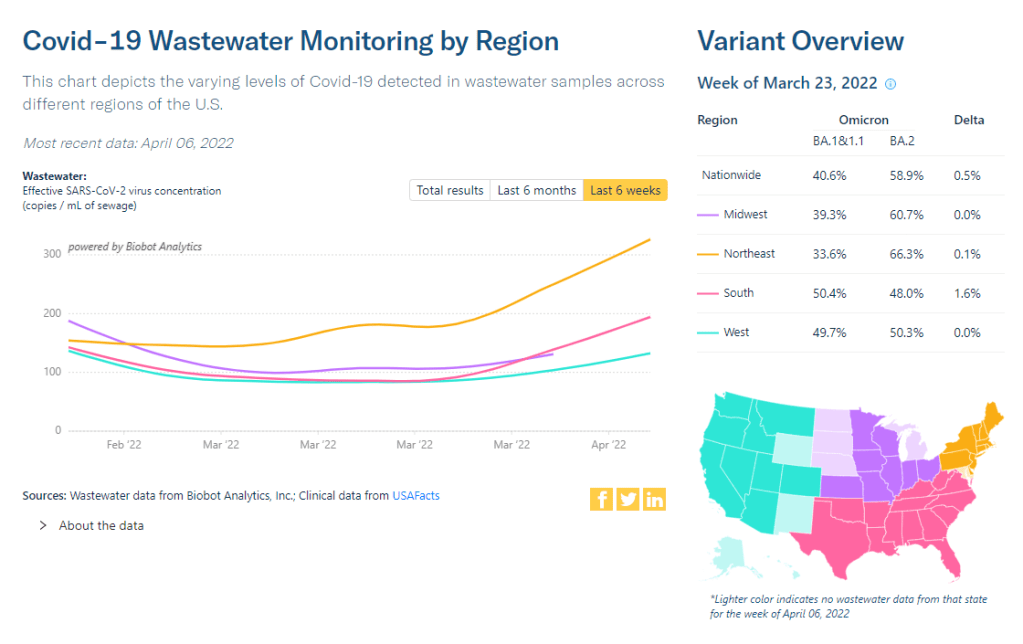
Coronavirus levels in wastewater are now rising in all regions of the country, according to Biobot. Screenshot taken on April 9.
In the past week (April 2 through 8), the U.S. reported about 190,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 27,000 new cases each day
57 total new cases for every 100,000 Americans
5% more new cases than last week (March 26-April 1)
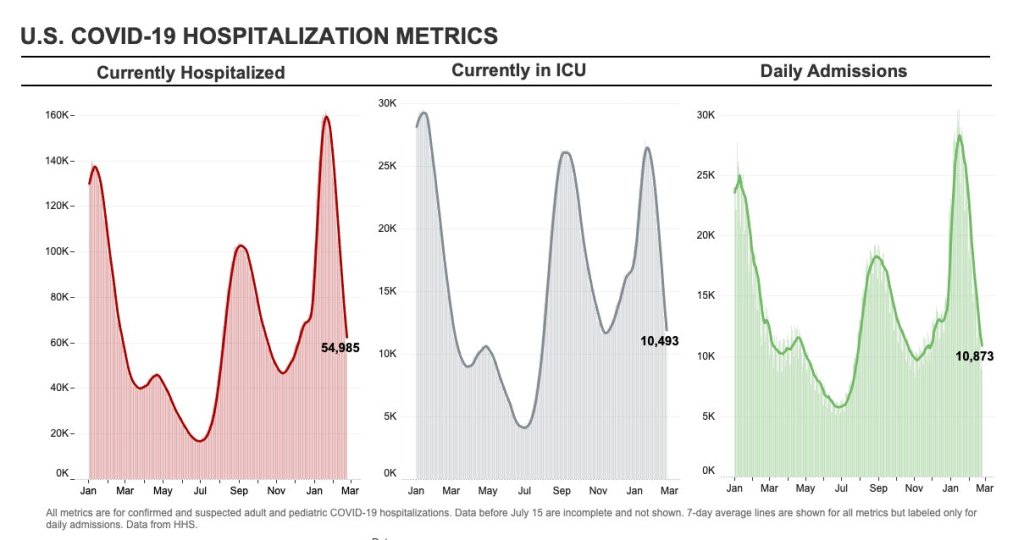
In the past week, the U.S. also reported about 10,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 1,400 new admissions each day
3.0 total admissions for every 100,000 Americans
10% fewer new admissions than last week
Additionally, the U.S. reported:
3,500 new COVID-19 deaths (1.1 for every 100,000 people)
100% of new cases are Omicron-caused; 72% BA.2-caused (as of April 2)
An average of 100,000 vaccinations per day (per Bloomberg)
After several weeks in a plateau, new COVID-19 cases in the U.S. are once again going up at the national level. The CDC reported an average of 27,000 new cases a day last week—less than one-tenth of what we saw during the Omicron surge, but still a notable uptick from the week prior.
National numbers of newly hospitalized patients and COVID-19 deaths are both still trending down; this is unsurprising, as trends in hospitalizations and deaths typically follow cases by several weeks.
That wastewater signal likely means that cases will keep going up in the next couple of weeks. BA.2 is a clear culprit for this: the more-contagious Omicron sublineage is now causing about three in four new COVID-19 cases in the U.S., according to the CDC’s latest estimates. BA.2’s dominance led the FDA to pull its emergency use authorization for Sotrovimab, a monoclonal antibody drug that works against Omicron BA.1—but not against BA.2,
As we’ve seen for the last couple of weeks, the Northeast continues to be a leader in case increases. Jurisdictions with the highest cases per capita in the week ending April 6 are Alaska, Vermont, Rhode Island, Washington, D.C., New York, Massachusetts, New Jersey, and Maine. All reported more than 100 new cases for every 100,000 residents, per the latest Community Profile report.
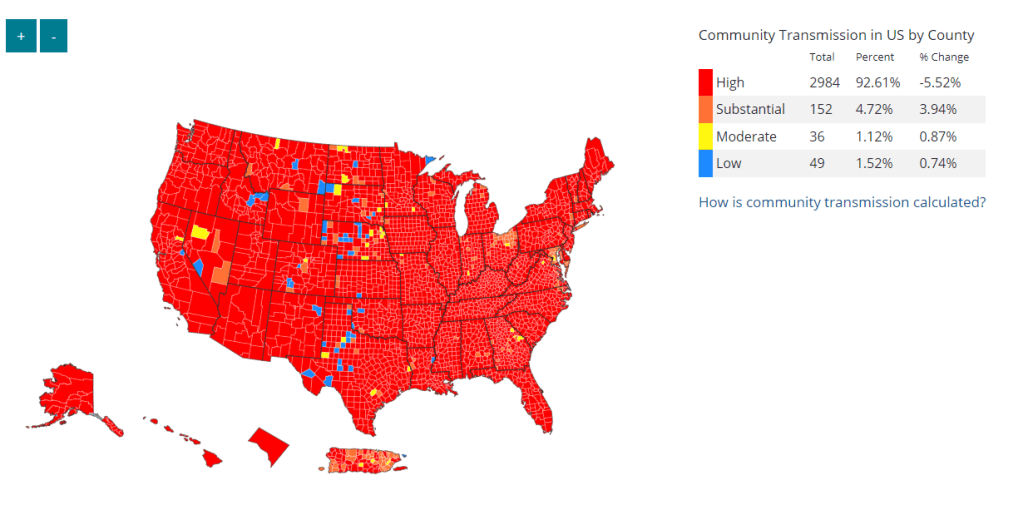
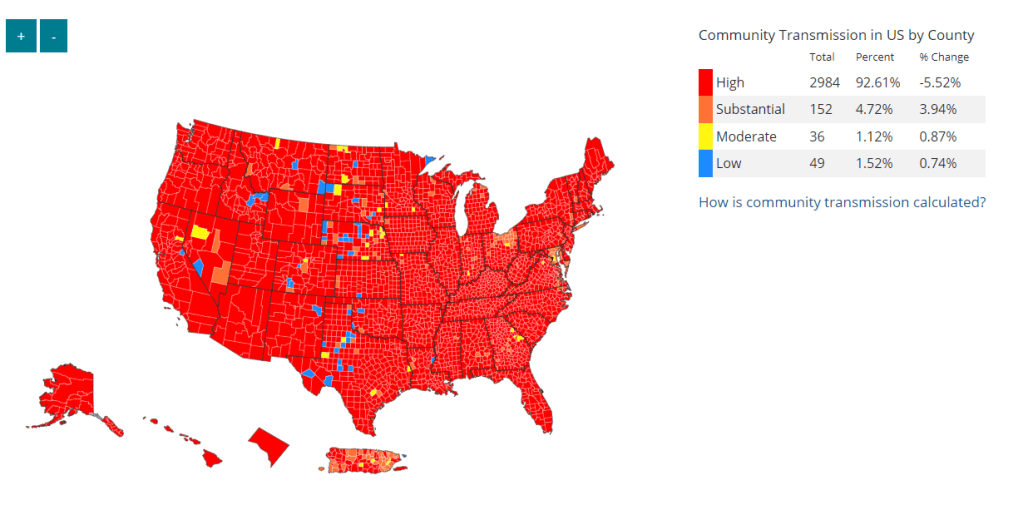
Under the CDC’s old community level guidance, all of these Northeast states (and Alaska) would be classified as seeing high transmission. But under the new, more lenient guidance, 99% of the country—including most counties in these states—are classified as “low” or “medium” community levels.
These lenient levels don’t account for warnings in our wastewater, not to mention under-testing as PCR sites close and at-home tests go unreported. As Katherine Wu wrote in The Atlantic this week, the U.S. may be facing a new surge, but it’s harder to accurately track COVID-19 now than it has been since spring 2020. Don’t let the low numbers fool you into thinking all is well.
BA.2 caused more than two-thirds of new COVID-19 cases in the Northeast in the week ending March 26, according to CDC estimates. It’s no coincidence that this region is also seeing cases start to tick up.
In the past week (March 26 through April 1), the U.S. reported about 180,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 26,000 new cases each day
55 total new cases for every 100,000 Americans
3% fewer new cases than last week (March 19-25)
In the past week, the U.S. also reported about 11,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 1,600 new admissions each day
3.3 total admissions for every 100,000 Americans
16% fewer new admissions than last week
Additionally, the U.S. reported:
4,400 new COVID-19 deaths (1.3 for every 100,000 people)
100% of new cases are Omicron-caused; 55% BA.2-caused (as of March 26)
An average of 90,000 vaccinations per day (per Bloomberg)
Nationwide, COVID-19 cases in the U.S. have reached a plateau. New cases decreased only 3% from the previous week to this week, following an 8% decrease the week before that. New hospitalizations and deaths are also declining slightly, approaching the same plateau pattern.
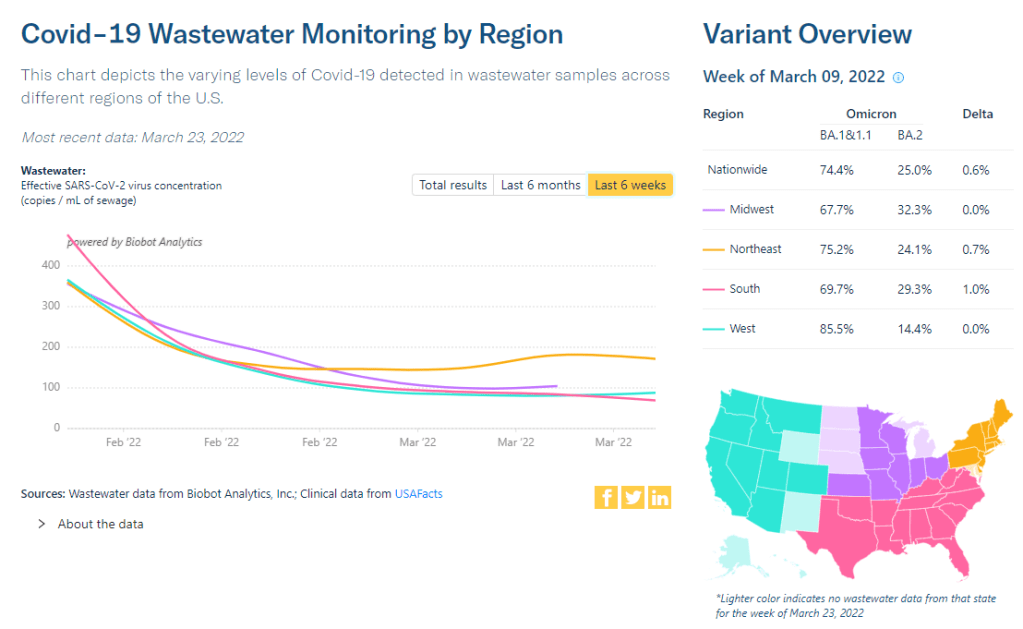
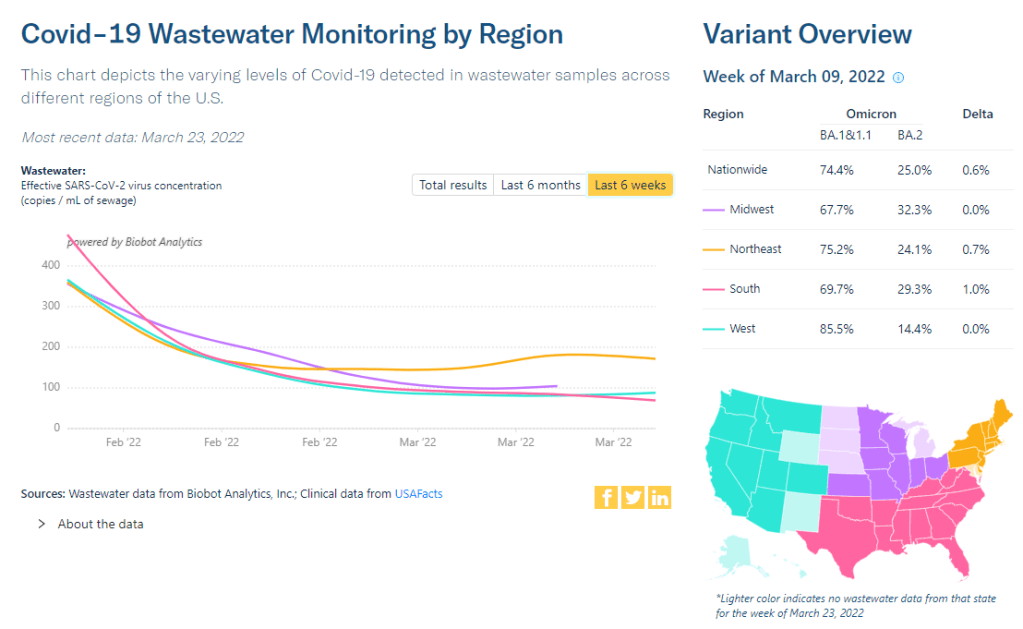
Wastewater is showing a similar pattern, too. The overall, national trend of coronavirus levels in wastewater has been in a plateau for a couple of weeks now, according to the Biobot dashboard. Regionally, the Northeast saw a slight uptick followed by an even slighter downturn, and the South may be seeing a slight uptick now.
BA.2, the Omicron sublineage that is more transmissible than the version of this variant that first reached us in the U.S., is now causing over half of new COVID-19 cases nationwide, according to CDC estimates. Two weeks ago, I wrote that 50% prevalence was a threshold for cases starting to increase in Europe; if the U.S. follows Europe (as we usually do), that means we’ll start seeing case increases here in the next week.
According to the CDC’s estimates, BA.2 is already causing almost 75% of new cases in the New England and New York/New Jersey regions. It’s unsurprising, then, that several Northeast states have reported case increases in the last week. According to the latest Community Profile Report, states that reported increases above 25% week-over-week include: Arizona, Alabama, Ohio, Delaware, North Carolina, Hawaii, Massachusetts, and New York.
New York City—an early hotspot for BA.2, as it was for the original Omicron strain in December—reported more than 100 cases for every 100,000 residents last week, according to both city data and the CDC’s figures.
Under the old CDC thresholds, this would have put the city in a “high transmission” zone, indicating that all residents should mask up in public, indoor spaces. However, the new CDC guidance places New York City in a “low” level, meaning masks are not recommended—a clear example of the lenience in this new guidance.
It’s good news that we’re not seeing a sharp BA.2-driven increase here in the U.S. yet, either within coronavirus levels in wastewater or within the case data. A BA.2 surge here may likely be a small bump rather than a huge wave. Still, the new lenience in safety measures—combined with federal funding running out for free testing, vaccinations, and other COVID-related coverage—is making me pretty nervous.
The Northeast has seen a small uptick in coronavirus levels in its wastewater in recent weeks, followed by a plateau. Chart via Biobot Analytics.
In the past week (March 19 through 25), the U.S. reported about 190,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 27,000 new cases each day
58 total new cases for every 100,000 Americans
5% fewer new cases than last week (March 12-18)
In the past week, the U.S. also reported about 13,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 1,800 new admissions each day
3.9 total admissions for every 100,000 Americans
21% fewer new admissions than last week
Additionally, the U.S. reported:
5,200 new COVID-19 deaths (1.6 for every 100,000 people)
100% of new cases are Omicron-caused; 35% BA.2-caused (as of March 19)
An average of 100,000 vaccinations per day (per Bloomberg)
New COVID-19 case numbers for the U.S. overall are still decreasing, according to the CDC’s data. But the drop from the previous week’s cases to this week’s cases (about 5%) is lower than any week-over-week change since Omicron peaked in January, suggesting that we’re heading for a plateau—if not a new increase.
Last week, I discussed a potential new surge in the U.S. driven by the Omicron sublineage BA.2, which is more transmissible than the version of Omicron we faced a couple of months ago. BA.2 caused about 35% of new COVID-19 cases nationwide in the week ending March 19, according to CDC estimates, up from 22% in the prior week.
As BA.2 slowly outcompetes the other Omicron sublineages in the U.S., we also continue to see case upticks in some parts of the country. States that reported case increases in the last week include Arkansas, Kentucky, Maine, New York, Colorado, Massachusetts, and Vermont, according to the March 24 Community Profile Report. (Arkansas and Kentucky reported week-over-week increases above 25%, while the other states here reported increases above 10%.)
Wastewater data align somewhat with these case increases. Biobot’s tracker shows a slight uptick (followed by a plateau) in coronavirus levels in the Northeast’s wastewater, at a regional level, along with plateaus in other parts of the country. And about 40% of sites in the CDC’s national wastewater network have reported increases over the last two weeks—though the CDC’s data are difficult to interpret, as this tracker doesn’t provide context on actual wastewater levels at each site.
To be clear, it’s good news that we aren’t seeing major case increases yet, just some small upticks. At the same time, numbers of newly hospitalized COVID-19 patients and deaths are dropping to levels not seen since last summer; this week, about 750 people died of the disease each day, according to the CDC—the first time this number has been under 1,000 in several months.
The 7-day avg for new hospital admissions in the U.S. (confirmed + suspected COVID) is now also at an all-time low pic.twitter.com/99LPzBCYKw
In a recent TIME article, several experts suggested that vaccines plus lingering immunity from the Omicron wave in December and January may protect the U.S. from a major surge with BA.2. Still, with safety measures dropping across the country, in the event that we do see a major new surge (from BA.2 or otherwise), we won’t be prepared to curb virus transmission in a meaningful way.
BA.2 caused about one in four U.S. COVID-19 cases in the week ending March 12, according to CDC estimates.
Two years into the pandemic, we now know some basic truisms about the coronavirus. For example: outdoor events are always safer than indoor events; older age is the most significant risk factor for severe symptoms; hospitalization trends typically follow case trends by a couple of weeks; and whenever Europe has a new surge, the U.S. is likely to also see a surge in the next month or so.
That last truism is particularly relevant right now, because Europe is experiencing a new surge. Cases are increasing in the U.K., Germany, the Netherlands, and many other countries. The new surge is likely due to European leaders’ decisions to end all COVID-19 safety measures in their countries, combined with the rise of Omicron sublineage BA.2.
As BA.2 prevalence increases here in the U.S.—and our leaders also end safety measures—we seem poised to follow in Europe’s footsteps once again. But a BA.2 surge is likely to look different from the intense Omicron surge that we experienced in December and January, in part because of leftover immunity from that Omicron surge.
Let’s go over what we know about BA.2, and what might happen in the next few weeks.
What is BA.2?
It’s important to note that this isn’t a new variant, at least not compared to the original Omicron strain. As I noted in a FAQ post about this strain back in January, South African scientists who originally characterized Omicron in November 2021 identified three sub-lineages: BA.1, BA.2, and BA.3.
BA.1 spread rapidly through the world, driving the surge that we experienced here in the U.S. in December through February. But BA.2, it turns out, is actually more transmissible than BA.1—allowing it to now outcompete that strain and contribute to case increases in countries that already faced major BA.1 surges.
How does BA.2 differ from BA.1, or original Omicron?
The main difference between these two strains is that BA.2 is more contagious: scientists estimate that BA.2 is about 30% more transmissible than other Omicron strains, if not more. (Note that this is a smaller difference than Omicron’s advantage over Delta and other earlier variants.)
In a recent report, the U.K. Health Security Agency estimated that someone infected with BA.2 would infect about 13.6% of their households and 5.3% of contacts outside of their households, compared to 10.7% of households and 4.2% outside contacts for other Omicron strains. The modest difference between these rates demonstrates why BA.2 is not outcompeting other Omicron strains as quickly as Omicron outcompeted Delta a couple of months ago.
Another notable feature of BA.2 is that, unlike BA.1, it can’t be identified with a PCR test. BA.1 has a mutation called S drop-out, which causes a special signal in PCR test results, allowing the variant to be flagged without sequencing; BA.2 doesn’t have this mutation. To be clear, a PCR test will still return a positive result for someone who is infected with BA.2—it’ll just take an additional sequencing step to identify that they have this particular strain.
Finally, one major challenge during the Omicron BA.1 surge has been that two of the three monoclonal antibody treatments used in the U.S. did not work well for people infected with Omicron. BA.2 may exacerbate this challenge, as some studies have suggested that the third treatment—called sotrovimab—continued working against BA.1, but may not hold up against BA.2. Luckily though, Eli Lilly (which developed one of the treatments that failed for BA.1) has produced an updated monoclonal antibody cocktail that does work for both Omicron strains.
How is BA.2 similar to BA.1, or original Omicron?
Two major pieces of good news here: 1) our existing COVID-19 vaccines work similarly well against BA.2 as they do against BA.1, and 2) prior infection with BA.1 seems to be protective against infection with BA.2.
Essentially, studies are showing that the two strains are close enough in their genetic profiles that antibodies from a BA.1 infection will provide some immunity against a BA.2 infection. And the same thing goes for vaccination, at least when it comes to protection against severe disease. A recent CDC study showed that, even during the Omicron surge, COVID-19 patients who had received three vaccine doses were far less likely to require mechanical ventilation or die from the disease than those who weren’t vaccinated.
There’s a flip side to this, though: for both BA.1 and BA.2, prior infection with a previous variant is not very protective against an Omicron infection. CDC seroprevalence data suggest that between 40% and 45% of Americans got infected with BA.1 during the winter surge; this means the remaining 55% to 60% of the population is susceptible to BA.2. Vaccines protect against severe disease and death from BA.2, but they don’t protect against BA.2 infection to the degree that they did against past variants.
This means that in terms of protection against infection, populations with high rates of vaccination or prior infection remain essentially naive to it. Though vaccines and prior infections still protect from severe disease and death (thanks to T-cell protection). 3/ pic.twitter.com/gmwlk2l7ZV
— Prof Francois Balloux (@BallouxFrancois) March 19, 2022
BA.2 and BA.1 are also similar in their severity. Both strains are less likely to cause severe disease than Delta; BA.1 had a 59% lower risk of hospital admission and 69% lower risk of death than Delta in the U.K., according to a new paper published this week in the Lancet.
It’s important to remember, however, that Delta was actually more severe than other variants that preceded it. As a result, “Omicron is about as mild/severe as early 2020 SARSCoV2,” wrote computational biologist Francois Balloux in his Twitter thread (referring to both BA.1 and BA.2).
What are the warning signs for a BA.2 surge in the U.S.?
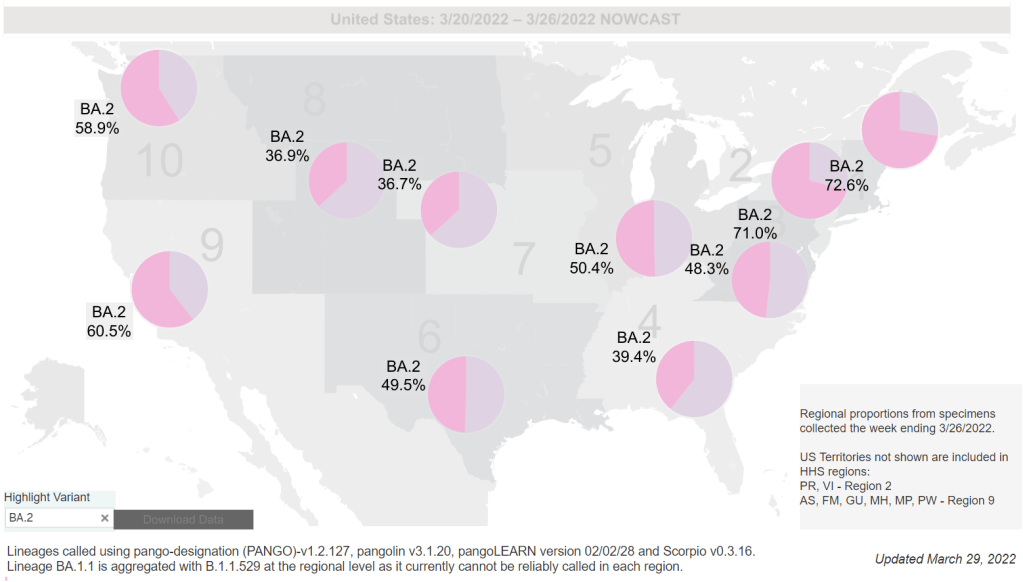
First of all, many U.S. experts consider case increases in Europe to be an early indicator of increases in the U.S. As I said at the top of the post, Europe is seeing a surge right now, and many of the countries reporting case increases have estimated over 50% of their cases are caused by BA.2.
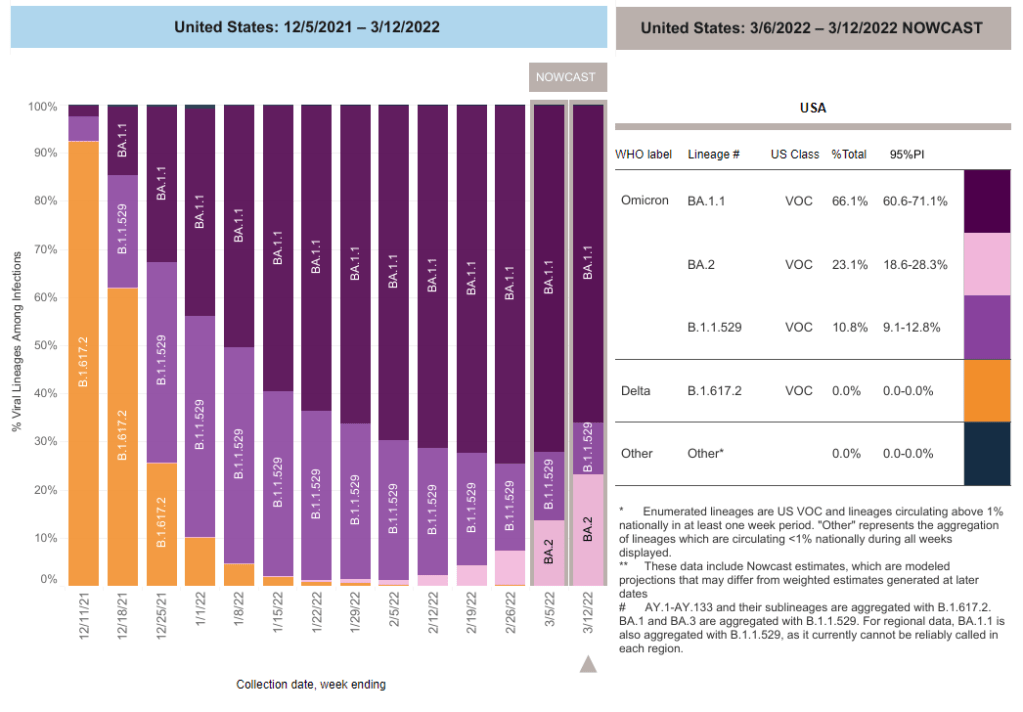
In the U.S., our BA.2 levels are lower: the CDC’s most recent estimates suggested that BA.2 was causing about 23% of new cases nationwide as of March 12. If BA.2 continues growing at the same rate we’ve seen in recent weeks, we have one or two more weeks before this variant hits 50% prevalence in the U.S.
“The tipping point seems to be right around 50%,” Keri Althoff, an epidemiologist at Johns Hopkins Bloomberg School of Public Health, told CNN. “That’s when we really start to see that variant flex its power in the population” as far as showing its severity.
At the same time, several Asian countries are also seeing major BA.2 surges at the moment. For example, Hong Kong was able to deal with early Omicron cases earlier in the winter, former COVID Tracking Project lead Erin Kissane pointed out in her Calm Covid newsletter; but now, the territory is facing a terrible BA.2 wave, driving what is now the world’s highest case fatality rate.
NEW: I’m not sure people appreciate quite how bad the Covid situation is in Hong Kong, nor what might be around the corner.
First, an astonishing chart.
After keeping Covid at bay for two years, Omicron has hit HK and New Zealand, but the outcomes could not be more different. pic.twitter.com/1Ol4HHs9kT
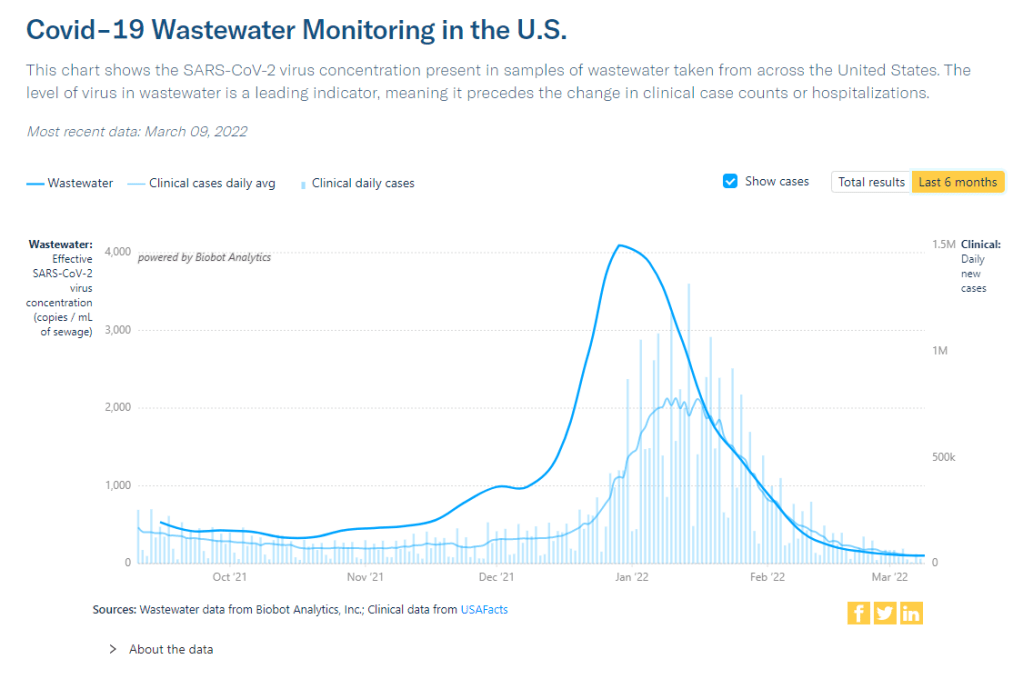
Here in the U.S., we’re also seeing warning signals in the form of rising coronavirus levels in wastewater. (Wastewater is considered an early indicator for surges, because coronavirus material often shows up in sewer systems before people begin to experience symptoms or get tested.) About one-third of sewershed collection sites in the CDC’s wastewater monitoring network are reporting increased virus prevalence in the two-week period ending March 15.
The CDC wastewater data must be interpreted cautiously, however, as this surveillance network is biased towards states like Missouri and Ohio, which have over 50 collection sites included in the national network. 12 states still do not have any collection sites in the network at all, while 23 states have fewer than 10. This recent Bloomberg article includes more context on interpreting wastewater data.
New York City is one place that’s reporting increased viral levels in wastewater, at the same time as the city health department reports that case numbers have plateaued—or may even be ticking up. An excellent time to loosen all mask and vaccination requirements, am I right?
What might a BA.2 surge in the U.S. look like?
Between the warning signals from Europe and the newly-lax safety measures throughout the U.S., it seems very likely that we will see a BA.2 surge in the coming weeks. The bigger question, though, is this surge’s severity: to what extent will it cause severe disease and death?
As I mentioned above, estimates suggest that about 40% to 45% of Americans have some Omicron antibodies from an infection earlier in the winter. At the same time, about 65% of the population is fully vaccinated and 45% of those fully vaccinated have received a booster shot, according to the CDC.
That’s a lot of people who are protected against severe COVID-19 symptoms, if they get infected with BA.2. But the U.S. has lower vaccination coverage than other countries, particularly when it comes to boosters. For example, in the U.K., 86% of eligible people are fully vaccinated and 67% are boosted, according to CNN. These lower vaccination rates contributed to the U.S.’s high mortality rate during the Omicron surge compared to other wealthy countries.
While the vaccines offer great protection, the U.S. appears to have given up on many other COVID-19 safety measures, like masks, social distancing, and limits on in-person gatherings. Without reinstating some of these measures, we would essentially be left without any tools to slow down the spread of BA.2; and even if some states and cities put safety measures in place, they’ll likely face more pushback now than they did in earlier surges.
To quote from Kissane’s newsletter:
In practical terms, with work and school happening in-person and without high-filtration (or any) masks or serious ventilation requirements in the US and most of Europe, governments in North America and Europe have made increased covid exposure essentially mandatory for most citizens.
I want to emphasize that for most vaccinated people, this increased risk probably won’t be a huge deal even if BA.2 causes a new case surge—they’ve either already racked up enough immunity to fight off BA.2 or they’ll be sick for a week.
One big caveat to this, though: we don’t have great data yet on how Omicron (or BA.2 specifically) might contribute to Long COVID rates; collecting data on this condition is very challenging and takes a lot of time. Studies suggest that vaccination reduces an individual’s risk of long-term symptoms if they get infected, but it does not eliminate this risk.
What can you do to prepare for this potential surge?
Here are a few things that I’m doing to prepare for a potential BA.2 surge in the coming weeks:
Promoting vaccination—particularly booster shots—to family members and friends.
Stocking up on good-quality masks (i.e. N95s and KN95s) and rapid tests. (Reminder, order a new round of free tests from covidtests.gov if you haven’t yet!)
Researching my options for COVID-19 treatments (antiviral pills and monoclonal antibodies) in the event that I get infected.
Getting tested frequently, particularly before attending indoor events (such as gathering with a few other friends, or going out to a movie theater.)
Watching wastewater and case trends in my area, and preparing to cut down on riskier behaviors if(/when) cases start rising.
I don’t know what BA.2 will mean for the US.
I do know this:
It hinges on vaccination/booster rates *now*.
So: 👆+
4th doses & Evusheld for immunocompromised ASAP, if not done.
Know where you’d get Paxlovid & Sotrovimab.
Order rapids now.
Get N95s or best possible now.
— Jeremy Faust MD MS (ER physician) (@jeremyfaust) March 16, 2022
As always, if you have any COVID-19 questions (about BA.2 or otherwise) that you’d like me to address, please reach out.
In the past week (March 12 through 18), the U.S. reported about 210,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 30,000 new cases each day
64 total new cases for every 100,000 Americans
17% fewer new cases than last week (March 5-11)
In the past week, the U.S. also reported about 16,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 2,300 new admissions each day
4.9 total admissions for every 100,000 Americans
27% fewer new admissions than last week
Additionally, the U.S. reported:
7,400 new COVID-19 deaths (2.2 for every 100,000 people)
100% of new cases are Omicron-caused; 23% BA.2-caused (as of March 12)
An average of 100,000 vaccinations per day (per Bloomberg)
National COVID-19 case numbers are still falling, as we reach two months since the peak of the Omicron surge. The U.S. reported about 30,000 new cases each day last week, according to the CDC; that’s the lowest this number has been since last summer.
Hospitalization and death numbers are also still falling. The CDC reports that only 2,300 new COVID-19 patients were admitted to U.S. hospitals each day last week, compared to almost ten times that number at Omicron’s peak. Hospital systems in all 50 states and D.C. are currently labeled as “having capacity” on the Circuit Breaker Dashboard.
While this is all good news, it’s unclear how long this lull in cases will last. BA.2, the Omicron sister strain, is slowly outcompeting the original variant thanks to its even-more-transmissible capabilities: it’s gone from causing about 2% of new COVID-19 cases nationwide in the week ending February 12 to causing 23% of new cases in the week ending March 12, according to CDC estimates.
This strain is wreaking havoc in Asia and Europe, and U.S. experts are concerned that we may see a new surge in the coming weeks. Wastewater data may also suggest an oncoming surge, as a growing number of sewershed collection sites are reporting increases in their coronavirus levels. (More on this later in the issue.)
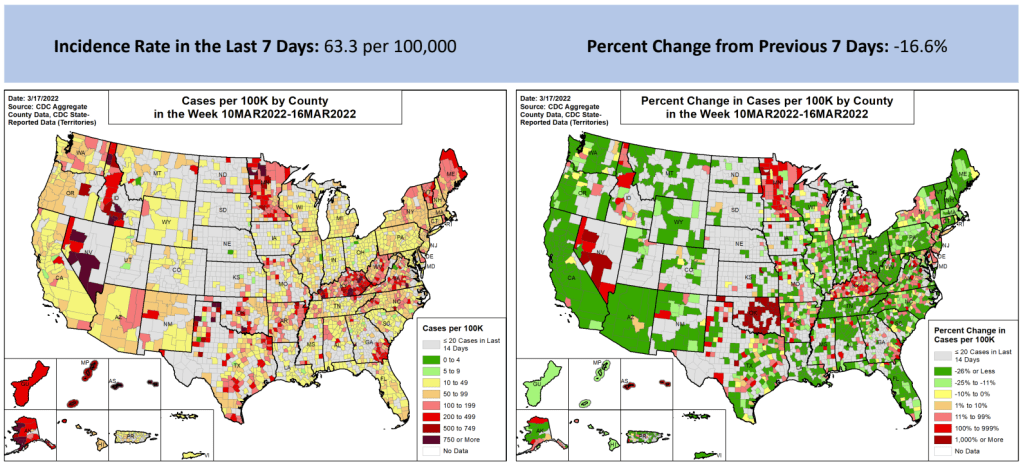
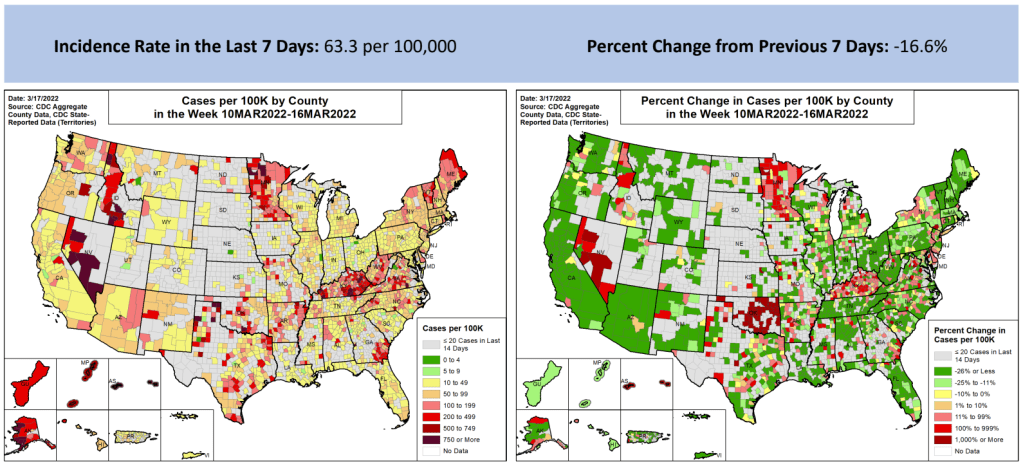
At the state level, a few places are beginning to see case increases: Washington, D.C., New York, Kentucky, Rhode Island, and Illinois all reported modest increases this week, according to the March 17 Community Profile Report. D.C. had the highest case increase, 20% more cases than the previous week. Some of these locations were also the first to be hit in the Omicron surge last December.
U.S. leaders should be taking advantage of this lull between surges to improve our preparedness: distribute masks and rapid tests, expand surveillance systems, and—most importantly—encourage people to get vaccinated so that they are protected when case rates rise again. Yet instead, Republicans in Congress are refusing to provide more public health funding, and the rate of Americans getting their first vaccine doses is lower than it has been since December 2020.
In the past week (March 5 through 11), the U.S. reported about 260,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 37,000 new cases each day
79 total new cases for every 100,000 Americans
29% fewer new cases than last week (February 26-March 4)
In the past week, the U.S. also reported about 22,000 new COVID-19 patients admitted to hospitals. This amounts to:
An average of 3,100 new admissions each day
6.6 total admissions for every 100,000 Americans
28% fewer new admissions than last week
Additionally, the U.S. reported:
8,200 new COVID-19 deaths (2.5 for every 100,000 people)
100% of new cases are Omicron-caused; 12% BA.2-caused (as of March 5)
An average of 100,000 vaccinations per day (per Bloomberg)
Note: I’m shifting the format of these National Numbers posts to focus more on hospitalizations and wastewater, as case data become both less reliable and less available in many parts of the U.S.
Overall, new COVID-19 cases are continuing to fall across the U.S. The country reported about 37,000 new cases a day last week, according to the CDC, compared to ten times that number in early February.
Case numbers have become less reliable lately as testing sites close and people are redirected to use at-home rapid tests, which are generally not reported. Still, we’re seeing a similar trend in new COVID-19 patients admitted to hospitals: both new cases and new admissions dropped almost 30% last week from the week prior.
More than 98% of the U.S. population now lives in a location with a low or medium COVID-19 Community Level, according to the CDC. But a few places did see case increases last week: these include Nebraska, Kentucky, Alaska, and Delaware, according to the March 10 Community Profile Report.
BA.2, the Omicron sister variant that is even more transmissible than the original version of this strain, is slowly gaining ground in the U.S.: it’s gone from causing an estimated 1% of cases in the first week of February to 12% in the first week of March, according to the CDC’s modeling.
It hasn’t impacted case trends here yet, but deserves close attention in the coming weeks and months. Gothamist has a helpful article about BA.2’s potential impact in New York, where the variant’s prevalence in wastewater is doubling statewide every two weeks.
Meanwhile, several European countries—including the U.K., Germany, the Netherlands, and others—reported case increases this week. This is likely due to ending pandemic safety measures, Omicron gaining its second wind, or some combination of the two; regardless, it doesn’t bode well for the U.S., which is also ending pretty much all pandemic safety measures.
The CDC is not publicly releasing a lot of its COVID-19 data. Last weekend, New York Times reporter Apoorva Mandavilli broke the news that the CDC has withheld a lot of its COVID-19 data from the public, including information on breakthrough cases, demographic data, and wastewater data. This news was honestly not surprising to me because it follows a pattern: the CDC doesn’t like to share information unless it can control the interpretations. But I appreciated the conversation brought on by this article, with public health experts saying they’d rather have imperfect data than a complete data void. (I agree!)
BA.2 is definitely more transmissible than the original Omicron strain, but it does not appear to be significantly more severe or more capable of evading vaccines. Two recent posts, one in the New York Times COVID-19 updates page and one from Your Local Epidemiologist, share some updates on what scientists have learned about BA.2 in the past couple of weeks. In the U.S. and other countries with BA.2, this sublineage doesn’t seem to be causing a major rise in cases—at least so far.
New CDC study shows the utility of rapid testing out of isolation. More than half of patients infected with the coronavirus tested positive on rapid antigen tests between five and nine days after their initial diagnosis or symptom onset, a new CDC report found. The report includes over 700 patients at a rural healthcare network in Alaska. These findings suggest that rapid testing out of isolation is a good way to avoid transmitting the virus to others, if one has the tests available.
January saw record-high coronavirus infections in hospitals.POLITICO reporters analyzed hospitalization data from the Department of Health and Human Services (HHS), finding that: “More than 3,000 hospitalized patients each week in January had caught Covid sometime during their stay, more than any point of the pandemic.” This high number demonstrates Omicron’s high capacity to infect other people.
Hong Kong’s surge shows the value of vaccinations. Hong Kong has been a global leader in keeping COVID-19 cases low throughout the pandemic, yet Omicron has tested this territory’s strategy—causing record cases and overwhelming hospitals. One major issue for Hong Kong has been low vaccination rates, particularly among the elderly, as people did not see the need to get vaccinated when cases in the territory were practically nonexistent.
In the past week (February 19 through 25), the U.S. reported about 526,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 75,000 new cases each day
160 total new cases for every 100,000 Americans
38% fewer new cases than last week (February 12-18)
Last week, America also saw:
42,000 new COVID-19 patients admitted to hospitals (13 for every 100,000 people)
12,000 new COVID-19 deaths (3.6 for every 100,000 people)
100% of new cases are Omicron-caused (as of February 19)
An average of 200,000 vaccinations per day (per Bloomberg)
The U.S. is now on week six of falling COVID-19 case numbers nationwide. New cases fell 38% from last week to this week, and are down 87% from one month ago. This is also the first week that the country has reported a daily new case average under 100,000 since early December.
Hospitalizations also continue to fall, with about 30% fewer new COVID-19 patients entering U.S. hospitals this week compared to last week. And death numbers have also begun to come down—though they are still high, with over 1,500 people dying of COVID-19 each day.
Case numbers are falling in every single U.S. state; five states and D.C. reported fewer than 100 new cases for every 100,000 residents in the past week, according to the latest Community Profile Report: Washington, Nebraska, Maryland, Nevada, and Ohio. Last week, Maryland was the first state to report case numbers below the CDC’s old high transmission threshold. (The new threshold is higher, which I’ll get into later this issue.)
To quote prolific COVID-19 data commentator (and my former COVID Tracking Project colleague) Conor Kelly, whose chart is featured above: “There’s not all that much interesting to report on with COVID data right now. Things are getting better fast everywhere. It’s just a question of how long it continues.”
That continuation depends largely on variants. As the Omicron surge recedes, how long will we see these decreases (or a plateau at low numbers) before a new variant drives another surge?
One key factor here is BA.2, the Omicron sub-lineage that has been slowly gaining ground in the U.S. over the past month as it is more transmissible than original Omicron. And I do mean slowly: according to CDC estimates, BA.2 went from causing an estimated 2% of new cases in the week ending February 12 to 4% in the week ending February 19. It seems to be having a limited impact on the country’s case decrease right now, but we’ll see if that changes in the coming weeks.
Meanwhile, America’s vaccination campaign is stalling. According to the Associated Press: “The average number of Americans getting their first shot is down to about 90,000 a day, the lowest point since the first few days of the U.S. vaccination campaign, in December 2020.” More investment into reaching people who remain unvaccinated (and unboosted) is necessary if we want to be prepared for potential future surges.
The majority of U.S. counties are still seeing high transmission, according to the CDC, but a few places like Maryland and New York City are starting to fall below this threshold.
In the past week (February 12 through 18), the U.S. reported about 850,000 new COVID-19 cases, according to the CDC. This amounts to:
An average of 122,000 new cases each day
259 total new cases for every 100,000 Americans
43% fewer new cases than last week (February 5-11)
Last week, America also saw:
60,000 new COVID-19 patients admitted to hospitals (18 for every 100,000 people)
14,000 new COVID-19 deaths (4.3 for every 100,000 people)
100% of new cases are Omicron-caused (as of February 12)
An average of 200,000 vaccinations per day (per Bloomberg)
New COVID-19 cases continue to drop in the U.S. as the country slowly comes down from its Omicron wave. This week, the country reported a total of 850,000 new cases, according to the CDC; it’s the first week under one million new cases have been reported since early December, though we are still seeing over 100,000 new cases a day.
Hospitalizations are also going down, with the Department of Health and Human Services reporting about 65,000 beds in use for confirmed and suspected COVID-19 patients as of Saturday. The hospital circuit breaker dashboard (by Jeremy Faust et al.) shows that the vast majority of U.S. hospitals have capacity, as of this week. Still, over 2,000 Americans continue to die of COVID-19 each day.
At the state level, we continue to see case decreases across the country. The one exception is Maine: this state saw a 350% increase in cases from last week to this week, according to the February 17 Community Profile Report. However, local reports suggest that a number of the new cases reported this week were backlogged—meaning the cases occurred weeks ago and were belatedly added to state tallies.
After over a month of falling case numbers nationwide, some parts of the country are finally dropping below the CDC’s high transmission threshold (100 new cases for every 100,000 residents reported in a week). Maryland is the first state to do this, with 92 new cases for every 100,000 residents reported in the week ending February 17.
New York City, where I live, also fell below the high transmission threshold this week, with 83 new cases for every 100,000 residents reported in the week ending February 15, according to city data. Both New York City and Maryland were early Omicron hotspots and have reported falling case numbers since early January.
While Omicron overall continues to cause 100% of new COVID-19 cases in the country, BA.2, the slightly-more-transmissible sister lineage, is starting to gain ground. The CDC estimates that BA.2 caused 3.9% of new cases in the week ending February 12, compared to 1.5% of new cases in the previous week. As BA.2 continues replacing original Omicron, we’ll see if this subvariant has an impact on the U.S.’s downward case trends.
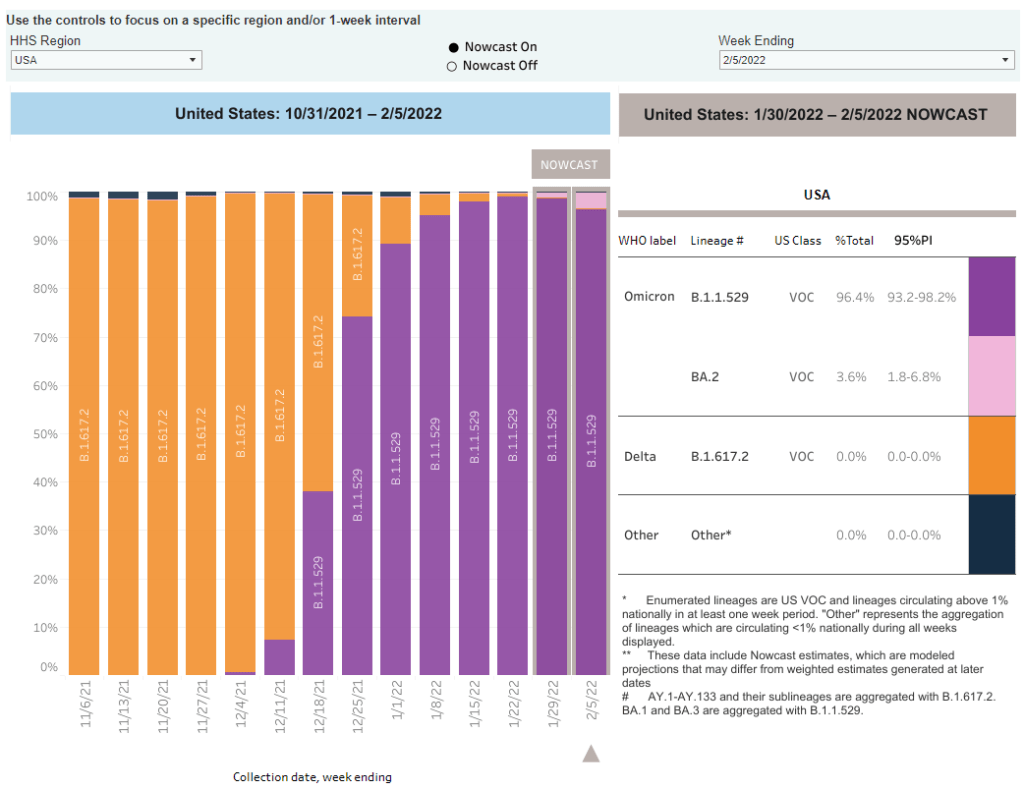
The CDC added BA.2 to its variant prevalence estimates. As I mentioned in today’s National Numbers post, the CDC is now splitting out its estimates of Omicron prevalence in the U.S. into original Omicron, also called B.1.1.529 or BA.1, and BA.2—a sister strain that’s capable of spreading faster than original Omicron. BA.2 has become the dominant variant in some parts of Europe and Asia, but seems to be present in the U.S. in fairly low numbers so far: the CDC estimates it caused about 3.6% of new cases nationwide in the week ending February 5, with a 95% confidence interval of 1.8% to 6.8%. The remainder of new cases last week were caused by original Omicron.
CDC describes its expanded genomic surveillance efforts in an MMWR study released this week. Between June 2021 and January 2022, the agency has extended its ability to monitor new variants spreading in the U.S., incorporating public repositories like GISAID into CDC data collection and developing modeling techniques that can produce more timely estimates of variant prevalence. (Remember: all variant data are weeks old, so the CDC uses modeling to predict the present.) According to the MMWR study, genomic sequencing capacity in the U.S. tripled from early 2021 to the second half of the year.
Vaccine effectiveness from a booster shot wanes several months after vaccination. In another MMWR study released this week, the CDC reports on mRNA vaccine effectiveness after two and three doses, based on data from a hospital network including hundreds of thousands of patients in 10 states. During the U.S.’s Omicron surge, researchers found, vaccine effectiveness against COVID-19 hospitalization was 91% two months after a third dose—but declined to 78% four months afterward. It’s unclear whether this declining effectiveness is a direct result of Omicron getting past the vaccine’s defenses, or whether we’d see similar declines with other variants. Also, the CDC’s findings are not stratified by age or other factors that make people more vulnerable to severe COVID-19.
Updated monoclonal antibody treatment from Eli Lilly gets FDA authorization. During the Omicron surge, one challenge for healthcare providers has been that, out of three monoclonal antibody treatments authorized by the FDA, only one retained effectiveness against this variant. (Monoclonal antibody treatments provide a boost to the immune system for vulnerable patients.) This week, however, the FDA authorized an updated version of Eli Lilly’s treatment that does work against Omicron, including against the BA.2 lineage. The federal government has purchased 600,000 courses of this new treatment.
More data released on South Africa’s mild Omicron wave. A new paper published in JAMA this week, from researchers at a healthcare provider in South Africa, compares COVID-19 hospitalizations during the Omicron surge to past surges. Among patients who visited the 49 hospitals in this provider’s network, about 41% of those who went to an emergency department with a positive COVID-19 test were admitted to the hospital during the Omicron surge—compared to almost 70% during South Africa’s prior surges. The paper provides additional evidence that Omicron is less likely to cause severe COVID-19 than past variants, though this likelihood is tied in part to high levels of vaccination and past infection in South Africa and other countries.
Omicron has been identified in white-tailed deer. New York City was an early Omicron hotspot in the U.S.; and the variant has been passed onto white-tailed deer in Staten Island, according to a new preprint posted this week (and not yet peer-reviewed). Scientists have previously identified coronavirus infections in 13 states, but finding Omicron is particularly concerning for researchers. “The circulation of the virus in deer provides opportunities for it to adapt and evolve,” Vivek Kapur, a veterinary microbiologist who was involved in the Staten Island study, told the New York Times.