nature and based on a patient survey, discusses Long COVID’s intersection with common psychiatric conditions such as depression and anxiety. The second, published in Fronteirs in Rehabilitation Science,is a review paper going over the reproductive health impacts of Long COVID. Long COVID frequently causes disruptions to the menstrual cycle, gonad function, fertility, and other areas of reproductive health, yet these symptoms are understudied.
FDA fully approves Paxlovid: The FDA has provided full approval to Pfizer for its antiviral COVID-19 pill, Paxlovid. Millions of Americans have received Paxlovid since it earned Emergency Use Authorization in late 2021, and many studies have shown that it’s effective in reducing the risk of severe COVID-19 symptoms. With the federal public health emergency’s end, the FDA has encouraged pharmaceutical companies to apply for full approval for their COVID-19 products so that they can permanently remain on the market; Paxlovid is a high-profile example of that trend.
Bivalent COVID-19 vaccines protect, but wane: The CDC published another study this week evaluating the bivalent (or Omicron-specific) COVID-19 booster shots. These vaccines clearly provide additional protection against severe COVID-19 symptoms, the study finds, but this immune system boost goes away after several months. In the study, vaccine effectiveness against hospitalization declined from 62% in early weeks post-vaccination, to 24% at three to six months post-vaccination. The study shows that additional boosters and/or newer vaccines are needed for vulnerable adults.
Value of regular testing for controlling outbreaks: Another notable new study: researchers at the University of Wyoming compared how well different mitigation strategies work for preventing the spread of COVID-19 and other diseases, using a model informed by both epidemiological and economic factors. They found that frequent testing—paired with isolation for people who tested positive—was more effective at reducing disease spread than physical distancing measures, like closing businesses or having employees work from home. The paper suggests that testing can help reduce illness while keeping businesses open.
Funding for a WHO disease surveillance initiative: The Rockefeller Foundation and World Health Organization recently announced a new partnership, with the foundation providing $5 million to support the WHO’s Hub for Pandemic and Epidemic Intelligence. This Hub was established in 2021, with goals including fostering global collaboration on disease surveillance, providing better (and more complete) data, and improving tools for public health decisions. Rockefeller’s support will help with scaling up genomic surveillance, real-time data collection, and more.
Long COVID care access challenges: A new paper, published this week in JAMA Network Open, shares the results of a survey by the Urban Institute think tank. The researchers surveyed about 9,500 adults, including 800 with self-reported Long COVID, about their experiences accessing medical care. The long-haulers were more likely to report difficulties with accessing and paying for care, compared to adults who don’t have the condition. To address this issue, the healthcare system needs to develop clinical guidelines for Long COVID, train workers about it, address insurance barriers, and more, the researchers said.
PolyBio announces Long COVID research agenda: Speaking of Long COVID: the PolyBio Research Foundation, a nonprofit devoted to Long COVID, ME/CFS, and other chronic conditions, has announced several research projects that it’s supporting. The projects will evaluate potential biological mechanisms underlying Long COVID symptoms, such as virus persisting in different parts of the body, changes in T cell activity, microclots, and more. PolyBio has a great reputation for pushing ahead post-viral disease research, and I’m looking forward to seeing the results of these studies.
Bivalent boosters hold up against XBB variants: Another new study that caught my attention this week: researchers at the University of North Carolina and North Carolina state health department reported on how well the bivalent, Omicron-specific boosters worked, based on the agency’s surveillance data. The study examined data from September 2022 through February 2023, a period when the BQ and XBB subvariants were dominating coronavirus spread. North Carolina residents who received the bivalent boosters were significantly less likely to experience severe COVID-19 symptoms, the researchers found, but their protection started to wane within a month after receiving the shots.
Resources on indoor air quality in schools: Journalist’s Resource recently updated this list of research and resources for journalists interested in covering indoor air quality in K-12 schools. The update follows a CDC report showing that many public schools across the U.S. have failed to upgrade their ventilation, despite federal funding to do so (which I covered last week). School air quality is a topic that deserves more reporting, especially from local journalists who can dig into how their school districts are doing.
Arizona county starts monitoring for a fungus in wastewater: I’m always on the lookout for new uses of wastewater surveillance, and one promising application could be tracking Candida auris, a fungal pathogen that’s resistant to common drugs and spreads quickly in healthcare settings. The Arizona state health department and a lab at the University of Arizona recently launched a pilot program to track this fungus through Yuma County’s wastewater. Arizona and neighboring southwest states have been a hotbed for C. auris; if this pilot is successful, other states could start similar efforts.
Second Omicron boosters for high-risk adults: The FDA and CDC are planning to authorize a second round of bivalent, Omicron-specific vaccines for high-risk adults, the Washington Post reported this week. This decision will apply to Americans over age 65 and those who have compromised immune systems, with these groups becoming eligible four months after their initial bivalent boosters. It’s unclear exactly when the decision will become official; the FDA and CDC will make authorizations sometime “in the next few weeks,” according to WaPo.
HHS announces (underwhelming) Long COVID progress: This week marks one year since Biden issued a presidential memo kicking off a “whole-of-government response” to Long COVID. The Department of Health and Human Services (HHS) commemorated the occasion with a fact sheet sharing the federal government’s progress so far. Unfortunately, that progress has been fairly minor, mostly consisting of reports and guidance that largely summarize existing government programs or build on existing systems (such as Veterans Affairs hospitals). Many of the Long COVID programs that Biden previously proposed have not received funding from Congress; meanwhile, the National Institutes of Health’s RECOVER initiative, the one program that has been funded, has faced a lot of criticism.
RECOVER PIs recommend action on treatment: Speaking of RECOVER: this week, a group of scientists leading research hubs within the national study called for federal funding that would support treatment. The principal investigators (PIs) of these hubs have developed expertise in Long COVID through recruiting and studying patients, leading them to identify gaps in available medical care for long-haulers. To respond, the PIs recommend that Congress allocate $37.5 million to support Long COVID medical care at the RECOVER research sites. Their proposed budget includes patient outreach, telehealth support, educating healthcare workers on Long COVID, and more.
Ventilation improvements in K-12 schools: The CDC released a new study this week in its Morbidity and Mortality Weekly Report, sharing results of a survey (conducted last fall) including about 8,400 school districts representing 62% of public school students in the U.S. Research company MCH Strategic Data asked the districts about how they’d improved ventilation in their school buildings, along with other COVID-19 safety measures. About half of the districts reported “maintaining continuous airflow in classrooms,” one-third reported HVAC improvements, 28% reported using HEPA filters, and 8% reported using UV disinfectants. The results indicate that many districts have a long way to go in upgrading their indoor air quality.
Flu vs. COVID-19 mortality risk: Ziyad Al-Aly and his colleagues at the VA healthcare system in St. Louis have published another paper analyzing COVID-19 through the VA’s electronic health records. This study, published in JAMA Network, describes the mortality risk of COVID-19 compared to seasonal flu for patients hospitalized during the 2022-2023 winter season. The researchers evaluated about 9,000 COVID-19 patients and 2,400 flu patients, finding that risk of death for COVID-19 patients in the 30 days following hospitalization was about 1.6 times as high as the risk of death for flu patients. Despite great advances in vaccines and treatments, COVID-19 remains more dangerous than other seasonal viruses, the study suggests.
Biobot launches mpox dashboard: This week, leading wastewater surveillance company Biobot Analytics launched a new dashboard displaying its mpox (formerly monkeypox) monitoring. Biobot tests for mpox at hundreds of sewage sites across the U.S., largely through its partnership with the CDC, and will continue this monitoring through at least summer 2023. The new dashboard shows mpox detections nationally over time and monitoring sites by state; it also includes some information on how mpox surveillance differs from COVID-19 surveillance.
New York State expands wastewater surveillance program: This week, the New York State health department announced a major investment in the state’s wastewater surveillance program: the program has received a $6.6 million grant from the CDC and $15 million from the governor (over the next three years). With this investment, New York’s wastewater surveillance network will grow from 125 to 215 testing sites and will expand from COVID-19 to include flu, RSV, hepatitis, norovirus, and antimicrobial resistance. This is great news for New York—I hope to see other states make similar investments.
Bivalent boosters vs. XBB lineages: The bivalent, Omicron-specific booster shots provide some protection against XBB.1.5 and related Omicron subvariants, according to a new study published this week in the CDC’s Morbidity and Mortality Weekly Report. CDC researchers used data from COVID-19 testing at pharmacies to compare results among people who had received the new booster and those who hadn’t. Booster recipients were significantly less likely to have a symptomatic XBB/XBB.1.5 infection compared to people who hadn’t received the shot, the researchers found (with a vaccine effectiveness value of 48%). While the boosters work less well against XBB.1.5 than they did against BA.4/BA.5, they’re still a valuable protective measure.
CDC overhauling data communications: The CDC is creating new internal offices that will change how it processes, publishes, and communicates about data, according to POLITICO. The new offices include an Office of Health Equity and an Office of Public Health Data, Surveillance, and Technology—both of which have new acting directors as of this week. It’s currently unclear what the new offices will do, exactly, or how they will improve upon a fractured nationwide health data system (with decisions about how to store and share key data largely left up to state agencies and private companies). Still, it’s good to see movement on the CDC’s efforts.
WHO deliberates ending the global health emergency: On Friday, a World Health Organization committee met to discuss whether the official global health emergency over COVID-19 should be ended. The committee’s decision will be made public tomorrow, as a recommendation to WHO Director-General Tedros Adhanom Ghebreyesus; Tedros will ultimately decide whether or not to end the emergency. Global health experts who spoke to STAT reporter Helen Branswell suggested that the WHO likely isn’t ready to end this emergency yet, but it may happen later in 2023.
KFF compiles Long COVID data: A new report from the Kaiser Family Foundation compiles and provides context for Long COVID data reported by the Census and CDC’s Household Pulse Survey. The share of people who reported ever having Long COVID symptoms following a COVID-19 case has declined slightly over time, the KFF report finds; this number went from 35% in June 2022 to 28% in January 2023. However, the number is still high and Long COVID can be debilitating for many, as 79% of people with Long COVID report limitations to their day-to-day activities.
Health of Congressional Districts: Finally: a new dashboard, published this week by researchers at NYU Langone Health, provides detailed health metrics for all 435 Congressional districts in the U.S. (plus Washington, D.C.). The dashboard is a helpful source for researchers and policymakers looking to understand health patterns in specific districts. One of its key metrics is a “COVID Local Risk Index” that reflects the risk residents face for severe health, social, and economic outcomes of COVID-19.
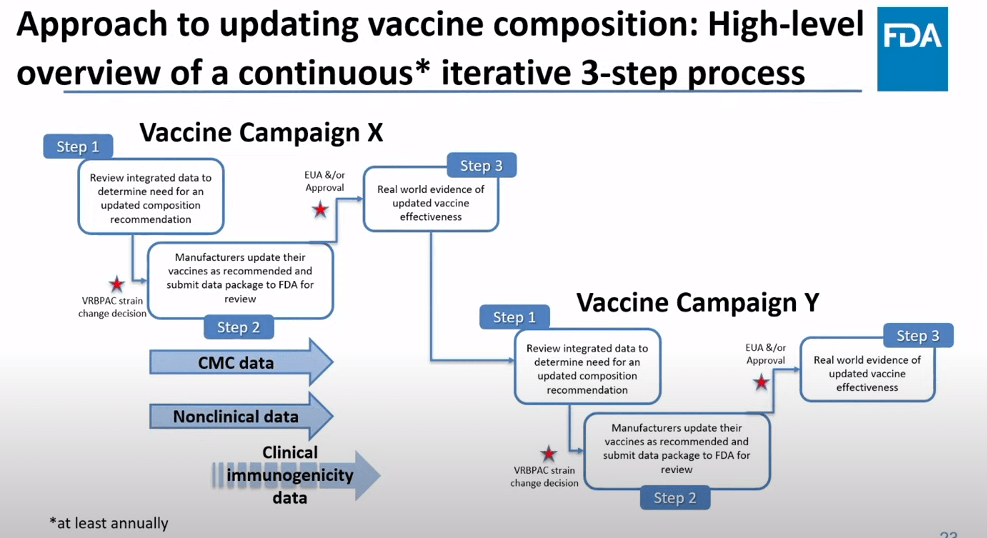
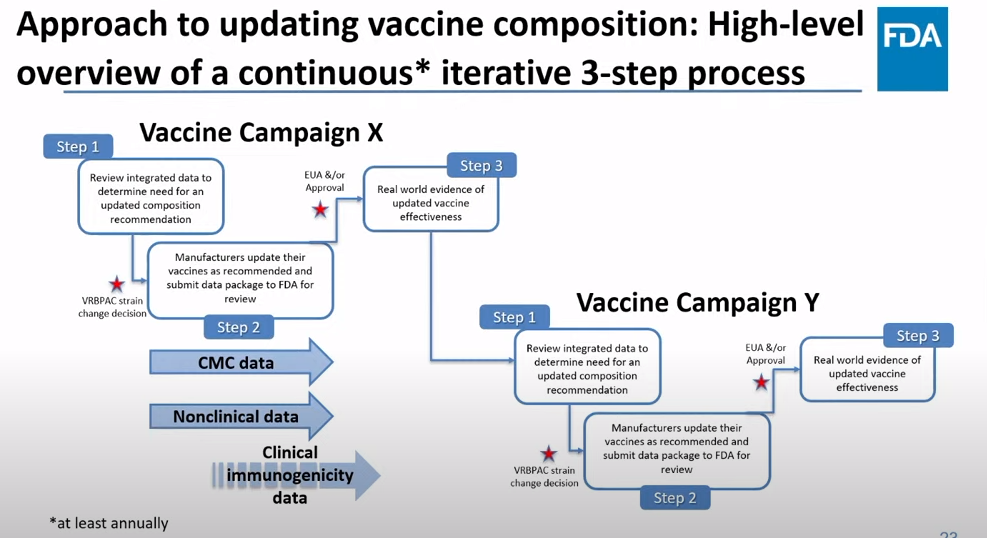
The FDA recommends that the U.S. shifts to annual COVID-19 vaccines, with a variety of data sources feeding into decision-making. Screenshot from the VRBPAC meeting on January 26, 2023.
On Thursday, the FDA’s Vaccines and Related Biological Products Advisory Committee (or VRBPAC) met to discuss the future of COVID-19 vaccines. While the committee readily agreed that our current, Omicron-specific shots are working well and should be used more broadly, it had a hard time answering other questions about future vaccine regimens—largely due to a lack of good data.
Now, the lack of good U.S. data on vaccine effectiveness is not a new problem. I personally have been writing about thissince fall 2021, to the point that I feel like a broken record for bringing it up again. To summarize: the U.S. has a fractured health system in which every state tracks vaccinations differently, with a lot of local public health departments and private companies in the mix, too. As a result, it’s challenging for researchers to determine exactly who is getting COVID-19 after vaccination and how the virus is impacting them.
This lack of detailed vaccine effectiveness data was a problem in fall 2021, when federal officials decided on an initial round of booster shots. And it’s still a problem in winter 2023, as the same officials attempt to plot out a future in which COVID-19 is another disease that we deal with on an annual basis.
But this week’s VRBPAC meeting revealed some other areas of data that are also lacking as we try to answer questions about future vaccines. Here’s my summary of five primary data gaps that came up at the meeting, and some suggestions for potential solutions.
Detailed vaccine effectiveness data
The biggest data gap, of course, is our lack of answers to the question: Who is getting sick with COVID-19 after vaccination? And related questions: How sick did they get? Which variants did they get sick with? What preexisting conditions or comorbidities did they have?
Our lack of standardized medical data in the U.S. makes it tough to answer these questions at the population level. Analyzing variants is particularly tricky, given that variant surveillance in the U.S. tends to be entirely anonymized—with no connections between the genomic sequencing of random PCR tests and the health outcomes (or vaccination statuses) of those patients. And analyzing preexisting conditions can be crucial as officials try to decide which groups of people need extra boosters, but these conditions often are not collected in standard databases or linked to COVID-19 records.
As a result, U.S. officials tend to rely on other countries with more comprehensive, standardized data systems for information on how well the vaccines work. We also have to rely on the pharmaceutical companies producing these vaccines, which often don’t openly share their data—they tend to present clinical trial results in press releases, over peer-reviewed studies. Companies also tend to do trials that align better with their own financial interests, rather than looking at the full scope of vaccine effectiveness.
Even in this week’s VRBPAC meeting, scientists from Moderna presented results from a clinical trial—conducted in the U.K.—that tested the company’s bivalent boosters against the original (non-Omicron) boosters.
Better tracking of variants
The primary reason why our COVID-19 vaccines require updates in the first place is the coronavirus’ continued evolution. Every new lineage of Omicron that rises to prevalence is either a bit better at spreading quickly, a bit better at evading immunity from prior infection or vaccination, or both. To successfully tweak our vaccines in the future, scientists will need to know which variants are out there and how dangerous they are.
Right now, variant tracking largely relies on PCR testing, as researchers randomly select some swab samples to sequence. But with fewer and fewer people getting PCR tests, the sample pool is dwindling. As a result, to stay ahead of new variants, the U.S. needs to diversify its surveillance options. That will likely include more variant sequencing from wastewater (as a population-level COVID-19 sample), more sequencing at hospitals and healthcare centers, and more travel surveillance focused on international variant patterns.
Variant surveillance will also need to inform how suited U.S.-developed COVID-19 vaccines are for the rest of the world. Right now, the pharmaceutical companies that have produced the most effective vaccines (i.e. Pfizer and Moderna) are American—so American regulators are essentially dictating vaccine policy for the world, even though their priority is the U.S. FDA official Jerry Weir said as much at the meeting. U.S. hegemony over COVID-19 vaccines will continue to be a complex, fraught topic going forward.
Tracking different types of immunity
At the VRBPAC meeting, Moderna, Pfizer, and Novavax all presented data on how well their vaccines work against currently-dominant coronavirus variants. While they included some clinical data (case rates, hospitalization rates), the presentations mostly focused on one metric: antibody titers. To calculate if a vaccine works against a certain variant, the easiest strategy is measuring the antibodies produced after a vaccinated blood sample is exposed to that variant.
While this is the easiest strategy, it’s far from the only way to examine how well a vaccine works. Members of the VRBPAC committee frequently asked the pharmaceutical companies for those other metrics: T cells, B cells, and more ways of measuring the immune system’s response to COVID-19. But the companies had little response to these questions. Even FDA and NIH officials at the meeting admitted that they still didn’t have a good understanding of how, exactly, our current vaccines impact our immune systems, beyond generating antibodies.
To better evaluate future vaccines, scientists will need to get better at measuring other aspects of our immune responses. That includes future mRNA vaccines as well as next-generation vaccines in the works right now, such as nasal vaccines (recently authorized in China and India) and vaccines designed to protect against all variants (currently in development at Duke University and other institutions).
I also think it’s worth noting that, as Katelyn Jetelina writes in her coverage of the VRBPAC meeting at Your Local Epidemiologist, the FDA could require pharmaceutical companies to study the immune system more holistically when they submit further vaccine updates for authorization. “The FDA could require sponsors to do detailed investigations, e.g. assessing lymph nodes, bone marrow, and breakthroughs,” she writes. “This would help us understand immunity better, so we can make better recommendations. It’s not clear why they aren’t pushing for this.”
Improving vaccine safety tracking
Two years after the first COVID-19 vaccines were authorized, we now know that the vaccines are overwhelmingly safe and effective. Most people have mild side effects following their shots, like sore arms and fatigue, but the benefits of getting vaccinated far outweigh the risks. However, some discussion at the VRBPAC meeting indicated that federal agencies could do a better job of tracking rare (yet important) serious side effects.
For example, a safety presentation from the Kaiser Permanente Vaccine Study Center suggested that there might be a small increase in stroke risk for older adults who get vaccinated. The risk has only appeared in one vaccine safety database so far and appears to be minimal, per the FDA, but it’s still worth closer examination.
In addition, as Helen Branswell and Matthew Herper discuss in the STAT News liveblog, the VRBPAC meeting didn’t present much new data about vaccine safety risks for children, such as myocarditis among boys and young men. Plus, we have limited data so far on whether vaccination may contribute to autoimmune conditions or Long COVID-like symptoms, a problem that has shown up in some studies and anecdotal reports.
If public health officials are going to continue encouraging Americans to get COVID-19 shots once a year (or more), they will need to thoroughly address concerns about these potential side effects. This is particularly true for young children, a group that’s been vaccinated at fairly low numbers so far.
Navigating COVID-19’s interactions with other vaccines
At the VRBPAC meeting, FDA officials suggested a potential future in which most Americans get one COVID-19 vaccine per year, on a similar timeline to the annual flu shot. Variant strains might be selected in the spring or summer, with vaccines developed and produced in time for a fall vaccination campaign. Some at-risk groups (older adults, people with compromised immune systems, etc.) might get two doses each year.
To make this possible, the VRBPAC committee members suggested that we’ll need to track how COVID-19 vaccines intersect with other vaccines. For example, if an older adult receives their flu shot and COVID-19 shot in the same doctor’s visit, does that dampen how well one or the other vaccine works? Does it increase the risks of severe side effects? We don’t know, at this point.
Another major area of future study will be how COVID-19 vaccines may fit into regular, childhood immunization schedules for young kids. Similarly to the COVID-19 plus flu question, scientists will need to track any potential interactions between COVID-19 shots and other regular shots—along with answering questions about how many shots are needed, timing between shots, and more.
One day, I’m sure, we will have a regular COVID-19 vaccination schedule in the U.S. that runs parallel to our flu vaccination schedule. But it will take time, discussions, and a lot more data to get there.
New CDC dashboards track respiratory illness hospitalizations: This week, the CDC released two new dashboards that combine COVID-19 data with data on other respiratory illnesses. First, the RESP-NET dashboard summarizes information from population-based hospital surveillance systems in 13 states for COVID-19, the flu, and RSV; it includes overall trends and demographic data. Second, the National Emergency Department Visits dashboard provides data on emergency department visits for COVID-19, the flu, RSV, and all three diseases combined; this dashboard includes data from all 50 states, though not all hospitals are covered.
Early results from NIH at-home test self-reporting: Last week, ABC News shared early results from MakeMyTestCount.org, an online tool run by the National Institutes of Health allowing Americans to self-report their rapid, at-home test results. Between the site’s launch in late November and early January, “24,000 people have reported a test result to the site,” according to ABC. (While the article says “people have reported,” I think this number actually represents the number of test results reported, given that the website doesn’t track when one person submits multiple test results over time.) The majority of results reported are positive and women are more likely to self-report than men, per ABC. It’s unclear how useful these early data may be for any analysis, but I’m glad to see some numbers becoming public.
New preprint updates county-level excess death estimates: A new preprint from Boston University demographer Andrew Stokes and colleagues, posted this week on medRxiv, shares updated estimates on excess deaths and COVID-19 deaths by U.S. county. According to the analysis, about 270,000 excess deaths were not officially attributed to COVID-19 during the first two years of the pandemic, representing 24% of all excess deaths during that time. And the analysis reveals regional patterns: for example, in the South and in rural patterns, excess deaths were less likely to be officially attributed to COVID-19. For more context on these data, see MuckRock’s Uncounted project (which is a collaboration with Stokes and his team).
Factors contributing to low bivalent booster uptake: Another notable paper from this week: results from a survey of Americans who were previously vaccinated about their reasons for receiving (or not receiving) a bivalent, Omicron-specific booster this fall, conducted by researchers at Duke University, Georgia Institute of Technology, and others. Among about 700 people who didn’t get the booster, their most common reasons were a lack of awareness that the respondent was eligible for this vaccine, a lack of awareness that the bivalent vaccine was widely available, and a perception that the respondent already had sufficient protection against COVID-19. This survey shows how governments at every level have failed to advertise the bivalent boosters, likely to dire results.
More wastewater surveillance on airplanes: And one more notable paper: researchers at Bangor University tested wastewater from three international major airports in the U.K., including samples from airplanes and airport terminals. About 93% of the samples from airplanes were positive for SARS-CoV-2, while among the airport terminal samples, 100% at two airports were positive and 85% at the third airport were positive. Similar to the study from Malaysia I shared last week, this paper suggests that there’s a lot of COVID-19 going around on air travel—to put it mildly. The paper also adds more evidence that airplane/airport wastewater can be a useful source for future COVID-19 surveillance.
Nursing home infections ran rampant early in the pandemic: A new report from the Health and Human Services Office of Inspector General examines how much COVID-19 spread through nursing homes in 2020. The report’s authors used Medicare data from about 15,000 nursing homes nationwide, identifying those with “extremely high infection rates” in spring and fall 2020. In more than 1,300 of these facilities, 75% or more of the Medicare patients had COVID-19 during these surges; the same facilities had way-above-average mortality rates. “These findings make clear that nursing homes in this country were not prepared for the sweeping health emergency that COVID-19 created,” the authors write in the report’s summary.
2022 America’s Health Rankings released: This week, the United Health Foundation released its 2022 edition of America’s Health Rankings, a comprehensive report providing data for more than 80 different health metrics at national and state levels. The 2022 report includes new metrics tailored to show COVID-related disparities; for example, Black and Hispanic Americans had higher rates of losing friends and family members to COVID-19 compared to other groups. I’ve used data from past iterations of this report in stories before, and I’m looking forward to digging into the 2022 edition.
FDA authorizes bivalent boosters for young kids: This week, the FDA revised the emergency use authorizations (EUAs) of both Pfizer’s and Moderna’s updated, Omicron-specific booster shots to include children between six months and five years old. Kids who previously got two shots of Moderna’s vaccine for this age group can receive a bivalent booster two months later, while kids who got two shots of Pfizer’s vaccine can receive a bivalent booster as their third dose. (Remember, Pfizer’s vaccine for this age group includes three doses.) The updated EUAs will help protect young children from Omicron infection, though uptake will likely be low.
CDC updates breakthrough case data: Speaking of the updated boosters: the CDC recently added data on these shots to its analysis of COVID-19 cases and deaths by vaccination status. In September, people who had received a bivalent, Omicron-specific boosters had a 15 times lower risk of dying from COVID-19 compared to unvaccinated people; and in October, bivalent-boosted people had a three times lower risk of testing positive compared to the unvaccinated. The CDC will update these data on a monthly basis.
Director Walensky discusses authority challenges: One bit of coverage from the Milken Future of Health Summit that caught my attention: CDC Director Dr. Rochelle Walensky talked about the agency’s limitations in collecting data from states, reports Rachel Cohrs at STAT News. Walensky specifically highlighted the challenges that the CDC might face in collecting data when the public health emergency for COVID-19 ends, something I’ve previously covered in this publication.
Boston establishes neighborhood-level wastewater testing: Finally, one bit of wastewater surveillance news: the city of Boston is setting up 11 new sites to test wastewater, giving local public health officials more granular information about how COVID-19 is spreading in the region. The new initiative is a partnership with Biobot Analytics, the same wastewater testing company that has long worked with Boston, the CDC, and public health institutions across the country. (Boston was one of the first cities to start doing this testing.) Also, speaking of Biobot: the company just added a nice chart of coronavirus variants in U.S. wastewater over time to its dashboard.
More data on the new, bivalent boosters: A new study, published this week in the CDC’s Morbidity and Mortality Weekly Report, has further evidence that the new, Omicron-specific booster shots provide additional protection against COVID-19 for people who previously received the original vaccines. Researchers used test results from pharmacies to compare symptomatic COVID-19 cases among people who had received the new boosters to those who had only received older vaccines. New booster recipients were less likely to get sick, they found, indicating protection against Omicron BA.4, BA.5, and their sublineages. In short: if you haven’t gotten one of the new boosters yet, now is a good time!
Patient-Led Research Collaborative announces grant winners: The Patient-Led Research Collaborative, an organization of Long COVID patient-researchers that has produced groundbreaking work about this condition, just announced the winners of its $5 million fund to support new biomedical research on Long COVID. The winning projects will pursue avenues of top priority to patients, such as understanding post-exertional malaise, testing for microclots, and a clinical trial for the drug naltrexone. Projects were themselves evaluated by a panel of patient experts and patients will be heavily involved in the resulting research. Congrats to the PLRC team on this announcement, and I look forward to following the results of these studies!
HHS publishes Health+ Long COVID report: Another piece of Long COVID news this week: the Department of Health and Human Services published a report summarizing interviews with people who have Long COVID. The report was one of several responses to the Biden administration’s call last spring for Long COVID research and support programs. It describes patients’ desires for meaningful research, better healthcare, financial support, and more. While this new report may not be adding much to the body of knowledge about Long COVID, it’s helpful to see this information coming from a major government source.
Football games associated with COVID-19 spread: And one more study that caught my attention this week: a new paper in JAMA Network Open describes a correlation between National Football League (NFL) games and COVID-19 spikes in the surrounding counties during the league’s 2020-2021 season. Counties hosting more popular games (with at least 20,000 fans present) were more likely to see increased COVID-19 spread afterwards. The paper shows how large events can contribute to widespread disease transmission, even among people who didn’t themselves attend the events.
CDC update on COVID-19 mortality trends: This week, the CDC published a detailed report about how deaths from COVID-19 have changed in 2022. Overall, between 2,000 and 4,500 COVID-19 deaths were reported each week between April and September 2022, the CDC researchers found; this is lower than at earlier points in the pandemic, but still represents a loss of more than 100,000 Americans over the course of a year. Older adults and those who were un- or under-vaccinated had a higher risk of death from COVID-19, the researchers found; racial and ethnic disparities have “decreased, but persisted.”
Moderna reports new data on its bivalent booster: Several studies in the lastcouple of weeks have indicated that the new, Omicron-specific boosters from Pfizer and Moderna are more effective against new variants than the older vaccines. Moderna provided additional data this week, reporting that its new booster led to five times more antibodies that neutralize Omicron BA.4 and BA.5 compared to earlier booster shots. While Moderna’s study hasn’t yet been peer-reviewed, the results are promising in following a trend from past studies, STAT’s Matthew Herper reports.
Booster shots could keep kids from missing school: Speaking of the new boosters: a new report from the Commonwealth Fund provides analysis of the boosters’ potential impact on school-aged children, as all kids older than five are eligible for the shots. If 80% of eligible Americans receive their bivalent boosters by the end of 2022, the report suggests, this could save over 46 million days of isolation and over 50,000 hospitalizations for school-aged children, along with other benefits. Even getting kids boosted at the level of flu vaccination in 2020-2021 would prevent millions of days of school from being lost.
Test to treat is inaccessible to rural Americans: A new study, published this week in JAMA Network Open, examined equity issues with the Biden administration’s Test to Treat initiative. The initiative was designed to provide locations where Americans could get a COVID-19 test and then, if they received a positive result, quickly receive a free antiviral drug. But many people don’t live near available locations, the researchers found: “approximately 15% of the overall US population, 30% of American Indian or Alaskan Native people, and 59% of the rural population lived more than 60 minutes from the nearest site,” they write.
Perception of local COVID-19 levels: A lot of people are acting with incorrect knowledge of their local COVID-19 risk, a new study in the CDC’s Morbidity and Mortality Weekly Report suggests. Researchers from several medical and public health institutions surveyed people who had recently tested positive for COVID-19 in Detroit, Michigan and DuPage County, Illinois, during June and July, 2022. About half of the 5,000 people surveyed said that they thought local COVID-19 transmission was “low or moderate,” even though it was actually at high levels in both places.